Embed Size (px)
Citation preview

1 | P a g e
Impact of haemostatic mechanisms on pathophysiology of preeclampsia
Chris Gardiner1, Manu Vatish2
1Haemostasis Research Unit, Department of Haematology, University College London, UK. 2Nuffield Department of Obstetrics and Gynaecology, University of Oxford, Oxford, UK. Corresponding author. Dr Chris Gardiner PhD, Haemostasis Research Unit, Department of Haematology, University College London1st Floor, 51 Chenies Mews,London WC1E 6HX. UK Phone: +44 (0)20 7679 6417 Fax: +44 (0)20 7679 6424

2 | P a g e
Placental formation Humans have haemochorial placentation in which the placenta is in direct contact with circulating
maternal blood. The placenta comprises fetal vasculature, stroma, immune cells and cytotrophoblast
which are extravillous and villous. During implantation, the maternal decidual arteries are invaded
by placental extravillous cytotrophoblasst resulting in the subsequent remodelling of the decidual
spiral arteries. During this process, placental extravillous cytotrophoblasts replace maternal
endothelial cells and disorganise the vascular smooth muscle cells (VSMC). This leads to a high flow
and low resistance placental circulation enabling effective exchange of nutrients across the chorionic
villi. The chorionic villi are covered in syncytiotrophoblasts, which are formed from a villous
cytotrophoblast layer, in direct contact with the maternal blood, and thus trophoblasts, rather than
the endothelium, form the exchange surface in the intervillous space and act as the gatekeeper
between maternal blood and embryonic tissues.
During implantation, tissue factor (TF) and plasminogen activator inhibitor-1 (PAI-1) play a key role in
creating a haemostatic envelope around the invading blastocyst thus preventing local decidual
haemorrhage [1-3]. Unlike other vascular beds, trophoblasts constitutively express TF. In normal
pregnancies TF procoagulant activity is held in check as the syncytiotrophoblast adapts a
pseudoendothelial phenotype through the expression of integrin αv/β3, PECAM-1 and E-cadherin
[4], endothelial protein C receptor (EPCR), thrombomodulin, annexin-V and the tissue factor
pathway inhibitors (TFPI-1 and TFPI-2). This prevents TF induced thrombin generation in healthy
pregnancies [5]. TF is essential for fetal and placental development and the prevention of placental
abruption in later pregnancy, as demonstrated by fetal lethality in TF knockout mice and supported
by the absence of reported deficiency states in humans [2].
The protease activated receptors PAR-1, PAR-2 and PAR-3 are also expressed on extravillous
trophoblasts (EVT) and syncytiotrophoblasts [6, 7] and mediate cytotrophoblast invasion via
thrombin (PAR-1 and PAR-3) and TF/FVIIa or TF/FXa (PAR-2) activation, whilst PAR-1 simultaneously
induces differentiation through nuclear recruitment of β -catenin and induction of Wnt-dependent
T-cell factor 4 [6, 8, 9].
Pre-eclampsia
Pre-eclampsia (PE) is a disorder of new onset hypertension and proteinuria, thrombocytopenia,
renal insufficiency or impaired liver function in the second half of pregnancy [10]. The origins of PE
lie in the placenta, and delivery remains the only effective treatment. PE is a complex syndrome
with several overlapping subtypes, e.g. early onset or late onset, with or without fetal
growth restriction (FGR) [11]. PE has been described as a two stage disease [12] with a first
(pre-clinical) stage comprising deficient remodelling of the uteroplacental spiral arteries (8–
18 weeks), dysfunctional perfusion and placental oxidative stress leading to the clinical
stage (after 20 weeks) characterised by maternal systemic inflammation and vascular
dysfunction. While this is undoubtedly true for early onset disease (<34 weeks gestation),
many cases of late onset PE have no antecedent placental pathology [13] and appear as two
distinct phenotypes as indicated by the placental histology. In general, placentae from early
onset PE are smaller than aged matched controls [14],with more infarction and are less well

3 | P a g e
developed, with reduced terminal villi volume and surface area [15, 16]. In contrast, late
onset PE placentas are frequently larger with similar morphology to normal term placentas
and some show increased arteriopathy [16].
The diverse nature of PE is also reflected by the maternal haemodynamic state. Early onset
PE and, to a lesser extent, normotensive FGR are preceded by increased total vascular
resistance and low cardiac output, where as those women destined to develop late onset PE
are characterised by low total vascular resistance and high cardiac output [17]. This has led
to the concept of “placental PE” in which an abnormal placenta interacts with normal
maternal vasculature leading to early onset disease, and “maternal PE” in which a normal
placenta interacts with abnormal vasculature to produce late onset disease [18]. Although
the aetiology of the different subtypes is clearly distinct, the maternal syndrome of
hypertension, proteinuria and oedema due as a result of vascular inflammation and
endothelial dysfunction represent a common pathway. This is driven by increased placental
release of the soluble isoforms of the vascular endothelial growth factor receptor 1
(sVEGFR1 or sFlt-1) and endoglin (soluble TGFβ-1 receptor) with reduced placental growth
factor (PlGF) [18].
