Embed Size (px)
Citation preview

Immunopharmacology:Immunosuppression in Organ
Transplanation
Prof D. A. Joyce Pharm 3320/3321
http://www.aihw.gov.au/WorkArea/DownloadAsset.aspx?id=10737422288
Organ Transplants, Australia
Organ Donors (2013)
Kidney 630
Liver 248
Heart 77
Lung 167
Pancreas 33
Bone Marrow 1,812 (2012)
http://www.anzdata.org.au/anzod/updates/anzod1989toCurrent.pdf
http://www.abmtrr.org/index.php/resources/data‐management/
Kidney

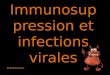
Inflammation and Immunity
Inflammation is what you see, clinically, in the pathological specimen or under the microscope. There are diagnostic “signs” at each level. EG, clinically: heat, redness, pain, swelling, disordered function
Immune response describes the events that take place during inflammation. Immunity results from an immune response.
Tuberculosis
Destroys & removes
foreign &damaged tissue, initiates repair
Chemicalmediators
Dilate blood vesselsFluid & protein extravasationRecruit more leukocytes
PainSwelling
Redness, Heat
A very rough summary of how an immune response to infection
causes inflammation
LeukocytesInfectiousagent
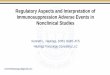
LymphoidMyelomonocytic
Erythroid
Megakaryocytic
