Embed Size (px)
Citation preview

C A n A d i A n V i s i o n f o r r h e u m A t o l o g y
In Supportive Care Oncology
I N S I D E T H I S I S S U E
RITUXIMAB IN RA TREATMENT Demonstrated efficacy of rituximab in patients failing TNF inhibitors
TOCILIZUMAB IN RA TREATMENT Studies show tocilizumab is effective and safe long-term
JUVENILE IDIOPATHIC ARTHRITISCatch-up growth in JIA and management of uveitis
VASCULITISEfficacy of rituximab from induction to maintenance
Interviews with Dr. Christian Pagnoux, Dr. Loic Guillevin, Dr. Edward Keystone, and Dr. Mark Genovese
www.newevidence.com
New Evidence in Rheumatology is an independent medical news reporting service providing educational updates on current medical events. Views expressed are those of the participants and do not necessarily reflect those of the publisher or the sponsor. Support for development and distribution of this report was provided by Hoffmann-La Roche Rheumatology. Any therapies mentioned in this report should be used in accordance with the recognized prescribing information. No claims or endorsements are made for any products, uses, or doses presently under investigation. Information provided herein is not intended to serve as the sole basis for individual care. Our objective is to facilitate understanding of current trends in rheumatology for physicians and allied healthcare providers.
PUBLICATIONS MAIL AGREEMENT NO. 41495516 RETURN UNDELIVERABLE CANADIAN ADDRESSES TO
NEW EVIDENCE 2645 BLOOR ST. WEST, SUITE 501
TORONTO ON M8X 1A3
Choosing the Right Fit Illuminating Treatment Alternatives
Number 9 • January 2013

C A n A d i A n V i s i o n f o r r h e u m A t o l o g y
In Supportive Care Oncology
I N S I D E T H I S I S S U E
RITUXIMAB IN RA TREATMENT Demonstrated efficacy of rituximab in patients failing TNF inhibitors
TOCILIZUMAB IN RA TREATMENT Studies show tocilizumab is effective and safe long-term
JUVENILE IDIOPATHIC ARTHRITISCatch-up growth in JIA and management of uveitis
VASCULITISEfficacy of rituximab from induction to maintenance
Interviews with Dr. Christian Pagnoux, Dr. Loic Guillevin, Dr. Edward Keystone, and Dr. Mark Genovese
www.newevidence.com
New Evidence in Rheumatology is an independent medical news reporting service providing educational updates on current medical events. Views expressed are those of the participants and do not necessarily reflect those of the publisher or the sponsor. Support for development and distribution of this report was provided by Hoffmann-La Roche Rheumatology. Any therapies mentioned in this report should be used in accordance with the recognized prescribing information. No claims or endorsements are made for any products, uses, or doses presently under investigation. Information provided herein is not intended to serve as the sole basis for individual care. Our objective is to facilitate understanding of current trends in rheumatology for physicians and allied healthcare providers.
PUBLICATIONS MAIL AGREEMENT NO. 41495516 RETURN UNDELIVERABLE CANADIAN ADDRESSES TO
NEW EVIDENCE 2645 BLOOR ST. WEST, SUITE 501
TORONTO ON M8X 1A3
Choosing the Right Fit Illuminating Treatment Alternatives
Number 9 • January 2013

New Evidence in Rheumatology | January 2013 1
In Supportive Care OncologyPublisherPaul Borlinha
Managing DirectorAnna Christofides, MSc, RD
Medical WritersWissam Assaily, PhD
Ghada Kurban, MSc, PhD Anna Christofides, MSc, RD
EditorsLeonie Bedford Troy D. Borlinha
Creative DirectorJobet Dimaculangan
Art DirectorAndrew Oyen
Website DesignRonaji Naranjo
Website DevelopmentXinyu Pu
New Evidence in Rheumatology is published by New Evidence
2645 Bloor St. West, Suite 501 Toronto, Ontario M8X 1A3
Correspondence should be addressed to:
New Evidence 2645 Bloor St. West, Suite 501
Toronto, Ontario M8X 1A3 fax: 416-503-1927
e-mail: [email protected] website: www.newevidence.com
To join our mailing list or to request back issues, please contact us by mail,
fax: 416-503-1927, or e-mail: [email protected]
New Evidence in Rheumatology is also available online at www.newevidence.com
Canada Post Canadian Publications Mail Product Sales Agreement
Number 41495516
New Evidence in Rheumatology is a publication
for Canadian rheumatology healthcare professionals. Our journal
provides rheumatology specialists with scientific data from research
presented at international and Canadian rheumatology confer-
ences. A special feature of the journal, the Canadian perspective,
gives key opinion leaders a forum to discuss recent developments
in rheumatology and to comment on how these advances may
shape Canadian clinical practice. In addition, the investigator
commentary sections provide information on key clinical studies
from interviews with principal investigators. New Evidence also
publishes discussion and expert opinion papers on timely topics
of interest to rheumatologists in Canada.
