Embed Size (px)
Citation preview

J Chin Med Assoc • May 2006 • Vol 69 • No 5224
CASE REPORT
Introduction
The genital examination, among the series of physicalexaminations for newborns, is often ignored byphysicians, although an imperforate hymen is not arare condition in female newborns. In the literature,imperforate hymen usually presents at puberty withprimary amenorrhea, abdominal pain, andhematocolpos. Infants with an imperforate hymenmay present with an abdominal mass, obstructiveuropathy, and hydrocolpos, which is difficult to detect.Lobar nephronia or acute focal bacterial nephritis(AFBN) is a rare pediatric condition that can be causedby either a hematogenous route or an ascendinginfection. The former is usually caused by Staphylococcusand the latter by a Gram-negative bacterial infection asa consequence of a congenital urinary tract anomaly.We report an unusual case of a 2-year-old girl with animperforate hymen and pyocolpos that compressedthe left ureter and caused a hydroureter, hydronephrosis,and lobar nephronia.
Imperforate Hymen Complicated withPyocolpos and Lobar Nephronia
Mao-Chang Shen1, Ling-Yu Yang1,2*1Department of Pediatrics, Taipei Veterans General Hospital, and 2National Yang-Ming
University School of Medicine, Taipei, Taiwan, R.O.C.
An imperforate hymen is not a rare condition in female newborns, but is often ignored in a genital examination
by physicians. Lobar nephronia is a rare condition in pediatric patients that can be screened by ultrasound or computed
tomography to distinguish it from a renal abscess. Treatment for lobar nephronia requires at least 14 days of
antimicrobial therapy and a follow-up assessment by renal ultrasonography or dimercaptosuccinic acid scan. We
report an unusual case of a 2-year-old girl with an imperforate hymen and pyocolpos. The pyocolpos compressed
the left lower ureter to cause hydroureter, hydronephrosis, and nephronia. Partial hymenotomy was performed to
drain the pus, and antibiotics were administered for a total of 3 weeks. There was a good outcome. This case
demonstrates the need to perform a full physical examination, particularly a genital examination, in newborns. Further,
if gynecologic pathology is suspected, then urologic screening studies are recommended to rule out potential associated
anomalies. [J Chin Med Assoc 2006;69(5):224–227]
Key Words: imperforate hymen, lobar nephronia, pyocolpos
Case Report
A 2-year-old girl was brought to our emergency roombecause of intermittent high fever (up to 42°C) ofunknown origin for the previous 4 days. Her parentssaid that the child had been lethargic and had a poorappetite; she had not had an upper respiratory tractor gastrointestinal tract infection, and there was nosignificant past medical or contributing family history.The physical examination revealed no abnormalfindings; however, a genital examination was not doneat that time. The laboratory findings showed: peripheralleukocyte count, 19,700/mm3; differential (segment/lymphocyte/monocyte) 80/4/11.2; and C-reactiveprotein, 12.01 mg/dL. Urinalysis revealed: whiteblood cell, 3+/HPF(high-power field); red blood cell,10/HPF; and positive nitrite reaction. She was admittedto our ward for further evaluation and treatment.
After admission, ampicillin and gentamicin wereadministered; however, the fever persisted even after48 hours of antibiotic treatment. Renal ultrasound
©2006 Elsevier. All rights reserved.
