Embed Size (px)
Citation preview

Annals of Surgical Oncology, 2(5):407--415 Published by Lippincott-Raven Publishers © 1995 The Society of Surgical Oncology, Inc.
Improved Survival in Young Women with Breast Cancer
Benjamin O. Anderson, MD, Ruby T. Senie, PhD, John T. Vetto, MD, George Y. Wong, PhD, Beryl McCormick, MD, and Patrick I. Borgen, MD
Background: Young age has been hypothesized to be an adverse prognostic factor for women with breast cancer. This association, based on historical data, may not reflect recent advances in breast cancer management.
Methods: A retrospective study was conducted of all women age 30 or younger who underwent definitive operation at our institution for primary operable breast carcinoma during one of two consecutive 20-year periods (1950-1969 or 1970-1989). All cancers were restaged according to current staging criteria. Actuarial survival and recurrence-free sur- vival rates from the two patient eras were compared with each other and with published statistics for older breast cancer patients.
Results: Eligibility criteria were met by 81 women from the 1950-1969 era and 146 women from the 1970-1989 era. Histologic diagnoses, tumor sizes, incidence of axillary nodal metastases, number of positive nodes, and American Joint Committee on Cancer stage at presentation were similarly distributed in the two eras. Despite these similarities, improved survival (p = 0.009) was observed in the later era. Local recurrences were also more common (p < 0.05) in the later era in association with less extensive resections. These local recurrences had an adverse impact on recurrence-free survival in the later era, but no concomitant decrease in overall survival was observed. Node-positive patients who re- ceived chemotherapy demonstrated a trend toward improved survival (p = 0.06) compared with node-positive patients who did not. Survival for patients in the later era was similar to that for older women as reported in other published series.
Conclusions: The stage of presentation of breast cancer in women 30 years or younger appears unchanged from prior decades, but survival has improved in association with the use of less extensive surgical resections and the introduction of cytotoxic chemotherapy. With current treatment, primary operable breast cancer in young women appears to have a similar prognosis to breast cancer in older women.
Key Words: Breast cancer--Young age--Local recurrence --Chemotherapy.
Breast cancer in young women has long been sus- pected to be an aggressive malignancy portending limited survival. In 1940, James Ewing wrote that " t he relatively malignant course of most structural
Received March 29, 1994; accepted August !, 1994. From the Departments of Surgery (B.O.A., R.T.S., P.I.B.)
and Radiation Oncology (B.M.) Memorial Sloan-Kettering Can- cer Center, New York, New York, and Division of General Sur- gery, Oregon Health Sciences University, Portland, Oregon (J.T.V.), and Strang Cancer Prevention Center, Cornell Univer- sity, New York, New York (G.Y.W.).
Address correspondence and reprint requests to Dr. Benjamin O. Anderson, University of Washington, Department of Sur- gery, Box 356410, Seattle, WA 98195, USA
Results of this study were presented at the 47th Annual Cancer Symposium of The Society of Surgical Oncology, Houston, Texas, March 17-20, 1994, and was judged "Best Clinical Pa- per" in the Resident/Fellow Essay Contest.
types of [breast cancer] in young subjects is widely r e c o g n i z e d " (1). H o w e v e r , recent inves t iga tors have questioned this traditional belief (2-4). Epste in notes that multiple studies favoring an associat ion between youth and disease aggression are balanced by others reporting comparable or bet ter outcomes in young patients with breast cancer (5).
Epidemiologic data conflict regarding the prog- nostic significance of young age at diagnosis. Swan- son reported data f rom the Surveillance, Epidemi- ology and End Results (SEER) program suggesting that women in their 20s and 30s have an increased likelihood of dying of breast cancer in the first 5 years after diagnosis (6). However , data f rom the Na t iona l Swedish C a n c e r Reg i s t ry shows that women with breast cancer diagnosed before the age of 30 have cumulat ive relative survival rates similar
407

408 B. O. ANDERSON ET AL.
to those for the breast cancer population as a whole (7). Neither report stratified young patients by TNM stage.
Studies of breast cancer in young women have generally been hindered by the low frequency of this disease in the 2nd and 3rd decades of life. Less than 0.5% of breast cancer cases occur in women age 30 or younger (7). Fewer than 2% of breast biopsies in women age 30 or younger demonstrate malignancy (8). Because of low patient accrual, pre- vious studies have been unable to answer whether young age at diagnosis is a predictor of poor out- come, after controlling for stage of disease (5,9).
Improved public awareness, widespread mam- mographic screening, optimal preoperative selec- tion, superior radiation therapy techniques, and the use of systemic chemotherapy have all contributed to modern breast cancer diagnosis and manage- ment. Between 1973 and 1987, the incidence of breast cancer in the United States increased 36%. Despite this increase, the annual mortality from breast cancer stabilized (26.9 to 27.1 per 100,000) (10). Previously, we found that women age 30 years or younger treated at Memorial Sloan-Kettering Cancer Center (MSKCC) between 1950 and 1970 had decreased survival compared with older pa- tients (11). In the current study, we ask whether current treatment has benefitted women in this young age group and assess whether breast cancer in young women still appears to be more aggressive than similarly staged disease in older women.
