Embed Size (px)
Citation preview

Inpatient Consultative Dermatology and Severe Cutaneous Adverse Reactions
Jeremy A. Schneider, MDAssistant Clinical Professor
UC San Diego Department of Dermatology

Objectives
• Brief overview of some of the most severe dermatologic conditions encountered in the inpatient setting, with a focus on DRESS/DIHS and SJS/TEN• Summarize the current data regarding the management of severe
cutaneous adverse reactions

Nightmare Fuel**not even close to comprehensive
• Infectious• Necrotizing fasciitis• Echthyma gangrenosum• Purpura fulminans, meningoccocemia• Rickettsial disease (e.g. RMSF)• Toxic shock syndrome
• Drug reactions• Stevens-Johnson Syndrome/Toxic Epidermal Necrolysis• Drug-induced hypersensitivity syndrome (DIHS)/Drug reaction with eosinophilia and systemic
symptoms (DRESS)• Immune reactions
• Graft-versus-host disease• Kawasaki disease (yes, even in adults)
• Malignancy• Sezary syndrome/CTCL
• Erythroderma (any etiology)
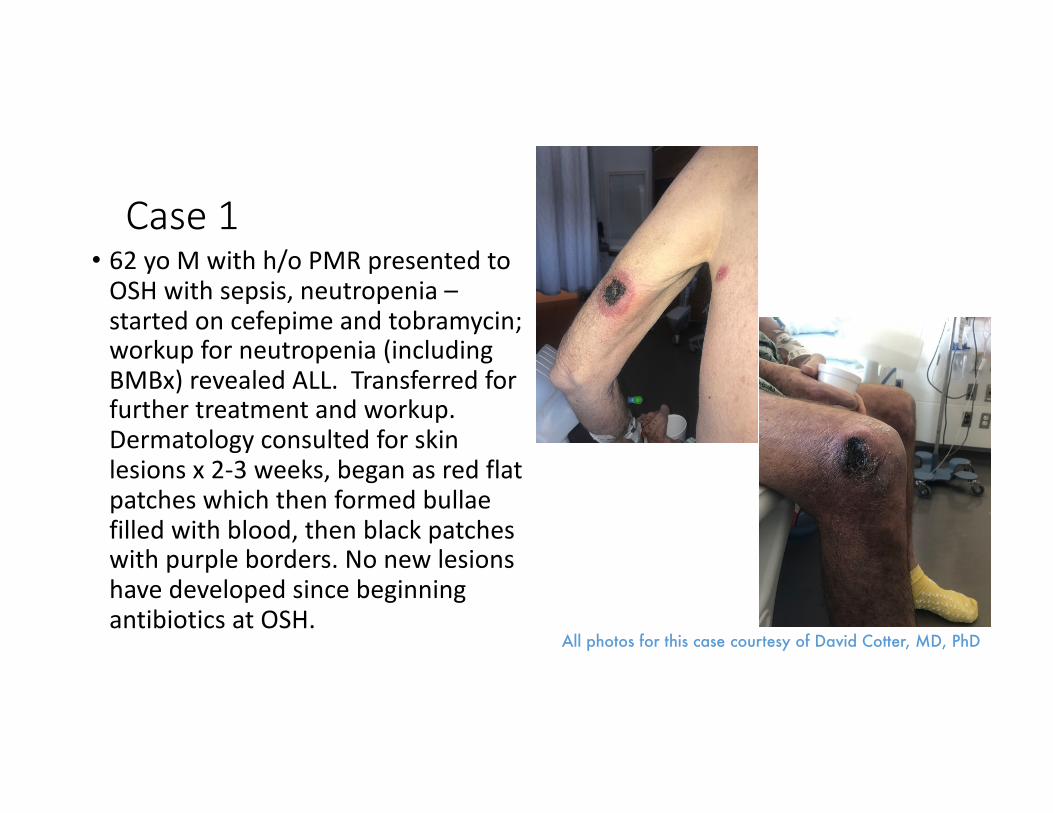
Case 1• 62 yo M with h/o PMR presented to
OSH with sepsis, neutropenia –started on cefepime and tobramycin; workup for neutropenia (including BMBx) revealed ALL. Transferred for further treatment and workup. Dermatology consulted for skin lesions x 2-3 weeks, began as red flat patches which then formed bullae filled with blood, then black patches with purple borders. No new lesions have developed since beginning antibiotics at OSH.
All photos for this case courtesy of David Cotter, MD, PhD

