-
Cancer Therapy: Preclinical
Tyrosine Phosphoproteomics Identifies Both Codrivers
andCotargeting Strategies for T790M-Related EGFR-TKIResistance in
Non–Small Cell Lung Cancer
Takeshi Yoshida1,5, Guolin Zhang1, Matthew A. Smith1, Alex S.
Lopez2, Yun Bai1, Jiannong Li1, Bin Fang3,John Koomen3, Bhupendra
Rawal4, Kate J. Fisher4, Ann Y. Chen4, Michiko Kitano5, Yume
Morita5,Haruka Yamaguchi5, Kiyoko Shibata5, Takafumi Okabe5, Isamu
Okamoto5, Kazuhiko Nakagawa5, andEric B. Haura1
AbstractPurpose: Irreversible EGFR-tyrosine kinase inhibitors
(TKI) are thought to be one strategy to overcome
EGFR-TKI resistance induced by T790M gatekeeper mutations in
non–small cell lung cancer (NSCLC), yet
they display limited clinical efficacy.Wehypothesized that
additional resistancemechanisms that cooperate
with T790M could be identified by profiling tyrosine
phosphorylation in NSCLC cells with acquired
resistance to reversible EGFR-TKI and harboring T790M.
Experimental Design: We profiled PC9 cells with TKI-sensitive
EGFR mutation and paired EGFR-TKI–
resistant PC9GR (gefitinib-resistant) cells with T790M using
immunoaffinity purification of tyrosine-
phosphorylated peptides and mass spectrometry–based
identification/quantification. Profiles of erlotinib
perturbations were examined.
Results:We observed a large fraction of the tyrosine
phosphoproteome was more abundant in PC9- and
PC9GR-erlotinib–treated cells, including phosphopeptides
corresponding to MET, IGF, and AXL signaling.
Activation of these receptor tyrosine kinases by growth factors
could protect PC9GR cells against the
irreversible EGFR-TKI afatinib. We identified a Src family
kinase (SFK) network as EGFR-independent and
confirmed that neither erlotinib nor afatinib affected Src
phosphorylation at the activation site. The SFK
inhibitor dasatinib plus afatinib abolished Src phosphorylation
and completely suppressed downstream
phosphorylated Akt and Erk. Dasatinib further enhanced antitumor
activity of afatinib or T790M-selective
EGFR-TKI (WZ4006) in proliferation and apoptosis assays in
multiple NSCLC cell lines with T790M-
mediated resistance. This translated into tumor regression in
PC9GR xenograft studies with combined
afatinib and dasatinib.
Conclusions: Our results identified both codrivers of resistance
along with T790M and support further
studies of irreversible or T790M-selective EGFR inhibitors
combinedwith dasatinib in patients withNSCLC
with acquired T790M. Clin Cancer Res; 20(15); 4059–74. �2014
AACR.
IntroductionDespite the benefits shown with EGFR-tyrosine
kinase
inhibitor (EGFR-TKI) treatment in patients with non–small
cell lung cancer (NSCLC) with TKI-sensitive EGFR muta-tions (1,
2), acquired resistance is a critical clinical problem.A secondary
point mutation in exon 20 of EGFR thatsubstitutesmethionine for
threonine at aminoacid position790 (T790M) was identified in
patients with NSCLC whodeveloped acquired resistance to gefitinib
or erlotinib (3, 4).Nearly 50% of patients with NSCLC with acquired
resis-tance to EGFR-TKIs have the T790M secondary mutation(5–7).
Irreversible EGFR-TKIs, such as CL387,785 (8),PF00299804 (9),
BIBW-2992 (afatinib; ref. 10), and HKI-272 (11), are thought to be
one strategy to overcomeT790M-induced resistance. However, a number
of studieshave shown their limited activity in cells with
T790Mmutations given the increased affinity of ATP binding toT790M
EGFR proteins or through mechanisms affectingother pathways such as
MET activation (8, 9, 12–18).Clinical studies have also highlighted
the limited efficacyof irreversible EGFR-TKIs. In the LUX-Lung 1
Trial,
Authors' Affiliations: 1Department of Thoracic Oncology, 2Tissue
Core,3Proteomics and Molecular Oncology Program, 4Biostatistics
Program, H.Lee Moffitt Cancer Center and Research Institute, Tampa,
Florida; and5Department of Medical Oncology, Kinki University
Faculty of Medicine,Osaka-Sayama, Osaka, Japan
Note: Supplementary data for this article are available at
Clinical CancerResearch Online
(http://clincancerres.aacrjournals.org/).
T. Yoshida and G. Zhang contributed equally to this article.
Corresponding Author: Eric B. Haura, Department of Thoracic
Oncology,H. LeeMoffitt Cancer Center andResearch Institute,
12902Magnolia Drive,Tampa, FL 33612. Phone: 181-3745-6827; Fax:
181-3745-6817; E-mail:[email protected]
doi: 10.1158/1078-0432.CCR-13-1559
�2014 American Association for Cancer Research.
ClinicalCancer
Research
www.aacrjournals.org 4059
on June 19, 2021. © 2014 American Association for Cancer
Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst June 11, 2014; DOI:
10.1158/1078-0432.CCR-13-1559
on June 19, 2021. © 2014 American Association for Cancer
Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst June 11, 2014; DOI:
10.1158/1078-0432.CCR-13-1559
on June 19, 2021. © 2014 American Association for Cancer
Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst June 11, 2014; DOI:
10.1158/1078-0432.CCR-13-1559
http://clincancerres.aacrjournals.org/http://clincancerres.aacrjournals.org/http://clincancerres.aacrjournals.org/
-
conducted to compare afatinib treatment versus placebo
inpatients with advanced NSCLC whose disease progressedafter
receiving first-generation EGFR-TKIs (erlotinib, gefiti-nib),
afatinib did not extend the primary endpoint ofoverall survival
despite significant improvements in pro-gression-free survival
(19). These preclinical and clinicalresults suggest that
irreversible EGFR-TKIs as single agentsare insufficient to overcome
resistance.
One strategy to improve on the limited efficacy of irre-versible
EGFR-TKI is through combination with other path-way inhibitors. For
example, studies that combined afatinibwith the anti-EGFR
monoclonal antibody cetuximab (20)or the PI3K/mTOR inhibitor PI-103
(12) and HKI-272combined with mTOR inhibitor rapamycin (21)
haveshown promise in overcoming T790M resistance. Anotherreason for
the limited efficacy of agents targeting T790Mcould be mediated
through other tyrosine kinases, such asreceptor tyrosine kinases
(RTK), which provide additionalprotection against EGFR-TKIs (22).
Recent studies haveshown that growth factor ligands can protect
oncogene-addicted cells from molecularly targeted agents;
thus,altered expression of these growth factor receptors
couldfurther identify resistance pathways (23–25).
We explored the underlying ability of some growth factorligands
to drive resistance to TKIs by examining the basaltyrosine
phosphoproteome and the effects of EGFR-TKIs onother RTKs. In this
study, we tested the hypothesis that aglobal evaluation of tyrosine
phosphorylation (using massspectrometry) between the sensitive and
resistant cells,along with EGFR perturbations, could identify
additionalresistancemechanisms that could give insight into
cotarget-ing strategies. Our results identified numerous
coexpressedRTKs and non-RTKs that, under proper
environmentalcircumstances, cooperate to drive resistance to
EGFR-TKIs.We further showed that Src family kinase (SFK)
signaling
was independent of EGFR signaling and that cotargetingSFKswith
afatinib led to combined growth suppression in invitro and in vivo
in cells with T790M. Globally, our resultssuggest that an unbiased
mass spectrometry approach canidentify codrivers of resistance that
can be cotargeted toenhance efficacy of targeted agents.
Materials and MethodsReagents
Gefitinib, erlotinib, afatinib, and WZ4002 were pur-chased from
Chemie Tek (Indianapolis, IN). CL-387,785was purchased from AXXORA
(San Diego, CA).
Cell cultureThe humanH1975, H460, A549, and H1299NSCLC cell
lines were obtained from American Type Culture Collec-tion. The
human HCC4006 NSCLC cells were kindly pro-vided by Dr. Paul Bunn
(University of Colorado, Aurora,CO). The human HCC827 NSCLC cells
were provided byDr. Jon Kurie (MD Anderson Cancer Center, Houston,
TX).The humanPC9NSCLC cell linewas kindly provided byDr.Hayata,
Tokyo Medical University (Tokyo, Japan). PC9GRcells were generated
by exposure of PC9 cells containing aTKI-sensitive EGFR mutation
(exon 19; E746-A750) togradually increasing concentrations of
gefitinib, beginningat 3 nM and up to 2 mM, for 3 months.
HCC4006-T790Mand HCC827-T790M cells were generated as
previouslydescribed (26). All cell lines have been maintained in
acentral repository at Moffitt since 2008. All cell lines hadbeen
authenticated by STR analysis (ACTG Inc, Wheeling,IL) as of
September 2010, and all cells had been routinelytested and were
negative for mycoplasma (PlasmoTest,InvivoGen, San Diego, CA). Cell
viability was determined
using the CellTiter-Glo� Luminescent Cell Viability
Assay(Promega, Madison, WI). Apoptosis assays were performedusing
PE-conjugatedmonoclonal active caspase-3 antibodyapoptosis kit (BD
Biosciences). Rescue experiments weredone as previously described
(27).
GenotypingTotal genomic DNA from parental and resistant
cells
was prepared using the DNeasy Blood & Tissue Kit (Qia-gen,
Valencia, CA) in accordance with the product man-ual. Direct DNA
sequencing was used to detect EGFRmutations as previously described
(28). We also appliedthe PCR-invader assay to detect minor
populations ofEGFR mutation, as previously described (29). MET
genecopy number per cell was determined by fluorescence insitu
hybridization with the use of the LSI D7S522 (7q31)Spectrum Orange
and chromosome 7 centromere (CEP7)Spectrum Green probes (Vysis;
Abbott), as previouslydescribed (30).
Tyrosine phosphoproteomicsTyrosine phosphopeptides were purified
according to the
manufacturer’s recommendations for the Cell SignalingPhosphoScan
kit (P-Tyr-100) (Cell Signaling Technology).Briefly, 2 � 108 cells
were lysed in urea buffer; extracted
Translational RelevanceAcquired resistance to EGFR-tyrosine
kinase inhibitor
(EGFR-TKI) is a critical clinical problem in patients
withnon–small cell lung cancer (NSCLC) with TKI-sensitiveEGFR
mutation. We applied mass spectrometry–basedtyrosine
phosphoproteomics to paired TKI-sensitive andresistant cell lines
to visualize molecular networks relat-ed to the acquired EGFR-TKI
resistance. The resultssuggest that multiple receptors and
signaling moleculessuch as MET, AXL, and IRS2 can collaborate to
driveresistance to EGFR-TKI. We also identified Src familykinases
(SFK) as a central signaling hub in TKI-resistantcells with T790M
gatekeeper mutation. SFK phosphor-ylationwas also detected
inhumanNSCLC sampleswithT790M. In vitro and in vivo experiments
demonstratedthat irreversible EGFR-TKI (afatinib) or
T790M-selectiveEGFR-TKI (WZ4006) combined with the SFK
inhibitordasatinib overcameT790M-mediated resistance,
therebynominating a new strategy for translation into the
clinic.
Yoshida et al.
