Embed Size (px)
Citation preview

01
Impact of Overall Survival in Advanced NSCLC EGFR+Dr. E. Omar Macedo PérezThoracic Tumors Clinic; INCan

02
Topics
• Review of OS data for chemotherapy:– Doublet with platinum– Histology-based therapy
• Review of OS data with bevacizumab
• Review of OS data with first-generation TKIs
• Review of OS for afatinib (2nd-Generation TKI): OS analysis of LUX-Lung 3 and 6
• Future of OS in NSCLC with EGFR mutated
• Conclusions
Afatinib is approved in a number of markets, including the EU, Japan, Taiwan and Canada under the brand name GIOTRIF® and in the U.S. under the brand name GILOTRIF® for use in patients with distinct types of EGFR mutation-positive NSCLC. Registration conditions differ internationally, please refer to locally approved prescribing information. Afatinib is under regulatory review by health authorities in other countries worldwide. Afatinib is not approved in other indications.

03
1. American Cancer Society Cancer Facts and Figures 2012.2. Epidemiology of Lung Cancer. Chest. 2007;132:29S-55S.3. GLOBOCAN 2012 (IARC).
Lung Cancer: First Cause of Death Due to Cancer Worldwide
• 1.8 million new cases/year
• 1.62 million deaths/year
• 226,000 new cases
• 160,000 deaths
04
GLO
BO
CA
N 2
012
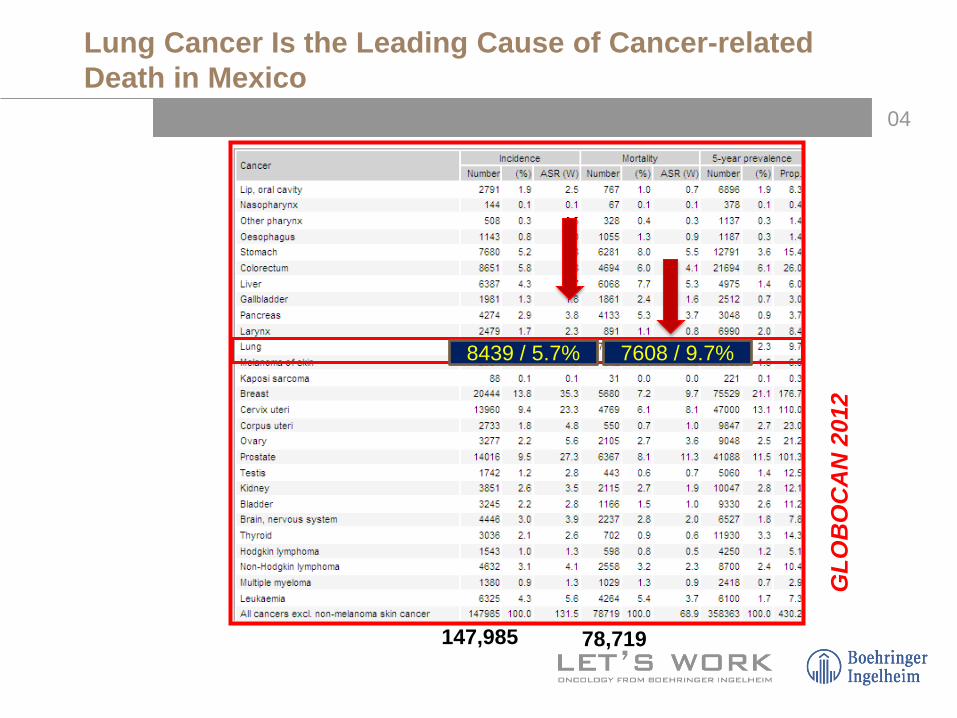
8439 / 5.7% 7608 / 9.7%
147,985 78,719
Lung Cancer Is the Leading Cause of Cancer-relatedDeath in Mexico

05
0
10
20
30
40
50
60
70
80
90
Stages I and II Stage III Stage IV
USA Mexico
15%
1.2%
25%
16.8%
82%
60%
SEER Cancer Statistics Review, 1975-2008.Macedo EO and Arrieta O. INCan Data 2009-2014.
85% will require palliative treatment!!
NSCLC: Stages at Diagnosis (USA vs Mexico)

06
AJCC 7th edition.
OS in Advanced Stages
07
Review of OS Data for Chemotherapy (First-Line)

08
Karnofsky DA, et al. Cancer. 1948;1:634-656.Kennedy BJ. Cancer. 1998;82:801-803.
1948

09
Progress in Lung Cancer Research
1995CT vs BSC:CT standard
2006QT +
Bevacizumab

010
NSCLC Collaborative Group. BMJ. 1995;311:899-909.
1995
Meta-analyses Confirm Survival Benefit With Chemotherapy in Advanced NSCLC
• N=778 patients
• 11 clinical trials
• Cisplatin plus etoposide or vinca alkaloids
• At 1 year, an absoluteimprovement in OS of 10%
• An increased median survivalof 1.5 months (P<0.0001)

011
New Drugs for Treatment of NSCLC
012
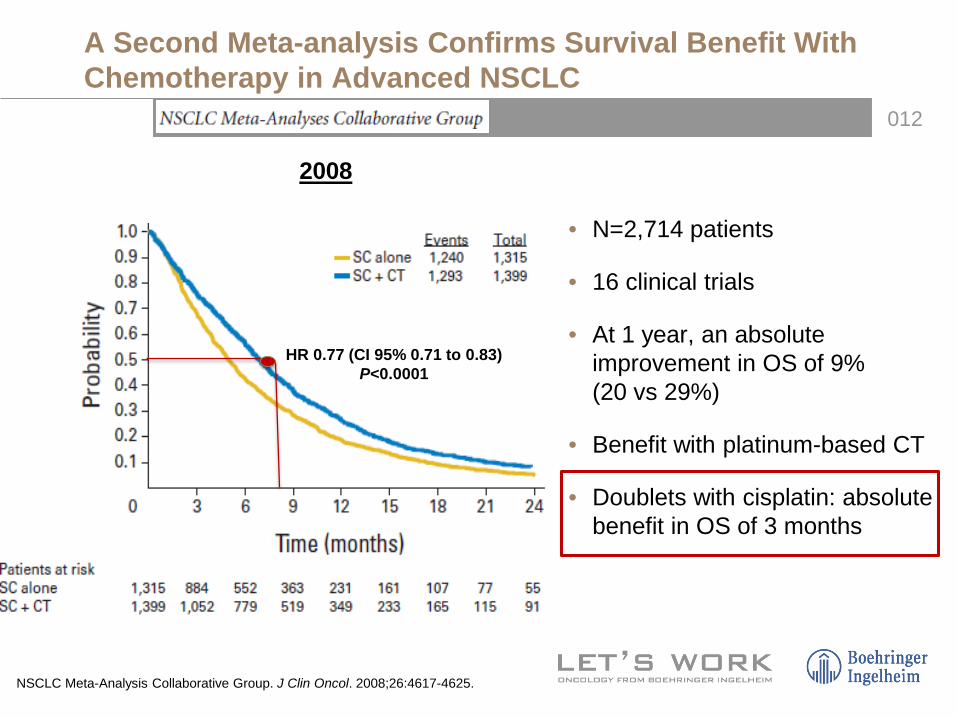
HR 0.77 (CI 95% 0.71 to 0.83)P<0.0001
A Second Meta-analysis Confirms Survival Benefit With Chemotherapy in Advanced NSCLC
2008
NSCLC Meta-Analysis Collaborative Group. J Clin Oncol. 2008;26:4617-4625.
• N=2,714 patients
• 16 clinical trials
• At 1 year, an absoluteimprovement in OS of 9% (20 vs 29%)
• Benefit with platinum-based CT
• Doublets with cisplatin: absolutebenefit in OS of 3 months

013
N = 1,207
ECOG 2002 Trial: Four Different Platinum-based Doublets With Similar OS
Schiller JH, et al. N Engl J Med. 2002;346:92-98.

014
CT OS(m)
1 Year (%)
PC 7.8 31
GC 8.1 36
DC 7.4 31
PCb 8.1 34
CT OS(m)
1 Year (%)
PCb 9.9 43
GC 9.8 37
CV 9.5 37
Pacli + carbo (PCb)Cis + vin (CV)
Ove
rall
surv
ival
%
100
80
60
40
20
00
Months Months
Ove
rall
surv
ival
30
Pacli + cis (PC)Gem + cis (GC)Doc + cis (DC) Pacli + carbo (PCb)
5 10 15 20 25
Pacli + carbo (PCb)Gem + cis (GC) Cis + vin (CV)
Months0
1.0
0.9
0.6
0.5
0.4
0.3
0.8
0.7
0.2
0.10
1.00.9
0.6
0.5
0.4
0.3
0.8
0.7
0.2
0.10
Ove
rall
surv
ival
305 10 15 20 250305 10 15 20 25
Several Combinations With Cisplatin:Reaching a Plateau in Efficacy
Kelly K, et al. J Clin Oncol. 2001;19:3210-3218. Schiller JH, et al. N Engl J Med. 2002;346:92-98. Scagliotti GV, et al. J Clin Oncol. 2002;20:4285-4291.
CT OS (m)
1 Year (%)
PCb 8.6 38
CV 8.1 36

015
Chemotherapy NumberPFS
(months)OS
(months)1-year survival
(%)ORR(%)
CDDP-Vinorelbine 202 4 months 8 months 36% 28
Carbo-Paclitaxel 208 4 months 8 months 38% 26
Paclitaxel-Carboplatin 299 3.1 months 7.8 months 34% 29
CDDP-Gemcitabine 301 4.2 months 8.1 months 36% 26
CDDP-Docetaxel 304 3.7 months 7.4 months 31% 31
CDDP-Paclitaxel 303 3.4 months 8.1 months 31% 29
CDDP-Vinorelbine 404 5.2 months 10.1 months 41% 30
CDDP-Docetaxel 408 5.2 months 11.3 months 46% 32
Carbo-Docetaxel 406 5.0 months 9.4 months 40% 26
CDDP-Vinorelbine 201 4.6 months 9.5 months 37% 29
CDDP-Gemcitabine 205 5.3 months 9.8 months 37% 28
Carboplatin-Paclitaxel 201 5.5 months 9.9 months 43% 31
Efficacy of CT in First Line Treatment of Advanced NSCLC
Kelly K, et al. J Clin Oncol. 2001;19:3210-3218. Schiller JH, et al. N Engl J Med. 2002;346:92-98.Fossella F, et al. J Clin Oncol. 2003;21:3016-3024.Scagliotti G, et al. J Clin Oncol. 2002;20:4285-4291.
≈5 months ≈8-10 months ≈40% ≈30%

016
Review of OS Data With Bevacizumab

017
Sandler A, et al. N Engl J Med. 2006;355:2542-2550.Reck M, et al. J Clin Oncol. 2009;27:1227-1234.Crinò L, et al. Lancet Oncol. 2010;11:733-740.
Bevacizumab in NSCLC

018
2 months OS:12.3 vs 10.3 mo
HR 0.79P=0.003
PFS:6.2 vs 4.5 mo
HR 0.66P<0.001
ECOG 4599: Paclitaxel–Carboplatin Alone or WithBevacizumab for Non–Small-Cell Lung Cancer
Sandler A, et al. N Engl J Med. 2006;355:2542-2550.

019
12.313.5*
14.613.3‡
Med
ian
OS
(mon
ths)
18
12
6
0E45991 AVAiL2 SAiL3 ARIES4
15 mg/kg 7.5/15 mg/kg 7.5 or 15 mg/kg 7.5 or 15 mg/kg
CT + Bevacizumab: Median OS >1 Year
1. Sandler A, et al. N Engl J Med. 2006;355:2542-2550; 2. Reck M, et al. Ann Oncol. 2010;21:1804-1809; 3. Crinò L, et al. Lancet Oncol. 2010;11:733-740; 4. Wozniak AJ, et al. ASCO 2010.