Perhaps unsurprisingly, given the heterogeneous nature of the condition, many pathogenic
mechanisms have been proposed and these have been recently reviewed [19].This review
will concentrate on haemostatic mechanisms responsible for placental dysfunction.
As previously discussed, tissue factor is essential for placental development. PAR signalling is
important in trophoblast differentiation and a failure of trophoblasts to adopt an
endothelial phenotype is associated with PE [4]. However, increased TF expression
[2](Girardi, 2010) and/or exposure of trophoblast TF to FVIIa during decidual haemorrhage
causes inappropriate activation of the coagulation cascade and this has been proposed as
the primary cause of impaired trophoblast invasion of the decidua (Lockwood et al., 2011).
Increased expression of TF in endothelium of the basal decidua is associated with bilateral
notching of the uterine artery and severe PE with FGR [20]. Aberrant syncytiotrophoblast TF
expression has been reported in PE [21, 22] with a corresponding reduction in TFPI1 [21]
and TFPI2 [23, 24]. We have also demonstrated increased tissue factor activity on
syncytiotrophoblast extracellular vesicles (STEV) released into the maternal circulation from
the placenta in PE [25].
Over expression of villous trophoblast PAR-1 is also a feature of early onset preeclampsia
[26]. Excessive thrombin activation of PAR-1 enhances sflt-1 expression and secretion by
trophoblasts through the PAR-1 /NADPH oxidase /ROS signalling pathway [27, 28](Zhao et
al., 2012, Huang et al., 2015). This is evinced by increased maternal markers of in vivo
thrombin generation and fibrin turnover [29-32]. This represents a clear link between
increased placental TF and the resultant thrombin activation of PAR-1 [33] leading to excess
sflt-1 secretion and maternal endothelial dysfunction. Perhaps of more importance to the
foetus is the localised effect of thrombin generation in the placenta. Perivillous fibrin

4 | P a g e
deposition and placental infarction are strongly associated with early onset PE and severe
disease [34] [35-37].
Infarction may lead to localised hypoxia and the expression of hypoxia-inducible factor 1-
alpha (HIF-1α). Several studies have shown that women with PE have persistently elevated
placental HIF-1α which promotes enhanced transcription of genes encoding sFlt-1, endoglin
and endothelin-1, all of which are known to contribute to preeclampsia [38-40]. Moreover,
expression of HIF-1α is upregulated not only by hypoxia, but also by inflammatory stimuli
(for example, thrombin, vasoactive peptides, cytokines, such as TNFα, and reactive oxygen
species [ROS]), especially those mediated by NF-κB, as the promoter of HIF-1α contains an
NF-κB binding site [19].
Changes in systemic maternal haemostasis Normal pregnancy is associated with a physiological increase in many procoagulant factors and
inhibitors of fibrinolysis. Increases in coagulation factors VII, VIII, X, XII and XIII, fibrinogen and von
Willebrand factor are all commonly observed and are maximal around term. Free protein S
decreases throughout pregnancy and this is reflected by increasing resistance to activated protein C
(APC). Fibrinolytic activity is reduced during pregnancy, as a result of increased levels of plasminogen
activator inhibitor-1 (PAI-1) from endothelial cells and plasminogen activator inhibitor-2 (PAI-2) from
the placenta [41]. These changes are necessary in order to meet the haemostatic challenge of
parturition but contribute to an increased risk of venous thromboembolism during pregnancy and
the puerperium. A benign gestational thrombocytopenia is not infrequently observed, particularly in
the third trimester but this is not associated with excessive platelet activation and is most probably
due to increased plasma volume. As might be expected, markers of in vivo thrombin generation
(thrombin-antithrombin complexes [TAT] and prothrombin fragment 1.2 [PF1.2]) are slightly
increased as is the endogenous thrombin potential (ETP) assay [42].
The association between coagulation activation and preeclampsia has been recognised since the
early 1950s. The shift in the haemostatic balance towards a procoagulant/hyperfibrinolytic picture
observed in normal pregnancy is exaggerated in preeclampsia. Many consider the haemostatic
changes observed in mild preeclampsia as an augmentation of the normal maternal physiological
response. This is in contrast to severe preeclampsia in which the imbalance of the haemostatic
system is pathological, reflecting the systemic inflammation and endothelial dysfunction
characteristic of the disease. In practice, a spectrum of haemostatic changes are observed; from the
subtle variations seen in mild preeclampsia to the unregulated disseminated intravascular
coagulation (DIC) observed in the HELLP (haemolysis, elevated liver enzymes and low platelets)
syndrome. Increased thrombomodulin activity, tissue factor activity and procoagulant phospholipids
are observed [43, 44].