Our January 2013 issue presents coverage of the 2012 American
College of Rheumatology (ACR)/Association of Rheumatology
Health Professionals (ARHP) Annual Scientific Meeting held in
Washington, D.C., on November 9–14, 2012. This issue focuses
on the long-term efficacy and safety of biologics in rheumatoid
arthritis, treatment alternatives in patients with inadequate
responses to tumour necrosis factor inhibitors, and advances
in the treatment and management of vasculitis and juvenile
idiopathic arthritis. We would like to thank Dr. Majed Khraishi,
Dr. Earl Silverman, Dr. Janet Pope, and Dr. Christian Pagnoux for
their Canadian perspectives. We would also like to thank Dr. Edward
Keystone, Dr. Mark Genovese, Dr. Christian Pagnoux, and Dr. Loïc
Guillevin for their investigator commentaries.
We invite you to visit our website at www.newevidence.com
for the online version of New Evidence and more reports on
current research. Slide presentations on various topics are available
for download.
www.newevidence.com
Cert no. SW-COC-003253

2 New Evidence in Rheumatology | January 2013
Contents
Tocilizumab in Rheumatoid Arthritis Treatment
8
Tocilizumab is Safe and Effective Over the Long Term in Patients with Rheumatoid Arthritis
• Long-term efficacy of tocilizumab monotherapy in patients with rheumatoid arthritis who were previously methotrexate naive or methotrexate free for six months (Jones G, et al. ACR 2012:454)
• Long-term safety of tocilizumab in patients with rheumatoid arthritis and a mean treatment duration of 3.7 years (Genovese, MC, et al. ACR 2012:1640)
• Safety and efficacy of subcutaneous tocilizumab versus intravenous tocilizumab in combination with traditional DMARDs in patients with moderate-to-severe rheumatoid arthritis (Burmester GR, et al. ACR 2012:2545)
• Lower than expected levels of DMARD acquisition immediately before and following biologic initiation in patients with rheumatoid arthritis (Choquette D, et al. ACR 2012:1841)
• Tocilizumab monotherapy compared with adalimumab monotherapy in patients with rheumatoid arthritis: results of a 24-week study (Kavanaugh A, et al. ACR 2012:772)
Canadian perspective by Dr. Majed Khraishi
Rituximab in Rheumatoid Arthritis Treatment
26
Rituximab is More Effective than Abatacept and Alternative Tumour Necrosis Factor Inhibitors (TNF-Is) in Patients Who Have Failed TNF-Is
• Factors influencing choice of rituximab versus an alternative TNF inhibitor following TNF inhibitor failure in patients with rheumatoid arthritis: sub-analysis of a global, observational comparative effectiveness study (Finckh A, et al. ACR 2012:456)
• Seropositive patients with rheumatoid arthritis who had an inadequate response to TNF inhibitors achieve improved clinical effectiveness after switching to rituximab versus switching to an alternative TNF inhibitor (Rubbert-Roth A, et al.