Clin Cancer Res; 20(15) August 1, 2014 Clinical Cancer
Research4060
on June 19, 2021. © 2014 American Association for Cancer
Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst June 11, 2014; DOI:
10.1158/1078-0432.CCR-13-1559
http://clincancerres.aacrjournals.org/
-
proteins (40–80 mg) were then reduced by
dithiothreitol,alkylated by iodoacetamide, and then digested by
trypsin.Peptidemixture was isolated from lysate using Sep-Pak
C18columns and then lyophilizated. Phosphorylated peptideswere
immunoaffinity purified using phosphotyrosine anti-body after
lyophilizated peptide mixture was dissolved.Volumesof
phosphotyrosine peptideswere thendownsizedto 20 mL by vacuum drying
for further experiments. Thefurther peptide mixture separation and
phosphosite assign-ing have been previously described (31). To
quantify eachtyrosine-contained peptide, we calculated peak area
[alsocalled extraction ion chromatography (EIC)] using Label-free
strategy and xCalibur as the tools. Identification
andquantification of some obscure peptides were manuallyverified.
After quantification, 774 phosphorylated tyrosinesites were
identified. An in-house algorithmwas implemen-ted to identify
unique phosphorylation tyrosine (pY) sites,remove redundant sites,
and merge miss-cleaved peptidesby using protein ID, peptide
sequence, and phosphoryla-tion start-site
index,withquantificationof peak areas.Whenonly identifiable to the
level of pairs of pYs (e.g., next to eachother or up to �11 amino
acids apart), then the indepen-dent unit for analysis was the
unique pY pair (instead ofsingle site). Mis-cleaved phosphopeptides
or fragments ofthe samephosphopeptidesweremerged. Peptides
sharedbymultiple proteins were annotated. Among which, two pairsof
sequences were potential results of co-elution and there-fore not
included in further analyses. A total of 524 uniquephosphotyrosine
units (pYs) or pY pairs were identified.Quantification and
stability of 5 MYG peptides acrosssamples were examined, with the
average of 3 of them usedfor normalizing the peak ratio areas
across 16 samples (8biological samples with technical duplicates)
so that thenormalized quantities across samples were
comparable.Reproducibility between technical replicates for each
pYwas estimated using Pearson correlation. The correspond-ing P
values were used to estimate false discovery rate. Hightechnical
reproducibility of FDR �1% was used in ourstudy. In addition, if
the pY was detected in at least halfof the samples in this study,
i.e., at least 8 of 16 samples, itpassed theQC criteria. Among the
524 unique pY units, 403of them passed the QC criteria and were
included in theanalyses. 377 of themwere unique pY sites while 26
of themwereuniquepYpairs. Averages of technical replicates
from8biological samples were used in the analyses. We used asimple
imputation (i.e., when one of technical replicates ismissing, the
detected value from the other remaining tech-nical replicate was
used). Data were analyzed in log2 scaleprior to parametric analyses
and also for ease of interpre-tation. For example, the difference
of 1 in log2 scale is a 2-fold change between two conditions.
Two-way ANOVAwith the interaction term was performed to answer
thefollowing three research questions: 1) Which tyrosine sitesare
differentially phosphorylated between the cell lineswithand without
drug resistance? 2) Which tyrosine sites aredifferentially
phosphorylated between the control and erlo-tinib-treated groups?
3) Which pYs phosphorylationresponse to treatment is different
between the resistant and
non-resistant cell line? To adjust for multiple
hypothesistesting, the resulting P values for the main effects of
cell lineand treatment as well as the cell line-by-treatment
interac-tion termwere used to estimate false discovery rate.We
usedFDR �20% to declare statistical significance. We
furtherperformed network analysis based on these potential
can-didates. Interactions among all identified tyrosine
phos-phorylated proteins were retrieved from the
MolecularInteraction database (MINT) (32); the IntAct database(33);
the Database of Interacting Proteins (DIP) (34); theGeneral
Repository for InteractionDatasets (BioGRID) (35)and the
Biomolecular Interaction Network Database(BIND) (36) using InnateDB
(37) and visualized in Cytos-cape 2.8.3 (38).
Protein expression analysisWestern blot analysis of whole cell
lysates was performed
as described previously (27). Primary antibodies to EGFR,MET,
pTyr 1234/1235 MET, IRS2, pTyr 1131 IGF1R, AXL,pTyr 702 AXL, Src,
pTyr 416 Src, Akt, pSer 473 Akt, Erk,pThr202/Tyr204 Erk, and PARP
were obtained from CellSignaling Technology. Primary antibodies to
pY1068-EGFRwere obtained from Invitrogen (Carlsbad, CA).
Primaryantibodies to b-actin were purchased from Sigma-Aldrich(St.
Louis, MO).
Assessment of tumor growth inhibition in vivoAll animal
procedures were approved by our Institutional
Animal Care and Use Committee. PC9GR cells (2�106)were injected
subcutaneously into the flank of 7-week-oldfemale athymic nude
mice. The mice were divided into 4treatment groups of 7 animals:
those treated over 3weeks bydaily oral gavage of vehicle, afatinib
(10 mg/kg), dasatinib(15 mg/kg), or both afatinib and dasatinib;
0.5% (wt/vol)aqueous solution of hydroxypropylmethylcellulose
wasused as vehicle for afatinib, and 50% propylene glycol wasused
as vehicle for dasatinib. Treatment was initiated whentumors in
each group achieved an average volume of 100mm3, with tumor volume
being determined twice weeklyfor 21 days after the onset of
treatment from caliper mea-surement of tumor length (L) and width
(W) according tothe formula LW2/2.
Src-Tyr416 immunohistochemistry stainingImmunohistochemistry
staining was performed to mea-
sure the expression of phosphor-Src (Tyr416) in paraffintissues
from 10 lung cancer patients with mutant-positiveEGFR T790M.
Slides were stained for phosphor-Src (Tyr416) (mousemonoclonal
antibody; Millipore) using a Ventana DiscoveryXT automated system
(Ventana Medical Systems, Tucson,AZ) following the manufacturer’s
protocol with proprietaryreagents. Briefly,
slidesweredeparaffinizedon the automatedsystem with EZ Prep
solution (Ventana). Enzymatic retrievalmethod was used in protease
1 at 4 minute (Ventana), CC1Standard and CC2 standard conditions.
The primary mono-clonal antibody (Millipore) reacts to secondary
antibody atdifferent dilution-titrations. Both primary and
secondary
Phosphoproteomics of EGFR-TKI Resistance
www.aacrjournals.org Clin Cancer Res; 20(15) August 1, 2014
4061
on June 19, 2021. © 2014 American Association for Cancer
Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst June 11, 2014; DOI:
10.1158/1078-0432.CCR-13-1559
http://clincancerres.aacrjournals.org/
-
antibodies were incubated following Ventana’s instructionand the
antibody product recommendation. The intensity ofphosphor-Src
expression was scored from 0–3 (0 ¼ noexpression, 1 ¼ weak
expression, 2 ¼ moderate expression,and 3 ¼ high expression), while
the cellularity was scoredfrom0–3 (0¼ 0%, 1¼ 1-33%, 2¼ 34-66%, and
3¼ >66%).The H scores formed by intensity of immunoactivity
timingcellularity were stratified as low (0–2), intermediate
(3–4),and high (6–9).
MET-pY100 proximity ligation and total METimmunofluorescence
Slides containing 5-mmsections were rehydrated throughxylene and
graded alcohols. Heat-induced epitope retrievalwas carried out in
Tris-EDTA (pH 9) in a pressure cooker for20 minutes and then
allowed to cool for 20 minutes.Nonspecific binding was blocked by
incubation with1.5% BSA, and primary antibodies were incubated
over-night in 1.5% BSA-PBST.
For proximity ligation, antibodies were rabbit anti-MET(clone
D1C2, Cell Signaling Technology) and mouse ant-pY100 (Cell
Signaling Technology). PLA probes were anti-rabbit (-)
andanti-mouse (þ) andwere incubated for 1hourin 0.15% BSA/PBST.
Detection was carried out using theDuoLink in situ PLA Far Red kit
(O-Link Biosciences,Uppsala, Sweden). AlexaFluor 488-conjugated
anti-cyto-keratin was used to demarcate epithelial regions
(cloneAE1/AE3, eBiosciences).
For immunofluorescence, antibodies were rabbit anti-MET
(cloneD1C2, Cell Signaling Technology) and detectedviaAlexaFluor
647-labeled anti-rabbit secondary antibodies(Invitrogen). Murine
pan-cytokeratin (clone AE1/AE3,Dako) was used to demarcate
epithelial regions (tumormask) and detected via AlexaFluor
555-labeled anti-mousesecondary antibodies (Invitrogen). Images
were acquiredon a PM2000.
Statistical methodsAnderson-Darling statistics and normal curves
were
examined to assess whether tumor measurements werenormally
distributed. A square-root transformation wasperformed on the tumor
measurements to make themapproximately normal. ANOVA test was used
to assesswhether there was a statistically significant difference
ontumor sizes measured across treatment groups at each timepoint.
Tukey-Kramer method was used to perform all pair-wise group
comparisons. All statistical analyses were per-formed using SAS
(version 9.2; SAS Institute; Cary, NC).
ResultsChronic gefitinib exposure of PC9 cells generatesstable
cell-autonomous resistance to EGFR-TKIs withT790M
After generation of PC9GR cells, we identified single-cellclones
of PC9GR cells that were highly resistant to
erlotinib(Supplementary Fig. S1A). Although PC9GR cells are
par-tially sensitive to the irreversible EGFR-TKI CL387,785
asexpected fromaprevious report (8), IC50 forCL387,785was
100-fold increased compared with parent PC9 cells
(Sup-plementary Fig. S1A). This resistancewas stable as it was
notreversed by culturing PC9GR cells for up to 6 months
ingefitinib-free medium (data not shown). PC9GR cellsacquired T790M
while retaining exon 19 E746-A750,
asdeterminedbybothdirectDNAsequencing andPCR-invad-er assay
(Supplementary Fig. S2A). In addition, we did notfind MET
amplification by FISH analysis in PC9GR cells(Supplementary Fig.
S2B), which is another mechanism ofacquired EGFR-TKI resistance in
NSCLC (28). Erlotinib stillhas partial inhibitory effects on EGFR
phosphorylation inPC9GR cells (Supplementary Fig. S1B), consistent
withprior studies that T790M typically emerges as a minorpopulation
and resistant cells retain drug-sensitive alleles(8, 33). However,
erlotinib could not completely inhibitdownstream pAkt and pErk in
PC9GR cells, consistent withresistance to EGFR-TKIs in the presence
of T790M (Supple-mentary Fig. S1B).
System-level comparison of tyrosine phosphorylationidentifies
common RTK pathways associated witherlotinib resistance
We hypothesized that erlotinib-resistant PC9GR cellscould
collect additional mechanisms of resistance throughacquired
alterations in tyrosine kinase signaling that couldcollaborate with
T790M to codrive resistance to EGFR-TKI.We therefore profiled
tyrosine kinase signaling by chartingtyrosine phosphorylated
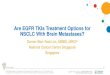
peptides in PC9 and PC9GR cells.As shown in our schema (Fig. 1),
tryptic peptides werederived from cellular protein lysates and
enriched withanti-phosphotyrosine (pTyr) antibodies followed by
iden-tification and quantification using liquid
chromatographycoupled with tandem mass spectrometry (LC/MS-MS;refs.
32, 34). Changes in peptides in PC9GR cells wereidentified and
compared with PC9 cells, thus allowing usto determine additional
changes beyond T790M that couldbe codrivers of TKI resistance. We
perturbed EGFR-drivensignaling in erlotinib-sensitive PC9 and
erlotinib-resistantPC9GR cells to identify EGFR-dependent
pathways/net-works and potential pathways/networks independent
ofEGFR signaling that could play a role in EGFR-TKI resis-tance.