Lymphoid lineage has left bone marrow by early postnatal life. Other lineages proliferate and differentiate in bone marrow through life
Haemopoetic Differentiation in Bone Marrow
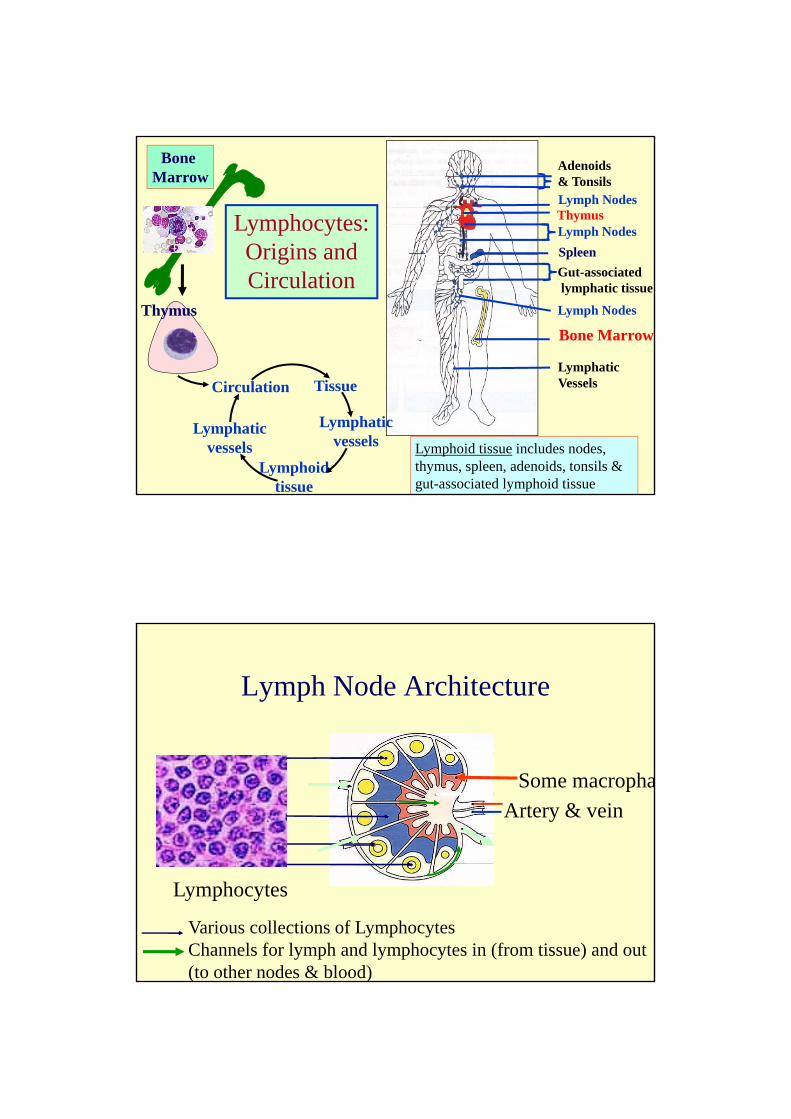
Bone Marrow
Gut-associatedlymphatic tissue
Lymph Nodes
LymphaticVessels
Lymph NodesThymus
Spleen
Adenoids& Tonsils
Lymph Nodes
TissueCirculation
Thymus
Bone Marrow
Lymphoidtissue
Lymphaticvessels
Lymphaticvessels
Lymphocytes: Origins and Circulation
Lymphoid tissue includes nodes, thymus, spleen, adenoids, tonsils & gut-associated lymphoid tissue
Lymph Node Architecture
Various collections of LymphocytesChannels for lymph and lymphocytes in (from tissue) and out (to other nodes & blood)
Lymphocytes
Artery & vein
Some macropha
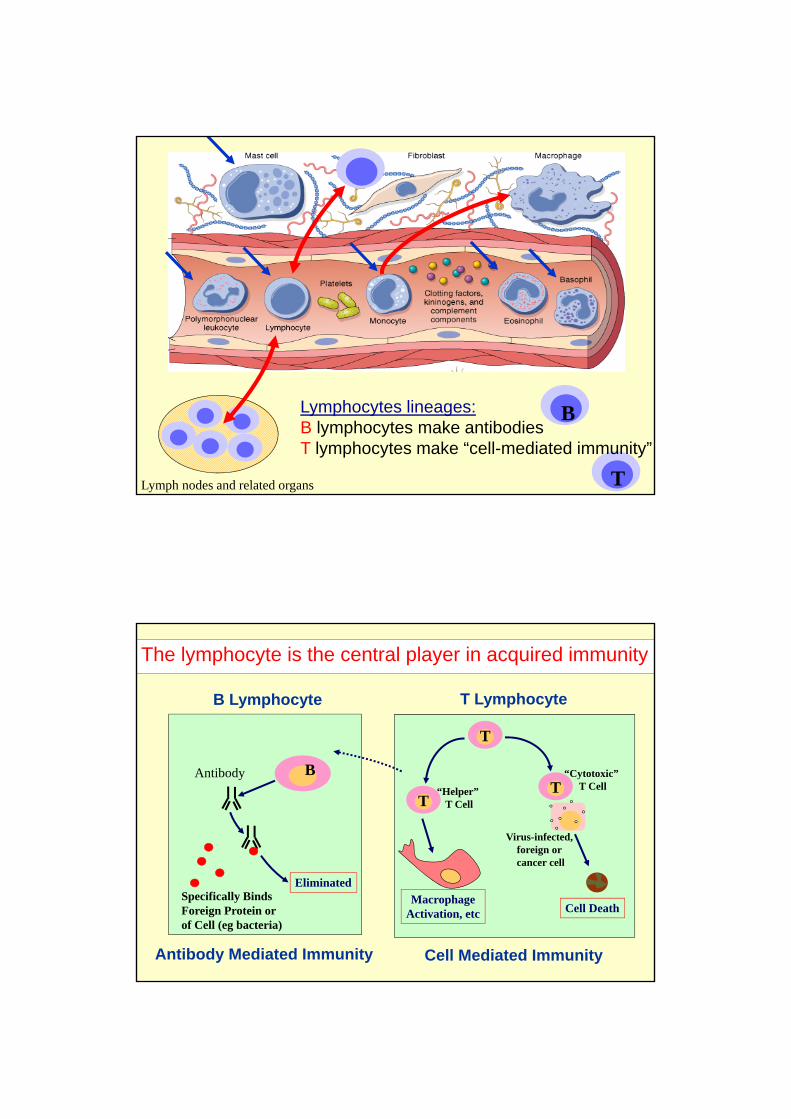
Lymph nodes and related organs T
Lymphocytes lineages:B lymphocytes make antibodiesT lymphocytes make “cell-mediated immunity”
B
T Lymphocyte
T
Cell Death
T
T
“Cytotoxic” T Cell
Virus-infected,foreign orcancer cell
MacrophageActivation, etc
“Helper” T Cell
BAntibody
EliminatedSpecifically BindsForeign Protein orof Cell (eg bacteria)
B Lymphocyte
Antibody Mediated Immunity Cell Mediated Immunity
The lymphocyte is the central player in acquired immunity