ACR 2012:467)
• Long-term safety of rituximab: 10-year follow-up in the rheumatoid arthritis global clinical trial program (van Vollenhoven RF,
et al. ACR 2012:459)
• Rituximab for the treatment of rheumatoid arthritis: treatment effectiveness in the CORRONA database (Harrold L. et al.
ACR 2012:464)
• Rituximab versus abatacept in patients with rheumatoid arthritis and an inadequate response to prior biologic therapy: a retrospective, single-centre study (Keystone E, et al.
ACR 2012:1299)
Canadian perspective by Janet PopeInvestigator Commentary
24
An interview with Dr. Mark Genovese on the long-term safety of tocilizumab in patients with rheumatoid arthritis
ACR/ARHP

New Evidence in Rheumatology | January 2013 3
Juvenile Idiopathic Arthritis
42
Tocilizumab Therapy is Effective in Systemic Juvenile Idiopathic Arthritis and Polyarticular JIA
• Catch-up growth during tocilizumab therapy for systemic juvenile idiopathic arthritis: two-year data from a phase III clinical trial (De Benedetti F, et al. ACR 2012:760)
• Efficacy and safety of tocilizumab in patients with polyarticular juvenile idiopathic arthritis: data from a phase III trial (Brunner H,
et al. ACR 2012:1597)
• Clinical course and outcomes of children with juvenile idiopathic arthritis-associated uveitis and idiopathic uveitis (Angeles-Han S, et al. ACR 2012:2005)
• A new measure of visual function for children with juvenile idiopathic arthritis-associated uveitis (Angeles-Han S, et al.
ACR 2012:1155)
Canadian perspective by Dr. Earl Silverman
Vasculitis
52
The Multifaceted Role of Rituximab in ANCA-Associated Vasculitis: From Induction to Maintenance
• Long-term outcome of patients with granulomatosis with polyangiitis (Wegener’s) treated with rituximab (Azar L, et al.
ACR 2012:1544)
• Rituximab versus azathioprine for maintenance in ANCA-associated vasculitis (Guillevin L, et al. ACR 2012:1652)
• Rituximab for ANCA-associated vasculitis: a meta-analysis of randomized trials (Mejia C, et al. ACR 2012:1543)
Canadian perspective by Dr. Christian Pagnoux
Investigator Commentary
40
An Interview with Dr. Edward Keystone on his retrospective single-centre study comparing rituximab with abatacept in patients with rheumatoid arthritis who had an inadequate response to prior biologic therapy
Investigator Commentaries
64
An Interview with Dr. Christian Pagnoux on the MAINRITSAN study that examined the efficacy and safety of rituximab compared with azathioprine for maintenance in antineutrophil cytoplasmic antibodies (ANCA)-associated vasculitis
An Interview with Dr. Loïc Guillevin on the MAINRITSAN study that examined the efficacy and safety of rituximab compared with azathioprine for maintenance in antineutrophil cytoplasmic antibodies (ANCA)-associated vasculitis
ACR/ARHP

4 New Evidence in Rheumatology | January 2013
ContributorsCanadian Perspectives
Janet Pope, MD, MPH, FRCPCDr. Janet Pope is currently Program Director and Division Head in Rheu-matology at St. Joseph’s Hospital in London, Ontario, and Professor of Medicine, Division of Rheumatology and Division of Epidemiology and
Biostatistics at the University of Western Ontario. She is Vice President of the Canadian Network for Improved Outcomes in Systemic Lupus Erythematosus and an investigator in the Canadian Scleroderma Research Group. Dr. Pope is also on the executive of the Canadian Rheumatology Research Consortium, and is a member of the Scleroderma Clinical Trials Consortium and the Canadian Arthritis Network. Her research includes epidemiologic studies in scleroderma, including outcome measurement, clinical trials, and disease manifestations. She also has an interest in hormonal changes in rheumatic diseases, outcomes in lupus, and biologic therapies in rheumatoid arthritis.