METHODS
Patient selection and exclusions This retrospective study included all women
treated at the MSKCC from the years 1950 to 1989 who (a) had primary operable breast carcinoma di- agnosed at or before the age of 30, (b) underwent definitive operation at our institution, and (c) were followed for at least 6 months after operation. Pa- tients were excluded if they (a) underwent primary operation (other than biopsy) at another center, (b) had locally advanced or metastatic (stages IIIB or IV) breast cancer at presentation, (c) had a histo- logic diagnosis other than adenocarcinoma, or (d) could not be restaged with available information. Patients who underwent primary treatment else- where were excluded to decrease the patient selec- tion bias inherent in a tertiary care center and to obtain the most accurate actuarial survival rates.
Data collection Data was collected through chart review and di-
rect patient or family member contact. To ensure staging uniformity, each cancer was restaged ac- cording to the most current (1992) American Joint Committee on Cancer (AJCC) system (12). Tumor size, nodal status, number of metastatic nodes, and histologic diagnosis were taken directly from the final pathology report. In cases where the patholog- ic description was insufficient to determine an exact or approximate tumor size (n = 55), the size esti- mated on clinical examination was used. In cases in which nodal metastases were identified but the pathologic description was inadequate to determine an exact or approximate number of positive nodes (n = 4), the nodal status was classified as node positive without further subclassification. To estab- lish a diagnosis of "favorable" ductal carcinoma variant (papillary, medullary, colloid, or tubular carcinoma), all of the ducts with malignant changes were required to demonstrate the specified charac- teristics. For the purposes of analysis, breast can- cers developing in the ipsilateral breast or chest wall following the original operation were assumed to be local recurrences rather than new primary cancers.
Statistical analysis Follow-up time was calculated using the date of
definitive operation as the index date. Actuarial sur- vival rates were calculated using the method of Ka- plan and Meier (13). Survival and relapse-free sur- vival curves were truncated at 10 years for statisti- cal comparison, because median survival time differed between the two patient eras. Differences in actuarial survival rates were compared using the log-rank test. Differences in the prevalence of risk factors and cancer therapies were compared using ×2 analysis (14). Multivariate analysis was per- formed using Cox's method of calculating the pro- portional hazard ratio. Statistical significance was defined at the p < 0.05 level. P values between 0.05 and 0.07 were considered to represent a suggestive trend not achieving statistical significance.
RESULTS
Patient population From 1950 to 1989, 425 women age 30 years and
younger were treated for breast cancer at the MSKCC. No males were identified as having devel- oped breast cancer in this age group.
Ann Surg Oncol, Vol. 2, No. 5, 1995
BREAST CANCER IN YOUNG WOMEN 409
NUMBER OF PATIENTS
60
n=Z27
50
40
30
2O
~° Rid 0 17 18 t9 20 21 22 23 24 25 26 27 28 29 30
AGE AT DIAGNOSIS (years)
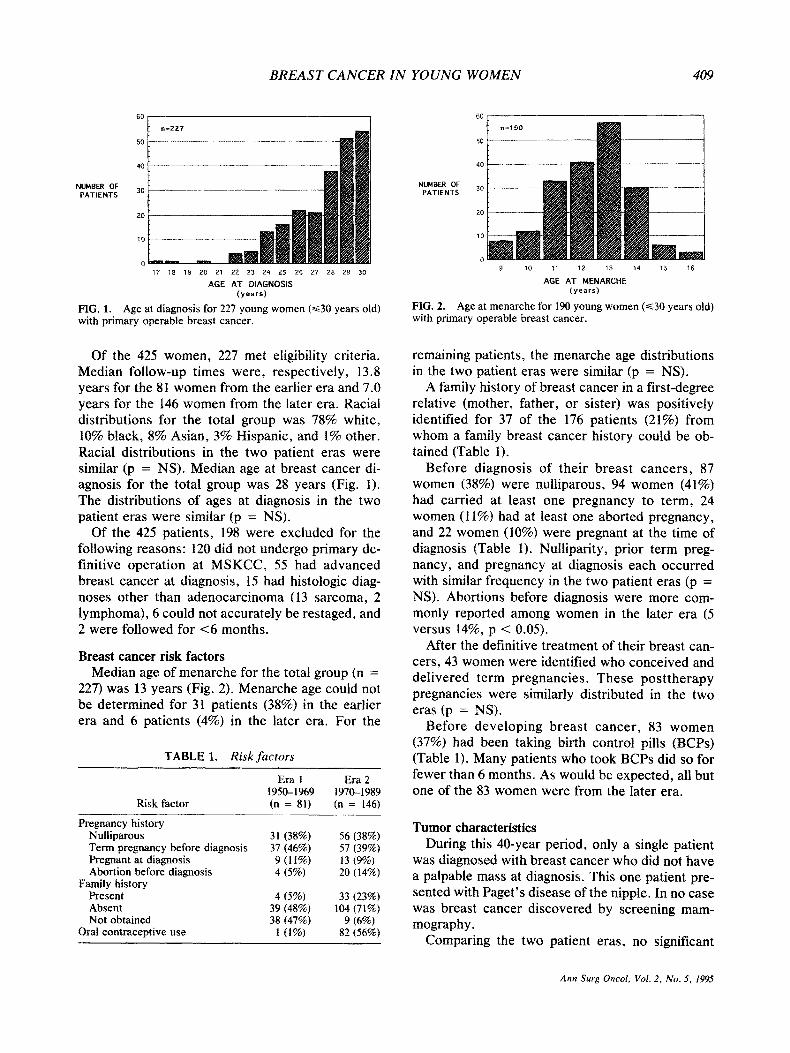
FIG. 1. Age at diagnosis for 227 young women (~<30 years old) with primary operable breast cancer.