020
3
7
10
12.5
0
2
4
6
8
10
12
14
BSC Monotherapy Doublets withcisplatin
CT + Bevacizumab
Med
ian
OS
(mon
ths)
1975 1990 2000 2006
OS in Advanced NSCLC: Urgent Need for New Treatment Options
NSCLC Cooperative Group, Meta-analysis. J Clin Oncol. 2008;26:4617-4625; Kelly K, et al. J Clin Oncol. 2001;19:3210-3218; Schiller JH, et al. N Engl J Med. 2002;346:92-98; Scagliotti G, et al. J Clin Oncol. 2002;20:4285-4291; Sandler A, et al. N Engl J Med. 2006;355:2542-2550.

021
Histology-based Therapy

022
Non-small-cell Lung Cancers: A Heterogeneous Set of Diseases
Chen Z, et al. Nat Rev Cancer. 2014;14;535-546.

023
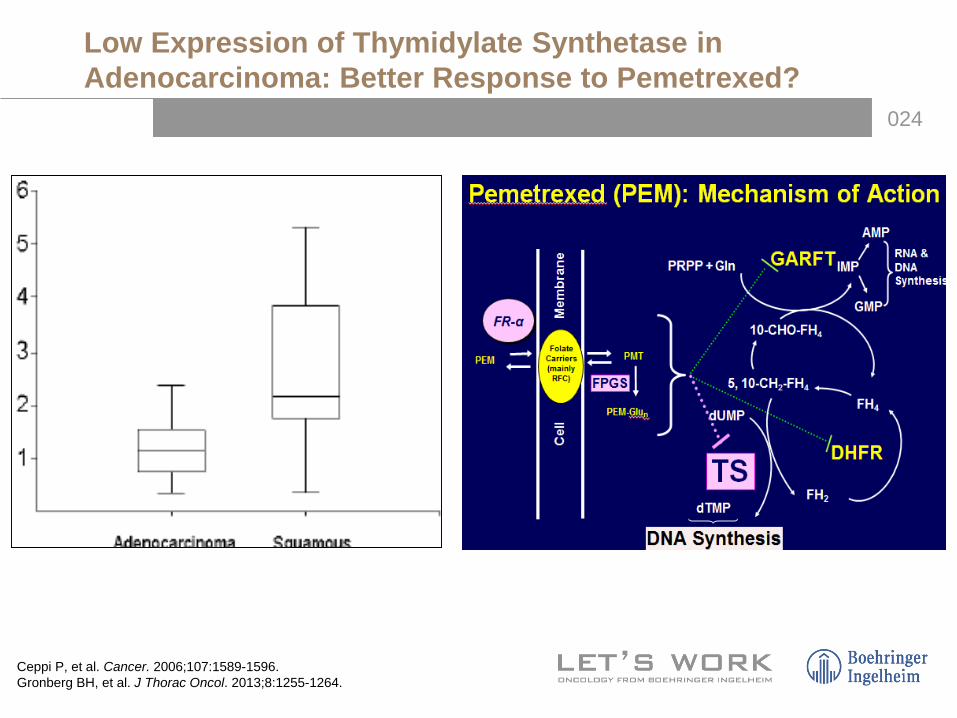
TS
• SCLC – High expression of TS• Squamous (SQ) – High expression of TS• Adeno – Low expression of TS
Thymidylate Synthetase in Lung Cancer
Bhattacharjee A, et al. Proc Natl Acad Sci U S A. 2001;98:13790-13795.
024
Low Expression of Thymidylate Synthetase in Adenocarcinoma: Better Response to Pemetrexed?
Ceppi P, et al. Cancer. 2006;107:1589-1596.Gronberg BH, et al. J Thorac Oncol. 2013;8:1255-1264.

025
Noninferiority study, 1725 patients
Phase III Study Comparing Cisplatin Plus GemcitabineWith Cisplatin Plus Pemetrexed in Chemotherapy-NaivePatients With Advanced-Stage NSCLC
Scagliotti V, et al. J Clin Oncol. 2008;26:3543-3551.

026
OS Squamous(n=172; 130 events)
Adj HR=1.563(95% CI: 1.079-2.264)
P=0.0182DocetaxelMedian = 7.4 months
PemetrexedMedian = 6.2 months
PemetrexedMedian = 9.3 months
DocetaxelMedian = 8.0 months
OS Nonsquamous(n=399; 279 events)
Adj HR=0.778(95% CI: 0.607-0.997)
P=0.0475
JMEI Study: Pemetrexed vs Docetaxel in Second-line (Retrospective Analyisis)
Hanna N, et al. J Clin Oncol. 2004;22:1589-1597.Peterson et al. ECCO. 2007.

027
ECOG 4599: Bevacizumab in Advanced nonsquamos NSCLC (OS)
ECOG 4599: Bevacizumab in Advanced Adenocarcinoma (OS)
Adenocarcinoma:Pemetrexed + Bevacizumab?
Adenocarcinoma: Better Results With Bevacizumab
2.3 months
3.9 months

028
Censoring rate for Pem+Cb+Bev was 27.8%; for Pac+Cb+Bev was 27.2%
1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
00 3 6 9 12 15 18 21 24 27 30 33 36 39
Time (months)
OS
prob
abili
ty
Pem+Cb+Bev
Pac+Cb+Bev
ASCO 2013.
POINTBREAK, a Randomised Phase III Trial: OS Since Induction Therapy (ITT)
Pem+Cb+Bev Pac+Cb+BevMedian OS (months) 12.6 13.4
HR (95% CI)P value
1.00 (0.86–1.16)
P=0.949

029
3
7
10
12.5 11.8
0
2
4
6
8
10
12
14
BSC Monotherapy Doublets withcisplatin
CT +Bevacizumab
CT byhistology
Med
ian
OS
(mon
ths)
1975 1990 2000 20082006
OS in Advanced NSCLC: Urgent Need for New Treatment Options

030
Target Therapy: Personalised Medicine

031
CPCP(≈15%)
Squamous cell(≈25%)
Adenocarcinoma(≈45-50%)
BAV(≈5%)
Large cell(≈5%)
Other (Not specified)
(≈10%)
Molecular Differences in Subtypes of Lung Cancer
Sun S, et al. Nat Rev Cancer. 2007;7:778-790.Lindeman NI. Arch Pathol Lab Med. 2013;137:828.

032
Molecular Alterations in NSCLC
Davidson MR. J Thorac Dis. 2013;5:S463-S478.

033
Adeno CG/CPNE Squamous cell CPCP
EGFR mutation ALK ROS/RET
HER2
BRAF KRAS
KRAS
Treatment According to Therapeutic Targets

034
OS According to Driver Mutations and Type of Treatment
Johnson B, et al. ASCO 2013. Abstract 8019.
Mutation + target therapy (n=313)Mutation without target therapy (n=265)No mutations CT (n=361)
100
80
60
40
20
0
Ove
rall
Surv
ival
(%)
0 1 2 3 4 5
Years

035
Review of OS Data With First-Generation EGFR TKIs

036
EGFR TKIs
Yu HA, et al. Clin Cancer Res. 2014;20:5898-5907.Janne. Mini Symposium MS27, WCLC 2013.
Drug Status FDACovalent-binding
Activity in T790M Structure Generation
Gefitinib Approved No No Quinazoline First
Erlotinib Approved No No Quinazoline First
Dacomitinib Phase III Yes No Quinazoline Second
Afatinib Approved Yes ± Quinazoline Second
AP26113 Phase I/II No ? Pyrimidine Third
CO-1686 Phase I Yes Yes Pyrimidine Third
AZD9291 Phase II Yes Yes Pyrimidine Third

037
IRESSA Registry in
Japan
ISEL
INTEREST
2002 200920072005
ISEL, INTEREST: non selective patients with previous treatment
2003Expression of EGFR protein
EGFR gene copy number
2004 2006 2008
History of Gefitinib
038
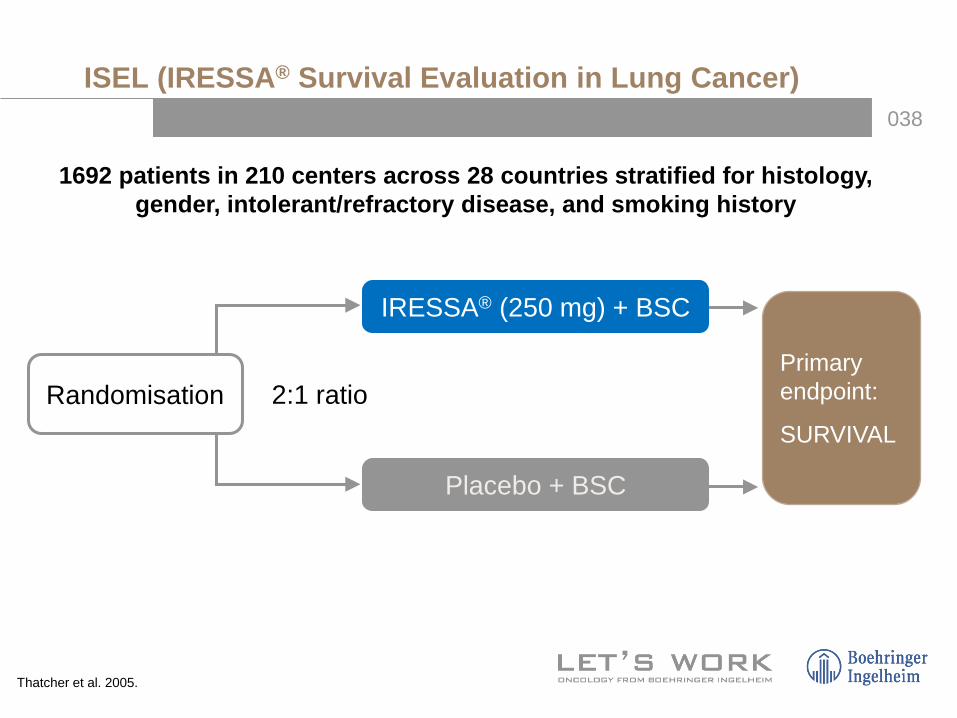
Randomisation
IRESSA® (250 mg) + BSC
Placebo + BSC
Primary endpoint:
SURVIVAL2:1 ratio
1692 patients in 210 centers across 28 countries stratified for histology, gender, intolerant/refractory disease, and smoking history
ISEL (IRESSA® Survival Evaluation in Lung Cancer)
Thatcher et al. 2005.

039
0 1 2 3 4 6 8 9 10 11 12 13 14 1
MonthsAt risk: 1692 1348 876 484 252 103 31
Patie
nts
surv
ivin
g (%
)
—— IRESSA®
------ Placebo
ORR: 7.1% vs 0.5%
ISEL Trial: Overall Population–Survival
Thatcher et al. 2005.
1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
00 2 4 6 8 10

040
PFS in overall population
Hazard ratio and 95% CI
Favours IRESSA® Favours placebo
Survival Response rate
Non-adenocarcinoma 4.6%
Never smoked 17.2%Ever smoked 5.2%
Refractory 7.8%
1 prior chemo 7.4%2 prior chemos 8.0%
PS 0,1 8.3%PS 2,3 6.6%
Male 4.9%
All patients 7.7%0.4 0.6 0.8 1 1.5
Adenocarcinoma 11.4%
Female 14.0%
ISEL Study: Effects in Subsets (1)
Thatcher et al. 2005.
Intolerant 7.2%

041
PFS in overall population
Survival Response ratePrior docetaxel
All patients
Asian ethnicity
Time since Dx: >12 mo
Time since Dx: <6 mo
<65 yrs
No prior docetaxel
≥65 yrs
Time since Dx: 6-12 mo
Non-Asian ethnicity
Hazard ratio and 95% CI
Favours IRESSA® Favours placebo
Prior chemo response: PD/NE
Prior chemo response: CR/PRPrior chemo response: SD
10.3%
7.7%
12.0%
9.3%
6.8%
7.1%
6.7%
8.7%
6.9%
6.5%
7.0%
8.9%8.0%
0.4 0.6 0.8 1 1.5
Effects in Subsets (2)
Thatcher et al. 2005.