Somalia, 1979
1796
Acquired Immunity• Specific: to a foreign protein (antigen)
• Learned: takes days – weeks to learn.
• Remembered: can be recalled years later
1157 b.c.
An antigen-specific lymphocyte learns and remembers
Is it only infection that causes immunity and inflammation?
• Infections, acute and chronic: – viral - bacterial, – protozoal - parasitic
• Foreign material– Appropriate– Excessive (allergies, eg, allergic asthma)– Transplanted organ (“Allogeneic” transplant)
• Tissue injury: – trauma - burns, – surgery - radiation (eg, sunburn)
• Autoimmunity: abnormal inflammatory reaction to normal tissue

1. Prevention of rejection in organ transplantation
- suppression of an “appropriate” immune reaction to a foreign tissue (eg heart, kidney, lung)
2. Treatment of autoimmune diseases
- Suppression of an inappropriate immune reaction to a “self” tissue (eg lupus nephritis)
• Treatment of severe allergy
- Suppression of an inappropriate immune reaction to a foreign antigen (eg glucocorticoids for allergic asthma)
Why Suppress Acquired Immunity?
Suppressing the Immune Response to a Transplanted Organ:
Control of T-lymphocyte Clonal Expansion

T-Lymphocyte infiltration in chronic allograft rejection
Kidney
Artery in heart
Liver
Lung
Allograft antigen carried by antigen presenting cells via lymphatics to lymphoid tissue
Chronic Allograft Rejection: Role of T‐Lymphocytes
Allograft‐specific T‐lymphocytes return to attack allograft

Allograft‐derived Antigen
Specific T‐lymphocyte clonal expansion
Allograft Recognition and T‐Lymphocyte Clonal Expansion in Lymphoid Tissue
TT
T
T
T
TT
Allograft cell destruction Rejection
Antigen Processing Cell
T-Cell Receptor recognises processed antigen
Specific for the antigen, i.e. highly variable
Variability generated by gene rearrangement during clonal selection in the thymus
Antigen-presenting cell (APC)
T-lymphocyte
Processed antigen is presented, bound by a specific protein complex (HLA complex) on the APC surface
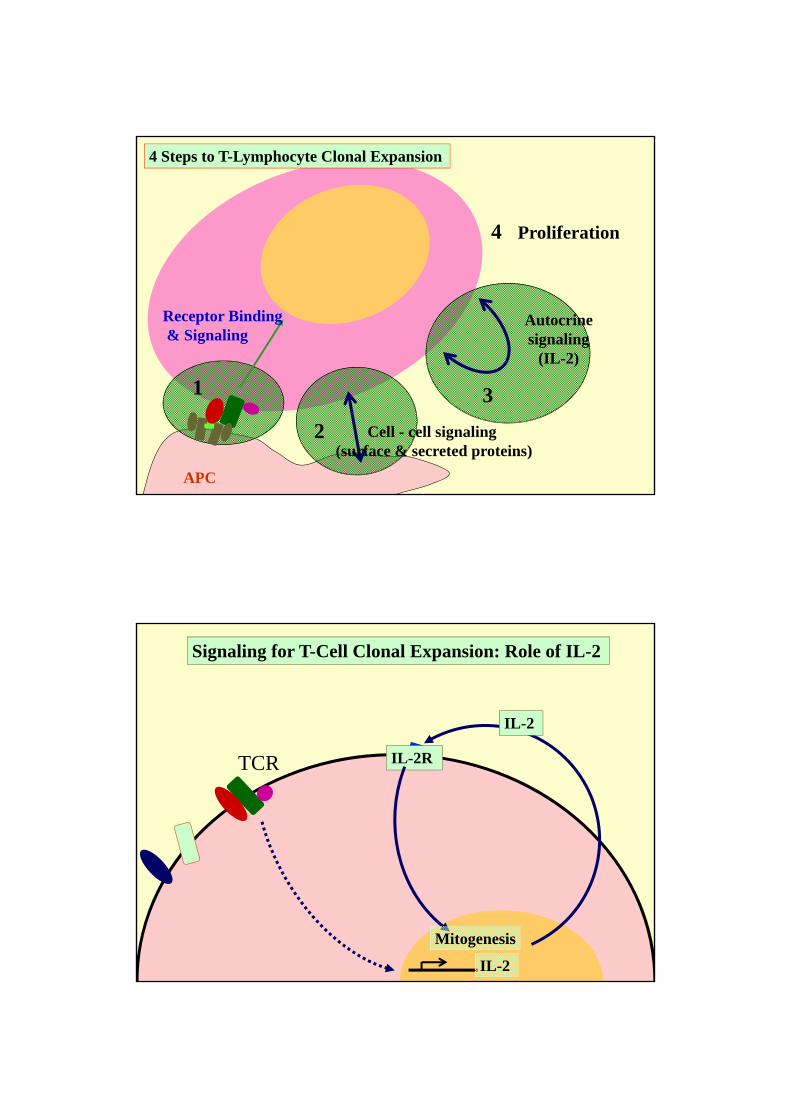
1
2
3
APC
Receptor Binding& Signaling
Cell - cell signaling(surface & secreted proteins)
Autocrinesignaling
(IL-2)
4 Proliferation
4 Steps to T-Lymphocyte Clonal Expansion
IL-2
IL-2R
IL-2
Mitogenesis
Signaling for T-Cell Clonal Expansion: Role of IL-2
TCR