Earl Silverman, MD, FRCPCDr. Earl Silverman is a Staff Rheu-matologist at The Hospital for Sick Children (SickKids) and is Director of the Paediatric Lupus Clinic. He is also a Senior Associate Scientist in the Physiology & Experimental
Medicine program at SickKids Research Institute and a Professor of Paediatrics & Immunology at the University of Toronto. Currently, he is the only Canadian advisor to the Arthritis Panel at the U.S. Food and Drug Administration. Dr. Silverman’s major interests are in pediatric systemic lupus erythematosus (SLE) and the etiology of neonatal lupus erythematosus (NLE). He is currently the pediatric investigator on a Canadian-wide study of pediatric- and adult-onset SLE. In addition to his clinical interests, Dr. Silverman is an active member in many national and international organizations including the Childhood Arthritis and Rheumatology Research Alliance, the Paediatric Rheumatology International Trials Organization, the lupus section of the American College of Rheumatology, and the Canadian Rheumatology Research Consortium.
Christian Pagnoux, MD, MPH, MScTrained in France, Dr. Christian Pagnoux graduated from Tours Medicine University in 1995 and completed his postgraduate training in internal medicine and clinical immunology at Paris-Descartes Uni-
versity in 2002. He also obtained a master’s degree in advanced immunology from the Pasteur Institute and another in methodology of clinical trials from the Diderot University (both in Paris). He has served as Vice President of the French Vasculitis Study Group (FVSG) since 2003 and continues to be involved as principal investigator or co-investigator in several therapeutic trials and cohort studies in vasculitis conducted by FVSG or the European Vasculitis Study Group. He recently completed a two-year clinical fellowship at Mount Sinai Hospital and the University Health Network (Toronto) that was partially funded by the Vasculitis Clinical Research Consortium and was subsequently appointed a full-time faculty member in the Division of Rheumatology at Mount Sinai Hospital in September 2012. Dr. Pagnoux founded CanVasc, the Canadian network for research on vasculitides, whose main objectives are to help conduct studies in the area of vasculitis, provide support and educational materials for physicians and trainees across Canada, and optimize patient care. He has written more than 100 peer-reviewed publications and several textbook chapters on vasculitis.
Majed Khraishi, MB, BCH., FRCPCDr. Majed Khraishi is a Clinical Professor of Medicine (Rheumatology) at Memorial University of Newfound-land (MUN) and the Medical Director of Rheumatology at Nexus Clinical Research in St. John’s, Newfoundland.
He graduated from Ain Shams University in Egypt after which he completed his internal medicine residency at MUN. After practising as a general internist for two years, he completed a fellowship in rheumatology at the University of Toronto. Since 1991, he has been a practising rheumatologist in St. John’s. Dr. Khraishi has a large clinical practice and is also involved in medical education and clinical research. He spent a sabbatical at Stanford University from 1995 to 1996 researching the gastro-intestinal adverse events of nonsteroidal anti-inflammatory drugs in rheumatoid arthritis (RA). His main interests are the therapeutics of RA, osteoarthritis (OA), and psoriatic arthritis. He has been involved as a principal investigator in over 60 pharmaceutical-sponsored therapeutic clinical studies (phase II, III, IV) in RA, OA, osteoporosis, psoriatic arthritis, and chronic pain. Many of these studies involved the use of biological agents.

New Evidence in Rheumatology | January 2013 5
Edward Keystone, MD, FRCPCDr. Edward Keystone is a Professor of Medicine at the University of Toronto, and a Senior Consultant in Rheumatology at Mount Sinai Hospital, Toronto. He is the Chair of the Canadian Rheumatology
Research Consortium, a national network of academic and community rheumatologists devoted to enhancing the scope and efficiency of clinical trials in Canada. Dr. Keystone founded the Arthritis and Autoimmunity Research Centre, a multidisciplinary centre devoted to epidemiological and translational research studies in autoimmune diseases at the University Health Network, Toronto. In 2003, he also established The Rebecca Macdonald Centre for Arthritis and Autoimmune Disease, a centre devoted to research into genomics, therapeutics, and outcomes in autoimmune inflammatory joint disease. He is the author of more than 180 peer-reviewed papers and book chapters, and has been the recipient of numerous teaching awards and honours, including the Senior Investigator Award of the Canadian Rheumatology Association and most recently, at ACR/ARHP 2008, the American College of Rheumatology’s Grand Master Award.
