Inpatient Glycemic Management Patients with Non-Critical
illness Approaches and Tools
Slide 3
Inpatient Glycemic Management Definition of terms: Hospital
hyperglycemia: Any BG > 140 mg/dl (7.8 mmol/L) Stress
hyperglycemia: Elevations in blood glucose levels that occur in
patients with no prior history of diabetes and A1c levels that are
not significantly elevated ( 140 mg/dl (7.8 mmol/L) Stress
hyperglycemia: Elevations in blood glucose levels that occur in
patients with no prior history of diabetes and A1c levels that are
not significantly elevated (
130 nonsurgical insulin-naive patients age 18-80 with known
type 2 diabetes admitted to noncritical care unit Randomly assigned
to sliding scale insulin (SSI) or a basal-bolus regimen with
glargine and glulisine 0.4 units per kg/day for BG 140-200 0.5
units per kg /day for BG > 200 50% given as glargine and 50% as
glulisine Oral antidiabetic drugs discontinued 2 hypoglycemic
events (BG < 60 mg/dl) in each group 130 nonsurgical
insulin-naive patients age 18-80 with known type 2 diabetes
admitted to noncritical care unit Randomly assigned to sliding
scale insulin (SSI) or a basal-bolus regimen with glargine and
glulisine 0.4 units per kg/day for BG 140-200 0.5 units per kg /day
for BG > 200 50% given as glargine and 50% as glulisine Oral
antidiabetic drugs discontinued 2 hypoglycemic events (BG < 60
mg/dl) in each group Randomized Study of Basal-Bolus Insulin
Therapy in the Inpatient Management of Patients With Type 2
Diabetes (RABBIT 2 Trial) Umpierrez et al. Diabetes Care. 30:2181
2007
Slide 18
*P
Adjusting scheduled insulin regimen If fasting and premeal BG
>140 mg/dl, dose of glargine increased by 20% For BG 140 mg/dl,
dose of glargine increased by 20% For BG
130 nonsurgical non-critically ill patients age 18-80 with
known type 2 diabetes admitted to noncritical care unit Half of
patients were receiving insulin prior to admission and received
similar outpatient insulin dose in the hospital Randomly assigned
to: Detemir once a day with premeal Aspart 3 times a day NPH and
regular twice a day before breakfast and dinner Dosing 0.4 units
per kg/day for BG 140-200 0.5 units per kg /day for BG > 200
Distribution of insulin Determir group: 50% given as detemir and
50% as aspart NPH group: 2/3 given as NPH and 1/3 as regular 130
nonsurgical non-critically ill patients age 18-80 with known type 2
diabetes admitted to noncritical care unit Half of patients were
receiving insulin prior to admission and received similar
outpatient insulin dose in the hospital Randomly assigned to:
Detemir once a day with premeal Aspart 3 times a day NPH and
regular twice a day before breakfast and dinner Dosing 0.4 units
per kg/day for BG 140-200 0.5 units per kg /day for BG > 200
Distribution of insulin Determir group: 50% given as detemir and
50% as aspart NPH group: 2/3 given as NPH and 1/3 as regular
Detemir with Aspart vs NPH with Regular Insulin Therapy in the
Inpatient Management of Patients With Type 2 Diabetes Umpierrez et
al. J Clin Endocrinol Metab. 94:564 2009 DEAN Trial
Slide 22
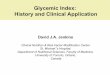
Changes in Mean Daily Glucose BG, mg/dL Duration of Therapy, d
Data are means SEM. Detemir + aspart NPH + regular Basal-bolus
regimen: detemir was given once daily; aspart was given before
meals. NPH/regular regimen: NPH and regular insulin were given
twice daily, two thirds in AM, one third in PM. Basal-bolus
regimen: detemir was given once daily; aspart was given before
meals. NPH/regular regimen: NPH and regular insulin were given
twice daily, two thirds in AM, one third in PM. Umpierrez GE, et
al. J Clin Endocrinol Metab. 2009;94(2):564-569. P=NS 100 120 140
160 180 200 220 240 Pre-Rx BG 0123456-10 DEAN Trial
Slide 23
Copyright 2009 The Endocrine Society Umpierrez, G. E. et al. J
Clin Endocrinol Metab 2009;94:564-569 Mean BG concentrations in
hospitalized patients treated with detemir/aspart or NPH/regular
Detemir/Aspart NPH/Regular DEAN Trial NPH/Regular BG < 40 mg/dl:
1.6% BG < 60 mg/dl: 25.4% NPH/Regular BG < 40 mg/dl: 1.6% BG