IL‐2
IL‐2R
IL‐2
Mitogenesis
Anti‐CD3
mTOR inhibitorsSirolimusEverolimus
Mycophenolate
Drugs that Prevent IL‐2‐Driven T‐Cell Clonal Expansion
Calcineurin InhibitorsCyclosporinTacrolimus Azathioprine
Glucocorticoids
IL‐2
IL‐2R
IL‐2
Mitogenesis
Anti‐CD3
Calcineurin InhibitorsCyclosporinTacrolimus
Glucocorticoids
Prevent TCR signalingfor IL-2 gene transcription
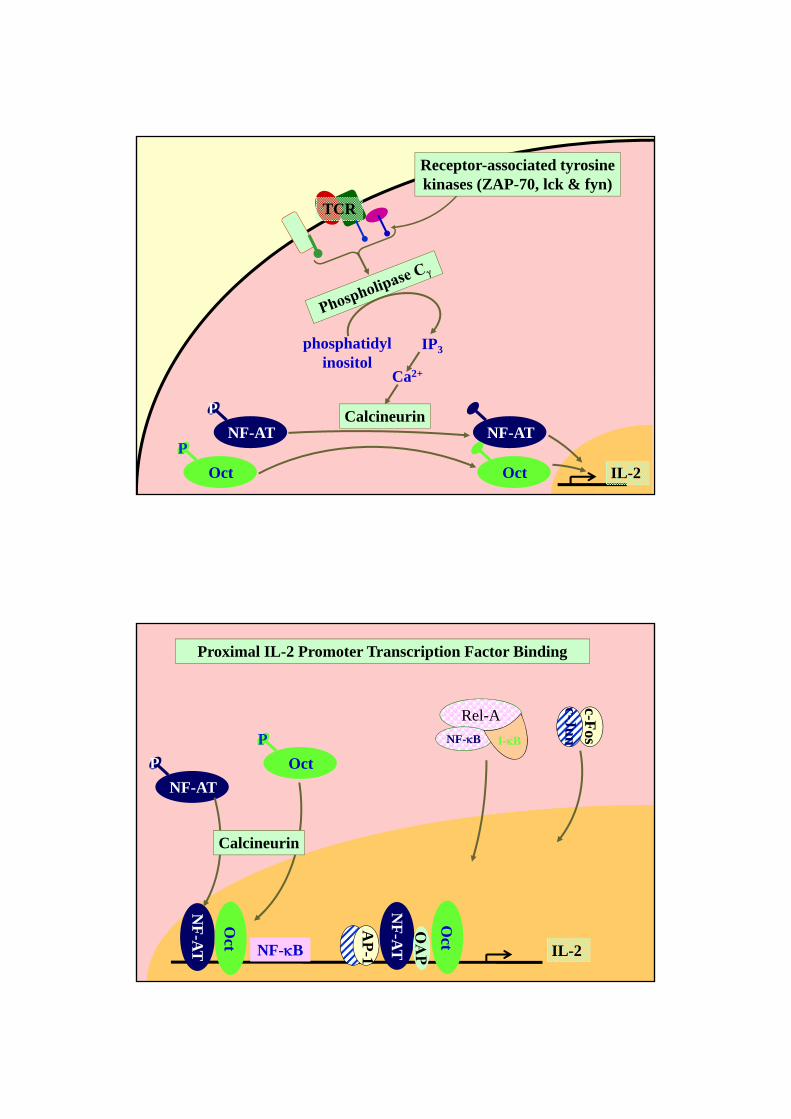
IL-2
TCR
Receptor-associated tyrosinekinases (ZAP-70, lck & fyn)
phosphatidylinositol
IP3
Ca2+
CalcineurinNF-AT
P
Oct
PNF-AT
Oct
IL-2
Proximal IL-2 Promoter Transcription Factor Binding
NF-AT
P Oct
P
NF
-AT
Oct
NF-B
NF
-AT
Oct
AP
-1
c-Fos
c-Jun
Calcineurin
Rel-A
NF-B I-B