Case 1

What would the best next step(s) be?
A. Biopsy for H&E and tissue cultureB. Collect blood culturesC. Begin broad spectrum antimicrobial treatment, including
antipseudomonal agentD. Debride necrotic tissueE. Consult orthopedic surgeryF. A and BG. B and CH. A, B, and CI. All of the above

Echthyma gangrenosum
• Presentation: painless red macules -> induration -> pustules and/or bullae -> gangrenous ulcers (rapid progression 12-18 hours); most common sites: anogenital, axillary sites• Pathophysiology: perivascular bacterial invasion of media and
adventitia of arteries and veins, resulting in ischemic necrosis• P. aeruginosa most common but other organisms described,
including (but not limited to): P. stutzeri, Aeromonas spp, Stenotrophomonas spp, Citrobacter spp, MRSA, atypical mycobacteria, Fusarium spp, Candida spp
Echthyma gangrenosum
• Evaluation:• Prompt collection of blood cultures• Culture of exudates from aspirate or swab of lesions• If above are negative, biopsy for tissue culture (bacterial, fungal,
mycobacterial) can help exclude other etiologies• Management• Empiric antimicrobial coverage including agent with antipseudomonal
activity; tailor to culture results• Severe/extensive necrosis may require debridement +/- skin grafting
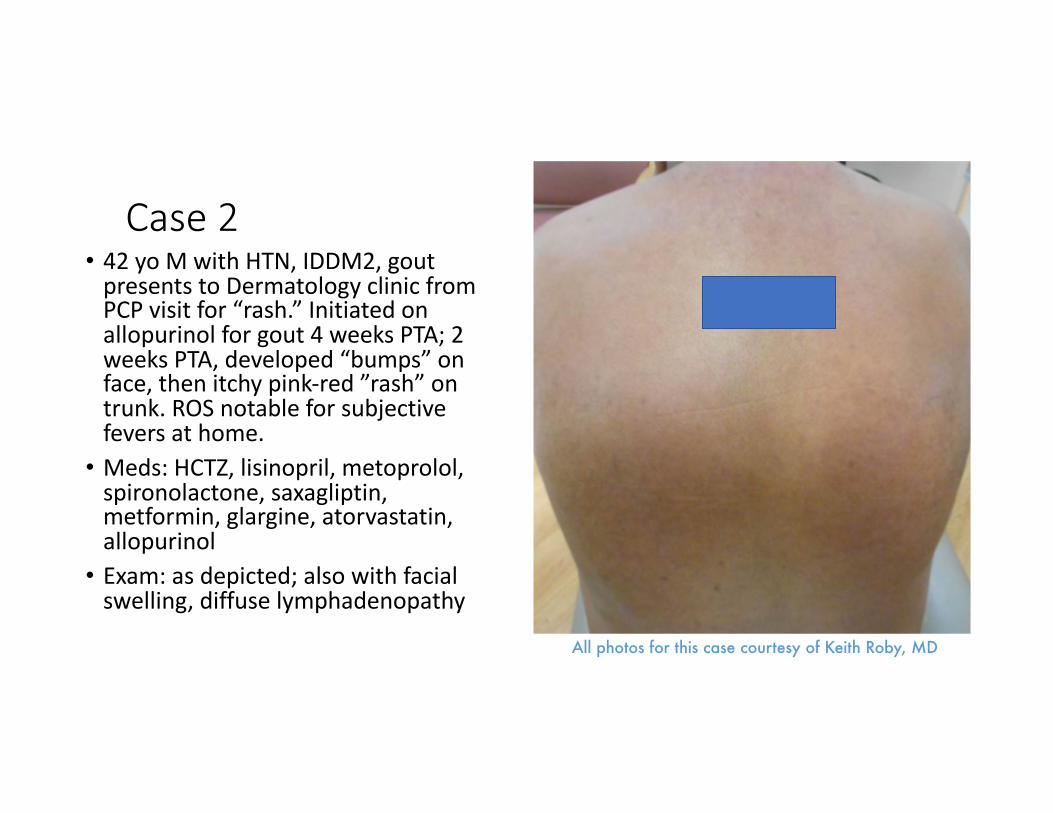
Case 2• 42 yo M with HTN, IDDM2, gout
presents to Dermatology clinic from PCP visit for “rash.” Initiated on
allopurinol for gout 4 weeks PTA; 2
weeks PTA, developed “bumps” on face, then itchy pink-red ”rash” on
trunk. ROS notable for subjective
fevers at home.
• Meds: HCTZ, lisinopril, metoprolol,
spironolactone, saxagliptin, metformin, glargine, atorvastatin,
allopurinol
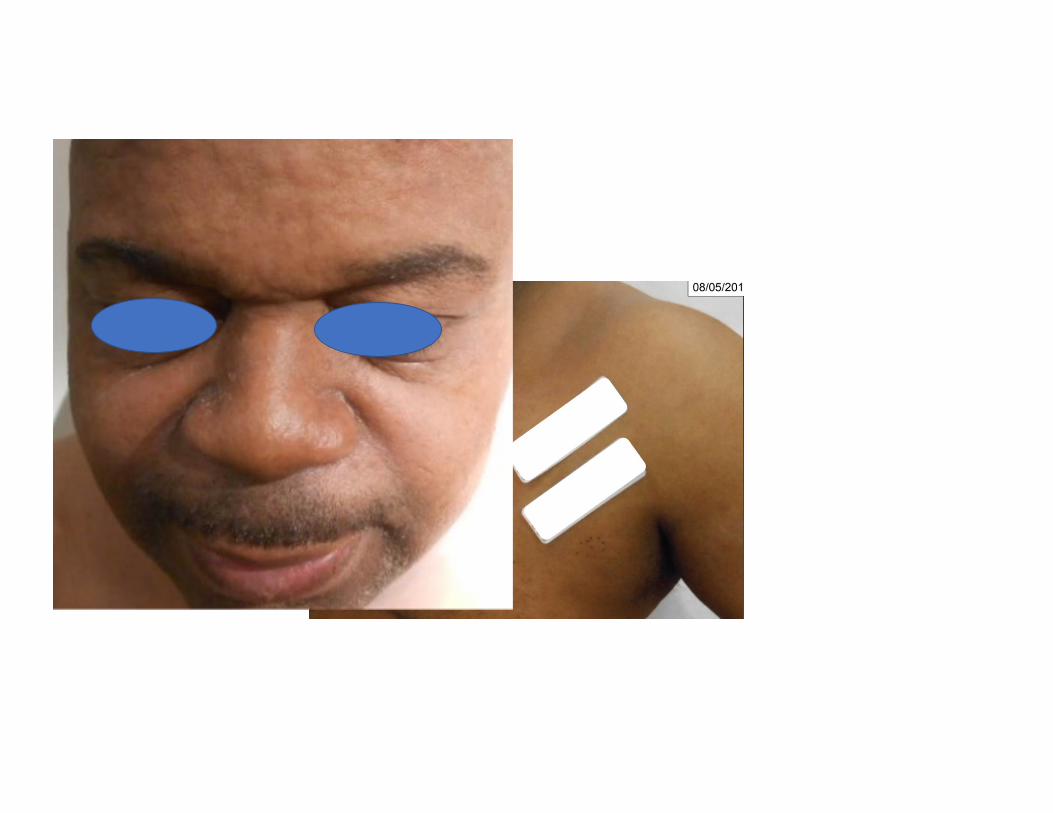
• Exam: as depicted; also with facial
swelling, diffuse lymphadenopathy
All photos for this case courtesy of Keith Roby, MD