< 60 mg/dl: 25.4% Detemir/Aspart BG < 40 mg/dl: 4.5% BG <
60 mg/dl: 32.8% Detemir/Aspart BG < 40 mg/dl: 4.5% BG < 60
mg/dl: 32.8% B L D HS
Slide 24
Umpierrez et al, J Clin Endocrinol Metab 94: 564569, 2009 DEAN
Trial Treatment with basal/bolus regimen with detemir once daily
and aspart before meals results in equivalent glycemic control and
no differences in the frequency of hypoglycemia compared to a
split-mixed regimen of NPH and regular insulin in patients with
type 2 diabetes. Commentary NPH insulin was administered twice a
day in this study Detemir insulin was administered once a day It is
possible that detemir insulin may need to be administered twice a
day Commentary NPH insulin was administered twice a day in this
study Detemir insulin was administered once a day It is possible
that detemir insulin may need to be administered twice a day
Slide 25
*p-values are from Wilcoxon Two-Sample Test Risk Factors for
Hypoglycemia Umpierrez et al, ADA Scientific Meeting, Poster #516
p-value * VariableBG < 60 mg/dlBG < 70 mg/dl Age0.0360.001
Weight0.0270.001 A1C0.5210.658 Creatinine0.0110.002 Enrollment
BG0.1660.319 Previous treatment 0.005
Treatment Algorithm For Patients Receiving Continuous Enteral
Nutrition 2 BG > 130 mg/dl Continue current regimen 2 BG >180
mg/dl in prior 24 hours Add 25-50% Correction Insulin to Glargine
Administer regular insulin q6h 2 BG >180 mg/dl in prior 24 hours
Add 25-50% Correction Insulin to Glargine Administer regular
insulin q6h Glargine 10 units + Correction Insulin q6h Patient with
no prior history diabetes started on EN All BG < 130 mg/dl
Discontinue BG Monitoring BG < 130 mg/dl x 48 hrs
Slide 40
Alternative Treatment Algorithm For Patients Receiving
Continuous Enteral Nutrition 2 BG > 130 mg/dl Continue regimen 2
BG >180 mg/dl in prior 24 hours 1 BG > 250 mg/dl in prior 24
hours 2 BG >180 mg/dl in prior 24 hours 1 BG > 250 mg/dl in
prior 24 hours Initiate correction insulin q6h All BG < 180
mg/dl Discontinue BG Monitoring BG < 130 mg/dl x 48 hrs Patient
with no prior history diabetes started on EN Start Scheduled
Insulin Therapy
Slide 41
GlargineCI*P value Mean CBG during study mg/dl1633116130.75
Hypoglycemia/pt days %2.74.8.34 Hyperglycemia/pt days %49.347.6.77
Blood Glucose Data on Participants According to Group Korytkowski
M, Salata R, Koerbel G et al Diabetes Care 32:594, 2009 There were
no group differences in adverse events. *CI= correction
insulin
Slide 42
Summary 50% of eligible subjects for this study had no previous
history of type 2 diabetes or hyperglycemia Both glargine and
correction insulin (CI) (with the addition of NPH) were effective
at achieving glycemic control in these patients with careful
glucose monitoring and adjustments of the insulin regimen 13/25
patients randomized to correction insulin alone required NPH
insulin to achieve glycemic control No severe hypoglycemia events
occurred during this study 50% of eligible subjects for this study
had no previous history of type 2 diabetes or hyperglycemia Both
glargine and correction insulin (CI) (with the addition of NPH)
were effective at achieving glycemic control in these patients with
careful glucose monitoring and adjustments of the insulin regimen
13/25 patients randomized to correction insulin alone required NPH
insulin to achieve glycemic control No severe hypoglycemia events
occurred during this study Korytkowski M, Salata R, Koerbel G et al
Diabetes Care 32:594, 2009
Slide 43
Implications of this study Bedside glucose monitoring is
recommended for all hospitalized patients with and without a prior
history of diabetes with initiation or augmentation of enteral
nutrition. Glargine insulin is effective at achieving and
maintaining glycemic control in patients receiving both continuous
and intermittent enteral nutrition without increasing the risk for
hypoglycemia. Bedside glucose monitoring is recommended for all
hospitalized patients with and without a prior history of diabetes
with initiation or augmentation of enteral nutrition. Glargine
insulin is effective at achieving and maintaining glycemic control