042O
S (%
)
0 2 4 6 8 10 12 14 160.0
1.0
0.8
0.6
0.4
0.2
HR 0.67; 95% CI 0.49, 0.92; P=0.012Never smokers (n=375)
GefitinibPlacebo
0 2 4 6 8 10 12 14 16
Ever smokers (n=1317)HR 0.92; 95% CI 0.79, 1.06; P=0.242
1.0
Time (Months)
0.0
0.8
0.6
0.4
0.2
0 2 4 6 8 10 12 14 16
HR 0.66; 95% CI 0.48, 0.91; P=0.010
Cox Regression Analysis
0 2 4 6 8 10 12 14 16
Nonasian Origin (n=1350)HR 0.92; 95% CI 0.80, 1.07; P=0.294
OS
(%)
Asian origin (n=342)
ISEL Study: OS by Smoking History and Ethnic Origin
Thatcher et al. 2005.

043

044
EGFR expression
+n=189
EGFR FISH +n=117
EGFR mutation +n=39
+++ n=24
4
3
n=16
n=73
n=84
n=8
Douillard. 2010.Soulières. ASCO 2011.
ISEL Trial: Overlap of Biomarkers (n=249) EGFR Gene Copy Number (FISH), IHC, or EGFR Mutation?

045
IPASS
IPASS: enrichment population, naive-treatment
Mutations in EGFR
History of Gefitinib
IRESSA Registry in
Japan
ISEL
INTEREST
2002 200920072005
ISEL, INTEREST: non selective patients with previous treatment
2003Expression of EGFR protein
EGFR gene copy number
2004 2006 2008
046
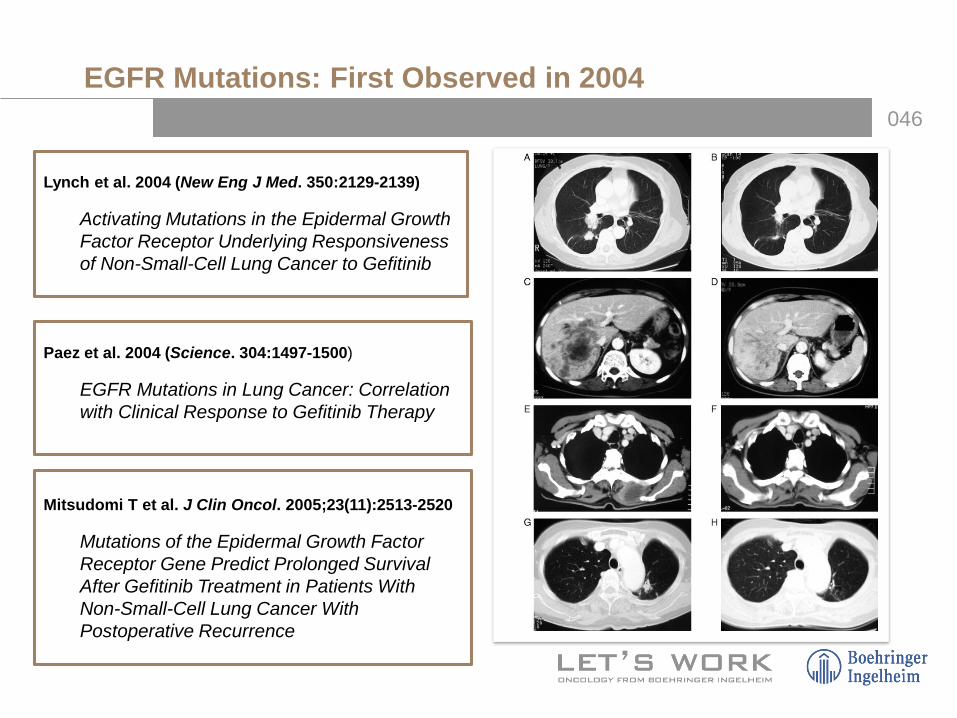
Lynch et al. 2004 (New Eng J Med. 350:2129-2139)
Activating Mutations in the Epidermal Growth Factor Receptor Underlying Responsiveness of Non-Small-Cell Lung Cancer to Gefitinib
Paez et al. 2004 (Science. 304:1497-1500)
EGFR Mutations in Lung Cancer: Correlation with Clinical Response to Gefitinib Therapy
Mitsudomi T et al. J Clin Oncol. 2005;23(11):2513-2520
Mutations of the Epidermal Growth Factor Receptor Gene Predict Prolonged Survival After Gefitinib Treatment in Patients With Non-Small-Cell Lung Cancer With Postoperative Recurrence
EGFR Mutations: First Observed in 2004
047
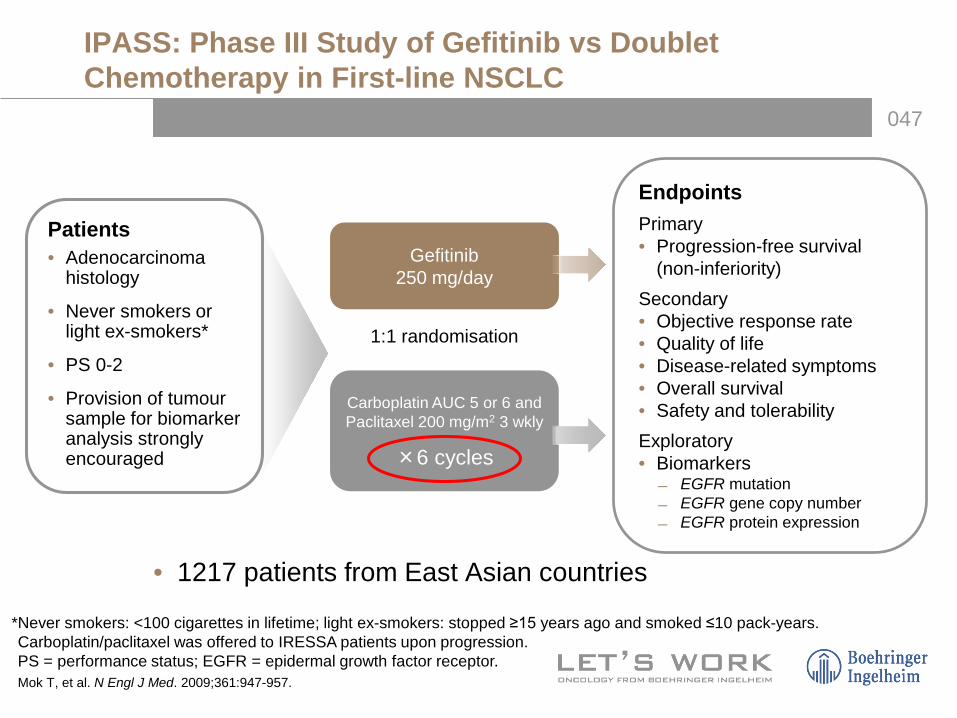
Gefitinib250 mg/day
Carboplatin AUC 5 or 6 and Paclitaxel 200 mg/m2 3 wkly
×6 cycles
1:1 randomisation
Patients• Adenocarcinoma
histology
• Never smokers or light ex-smokers*
• PS 0-2
• Provision of tumour sample for biomarker analysis strongly encouraged
EndpointsPrimary• Progression-free survival
(non-inferiority)Secondary• Objective response rate• Quality of life• Disease-related symptoms• Overall survival• Safety and tolerabilityExploratory• Biomarkers
EGFR mutation EGFR gene copy number EGFR protein expression
*Never smokers: <100 cigarettes in lifetime; light ex-smokers: stopped ≥15 years ago and smoked ≤10 pack-years.Carboplatin/paclitaxel was offered to IRESSA patients upon progression.PS = performance status; EGFR = epidermal growth factor receptor.Mok T, et al. N Engl J Med. 2009;361:947-957.
IPASS: Phase III Study of Gefitinib vs Doublet Chemotherapy in First-line NSCLC
• 1217 patients from East Asian countries

048
IPASS: EGFR Mutation Is a Strong Predictor for Differential PFS Benefit Between Gefitinib and Doublet Chemotherapy (L858R, Del exon 19)
Mok T, et al. N Engl J Med. 2009;361:947-957.
EGFR M+HR=0.48, 95% CI 0.36, 0.64 P<0.0001EGFR M-HR=2.85, 95% CI 2.05, 3.98 P<0.0001Treatment by subgroup interaction test, P<0.0001
0 4 8 12 16 20 24
Time from randomisation (months)
0.0
0.2
0.4
0.6
0.8
1.0
Prob
abili
ty o
f PFS
Gefitinib EGFR M+ (n=132)Gefitinib EGFR M- (n=91)Carboplatin/paclitaxel EGFR M+ (n=129)Carboplatin/paclitaxel EGFR M- (n=85)3.4 months

049
Treatment by subgroup interaction test P value
P=0.0437 for EGFRgene copy number
P=0.2135 for EGFRexpression
P<0.0001 for EGFRmutation
Favours gefitinib Favours carboplatin/paclitaxel
Known mutation status
EGFR Mutation+
EGFR Mutation-
Known expression status
EGFR +
EGFR -
Known FISH status
EGFR FISH+
EGFR FISH-
0.25 0.5 1.0 2.0 4.0Hazard Ratio (Gefitinib: Carboplatin/Paclitaxel) and 95% CI
IPASS: PFS by Biomarkers (ITT)
Fukuoka M, et al. J Clin Oncol. 2011;29:2866-2871.
050
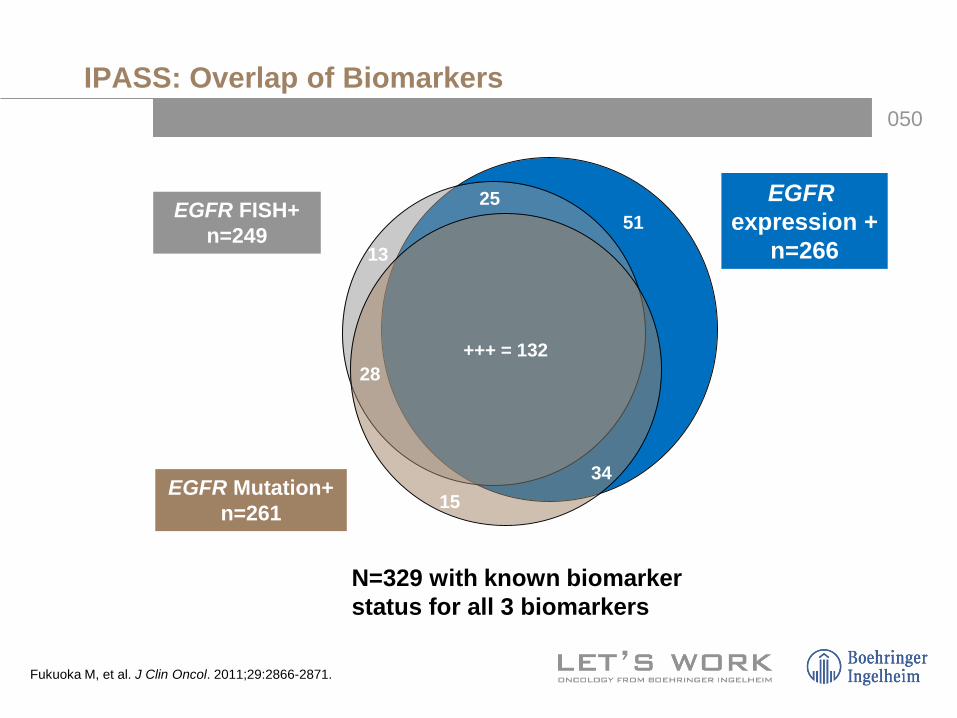
N=329 with known biomarker status for all 3 biomarkers
EGFR Mutation+ n=261
EGFR FISH+ n=249
+++ = 132
2551
13
28
1534
EGFRexpression +
n=266
IPASS: Overlap of Biomarkers
Fukuoka M, et al. J Clin Oncol. 2011;29:2866-2871.