The role of platelets The association of excessive platelet activation and consumption in PE has been recognised for many
years [45, 46]. There is now ample evidence to implicate platelet activation in the pathogenesis of
PE. Platelet activation may occur several weeks prior to the onset of symptomatic PE [47, 48];
Increased mean platelet volume in late first trimester of pregnancy has been reported to predict
intrauterine growth restriction and PE [49]; Platelet-derived soluble factors are reported to regulate

5 | P a g e
human extravillous trophoblast differentiation and invasion into maternal spiral arteries [50]; Low
dose aspirin (LDA) initiated before the 16th week of gestation significantly reduces the incidence and
severity of preeclampsia, FGR and preterm birth, whereas LDA initiated after the 16th week has little
effect on pregnancy outcome [51]; Increased platelet-leucocyte aggregates are observed in PE
compared to normotensive pregnancies [44, 52] and these have been identified as a significant
source of extraplacental sflt-1 in women with PE during pregnancy and for several months post-
partum [53, 54].
We have demonstrated that platelets take up extracellular vesicles derived from the
syncytiotrophoblast (STEVs) in vitro [55, 56] and that placenta-specific proteins and mRNA are
detectable in platelets isolated from the peripheral blood of pregnant women. Furthermore,
incubation of platelets with STEV leads to platelet degranulation in vitro (unpublished data). This is
consistent with previous reports of reduced aggregation response to weak agonists in platelets from
PE women due to “exhausted” platelets [57-60]. It is possible that systemic release of vasoactive
substances by platelets during PE may contribute to vascular dysfunction. Most recently, it has been
shown that endothelial EVs cause the accumulation of activated platelets within the placental
vascular bed leading to inflammasome activation in trophoblasts in a mouse model of PE [61].
The role of neutrophils Normal pregnancy is characterized by the presence of innate immune cells at the feto-maternal
interface from the first trimester. It has been proposed that TLR stimulated trophoblasts recruit
neutrophils via the release of IL-8 [62]. IL-8 and STEV released from placental explants induce the
formation of neutrophil extracellular traps (NETs) in vitro [63]. Furthermore NETs have been
demonstrated in the intervillous space of placentae from pre-eclamptic women and it has been
proposed that NET formation may be responsible for the increased cell-free DNA observed in the
plasma of women with PE [64]. As NETs are known to promote thrombosis in a P-selectin-dependent
manner [65, 66] it is possible that NET formation may contribute to placental infarction.
In a rat model of PE, neutrophil depletion was shown to attenuate placental ischaemia-associated
hypertension, suggesting a significant role for neutrophils in the pathogenesis of PE [67]. It has been
reported that activated endothelial cells induce NET formation which in turn causes further
endothelial damage [68]. This, and the association of NETs with thrombotic microangiopathies [69],
suggest a role for systemic NET involvement in fulminating PE and HELLP syndrome.
Anti-phospholipid antibodies and PE Maternal antiphospholipid antibodies (aPL) are associated with recurrent miscarriage, intrauterine
death, preeclampsia, intrauterine growth restriction and premature birth [70]. For many years, it has
been assumed that the role of aPL in the pathogenesis obstetric antiphospholipid syndrome (APS) is
primarily thrombotic. However, recent findings question the validity of this assumption. Combined
LDA and heparin are effective in improving pregnancy outcome in women with APS and a history of
early pregnancy loss [71-73] but women with APS and prior fetal loss remain at high risk of placenta-
mediated complications despite treatment with LDA and LMWH [74].
Heparin appears to exert its protective effect through the inhibition of complement activation [75].
aPL cause a complement-independent inflammatory response by signalling through TLR-4 on EVT

6 | P a g e
[76] whereas pregnancies in mice infused with non-complement-fixing β2GP1 single chain antibody
were unaffected [77]. Furthermore, inhibition of C3 convertase prevented fetal loss and growth
retardation in mice injected with human aPL [78]. A recent clinical trial reported pravastatin
improved pregnancy outcome in women with APS who were refractory to LMW/LDA and previously
developed PE [79]
Conclusions
It is clear that haemostatic mechanisms play an important role in the pathogenesis of PE. It is hoped
that our increased knowledge in this field will identify new therapeutic strategies for the treatment
and prevention of this dangerous condition.
Conflict of interest statement
The University College London has received an unrestricted educational grant from Sysmex Inc. in
the last 12 months. MV has received research support from Roche Diagnostics.