After 1-hour erlotinib treatment, cell pellets werecollected and
pTyr peptides were identified in untreatedand treated PC9 and PC9GR
cells. Changes in peptides wereidentified compared with control
vehicle-treated cells ineach of the two cell lines. We hypothesized
that thisapproachwould identify downstream signaling events driv-en
by mutated EGFR but could also potentially identifyproteins or
pathways activated by TKI or unaltered by TKIthat could, under the
correct circumstances, potentiate drugresistance. In total, between
the two cell lines, we identified403 pTyr peptides corresponding to
265 unique phospho-proteins. Examples of extracted ion
chromatograms for pTyrpeptides corresponding to EGFR and MET are
shown inSupplementary Figs. S3 and S4.
We next compared changes in pTyr abundance betweenPC9 and PC9GR
cells (Fig. 2A; Supplementary Table S1).We found 110 unique pTyr
peptides (76 proteins) that were
Yoshida et al.
Clin Cancer Res; 20(15) August 1, 2014 Clinical Cancer
Research4062
on June 19, 2021. © 2014 American Association for Cancer
Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst June 11, 2014; DOI:
10.1158/1078-0432.CCR-13-1559
http://clincancerres.aacrjournals.org/
-
more abundant in the PC9GR cells, whereas 77 unique pTyrpeptides
(55 proteins) were less abundant in PC9GR cellsthan in PC9 cells.
Compared with PC9 cells, PC9GR cellsdemonstrated increased amounts
of pTyr peptides corre-sponding to numerous RTKs, some of which
could bepotential codrivers of resistance in PC9GR cells under
thecorrect environmental circumstances. We observed a
clearsubnetwork characterized by hyperactive MET signaling(Fig. 2A,
right) despite the lack of MET gene amplification.We observed
nearly 11-fold more MET pTyr peptidesin PC9GR than in PC9 cells.
Similarly, we observed nearly>10-fold more pTyr peptides
corresponding to ROR1 orneurotrophic tyrosine kinase receptor
related-1 (pTyr-789,�13-fold; pTyr-828, �34-fold). ROR1 is a
pseudokinasethat cooperates with MET to promote tumorigenesis
(35).Tyrosine phosphorylation of the MET adaptor proteinsGab1 and
Gab2 were also more abundant in PC9GR cells.In addition, pTyr
peptides corresponding to the AXL
RTK were increased approximately 8-fold in PC9GR cells.AXL
upregulation has recently been shown to be a mech-anism of acquired
resistance of lung cancer cells to EGFR-TKI (36). Finally,
increased abundance of multiple pep-tides corresponding to IRS2
(pTyr-675, 4.97-fold; pTyr-598, 5.47-fold; pTyr-823, 9.55-fold;
pTyr-653, 19.93-fold;and pTyr-742, 21.29-fold), an adaptor protein
linkinginsulin and insulin-like growth factor (IGF) signaling
toPI3K signaling, was observed in PC9GR cells comparedwith parent
PC9 cells. This suggested that either moreinsulin or IGF signaling
exists in these cells or more IRS2protein is expressed. We
confirmed higher levels of tyro-sine-phosphorylated MET and AXL in
PC9GR than in PC9cells and also found more total IRS2 protein in
PC9GRthan in PC9 cells (Fig. 2B). Despite the increased levels
ofMET signaling, we found minimal effects of combinedMET-TKI
(PHA665752) and EGFR-TKI (erlotinib or irre-versible CL387,785) in
PC9GR cells (Fig. 2C). While MET
signaling is hyperactivated, in this context, it is
notresponsible for affecting cell survival.
To examine whether changes of MET, IRS2, or AXL aredriven
specifically by T790M, we examined phosphoryla-tion of these
molecules in lung cancer cell lines (HCC4006and HCC827) engineered
to express an exon 19 E746-A750þ T790M allele. (Fig. 2B). We
observed less pMET, less totalMET, slightlymore abundant pAXL, and
similar total AXL inHCC4006-T790M cells compared with parent
HCC4006cells. We found equivalent pMET and total MET, less pAXLand
equivalent total AXL inHCC827-T790Mcells comparedwith parent HCC827
cells. The levels of IRS2 protein wereunchanged across these
HCC4006 and HCC827 cell linesunlike in PC9 and PC9GR cells. These
results suggest thatchanges of MET, IRS2, or AXL are not dependent
on EGFR-T790M but rather are likely to occur on a cell by cell
basis.
Perturbations by EGFR-TKI identify downstreamproteins and
proteins involved in adaptive andmicroenvironment-derived
responses
Wenext compared alterations in pTyr peptide abundancein both
cell lines following erlotinib exposure (Supplemen-tary Table S1).
We identified pTyr peptides with >1.5-foldchange differences
from control (P < 0.05). In PC9 cells, weobserved 31 less
abundant and 45 more abundant uniquepTyr peptides following 1 hour
of erlotinib treatment (Fig.3A). As expected, PC9GR cells displayed
a more bluntedresponse to erlotinib than PC9 cells; nonetheless, we
didobserve congruent changes in most pTyr peptides, thusincreasing
our confidence that these pTyr peptides andpathways are downstream
of mutant EGFR given theexpected biologic responses with cells
harboring T790Mmutations. Among the reduced pTyr peptides, we
observedMK01, SHC1, GAB1, EGFR, and ERBB3 consistent withtheir
known roles in ERBB signaling. Interestingly, we alsoobserved
reductions in peptides corresponding to Ras
Quantification (EIC)
Drug treatment Lysate Digestion
Tyrosine proteome
Anti-pTyr100 Ab
LC/MS-MS
PC9GRPC9 parental
DMSO DMSO DrugDrug
Drug
DMSO
–2.5
–2.0
–1.5
–1.0
–0.5
0.0
0.5
1.0
1.5
2.0
2.5
Drug response
Figure 1. Phosphoprotein networkassociated with mutant EGFR
andT790M tyrosine kinase signaling.Workflow of
quantitativephosphoproteomics analysis. EIC,extracted ion
chromatography(used to quantify peptideabundance for each of
theidentified tyrosine-containingpeptides).
Phosphoproteomics of EGFR-TKI Resistance
www.aacrjournals.org Clin Cancer Res; 20(15) August 1, 2014
4063
on June 19, 2021. © 2014 American Association for Cancer
Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst June 11, 2014; DOI:
10.1158/1078-0432.CCR-13-1559
http://clincancerres.aacrjournals.org/
-
Yoshida et al.
Clin Cancer Res; 20(15) August 1, 2014 Clinical Cancer
Research4064
on June 19, 2021. © 2014 American Association for Cancer
Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst June 11, 2014; DOI:
10.1158/1078-0432.CCR-13-1559
http://clincancerres.aacrjournals.org/
-
signaling, including SYGP1 or SynGAP, which can affectERK and
p38 MAPK functions in neurons (37, 38). Tyro-sine-phosphorylated
Rab7A (also known as Ras-relatedprotein Rab-7a) was likewise
reduced by erlotinib and hasbeen linked to EGFR trafficking in
endosomes (39).Interestingly, we observed that nearly equal amounts
of
pTyr peptides were increased by erlotinib compared withpeptides
reduced by erlotinib (45 up and 31down in PC9; 26up and 30 down in
PC9GR). We found more abundantpTyr peptides for IRS2,MET, YES, AXL,
FAK, ERBB2, andBRK(PTK6) following erlotinib treatment, and this
pattern wasconsistent across both PC9 and PC9GR cells (Fig. 3B).
Wehypothesized that the increased levels of RTK identifiedthrough
our approach could cooperate with exogenousligands and promote
EGFR-TKI resistance. Recent studieshave highlighted the ability of
growth factor ligands to pro-mote resistance to targeted agents
(23–25). We thereforetested if the increased pTyr in key RTK could
cooperate withgrowth factor ligands to drive resistance to
EGFR-TKI. Weincubated PC9 and PC9GR cells with cognate ligands
corre-sponding to the upregulated RTK in PC9GR, including
IGF1,hepatocyte growth factor (HGF), and GAS6 (the ligand forAXL
RTK), and determined the effects on erlotinib sensitivityin PC9
cells and afatinib sensitivity in PC9GR cells (Fig.
3C).Interestingly, HGF and IGF but not GAS6 had protectiveeffects
on both PC9 cells exposed to erlotinib and PC9GRcells exposed to
afatinib. In PC9 cells, the shift in IC50 wasrather modest;
however, in PC9GR cells, the effect was moredramatic. This shift
pattern was consistent between both celllines, with HGF having more
of an effect than IGF1, whereasno effect was seen with activation
of AXL by GAS6 in thesecells. UsingWestern blotting, we examined
the effects of theseligands on EGFR signaling with or without
EGFR-TKI in bothPC9 and PC9GR cells. HGF activated pMET in both PC9
andPC9GR cells (Supplementary Fig. S5A and S5B). This HGF-induced
activation of pMET and downstream pAkt and pErkwere not inhibited
by erlotinib in PC9 or by afatinib inPC9GR cells (Supplementary
Fig. S5A and S5B). These resultsalso suggest thatMETactivation
inPC9andPC9GRcells is notdependent on EGFR signaling.On the other
hand, we did notobserve clear ligand-dependent activation of
correspondingRTKs or sustained activation of pAkt and pErk in the
presenceof EGFR-TKIs in IGF1-induced or Gas6-induced PC9 andPC9GR
cells (Supplementary Fig. S5C–S5F). These results areconsistent
with our data showing that IGF1 andGas6 had less
rescue effects compared with HGF in these cells (see Fig.
3C).These results suggest that altered RTK identified by
phospho-proteomics can be codrivers of resistance under specific
en-vironmental circumstances. Furthermore, the increased levelsof
multiple RTKs in response to erlotinib suggest innatepriming of
RTK, where RTKs are primed to cooperate withgrowth factor ligands
through intracellular mechanisms.
Afatinib combined with dasatinib inhibits EGFRsignaling more
efficiently than either agent alone inTKI-resistant NSCLC cells
with T790M
We reexamined our data for pTyr peptides that were notperturbed
by EGFR-TKI and were not different betweenthe PC9 and PC9GR cell
lines. We hypothesized that thisanalysis may uncover parallel
signaling pathways thatcooperate with EGFR to maintain cellular
growth and/orsurvival. We identified 31 proteins that fulfilled
thiscriterion, including multiple SFKs as well as CSK, PKCD,MAPK3,
PIK3R2, SYK, TNK2, EPHB2, EPHA4, FAK, andPTK2B. We observed no
changes in pTyr peptides corre-sponding to SFKs, including the pTyr
peptide LIEDNEy-TAR corresponding to the common autocatalytic
sitein c-SRC, YES, and FYN, following EGFR-TKI, suggestingthis as
an EGFR-independent pathway. We linked SFKproteins to other
proteins found in our entire datasetthrough interaction databases
(Fig. 4A), identifying alarge group of proteins (N ¼ 28) with
reported interac-tions with SFK proteins (gray circles) that were
alsounchanged by erlotinib. In addition, we identified poten-tial
interactions between SFK and proteins either alteredby erlotinib
(gray parallelogram and diamond) or alteredin PC9GR compared with
PC9 cells (gray V and dia-mond). For example, SRC can cooperate
with EGFR, MET,ERBB3, SHC1, CBL, and STAT3 signaling nodes
(grayparallelogram) that we previously identified as beingaltered
by erlotinib and different between PC9 andPC9GR cells.
On the basis of this observation, we hypothesized
thatcotargeting SFKs and EGFR T790M with dasatinib andafatinib,
respectively, may produce additive or synergisticanti-tumor
effects. Furthermore, our previous studies sug-gested that the
antitumor effects of dasatinib are mediatedin part by direct EGFR
inhibition that ismitigated by gain ofT790M in EGFR (32). However,
these studies also suggestedthat irreversible EGFR-TKIs combined
with dasatinib could
Figure 2. Phosphoproteins associated with T790M-mediated
resistance. A, connectivity of MET protein was determined using
protein–protein interactiondatabases tobetter aid in
visualizingdifferentially expressedproteins thatmaybe
associatedwithPC9GRcells. The left histograph showschangeof pTyr
sitesin PC9GR cells compared with in PC9 cells. The fold change (P
< 0.05, fold change > 1.5) of all tyrosine peptides were
presented in log2 scale. Red barshows the tyrosine phosphosites of
MET network proteins in PC9GR cells. Right, the MET network.