in patients receiving both continuous and intermittent enteral
nutrition without increasing the risk for hypoglycemia. Korytkowski
M, Salata R, Koerbel G et al Diabetes Care 32:594, 2009
Slide 44
Glycemic Management of the Patient Receiving Enteral Nutrition
Continuous enteral nutrition (EN) Basal: 40-50% of TDD as long or
intermediate acting insulin given once twice a day Short acting
50-60% of TDD given q6h Cycled enteral nutrition Intermediate
acting insulin given together with a rapid or short acting insulin
with start of TF Rapid or short acting insulin administered q4 to 6
hours for duration of EN administration Correctional insulin given
for BG above goal range Bolus enteral nutrition Rapid acting analog
or short acting insulin given prior to each bolus Continuous
enteral nutrition (EN) Basal: 40-50% of TDD as long or intermediate
acting insulin given once twice a day Short acting 50-60% of TDD
given q6h Cycled enteral nutrition Intermediate acting insulin
given together with a rapid or short acting insulin with start of
TF Rapid or short acting insulin administered q4 to 6 hours for
duration of EN administration Correctional insulin given for BG
above goal range Bolus enteral nutrition Rapid acting analog or
short acting insulin given prior to each bolus
Slide 45
Glycemic Management of the Patient Receiving Enteral Nutrition
Suggested Dose of short acting insulin can be based on anticipated
dose of carbohydrate Example: 67 yo woman receiving Peptamin with
calculated 188 G of carbohydrate over 24 hrs Insulin to
carbohydrate ratio: 1 unit/10 G Calculated total insulin dose 19
units Administered total insulin dose over 24 h 20 units BG over 1
st 36 hours 90-135 mg/dl Suggested Dose of short acting insulin can
be based on anticipated dose of carbohydrate Example: 67 yo woman
receiving Peptamin with calculated 188 G of carbohydrate over 24
hrs Insulin to carbohydrate ratio: 1 unit/10 G Calculated total
insulin dose 19 units Administered total insulin dose over 24 h 20
units BG over 1 st 36 hours 90-135 mg/dl
Slide 46
Recommendations for Patients Receiving Parenteral and Enteral
Nutrition Initiate bedside capillary blood glucose (CBG) monitoring
for all patients receiving enteral nutrition (EN). Continue glucose
monitoring during upward (or downward) titrations of enteral
nutrition Initiate correctional insulin for any patient with CBG
levels > 140 mg/dL during EN. Consider use diabetes-specific
formulas in patients with pre-existing diabetes. Consider use of
Diabetes-specific formulas in patients with new onset or difficult
to control hyperglycemia. Initiate bedside capillary blood glucose
(CBG) monitoring for all patients receiving enteral nutrition (EN).
Continue glucose monitoring during upward (or downward) titrations
of enteral nutrition Initiate correctional insulin for any patient
with CBG levels > 140 mg/dL during EN. Consider use
diabetes-specific formulas in patients with pre-existing diabetes.
Consider use of Diabetes-specific formulas in patients with new
onset or difficult to control hyperglycemia.
Slide 47
Glycemic Management of the Patient Receiving Enteral Nutrition
Patients who already have an underlying diagnosis of diabetes are
likely to experience further elevations in blood glucose levels
with the initiation of enteral nutrition 1. Patients receiving EN
often have a higher severity of illness that those who do not.
Unanticipated dislodgement of a feeding tube, temporary
discontinuation of the feedings, or changes in the rate of
administration can result in hypoglycemia. Protocols for avoidance
and early treatment of hypoglycemia are recommended in case of
abrupt discontinuation of EN. For example: Keep order in place to
start dextrose-containing IVFs in event of abrupt discontinuation
of EN Patients who already have an underlying diagnosis of diabetes
are likely to experience further elevations in blood glucose levels
with the initiation of enteral nutrition 1. Patients receiving EN
often have a higher severity of illness that those who do not.