Mark Genovese, MD, FRCPCDr. Mark Genovese is a Professor of Medicine and Co-Chief of the Division of Immunology and Rheu-matology at Stanford University Medical Center. Dr. Genovese has established a clinical research program
that focuses on bench-to-bedside translational medicine in autoimmune diseases. He has designed and participated in many investigator-initiated studies and multicentre trials investigating novel therapies and therapeutic strategies for the treatment of autoimmune diseases and arthritis. In addition, he collaborates with several other investigators on studies of biomarkers, chemokines, cytokines, and cell surface markers associated with disease progression and response to therapy. Since joining the faculty at Stanford, Dr. Genovese has served as an editor for the textbook Primary Care Rheumatology and as an associate editor for Kelley’s Essentials of Internal Medicine. Dr. Genovese is a reviewer for numerous medical journals, a board member of the Stanford Clinical Translational Research Unit, the recipient of a Center of Immunology at Stanford clinical scholars’ award, and the 2008 recipient of the American College of Rheumatology Henry Kunkel award.
Loïc Guillevin, MDDr. Loïc Guillevin is a Professor of Medicine and Therapeutics, Head of the Department of Internal Medicine, Cochin Hospital, Paris Descartes University, Sorbonne Paris Cité and Head of the National Referral Centre for Rare Autoimmune and Systemic diseases, Vasculitis and Scleroderma.
Dr. Guillevin is also the Coordinator of the French Vasculitis Study Group. He is a member of several national and inter-national scientific society boards and is involved with several interest groups that focus on systemic and autoimmune diseases, and hemapheresis. He is president of the French committee for clinical research and President of the French National Society of Internal Medicine. Dr. Guillevin has published more than 750 scientific and teaching papers, and published or participated in the preparation of several scientific books. He is a fellow of the Royal College of Physicians, a fellow of the European Federation of Internal Medicine, and a member of the National Academy of Medicine.
Christian Pagnoux, MD, MPH, MScTrained in France, Dr. Christian Pagnoux graduated from Tours Medicine University in 1995 and completed his postgraduate training in internal medicine and clinical immunology at Paris-Descartes Uni-
versity in 2002. He also obtained a master’s degree in advanced immunology from the Pasteur Institute and another in methodology of clinical trials from the Diderot University (both in Paris). He has served as Vice President of the French Vasculitis Study Group (FVSG) since 2003 and continues to be involved as principal investigator or co-investigator in several therapeutic trials and cohort studies in vasculitis conducted by FVSG or the European Vasculitis Study Group. He recently completed a two-year clinical fellowship at Mount Sinai Hospital and the University Health Network (Toronto) that was partially funded by the Vasculitis Clinical Research Consortium and was subsequently appointed a full-time faculty member in the Division of Rheumatology at Mount Sinai Hospital in September 2012. Dr. Pagnoux founded CanVasc, the Canadian network for research on vasculitides, whose main objectives are to help conduct studies in the area of vasculitis, provide support and educational materials for physicians and trainees across Canada, and optimize patient care. He has written more than 100 peer-reviewed publications and several textbook chapters on vasculitis.
Investigator Commentaries

New Evidence in Rheumatology | January 2013 7
ACR/ARHP2012 Annual Scientific Meeting
Welcome to the New Evidence coverage of the 2012 American College of Rheumatology (ACR) and the Association of Rheumatology Health Professionals (ARHP) annual meeting held in Washington, D.C., from November 9–14. ACR is a premiere platform for the exchange of scientific and clinical information on rheumatic diseases. 2012 marks ACR’s 76th consecutive year, with over 16,000 attendees from around the world participating at the meeting in Washington.