Cyclosporin
NCH3
OH
Tacrolimus (FK506)
Fungal-derived macrolide
Fungal peptide
IL-2
Action of Cyclosporin or Tacrolimus
NF-AT
P Oct
P
NF
-AT
Oct
NF-B
NF
-AT
Oct
AP
-1
Calcineurin
Cyclo
Cyclophilin
Cyclo
Tac
FKBP
Tac
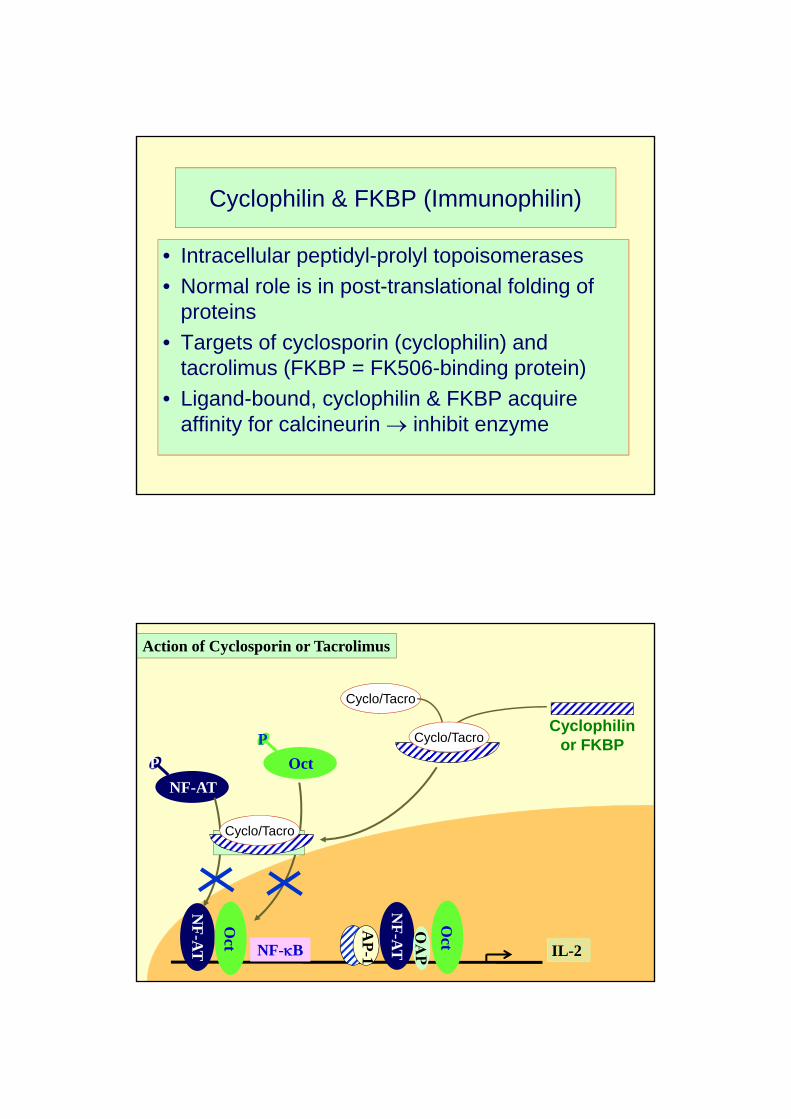
Cyclophilin & FKBP (Immunophilin)
• Intracellular peptidyl-prolyl topoisomerases
• Normal role is in post-translational folding of proteins
• Targets of cyclosporin (cyclophilin) and tacrolimus (FKBP = FK506-binding protein)
• Ligand-bound, cyclophilin & FKBP acquire affinity for calcineurin inhibit enzyme
IL-2
Action of Cyclosporin or Tacrolimus
NF-AT
P Oct
P
NF
-AT
Oct
NF-B
NF
-AT
Oct
AP
-1
Calcineurin
Cyclo/Tacro
Cyclophilinor FKBPCyclo/Tacro
Cyclo/Tacro

