Embed Size (px)
Citation preview

Inhibición irreversible de EGFR: experiencia clínica en primera línea de tratamiento de CPNCP
EGFRmutado
Edurne ArriolaHospital del Mar
Barcelona

Inhibición de EGFR• Aproximadamente entre un 10‐15% de los pacientes con CPNCP tienen una mutación
en EGFR• La mayoría son mutaciones de sensibilidad, más frecuentes deleciones exon 19 y
mutación L858R exón 21• Gefitinib y más recientemente erlotinib aprobados en España para tratamiento en
primera línea
Mok et al. NEJM 2009; Rosell et al. Lancet Oncol. 2012

Afatinib is an orally available, irreversible ErbB FamilyBlocker, with high efficacy potential.
Inhibition of ErbB Family receptor heterodimerization
Li D, et al. Oncogene 2008;27:4702–11.
Afatinib: an irreversible ErbB Family Blocker

LUX‐Lung 3: a randomized, open‐label, Phase IIIstudy of afatinib vs cisplatin/pemetrexed as 1st‐linetreatment for patients with advancedadenocarcinoma of the lung harboring EGFR‐activating mutations
J.C.‐H. Yang, M. Schuler, N. Yamamoto, K. O’Byrne, V. Hirsh, T. Mok, S.L. Geater, S. Orlov, C.‐M. Tsai, M. Boyer, W.‐C. Su, J. Bennouna, T. Kato, V. Gorbunova, K.H. Lee, R. Shah, D. Massey, R. Lorence, M. Shahidi, L. Sequist, on behalf of all LUX‐Lung 3 investigators
Sequist et al., J Clin Oncol 31:3327–3334
Pivotal trial

Study design
Primary endpoint: PFS (RECIST 1.1, independent review)‡Secondary endpoints: ORR, DCR, DoR, tumor shrinkage, OS, PRO§, safety, PK
Randomization 2:1 Stratified by:
EGFR mutation (Del19/L858R/other) Race (Asian/non‐Asian)
Afatinib 40 mg/day†Cisplatin + Pemetrexed 75 mg/m2 + 500 mg/m2
i.v. q21 days, up to 6 cycles
Stage IIIB (wet)/IV lung adenocarcinoma (AJCC version 6)
EGFR mutation in tumor(central lab testing; Therascreen EGFR29* RGQ PCR)
*EGFR29:19 deletions in exon 19, 3 insertions in exon 20, L858R, L861Q, T790M, G719S, G719A and G719C (or G719X), S768I. †Dose escalated to 50 mg if limited AEobserved in cycle 1. Dose reduced by 10 mg decrements in case of related G3 or prolonged G2 AE.‡Tumor assessments: q6 weeks until Week 48 and q12 weeks thereafteruntil progression/start of new therapy. §Patient‐reported outcomes: Q‐5D, EORTC QLQ‐C30 and QLQ‐LC13 at randomization and q3 weeks until progression or new anti‐cancer therapy. Sequist et al., J Clin Oncol 31:3327–3334. Yang et al., ASCO 2012

Primary endpoint: PFS Progression‐free
survival (prob
ability)
1.0
0.8
0.6
0.4
0.2
0.0
Number at riskAfatinib 230 180 151 120 77 50 31 10 3 0Cis/Pem 115 72 41 21 11 7 3 2 0 0
Progression‐free survival (months)0 3 6 9 12 15 18 21 24 27
Afatinib n=230
Cis/pem n=115
PFS event, n (%) 152 (66) 69 (60)
Median PFS (months) 11.1 6.9
Hazard ratio(95% confidence interval)
0.58 (0.43–0.78)p=0.0004
47%
22%
Independent review ‒ all randomized patients
Sequist et al., J Clin Oncol 31:3327–3334. Yang et al., ASCO 2012

Progression‐free
survival (prob
ability)
1.0
0.8
0.6
0.4
0.2
0.0
Number at riskAfatinib 204 169 143 115 75 49 30 10 3 0Cis/Pem 104 62 35 17 9 6 2 2 0 0
Progression‐free survival (months)0 3 6 9 12 15 18 21 24 27
Afatinib n=204
Cis/pem n=104
PFS event, n (%) 130 (64) 61 (59)
Median PFS (months) 13.6 6.9
Hazard ratio(95% confidence interval)
0.47 (0.34–0.65)p<0.0001
PFS: Common mutations (Del19/L858R)
Independent review (n=308)
51%
21%