Rheumatoid arthritis (RA) is a disease that requires long-term therapy. Long-term exposure of patients to first- and second-line therapies, which include disease-modifying antirheumatic drugs and tumour necrosis factor inhibitors, often results in inadequate responses (IR). Choosing the right fit from the available treatment alternatives is a major challenge in RA. Recent advances have mitigated this challenge by adding new options to standard treatments and exploring the use of alternative medications earlier in the treatment algorithm. Our ACR 2012 issue explores this with studies that investigate head-to-head comparisons of biologics in patients with an IR to prior therapy and the factors that help determine appropriate treatment choices. In addition, a new treatment for patients with polyarticular juvenile arthritis, long-terms safety studies on biologics in RA, and progress in the treatment of vasculitis are presented. Included in this issue are investigator commentaries and Canadian perspectives that provide insight into important findings and their impact on clinical practice.
We hope you enjoy this issue of New Evidence and look forward to seeing you at the next ACR conference in San Diego, California.
8 New Evidence in Rheumatology | January 2013
Interleukin-6 (IL-6) is a powerful proinflammatory cytokine with many important functions that include promoting the differentiation of pre-B cells to antibody-producing B cells and regulating the balance of regulatory T cells (Treg) to helper T cells (Th17).1 The dysregulation of IL-6 production leading to an imbalance between Treg and Th17 cells is thought to be the underlying cause responsible for the pathology of rheumatoid arithritis (RA).
Several short-term clinical trials have shown tocilizumab to be very effective both as monotherapy and in combination with methotrexate.2 Data on the long- term safety and efficacy of tocilizumab monotherapy treatment, however, are limited. The long-term five-year extension study, STREAM, published in 2011 by Nishimoto et al., was the first to demonstrate the long-term efficacy and safety of tocilizumab monotherapy in patients with RA.3 At ACR 2012 two more studies addressed whether the long-term efficacy of tocilizumab monotherapy or tocilizumab in combination with disease-modifying antirheumatic drugs (DMARDs) can be maintained after an adequate response has been achieved. These studies also addressed whether or not safety profiles remained stable.
At ACR 2012, investigators presented data on the long-term safety and efficacy of tocilizumab treatments in RA, the safety and efficacy of tocilizumab monotherapy compared with adalimumab, the safety and efficacy of a subcutaneous (sc) formulation of intravenous (iv)
tocilizumab, and an examination of noncompliance of patients taking DMARDs alongside biologics. This article reports on five presentations given at ACR:
• A long-term extension study on patients in the AMBITION (Actemra versus Methotrexate double-Blind Investigative Trial In mONotherapy) trial that examined the long-term safety and efficacy of tocilizumab monotherapy. The study demonstrated that tocilizumab monotherapy remained safe and effective over the 240 weeks of the study period.
• A long-term study further exploring the safety of more than one dose of tocilizumab therapy in five phase III clincal trials over a period of 3.7 years. The study confirmed that the safety profile remained stable over 3.7 years and that no new safety signals were identified.
• A phase IV study on the efficacy and safety of tocilizumab monotherapy vs. adalimumab. The study demonstrated that tocilizumab was not only more effective, but was also just as safe as adalimumab in reducing symptoms in patients with RA.
• A study on the safety and efficacy of novel tocilizumab sc vs. tocilizumab iv. Tocilizumab sc was shown to be as safe and effective as tocilizumab iv.
• An examination of DMARD aquisition by patients before and after biologic intitiation. The study showed a lower than expected DMARD aquisition and addressed how this could be mitigated.
Tocilizumab is Safe and Effective Over the Long Term in Patients with Rheumatoid Arthritis
References: 1. Kimura A, Kishimoto T. IL-6: regulator of Treg/Th17 balance. Eur J Immunol 2010;40:1830–5. 2. Ogata A, Hirano T, Hishitani Y, et al. Safety and efficacy of tocilizumab for the treatment of rheumatoid arthritis. Clin Med Insights Arthritis Musculoskelet Disord 2012;5:27–42. 3. Nishimoto N, Miyasaka N, Yamamoto K, et al. Long-term safety and efficacy of tocilizumab, an anti-IL-6 recep-tor monoclonal antibody, in monotherapy, in patients with rheumatoid arthritis (the STREAM study): evidence of safety and efficacy in a 5-year extension study. Ann Rheum Dis 2009;68:1580–4.