051
Higher RR with CT in EGFR mutated vs EGFR WT 4 or 6 cycles of CT?
IPASS: ORR
Mok T, et al. N Engl J Med. 2009;361:947-957.
EGFR+ EGFR- PORR with CT 47.3% 23.5% <0.001ORR with TKI 71.2% 1.1% <0.00001

052
Seven prospective trials; NSCLC patients with EGFR mutations
RRs were 76% vs 24.6% (P<0.001)4.7 months
Combined Survival Analysis of Prospective Clinical Trials of Gefitinib for NSCLC EGFR+
Satoshi M, et al. Clin Cancer Res. 2009;15:4493-4498.
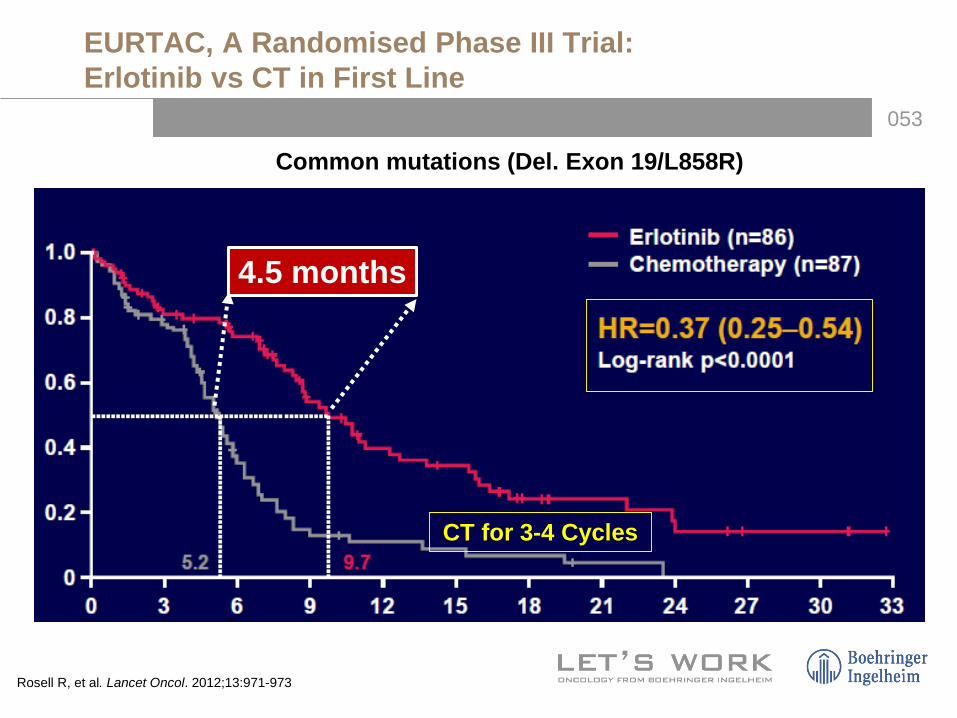
053
Common mutations (Del. Exon 19/L858R)
4.5 months
CT for 3-4 Cycles
EURTAC, A Randomised Phase III Trial: Erlotinib vs CT in First Line
Rosell R, et al. Lancet Oncol. 2012;13:971-973

054
8.5 months
An open-label, randomised, phase 3 trial at 22 centres in China (N=154)CT × 4 cycles
Erlotinib vs CT as First-line Treatment for Patients With Advanced EGFR+ NSCLC (OPTIMAL, CTONG-0802)
Zhou C, et al. Lancet Oncol. 2011;12:735-742.

055
×6
×4
Summary of Phase III Trials of First-Generation TKI vs CT in First-line in Advanced NSCLC EGFR+
×6
×6
×4
×4

056
Day 0 Day 14Advantages:
1. High Response Rate1:*60-80% vs 20-30%
2. Rapid Responses2: *2 Ws vs 6 Ws.
3. Quality of Life3:*<adverse events
4. > PFS4: *10-13 vs 5-6 months
5. < progression to CNS5
TKI vs CT in First-line (NSCLC EGFR+)
1. Jancarikova D, et al. Anticancer Res. 2007;27:1879-1882; 2. Mok TS, et al. N Engl J Med. 2009;361:947-957; 3. Maemondo M, et al. N Engl J Med. 2010;362:2380-2388; 5. Rosell R, et al. Lancet Oncol. 2012;13:239-246.

057
PFS
How do they compare?
GefitinibClinical Trial A vs C9.5 Months
(4 C of CT 6.3) 3.2 monthsQT
ErlotinibClinical Trial B vs C9.7 Months
(4 C of CT 5.2) 4.5 monthsQT
AfatinibClinical Trial D vs C13.6 Months
(6 C of CT 6.9) 6.7 monthsQT
Gefitinib Erlotinib
QT QT
Indirect comparison: A vs B; A vs D and B vs D
Afatinib
QT
058
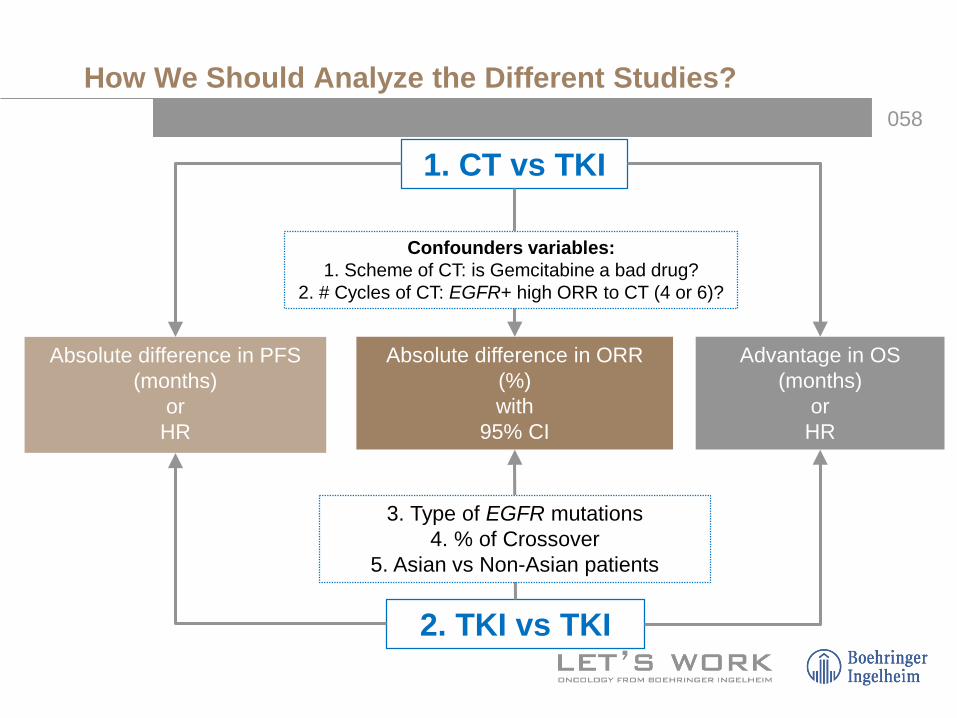
Absolute difference in PFS(months)
orHR
Absolute difference in ORR(%)with
95% CI
Advantage in OS(months)
orHR
1. CT vs TKI
2. TKI vs TKI
Confounders variables: 1. Scheme of CT: is Gemcitabine a bad drug?
2. # Cycles of CT: EGFR+ high ORR to CT (4 or 6)?
3. Type of EGFR mutations4. % of Crossover
5. Asian vs Non-Asian patients
How We Should Analyze the Different Studies?
059
Review of OS for Afatinib(2nd-Generation TKI): OS Analysis of LUX-Lung 3 and 6

060
PFS
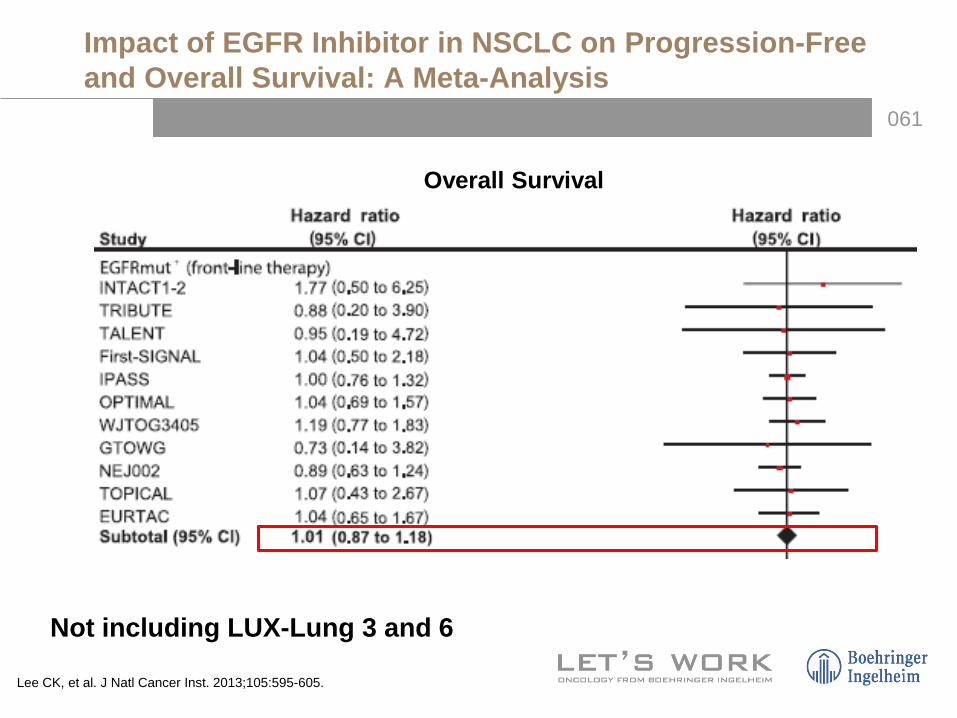
Impact of EGFR Inhibitor in NSCLC on Progression-Free and Overall Survival: A Meta-Analysis
Lee CK, et al. J Natl Cancer Inst. 2013;105:595-605.
061
Overall Survival
Not including LUX-Lung 3 and 6
Impact of EGFR Inhibitor in NSCLC on Progression-Free and Overall Survival: A Meta-Analysis
Lee CK, et al. J Natl Cancer Inst. 2013;105:595-605.
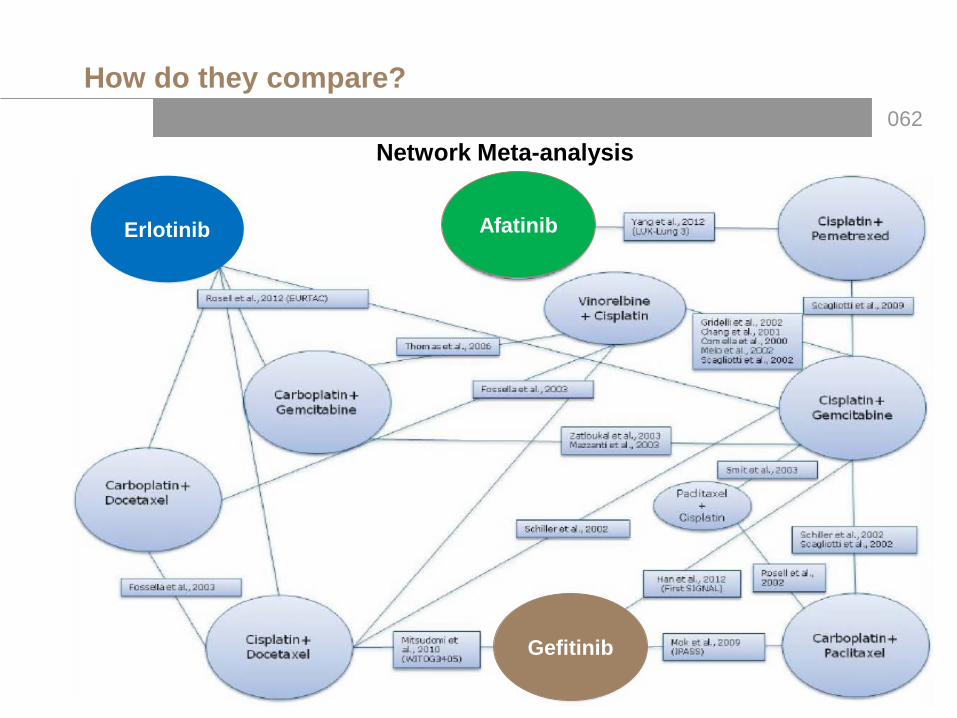
062Network Meta-analysis
AfatinibErlotinib
Gefitinib
How do they compare?