IL-2
Action of Cyclosporin or Tacrolimus
NF-AT
P Oct
P
NF-B
AP
-1
Calcineurin
Cyclo/Tacro
Cyclophilinor FKBPCyclo/Tacro
Cyclo/Tacro
Glucocorticoids
• Suppress IL-2 gene transcription
• Reduce IL-2 mRNA stability

Glucocorticoids
=O in cortisone
Hydrocortisone (cortisol)
**
F
PrednisolonePotent synthetic glucocorticoid
DexamethasoneVery potent glucocorticoid(Methylated & fluorinated)
Also many other potent synthetic glucocorticoids
*
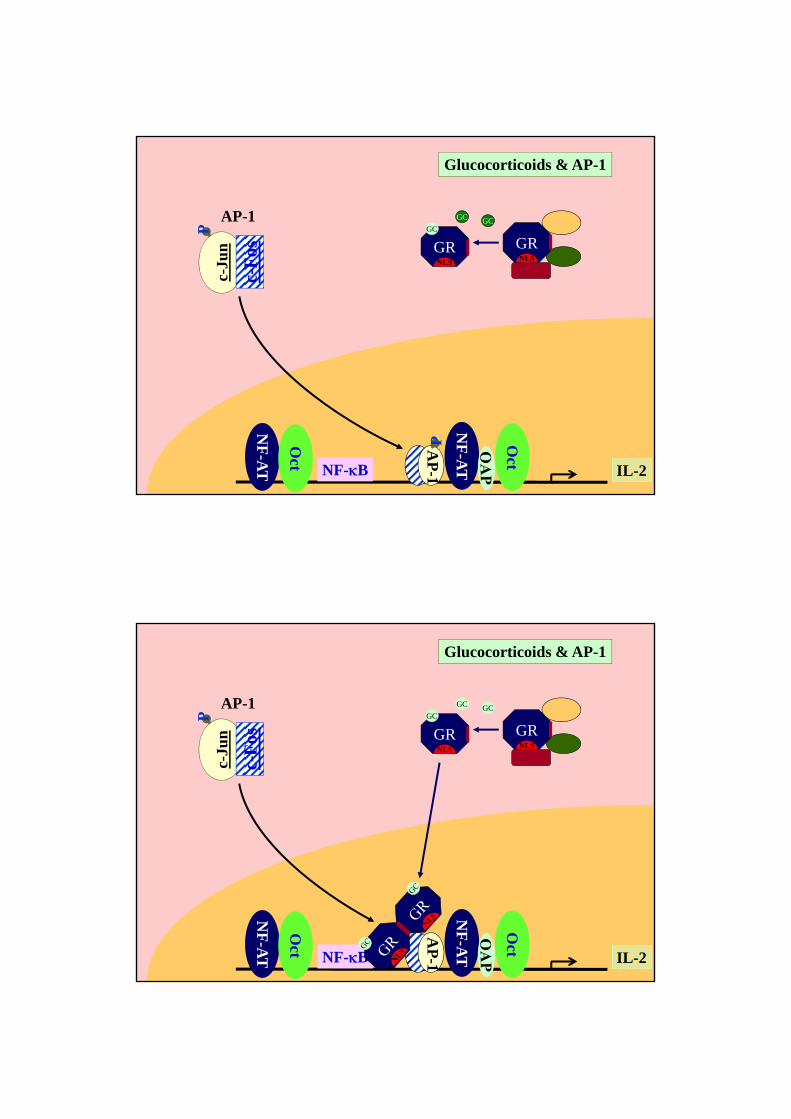
Steroid bound to circulating corticosteroid binding globulin
Steroid binds cytosolic glucocorticoid receptor, which translocates to nucleus
Steroid-receptor complex binds recognition sequences on promoter of responsive genes, stimulating transcription.