Statistically decreased or increased pTyr peptides wereinput into
Cytoscape 2.8.3, and protein–protein interactions were identified
using InnateDB based on molecular interactions and functional
relationsfrom public sources. Shapes reflect types of proteins
shown in figure. Pink circle represents the pTyr peptides
significantly different between PC9 andPC9GR cells and different
between erlotinib-treated and control cells (P < 0.05; fold
change >1.5). Color scale corresponds to fold change in Log2
scale. Theyellow lines represent the direct interaction with MET.
B, Western blotting of selected proteins in PC9, PC9GR, HCC4006,
HCC4006-T790M, HCC827,HCC827-T790M cells. Membranes were blotted
with pTyr 1234/1235 MET, total MET, pTyr 702 AXL, total AXL, and
total IRS2 antibodies in PC9, PC9GR,HCC4006, HCC4006-T790M, HCC827,
HCC827-T790M cells with actin confirming equal protein loading. C,
PC9GR cells were treated for 72 hours withincreasing concentrations
of erlotinib alone, CL387,785 alone, PHA665752 alone, erlotinib þ
PHA665752, or CL387,785 þ PHA665752. Data generated bycell
viability assay (CellTiter-Glo) are expressed as a percentage of
the value for untreated cells. Determinations were done in
triplicate. Please view onlineversion for full details.
Phosphoproteomics of EGFR-TKI Resistance
www.aacrjournals.org Clin Cancer Res; 20(15) August 1, 2014
4065
on June 19, 2021. © 2014 American Association for Cancer
Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst June 11, 2014; DOI:
10.1158/1078-0432.CCR-13-1559
http://clincancerres.aacrjournals.org/
-
B C
Fo
ld c
han
ge
MET pY1234 AXL pY702 IRS2 pY675 IRS2 pY8230
5
10
15
20
25PC9PC9-ErlotinibPC9GRPC9GR-Erlotinib
Erlotinib-PC9GRErlotinib-PC9
–6.81 –0.58 1.63 4.84
GAB1 pY259
RAB7A pY183EGFR pY1197
CBL pY674SHC1 pY427
ERBB3 pY1276
EGFR pY1092ERBB3 pY1159EGFR pY1172EGFR pY998
CBLB pY889ERBB3 pY1307
GAB1 pY659
EGFR pY1138SHC1 pY349
MAPK1 pY187
Fold change (log2)–7 –6 –5 –4 –3 –2 –1 0 1 32 54 6 7
SHB pY114
ERBB2 pY1023
PTK6 pY114
PXN pY118
MET pY1234
TNS1 pY1254
TNS1 pY1404
NEDD9 pY166
GLUL pY185 TAGLN2 pY192
YES1 pY222
BCAR1 pY234
ANXA2 pY24
SHB pY268
NEDD9 pY317
NEDD9 pY345
HIPK3 pY359
STAT3 pY705
EPS8 pY774
PTK2 pY861
PXN pY88
INPPL1 pY886
NUP205 pY902
ACTB pY91
MAGED1 pY92
A
PC9GR
0.1 1 10 100 1,0000
25
50
75
100 CtrHGFIGF1GAS6
Erlotinib (nmol/L)
Rel
ativ
e ce
ll vi
alb
ility
0.1 1 10 100 1,0000
25
50
75
100 CtrHGFIGF1GAS6
Afatinib (nmol/L)
Rel
ativ
e ce
ll vi
alb
ility
Afatinib
PC9GR 193.00+ HGF 50 ng/mL >1000+ IGF1 50 ng/mL 422.30+ Gas6
800 ng/mL 174.00
ErlotinibIC50 nmol/L
IC50 nmol/L
PC9 6.94+ HGF 50 ng/mL 28.74+ IGF1 50 ng/mL 14.09+ Gas6 200
ng/mL 6.99
pY187
RAB7A
pY259
pY659
GAB1pY1138pY1172
SHC1
pY998CBL
pY1197
EGFR
pY674pY427
pY349
ERBB3
pY1276
pY1159
MAPK1
pY1307pY1172pY1197
CBLB
EGFR
pY1092
pY1138
pY1307
pY1159
pY1276
ERBB3
pY187MAPK1
pY427pY349
SHC1
pY259
pY659
GAB1
CBL
pY674
pY998
pY1092
pY1234METSTAT3
pY705
pY166pY317
pY774
NEDD9
pY345
pY114pY1404 pY268pY1254
pY91
ACTB
BCAR1
pY234
TNS1
EPS8
SHB
pY705
pY222YES1pY861
BCAR1
PTK2
pY1404
STAT3
TNS1pY234
pY24
pY91
TAGLN2
ACTB
PXN
pY114
ANXA2
ERBB2PTK6
pY1023
SHB
pY317
pY268
pY118
pY88
pY345
pY114
NEDD9
pY166
EPS8
pY185
MAGED1
pY192
pY902
pY774 HIPK3GLUL
pY92
NUP205
pY359
MET
pY1234pY886
INPPL1pY1254
Figure 3. Erlotinib perturbations inPC9andPCGRcell lines. A,
effects of erlotinib on tyrosine containing phosphoproteomes inPC9
andPC9GRcell lines. Left,erlotinib-induced changes (P < 0.05;
fold change >1.5) of pTyr sites in PC9 (bars) and PC9GR (�)
cells. Four subnetworks were created within different
catalogproteins (blue circle) based on increased or decreased pTyr
sites in PC9 and PC9GR cells. Color scale represents the fold
change of each pTyr site. B,
pTyrpeptideabundancemeasuredbyEICacross
erlotinib-treatedPC9andPC9GRcells forMET,AXL, and IRS2pTyr
peptides.Y-axis indicates fold change abovePC9 untreated pTyr
abundance. C, PC9 or PC9GR cells were seeded in 96-well plates for
24 hours and then exposed to HGF or IGF1 (50 ng/mL) or GAS6(200
ng/mL) and concomitantly exposed to increasing concentrations of
relevant kinase inhibitor. After 72 hours, cell viability was
assessed. IC50 wascalculated for each condition. Please view online
version for full details.
Yoshida et al.
Clin Cancer Res; 20(15) August 1, 2014 Clinical Cancer
Research4066
on June 19, 2021. © 2014 American Association for Cancer
Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst June 11, 2014; DOI:
10.1158/1078-0432.CCR-13-1559
http://clincancerres.aacrjournals.org/
-
inhibit EGFR T790M. Thus, we examined the effects oferlotinib,
afatinib, dasatinib, or combined afatinib anddasatinib on EGFR
signaling in PC9GR and H1975 cells,both resistant cell lines
against EGFR-TKI because of T790M(Fig. 4B). In both cell lines,
erlotinib inhibited neither EGFRnor SFKs, and no complete
suppression of pAkt and pErk(both essential downstream molecules of
EGFR) wasobserved. We found that afatinib could inhibit
pEGFR;however, SFKs were again unaltered. These results
witherlotinib and afatinib are consistent with our pTyr
massspectrometry results that detected no changes in pTyr
SFKsfollowing erlotinib exposure. We also found that combin-ing
afatinib and dasatinib resulted in more efficient inhi-bition of
pAkt and pErk in PC9GR and H1975 cells thaneach agent alone,
suggesting that SFKs are cosignals relatedto EGFR T790M and that
irreversible EGFR-TKIs combinedwith SFKs more efficiently block
EGFR signaling in NSCLCcells harboring T790M.
Afatinib combined with dasatinib effectively inhibitscell growth
and significantly increases apoptotic cellsin TKI-resistant NSCLC
cells with T790MGiven that the combination of afatinib and
dasatinib
efficiently inhibited EGFR signaling inNSCLC cells
harboringT790M, we examined the effects of this combination on
cellproliferation and apoptosis in PC9GR and H1975 cells. Wefound
reduced IC50 levels in PC9GR and H1975 cells versuseither agent
alone (Fig. 4C; Supplementary Tables S2 and S3).We examined the
effects of combining afatinib plus dasatinibin other NSCLC cells
with T790M (HCC4006-T790M andHCC827-T790M cells), cells with
TKI-sensitive EGFR muta-tion only (PC9,HCC4006, andHCC827 cells),
and cells withwild-type EGFR (H460, A549, andH1299
cells).Weobservedreduced IC50 for afatinib plus dasatinib versus
either agentalone in HCC4006-T790M and HCC827-T790M cells
(Sup-plementary Fig. S6), whereas curves for this combinationwere
mostly overlapped with those for afatinib or dasatinibalone in PC9,
HCC4006, and HCC827 cells with TKI-sensi-tive EGFR mutation only
(Supplementary Fig. S7) or H460,A549, andH1299 cells with wild-type
EGFR (SupplementaryFig. S8). We also found that dasatinib combined
withCL387,785, another irreversible EGFR-TKI, reduced IC50versus
either agent alone in PC9GR cells (SupplementaryFig. S9).
Furthermore, we also detected more apparent PARPcleavage when
agents were combined than when used aloneor when cells were
erlotinib treated (see Fig. 4B). Similar toresults with afatinib,
when we examined the effects of com-bined dasatinib with WZ4002,
another T790M-specificEGFR-TKI (40), IC50 was reduced versus when
agents wereused alone (Fig. 4D; Supplementary Tables S2 and
S3).
Rescue experiments revealed that dasatinib enhancedantitumor
effects of afatinib by inhibition of SRC andFYNAlthough our
clustering approach and dasatinib results
strongly implicated SFKs as the key target, we examined thisin
more detail given the extensive promiscuousness ofdasatinib. Using
dasatinib-insensitive alleles expressed in
lentiviral vectors, we investigated whether dasatinib-resis-tant
forms of key SFKs could rescue effects of dasatinib (32).To test
which SFK is critical as a dasatinib target in NSCLCcells harboring
T790M when combined with afatinib, weinfected cells with lentivirus
expressing either wild-typekinases or kinase alleles with
drug-resistant gatekeepermutations of SFKs (SRC, LYN, FYN, and FRK)
and examinedcell viability in response to increasing concentrations
ofdasatinib plus afatinib (Fig. 4E). Our results show that SRCand
FYN were able to rescue PC9GR cells from dasatinibplus afatinib.
However, no effects were observed with LYNand FRK, suggesting that
SRC and FYN are essential SFKs asdasatinib targets in NSCLC cells
with T790M.
Dasatinib enhances the antitumor activity of afatinibin vitro
and in vivo
To evaluate more formally whether our combinationeffects were
because of additional cell death, we measuredcaspase-3–positive
cells following TKI treatment (Fig. 5A).In PC9GR cells, both
erlotinib and dasatinib had noeffects on apoptosis, but the
combination had modesteffects. Afatinib led to more apoptosis,
which was furtherincreased when combined with dasatinib. Similar
effectsof afatinib plus dasatinib on apoptosis were observed
inHCC4006-T790M and HCC827-T790M cells (Supple-mentary Fig. S10).
WZ4002 also induced apoptosis as asingle agent, which was
potentiated when combined withdasatinib. In H1975 cells, similar
effects were observed,with dasatinib increasing apoptosis when
added to afa-tinib and WZ4002. These results indicate that Src
inhi-bitors enhance antiproliferative and proapoptotic effectsof
irreversible or T790M-selective EGFR-TKIs in NSCLCcells with
T790M.