063
Including Seven eligible trials (1,649 patients)
Treatment with EGFR TKI compared with CT was associated with a 63%reduction in the risk of progressive disease (HR 0.37, 95% CI 0.32 to 0.42, P<0.001)
Impact of Specific EGFR Mutations and Clinical Characteristics on Outcomes After Treatment With TKIs vs Chemotherapy in EGFR-Mutant Lung Cancer: A Meta-Analysis
Lee CK, et al. J Clin Oncol. 2015;33:1958-1965.

Lee CK, et al. J Clin Oncol. 2015;33:1958-1965.

065
OS With TKIS vs CT in Common Mutations:A Meta-analysis
• Multiple phase 3 trials with first-generation TKIs have evaluated OS: – None showed an OS benefit (neither in ITT or in EGFR mutational subgroup
analysis)
Lee CK, et al. J Clin Oncol. 2015;33:1958-1965.

066
Advanced NSCLC EGFR+
Treatment A
Treatment B
EVENT
Classic Randomised Clinical Trial
EVENT
Treatment A
Treatment B
PD
Treatment B
Treatment AAdvanced NSCLC
EGFR+
Crossover Randomised Clinical Trial
PD
No Benefit in OS With TKIs: Really?

067
Afatinib: Structure and Binding
Li D, et al. Oncogene. 2008;27:4702-4711. Solca F, et al. J Pharmacol Exp Ther. 2012;343:342-350.
ErbB3 does not have a kinase domain and cannot be directly blocked by afatinib

068
ErbB3 does not have a kinase domain and cannot be directly blocked by afatinib
Li D, et al. Oncogene. 2008;27:4702-4711; Solca F, et al. J Pharmacol Exp Ther. 2012;343:342-350; Yang JC, et al. Lancet Oncol. 2012;13:539-548.
Afatinib: An Irreversible ErbB Family Blocker

069
Afatinib: Preclinica Data
Li D, et al. Oncogene. 2008;27:4702-4711.Solca F, et al. J Pharmacol Exp Ther. 2012;343:342-350.
*ErbB3 does not have a kinase domain and cannot be directly blocked by afatinib
*

070
AFATINIB: Good Activity in Resistant Cells to Gefitinib and Erlotinib
1. Li D, et al. Oncogene. 2008;27:4702-4711.2. Solca F, et al. Proceedings, AACR-NCI-EORTC International Conference on MolecularTargets and Cancer Therapeutics. 2005;118:Abstract A242.
Mutation WT Sensitivity Resistance
Wild-typeH1666
L858RH3255
L858R+T790MNCI1975
Target Type of Interaction
Afatinib1 60 0.7 99 EGFR/HER2 Irreversible
Gefitinib1 157 5 >4000 EGFR Reversible
Erlotinib1 110 40 >4000 EGFR Reversible
Lapatinib1 534 63 >4000 EGFR/HER2 Reversible
CP 714,7242 >4000 561 >4000 HER2 Reversible
EC50 values for the inhibitory activities of different compounds on the proliferation of NSCLC cells with EGFR mutations

071
LUX-Lung 3 and 6: Study Rationale
• EGFR+ Lung cancer: subgroup with sensivity to TKI, including PFS benefit compared with first-line CT in randomised trials1-5
• Afatinib demonstrated efficacy in lung adenocarcinoma patients with EGFR+ (LUX-Lung 2)6:
– ORR: 66%, median PFS 12 months (first-line; independent review)– Median PFS: 13.7 months among Del19/L858R (independent review)
• Cisplatin/pemetrexed is a highly effective and well-tolerated first-line CT to advanced lung adenocarcinoma,7 but it has not been compared with TKI in EGFR mutation-positive patients
• Cisplatin/gemcitabine is the approved standard CT in China8

072
Afatinib 40 mg/db
Cisplatin + Pemetrexed75 mg/m2 + 500 mg/m2
IV q21d, up to 6 cycles
Stage IIIB/IV Lung adenocarcinoma with EGFR mutation(central lab testing; TheraScreen® EGFR29a RGQ PCR)
Cisplatin + Gemcitabine75 mg/m2 + 1000 mg/m2 D1, D8
IV q21d, up to 6 Cycles
Randomised 2:1 Stratification: type of mutation (Del19/L858R/otros)
Primary Objective: PFS (RECIST 1.1, independent review)c
Secondary Objectives: OS, PROd, ORR, DCR, DOR, tumour shrinkage, securityaEGFR29: 19 deletions in exon 19, 3 insertions in exon 20, L858R, L861Q, T790M, G719S, G719A and G719C (or G719X), S768I.bDose escalated to 50 mg if limited AE observed in cycle 1. Dose reduced by 10-mg decrements in case of related G3 or prolonged G2 AE.cTumour assessments: q6 weeks until week 48 and q12 weeks thereafter until progression/start of new therapy. dPatient-reported outcomes: EQ-5D, EORTC QLQ-C30 and LC 13 at randomisation and q3 weeks until progression or new anticancer therapy. Note: 24 patients in LUX-Lung 3 and 28 patients in LUX-Lung 6 were still on treatment as of December 2013.RGQ = rotor-gene Q; PCR = polymerase chain reaction; PFS = progression-free survival; RECIST = Response Evaluation Criteria in Solid Tumours; ORR = objective response rate; DCR = disease control rate; DOR = duration of response; OS = overall survival.1. Sequist LV, et al. J Clin Oncol. 2013;31:3327-3334; 2. Wu YL, et al. Lancet Oncol. 2014;15:213-222.
LUX-Lung 62(n=364; Asians pts)
LUX-Lung 3 and 6
LUX-Lung 31(n=345; Asians & Caucasian pts)

073
LUX-Lung 3 and 6: Patient Demographics and Clinical Characteristics
1. Sequist LV, et al. J Clin Oncol. 2013;31:3327-3334.2. Wu YL, et al. Lancet Oncol. 2014;15:213-222.

074
Meta-analyisis: Demographic Characteristics
Lee CK, et al. J Clin Oncol. 2015;33:1958-1965.

075
6.7 months
LUX-Lung 3: Progression-Free Survival(Common Mutations: L858R, Del Exon 19)
Sequist LV, et al. J Clin Oncol. 2013;31:3327-3334.

076
47%
22%
54%
2%
LUX-Lung 3 and LUX-Lung 6: Primary End Point PFS in Patients With Common Mutations by Independent Review
Sequist LV, et al. J Clin Oncol. 2013;31:3327-3334.Wu YL, et al. Lancet Oncol. 2014;15:213-222.
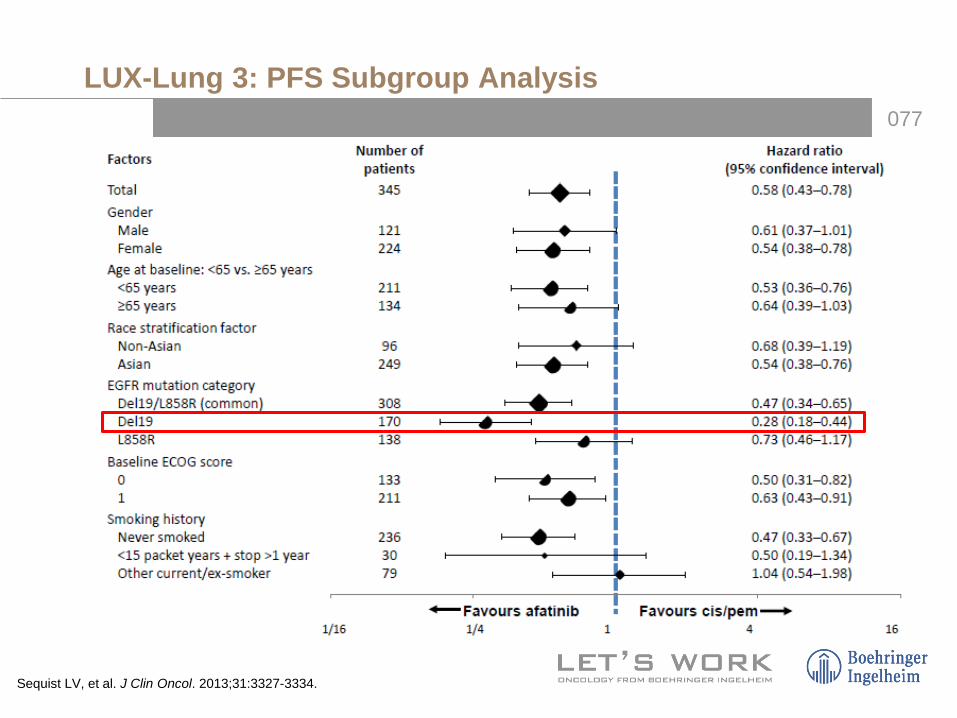
077
LUX-Lung 3: PFS Subgroup Analysis
Sequist LV, et al. J Clin Oncol. 2013;31:3327-3334.
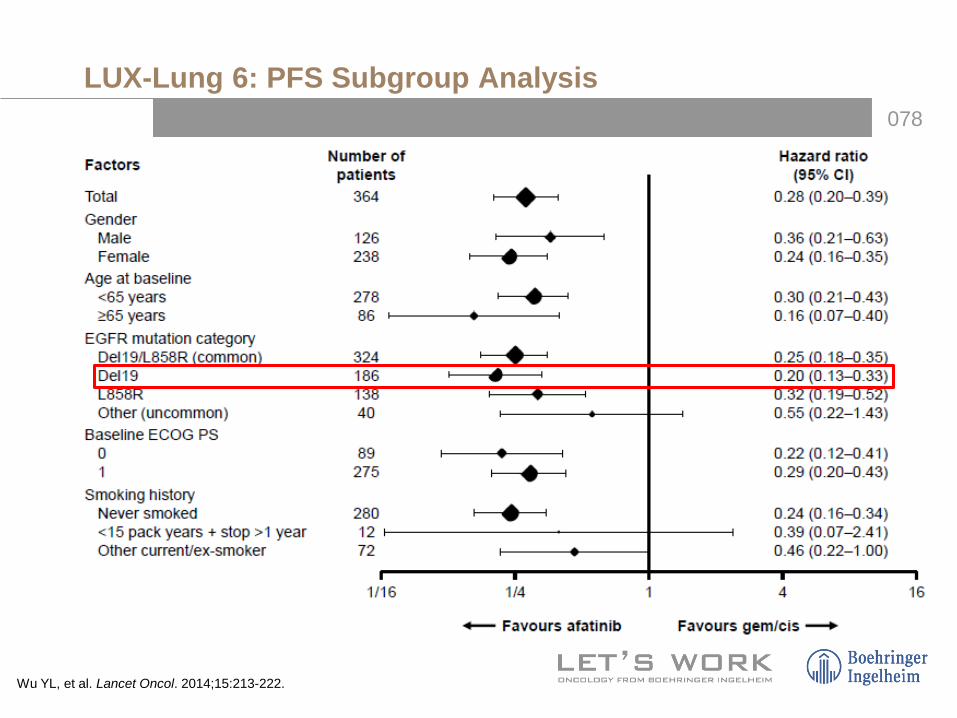
078
LUX-Lung 6: PFS Subgroup Analysis
Wu YL, et al. Lancet Oncol. 2014;15:213-222.
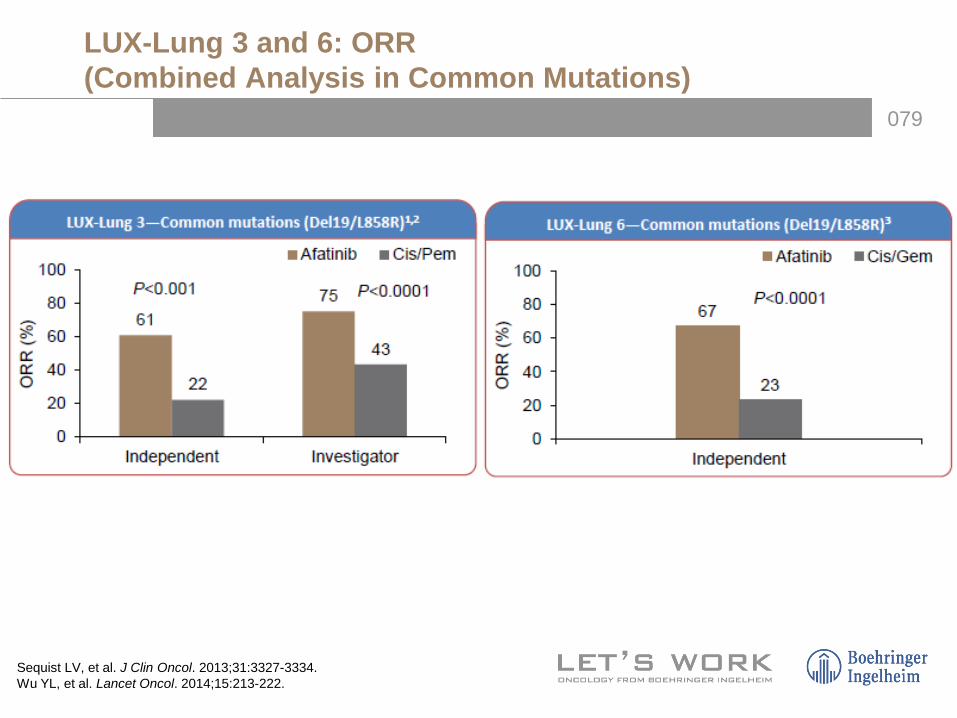
079
LUX-Lung 3 and 6: ORR(Combined Analysis in Common Mutations)
Sequist LV, et al. J Clin Oncol. 2013;31:3327-3334.Wu YL, et al. Lancet Oncol. 2014;15:213-222.