Of the 425 women, 227 met eligibility criteria. Median follow-up times were, respectively, 13.8 years for the 81 women from the earlier era and 7.0 years for the 146 women from the later era. Racial distributions for the total group was 78% white, 10% black, 8% Asian, 3% Hispanic, and 1% other. Racial distributions in the two patient eras were similar (p = NS). Median age at breast cancer di- agnosis for the total group was 28 years (Fig. t). The distributions of ages at diagnosis in the two patient eras were similar (p = NS).
Of the 425 patients, 198 were excluded for the following reasons: 120 did not undergo primary de- finitive operat ion at MSKCC, 55 had advanced breast cancer at diagnosis, 15 had histologic diag- noses other than adenocarcinoma (13 sarcoma, 2 lymphoma), 6 could not accurately be restaged, and 2 were followed for <6 months.
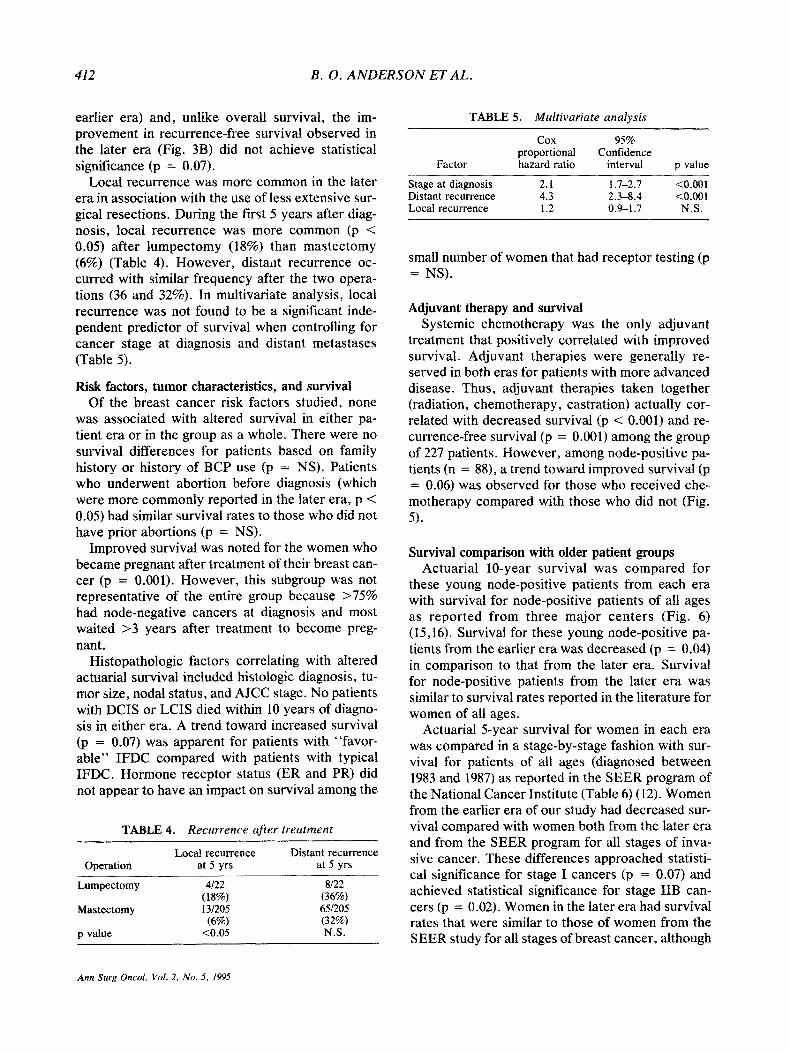
Breast cancer risk factors Median age of menarche for the total group (n =
227) was 13 years (Fig. 2). Menarche age could not be determined for 31 patients (38%) in the earlier era and 6 patients (4%) in the later era. For the
TABLE 1. Risk factors
Risk factor
Era 1 Era 2 1950-1969 1970-1989 (n = 81) (n = 146)
Pregnancy history Nulliparous 31 (38%) 56 (38%) Term pregnancy before diagnosis 37 (46%) 57 (39%) Pregnant at diagnosis 9 (1 !%) 13 (9%) Abortion before diagnosis 4 (5%) 20 (14%)
Family history Present 4 (5%) 33 (23%) Absent 39 (48%) 104 (71%) Not obtained 38 (47%) 9 (6%)
Oral contraceptive use 1 (1%) 82 (56%)
60
n=190
50 - -
NUMBER OF °0 -- L PATIENTS 3O
ZO
10
0 9 10 11 12 13 14 15 16
AGE AT MENARCHE (years)
FIG, 2. Age at menarche for 190 young women (~<30 years old) with primary operable breast cancer.
remaining patients, the menarche age distributions in the two patient eras were similar (p = NS).