What would be the next best step(s)?
A. Check CBC with manual diffB. Check CMP including LFTsC. Pulmonary imaging (CXR or CT chest)D. EKG and echocardiogram, serum troponinsE. Check a thyroid panelF. Check a CKG. Start IVIGH. Start high dose systemic corticosteroidsI. All of the above except GJ. All of the above except H

Day 3

Drug-induced hypersensitivity syndrome
• AKA Drug reaction with eosinophilia and systemic symptoms (DRESS)• Rash, fever, malaise, lymphadenopathy, facial edema,
hematologic abnormalities (eosinophilia, atypical lymphocytes), lymphadenopathy, liver, kidney, and/or lung involvement• Long latency between exposure and onset (2-8 weeks)• Strong activation of drug-specific T cells (CD8 , CD4 and T-regs);
role of viral reactivation unclear (cause or effect?) but frequent (HHV-6, HHV-7, EBV, CMV)

Table adapted from Kardaun et al. 2014.
Score -1 0 1 2 Min Max
Fever>/=38.5 C No/U Yes -1 0
Enlarged lymph nodes No/U Yes 0 1
Eosinophilia if leukocytes>4000 No/U 700-1499/uL
>/=1500/uL
0 2
Eosinophilia if leukocytes <4000 10-19.9% >/= 20% 0 2
Atypical lymphocytes No/U Yes 0 1
Skin involvement -2 2
Rash >50% No/U Yes
Rash suggesting DRESS No U Yes
Biopsy suggesting DRESS No Yes/U
Organ involvement 0 2
Liver No/U Yes
Kidney No/U Yes
Lung No/U Yes
Muscle/heart No/U Yes
Pancreas No/U Yes
Other organ(s) No/U Yes
Resolution >/=15 days No/U Yes -1 0
Evalutation other potential causes 0 1
ANA
Blood culture
Serology for HAV/HBV/HCV
Chlamydia-/Mycoplasma pneumoniae
Other serology/PCR
If none positive and 3 or more negative Yes
TOTAL SCORE -4 9
<2: no case; 2-3: possible; 4-5: probable; >5: definite
DIHS/DRESS Management
• Withdrawal of offending drug (and any nonessential medications)• Without systemic involvement or LFT elevation < 3 times ULN can
treat symptoms with high or super high potency topical corticosteroids• Patients with severe hepatitis should be promptly referred to
hepatologist as may evolve to ALF requiring transplantation• Severe interstitial nephritis or interstitial pneumonia, prednisone 0.5
to 2 mg/kg per day until clinical improvement/normalization of laboratory parameters; SLOW taper over 8-12 weeks

Case 3• 66 yo F with multiple myeloma and
NHL s/p R-CHOP x 6 cycles (completed 6 months PTA) and autologous SCT (1 month PTA) admitted for cough, nausea, decreased oral intake, and fever.Started treatment for CT finding of atypical PNA v aspiration. Dermatology consulted for “progressive rash” 1 week into admission. Patient and family report that, since admission, developed conjunctival injection followed by peeling skin on chest, shoulders, and then upper thighs. No oral or genital mucosal involvement.

What is your next step?A. Create medication timeline and discontinue culprit and nonessential medicationsB. Check quantitative immunoglobulins and initiate IVIG therapyC. Start cyclosporine therapyD. Check quantiferon TB test and start TNF-alpha inhibitorE. Start high dose corticosteroidsF. A and BG. A and CH. A and DI. A and EJ. A and adjunctive therapy will depend on patient’s comorbidities and
relative/absolute contraindications to individual therapeutic options

Med timeline:• Fluconazole (started 3 months prior to
rash)• Acyclovir (2.5 weeks prior to rash)• Sulfamethoxazole-trimethoprim (2.5
weeks prior to rash)• Azithromycin (3 weeks prior to rash)• Vancomycin (1-3 days prior to rash)• Cefepime (1-3 days prior to rash)• Ciprofloxacin (1 month prior to rash)• Moxifloxacin (started after rash)

Table from Schneider JA and Cohen PR. “Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis: A Concise Review with a Comprehensive Summary of Therapeutic Interventions Emphasizing Supportive Measures.” 2017.

Lessons learned
• Echthyma gangrenosum, while typically associated with Pseudomonas, can be caused by multiple other infectious agents• Severity of erythema may be underestimated in skin of color• DRESS/DIHS may progress to exfoliative and bullous lesions, which
may create diagnostic confusion• SCORTEN is most accurate on hospital days 1 and 3• Evidence-based management for severe cutaneous adverse reactions
continues to evolve• supportive care differs from that of burn patients with same BSA• adjunctive therapy should be tailored based on patient’s comorbidities/risk
factors
Acknowledgements