*Correspondence to: Dr. Ling-Yu Yang, Division of Pediatric Nephrology, Department of Pediatrics, TaipeiVeterans General Hospital, 201, Section 2, Shih-Pai Road, Taipei 112, Taiwan, R.O.C.E-mail: [email protected] • Received: September 30, 2005 • Accepted: December 26, 2005
*050916/Imper/out/ppp 5/10/06, 3:32 PM224
Imperforate hymen complicated with pyocolpos
J Chin Med Assoc • May 2006 • Vol 69 • No 5 225
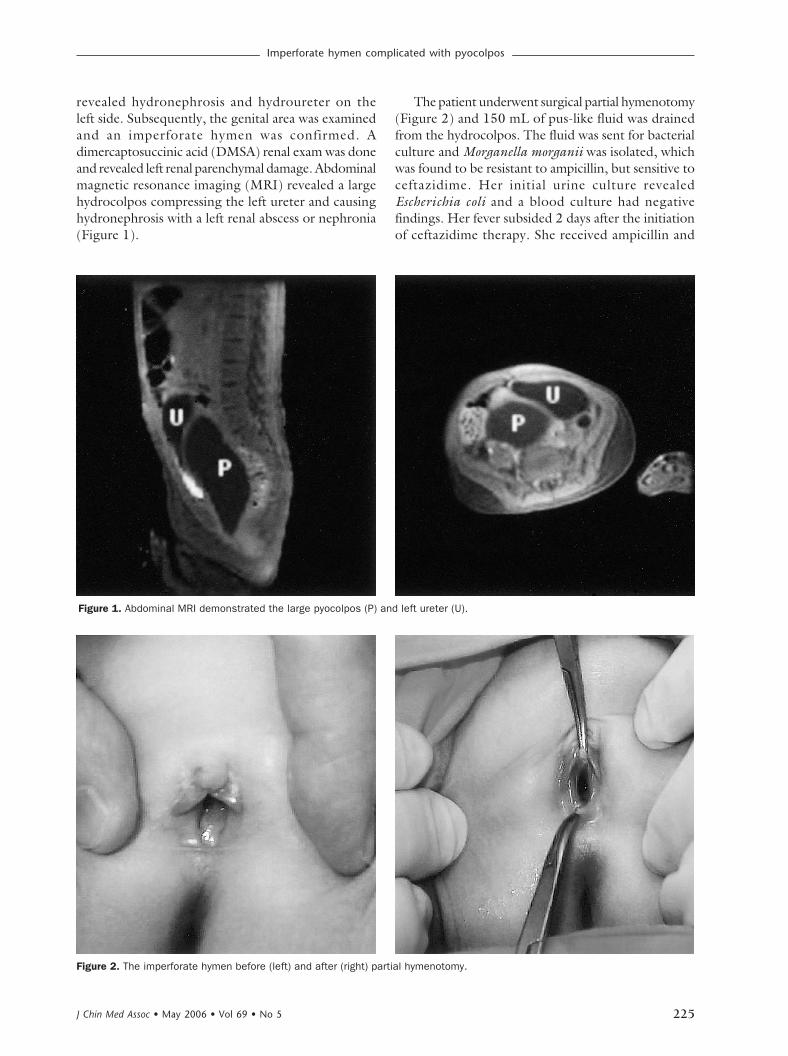
revealed hydronephrosis and hydroureter on theleft side. Subsequently, the genital area was examinedand an imperforate hymen was confirmed. Adimercaptosuccinic acid (DMSA) renal exam was doneand revealed left renal parenchymal damage. Abdominalmagnetic resonance imaging (MRI) revealed a largehydrocolpos compressing the left ureter and causinghydronephrosis with a left renal abscess or nephronia(Figure 1).
The patient underwent surgical partial hymenotomy(Figure 2) and 150 mL of pus-like fluid was drainedfrom the hydrocolpos. The fluid was sent for bacterialculture and Morganella morganii was isolated, whichwas found to be resistant to ampicillin, but sensitive toceftazidime. Her initial urine culture revealedEscherichia coli and a blood culture had negativefindings. Her fever subsided 2 days after the initiationof ceftazidime therapy. She received ampicillin and
Figure 2. The imperforate hymen before (left) and after (right) partial hymenotomy.
Figure 1. Abdominal MRI demonstrated the large pyocolpos (P) and left ureter (U).
*050916/Imper/out/ppp 5/10/06, 3:32 PM225

M.C. Shen, L.Y. Yang
J Chin Med Assoc • May 2006 • Vol 69 • No 5226
gentamicin for 7 days and ceftazidime for another 14days. The follow-up urine analysis and vaginal bacterialculture were normal. A follow-up renal ultrasounddemonstrated resolution of the nephronia 2 weekslater. Because the parents were returning home to theUSA, she was discharged and received follow-up carethere.
Discussion
Pyocolpos, an infected fluid collection within thevagina, is a rare condition. The etiology may includean imperforate hymen, a transverse vaginal septum,and maternal estrogen overstimulation.1 Clinicalsymptoms are usually insidious, unless it becomes anevident mass in the lower abdomen or when itcompresses the ureter and causes hydronephrosis or aurinary tract infection. Treatment is dependent uponthe etiology. If it is caused by an imperforate hymen,then a hymenotomy should be performed.2
An imperforate hymen is not a rare condition infemale newborns. The incidence can be 1 in 1,000,3
but genital examination is frequently ignored in thephysical examination of newborns. Morganellamorganii is normal flora in the gastrointestinal tract,but not in the genitourinary tract. In this patient, thepyocolpos may have resulted from bacterial seeding bya hematogenous route.4
Lobar nephronia, also known as acute focal bacterialnephritis (AFBN), is a renal mass caused by focalinfection without liquefaction. The process usuallyinvolves 1 or more renal lobules. AFBN may occurnear a renal abscess, so it can reasonably be assumedto precede or lead to a renal abscess. An AFBN orrenal abscess may result from spreading via thehematogenous route or an ascending infection.Because of the high incidence of urinary tractabnormalities, urologic evaluation, such as avoidingcystourethrogram (VCUG), is warranted.5 An AFBNis usually distinguished from a renal abscess by renalultrasonography. The former shows a focal hypo-echoic area with poorly defined margins and the lattershows clearly defined margins and a central anechoicarea. A computed tomography (CT) scan is consideredthe most sensitive and specific radiologic modality todiagnose AFBN by demonstrating a solid wedge-shaped area that contains poorly marginated regionsof decreased enhancement.6 We ordered renalultrasound as a screening test to detect renal swelling,bulging, or enlargement; however, in the opinion ofSoulen and colleagues,7 renal ultrasound should notbe used for lesions that may require invasive therapy.
