Embed Size (px)
Citation preview
Professor Martin Schuler MDWest German Cancer Center Essen, Germany
Right patient, right treatment: Insights in EGFR mutation-positive NSCLC

Question: What is your current standard-of-care in the first-line treatment of patients with Del19 NSCLC?
1. Afatinib*
2. Chemotherapy
3. Erlotinib
4. Gefitinib
5. Other
*Afatinib is approved in a number of markets, including the EU, Japan, Taiwan and Canada, under the brand name GIOTRIF® and in the USA under the brand name GILOTRIF® for use in patients with distinct types of EGFR mutation-positive NSCLC. Registration conditions differ internationally, please refer to locally approved prescribing information. Afatinib is under regulatory review by health authorities in other countries worldwide. Afatinib is not approved in other indications.

Question: What is your current standard-of-care in the first-line treatment of patients with L858R NSCLC?
1. Afatinib
2. Chemotherapy
3. Erlotinib
4. Gefitinib
5. Other

Afatinib: An irreversible ErbB family blocker
Li D, et al. Oncogene 2008;27:4702–11; Solca F, et al. J Pharmacol Exp Ther 2012;343:342–50; Yang J, et al. Lancet Oncol 2012;13:539–48
Molecular potency and selectivity
IC50 (nM)
EGFR 0.5
HER2 14
ErbB4 1
HGFR >10,000
VEGFR2 >100,000
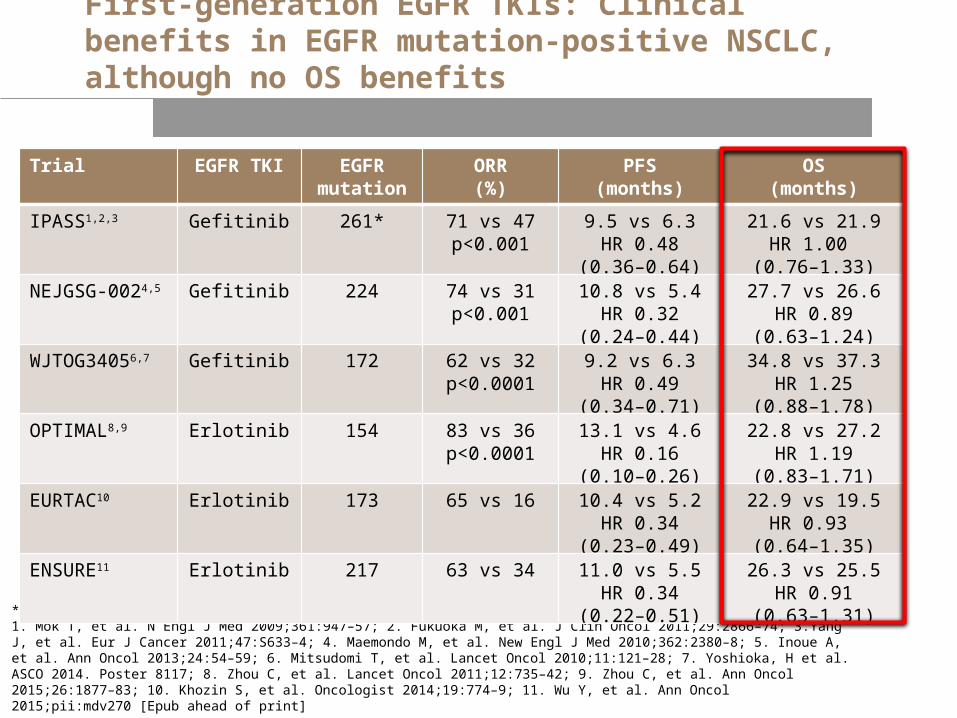
First-generation EGFR TKIs: Clinical benefits in EGFR mutation-positive NSCLC, although no OS benefits
*Out of a total of 1217 patients.1. Mok T, et al. N Engl J Med 2009;361:947–57; 2. Fukuoka M, et al. J Clin Oncol 2011;29:2866–74; 3.Yang J, et al. Eur J Cancer 2011;47:S633–4; 4. Maemondo M, et al. New Engl J Med 2010;362:2380–8; 5. Inoue A, et al. Ann Oncol 2013;24:54–59; 6. Mitsudomi T, et al. Lancet Oncol 2010;11:121–28; 7. Yoshioka, H et al. ASCO 2014. Poster 8117; 8. Zhou C, et al. Lancet Oncol 2011;12:735–42; 9. Zhou C, et al. Ann Oncol 2015;26:1877–83; 10. Khozin S, et al. Oncologist 2014;19:774–9; 11. Wu Y, et al. Ann Oncol 2015;pii:mdv270 [Epub ahead of print]