References• Chung WH, Hung SI, Yang JY, Su SC, Huang SP, Wei CY, Chin SW, Chiou CC, Chu SC, Ho HC, Yang CH, Lu CF, Wu JY, Liao YD, Chen YT. Granulysin is a key mediator for
disseminated keratinocyte death in Stevens-Johnson syndrome and toxic epidermal necrolysis. Nat Med. 2008;14(12):1343-50.
• Downey A, Jackson C, Harun N, Cooper A. Toxic epidermal necrolysis: review of pathogenesis and management. J Am Acad Dermatol. 2012;66:995-1003.
• Guegan S, Bastuji-Garin S, Poszepczynska-Guigne E, Roujeau JC, Revuz J. Performance of the SCORTEN during the first five days of hospitalization to predict the prognosis of epidermal necrolysis. J Invest Dermatol. 2006;126(2):272-6.
• Husain Z, Reddy BY, Schwartz RA. DRESS syndrome: Part I. Clinical perspectives. Journal of the American Academy of Dermatology. 2013 May 31;68(5):693-e1.
• Hazin R, Ibrahimi OA, Hazin MI, Kimyai-Asadi A. Stevens-Johnson syndrome: pathogenesis diagnosis, and management. Ann Med. 2008;40:129-38.
• Huang YC, Li YC, Chen TJ. The efficacy of intravenous immunoglobulin for the treatment of toxic epidermal necrolysis: a systematic review and meta-analysis. Br J Dermatol. 2012 Aug;167(2):424-32.
• Husain Z, Reddy BY, Schwartz RA. DRESS syndrome: Part II. Management and therapeutics. Journal of the American Academy of Dermatology. 2013 May 31;68(5):709-e1.
• Kardaun SH, Sidoroff A, Valeyrie-Allanore L, Halevy S, Davidovici BB, Mockenhaupt M, Roujeau JC. Variability in the clinical pattern of cutaneous side-effects of drugs with systemic symptoms: does a DRESS syndrome really exist?. British Journal of Dermatology. 2007 Mar 1;156(3):609-11.
• Kardaun SH, Mockenhaupt M, Roujeau JC. Comments on: DRESS syndrome. Journal of the American Academy of Dermatology. 2014 Nov 1;71(5):1000-.
• Kirchhof MG, Miliszewski MA, Sikora S, Papp A, Dutz JP. Retrospective review of Stevens-Johnson syndrome/toxic epidermal necrolysis treatment comparing intravenous immunoglobulin with cyclosporine. J Am Acad Dermatol. 2014;71(5):941.
• Kumar P and Kanti Das, N. Cyclosporine in toxic epidermal necrolysis: a brief review of the emerging therapeutic modality. Dermatol Online J. 2016;22(10).
References (continued)• Lee HY, Fook-Chong S, Koh HY, Thirumoorthy T, Pang SM. Cyclosporine treatment for Stevens-Johnson syndrome/toxic epidermal necrolysis: Retrospective analysis
of a cohort treated in a specialized referral center. J Am Acad Dermatol. 2017 Jan;76(1):106-113.
• Lee HY, Lim YL, Thirumoorthy T, Pang SM. The role of intravenous immunoglobulin in toxic epidermal necrolysis: a retrospective analysis of 64 patients managed in a specialized centre. Br J Dermatol. 2013 Dec;169(6):1304-9.
• Mayes T, Gottschlich M, Khoury J, Warner P, Kagan R. Energy requirements of pediatric patients with Stevens-Johnson syndrome and toxic epidermal necrolysis. Nutr Clin Pract. 2008;23(5):547.
• Roujeau JC, Bastuji-Garin S. Systematic review of treatments for Stevens-Johnson syndrome and toxic epidermal necrolysis using the SCORTEN score as a tool for evaluating mortality. Ther Adv Drug Saf. 2011;2(3):87.
• Sassolas B, Haddad C, Mockenhaupt M, Dunant A, Liss Y, Bork K, Haustein UF, Vieluf D, Roujeau JC, Le Louet H. ALDEN, an algorithm for assessment of drug causality in Stevens–Johnson syndrome and toxic epidermal necrolysis: comparison with case–control analysis. Clinical Pharmacology&Therapeutics. 2010 Jul 1;88(1):60-8.
• Schneck J, Fagot JP, Sekula P, Sassolas B, Roujeau JC, Mockenhaupt M. Effects of treatments on the mortality of Stevens-Johnson syndrome and toxic epidermal necrolysis: A retrospective study on patients included in the prospective EuroSCAR Study. J Am Acad Dermatol. 2008;58(1):33.
• Schneider JA, Cohen PR. Stevens-Johnson syndrome and toxic epidermal necrolysis: a concise review with a comprehensive summary of therapeutic interventions emphasizing supportive measures. Advances in therapy. 2017 Jun 1;34(6):1235-44.
• Shiga S, Cartotto R. What are the fluid requirements in toxic epidermal necrolysis? J Burn Care Res. 2010;31(1):100–4.
• Valeyrie-Allanore L, Wolkenstein P, Brochard L, Ortonne N, Maître B, Revuz J, Bagot M, Roujeau JC. Open trial of ciclosporin treatment for Stevens-Johnson syndrome and toxic epidermal necrolysis. Br J Dermatol. 2010;163(4):847.
• Wojtkiewicz A, Wysocki M, Fortuna J, Chrupek M, Matczuk M, Koltan A. Beneficial and rapid effect of infliximab on the course of toxic epidermal necrolysis. Acta Derm Venereol. 2008;88(4):420-1.
• Zárate-Correa LC, Carrillo-Gómez DC, Ramírez-Escobar AF, Serrano-Reyes C. Toxic epidermal necrolysis successfully treated with infliximab.





