7 | P a g e
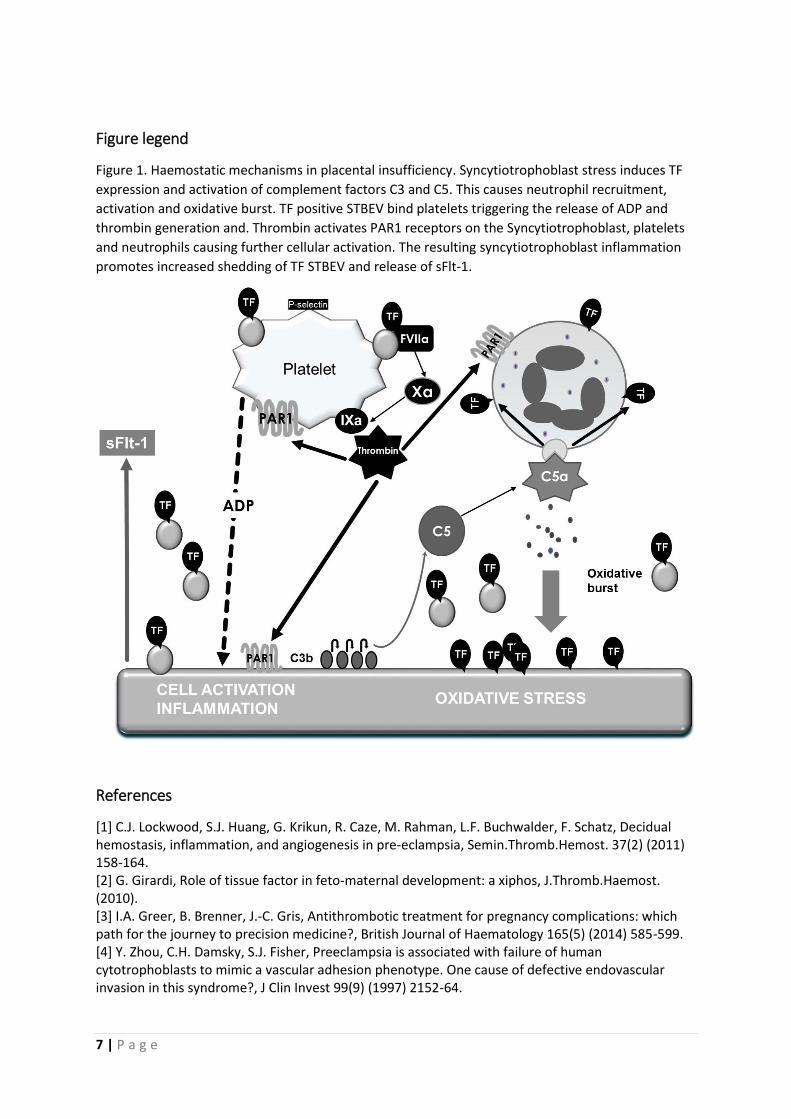
Figure legend
Figure 1. Haemostatic mechanisms in placental insufficiency. Syncytiotrophoblast stress induces TF
expression and activation of complement factors C3 and C5. This causes neutrophil recruitment,
activation and oxidative burst. TF positive STBEV bind platelets triggering the release of ADP and
thrombin generation and. Thrombin activates PAR1 receptors on the Syncytiotrophoblast, platelets
and neutrophils causing further cellular activation. The resulting syncytiotrophoblast inflammation
promotes increased shedding of TF STBEV and release of sFlt-1.
References
[1] C.J. Lockwood, S.J. Huang, G. Krikun, R. Caze, M. Rahman, L.F. Buchwalder, F. Schatz, Decidual hemostasis, inflammation, and angiogenesis in pre-eclampsia, Semin.Thromb.Hemost. 37(2) (2011) 158-164. [2] G. Girardi, Role of tissue factor in feto-maternal development: a xiphos, J.Thromb.Haemost. (2010). [3] I.A. Greer, B. Brenner, J.-C. Gris, Antithrombotic treatment for pregnancy complications: which path for the journey to precision medicine?, British Journal of Haematology 165(5) (2014) 585-599. [4] Y. Zhou, C.H. Damsky, S.J. Fisher, Preeclampsia is associated with failure of human cytotrophoblasts to mimic a vascular adhesion phenotype. One cause of defective endovascular invasion in this syndrome?, J Clin Invest 99(9) (1997) 2152-64.

8 | P a g e
[5] R. Sood, S. Kalloway, A.E. Mast, C.J. Hillard, H. Weiler, Fetomaternal cross talk in the placental vascular bed: control of coagulation by trophoblast cells, Blood 107(8) (2006) 3173-80. [6] P.J. O'Brien, H. Koi, S. Parry, L.F. Brass, J.F. Strauss, 3rd, L.P. Wang, J.E. Tomaszewski, L.K. Christenson, Thrombin receptors and protease-activated receptor-2 in human placentation: receptor activation mediates extravillous trophoblast invasion in vitro, Am J Pathol 163(4) (2003) 1245-54. [7] S.C. Even-Ram, S. Grisaru-Granovsky, D. Pruss, M. Maoz, Z. Salah, Y. Yong-Jun, R. Bar-Shavit, The pattern of expression of protease-activated receptors (PARs) during early trophoblast development, J Pathol 200(1) (2003) 47-52. [8] S. Grisaru-Granovsky, M. Maoz, O. Barzilay, Y.J. Yin, D. Prus, R. Bar-Shavit, Protease activated receptor-1, PAR1, promotes placenta trophoblast invasion and beta-catenin stabilization, J Cell Physiol 218(3) (2009) 512-21. [9] M. Knofler, J. Pollheimer, Human placental trophoblast invasion and differentiation: a particular focus on Wnt signaling, Front Genet 4 (2013) 190. [10] ACOG, Hypertension in pregnancy. Report of the American College of Obstetricians and Gynecologists' Task Force on Hypertension in Pregnancy, Obstetrics and gynecology 122(5) (2013) 1122-31. [11] L. Myatt, C.W. Redman, A.C. Staff, S. Hansson, M.L. Wilson, H. Laivuori, L. Poston, J.M. Roberts, Strategy for standardization of preeclampsia research study design, Hypertension 63(6) (2014) 1293-301. [12] C.W. Redman, I.L. Sargent, Latest advances in understanding preeclampsia, Science 308(5728) (2005) 1592-1594. [13] C.W. Redman, I.L. Sargent, A.C. Staff, IFPA Senior Award Lecture: making sense of pre-eclampsia - two placental causes of preeclampsia?, Placenta 35 Suppl (2014) S20-5. [14] B. Dahlstrom, P. Romundstad, P. Oian, L.J. Vatten, A. Eskild, Placenta weight in pre-eclampsia, Acta Obstet Gynecol Scand 87(6) (2008) 608-11. [15] M. Egbor, T. Ansari, N. Morris, C.J. Green, P.D. Sibbons, Morphometric placental villous and vascular abnormalities in early- and late-onset pre-eclampsia with and without fetal growth restriction, BJOG 113(5) (2006) 580-9. [16] J.L. van der Merwe, D.R. Hall, C. Wright, P. Schubert, D. Grové, Are early and late preeclampsia distinct subclasses of the disease--what does the placenta