Unanticipated dislodgement of a feeding tube, temporary
discontinuation of the feedings, or changes in the rate of
administration can result in hypoglycemia. Protocols for avoidance
and early treatment of hypoglycemia are recommended in case of
abrupt discontinuation of EN. For example: Keep order in place to
start dextrose-containing IVFs in event of abrupt discontinuation
of EN
Slide 48
Enteral Nutritional Support and Use of Diabetes Specific
Formulas Standard formulas High in carbohydrate Low Fat Low fiber
Standard formulas High in carbohydrate Low Fat Low fiber Diabetes
Specific Formulas 3540% of calories from carbohydrate 15% of
calories from fructose 40-50% of calories from fat with a large
contribution from MUFAs (e.g. >60% of fat calories) Diabetes
Specific Formulas 3540% of calories from carbohydrate 15% of
calories from fructose 40-50% of calories from fat with a large
contribution from MUFAs (e.g. >60% of fat calories) Marinos et
al. Diabetes Care 28:2267 2005
Slide 49
Postprandial Rise in Blood Glucose and Type of EN Formula
Marinos et al Diabetes Care 28:2267 2005 N = 20 Hi MUFA fructose
fibre Peters 1989 N = 40 Hi MUFA fructose fibre Stanz Paris 1998 N
= 12 Hi MUFA fructose fibre Stanz Paris 1998 N = 61 Hi MUFA
fructose fibre Mesejo 2003 Meta analysis Long term N = 34 Hi MUFA
fructose fibre Craig 1998 N = 11 Hi MUFA fructose fibre del Carmen
Crespillo 2003 Meta analysis Short term Meta analysis All studies
Favors specific Favors Standard -6 -4 -2 0 2 4 6 Postprandial rise
in BG reduced by 18 mg/dl (1.03 mmol)
Slide 50
Peak Blood Glucose and Type of EN Formula Marinos et al
Diabetes Care 28:2267 2005 N = 24 Hi MUFA fructose fibre Hofman
2004 Meta analysis Favors specific Favors Standard -3 -2 -1 0 1 2 3
N = 20 Hi MUFA fructose fibre Hofman 2004 Postprandial rise in BG
reduced by 29 mg/dl (1.59 mmol)
Slide 51
Glycemic Management of the Patient Receiving TPN Usual method
Adding incremental doses of insulin to TPN based on previous days
requirement of correctional (sliding scale insulin) Other
(preferred?) Use of a separate IV insulin infusion titrated
according to bedside glucose levels There are no controlled trials
examining different strategies for achieving glycemic control in
this group of patients Usual method Adding incremental doses of
insulin to TPN based on previous days requirement of correctional
(sliding scale insulin) Other (preferred?) Use of a separate IV
insulin infusion titrated according to bedside glucose levels There
are no controlled trials examining different strategies for
achieving glycemic control in this group of patients
Slide 52
Glycemic Management of the Patient Receiving TPN Suggested In
patients with known type 2 diabetes, add 1 unit for each 10 Grams
of carbohydrate in the solution Initiate Correctional Insulin Scale
for BG > 140 mg/dl Add 60 to 100% of previous days correctional
insulin dose to next days TPN solution Consider Add basal long or
intermediate acting insulin at a dose of 0.2 to 0.4 units per kg
per day Suggested In patients with known type 2 diabetes, add 1
unit for each 10 Grams of carbohydrate in the solution Initiate
Correctional Insulin Scale for BG > 140 mg/dl Add 60 to 100% of
previous days correctional insulin dose to next days TPN solution
Consider Add basal long or intermediate acting insulin at a dose of
0.2 to 0.4 units per kg per day
Slide 53
Frequency of hyperglycemia in patients receiving high dose
steroids % % Donihi A et al Endocrine Practice 12:358, 296 > 1
BG > 200 mg/dl> 2 BG > 200 mg/dl 64 56 81 52 41 75 0 0 30
60 90 All No Hx DM Hx DM
Slide 54
Steroid Therapy and Inpatient Glycemic Control The majority of
patients receiving > 2 days of glucocorticoid therapy at a dose
equivalent of at least 40 mg per day of Prednisone developed
hyperglycemia No glucose monitoring was performed in 24% of
patients receiving high dose glucocorticoid therapy The majority of
patients receiving > 2 days of glucocorticoid therapy at a dose
equivalent of at least 40 mg per day of Prednisone developed
hyperglycemia No glucose monitoring was performed in 24% of
patients receiving high dose glucocorticoid therapy Donihi A et al
Endocrine Practice 12:358, 296
Slide 55
Risk for New Onset Diabetes with Glucocorticoid Therapy Clore
JN, Thurber-Hay L. Endocrine Practice 15:469 2009
Slide 56
One Suggested Approach for Treatment of Hyperglycemia in
Patients Receiving Glucocorticoid Therapy Clore JN, Thurber-Hay L.