Although CT scan is the preferred form of imaging,it is best used only in children showing abnormalitieson the ultrasonography and who do not respond wellto antibiotics, or when a renal abscess is clinicallysuspected.5 The DMSA scans are the imaging modalityof choice for detecting renal scarring in children andmight be useful in the follow-up during the late phaseof an AFBN,8 although AFBN is rare among thepediatric population. Symptoms of AFBN are usuallynonspecific and most patients have fever, abdominalpain, and flank pain. Antimicrobial therapy tailoredto the urinary pathogens is recommended inAFBN for a minimum of 14 days. The resolution ofinf lammatory changes, as detected on theultrasonography, starts after 4–6 weeks of treatmentin uncomplicated cases.9,10 Follow-up studies oftendetect renal scarring in the majority of the childrenaffected with AFBN.11–14 As we learned from thiscase, the importance of a detailed physical examinationto include the genital area cannot be overestimated.Because of the high incidence of associated urinarytract abnormalities and urinary tract infection, aninitial renal ultrasonography or even a whole abdomenultrasonography and a urologic evaluation forscreening are recommended.
References
1. Heller DS. Lower genital tract disease in children andadolescents: a review. J Pediatr Adolesc Gynecol 2005;18:75–83.
2. Brevetti LS, Kimura K, Brevetti GR, Lawrence JP, Soper RT.Pyocolpos: diagnosis and treatment. J Pediatr Surg 1997;32:110–1.
3. Kahn R, Duncan B, Bowes W. Spontaneous opening ofcongenital imperforated hymen. J Pediatr 1975;87:768–70.
4. Rosenberg-Arska M, Visser MR. Enterobacteriaceae. In: CohenJ, Powderly WG, Berkley SF, Calandra T, eds. Cohen &Powderly: Infectious Diseases, 2nd edition. Philadelphia: Mosby,2004:2199–201.
5. Uehling DT, Hahnfeld LE, Scanlan KA. Urinary tractabnormalities in children with acute focal bacterial nephritis.BJU Int 2000;85:885–8.
6. Gold RP, McClennan BL, Rettenberg RR. CT appearance ofacute inflammatory diseases of the renal interstitium. Am JRoentgenol 1983;141:343–9.
7. Soulen MC, Fishman EK, Goldman SM, Gatewood OM. Bacterialrenal injection: role of CT. Radiology 1989;171:703–7.
8. Clautice-Engle T, Jeffrey RB. Renal hypoperfusion: valueof power Doppler imaging. Am J Roentgenol 1997;168:1227–31.
9. Kline MW, Kaplan SL, Baker CJ. Acute focal bacterial nephritis:diverse clinical presentation in pediatric patients. Pediatr InfectDis 1988;7:346–9.
10. Rathore MH, Barton LL, Luisiri A. Acute lobar nephronia: areview. Pediatrics 1991;87:728–34.
11. Siegel AJ, Glaiser CM. Acute focal bacterial nephritis in children:significance of reflux. Am J Roentgenol 1981;137:257–60.
*050916/Imper/out/ppp 5/10/06, 3:32 PM226

Imperforate hymen complicated with pyocolpos
J Chin Med Assoc • May 2006 • Vol 69 • No 5 227
12. Rushton HG, Majd M, Jantausch B, Wiedermann BL, BelmanAB. Renal scarring following reflux and nonrefluxpyelonephritis in children: evaluation with 99mtechnetium -dimercaptosuccinic acid scintigraphy. J Urol 1992;147:1327–32.
13. Nosher JL, Tamminen JL, Anorosa JK, Kallich M. Acute focalbacterial nephritis. Am J Kidney Dis 1988;11:36–42.
14. Benador D, Benador N, Slosman D, Mermillod B, Girardin E.Are younger children at highest risk of renal sequelae afterpyelonephritis? Lancet 1997;349:17–9.
*050916/Imper/out/ppp 5/10/06, 3:32 PM227





