A family history of breast cancer in a first-degree relative (mother, father, or sister) was positively identified for 37 of the 176 patients (21%) from whom a family breast cancer history could be ob- tained (Table 1).
Before diagnosis of their b reas t cance r s , 87 women (38%) were nulliparous, 94 women (41%) had carried at least one pregnancy to term, 24 women (11%) had at least one aborted pregnancy, and 22 women (10%) were pregnant at the time of diagnosis (Table 1). Nulliparity, prior term preg- nancy, and pregnancy at diagnosis each occurred with similar f requency in the two patient eras (p = NS). Abortions before diagnosis were more com- monly reported among women in the later era (5 versus 14%, p < 0.05).
After the definitive treatment of their breast can- cers, 43 women were identified who conceived and del ivered term pregnancies . These pos t the rapy pregnancies were similarly distributed in the two eras (p --- NS).
Before deve loping b reas t cancer , 83 w o m e n (37%) had been taking birth control pills (BCPs) (Table 1). Many patients who took BCPs did so for fewer than 6 months. As would be expected, all but one of the 83 women were from the later era.
Tumor characteristics During this 40-year period, only a single patient
was diagnosed with breast cancer who did not have a palpable mass at diagnosis. This one patient pre- sented with Paget 's disease of the nipple. In no case was breast cancer discovered by screening mam- mography.
Comparing the two patient eras, no significant
Ann Surg Oncol, Vol. 2, No. 5, 1995

410 B. O. A N D E R S O N E T A L .
differences in the distribution of tumor histologies was apparent (Table 2). Purely in situ carc inoma (DCIS or LCIS with no invasive or microinvasive component) was identified in 23 women (I0%). Al- though a greater proport ion of women from the later era had ductal or lobular in situ carcinoma, the dif- ference was not statistically significant (7 versus 12%, p = NS). Infiltrating ductal carc inoma (IFDC) and its histologic var iants was identified in 202 women (89%). The incidence of IFDC was similar in the two patient eras (91 versus 88%, p = NS). Of the 202 I F D C cases , 29 were " f a v o r a b l e " variants that were evenly distributed in the two patient eras (15 versus 14%, p = NS). Infiltrating lobular carci- noma was rare, occurring in two women (1%), one f rom each era.
No differences were identified in the distribution of any factor(s) that define current staging criteria (Table 2). Variables that were similarly distributed in the two patient eras included histologic diagno- sis, t umor size, incidence of axillary nodal me- tastases, number of posit ive axillary nodes, and fi- nal AJCC stage (p = NS).
Tumor estrogen receptor (ER) status was deter- mined for 65 women (29%) beginning in the 1970s. Of those who were tested, 43 women (66%) had ER-negat ive tumors and 22 women (34%) had ER- posit ive tumors . Progesterone receptor (PR) status
TABLE 2. Staging
Tumor staging
Era 1 Era 2 1950-1969 1970--1989 (n = 81) (n = 146)
Histologic diagnosis Lobular carcinoma in situ 1 (1%) 1 (1%) Ductal carcinoma in situ 5 (6%) 16 (11%) Infiltrating ductal carcinoma (IFDC) 63 (78%) 110 (75%) Favorable IFDC 11 (14%) 18 (12%) Infiltrating lobular carcinoma 1 (1%) 1 (1%)
Tumor size (cm) In situ (any size) 6 (7%) i7 (12%) ~<2,0 27 (33%) 57 (39%) 2.1-5.0 43 (53%) 58 (40%) >~5.1 5 (6%) 14 (10%)
Nodal metastases Node negative 50 (62%) 89 (61%) 1-3 9 (11%) 29 (20%) 4-10 10 (12%) 19 (13%) >10 8 (10%) 9 (6%)
AJCC stage 0 6 (7%) 17 (12%) I 19 (23%) 38 (26%) IIA 30 (37%) 50 (34%) IIB 23 (28%) 25 (17%) IliA 3 (4%) 16 (11%)
AJCC, American Joint Committee on Cancer.
Ann Surg Oncol, Vol. 2, No. 5, 1995
TABLE 3. Treatment
Treatment
Era 1 Era 2 1950-1969 1970-1989 (n = 81) (n = 146)
Operative selection Lumpectomy 1 (1%) 21 (14%) Simple mastectomy 1 (1%) 0 (0%) Modified radical mastectomy 1 (1%) 89 (61%) Radical mastectomy 70 (86%) 33 (23%) Extended radical mastectomy 8 (10%) 3 (2%)
Adjuvant treatment None 41 (51%) 82 (56%) Radiation therapy alone 30 (37%) 11 (8%) Radiation + chemotherapy 0 (0%) 17 (12%) Chemotherapy alone 0 (0%) 36 (25%) Castration (oophorectomy) I0 (12%) 0 (0%)
was also determined in 52 patients: 19 were PR pos- itive and 33 were PR negative.