Endocrine Practice 15:469 2009 Prednisone (mg/day)NPH
(units/kg/day)* > 400.4 300.3 200.2 100.1 *Administered in AM at
time of prednisone administration Glargine preferred if
dexamethasone used or Prednisone given twice a day *Administered in
AM at time of prednisone administration Glargine preferred if
dexamethasone used or Prednisone given twice a day
Slide 57
How do Steroids Differ in their Effects? Steroid Potency and
Duration of Action 20mg/d of prednisone ~= 80mg/d of hydrocortisone
~= 16mg/d of methylprednisolone ~= 3mg/d dexamethasone)
Glucocorticoid PotencyBiologic Half Life Hydrocortisone18-12 hours
Prednisone418-36 hours Methylprednisolone518-36 hours
Dexamethasone30-4036-54 hours
Slide 58
Steroid Therapy and Glycemic Control General Guidelines The
majority of patients (but not all) receiving high dose
glucocorticoid therapy will experience elevations in blood glucose
For patients without prior DM or hyperglycemia or those with
diabetes controlled with oral agents: Initiate glucose monitoring
with low dose correction insulin scale administered prior to meals
For patients previously treated with insulin Increase total daily
dose by 20 to 40% with start of high dose steroid therapy Increase
correctional insulin by one step (low to moderate dose) Adjust
insulin as needed to maintain glycemic control The majority of
patients (but not all) receiving high dose glucocorticoid therapy
will experience elevations in blood glucose For patients without
prior DM or hyperglycemia or those with diabetes controlled with
oral agents: Initiate glucose monitoring with low dose correction
insulin scale administered prior to meals For patients previously
treated with insulin Increase total daily dose by 20 to 40% with
start of high dose steroid therapy Increase correctional insulin by
one step (low to moderate dose) Adjust insulin as needed to
maintain glycemic control
Slide 59
IV Insulin Infusions may be required to maintain glycemic
control in some patients Steroid Therapy and Glycemic Control
General Guidelines
Slide 60
Glucocorticoid Therapy Suggested approach : Institute glucose
monitoring for at least 48 hours in all patients Prescribe insulin
therapy as needed according to results of bedside BG monitoring
During initiation and taper of steroid therapy, proactive
adjustment of insulin therapy can help avoid uncontrolled
hyperglycemia and hypoglycemia. Suggested approach : Institute
glucose monitoring for at least 48 hours in all patients Prescribe
insulin therapy as needed according to results of bedside BG
monitoring During initiation and taper of steroid therapy,
proactive adjustment of insulin therapy can help avoid uncontrolled
hyperglycemia and hypoglycemia.
Slide 61
Bromage et al. Surg Gynecol Obstet June 1971 Changes in Blood
Glucose During Surgery in Patients without Diabetes General
Anesthesia Epidural Anesthesia % Change in blood glucose 70%
Slide 62
Pre-Op Recommendations for Patients Admitted Day of Surgery
Oral Hypoglycemic Agents Withhold oral agents the morning of
surgery Insulin is necessary to control blood glucose in patients
with BG > 150 during surgery Oral agents can be resumed
postoperatively when Patient is reliably taking PO Risk of liver,
kidney and heart failure are minimized Withhold oral agents the
morning of surgery Insulin is necessary to control blood glucose in
patients with BG > 150 during surgery Oral agents can be resumed
postoperatively when Patient is reliably taking PO Risk of liver,
kidney and heart failure are minimized
Slide 63
Give at least 50 to 70 % of usual dose of NPH insulin and 70 to
100 % of detemir or glargine insulin For patients receiving premix
insulin (70/30 or 75/25), give 1/3 of total dose as NPH insulin
prior to the procedure For patients undergoing prolonged procedures
(e.g. CABG) hold SQ insulin and start IV insulin infusion Give at
least 50 to 70 % of usual dose of NPH insulin and 70 to 100 % of
detemir or glargine insulin For patients receiving premix insulin
(70/30 or 75/25), give 1/3 of total dose as NPH insulin prior to
the procedure For patients undergoing prolonged procedures (e.g.