Trial EGFR TKI EGFR mutation
ORR(%)
PFS(months)
OS(months)
IPASS1,2,3 Gefitinib 261* 71 vs 47p<0.001
9.5 vs 6.3HR 0.48
(0.36–0.64)
21.6 vs 21.9HR 1.00
(0.76–1.33)
NEJGSG-0024,5 Gefitinib 224 74 vs 31p<0.001
10.8 vs 5.4HR 0.32
(0.24–0.44)
27.7 vs 26.6HR 0.89
(0.63–1.24)
WJTOG34056,7 Gefitinib 172 62 vs 32p<0.0001
9.2 vs 6.3HR 0.49
(0.34–0.71)
34.8 vs 37.3HR 1.25
(0.88–1.78)
OPTIMAL8,9 Erlotinib 154 83 vs 36p<0.0001
13.1 vs 4.6HR 0.16
(0.10–0.26)
22.8 vs 27.2HR 1.19
(0.83–1.71)
EURTAC10 Erlotinib 173 65 vs 16 10.4 vs 5.2HR 0.34
(0.23–0.49)
22.9 vs 19.5HR 0.93
(0.64–1.35)
ENSURE11 Erlotinib 217 63 vs 34 11.0 vs 5.5HR 0.34
(0.22–0.51)
26.3 vs 25.5HR 0.91
(0.63–1.31)
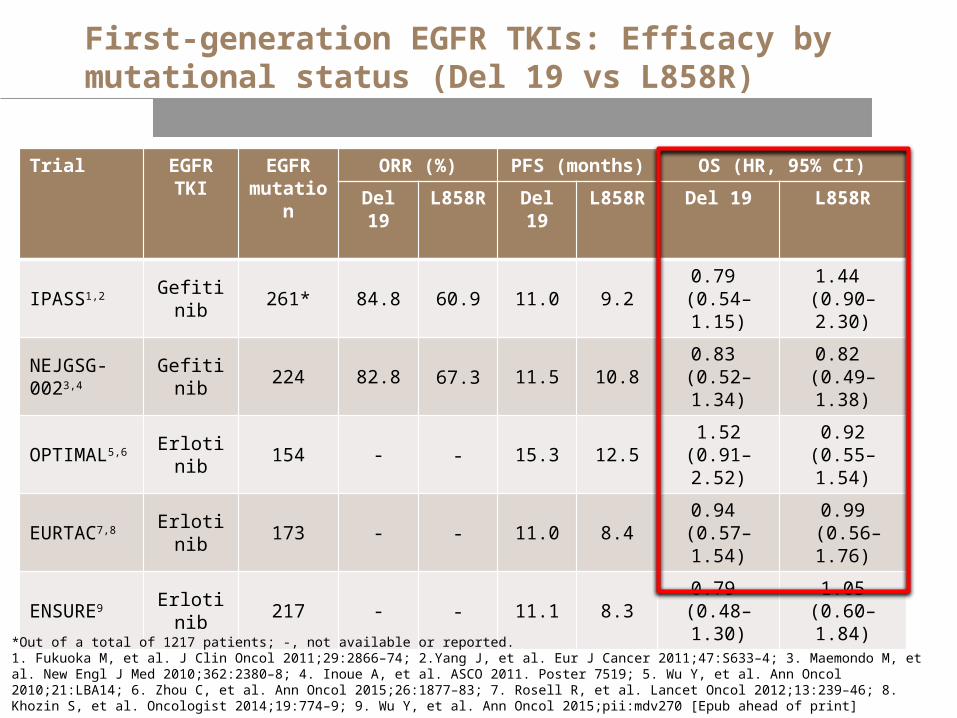
Trial EGFR TKI
EGFR mutation
ORR (%) PFS (months) OS (HR, 95% CI)
Del 19 L858R Del 19 L858R Del 19 L858R
IPASS1,2 Gefitinib 261* 84.8 60.9 11.0 9.2 0.79 (0.54–1.15)
1.44 (0.90–2.30)
NEJGSG-0023,4 Gefitinib 224 82.8 67.3 11.5 10.8 0.83
(0.52–1.34)0.82
(0.49–1.38)
OPTIMAL5,6 Erlotinib 154 - - 15.3 12.5 1.52(0.91–2.52)
0.92(0.55–1.54)
EURTAC7,8 Erlotinib 173 - - 11.0 8.4 0.94 (0.57–1.54)
0.99 (0.56–1.76)
ENSURE9 Erlotinib 217 - - 11.1 8.3 0.79 (0.48–1.30)
1.05(0.60–1.84)
First-generation EGFR TKIs: Efficacy by mutational status (Del 19 vs L858R)
*Out of a total of 1217 patients; -, not available or reported.1. Fukuoka M, et al. J Clin Oncol 2011;29:2866–74; 2.Yang J, et al. Eur J Cancer 2011;47:S633–4; 3. Maemondo M, et al. New Engl J Med 2010;362:2380–8; 4. Inoue A, et al. ASCO 2011. Poster 7519; 5. Wu Y, et al. Ann Oncol 2010;21:LBA14; 6. Zhou C, et al. Ann Oncol 2015;26:1877–83; 7. Rosell R, et al. Lancet Oncol 2012;13:239–46; 8. Khozin S, et al. Oncologist 2014;19:774–9; 9. Wu Y, et al. Ann Oncol 2015;pii:mdv270 [Epub ahead of print]