Operative and adjuvant therapy (Table 3) Operat ive therapy significantly changed be tween
the two patient eras, with more radical operat ions being supplanted by less extensive resections. In the later era, more women underwent lumpec tomy or modif ied radical m a s t e c t o m y , whereas f ewer women underwent radical or extended radical mas- tec tomy (p < 0.05).
Adjuvant therapy also changed be tween the two patient eras. In the later era, fewer women received adjuvant radiation (37 versus 19%, p < 0.05) and selected women received adjuvant chemothe rapy (0 versus 36%, p < 0.05) with or without radiation. Radiation therapy was used in conjunct ion with lumpec tomy as standard care evolved in the later era.
Recurrence and survival Actuarial survival was increased (p = 0.009) for
women treated be tween 1970 and 1989 compared with women from the earlier (1950-1969) t reatment era (Fig. 3A). Among patients who died of breast cancer, median survival after initial t rea tment was longer for women treated in the later era (3.2 years versus 2.8 years in the earlier era). Similarly, me- dian su rv iva l a f t e r r e c u r r e n c e was longe r for women treated in the later era (2.3 years versus I. 1 years in the earlier era).
Local recurrence was relatively more c o m m o n in the later era (Fig. 4). Overall , 38 patients (47%) in the earlier era and 45 patients (31%) in the later era developed recurrence breast cancer (local and/or distant) during the first 10 years after pr imary treat- ment. Among these, local recurrence developed in 5

BREAST CANCER IN YOUNG WOMEN 411
A
ACTUARIAL SURVIVAL
1 . 0 '
0.8
0.6
0.4
. . . . . . . . 1 9 5 0 - 6 9 p = 0.009
0 . 0 I I , l , I I , I
0 2 4 6 8 10 TIME AFTER DIAGNOSIS
patients a t r isk a t ( yea rs ) o, 5 and 10 years .
1 9 7 0 - 8 9 . . . . 1 4 6 . . . . . . . . . . . . . . . . . . . . . . . . . 9 5 . . . . . . . . . . . . . . . . . . . . . . . . . 4 3 1 9 5 0 - 6 9 . . . . 8 1 . . . . . . . . . . . . . . . . . . . . . . . . . 5 5 . . . . . . . . . . . . . . . . . . . . . . . . . 4 4
B 1.0'
0.8
ACI'UARIAL 0.6 RELAPSE-FREE
SURVIVAL 0.4
--- . .... -+ .......... 4... _ _wr, .,F ......... +
+ 1 9 7 0 - 8 9 ] 0.2 . . . . . . . . 1 9 5 0 - 6 9 p = 0.07
0 . 0 , I , I , I I
0 2 4 6 8 t 0 TIME AFTER DIAGNOSIS
Pltients I t r isk a t ( y e a r s ) o, 5 and l O yea~ :
1 9 7 0 - 8 9 . . . . 1 4 6 . . . . . . . . . . . . . . . . . . . . . . . . . 8 6 . . . . . . . . . . . . . . . . . . . . . . . . . 41 1 9 5 0 - ( ; 9 . . . . 8 1 . . . . . . . . . . . . . . . . . . . . . . . . . 4 7 . . . . . . . . . . . . . . . . . . . . . . . . . 4 2
FIG. 3. Actuarial survival (A) and recurrence- free survival (B) after definitive operation for breast cancer in young women (~<30 years old) from two consecutive 20-year eras (1950-1969 or 1970--1989). Actuarial survival was increased (p = 0.009) for women from the later era. Ac- tuarial recurrence-free survival appeared to be increased for women from the later era, but this trend did not achieve statistical significance (p = 0.07).
patients (6%) in the earlier era and 15 patients (10%) in the later era. Therefore , the relative rate of local recurrence was 13% (5 of 38) in the earlier era and 33% (15 of 45) in the later era.
The higher rate of local recurrence negatively in- fluenced recurrence-free survival in the later era. In
FIG. 4. Patterns of recurrence during the first decade after defini- tive operation for breast cancer in young women (~<30 years old) from two c o n s e c u t i v e 20-year e ras (1950-1969 [left] or 1970-1989 [right]). Five of 38 patients (13%) had local recurrence in the earlier era. Fifteen of 45 patients (33%) had local recurrence in the later era. Thus, local recurrence was rel- atively more common in the later era (p < 0.05). 1 9 5 0 - 1 9 6 9
both eras, local recurrence manifested earlier than did distant recurrence at a median time of 11.8 months for local recurrence versus 20.7 months for distant recurrence. As a result, the overall median time to recurrence (local and/or distant) in the later era was shortened (1.4 years versus 1.8 years in the
Im LOCAL ONLY
m ~ + DISTJ~I"
[ ] DtsrANT ONLY [] NO REOJRm,~
1 9 7 0 - 1 9 8 9
Ann Surg Oncot, Vol. 2, No. 5, 1995
412 B. O. A N D E R S O N ET AL.
earlier era) and, unlike overall survival, the im- provement in recurrence-free survival observed in the later era (Fig. 3B) did not achieve statistical significance (p = 0.07).