080
LUX-Lung 3 and 6: Most Frequent AEs
Sequist LV, et al. J Clin Oncol. 2013;31:3327-3334.Wu YL, et al. Lancet Oncol. 2014;15:213-222.

081
LUX-Lung 3 and 6: Summary of AEs
Sequist LV, et al. J Clin Oncol. 2013;31:3327-3334.Wu YL, et al. Lancet Oncol. 2014;15:213-222.

082
LUX-Lung 3: Quality of Life
Sequist LV, et al. J Clin Oncol. 2013;31:3327-3334.

083
LUX-Lung 3 and 6: OS in Common Mutations
• Multiple phase 3 trials with first-generation TKIs have evaluated OS: – None showed an OS benefit (neither in ITT or in EGFR
mutational subgroup analysis)
Lee CK, et al. J Clin Oncol. 2015;33:1958-1965.

084
LUX-Lung 3: Overall Survival
Yang JC, et al. Lancet Oncol. 2015;16:141-151.

085
-100
-80
-60
-40
-20
0
20
40
60
80
100
120
Cam
bio
máx
imo
vs b
asal
(%) Exon 20 insertions (n=20)
T790M de novo (n=14):T790M alone, T790M+Del19, T790M+L858R, T790M+G719X, T790M+L858R+G719X
Others (n=33):L861Q, G719X, G719X+S768I, G719X+L861Q, E709G or V+L858R, S768I+L858R, S768I, L861P, R776H+L858R, L861Q+Del19, K739_1744dup6
T790M Exon 20 insertions
Others
ORR (%) 14.3 8.7 71.1
RCD (%) 64.2 65.2 84.2
PFS (months) 2.9 2.7 10.7
OS (months) 14.9 9.4 18.6
120 -
100 -
80 -
60 -
40 -
20 -
0 -
–20 -
–40 -
–60 -
–80 -
–100 -
Uncommon Mutations: Heterogeneous SubgroupM
axim
um C
hang
e vs
Bas
elin
e (%
)
086
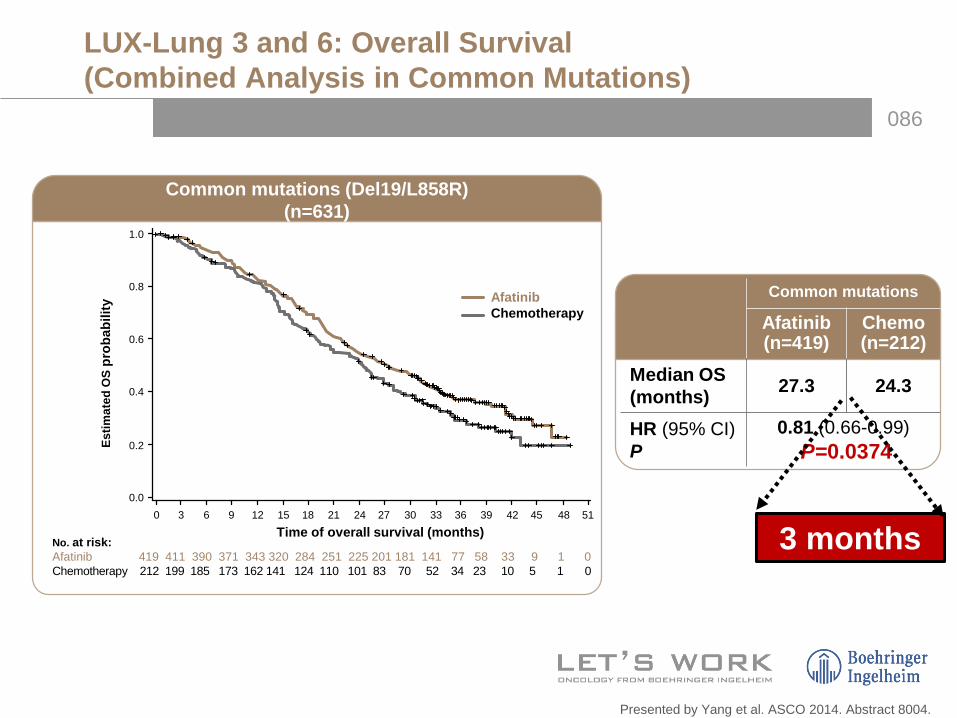
Common mutations
Afatinib (n=419)
Chemo(n=212)
Median OS (months) 27.3 24.3
HR (95% CI) P
0.81 (0.66-0.99)P=0.0374
Common mutations (Del19/L858R) (n=631)
Time of overall survival (months)
Estim
ated
OS
prob
abili
ty
0.0
0.2
0.4
0.6
0.8
1.0
0 3 6 9 12 15 18 21 24 27 30 33 36 39 42 45 48 51
No. at risk:Afatinib 419 411 390 371 343 320 284 251 225 201 181 141 77 58 33 9 1 0Chemotherapy 212 199 185 173 162 141 124 110 101 83 70 52 34 23 10 5 1 0
AfatinibChemotherapy
Presented by Yang et al. ASCO 2014. Abstract 8004.
3 months
LUX-Lung 3 and 6: Overall Survival(Combined Analysis in Common Mutations)

087
LUX-Lung 3
1.0
0.8
0.6
0.4
0.2
0
Estim
ated
OS
prob
abili
ty
0 3 6 9 12 15 18 21 24 27 30 33 36 39 42 45 48 51
Time (months)
203 197 188 181 171 162 143 133 121 108 101 90 58 49 32 9 1 0
104 98 92 86 81 71 63 55 52 47 40 35 26 20 10 5 1 0
Afatinib
Cis/Pem
No of patients
1.0
0.8
0.6
0.4
0.2
0Es
timat
ed O
S pr
obab
ility
0 3 6 9 12 15 18 21 24 27 30 33 36 39 42 45
Time (months)
216 214 202 190 172 158 141 118 104 93 80 51 19 9 1 0
108 101 93 87 81 70 61 55 49 36 30 17 8 3 0 0
Afatinib
Cis/Gem
No of patients
Presented by Yang et al. ASCO 2014. Abstract 8004.
PFS in overall population
Afatinib (n=203)
Cis/Pem(n=104)
Median, months 31.6 28.2HR (95% CI),
P value0.78 (0.58-1.06),
P=0.1090
PFS in overall population
Afatinib (n=216)
Cis/Gem (n=108)
Median, months 23.6 23.5HR (95% CI),
P value0.83 (0.62-1.09),
P=0.1756
LUX-Lung 6
AfatinibCis/Gem
AfatinibCis/Pem
LUX-Lung 3 and 6: Common Mutations
3 months