Gemcitabine/Cisplatin 1000 mg/m2 D1, D8 + 75 mg/m2
IV q21 days, up to 6 cyclesAfatinib 40 mg/day†
Cisplatin/Pemetrexed 75 mg/m2 + 500 mg/m2
IV q21 days, up to 6 cycles
Stage IIIB (wet)/IV lung adenocarcinomaEGFR mutation in tumour
(central lab testing; Therascreen EGFR29* RGQ PCR)
LUX‐Lung 31 LUX‐Lung 62 (Asian pts)
Randomisation 2:1 Stratified by:
EGFR mutation (Del19/L858R/other)
Primary endpoint: PFS (RECIST 1.1, independent review)‡Secondary endpoints: ORR, DCR, DoR, tumour shrinkage, OS, PRO§, safety
*EGFR29: 19 deletions in exon 19, 3 insertions in exon 20, L858R, L861Q, T790M, G719S, G719A and G719C (or G719X), S768I. †Dose escalated to 50 mg iflimited AE observed in cycle 1. Dose reduced by 10‐mg decrements in case of related G3 or prolonged G2 AE. ‡Tumour assessments: q6 weeks until Week 48and q12 weeks thereafter until progression/start of new therapy. §Patient‐reported outcomes: EQ‐5D, EORTC QLQ‐C30 and LC 13 at randomisation and q3weeks until progression or new anti‐cancer therapy. 1. Sequist LV, et al. J Clin Oncol. 2013;31:3327‐3334. 2. Wu Y‐L, et al. Abstract 8016. Poster presented atASCO 2013.
LUX‐Lung 3 and Lux‐Lung 6: Study design

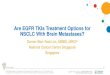
Primary endpoint: PFS LL3 & 6 superimposed Progression‐free
survival (prob
ability)
1.0
0.8
0.6
0.4
0.2
0.0
Number at riskAfatinib 230 180 151 120 77 50 31 10 3 0Cis/Pem 115 72 41 21 11 7 3 2 0 0Afatinib 242 208 166 126 89 60 35 12 4 0Cis/Gem 122 70 25 8 1 0 0 0 0 0
Progression‐free survival (months)0 3 6 9 12 15 18 21 24 27
47%
22%
Independent review ‒ all randomized patients
2%
LUX‐Lung 3, n=345
(A vs Pem/Cis )
LUX‐Lung 6, n=364(A vs Gem/Cis)
Median PFS 11.1 vs 6.9 11.0 vs 5.6
HR for PFS 0.58 0.28
12 months PFS
47% vs 22% 47% vs 2%
Sequist et al., J Clin Oncol 31:3327–3334. Yang et al., ASCO 2012

Secondary Endpoints: Response and Disease Control
Independent Review
LUX‐Lung 31 LUX‐Lung 62
Afatinib n=230
Cis/Pemn=115
Afatinib n=242
Gem/Cisn=122
Objective response (CR+PR), % 56 23 67 23
Disease control (CR+PR+SD), % 90 81 93 76
Median duration of response, months (95% CI)
11.1(8.5, 12.6)
5.5 (4.1, 8.3)
9.7 ( 8.3, 12.5)
4.3 ( 2.8, 5.8)
Median duration of disease control, months (95% CI)
13.6 (10.8, 13.8)
8.1 (6.7, 9.5)
11.1 ( 9.7, 13.8)
5.7 ( 5.5, 6.9)
1. Sequist LV, et al. J Clin Oncol. 2013;31:3327‐3334.2. Wu Y‐L, et al. Abstract 8016. Poster presented at ASCO 2013.

Adverse Event Overall SummaryLUX‐Lung 3 LUX‐Lung 6
Patients with Afatinibn= 229 (%)
Pem/Cisn=111 (%)
AfatinibN=239 (%)
Gem/CisN=113 (%)
Any AE 100 98 100 99
Drug‐related AEs 100 96 99 99
Any AEs grade ≥ 3 61 57 47 62
Drug‐related AE grade ≥ 3 49 48 36 60
AEs leading to dose reduction 52 16* 32 27*
AEs leading to discontinuation of treatment
14 15 10 40
Drug‐related AEs leading to discontinuation
8 12 6 40
SAE 29 23 15 11
Drug‐related SAE 14 14 6 7
AE leading to death 6 3 6 3
Related AE leading to death 1.7 (4pt) 0 0.4 (1pt) 0.9 (1pt)1. Sequist LV, et al. J Clin Oncol. 2013;31:3327‐3334.
2. Wu Y‐L, et al. Abstract 8016. Poster presented at ASCO 2013.