The Glucocorticoid Receptor (GR)
Ligand-binding domain
Regulatory domain: binds chaperones & other proteins
Zn fingers in DNA-binding domain
Transactivation domain: binds proteins that
activate transcription
Rang et al, Pharmacology, Elsevier
Glucocorticoid Receptor Activation
GRNLS
GCGC
GRNLS
GC
GRNLS
GC
GRNLS
GC
GRE
Cytoplasmic glucocorticoid
receptor & chaperone proteins
XXXXXXXXXXXXXGGTACAnnnTGTTCTXXXXXXXXXXXXX
Ligand binding releases chaperones & reveals nuclear localisation signal &
dimerisation site
Nuclear localisation signal allows recognition by nuclear pore complex
and access to nucleus
Receptor interacts with glucocorticoid response element (GRE) through Zinc
FingersTranscriptional
activation
2
3
1
4
5
IL-2
Glucocorticoids & AP-1
NF
-AT
Oct
NF-B
NF
-AT
Oct
AP
-1
GRNLS
GCGC
GRNLS
GCc-
Jun
P
c-F
os
AP-1
P
IL-2
Glucocorticoids & AP-1
NF
-AT
Oct
NF-B
NF
-AT
Oct
AP
-1
GRNLS
GCGC
GRNLS
GC
c-Ju
nP
c-F
os
AP-1

Cytoplasm
Nucleus
Leucine-zipped dimers
Rel/NF-B Family Transcription Factors
NF-B family includes– NF-B1 (p50)
– Rel-A (p65)
– NF-B2 (p52)
– c-Rel (p75)
– Rel-B (p68)
IB family includes– IB ,,,,
Rel-A
NF-B1 I-BComplexed to IB protein
Cytoplasm-resident, until activation
NF-B Signalling
Rel-A
NF-B I-B
Rel
-A
NF
-B
I-B Degradation
Cytoplasm
Nucleus
A C C GC T T C C T C CA GA T GA GC T C A T GGGT T T C T C CA C C A A GGA A GT T T T C C GC T GG
NF-B Binding Sequence
Gene Promoter
Cell Surface Receptor Activation
Phosphorylation of Serine 32 & 36 of I-B
Nuclear Localisation Signal on NF-B revealed
Binds NF-B-response element
2
3
1
4
5

IL-2
Glucocorticoids & NFB
NF
-AT
Oct
NF-B
NF
-AT
Oct
AP
-1
Rel-A
NF-B I-B
Rel
-A
NF
-B
GRNLS
GCGC
Glucocorticoids Induce IB Gene Transcription
Rel-A
NF-B I-B
GRNLS
GC
GRNLS
GC
I-B
I-B
Rel-A
NF-B
GGTACAnnnTGTTCT

c-Fos
c-Jun
IL-2
NF
-AT
Oct
NF-B
NF
-AT
Oct
AP
-1
Glucocorticoids & IL-2 Gene Transcription: Summary
GRNLS
GC
GRNLS
GC
Rel-A
NF-B I-B
Coding Region 3’ UTRPromoter
mRNA Synthesis
Coding
3’UTR
AAAAAAAAA
Poly-A
AU-rich region
IL-2
AcceleratedDegradation
IL-2 mRNA Degradationglucocorticoids

• Fungal-derived macrolides
• Structurally related to cyclosporine & tacrolimus
• Bind immunophilin FKBP and the complex targets a serine – threonine kinase “Mammalian Target of Rapamycin” (mTOR)
• Do not inhibit calcineurin
• Inhibit mitogenic response to IL-2 and other growth factors
For detailed pathways, see: http://www.biocarta.com/pathfiles/m_mTORPathway.asp
Sirolimus (Rapamycin) and Everolimus:targeting growth factor (incl IL-2) response
Sirolimus Everolimus
Sirolimus (Rapamycin) and Everolimus:targeting growth factor (incl IL-2) response

Prevent mitogenic response to IL-2 & other growth factors
Sirolimus & Everolimus
IL-2 & other growth factors
IL-2R & other growth factor receptors
Mitogenesis
TCR PI3Kinase/AKT pathway
mTORSir/Ever
Serine/threonine kinase
Translation of mRNA for cell-cycle progression proteins (eg. cyclin D1)
Degradation of p27 cell-cycle inhibitor
FKBP
Sir/Ever
CDK: cyclin-dependent kinase
mTOR
P27 degradation in late G1
Cyclin E
CDK2 p27
Cyclin E
CDK2
G0
G1
G2
S
M
CDK2/cyclin E complex inhibited by p27-CDK-inhibitor during G0 & G1
G1 S Transition
FKBP
Sir/Ever
Sir/Ever