We hypothesized that the enhanced apoptosis withcombined
afatinib and dasatinib would translate intoimproved in vivo effects
on tumor growth. We examinedthe antitumor effects of this
combination in mouse xeno-graft models with PC9GR cells. As single
agents, afatinib(10 mg/kg) or dasatinib (15 mg/kg) had modest
effectson inhibiting tumor growth in PC9GR xenografts;however, when
combined, we observed significantly great-er inhibition of growth,
including tumor regression con-sistent with our apoptosis results
(Fig. 5B). These resultsdemonstrate that Src inhibitors effectively
enhance anti-tumor effects of irreversible EGFR-TKI in
gefitinib-resistantNSCLC xenografts with T790M, providing a
rationale toevaluate this strategy in patients with NSCLC who
haveacquired EGFR-TKI resistance related to T790M.
Tyrosine phosphoproteomes in lung adenocarcinomasamples with
TKI-sensitive EGFR mutations
To validate that our cell line models and data are appli-cable
to human lung cancer tissues, we conducted a massspectrometry
tyrosine phosphoproteomics analysis on fourNSCLC tumor samples with
TKI-sensitive EGFRmutations.In total, we identified 279 unique pTyr
sites correspondingto 189 unique proteins across all four tumor
samples. Foreach tumor, we identified 158, 153, 157, and 109
unique
Phosphoproteomics of EGFR-TKI Resistance
www.aacrjournals.org Clin Cancer Res; 20(15) August 1, 2014
4067
on June 19, 2021. © 2014 American Association for Cancer
Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst June 11, 2014; DOI:
10.1158/1078-0432.CCR-13-1559
http://clincancerres.aacrjournals.org/
-
pTyr sites corresponding to 117, 95, 111, and 87
proteins,respectively (Supplementary Table S4). Importantly,
83unique pTyr sites on 65 proteins identified from massspectrometry
experiments in PC9 cells were also observedactive in human patient
tissues (Supplementary Fig. S11and Supplementary Table S5). This
included: EGFR(pTyr1172, 1197), MET (pTyr1234), SFKs including
SRC(pTyr 419), FYN (pTyr 214, 420), LYN (pTyr 32, 193, 104,397),
YES1 (pTyr223, 426), MK01 (pTyr 187), MK03 (pTyr204), STAT3 (pTyr
705), and AXL (pTyr 886). These resultsin human tumor tissues
frompatients with EGFRmutationswell validate our findings gained
from cell line model,
suggesting the potential of clinical application of our
find-ings in this study.
Activation of Src or MET in human lung tumor sampleswith T790M
gatekeeper EGFR mutations
To validate that Src phosphorylation is indeed observedas a
target in human NSCLC samples with T790M gate-keeper mutation, we
examined the expression of phos-phorylated Src (Tyr 416) in tumor
samples with T790Musing immunohistochemical staining. We found pSrc
inall EGFR T790M-positive tissue specimens, including 2paired
samples of pre- and post-EGFR-TKI treatment, with
Proteins: no change in the PC9GR compared to PC9, also no
response to erlotinib
B
CTTN
pY194
LYN
pY421
pY702
pY508
pY227
AXL
PTK2
pY293
pY341pY30
pY576
CTNNB1
GAB2
ITGB1PXN
pY88TYK2
pY292
pY397SDCBP
pY46
pY313
pY783PRKCD
pY780
TNS3pY296
pY359
SYKpY417
pY601pY163
PAG1TGM2
pY222pY904
pY334pY228
YES1
pY446
pY 334
pY193CTNND1
PTK2B
pY1138
pY869
pY1092
pY1172
pY1197pY998
EGFR
MCAM
TNK2
EPHA4BCAR1
MPZL1
FYN
CDCP1
CDKL5
PTPRA
PTPN11
PIK3R2
METpY1003
pY1234
pY427pY349
pY 204pY204
pY 427
MAPK3
SHC1
pY525
SHB
pY 774
pY774
pY 114
pY114
EPS8
pY214
pY345
pY317
pY261pY106
pY166
NEDD9
ELF2pY1307
pY91pY1159
pY1276
pY287
ERBB3 ACTB
PTPN6
EPHB2SRC
ERBB2
WASL
SHANK2
ASAP2
CSK
pY705
CBL
pY 705
pY674
pY 674
STAT3
pY 317pY802pY579 pY584pY369
pY241
pY491
pY629
pY268
pY177
pY 345
pTyr sites up-regulated by erlotinib or higher expression in
PC9GR than PC9
A
pTyr sites down-regulated by erlotinib or lower expression in
PC9GR than PC9
Proteins: altered by erlotinib only Proteins: altered in PC9GR
compared to PC9
Proteins: altered by erlotinib and in PC9GR compared to PC9
PARP
PC9GR (Ex19del + T790M)
Actin
p-Erk
p-Akt
p-EGFR
p-Src
Akt
Erk
EGFR
Src
Erlo
tinib
100
nm
ol/L
Con
t
10 n
mol
/L
100
nmol
/L
Afatinib
10 n
mol
/L
100
nmol
/L
Dasatinib
10 n
mol
/L
100
nmol
/L
Combination
H1975 (L858R + T790M)
PARP
Actin
p-Erk
p-Akt
p-EGFR
p-Src
Akt
Erk
EGFR
Src
Con
t
10 n
mol
/L
100
nmol
/L
Afatinib
10 n
mol
/L
100
nmol
/L
Dasatinib
10 n
mol
/L
100
nmol
/L
Combination
Erlo
tinib
100
nm
ol/L
OCLNpY 287
Figure 4. Effects of dasatinib combined with afatinibon EGFR
signaling and cell growth in gefitinib-resistant NSCLC cells with
T790M. A, pTyr proteinscorresponding to pTyr peptides identified in
PC9and PC9GR cells are linked to SFK using InnateDBto capture
literature reports and displayed inCytoscape. Pink circle, pTyr
sites upregulated byerlotinib or higher expression in PC9GR than in
PC9cells. Blue circle, pTyr sites downregulated byerlotinib or less
expression in PC9GR than in PC9cells. Yellow circles or V, SFK
(SRC, YES1, FYN).Gray circle, pTyr proteins showing no
differencebetween PC9 and PC9GR cells and no change witherlotinib
treatment. Gray parallelogram, pTyrproteins altered by erlotinib
across PC9andPC9GRdatasets. Gray V, pTyr proteins different
betweenPC9 andPC9GR cells. Gray diamond, pTyr proteinsdifferent
between PC9 and PC9GR cells andshowing changes with erlotinib
treatment. B,PC9GR and H1975 cells were incubated for 6 hours(or 24
hours for PARP) in the absence or presence oferlotinib (100
nmol/L), afatinib (10 and 100 nmol/L),dasatinib (10 and 100
nmol/L), or afatinib anddasatinib in combination (10 and 100
nmol/L), asindicated. Cell lysates were subjected to
proteinexpression analysis with antibodies to pEGFR,EGFR, pAkt,
Akt, pErk, Erk, pSrc family, Src, orPARP along with antibodies to
b-actin as a loadingcontrol. (Continued on the following page.)
Yoshida et al.
Clin Cancer Res; 20(15) August 1, 2014 Clinical Cancer
Research4068
on June 19, 2021. © 2014 American Association for Cancer
Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst June 11, 2014; DOI:
10.1158/1078-0432.CCR-13-1559
http://clincancerres.aacrjournals.org/
-
E
C
D
Drug Sensitivity in PC9GR
1 10 100 1,000 10,0000
25
50
75
100
AfatinibErlotinib
Afatinib + DasatinibDasatinib
Drug concentration (nmol/L)
1 10 100 1,000 10,000
Drug concentration (nmol/L)
1 10 100 1,000 10,000
Drug concentration (nmol/L)
1 10 100 1,000 10,000
Drug concentration (nmol/L)
1 10 100 1,000 10,000
Drug concentration (nmol/L)
1 10 100 1,000 10,000
Drug concentration (nmol/L)
1 10 100 1,000 10,000
Drug concentration (nmol/L)
1 10 100 1,000 10,000
Drug concentration (nmol/L)
Cel
l via
bilit
y (%
)C
ell v
iabi
lity
(%)
Cel
l via
bilit
y (%
)
Cel
l via
bilit
y (%
)
Cel
l via
bilit
y (%
)
Cel
l via
bilit
y (%
)
Cel
l via
bilit
y (%
)
Drug Sensitivity in H1975
0
25
50
75
100
AfatinibErlotinib
Afatinib + DasatinibDasatinib
Cel
l via
bilit
y (%
)
Drug sensitivity in PC9GR
0
25
50
75
100
WZ4002Erlotinib
WZ4002 + DasatinibDasatinib
Drug Sensitivity in H1975
0
25
50
75
100
WZ4002Erlotinib
WZ4002 + DasatinibDasatinib
0
25
50
75
100
SRC-WT vs. Afatinib + Dasatinib
SRC-MT vs. Afatinib + Dasatinib
0
25
50
75
100
FYN-WT vs. Afatinib + Dasatinib
FYN-MT vs. Afatinib + Dasatinib
0
25
50
75
100
LYN-WT vs. Afatinib + Dasatinib
LYN-MT vs. Afatinib + Dasatinib
0
25
50
75
100
FRK-WT vs. Afatinib + Dasatinib
FRK-MT vs. Afatinib + Dasatinib
Figure 4. (Continued. ) C, PC9GR and H1975 cells were treated
for 72 hours with increasing concentrations of erlotinib alone,
afatinib alone, dasatinibalone, or afatinib þ dasatinib. D, PC9GR
and H1975 cells were treated for 72 hours with increasing
concentrations of erlotinib alone, WZ4002 alone,dasatinib alone, or
WZ4002 þ dasatinib. Data generated by cell viability assay
(CellTiter-Glo) are expressed as a percentage of the value for
untreatedcells. Determinations were done in triplicate. E, PC9GR
cells were infected with lentivirus expressing wild-type and mutant
gatekeeper forms ofeach indicated Src family kinase for 48 hours.
Subsequently, cells were exposed to increasing concentrations of
afatinib plus dasatinib for 72 hours,after which cell viability was
assessed by cell viability assay (CellTiter-Glo). Data are
expressed as a percentage of the value for untreated
cells.Determinations were done in triplicate. Please view online
version for full details.
Phosphoproteomics of EGFR-TKI Resistance
www.aacrjournals.org Clin Cancer Res; 20(15) August 1, 2014
4069
on June 19, 2021. © 2014 American Association for Cancer
Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst June 11, 2014; DOI:
10.1158/1078-0432.CCR-13-1559
http://clincancerres.aacrjournals.org/
-
varied intensities and cellularity (Table 1; Fig. 5C).
Theseresults confirmed results from cell lines that Src
activitypersists in EGFR T790M-positive tumor tissues. We fur-ther
examined changes in tyrosine phosphorylated METexpression in
matched pre- and post-EGFR-TKI treatmentpatient tumor tissue
specimens. We found evidence forincreased tyrosine phosphorylated
MET in one patient(patient 10 in Table 1) that was not due to
increased totalMET protein (Fig. 5D), whereas no evidence was
foundin the second patient (patient 9 in Table 1) for which pre-and
posttreatment biopsy tissues were available for study.These results
provide further support using tumor tissuesthat MET tyrosine
phosphorylation can occur in T790M-containing tissues and this can
be independent of totalMET expression.
DiscussionWe applied tyrosine phosphorylation profiling
using
LC/MS-MS to directly compare an EGFR-TKI–sensitivecell line
versus its acquired resistance counterpart touncover additional
resistance mechanisms and proposecotargeting strategies to enhance
the effects of agentsspecifically targeting the T790M EGFR allele.
To ourknowledge, this is the first such report to apply a
massspectrometry–based phosphoproteomics approach tocompare the
molecular networks between EGFR-TKI–sensitive and -resistant pairs.