Tocilizumab in Rheumatoid Arthritis Treatment

New Evidence in Rheumatology | January 2013 9
ACR/ARHP
Jones G, et al. ACR 2012:454
Long-term efficacy of tocilizumab monotherapy in patients with RA who were previously methotrexate naive or methotrexate free for six months
Background
Approximately one third of patients receive biologics as monotherapy without disease-modifying antirheumatic drugs (DMARDs).1 The safety and efficacy of tocilizumab monotherapy have been demonstrated in several randomized clinical trials in patients with rheumatoid arthritis (RA) who had an inadequate response to either methotrexate or DMARDs. The AMBITION (Actemra versus Methotrexate double-Blind Investigative Trial In mONotherapy) trial was the first trial to demonstrate the clinical superiority of biologic monotherapy over methotrexate monotherapy at the typical methotrexate dosing regimens used in Europe and the U.S.
The objectives of this long-term extension (LTE) study were to:
• Evaluate the long-term efficacy of tocilizumab in patients with RA who were randomly assigned to tocilizumab monotherapy in the AMBITION core study and who remained on tocilizumab monotherapy in the LTE study for up to 240 weeks;
• Characterize the rate, timing, and nature of the addition of DMARDs in those patients randomly assigned to tocilizumab monotherapy in the AMBITION core study and who later added DMARDs in the LTE study.
Study design
• AMBITION was a 24-week randomized controlled trial in patients who had active RA and who were either methotrexate naive or methotrexate free for six months before entering the study.
• The LTE study was a post-hoc exploratory analysis of patients assigned to tocilizumab monotherapy in the AMBITION study.
• Patients were randomly assigned to either tocilizumab (8 mg/kg) administered intravenously every four weeks or methotrexate (7.5–20 mg) administered orally every week for 24 weeks.
• At week 24, patients completing AMBITION could enrol in the LTE study at their own or the investiga-tor’s discretion.
• During the LTE study, patients were given metho-trexate or any other allowable DMARD if they did not achieve a 50% improvement in tender joint
count (TJC) and swollen joint count (SJC) from baseline of the AMBITION core study.
Key findings
• Patients (n = 243) who were assigned to tocilizumab monotherapy in the AMBITION study were tran-sitioned into the LTE study.
Of the 243 patients, 139 (57.2%) remained on monotherapy in the LTE study until withdrawal or data cut, and 104 added a DMARD.
– Of the 139 patients who remained on tocilizumab monotherapy 27% had withdrawn by week 240. Of the 104 patients who added a DMARD, 30% had withdrawn by week 240.
• Compared with patients who remained on mono-therapy, a higher proportion of patients who added a DMARD withdrew because of adverse events (AEs).
• In patients who remained on tocilizumab mono-therapy, mean SJC and TJC decreased sharply during the first 24 weeks of tocilizumab treatment in the AMBITION core study; levels continued to decrease or were maintained thereafter in the LTE study. (Figure 1)
• At week 24, the proportions of patients remaining on tocilizumab monotherapy who achieved 28-joint disease activity score (DAS28) <2.6 and DAS28 ≤3.2 increased sharply to 40.1% and 54.0%, respectively (AMBITION core study); these scores continued to increase or were maintained in the LTE study. (Figure 2)
• The proportions of patients remaining on tocilizumab monotherapy who achieved clinical disease activity index (CDAI) remission and CDAI low disease activity increased sharply to 16.7% and 47.8%, respectively, at week 24 (AMBITION core study), and continued to increase or were maintained thereafter.
• For patients (n = 104) who added a DMARD, the median time to the first DMARD addition was 26 weeks. (Figure 3)
The addition of DMARDs occurred early for most patients, either before or within three weeks of entering the study.
• There was no association between baseline metho-trexate experience status and whether a DMARD was added.