reveal?, Hypertens Pregnancy 29(4) (2010) 457-67. [17] H. Valensise, B. Vasapollo, G. Gagliardi, G.P. Novelli, Early and late preeclampsia: two different maternal hemodynamic states in the latent phase of the disease, Hypertension 52(5) (2008) 873-80. [18] A.C. Staff, S.J. Benton, P. von Dadelszen, J.M. Roberts, R.N. Taylor, R.W. Powers, D.S. Charnock-Jones, C.W. Redman, Redefining preeclampsia using placenta-derived biomarkers, Hypertension 61(5) (2013) 932-42. [19] T. Chaiworapongsa, P. Chaemsaithong, L. Yeo, R. Romero, Pre-eclampsia part 1: current understanding of its pathophysiology, Nature reviews. Nephrology 10(8) (2014) 466-80. [20] S. Di Paolo, P. Volpe, G. Grandaliano, G. Stallone, A. Schena, P. Greco, L. Resta, L. Selvaggi, R. Cincione, F.P. Schena, L. Gesualdo, Increased placental expression of tissue factor is associated with abnormal uterine and umbilical Doppler waveforms in severe preeclampsia with fetal growth restriction, J.Nephrol. 16(5) (2003) 650-657. [21] Y. Teng, R. Jiang, Q. Lin, C. Ding, Z. Ye, The relationship between plasma and placental tissue factor, and tissue factor pathway inhibitors in severe pre-eclampsia patients, Thromb.Res. 126(1) (2010) e41-e45. [22] P. Redecha, R.N. van, D. Torry, G. Girardi, Pravastatin prevents miscarriages in mice: role of tissue factor in placental and fetal injury, Blood 113(17) (2009) 4101-4109. [23] Y. Xiong, Q. Zhou, F. Jiang, S. Zhou, Y. Lou, Q. Guo, W. Liang, D. Kong, D. Ma, X. Li, Changes of plasma and placental tissue factor pathway inhibitor-2 in women with preeclampsia and normal pregnancy, Thromb Res 125(6) (2010) e317-22.

9 | P a g e
[24] M. Ogawa, S. Yanoma, Y. Nagashima, N. Okamoto, H. Ishikawa, A. Haruki, E. Miyagi, T. Takahashi, F. Hirahara, Y. Miyagi, Paradoxical discrepancy between the serum level and the placental intensity of PP5/TFPI-2 in preeclampsia and/or intrauterine growth restriction: possible interaction and correlation with glypican-3 hold the key, Placenta 28(2-3) (2007) 224-32. [25] C. Gardiner, D.S. Tannetta, C.A. Simms, P. Harrison, C.W. Redman, I.L. Sargent, Syncytiotrophoblast microvesicles released from pre-eclampsia placentae exhibit increased tissue factor activity, PLoS.One. 6(10) (2011) e26313. [26] O. Erez, R. Romero, S.S. Kim, J.S. Kim, Y.M. Kim, D.E. Wildman, N.G. Than, S. Mazaki-Tovi, F. Gotsch, B. Pineles, J.P. Kusanovic, J. Espinoza, P. Mittal, M. Mazor, S.S. Hassan, C.J. Kim, Over-expression of the thrombin receptor (PAR-1) in the placenta in preeclampsia: a mechanism for the intersection of coagulation and inflammation, J.Matern.Fetal Neonatal Med. 21(6) (2008) 345-355. [27] Y. Zhao, K. Koga, Y. Osuga, M. Nagai, G. Izumi, M. Takamura, M. Harada, Y. Hirota, O. Yoshino, Y. Taketani, Thrombin enhances soluble Fms-like tyrosine kinase 1 expression in trophoblasts; possible involvement in the pathogenesis of preeclampsia, Fertil Steril 98(4) (2012) 917-21. [28] Q.T. Huang, J.H. Chen, L.L. Hang, S.S. Liu, M. Zhong, Activation of PAR-1/NADPH oxidase/ROS signaling pathways is crucial for the thrombin-induced sFlt-1 production in extravillous trophoblasts: possible involvement in the pathogenesis of preeclampsia, Cell Physiol Biochem 35(4) (2015) 1654-62. [29] K. de Boer, J.W. ten Cate, A. Sturk, J.J. Borm, P.E. Treffers, Enhanced thrombin generation in normal and hypertensive pregnancy, Am.J.Obstet.Gynecol. 160(1) (1989) 95-100. [30] Y. Cadroy, H. Grandjean, J. Pichon, R. Desprats, A. Berrebi, A. Fournie, B. Boneu, Evaluation of six markers of haemostatic system in normal pregnancy and pregnancy complicated by hypertension or pre-eclampsia, Br.J.Obstet.Gynaecol. 