The driving force behindthis approach is the limited efficacy of
irreversible EGFR-TKIs in targeting T790M, as shown in both
preclinicaland clinical studies (8, 9, 12, 14–19), and the ability
of
A
B
PC9GR (Ex19del +T790M) H1975 (L858R +T790M)
PC9GR
0
10
20
30
40
Treatment (48 h)
DMSO
E 10
0 nmo
l/L
A 10
0 nmo
l/L
D 10
0 nmo
l/L
E 10
0 nmo
l/L +
D 10
0 nmo
l/L
A 10
0 nmo
l/L +
D 10
0 nmo
l/L
W 10
0 nmo
l/L
W 10
0 nmo
l/L +
D 10
0 nmo
l/L
DMSO
E 10
0 nmo
l/L
A 10
0 nmo
l/L
D 10
0 nmo
l/L
E 10
0 nmo
l/L +
D 10
0 nmo
l/L
A 10
0 nmo
l/L +
D 10
0 nmo
l/L
W 10
0 nmo
l/L
W 10
0 nmo
l/L +
D 10
0 nmo
l/L
Treatment (48 h)
Cas
pas
e-3–
po
siti
ve c
ells
(%
)
0
10
20
30
40
Cas
pas
e-3–
po
siti
ve c
ells
(%
)
H1975
In vivo activity in PC9GR cells
0 2 4 6 8 10 12 14 16 18 20 220
50
100
150
200
250
300
350
400
450
500
550
600
650
700 Control
Afatinib
Dasatinib
Afatinib + Dasatinib
Days
Tu
mo
r vo
lum
e (m
m3 )
Figure 5. Effects of dasatinibcombined with afatinib onapoptosis
and in vivo tumorregression in gefitinib-resistantNSCLC cells with
T790M. A,apoptosis assay was carried outusing PE-conjugated
caspase-3antibody, following incubation ofPC9GR or H1975 cells for
72 hourswith DMSO, erlotinib (E), dasatinib(D), erlotinib þ
dasatinib, afatinib(A), afatinib þ dasatinib, WZ4002(W), and WZ4002
þ dasatinib.Values are expressed as apercentage of
caspase-3-positivecells. Determinations were done intriplicate.
Bars, SD. �, P < 0.001versus DMSO or each single agent(Student t
test). B, Nude mice withtumor xenografts established bysubcutaneous
implantation ofPC9GR cells were treated daily for21 days with
vehicle (control),afatinib (10 mg/kg), dasatinib (15mg/kg), or
afatinib þ dasatinib byoral gavage. Tumor volume wasdetermined at
the indicated timesafter the onset of treatment. Points,mean of
values from 5 mice/group;bars, SE. �, P < 0.05 for
afatinibcombined with dasatinib versuscontrol or each agent alone
byANOVA (Tukey–Kramercomparison). (Continued on thefollowing
page.)
Yoshida et al.
Clin Cancer Res; 20(15) August 1, 2014 Clinical Cancer
Research4070
on June 19, 2021. © 2014 American Association for Cancer
Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst June 11, 2014; DOI:
10.1158/1078-0432.CCR-13-1559
http://clincancerres.aacrjournals.org/
-
other tyrosine kinases, especially RTKs, to limit
EGFR-TKIefficacy. Through a systematic interrogation of pTyr
pep-tides and proteins using LC/MS-MS, we identified bothRTKs and
non-RTKs able to be recruited to confer erlo-
tinib sensitivity. In PC9GR cells, we identified higherlevels of
pTyr peptides corresponding to MET signaling,including more MET,
ROR1, and Gab1/2 proteins. Inter-estingly, this coordinated
activation of MET signalingwas not secondary to MET gene
amplification, as ourFISH results revealed no amplification of the
MET gene.The results with the basal phosphoproteome corre-sponded
to HGF’s strong effects in protecting both PC9and PC9GR cells from
erlotinib or afatinib, respectively.In addition, these results
suggest a form of "lineage"addiction, whereby resistant cells with
T790M can carryforward RTKs that can cooperate to drive
resistance.Importantly, these results suggest that interrogating
pro-tein activation status or network signaling may
highlightproteins that play a role in protecting cells against
EGFR-TKI, especially when in a microenvironment rich withcognate
growth factor ligands. Despite observing moreAXL pTyr peptides in
PC9GR cells, we demonstrated noability of AXL pathway activation by
Gas6 ligand to driveresistance to either erlotinib or afatinib. The
reasons forthis are not clear, but one limit of our approach was
thelack of absolute measurements of pTyr peptides. It ispossible
that, compared with MET or IRS2 pTyr peptides,pTyr peptides
corresponding to AXL are far lower inabsolute amount and thus are
inefficient to compete fordownstream signaling effectors. It will
be interesting andimportant to determine how basal
phosphoproteomemeasurements can predict the effects of growth
factorprotection against targeted agents. As AXL signaling
stillremains poorly understood, another explanation for ourresults
could be the limited or absence of key adaptors orother effector
proteins involved in AXL signaling.
Using pTyr peptide data obtained from both PC9 andPC9GR cells
exposed to erlotinib, we identified proteinsdownstream of EGFR in
these cells with mutant gain-of-function EGFR proteins. One of the
more interestingfindings was that nearly half of the statistically
significantpTyr peptides were increased in abundance
followingerlotinib treatment. It is increasingly recognized
thatsignaling pathways display large amounts of crosstalkand that
adaptive resistance mechanisms have beenobserved in cells exposed
to targeted agents (41). Ourresults match our investigations using
purified Srchomology-2 domains to profile tyrosine kinase
signalingin lung cancer cells, where we observed increased
pTyrsignaling in multiple lung cancer cells exposed to TKIs(42).
Similar events have also been observed in crizoti-nib-treated
EML4-ALK cells and dasatinib-treated DDR2-mutant lung cancer cells,
arguing that these paradoxicalchanges are consistent across
multiple tumor types andkinase inhibitors (unpublished
observations). Theunderlying mechanisms of these changes require
addi-tional study, as they could be important in promotingadaptive
resistance to targeted agents and could in somecases cooperate with
microenvironmental factors, suchas growth factors, to limit TKI
efficacy. Collectively, theseresults suggest that cell intrinsic
(receptors, signalingproteins) and extrinsic (ligands) factors can
collaborate
H score: 9
H score: 3
H score: 6
Pretreatment Posttreatment
ME
T-p
Y10
0 P
LAT
otal
ME
T IF
C
D
Figure 5. (Continued. ) C, evidence for activation of Src in the
T790M-positive biopsy specimens. Immunohistochemical staining was
used todetect expression of tyrosine phosphorylation Src (Tyr416)
in 10 EGFRT790M-positive tissue specimens. H score (intensity �
cellularity) wascalculated for each sample, with scores 0 and 9
representing the lowestand highest expression, respectively. Three
representative�200 imagesshow the different levels of pSrc
expression in EGFR T790M-positivehuman lung specimen. D, evidence
for increased MET tyrosinephosphorylation in posttreatment T790M
biopsy specimens. Proximityligation assays (PLA) for MET and pY100
were performed to assess METphosphorylation in serial biopsy
specimens obtained from anadenocarcinomapatient (right lung, lower
lobe, 33months apart). Originalbiopsy confirmed EGFR exon21 L858R
mutation; rebiopsy confirmedL858R/T790M mutation. Top, evidence of
MET-pY PLA signal inpretreatment biopsy, while clusters of highly
phosphorylated MET areobserved in the posttreatment biopsy. MET-pY
PLA was localized tocytokeratin (þ)-staining regions (data not
shown). Bottom, increasedMET-pY PLA signal is not due to increased
total MET protein.
Phosphoproteomics of EGFR-TKI Resistance
www.aacrjournals.org Clin Cancer Res; 20(15) August 1, 2014
4071
on June 19, 2021. © 2014 American Association for Cancer
Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst June 11, 2014; DOI:
10.1158/1078-0432.CCR-13-1559
http://clincancerres.aacrjournals.org/
-
to drive resistance to kinase inhibitors in a
systems-levelmanner.
Our phosphoproteomics analyses in PC9 and PC9GRcells
demonstrated that SFKs are also critical as an EGFR-independent
cosignal in NSCLC cells with T790M. Theseresults were enabled by
tyrosine phosphorylation profil-ing combined with analysis of
proteins based on knownprotein–protein interactions. We validated
the inferencesderived from the phosphoproteomics by showingthat
afatinib combined with dasatinib resulted in antitu-mor activity
regarding cell proliferation and apoptosis inPC9GR, H1975,
HCC4006-T790M, and HCC827-T790Mcells (each harboring T790M). These
results appear to begeneralized to additional T790M EGFR-TKIs, as
dasatinibdemonstrated similar combination effects with
theT790M-selective EGFR-TKI WZ4002 (40). We did notobserve
combination effects with afatinib plus dasatinibcompared with
either agent alone in cells with TKI-sen-sitive EGFRmutation only
(PC9, HCC4006, and HCC827cells) or wild-type EGFR (H460, A549, and
H1299 cells).The enhanced apoptosis with combined afatinib
anddasatinib in the cells with T790M translated intoimproved in
vivo effects on tumor growth in PC9GR cells.Collectively, our
results suggest that dasatinib can begenerally used as a
combination therapy with irreversibleor T790M-selective EGFR-TKIs
for patients with NSCLCwho acquired EGFR-TKI resistance associated
withT790M.
As our approach was limited to examining the
tyrosinephosphoproteome, we were unable to detect serine/thre-onine
signaling including mTOR/AKT or MEK/Erk path-ways both of which are
also essential for carcinogenesis.Previous studies have indicated
that mTOR inhibitorcombined with MEK inhibitor or irreversible
EGFR-TKIis potential strategy to overcome T790M (21, 43).
Furtherstudies examining the global phosphoproteome, such aswith
immobilized metal affinity chromatography which
can detect serine/threonine phosphopeptides (44), couldidentify
other proteins and pathways that may play rolesin EGFR TKI
resistance.
Although single-agent dasatinib has no activity inpatients with
NSCLC with TKI-sensitive EGFR mutationwho acquired resistance to
EGFR-TKI (45), our resultssuggest a role for SFKs in maintaining
downstream sig-naling despite irreversible EGFR-TKIs and support
furtherstudies of irreversible EGFR-TKIs combined with dasati-nib
in patients with NSCLC who acquire resistance toEGFR-TKI. Src is
known to be both an upstream activatorand a downstream mediator of
EGFR, and its phosphor-ylation is detected in about one-third of
lung cancertumors (46, 47). Although MET activation might not
bealways observed in the presence of T790M based on our invitro and
tumor tissue analysis, pSrc seems to be generallydetected in our
NSCLC tumor samples harboring T790M,consistent with our results of
cell models. In addition, ourmass spectrometry data from tumor
samples with TKI-sensitive EGFR mutation demonstrated a high degree
ofoverlap with results from cell models, thereby validatingthe
overall approach. These results from tumor samplessuggest that our
results from lung cancer cell line modelsare applicable to
translate in to the clinic. Our previouschemical and
phosphoproteomic characterization iden-tified nearly 40 different
kinase targets of dasatinib andshowed that SRC, FYN, and EGFR are
relevant targets fordasatinib action in NSCLC (32). Our recent
phase I/IIstudy showed that dasatinib combined with erlotinib
istolerable, with 63% of patients with advanced NSCLCshowing
disease control, including two having partialresponse and one
having bone response (48). Anothergroup also showed that dasatinib
combined with erloti-nib is safe and feasible in NSCLC (49).