088
Yang et al. ASCO 2014. Abstract 8004.1. Sequist et al. J Clin Oncol. 2013;31:3327; 2. Wu et al. Lancet Oncol. 2014;15:213; 3. Mok et al. N Engl J Med. 2009;361:947; 4. Fukuoka et al. J Clin Oncol. 2011;29:2866; 5. Yang et al. Eur J Cancer. 2011;(suppl 1):S633; 6. Maemondo et al. N Engl J Med. 2010;362:2380; 7. Inoue et al. Ann Oncol. 2013;24:54; 8. Mitsudomi et al. Lancet Oncol. 2010;11:121; 9. Rosell et al. Lancet Oncol. 2012;13:239; 10. TARCEVA® (erlotinib) prescribing information, 2013; 11. Zhou et al. Lancet Oncol. 2011;12:735; 12. Wu et al. J Thorac Oncol. 2013;8(suppl 2):P1.11-021.
Study PFSHR (95% CI)
LUX-Lung 31
Del19 0.28 (0.18–0.44)L858R 0.73 (0.46–1.17)
LUX-Lung 62
Del19 0.20 (0.13–0.33)L858R 0.32 (0.19–0.52)
IPASS3–5
Del19 0.38 (0.26–0.56)L858R 0.55 (0.35–0.87)
NEJ0026,7
Del19 0.35 (0.23–0.52)L858R 0.32 (0.20–0.50)
WJTOG34058
Del19 0.45 (0.27–0.77)L858R 0.51 (0.29–0.90)
EURTAC9,10
Del19 0.30 (0.18–0.50)L858R 0.55 (0.29–1.02)
OPTIMAL11
Del19 0.13 (0.07–0.25)L858R 0.26 (0.14–0.49)
ENSURE12
Del19 0.20 (0.12–0.33)L858R 0.54 (0.32–0.90)
Favorece QuimioterapiaFavorece TKIFavorece QuimioterapiaFavorece TKI10.50 1.5 0 1 2 3
OSHR (95% CI)
0.54 (0.36–0.79)1.30 (0.80–2.11)
0.64 (0.44–0.94)1.22 (0.81–1.83)
0.79 (0.54–1.15)1.44 (0.90–2.30)
0.83 (0.52–1.34)0.82 (0.49–1.38)
NANA
0.94 (0.57–1.54)0.99 (0.56–1.76)
NANA
NANA
HRs for PFS and OS in Patients With Del19 and L858R
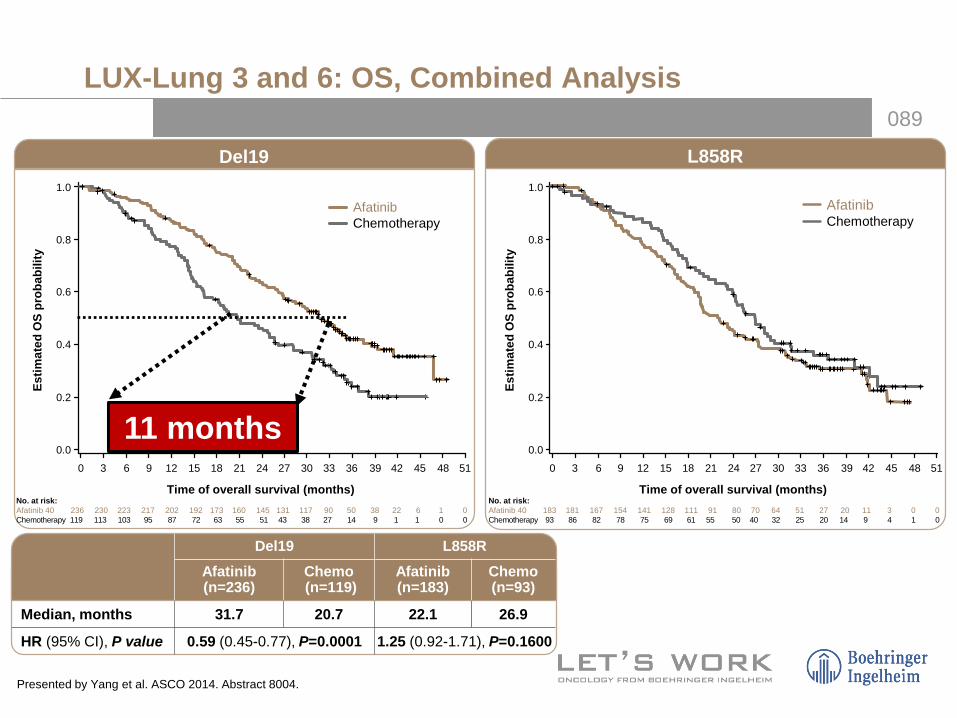
089
L858RDel19
No. at risk:Afatinib 40 236 230 223 217 202 192 173 160 145 131 117 90 50 38 22 6 1 0Chemotherapy 119 113 103 95 87 72 63 55 51 43 38 27 14 9 1 1 0 0
0 6 9 12 15 18 21 24 27
0.4
0.6
0.8
1.0
Time of overall survival (months)
Estim
ated
OS
prob
abili
ty
0.0
3 30 33 36 39 42 45 48 51
0.2
0.4
0.6
0.8
1.0
Estim
ated
OS
prob
abili
ty
0.0
0 6 9 12 15 18 21 24 273 30 33 36 39 42 45 48 51
0.2
No. at risk:Afatinib 40 183 181 167 154 141 128 111 91 80 70 64 51 27 20 11 3 0 0Chemotherapy 93 86 82 78 75 69 61 55 50 40 32 25 20 14 9 4 1 0
Time of overall survival (months)
AfatinibChemotherapy
AfatinibChemotherapy
Del19 L858RAfatinib (n=236)
Chemo(n=119)
Afatinib (n=183)
Chemo (n=93)
Median, months 31.7 20.7 22.1 26.9
HR (95% CI), P value 0.59 (0.45-0.77), P=0.0001 1.25 (0.92-1.71), P=0.1600
11 months
LUX-Lung 3 and 6: OS, Combined Analysis
Presented by Yang et al. ASCO 2014. Abstract 8004.

090
LUX-Lung 6LUX-Lung 3
112 108 105 102 96 93 83 80 72 62 58 51 34 30 21 6 1 0
57 55 50 46 43 37 33 27 25 22 20 16 10 6 1 1 0 0
Afatinib
Cis/Pem
No of patients:124 122 118 115 106 99 90 80 73 69 59 39 16 8 1 0
62 58 53 49 44 35 30 28 26 21 18 11 4 3 0 0
1.0
0.8
0.6
0.4
0.2
0
Estim
ated
OS
prob
abili
ty
0 3 6 9 12 15 18 21 24 27 30 33 36 39 42 45 48 51
Time (months)
1.0
0.8
0.6
0.4
0.2
0Es
timat
ed O
S pr
obab
ility
0 3 6 9 12 15 18 21 24 27 30 33 36 39 42 45
Time (months)
Afatinib
Cis/Gem
No of patients:
PFS in overall population
Afatinib (n=112)
Cis/Pem (n=57)
Median, months 33.3 21.1
HR (95% CI) P value
0.54 (0.36–0.79)P=0.0015
AfatinibCis/Pem
AfatinibCis/Gem
OS: Subgroup Del Exon 19
12.2 months 13 months
Presented by Yang et al. ASCO 2014. Abstract 8004.
PFS in overall population
Afatinib (n=124)
Cis/Gem (n=62)
Median, months 31.4 18.4
HR (95% CI) P value
0.64 (0.44–0.94)P=0.0229

091
Afatinib
Chemotherapy
PD
Chemotherapy
TKIAdvanced Lung
Adenoca EGFR+
LUX-Lung 3 Study
71%
75%
Afatinib
Chemotherapy
PD
Chemotherapy
TKI
LUX-Lung 6 Study
58.8%
56.5%Advanced LungAdenoca EGFR+
LUX-Lung 3 and 6: Crossover (%)
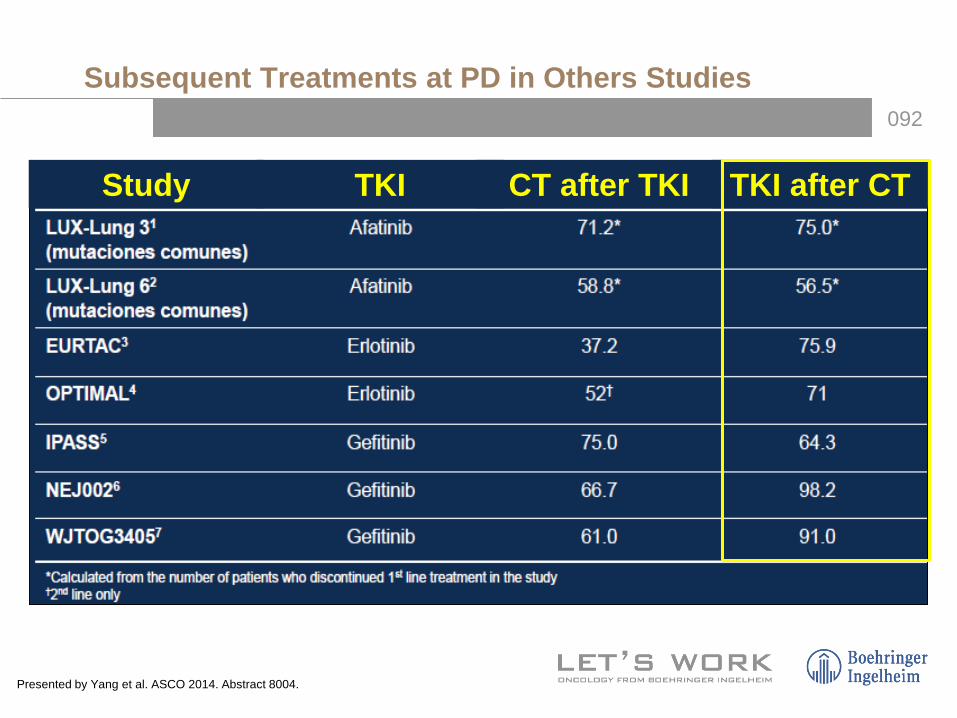
092
Study TKI CT after TKI TKI after CT
Subsequent Treatments at PD in Others Studies
Presented by Yang et al. ASCO 2014. Abstract 8004.

093
LUX-Lung 3 LUX-Lung 6Afatinib(n=203)
Cis/Pem(n=104)
Afatinib(n=216)
Cis/Gem(n=108)
Discontinued treatment, n (%) 184 (100) 104 (100) 194 (100) 108 (100)
Subsequent systemic therapy, n (%)a 144 (78) 88 (85) 123 (63) 70 (65)
Chemotherapy, n (%) 131 (71) 49 (47) 114 (59) 29 (27)
EGFR TKI, n (%)
Erlotinib Gefitinib Afatinib AZD9291DacomitinibIcotinibEGFR TKI combinations
81 (44)
61 (33)28 (15)
2 (1)2 (1)
––
5 (3)
78 (75)
46 (42)44 (42)
7 (7)1 (1)1 (1)
–9 (9)
50 (26)
21 (11)19 (10)
–––
11 (6)5 (3)
61 (56)
22 (20)39 (36)
–––
3 (3)3 (3)
Other systemic therapyb, n (%) 5 (3) 2 (2) 3 (2) 4 (4)
Radiotherapy, n (%) 32 (17) 21 (20) 4 (2) 0 (0)aCollection of data on subsequent therapies still ongoing. bIncludes investigational agents, monoclonal antibodies, non-EGFR targeting protein kinase inhibitors etc.
LUX-Lung 3 and 6: Subsequent Treatments at PD
Presented by Yang et al. ASCO 2014. Abstract 8004.

094
OS in Patients With Del 19 Mutations in Countries With Reimbursement Policies
Presented by Yang et al. ASCO 2014. Abstract 8004.

095
Exon19
Afatinib: Mechanism of Action
Bronte G, et al. Crit Rev Oncol/Hematol. 2014;89:300-313.

096
Cys773 and Cys 805
Erlo/Gefitinib/AfatinibY1173 and Y1068
Afatinib, a Different Drug: Action Mechanism
Nelson V, et al. Onco Targets Ther. 2013;6:135-143.Solca F, et al. J Pharmacol Exp Ther. 2012. 343:342-350.

097
Sensitivity and Kinase Activity of Epidermal Growth Factor Receptor (EGFR) Exon 19 and Others to EGFR Tyrosine Kinase Inhibitors
Furuyama K, et al. Cancer Sci. 2013;104:584-589.