100(5) (1993) 416-420. [31] B. Pinheiro Mde, D.R. Junqueira, F.F. Coelho, L.G. Freitas, M.G. Carvalho, K.B. Gomes, L.M. Dusse, D-dimer in preeclampsia: systematic review and meta-analysis, Clin Chim Acta 414 (2012) 166-70. [32] A. Halligan, J. Bonnar, B. Sheppard, M. Darling, J. Walshe, Haemostatic, fibrinolytic and endothelial variables in normal pregnancies and pre-eclampsia, Br.J.Obstet.Gynaecol. 101(6) (1994) 488-492. [33] G. Krikun, S.T. Huang, F. Schatz, C. Salafia, C. Stocco, C.J. Lockwood, Thrombin activation of endometrial endothelial cells: a possible role in intrauterine growth restriction, Thromb Haemost 97(2) (2007) 245-53. [34] M.T. Vinnars, J. Nasiell, S. Ghazi, M. Westgren, N. Papadogiannakis, The severity of clinical manifestations in preeclampsia correlates with the amount of placental infarction, Acta Obstet Gynecol Scand 90(1) (2011) 19-25. [35] A. Kanfer, J.F. Bruch, G. Nguyen, C.J. He, F. Delarue, A. Flahault, C. Nessmann, S. Uzan, Increased placental antifibrinolytic potential and fibrin deposits in pregnancy-induced hypertension and preeclampsia, Lab Invest 74(1) (1996) 253-258. [36] E. Ferrazzi, G. Bulfamante, R. Mezzopane, A. Barbera, A. Ghidini, G. Pardi, Uterine Doppler Velocimetry and Placental Hypoxic-ischemic Lesion in Pregnancies with Fetal Intrauterine Growth Restriction, Placenta 20(5–6) (1999) 389-394. [37] D.J. Roberts, M.D. Post, The placenta in pre-eclampsia and intrauterine growth restriction, J Clin Pathol 61(12) (2008) 1254-60. [38] K.G. Pringle, K.L. Kind, A.N. Sferruzzi-Perri, J.G. Thompson, C.T. Roberts, Beyond oxygen: complex regulation and activity of hypoxia inducible factors in pregnancy, Hum Reprod Update 16(4) (2010) 415-31. [39] O. Nevo, N. Soleymanlou, Y. Wu, J. Xu, J. Kingdom, A. Many, S. Zamudio, I. Caniggia, Increased expression of sFlt-1 in in vivo and in vitro models of human placental hypoxia is mediated by HIF-1, Am J Physiol Regul Integr Comp Physiol 291(4) (2006) R1085-93.

10 | P a g e
[40] A. Rajakumar, H.M. Brandon, A. Daftary, R. Ness, K.P. Conrad, Evidence for the functional activity of hypoxia-inducible transcription factors overexpressed in preeclamptic placentae, Placenta 25(10) (2004) 763-9. [41] M. Hellgren, Hemostasis during normal pregnancy and puerperium, Semin.Thromb.Hemost. 29(2) (2003) 125-130. [42] A. Rosenkranz, M. Hiden, B. Leschnik, E.C. Weiss, D. Schlembach, U. Lang, S. Gallistl, W. Muntean, Calibrated automated thrombin generation in normal uncomplicated pregnancy, Thromb.Haemost. 99(2) (2008) 331-337. [43] A. Rousseau, R. Favier, D.P. Van, Elevated circulating soluble thrombomodulin activity, tissue factor activity and circulating procoagulant phospholipids: new and useful markers for pre-eclampsia?, Eur.J.Obstet.Gynecol.Reprod.Biol. 146(1) (2009) 46-49. [44] M.G. Macey, S. Bevan, S. Alam, L. Verghese, S. Agrawal, S. Beski, R. Thuraisingham, P.K. Maccallum, Platelet activation and endogenous thrombin potential in pre-eclampsia, Thromb.Res. (2009). [45] C.W. Redman, J. Bonnar, L. Beilin, Early platelet consumption in pre-eclampsia, BMJ 1(6111) (1978) 467-469. [46] M.L. Socol, C.P. Weiner, G. Louis, K. Rehnberg, E.C. Rossi, Platelet activation in preeclampsia, Am J Obstet Gynecol 151(4) (1985) 494-7. [47] I. Rakoczi, F. Tallian, S. Bagdany, I. Gati, Platelet life-span in normal pregnancy and pre-eclampsia as determined by a non-radioisotope technique, Thromb Res 15(3-4) (1979) 553-6. [48] S.L. Janes, P.M. Kyle, C. Redman, A.H. Goodall, Flow cytometric detection of activated platelets in pregnant women prior to the development of pre-eclampsia, Thromb.Haemost. 