On the basis of these clinical studies along with theexperiments
reported here, dasatinib has potential clinicalactivity in NSCLC
treatment, but this is limited to
Table 1. Src phosphorylation detected in human NSCLC samples
with T790M gatekeeper mutation
Patient ID EGFR mutant H score Intensity Cellularity
1 T790M/L858R 3 1 32 T790M/19del(E746-A750) 4 2 23
T790M/19del(E746-A750) 6 2 34 T790M/L858R 6 2 35
T790M/19del(E746-A750) 6 2 36 T790M/19del(E746-A750) 9 3 37
T790M/19del(E746-A750) 9 3 38 T790M/L858R 9 3 39 (Pre-TKI)
19del(E746-A750) 9 3 39 (Post-TKI) T790M/19del(E746-A750) 9 3 310
(Pre-TKI) L858R 4 2 210 (Post-TKI) T790M/L858R 9 3 3
NOTE: Patient 9 was treated with "gefitinib and erlotinib."
Patient 10 was treated with "gefitinib and erlotinib þ ARQ197
(MET-TKI)."
Yoshida et al.
Clin Cancer Res; 20(15) August 1, 2014 Clinical Cancer
Research4072
on June 19, 2021. © 2014 American Association for Cancer
Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst June 11, 2014; DOI:
10.1158/1078-0432.CCR-13-1559
http://clincancerres.aacrjournals.org/
-
combinationswith T790M-targeted agents and in genotype-specific
patients. Thiswill be formally tested in a phase I trialof afatinib
and dasatinib (NCT01999985). Our results alsohighlight the ability
of phosphoproteomics to identify otherimportantmediators of drug
sensitivity, and examinationofthese proteins may be important in
clinical studies ofT790M-targeting agents.
Disclosure of Potential Conflicts of InterestE.B. Haura reports
receiving a commercial research grant from Boehrin-
ger-Ingelheim. No potential conflicts of interest were disclosed
by the otherauthors.
Authors' ContributionsConception and design: T. Yoshida, G.
Zhang, E.B. HauraDevelopment of methodology: T. Yoshida, G. Zhang,
M.A. Smith,A.S. Lopez, Y. Bai, J. Koomen, E.B.
HauraAcquisitionofdata (provided animals, acquired
andmanagedpatients,provided facilities, etc.): T. Yoshida, G.
Zhang, M.A. Smith, B. Fang,J. Koomen, K. Nakagawa, E.B.
HauraAnalysis and interpretation of data (e.g., statistical
analysis, biosta-tistics, computational analysis):G. Zhang, M.A.
Smith, A.S. Lopez, Y. Bai,B. Fang, B. Rawal, K.J. Fisher, A.Y.
Chen, I. Okamoto, K. Nakagawa, E.B.HauraWriting, review, and/or
revisionof themanuscript: T. Yoshida,G. Zhang,M.A. Smith, B. Fang,
J. Koomen, B. Rawal, A.Y. Chen, K. Nakagawa,E.B. Haura
Administrative, technical, or material support (i.e., reporting
or orga-nizing data, constructing databases): T. Yoshida, G. Zhang,
M.A. Smith,A.S. Lopez, Y. Bai, J. Li, M. Kitano, Y. Morita, H.
Yamaguchi, K. Shibata,T. Okabe, I. Okamoto, K. Nakagawa, E.B.
HauraStudy supervision: K. Nakagawa, E.B. Haura
AcknowledgmentsThe authors thank the Moffitt pY Group, the Kinki
University Medical
Oncology Research Group, Tsutomu Iwasa, and Kunio Okamoto for
helpfuldiscussions, Rasa Hamilton for editorial assistance, Fumi
Kinose for assis-tance with cell culture, and Linda Ley and Carol
Ulge for administrativeassistance. The authors also thank BML, Inc
and SRL, Inc for technicalassistance.
Grant SupportThe work was partially funded by grants from the
Moffitt Cancer Center
SPORE in Lung Cancer (P50-CA119997), the V Foundation for
CancerResearch, and in part by the National Cancer Institute, part
of the NIH,through grant number 2 P30-CA76292-14, which provide
support to theProteomics Core, the Flow Cytometry Core, the Tissue
Core, and the AnimalFacility at the H. Lee Moffitt Cancer Center
and Research Institute, an NCI-designated Comprehensive Cancer
Center.
The costs of publication of this article were defrayed in part
by thepayment of page charges. This article must therefore be
hereby markedadvertisement in accordance with 18 U.S.C. Section
1734 solely to indicatethis fact.
Received June 13, 2013; revised April 9, 2014; accepted April
23, 2014;published OnlineFirst June 11, 2014.
References1. Mok TS, Wu YL, Thongprasert S, Yang CH, Chu DT,
Saijo N, et al.
Gefitinib or carboplatin-paclitaxel in pulmonary
adenocarcinoma.N Engl J Med 2009;361:947–57.
2. Mitsudomi T, Morita S, Yatabe Y, Negoro S, Okamoto I,
Tsurutani J,et al. Gefitinib versus cisplatin plus docetaxel in
patients with non-small-cell lung cancer harbouring mutations of
the epidermal growthfactor receptor (WJTOG3405): an open label,
randomised phase 3 trial.Lancet Oncol 2010;11:121–8.
3. Kobayashi S, Boggon TJ, Dayaram T, Janne PA, Kocher O,
MeyersonM, et al. EGFRmutation and resistanceof non-small-cell
lungcancer togefitinib. N Engl J Med 2005;352:786–92.
4. Pao W, Miller VA, Politi KA, Riely GJ, Somwar R, Zakowski MF,
et al.Acquired resistance of lung adenocarcinomas to gefitinib or
erlotinib isassociated with a second mutation in the EGFR kinase
domain. PLoSMed 2005;2:e73.
5. Kosaka T, Yatabe Y, Endoh H, Yoshida K, Hida T, Tsuboi M, et
al.Analysis of epidermal growth factor receptor genemutation in
patientswith non-small cell lung cancer and acquired resistance to
gefitinib.Clin Cancer Res 2006;12:5764–9.
6. Sequist LV, Waltman BA, Dias-Santagata D, Digumarthy S, Turke
AB,Fidias P, et al. Genotypic and histological evolution of lung
cancersacquiring resistance to EGFR inhibitors. Sci Transl Med
2011;3:75ra26.
7. Yu HA, Arcila ME, Rekhtman N, Sima CS, Zakowski MF, Pao W, et
al.Analysis of tumor specimens at the time of acquired resistance
toEGFR-TKI therapy in 155 patients with EGFR-mutant lung
cancers.Clin Cancer Res 2013;19:2240–7.
8. Engelman JA, Mukohara T, Zejnullahu K, Lifshits E, Borras AM,
GaleCM, et al. Allelic dilution obscures detection of a
biologically significantresistance mutation in EGFR-amplified lung
cancer. J Clin Invest2006;116:2695–706.
9. Engelman JA, Zejnullahu K, Gale CM, Lifshits E, Gonzales AJ,
Shi-mamura T, et al. PF00299804, an irreversible pan-ERBB
inhibitor, iseffective in lung cancer models with EGFR and ERBB2
mutations thatare resistant to gefitinib. Cancer Res
2007;67:11924–32.
10. Li D, Ambrogio L, Shimamura T, Kubo S, Takahashi M, Chirieac
LR,et al. BIBW2992, an irreversible EGFR/HER2 inhibitor highly
effectivein preclinical lung cancer models. Oncogene
2008;27:4702–11.
11. Kwak EL, Sordella R, Bell DW, Godin-Heymann N, Okimoto
RA,Brannigan BW, et al. Irreversible inhibitors of the EGF receptor
maycircumvent acquired resistance to gefitinib. Proc Natl Acad Sci
U S A2005;102:7665–70.
12. Sos ML, Rode HB, Heynck S, Peifer M, Fischer F, Kluter S, et
al.Chemogenomic profiling provides insights into the limited
activity ofirreversible EGFR inhibitors in tumor cells expressing
the T790MEGFRresistance mutation. Cancer Res 2010;70:868–74.
13. Yun CH, Mengwasser KE, Toms AV, Woo MS, Greulich H, Wong
KK,et al. The T790M mutation in EGFR kinase causes drug resistance
byincreasing the affinity for ATP. Proc Natl Acad Sci U S A
2008;105:2070–5.
14. Yu Z, Boggon TJ, Kobayashi S, Jin C, Ma PC, Dowlati A, et
al.Resistance to an irreversible epidermal growth factor receptor
(EGFR)inhibitor in EGFR-mutant lung cancer reveals novel treatment
strate-gies. Cancer Res 2007;67:10417–27.
15. Godin-Heymann N, Ulkus L, Brannigan BW, McDermott U, Lamb
J,Maheswaran S, et al. The T790M "gatekeeper" mutation in
EGFRmediates resistance to low concentrations of an irreversible
EGFRinhibitor. Mol Cancer Ther 2008;7:874–9.
16. Shimamura T, Li D, Ji H, Haringsma HJ, Liniker E, Borgman
CL,et al. Hsp90 inhibition suppresses mutant EGFR-T790M
signalingand overcomes kinase inhibitor resistance. Cancer Res
2008;68:5827–38.
17. Yamada T, Matsumoto K, Wang W, Li Q, Nishioka Y, Sekido Y,
et al.Hepatocyte growth factor reduces susceptibility to an
irreversibleepidermal growth factor receptor inhibitor in
EGFR-T790M mutantlung cancer. Clin Cancer Res 2010;16:174–83.
18. Ercan D, Zejnullahu K, Yonesaka K, Xiao Y, Capelletti M,
Rogers A,et al. Amplification of EGFRT790Mcauses resistance to an
irreversibleEGFR inhibitor. Oncogene 2010;29:2346–56.
19. Miller VA, Hirsh V, Cadranel J, Chen YM, Park K, Kim SW, et
al. Afatinibversus placebo for patients with advanced, metastatic
non-small-celllung cancer after failure of erlotinib, gefitinib, or
both, and one or twolines of chemotherapy (LUX-Lung 1): a phase
2b/3 randomised trial.Lancet Oncol 2012;13:528–38.
20. Regales L, Gong Y, Shen R, de Stanchina E, Vivanco I, Goel
A, et al.Dual targeting of EGFR can overcome a major drug
resistance
www.aacrjournals.org Clin Cancer Res; 20(15) August 1, 2014
4073
Phosphoproteomics of EGFR-TKI Resistance
on June 19, 2021. © 2014 American Association for Cancer
Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst June 11, 2014; DOI:
10.1158/1078-0432.CCR-13-1559
http://clincancerres.aacrjournals.org/
-
mutation in mouse models of EGFR mutant lung cancer. J Clin
Invest2009;119:3000–10.
21. Li D, Shimamura T, Ji H, Chen L, Haringsma HJ, McNamara K,
et al.Bronchial and peripheral murine lung carcinomas induced by
T790M-L858R mutant EGFR respond to HKI-272 and rapamycin
combinationtherapy. Cancer Cell 2007;12:81–93.
22. Stommel JM, Kimmelman AC, Ying H, Nabioullin R, Ponugoti
AH,Wiedemeyer R, et al. Coactivation of receptor tyrosine kinases
affectsthe response of tumor cells to targeted therapies.
Science2007;318:287–90.
23. Wilson TR, Fridlyand J, Yan Y, Penuel E, Burton L, Chan E,
et al.Widespread potential for growth-factor-driven resistance to
antican-cer kinase inhibitors. Nature 2012;487:505–9.
24. Harbinski F, Craig VJ, Sanghavi S, Jeffery D, Liu L,
Sheppard KA, et al.Rescue screens with secreted proteins reveal
compensatory potentialof receptor tyrosine kinases in driving
cancer growth. Cancer Discov2012;2:948–59.
25. Yano S, Wang W, Li Q, Matsumoto K, Sakurama H, Nakamura T,
et al.Hepatocyte growth factor induces gefitinib resistance of lung
adeno-carcinoma with epidermal growth factor receptor-activating
muta-tions. Cancer Res 2008;68:9479–87.