Local recurrence was more common in the later era in association with the use of less extensive sur- gical resections. During the first 5 years after diag- nosis, local recurrence was more common (p < 0.05) after lumpectomy (18%) than mastectomy (6%) (Table 4). However, distant recurrence oc- curred with similar frequency after the two opera- tions (36 and 32%). In multivariate analysis, local recurrence was not found to be a significant inde- pendent predictor of survival when controlling for cancer stage at diagnosis and distant metastases (Table 5).
Risk factors, tumor characteristics, and survival Of the breast cancer risk factors studied, none
was associated with altered survival in either pa- tient era or in the group as a whole. There were no survival differences for patients based on family history or history of BCP use (p = NS). Patients who underwent abortion before diagnosis (which were more commonly reported in the later era, p < 0.05) had similar survival rates to those who did not have prior abortions (p = NS).
Improved survival was noted for the women who became pregnant after treatment of their breast can- cer (p = 0.001). However, this subgroup was not representative of the entire group because >75% had node-negative cancers at diagnosis and most waited >3 years after treatment to become preg- nant.
Histopathologic factors correlating with altered actuarial survival included histologic diagnosis, tu- mor size, nodal status, and AJCC stage. No patients with DCIS or LCIS died within 10 years of diagno- sis in either era. A trend toward increased survival (p = 0.07) was apparent for patients with "favor- able" IFDC compared with patients with typical IFDC. Hormone receptor status (ER and PR) did not appear to have an impact on survival among the
T A B L E 4. Recurrence a f ter t r ea tmen t
Operation Local recurrence Distant recurrence
at 5 yrs at 5 yrs
Lumpectomy 4/22 8/22 (18%) (36%)
Mastectomy 13/205 65/205 (6%) (32%)
p value <0.05 N.S.
TABLE 5. Mul t ivar ia te analys is
Cox 95% proportional Confidence
Factor hazard ratio interval p value
Stage at diagnosis 2.1 t .7-2.7 <0.001 Distant recurrence 4.3 2.3-8.4 <0.001 Local recurrence 1.2 0.9-1.7 N.S.
small number of women that had receptor testing (p = NS).
Adjuvant therapy and survival Systemic chemotherapy was the only adjuvant
treatment that positively correlated with improved survival. Adjuvant therapies were generally re- served in both eras for patients with more advanced disease. Thus, adjuvant therapies taken together (radiation, chemotherapy, castration) actually cor- related with decreased survival (p < 0.001) and re- currence-free survival (p = 0.001) among the group of 227 patients. However, among node-positive pa- tients (n = 88), a trend toward improved survival (p = 0.06) was observed for those who received che- motherapy compared with those who did not (Fig. 5).
Survival comparison with older patient groups Actuarial 10-year survival was compared for
these young node-positive patients from each era with survival for node-positive patients of all ages as reported from three major centers (Fig. 6) (15,16). Survival for these young node-positive pa- tients from the earlier era was decreased (p = 0.04) in comparison to that from the later era. Survival for node-positive patients from the later era was similar to survival rates reported in the literature for women of all ages.
Actuarial 5-year survival for women in each era was compared in a stage-by-stage fashion with sur- vival for patients of all ages (diagnosed between 1983 and 1987) as reported in the SEER program of the National Cancer Institute (Table 6) (12). Women from the earlier era of our study had decreased sur- vival compared with women both from the later era and from the SEER program for all stages of inva- sive cancer. These differences approached statisti- cal significance for stage I cancers (p = 0.07) and achieved statistical significance for stage liB can- cers (p = 0.02). Women in the later era had survival rates that were similar to those of women from the SEER study for all stages of breast cancer, although
Ann Surg Oncol, Vol. 2, No. 5, 1995

B R E A S T C A N C E R I N Y O U N G W O M E N 413
FIG. 5. Actuarial survival after definitive op- eration for node-positive breast cancer in young women (~30 years old) who did or did not re- ceive chemotherapy. A trend toward increased actuarial survival (p = 0.06) was observed for node-positive women who did receive chemo- therapy.
ACTUARIAL SURVIVAL
1.0
0.8
0.6
0.4
0.2
. - - Z
N O D E - P O S I T I V E P A T I E N T S :
N ..... C H E M O T H E R A P Y
: N O C H E M O T H E R A P Y p = 0 . 0 6
0 .0 v I ~ I , I I I
0 2 4 6 8 10 TIME AFTER DIAGNOSIS
Patients ;It risk at ( y e a r s ) O. 5 and 10 yea's:
CHEMO . . . . 43 . . . . . . . . . . . . . . . . . . . . . . . . . 19 . . . . . . . . . . . . . . . . . . . . . . . . . 5 NO CHEMO . . . . 4S . . . . . . . . . . . . . . . . . . . . . . . . . 20 . . . . . . . . . . . . . . . . . . . . . . . . . 10
the power of this subset analysis was limited by small numbers of patients in each group.