CABG) hold SQ insulin and start IV insulin infusion Pre-op
Recommendations for Patients Admitted Day of Surgery Insulin
Treated Patients
Slide 64
Mucha et al. Diabetes Care 27:1209 2004 Study of Glargine
Insulin During Fasting in Subjects with Type 1 Diabetes Plasma
glucose mg/dl Fasting Control Usual dose of glargine insulin
administered while fasting or on another day in combination with
usual prandial insulin (Control) N = 15 This study suggests the
safety of administering a percentage of basal insulin when a
patient is made NPO.
Slide 65
DC insulin pump and change to IV insulin according to patients
current basal rate If basal rate < 1 unit/h, start IV insulin at
0.5 units/h h If basal rate 1-2 units/h, start IV insulin at 1
units/h Preoperative Recommendations Patients using insulin pump
therapy Hypoglycemia and hyperglycemia are treated in manner
similar to that of patients receiving SQ insulin pre-op
Slide 66
General Guidelines Inpatient use of U500 insulin is reserved
for patients who use this concentrated form of regular insulin as
outpatients and who demonstrate a similar or greater degree of
insulin resistance at time of hospital admission. To avoid dosing
errors that have potential for hypoglycemia, many hospitals
regulate the administration of U500 insulin by requiring one or all
of the following: Order written as volume to be given using a TB
syringe All doses prepared in pharmacy Alerts in patient room and
on patient medicine administration record General Guidelines
Inpatient use of U500 insulin is reserved for patients who use this
concentrated form of regular insulin as outpatients and who
demonstrate a similar or greater degree of insulin resistance at
time of hospital admission. To avoid dosing errors that have
potential for hypoglycemia, many hospitals regulate the
administration of U500 insulin by requiring one or all of the
following: Order written as volume to be given using a TB syringe
All doses prepared in pharmacy Alerts in patient room and on
patient medicine administration record Can U500 Regular Insulin Be
Used in the Hospital?
Slide 67
Management of Hyperglycemia in the Hospital and Patient Safety
Concern Both under and over-treatment of hyperglycemia create
safety concerns in hospitalized patients. Areas of risk: Changes in
carbohydrate or food intake Changes in clinical status or
medications Failure to adjust therapy based on BG patterns
Prolonged use of SSI as monotherapy Poor coordination of BG testing
with insulin administration and meal delivery Poor communication
during patient transfers Errors in order writing and transcription
Both under and over-treatment of hyperglycemia create safety
concerns in hospitalized patients. Areas of risk: Changes in
carbohydrate or food intake Changes in clinical status or
medications Failure to adjust therapy based on BG patterns
Prolonged use of SSI as monotherapy Poor coordination of BG testing
with insulin administration and meal delivery Poor communication
during patient transfers Errors in order writing and
transcription
Slide 68
Summary BG levels of 100-180 mg/dl are suggested for the
majority of non-critically ill patients Insulin therapy the
preferred method for achieving and maintaining glycemic control in
the hospital Scheduled SQ Basal Bolus insulin therapy is effective
and safe for treatment of hyperglycemia in non-critically ill
patients Correction insulin alone may be appropriate for periods of
< 24 to 48 hours in patients without a prior history of diabetes
or prior insulin therapy with initiation of therapies known to be
associated with high risk for hyperglycemia (TPN, EN, Steroids)
Prolonged monotherapy with correction insulin is inappropriate once
an insulin requirement is established with correction insulin
Proactive adjustments in the hypoglycemic regimen are required for
both initiation and tapering of steroid therapy BG levels of
100-180 mg/dl are suggested for the majority of non-critically ill
patients Insulin therapy the preferred method for achieving and
maintaining glycemic control in the hospital Scheduled SQ Basal
Bolus insulin therapy is effective and safe for treatment of
hyperglycemia in non-critically ill patients Correction insulin
alone may be appropriate for periods of < 24 to 48 hours in
patients without a prior history of diabetes or prior insulin
therapy with initiation of therapies known to be associated with
high risk for hyperglycemia (TPN, EN, Steroids) Prolonged
monotherapy with correction insulin is inappropriate once an
insulin requirement is established with correction insulin
Proactive adjustments in the hypoglycemic regimen are required for
both initiation and tapering of steroid therapy