26. Machida K, Eschrich S, Li J, Bai Y, Koomen J, Mayer BJ, et
al.Characterizing tyrosine phosphorylation signaling in lung cancer
usingSH2 profiling. PLoS ONE 2010;5:e13470.
27. Naoki K, Soejima K, Okamoto H, Hamamoto J, Hida N, Nakachi
I, et al.The PCR-invadermethod (structure-specific 50
nuclease-basedmeth-od), a sensitive method for detecting EGFR gene
mutations in lungcancer specimens; comparison with direct
sequencing. Int J ClinOncol 2011;16:335–44.
28. Engelman JA, Zejnullahu K, Mitsudomi T, Song Y, Hyland C,
Park JO,et al. MET amplification leads to gefitinib resistance in
lung cancer byactivating ERBB3 signaling. Science
2007;316:1039–43.
29. Zhang G, Fang B, Liu RZ, Lin H, Kinose F, Bai Y, et al.
Massspectrometrymapping of epidermal growth factor receptor
phosphor-ylation related to oncogenic mutations and tyrosine kinase
inhibitorsensitivity. J Proteome Res 2011;10:305–19.
30. Lynn DJ, Winsor GL, Chan C, Richard N, Laird MR, Barsky A,
et al.InnateDB: facilitating systems-level analyses of the
mammalian innateimmune response. Mol Syst Biol 2008;4:218.
31. Saito R, Smoot ME, Ono K, Ruscheinski J, Wang PL, Lotia S,
et al.A travel guide to Cytoscape plugins. Nat Methods
2012;9:1069–76.
32. Li J, Rix U, Fang B, Bai Y, Edwards A, Colinge J, et al. A
chemical andphosphoproteomic characterization of dasatinib action
in lung cancer.Nat Chem Biol 2010;6:291–9.
33. Ogino A, Kitao H, Hirano S, Uchida A, Ishiai M, Kozuki T, et
al.Emergence of epidermal growth factor receptor T790M
mutationduring chronic exposure to gefitinib in a non small cell
lung cancercell line. Cancer Res 2007;67:7807–14.
34. Rush J, Moritz A, Lee KA, Guo A, Goss VL, Spek EJ, et al.
Immu-noaffinity profiling of tyrosine phosphorylation in cancer
cells. NatBiotechnol 2005;23:94–101.
35. Gentile A, Lazzari L, Benvenuti S, Trusolino L, Comoglio PM.
Ror1 is apseudokinase that is crucial forMet-driven tumorigenesis.
Cancer Res2011;71:3132–41.
36. Zhang Z, Lee JC, Lin L, Olivas V, Au V, LaFramboise T, et
al. Activationof the AXL kinase causes resistance to EGFR-targeted
therapy in lungcancer. Nat Genet 2012;44:852–60.
37. Komiyama NH, Watabe AM, Carlisle HJ, Porter K, Charlesworth
P,Monti J, et al. SynGAP regulates ERK/MAPK signaling,
synapticplasticity, and learning in the complex with postsynaptic
density 95and NMDA receptor. J Neurosci 2002;22:9721–32.
38. Rumbaugh G, Adams JP, Kim JH, Huganir RL. SynGAP
regulatessynaptic strength and mitogen-activated protein kinases in
culturedneurons. Proc Natl Acad Sci U S A 2006;103:4344–51.
39. Cantalupo G, Alifano P, Roberti V, Bruni CB, Bucci C.
Rab-interactinglysosomal protein (RILP): the Rab7 effector required
for transport tolysosomes. EMBO J 2001;20:683–93.
40. Zhou W, Ercan D, Chen L, Yun CH, Li D, Capelletti M, et al.
Novelmutant-selective EGFR kinase inhibitors against EGFR T790M.
Nature2009;462:1070–4.
41. Chandarlapaty S. Negative feedback and adaptive resistance
to thetargeted therapy of cancer. Cancer Discov 2012;2:311–9.
42. MachidaK, ThompsonCM,DierckK, Jablonowski K, KarkkainenS,
LiuB, et al. High-throughput phosphotyrosine profiling using
SH2domains. Mol Cell 2007;26:899–915.
43. Faber AC, Li D, Song Y, Liang MC, Yeap BY, Bronson RT, et
al.Differential induction of apoptosis in HER2 and EGFR addicted
can-cers following PI3K inhibition. Proc Natl Acad Sci U S A
2009;106:19503–8.
44. Kim JY,Welsh EA, Oguz U, Fang B, Bai Y, Kinose F, et al.
Dissection ofTBK1 signaling via phosphoproteomics in lung cancer
cells. Proc NatlAcad Sci U S A 2013;110:12414–9.
45. Johnson ML, Riely GJ, Rizvi NA, Azzoli CG, Kris MG, Sima
CS,et al. Phase II trial of dasatinib for patients with acquired
resistanceto treatment with the epidermal growth factor receptor
tyrosinekinase inhibitors erlotinib or gefitinib. J Thorac Oncol
2011;6:1128–31.
46. Zhang J, KalyankrishnaS,WislezM, ThilaganathanN, Saigal
B,WeiW,et al. SRC-family kinases are activated in non-small cell
lung cancerand promote the survival of epidermal growth factor
receptor-depen-dent cell lines. Am J Pathol 2007;170:366–76.
47. Leung EL, Tam IY, Tin VP, Chua DT, Sihoe AD, Cheng LC, et
al.SRC promotes survival and invasion of lung cancers with
epider-mal growth factor receptor abnormalities and is a potential
can-didate for molecular-targeted therapy. Mol Cancer Res
2009;7:923–32.
48. Haura EB, Tanvetyanon T, Chiappori A, Williams C, Simon G,
AntoniaS, et al. Phase I/II study of the Src inhibitor dasatinib in
combinationwith erlotinib in advanced non-small-cell lung cancer. J
Clin Oncol2010;28:1387–94.
49. Johnson FM, Tang X, Tran HT, McIntyre C, Price J, Lee JJ, et
al. Aphase I/II study combining dasatinib (D) and erlotinib (E) in
non-smallcell lung cancer. J Clin Oncol 31, 2013 (suppl; abstr
8102).
Clin Cancer Res; 20(15) August 1, 2014 Clinical Cancer
Research4074
Yoshida et al.
on June 19, 2021. © 2014 American Association for Cancer
Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst June 11, 2014; DOI:
10.1158/1078-0432.CCR-13-1559
http://clincancerres.aacrjournals.org/
-
Correction
Correction: Tyrosine PhosphoproteomicsIdentifies Both Codrivers
and CotargetingStrategies for T790M-Related EGFR-TKIResistance in
Non–Small Cell Lung Cancer
In this article (ClinCancer Res
2014;20:4059–74),whichwaspublished in theAugust1, 2014, issue of
Clinical Cancer Research (1), an author's name was misprinted.The
corrected name should read as follows: "Y. Ann Chen." The authors
regret thiserror.
Reference1. Yoshida T, Zhang G, Smith MA, Lopez AS, Bai Y, Li J,
et al. Tyrosine phosphoproteomics identifies
both codrivers and cotargeting strategies for T790M-related
EGFR-TKI resistance in non–small celllung cancer. Clin Cancer Res
2014;20:4059–74.
Published online August 3, 2015.doi:
10.1158/1078-0432.CCR-15-1183�2015 American Association for Cancer
Research.
ClinicalCancerResearch
www.aacrjournals.org 3571
-
2014;20:4059-4074. Published OnlineFirst June 11, 2014.Clin
Cancer Res Takeshi Yoshida, Guolin Zhang, Matthew A. Smith, et
al.
Small Cell Lung Cancer−Non Cotargeting Strategies for
T790M-Related EGFR-TKI Resistance in
Tyrosine Phosphoproteomics Identifies Both Codrivers and
Updated version
10.1158/1078-0432.CCR-13-1559doi:
Access the most recent version of this article at:
Material
Supplementary
http://clincancerres.aacrjournals.org/content/suppl/2014/06/16/1078-0432.CCR-13-1559.DC1
Access the most recent supplemental material at:
Cited articles
http://clincancerres.aacrjournals.org/content/20/15/4059.full#ref-list-1
This article cites 48 articles, 25 of which you can access for
free at:
Citing articles
http://clincancerres.aacrjournals.org/content/20/15/4059.full#related-urls
This article has been cited by 11 HighWire-hosted articles.
Access the articles at:
E-mail alerts related to this article or journal.Sign up to
receive free email-alerts
Subscriptions
Reprints and
[email protected]
To order reprints of this article or to subscribe to the
journal, contact the AACR Publications Department at
Permissions
Rightslink site. Click on "Request Permissions" which will take
you to the Copyright Clearance Center's (CCC)
.http://clincancerres.aacrjournals.org/content/20/15/4059To
request permission to re-use all or part of this article, use this
link
on June 19, 2021. © 2014 American Association for Cancer
Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst June 11, 2014; DOI:
10.1158/1078-0432.CCR-13-1559
http://clincancerres.aacrjournals.org/lookup/doi/10.1158/1078-0432.CCR-13-1559http://clincancerres.aacrjournals.org/content/suppl/2014/06/16/1078-0432.CCR-13-1559.DC1http://clincancerres.aacrjournals.org/content/20/15/4059.full#ref-list-1http://clincancerres.aacrjournals.org/content/20/15/4059.full#related-urlshttp://clincancerres.aacrjournals.org/cgi/alertsmailto:[email protected]://clincancerres.aacrjournals.org/content/20/15/4059http://clincancerres.aacrjournals.org/
/ColorImageDict > /JPEG2000ColorACSImageDict >
/JPEG2000ColorImageDict > /AntiAliasGrayImages false
/CropGrayImages false /GrayImageMinResolution 200
/GrayImageMinResolutionPolicy /Warning /DownsampleGrayImages true
/GrayImageDownsampleType /Bicubic /GrayImageResolution 300
/GrayImageDepth -1 /GrayImageMinDownsampleDepth 2
/GrayImageDownsampleThreshold 1.50000 /EncodeGrayImages true
/GrayImageFilter /DCTEncode /AutoFilterGrayImages true
/GrayImageAutoFilterStrategy /JPEG /GrayACSImageDict >
/GrayImageDict > /JPEG2000GrayACSImageDict >
/JPEG2000GrayImageDict > /AntiAliasMonoImages false
/CropMonoImages false /MonoImageMinResolution 600
/MonoImageMinResolutionPolicy /Warning /DownsampleMonoImages true
/MonoImageDownsampleType /Bicubic /MonoImageResolution 900
/MonoImageDepth -1 /MonoImageDownsampleThreshold 1.50000
/EncodeMonoImages true /MonoImageFilter /CCITTFaxEncode
/MonoImageDict > /AllowPSXObjects false /CheckCompliance [ /None
] /PDFX1aCheck false /PDFX3Check false /PDFXCompliantPDFOnly false
/PDFXNoTrimBoxError true /PDFXTrimBoxToMediaBoxOffset [ 0.00000
0.00000 0.00000 0.00000 ] /PDFXSetBleedBoxToMediaBox true
/PDFXBleedBoxToTrimBoxOffset [ 0.00000 0.00000 0.00000 0.00000 ]
/PDFXOutputIntentProfile (None) /PDFXOutputConditionIdentifier ()
/PDFXOutputCondition () /PDFXRegistryName () /PDFXTrapped
/False
/CreateJDFFile false /Description > /Namespace [ (Adobe)
(Common) (1.0) ] /OtherNamespaces [ > /FormElements false
/GenerateStructure false /IncludeBookmarks false /IncludeHyperlinks
false /IncludeInteractive false /IncludeLayers false
/IncludeProfiles false /MarksOffset 18 /MarksWeight 0.250000
/MultimediaHandling /UseObjectSettings /Namespace [