74(4) (1995) 1059-1063. [49] M. Kanat-Pektas, U. Yesildager, N. Tuncer, D.T. Arioz, G. Nadirgil-Koken, M. Yilmazer, Could mean platelet volume in late first trimester of pregnancy predict intrauterine growth restriction and pre-eclampsia?, J Obstet Gynaecol Res 40(7) (2014) 1840-5. [50] Y. Sato, H. Fujiwara, B.X. Zeng, T. Higuchi, S. Yoshioka, S. Fujii, Platelet-derived soluble factors induce human extravillous trophoblast migration and differentiation: platelets are a possible regulator of trophoblast infiltration into maternal spiral arteries, Blood 106(2) (2005) 428-35. [51] S. Roberge, Y. Giguere, P. Villa, K. Nicolaides, M. Vainio, J.C. Forest, P. von Dadelszen, D. Vaiman, S. Tapp, E. Bujold, Early administration of low-dose aspirin for the prevention of severe and mild preeclampsia: a systematic review and meta-analysis, Am J Perinatol 29(7) (2012) 551-6. [52] M.R. Holthe, T. Lyberg, A.C. Staff, L.N. Berge, Leukocyte-platelet interaction in pregnancies complicated with preeclampsia, Platelets. 16(2) (2005) 91-97. [53] A. Rajakumar, H.M. Michael, P.A. Rajakumar, E. Shibata, C.A. Hubel, S.A. Karumanchi, R. Thadhani, M. Wolf, G. Harger, N. Markovic, Extra-placental expression of vascular endothelial growth factor receptor-1, (Flt-1) and soluble Flt-1 (sFlt-1), by peripheral blood mononuclear cells (PBMCs) in normotensive and preeclamptic pregnant women, Placenta 26(7) (2005) 563-73. [54] H.D. Major, R.A. Campbell, R.M. Silver, D.W. Branch, A.S. Weyrich, Synthesis of sFlt-1 by platelet-monocyte aggregates contributes to the pathogenesis of preeclampsia, Am J Obstet Gynecol 210(6) (2014) 547.e1-7. [55] C. Gardiner, N.A. Redgrave, R.A. Dragovic, D.S. Tannetta, C.W.G. Redman, I.L. Sargent, Blood platelets interact with syncytiotrophoblast vesicles, Journal of Extracellular Vesicles 1(Supplement 1) (2012) 16-16. [56] D.S. Tannetta, K. Hunt, C.I. Jones, N. Davidson, C.H. Coxon, D. Ferguson, C.W. Redman, J.M. Gibbins, I.L. Sargent, K.L. Tucker, Syncytiotrophoblast Extracellular Vesicles from Pre-Eclampsia Placentas Differentially Affect Platelet Function, PloS one 10(11) (2015) e0142538. [57] K.A. Whigham, P.W. Howie, A.H. Drummond, C.R. Prentice, Abnormal platelet function in pre-eclampsia, Br J Obstet Gynaecol 85(1) (1978) 28-32. [58] L.A. Norris, N. Gleeson, B.L. Sheppard, J. Bonnar, Whole blood platelet aggregation in moderate and severe pre-eclampsia, Br J Obstet Gynaecol 100(7) (1993) 684-8.

11 | P a g e
[59] S.L. Janes, A.H. Goodall, Flow cytometric detection of circulating activated platelets and platelet hyper-responsiveness in pre-eclampsia and pregnancy, Clinical science 86(6) (1994) 731-9. [60] S. Ahlawat, H.P. Pati, N. Bhatla, L. Fatima, S. Mittal, Plasma platelet aggregating factor and platelet aggregation studies in pre-eclampsia, Acta Obstet Gynecol Scand 75(5) (1996) 428-31. [61] S. Kohli, S. Ranjan, J. Hoffmann, M. Kashif, E.A. Daniel, M.M. Al-Dabet, F. Bock, S. Nazir, H. Huebner, P.R. Mertens, K.D. Fischer, A.C. Zenclussen, S. Offermanns, A. Aharon, B. Brenner, K. Shahzad, M. Ruebner, B. Isermann, Maternal extracellular vesicles and platelets promote preeclampsia through inflammasome activation in embryonic trophoblast, Blood (2016). [62] V.M. Abrahams, I. Visintin, P.B. Aldo, S. Guller, R. Romero, G. Mor, A role for TLRs in the regulation of immune cell migration by first trimester trophoblast cells, J Immunol 175(12) (2005) 8096-104. [63] A.K. Gupta, P. Hasler, W. Holzgreve, S. Gebhardt, S. Hahn, Induction of neutrophil extracellular DNA lattices by placental microparticles and IL-8 and their presence in preeclampsia, Human immunology 66(11) (2005) 1146-54. [64] A. Gupta, P. Hasler, S. Gebhardt, W. Holzgreve, S. Hahn, Occurrence of neutrophil extracellular DNA traps (NETs) in pre-eclampsia: a link with elevated levels of cell-free DNA?, Ann N Y Acad Sci 1075 (2006) 118-22. [65] T.A. Fuchs, A. Brill, D. Duerschmied, D. Schatzberg, M. Monestier, D.D. Myers, Jr., S.K. Wrobleski, T.W. Wakefield, J.H. Hartwig, D.D. Wagner, Extracellular