Most frequent related AEs with afatinib LL3: Afatinib n=229 (%) LL6: Afatinib n =239 (%)
All g3 g4 All g3 g4
Diarrhoea 95 14 88 5
Rash/acne* 89 16 81 14 0.4
Stomatitis/mucositis* 72 8 0.4 52 5
Paronychia 57 11 34
ALT increase 7 0.4 20 2
AST increase 5 0.4 15 0.4
Epistaxis 13 13 0.4
Pruritus 19 0.4 11 0.4
Decreased appetite 21 3 10 1
Fatigue* 18 1 10 0.4
Ocular* 18 0.4 6
Dry skin 29 0.4 5
Cheilitis 12 0 3
* Grouped
term
1. Sequist LV, et al. J Clin Oncol. 2013;31:3327‐3334.2.

Time to symptom deterioration
First‐line afatinib significantly delayed time to deterioration for cough and dyspnoea
Time to deterioration for pain favoured afatinib (HR=0.83; p=0.1913)
Cough Dyspnoea
Sequist et al., J Clin Oncol 31:3327–3334. Yang et al., ASCO 2012. James Chih‐Hsin Yang et al., J Clin Oncol 2013 Sep 20;31(27):3342‐3350

SummaryLUX‐Lung 3 is the largest global prospective trial in EGFR mutation‐positive lung cancer andthe first using cisplatin and pemetrexed as the comparator
LUX‐Lung 3met its primary endpoint of PFS (independent review)
⁻Overall study population: Median PFS of 11.1 months for afatinib; 6.9 months for chemotherapy (HR=0.58 [95% CI:0.43–0.78]; p=0.0004)⁻Patients with common mutations (Del19+L858R): Median PFS of 13.6 months for afatinib; 6.9 months for chemotherapy(HR=0.47 [95% CI: 0.34–0.65]; p<0.0001)⁻Consistent efficacy in all relevant subgroups.
Afatinib significantly improved rates of response and disease control versuschemotherapy.
Safety profile consistent with previous afatinib studies. Diarrhea and rash were the mostfrequent AEs; manageable with low treatment discontinuation rate.
First‐line afatinib significantly prolonged PFS with associated delay in worsening of lungcancer‐related symptoms and improvement in quality of life in EGFR mutation‐positive lungadenocarcinoma patients.
Sequist et al., J Clin Oncol 31:3327–3334. Yang et al., ASCO 2012. James Chih‐Hsin Yang et al., J Clin Oncol 2013 Sep 20;31(27):3342‐3350

Indication
Giotrif as monotherapy is indicated for thetreatment of EGFR TKI‐naïve adult patients withlocally advanced or metastatic NSCLC withactivating EGFR mutations.
http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Product_Information/human/002280/WC500152392.pdf

Caso clínico•Paciente mujer de 70 años•Antecedentes patológicos:•HTA en tratamiento con valsartan•Diabetes mellitus con metformina 850mg 0‐1‐1•Dislipemia en tratamiento con simvastatina 10 mg/d

Primer síntoma:• Abril 2013: •Disnea de medianos esfuerzos progresiva
• Rx tórax(3/6/13):• Condensación lóbulo inferior derecho: antibiótico
• Ante la no mejoría se deriva a nuestro centro al circuito de diagnóstico rápido de cáncer de pulmón
17

Analítica y TC:• Analítica (25/07/2013): normal.• TC toráx‐abdomen superior (04/07/2013): Ocupación del espacio aéreo en pulmon derecho por parte de componente solido todo indicativo de proceso neoformativo tipo adenocarcinoma como primera opción. No se aprecian adenopatias ni claras lesiones secundarias. El estadiaje TC seria T4 N0 M0 asociado a presencia de probable linfangitis
18

PET/TC:• PET (29/07/2013): lesión hipermetabólica (SUV 8) pulmonar derecha con afectación del LM, LID y probablemente del LSD sugestiva de un proceso neoproliferativo primario.
19

FBS y AP:• PFR (25/07/2013): FEV1 57% ref., FEV1 910 ml; DLCO 56% ref., KCO 71% ref.).
• BRONCOFIBROSCÒPIA (31/07/2013): estenosis concéntrica sin infiltración del bronquio lobar inferior derecho. BAS, cepillado bronquial i biopsias transbronquiales.
• AP: Adenocarcinoma con patrón de crecimiento predominantemente acinar
• EGFRmutación exón 19 (E746_S752delinsV).
20

Tratamiento:• Agosto 2013: Inicia afatinib 40mg/día• Síntomas:•Resolución de la disnea, ECOG PS:0
• Toxicidades:•Rash cutáneo G1•Mucositis G2•Diarreas G2
• Disminución dosis afatinib a 30mg/24• Desde entonces, resolución toxicidades
21

Pre afatinib Post afatinib

Seguimiento:• Marzo 2014: Último control clínico y por TC•Asintomática•No toxicidades•No evidencia de progresión
23