DISCUSSION
In this study, primary operable breast cancer di- agnosed in women 30 years or younger was ana- lyzed, comparing two sequential 20-year eras of di- agnosis and management (1950--1969 versus 1970-- 1989). We have previously reported that young women treated in the earlier era had decreased sur- vival compared with breast cancer patients of all ages taken as a group, i.e., mostly older patients (11).
The specific goals of this analysis were to (a) identify a group of women age 30 years or younger
60 NODE-POSITIVE PATIENTS
T , ¢ / / / / A
Y////A . . . . . . . / I / / I t A
4 0 - - " / 1 1 1 1 / - - " ~ ' / I / / / ~ / Y / / / / A ~.-.'H~ 10 -YEAR ¢ 1 1 1 / I ,
ACTUARIAL , / / . . " / .-'d / / / / / / # SURVIVAL / / / / / . . - j
¢ ,6 ) V / / / / / ,
e / / / / / ~
t / z / i / ¢ e / / / z l ~ z / l l / / ~
Zn=yy/~ ;n.=.~43.: 1950 -69 1970 -89 MSKCC MO ~ ~ "1~ INSI"
YOUNG WOMEN WOMEN OF ALL AGES
FIG. 6. Actuarial 10-year survival after definitive operation for node-positive breast cancer in young women (<~30 years old) from two consecutive 20-year eras (1950-1969 or 1970-1989) and for patients of all ages from three independent patient series (15,16). Actuarial survival for node-positive young women from the later era was increased (p = 0.04) compared with women from the earlier era but appeared similar to survival for node- positive women of all ages as reported in the literature.
treated for primary operable breast cancer during two sequential 20-year periods (1950-1969 or 1970- 1989), (b) characterize breast cancer risk factors for the total group and compare their relative distribu- tions in the two patient eras, (c) determine each patient's breast cancer stage at presentation using current staging criteria, (d) assess survival and re- currence-free survival rates for each of the two study groups, and (e) compare these survival rates with each other and with published statistics for similarly staged breast cancer patients in the gen- eral population.
The principal observations of the current study were that (a) breast cancer presented at similar stages in the two eras, but women treated in the later era had improved survival; (b) the relative in- crease in local recurrence in the later era (appar- ently related to the use of less radical resections) could not be shown to have an adverse impact on overall survival; (c) the survival benefit seen with node-positive cancers was associated with the use of systemic chemotherapy; and (d) survival for node-positive patients in the later era was similar to
T A B L E 6. S u r v i v a l by stage at d i a g n o s i s
5-Yr actuarial survival
Cancer Young women Young women All ages stage 1950-1969 1970-1989 (SEER data)
I 84.2 ---+ 8.4% 97.0 --+ 2.7% 95% (n = 19) (n = 38) (n = 16,519)
IIA 76.1 --+ 7.9% 80.2 --. 5.9% 86% (n = 30) (n = 50) (n = 14,692)
liB 47.8 +- 10.4% 68.2 -+ 10.0% 70% (n = 23) (n = 25) (n = 8,283)
I l iA 33.3 +- 27.2% 38.9 --+- 13.4% 52% (n = 3) (n = 16) (n = 1,656)
Ann Surg Oncot, re'ot. 2, No. 5, 1995

414 B. O. ANDERSON ET AL.
that for node-positive women in the general popu- lation, i.e., mostly older patients.
The increased incidence of local recurrence in the later era and its association with the use of less extensive resections is noteworthy. Patients who underwent breast conservation surgery had signifi- cantly increased local recurrence rates (18 versus 6% for mastectomy at 5 years). However, no cor- responding decrease in overall survival in the lump- ectomy patients was observed. Rather, a similar percentage of women who underwent lumpectomy developed synchronous or metachronous distant re- currences as did those who underwent mastectomy (36 versus 32%) at 5 years. These data are consis- tent with Bernard Fisher's hypothesis that local re- currence is a marker of risk for, rather than a cause of, distant metastases (17). However, longer follow- up beyond 5 years would be needed to further sup- port or refute this hypothesis.
All women in both eras presented with a physical finding indicative of malignant pathology. In no case was breast cancer diagnosed by screening mammography. Thus, we would agree that the ben- efits of screening mammography, which decreases cancer mortality for women older than age 50 (18), remains unproven for women 30 years or younger. It is known that 45% of women 30 years or younger with clinically evident disease will not demonstrate focal abnormalities on a mammogram because of high parenchymal density (19).
Young patients with breast cancer are more likely to have a positive family history than older women who develop the disease. Among these women who knew their family cancer history, 21% described breast cancer in a first-degree relative. Only 11% of breast cancer patients of all ages have a first-degree relative with breast cancer (20).
The association between young age at diagnosis and family history of breast cancer may be ex- plained by Knudsen's "two-hit" model of carcino- genesis (21). Hypothetically, a women inheriting a gene predisposing her to breast cancer (e.g., BRCA1 or mutated p53) is at risk for developing cancer at an earlier age because fewer subsequent somatic mutations would be necessary to acquire frankly malignant breast cancer cells. The associa- tion between young age and family history pre- dicted by the Knudsen model and observed in our patient population explains the tendency seen in fa- milial breast cancer toward earlier age at diagnosis with successive generations (22).