DNA traps promote thrombosis, Proc Natl Acad Sci U S A 107(36) (2010) 15880-5. [66] J. Etulain, K. Martinod, S.L. Wong, S.M. Cifuni, M. Schattner, D.D. Wagner, P-selectin promotes neutrophil extracellular trap formation in mice, Blood (2015). [67] J.F. Regal, K.E. Lillegard, A.J. Bauer, B.J. Elmquist, A.C. Loeks-Johnson, J.S. Gilbert, Neutrophil Depletion Attenuates Placental Ischemia-Induced Hypertension in the Rat, PloS one 10(7) (2015) e0132063. [68] A.K. Gupta, M.B. Joshi, M. Philippova, P. Erne, P. Hasler, S. Hahn, T.J. Resink, Activated endothelial cells induce neutrophil extracellular traps and are susceptible to NETosis-mediated cell death, FEBS Lett 584(14) (2010) 3193-7. [69] T.A. Fuchs, J.A. Kremer Hovinga, D. Schatzberg, D.D. Wagner, B. Lammle, Circulating DNA and myeloperoxidase indicate disease activity in patients with thrombotic microangiopathies, Blood 120(6) (2012) 1157-64. [70] S. Miyakis, M.D. Lockshin, T. Atsumi, D.W. Branch, R.L. Brey, R. Cervera, R.H. Derksen, P.G. De Groot, T. Koike, P.L. Meroni, G. Reber, Y. Shoenfeld, A. Tincani, P.G. Vlachoyiannopoulos, S.A. Krilis, International consensus statement on an update of the classification criteria for definite antiphospholipid syndrome (APS), J.Thromb.Haemost. 4(2) (2006) 295-306. [71] M. Empson, M. Lassere, J. Craig, J. Scott, Prevention of recurrent miscarriage for women with antiphospholipid antibody or lupus anticoagulant, The Cochrane database of systematic reviews (2) (2005) Cd002859. [72] L.S. Noble, W.H. Kutteh, N. Lashey, R.D. Franklin, J. Herrada, Antiphospholipid antibodies associated with recurrent pregnancy loss: prospective, multicenter, controlled pilot study comparing treatment with low-molecular-weight heparin versus unfractionated heparin, Fertil Steril 83(3) (2005) 684-90. [73] U.M. Fouda, A.M. Sayed, A.M. Abdou, D.I. Ramadan, I.M. Fouda, M.M. Zaki, Enoxaparin versus unfractionated heparin in the management of recurrent abortion secondary to antiphospholipid syndrome, Int J Gynaecol Obstet 112(3) (2011) 211-5. [74] S. Bouvier, E. Cochery-Nouvellon, G. Lavigne-Lissalde, E. Mercier, T. Marchetti, J.P. Balducchi, P. Mares, J.C. Gris, Comparative incidence of pregnancy outcomes in treated obstetric antiphospholipid syndrome: the NOH-APS observational study, Blood 123(3) (2014) 404-13. [75] G. Girardi, P. Redecha, J.E. Salmon, Heparin prevents antiphospholipid antibody-induced fetal loss by inhibiting complement activation, Nature medicine 10(11) (2004) 1222-6.
12 | P a g e
[76] M.J. Mulla, J.J. Brosens, L.W. Chamley, I. Giles, C. Pericleous, A. Rahman, S.K. Joyce, B. Panda, M.J. Paidas, V.M. Abrahams, Antiphospholipid antibodies induce a pro-inflammatory response in first trimester trophoblast via the TLR4/MyD88 pathway, American journal of reproductive immunology (New York, N.Y. : 1989) 62(2) (2009) 96-111. [77] C. Agostinis, P. Durigutto, D. Sblattero, M.O. Borghi, C. Grossi, F. Guida, R. Bulla, P. Macor, F. Pregnolato, P.L. Meroni, F. Tedesco, A non-complement-fixing antibody to beta2 glycoprotein I as a novel therapy for antiphospholipid syndrome, Blood 123(22) (2014) 3478-87. [78] V.M. Holers, G. Girardi, L. Mo, J.M. Guthridge, H. Molina, S.S. Pierangeli, R. Espinola, L.E. Xiaowei, D. Mao, C.G. Vialpando, J.E. Salmon, Complement C3 activation is required for antiphospholipid antibody-induced fetal loss, J Exp Med 195(2) (2002) 211-20. [79] E. Lefkou, A. Mamopoulos, T. Dagklis, C. Vosnakis, D. Rousso, G. Girardi, Pravastatin improves pregnancy outcomes in obstetric antiphospholipid syndrome refractory to antithrombotic therapy, J Clin Invest 126(8) (2016) 2933-40.





