For detailed pathways, see: http://www.biocarta.com/pathfiles/m_mTORPathway.asp
mTOR regulation of translation
mRNA’s for many labile cell-cycle regulating proteins have characteristic sequences or structures
mTOR has two targets that are particularly important in regulating translation of these mRNA’s
They are:
EIF-4E-binding protein-1, which releases eukaryotic initiation factor-4E when it is phosphorylated. EIF-4E contributes to initiation of translation
40-S ribosome subunit
Sirolimus – FKBP and everolimus – FKBP complexes inhibits these mTOR actions also
mTOR
mTOR
p70s6 KinasemTOR
40
FKBP
EIF-4E
40-S ribosome subunit
mTOR regulation of translation
mRNA
Cell-cycle proteins
Sir/Ever
Sir/Ever

Mycophenolate
• Fungal derived
• Inhibitor of de-novo guanosine monophosphate synthesis
• B and T cells depend on de-novo synthesis:-lack salvage pathway for guanine recovery
• Specific inhibition of DNA synthesis, RNA synthesis & other GTP or cGMP requiring pathways in lymphocytes
Ribose-5P + ATP
5-phosphoribosyl-1-pyrophosphate (PRPP)
Guanine Guanosine MP Inosine MP Adenosine MP
Salvage Pathway(deficient in T & B cells)
IMP dehydrogenase
Mycophenolate

CD3- protein of the TCR- contributes to signaling
APC
T
IL-2
Prevent activation of T-cell via TCRAnti-CD3 Antibody
T
CD3
IL-2
Anti-CD3 Antibody

IL-2
Anti-CD3
Mitogenesis
Sirolimus
Mycophenolate
IL-2
Summary:Preventing IL-2-Driven T-Cell Clonal Expansion
CyclosporinTacrolimusGlucocorticoids
Glucocorticoids
Clinical Pharmacology: Clinical Use of Immunosuppressive Drugs in
Preventing Transplant Rejection
The Clinical Problem• Inadequate immunosupression allows transplant rejection• Excessive immunosupression brings infection risk• Calcineurin and mTOR have widespread physiological
functions, so inhibition brings toxicity in various tissues• Drug effects relate to tissue exposure• The drugs have variable pharmacokinetics, obscuring the
relationship between doses and tissue exposure

Clinical Pharmacology: Main reasons of variable pharmacokinetics
• Cyclosporin, tacrolimus, sirolimus and everolimus are all eliminated largely by cytochrome P450 3A4 (CYP 3A4), which is subject to inhibition and induction by other drugs
• Cyclosporin, tacrolimus, sirolimus and everolimus are all also substrates for the ABC-family transporter, p-glycoprotein* in the gut, so are subject to absorption interactions. Especially relevant for cyclosporin.
• Mycophenolate is glururonidated in the liver. Glucuronides are excreted into the bile, reabsorbed and renally excreted. They may be retained in renal failure. De-conjugation by gut bacteria, which is normally inconsequential, may then allow accumulation of the parent mycophenolate.
* aka multi-drug resistance transporter-1; PGP/MDR-1
Improving the Risk-Benefit Ratio: Multiple Drug Targets
• Typically, two or more drug are used together, at doses less than would be needed individually to prevent rejection– Additive efficacy
– Different toxicity
EG: sirolimus or mycophenolate + low dose calcineurin inhibitor + low dose prednisolone during maintenance

Optimising Tissue Exposure: Therapeutic Drug Monitoring
• Tacrolimus, sirolimus, everolimus have long t½ . Pre-dose
blood concentration (ie, trough, also called “C0”) provide
good guide to tissue exposure
• Cyclosporin AUC predicts response & toxicity, but very
variable absorption, so C0 is a poor predictor of AUC. C2 is
a better predictor
0
500
1000
1500
2000
0 4 8 12 16 20 24
Time – hours
C2 C0
Cyclosporin µg/L
AUC0‐4
Mycophenolate TDMMPA
MPA glucuronides
Biliary excretionGut hydrolysis
MPA
MPA reabsorbed
More variable relationship between C0 (C12) and AUC
Figurski et al. Ther Drug Monit 2009;31:717–726