Del19 L858R
Afatinib (n=112) Cis/Pem (n=57) Afatinib (n=91) Cis/Pem (n=47)
Median, months 33.3 21.1 27.6 40.3
HR (95% CI) p value 0.54 (0.36–0.79) p=0.0015 1.30* (0.80–2.11) p=0.29
Preplanned OS analysis of LUX-Lung 3: Mutation subgroups
*HR 1.02 (0.62–1.69) when adjusted for baseline imbalances.Yang J, et al. Lancet Oncol 2015;16:141–51
Del19
Time of overall survival (months)
0 3 6 9 12 15 18 21 24 270.0
0.2
0.4
0.6
0.8
1.0E
stim
ated
OS
pro
babi
lity
30 33 36 39 42 45 48 51
AfatinibCis/Pem
No. at risk:Afatinib 112 108 105 102 96 93 83 80 72 62 58 51 34 30 21 6 1 0Cis/Gem 57 55 50 46 43 37 33 27 25 22 20 16 10 6 1 1 0 0
Del19
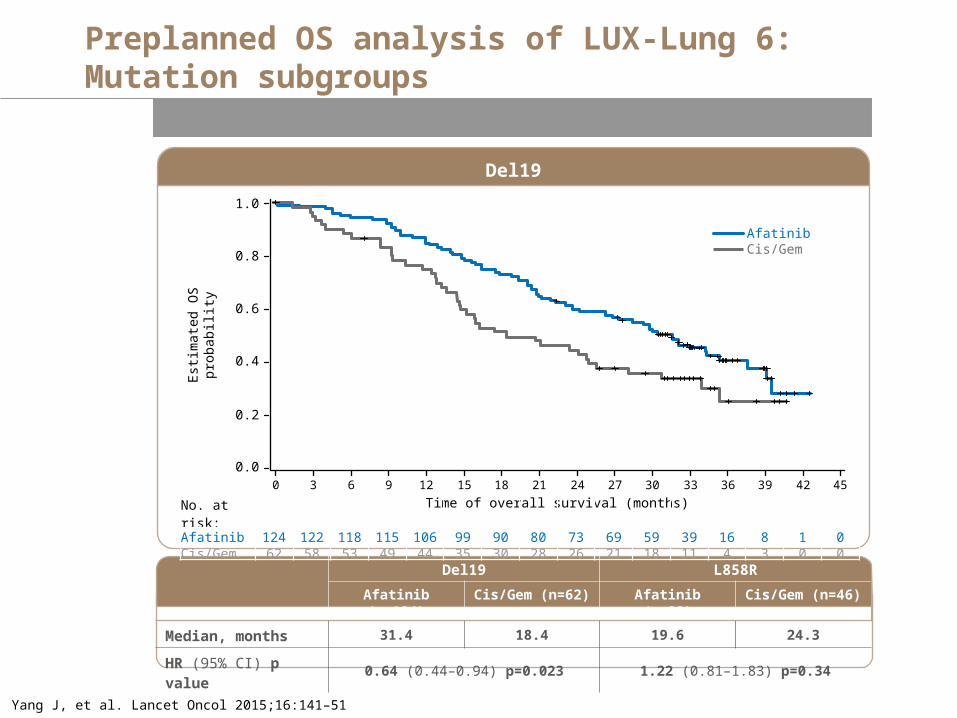
Preplanned OS analysis of LUX-Lung 6: Mutation subgroups
Yang J, et al. Lancet Oncol 2015;16:141–51
Time of overall survival (months)0 3 6 9 12 15 18 21 24 27
0.0
0.2
0.4
0.6
0.8
1.0E
stim
ated
OS
pro
babi
lity
30 33 36 39 42 45
Del19 L858R
Afatinib (n=124) Cis/Gem (n=62) Afatinib (n=92) Cis/Gem (n=46)
Median, months 31.4 18.4 19.6 24.3
HR (95% CI) p value 0.64 (0.44–0.94) p=0.023 1.22 (0.81–1.83) p=0.34
AfatinibCis/Gem
No. at risk:Afatinib 124 122 118 115 106 99 90 80 73 69 59 39 16 8 1 0Cis/Gem 62 58 53 49 44 35 30 28 26 21 18 11 4 3 0 0
Key practical considerations in the management of EGFR mutation positive NSCLC