Young women with a family history of breast can-
cer demonstrated survival rates similar to those of young women with no family history of cancer in our study. This finding suggests that a woman who has a positive family history and who develops breast cancer at a young age does not necessarily have a poor prognosis.
Among adjuvant treatments, only chemotherapy was positively associated with improved survival and only in node-positive patients. The improve- ment approached but did not achieve statistical sig- nificance, presumably because of the small number of patients in each group. Our data support the hy- pothesis that adjuvant chemotherapy arrests micro- scopic disease that manifests as distant, ultimately fatal metastases.
In summary, our study suggests that young age at breast cancer diagnosis is not a poor prognostic in- dicator independent from stage at diagnosis. Rather, young women with early breast cancers have prognoses that with current management are similar to those for older women with disease of similar stage. It is possible that changes in environ- mental factors, dietary habits, or reproductive his- tories have also influenced the biology of the breast cancer in an epigenetic manner, resulting in an al- tered virulence of the disease.
Acknowledgment: We thank Dr. Celia Menedez-Botet, Raffi Chaglassian, Kathy Tran, and Vivian Wu for their invaluable assistance in data collection and chart review.
REFERENCES
1. Ewing J. Epithelial and other tumors of the breast. In: Ewing J, ed. Neoplastic diseases, a treatise on tumors, 4th ed. Philadelphia: WB Saunders, 1940:587--8.
2, Muscolino G, Villani C, Bedini AV, Luini A, Salvadori B. Young age is not an ominous prognostic factor in breast cancer patients. Tumori 1987;73:233-5.
3. Backhouse CM, Lloyd-Davies ERV, Shousha S, Burn JI. Carcinoma of the breast in women aged 35 or less. Br J Surg 1987;74:591-3.
4. Editorial. Breast cancer in young women. Br Med J 1975;2: 649-50.
5. Epstein R. Analysis of natural history of breast cancer in young women. Lancet 1992;340:1287.
6. Swanson GM. Breast cancer in younger women: survival patterns. Female Patient t993;18:53-6.
7. Adami HO, Malker B, Holmberg L, Persson I, Stone B. The relation between survival and age at diagnosis in breast can- cer. New Engl J Med 1986;315:559-63.
8. Ferguson CM, Powell RW. Breast masses in young women. Arch Surg 1989;124:1338-41.
9. Breast cancer in young women: more questions than an- swers. Oncot Bull 1993;16:14--8.
10. Qualters JR, Lee NC, Smith RA, Aubert RE. Breast and cervical cancer surveillance, United States, 1973-1987. Mor- bidity Mortality Weekly Rep 1992;41:1-15.
11. Lee CG, McCormick B, Mazumdar M, Vetto J, Borgen PI.
Ann Surg Oncot, Vol. 2, No. 5. 1995

B R E A S T C A N C E R I N Y O U N G W O M E N 415
Infiltrating breast carcinoma in patients age 30 years and younger: long term outcome for life, relapse, and second primary tumors, lnt J Radiat Oncol Biol Phys 1992;23:969- 75.
12. Breast cancer staging. In: American Joint Committee on Cancer. Manual for staging of cancer, 4th ed. Philadelphia: JB Lippincott, 1992:149-54.
13. Kaplan EL, Meier P. Nonparametric estimation from incom- plete observations. Am Stat Assoc J 1958;53:457-81.
14. Glantz SA. The chi-square test statistic. In: Primer ofbio- statistics, 2nd ed. New York: McGraw-Hill, 1987:122-6.
15. Schottenfeld D, Nash AG, Robbins GF, Beattie EJ. Ten- year results of the treatment of primary operable breast car- cinoma: a summary of 304 patients evaluated by the TNM system. Cancer 1976;38:1001-7.
16. Cascinelli N, Singletary E, Greco M, et al. Long-term sur- vival and prognostic factors for 2170 breast cancer patients treated at two cancer centers. Tumori 1989;75:123-31.
17. Fisher B, Anderson S, Fisher ER, et al. Significance of ip- silateral breast tumour recurrence after lumpectomy. Lancet 1991 ;338(8763):327-31.
18. Smart CR, Hartmann WH, Beahrs OH, Garfinkel L. Insights into breast cancer screening of younger women. Cancer Suppl 1993;72:1449-56.
19. Liberman L, Giess C, Borgen PI, Deutch BM, Dershaw DD. Presented at the 78th Scientific Assembly of the Radiologic Society of North America, Chicago, Illinois, 1992.
20. Adami HO, Hansen J, Jung B, Rimsten A. Familiality in breast cancer: a case-control study in a Swedish population. Br J Cancer 1980;42:71-7.
21. Knudson AG Jr. Mutation and cancer: statistical study of retinoblastoma. Proc Natl Acad Sci USA 1971;68:820-3.
22. Senie RT, Simkovich A, Kinne DW, Borgen PI. Genera- tional shifting in mean age at diagnosis of breast cancer [Ab- stract]. Breast Cancer Res Treat 1993;27:173.
Ann Surg Oncot, Vot. 2, No. 5, 1995





