098
Primary objective: OSSub-analysis: Type of EGFR mutation
LUX-Lung 7

099
Future of OS in NSCLC With EGFR Mutations
0100
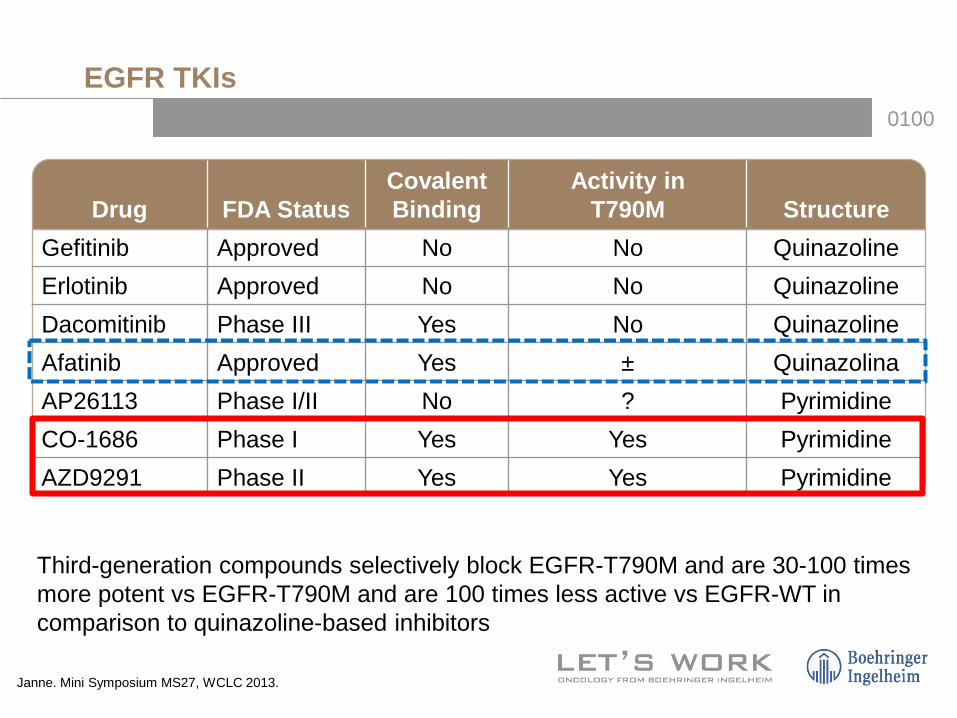
Drug FDA StatusCovalent Binding
Activity in T790M Structure
Gefitinib Approved No No QuinazolineErlotinib Approved No No QuinazolineDacomitinib Phase III Yes No QuinazolineAfatinib Approved Yes ± QuinazolinaAP26113 Phase I/II No ? PyrimidineCO-1686 Phase I Yes Yes PyrimidineAZD9291 Phase II Yes Yes Pyrimidine
Janne. Mini Symposium MS27, WCLC 2013.
Third-generation compounds selectively block EGFR-T790M and are 30-100 times more potent vs EGFR-T790M and are 100 times less active vs EGFR-WT in comparison to quinazoline-based inhibitors
EGFR TKIs
0101
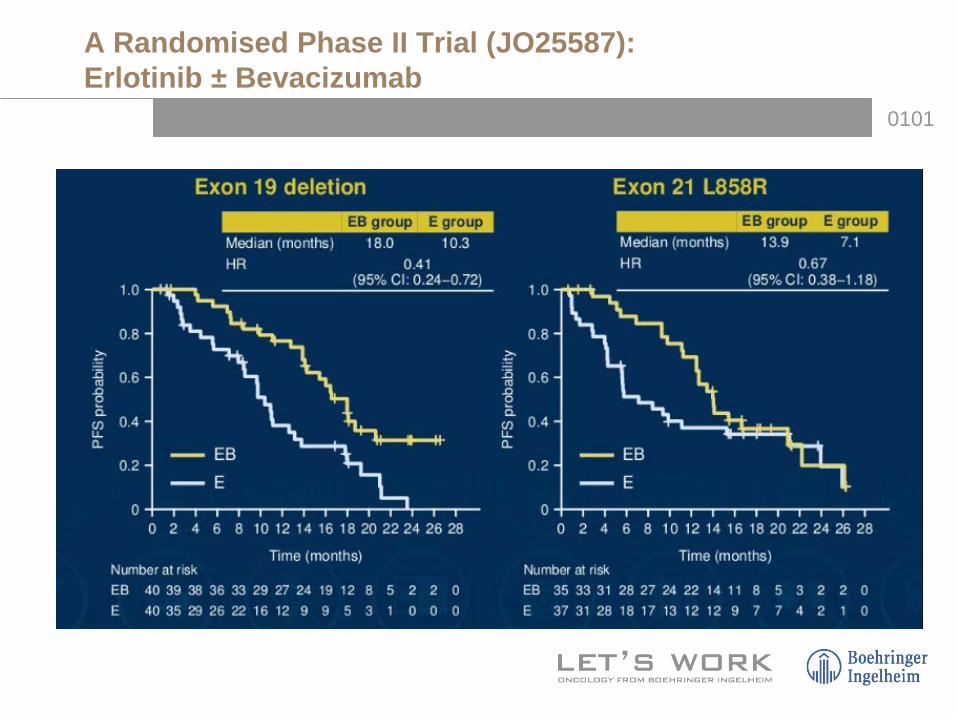
A Randomised Phase II Trial (JO25587): Erlotinib ± Bevacizumab

0102
AZD 9291 (AURA Study)

0103
AZD 9291
0104

0105
Rociletinib After Gefitinib or Erlotinib: Best ORR (All Doses) in 243 Patients T790M+
0106
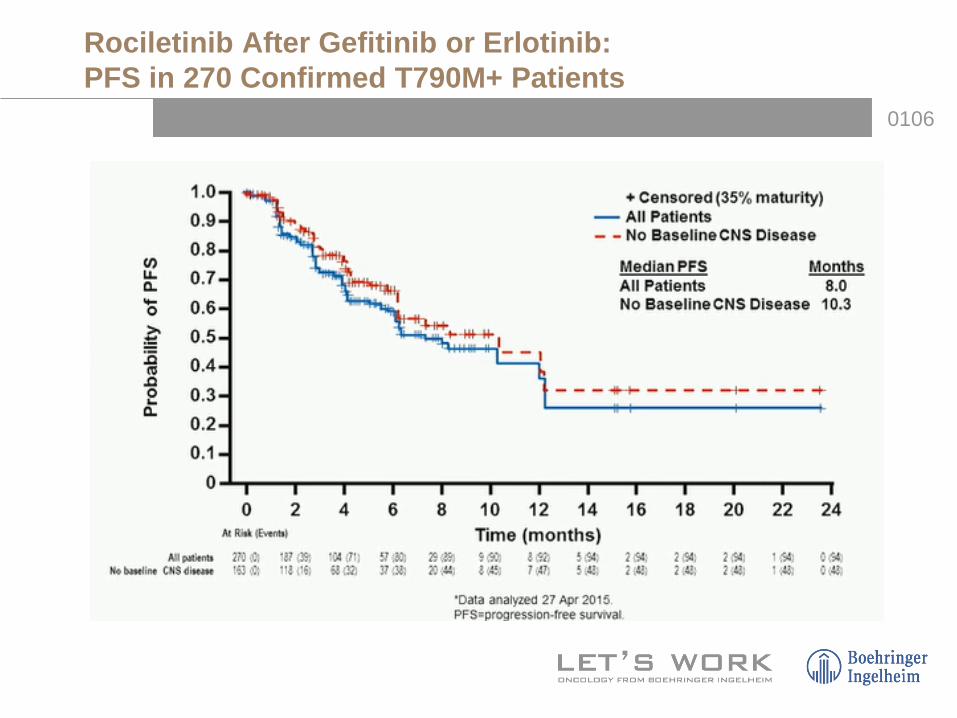
Rociletinib After Gefitinib or Erlotinib: PFS in 270 Confirmed T790M+ Patients

0107
Quantitative and Sensitive BEAMing Test(Sysmex Inostics) Used for Plasma EGFR Mutation Testing

0108
Plasma Testing for T90M Has Good Sensitivity and Likely Good Specificity
• Plasma testing: goodoption
• T790M tissue plasma are not false positives. -790M was confirmed in plasma on subsequent testing in 5/7 samples
Tissue as reference T790M Activating mutationsPositive percent agreement 81% (155/192) 87% (193/221)

0109
32% 25%
PFS 4.7 months
Janjigian Y, et al. Cancer Discov. 2014;4:1036-1045.
Phase I/II Study of Afatinib + Cetuximab

0110
Source: Compiled by Neeta Somaiah & George Simon.
Approved/Launched SRC inhibitors
Inh. of PI3K, mTOR, AKT, MAPK/ERK
Apoptosis agonists
Anti-FGFR
DNA replication inhibitors
Antiangiogenics
Inhibitors of Mitosis/Topoisomerases
Others
Alkylating agents
Protein degradation
Anti-IGFR
Immunostimulants/Vaccines
TKI-EGFR
Anti-VEGFFosbretabulin (CA4P)
ABT-751
ANG-615
NPI-2358
ASA404
AfliberceptIVandetanib
ARamucirumabIXL-647
IAV-951
CT-322
ABevacizumab
Ixabepilone
BI-2536
ARRAY520
Vorinostat
RetaspimycinEtinostat
AUY922
Everolimus (RAD-001)Sirolimus (Rapamycin)
Temsirolimus (CCI-779)Enzostaurin
Deforolimus (AP23573)
AZD-6244 PX-866
OSI-027
AZD-8055
I XL-184
Figitumumab (CP-751871)
AVE-1642A Cixutumumab
A AMG-479
OSI-906
= IV & PO= PO= IV= 1st-line
= 2nd-line= 1st and 2nd line
= 3rd-line
= Undeclared
PF-2341066
MetMab
BHB022
Dulanermin (AMG-951)A Mapatumumab
AApomabAMG655
LCL-161
YM-155
I Dasatinib (Sprycel)AZD-0530
KX2-391
IBrivanibAV-370
ITKI-258
AG-014699ABT-888
CS-7017
Phase III
Phase II
Phase I
Stem Cell (PPAR, Hedgehog)
IPI-926
XL-281
BMS833923
BIBW2992
I PF-00299804
IBMS-690514
Cisplatin
CarboplatinIfosfamide
ACetuximabI Erlotinib
Docetaxel
Antimetabolites
= SCLC
Etoposide
Gemcitabine
Irinotecan
Paclitaxel
Pemetrexed
Vinorelbine/ Vinblastine
Paclitaxel (Albumin B.)
Liposomal Cisplatin
Panobinostat
GDC0449
AMG102
AEG35156
A Bavituximab
I Cediranib
APanitumumabANimotuzumab
Matuzumab
Gefitinib
I Sunitinib
SorafenibI Axitinib
I Motesanib
A R-1507
XL-228
MKC-1Oblimersen
Cilengitide
TalactoferrinSapacitabine
ReolysinIrvalec (Custirsen)
Mage-A3Stimuvax
PF-3512676 (agatolimod)
Tremelimumab
Imprime PGG
GVAX
CimaVax EGF
AVE-8062
Pralatrexate
ARQ197Apricoxib
IABT-869
ARRY-886
ARC-100
AS-1411
BI-6727
Decitabine
Cositecan
Glufosfamide
Eribulin
I Bosutinib
Kahalalide F
IMO-2055
EC-145
AF-50035
GI4000
KOS-1584A Lexatumumab
ARQ-621
Lip. PaclitaxelCamptothecin
ISIS-23722
PEG-Irinotecan
MDX-1105
AIntetumumab
IE-7080
AMP-001
IMGN-242
IDanusertib
JNJ-26854165
Vical-2 vaccine
A
Itipifarnib
Pertuzumab
INeratinib
A Naptumomab
MGCD-0103
AMORab-009
MP-470
V-930VX-001
Vinorelbine (emulsion)
V-935
Crinobulin
Registered
XL-999IBIBF-1120
I
XL-184 II BMS-690514
I Pazopanib
SNX5542
TemozolomidePicoPt
Obatoclax
AT-101
Zibotentan
Amrubicin
PF-00299804 I
Topotecan
ABT-263
INeratinib
BEZ-235 / BTGT226 / BKM
Inh. of Bcl-2
obatoclax
A
I
BSI-201
Auristatin PE
ADH-1 (Exherin)I = TKIA = Antibody
Zometa
bexarotene
LucanixNOV-002
belinostat
CYT-997
AMG-386
Retaspimycin
ABT-263
BNC-105
rebimastat
Treatment Options in NSCLC110

0111
OS in Advanced EGFR-Mutated Lung Cancer
3 7
10 13
36
48
60
0
10
20
30
40
50
60
70
Palliative Care(PC)
Single-agent PC Platinum-basedCT
CT +Bevacizumab
TKI + PreviousTx
New TKI +Previous Tx
Inmunotherapy+ Previous Tx
Med
ian
Sur
viva
l (m
onth
s)
19751990
20002006
2010
2014
2016

0112
Conclusions [1]
• Important advances in treatment of NSCLC: – Chemotherapy time: median OS 10 months– CT plus bevacizumab time: median OS 12.3 months– First-generation EGFR TKIs : median PFS 10 months, OS 27 months,
without benefit in OS compared with Chemotherapy arm (includedDel exon and L858R)
• Afatinib: first TKI that improved OS compared with CT in EGFR Del 19:
– LUX-Lung 3: median 33.3 vs 21.1 mo, HR=0.54, P=0.0015– LUX-Lung 6: median 31.5 vs 18.4 mo, HR=0.64, P=0.0229
• Del 19 and L858R: two different populations Studies withdifferent design
• Afatinib in first-line: standard of care in patients with EGFR Del19 and good option in other EGFR mutations (L858R)

0113
Conclusions [2]
• Del 19 and L858R are two different populations:– Studies with different designs– Afatinib: different mechanism of action
• Afatinib in first-line: standard of care in patients withEGFR Del19 and good option in other EGFR mutations (L858R)
• New TKIs (AZD 9291, rociletinib): – Excellent option after PD to TKI (first or second
generation)