What would you do?
Newly diagnosed advanced or metastatic NSCLC (adeno) not suitable for surgical
resection
1) Start chemotherapy immediately?
2) Perform biomarker analysis and treat based on analysis
results?

What would you do?
• Therascreen EGFR PCR test turnaround time:1
– 4.9 business days (95% CI 4.5–5.5 days)
• Actual time from the test request to the result:– 17.8 days (95% CI 16.4–19.4 days)
1. https://www.nice.org.uk/guidance/dg9/chapter/5-Outcomes(Accessed 20 August 2015)
Newly diagnosed advanced or metastatic NSCLC (adeno) not suitable for surgical
resection
1) Start chemotherapy immediately?
2) Perform biomarker analysis and treat based on analysis
results?

Question: What is the key factor determining your therapy choice in first-line EGFR mutation-positive NSCLC?
1. Efficacy
2. Safety
3. Quality-of-life/symptom improvement
4. Convenience
5. Other
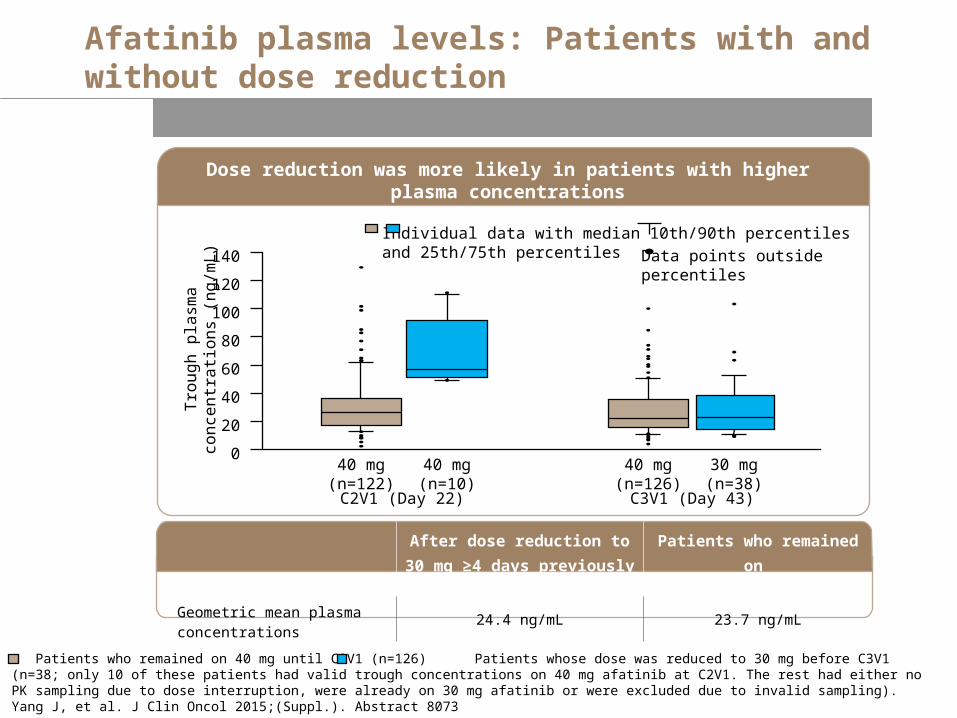
Afatinib plasma levels: Patients with and without dose reduction
Dose reduction was more likely in patients with higher plasma concentrations
140
120
100
80
60
40
20
0Tro
ug
h p
lasm
a c
on
cen
tra
tion
s (n
g/m
L)
C3V1 (Day 43)
40 mg(n=126)
30 mg(n=38)
C2V1 (Day 22)
40 mg(n=122)
40 mg(n=10)
Individual data with median and 25th/75th percentiles
10th/90th percentiles
Data points outside percentiles
After dose reduction to 30 mg ≥4 days previously (n=38)
Patients who remained on 40 mg (n=126)
Geometric mean plasma concentrations
24.4 ng/mL 23.7 ng/mL
Patients who remained on 40 mg until C3V1 (n=126) Patients whose dose was reduced to 30 mg before C3V1 (n=38; only 10 of these patients had valid trough concentrations on 40 mg afatinib at C2V1. The rest had either no PK sampling due to dose interruption, were already on 30 mg afatinib or were excluded due to invalid sampling).Yang J, et al. J Clin Oncol 2015;(Suppl.). Abstract 8073

Median PFS similar in patients who had afatinib dose reductions in the first 6 months and those who remained on afatinib 40 mg once daily
Tolerability-guided dose modification and PFS
CI, confidence interval; HR, hazard ratio.Yang J, et al. J Clin Oncol 2015;(Suppl.). Abstract 8073
No. at risk<40 mg in first 6 months≥40 mg for first 6 months
105124
8793
7576
5862
4136
2624
1516
64
21
00
Time (months)
1.0
0.6
0.4
0.2
0
Es
tim
ate
d P
FS
pro
ba
bil
ity
0 3 6 9 12 15 18 21 24 27
0.8
<40 mg in first 6 months
≥40 mg in first 6 months
<40 mg in first 6 months (n=105)
≥40 mg for first 6 months (n=124)
Median PFS, months 11.3 11.0
HR (95% CI); p value 1.25 (0.91–1.72); 0.175

Summary and conclusion
• First-generation EGFR TKIs have provided significant clinical benefits to patients with EGFR mutation-positive NSCLC. However, no OS advantage has been formally demonstrated so far
• First-line afatinib significantly improved OS vs chemotherapy in EGFR Del19 patients in two randomised trials
– LUX-Lung 3: median 33.3 vs 21.1 months, HR 0.54, p=0.0015– LUX-Lung 6: median 31.4 vs 18.4 months, HR 0.64, p=0.023
• No significant difference in OS of patients with L858R mutations treated with afatinib, individually, or in exploratory combined analysis
– However, benefit in PFS, ORR and PRO have been demonstrated in LUX-Lung 3 and 6
• Afatinib also showed robust activity in patients with most frequent uncommon EGFR mutations including those with point mutations or duplications in exons 18–21 (ORR 71.1%, PFS 10.7 months, OS 19.4 months)
• Certain practical considerations may be important in maximising benefit in first-line treatment of patients with EGFR mutation+ NSCLC and should be kept in mind when managing these patients
Questions and discussion





