10 New Evidence in Rheumatology | January 2013
Figure 1. Mean (SD) for SJC (66) over time up to week 240 in patients who remained on tocilizumab monotherapy
Figure 2a. Absolute numbers and percentages of patients who achieved DAS28 remission (DAS28 <2.6) of all patients who continued tocilizumab monotherapy in the LTE study
*Numbers of patients with valid assessments
SD = standard deviation; SJC = swollen joint counts
2400 12 24 36 48 60 72 84 96 108 120 132 144 156 168 180 192 204 216 228
90139N* 139 138 130 132 125 126 123 124 119 121 116 117 115 113 111 108 103 102 100
Weeks
Mea
n (
SD)
SJC
–10
50
60
70
40
30
20
10
0
*Absolute numbers of patients achieving DAS28 <2.6†Numbers of patients with valid assessments
DAS28 = 28-joint disease activity score; LTE = long-term extension
2400 12 24 36 48 60 72 84 96 108 120 132 144 156 168 180 192 204 216 228
580n* 37 55 54 55 61 65 70 69 70 69 74 65 66 70 72 73 67 62 61
87138N† 138 137 128 128 123 121 121 121 118 115 110 111 109 111 107 107 99 100 97
Weeks
Pati
ents
, %
0
60
70
80
50
40
30
20
10

New Evidence in Rheumatology | January 2013 11
ACR/ARHP
Figure 2b. Absolute numbers and percentages of patients who achieved CDAI remission (CDAI ≤2.8) of all patients who continued tocilizumab monotherapy in the LTE study
Figure 3. Kaplan-Meier plot of time to addition of first DMARD
+ = censored
DMARD = disease-modifying antirheumatic drug; TCZ = tocilizumab
240 252 264 276 288 3000 12 24 36 48 60 72 84 96 108 120 132 144 156 168 180 192 204 216 228
Weeks from TCZ monotherapy
Pro
bab
ility
of
add
ing
fir
st D
MA
RD
0.0
0.6
0.7
0.8
0.5
0.4
0.3
0.2
0.1
0.9
1.0
*Absolute numbers of patients achieving CDAI remission†Numbers of patients with valid assessments
CDAI = clinical disease activity index; LTE = long-term extension
2400 12 24 36 48 60 72 84 96 108 120 132 144 156 168 180 192 204 216 228
370n* 13 23 24 31 34 36 38 36 41 52 48 41 37 43 42 43 47 39 43
90138N† 139 138 129 133 125 124 123 125 120 121 116 117 114 112 110 109 104 103 100
Weeks
Pati
ents
, %
0
30
35
40
25
20
15
10
5
45
50
Key conclusions
■ Tocilizumab monotherapy provided durable efficacy over time.
■ Regardless of whether or not a DMARD was added, there was no association with baseline methotrexate experience status.
■ The most common reason for withdrawal among patients who remained on tocilizumab monotherapy and those who added DMARDs was AEs; the proportion of patients withdrawing for this reason was higher in those who added DMARDs (20.2%) than in those who remained on monotherapy (10.8%).
Reference: 1. Jones G, Sebba A, Lepley D, et al. Long-term efficacy of tocilizumab monotherapy in patients with rheumatoid arthritis previously methotrexate naive or methotrexate free for 6 months. ACR Annual meeting Abstracts 2012;64:454.

12 New Evidence in Rheumatology | January 2013
Genovese, MC, et al. ACR 2012:1640
Long-term safety of tocilizumab in patients with rheumatoid arthritis and a mean treatment duration of 3.7 years
Background
Tocilizumab is approved for the treatment of adult patients with moderate-to-severe active rheumatoid arthritis (RA) who have an inadequate response (IR) to disease-modifying antirheumatic drugs (DMARDs) or tumour necrosis factor inhibitors (TNF-Is). Since the advent of tocilizumab, several phase III trials have pro-vided over 12,293 patient-years (pt-years) of safety data.1
The objective of this study was to further assess long-term safety data from patients with rheumatoid arthritis (RA) who received more than one dose of tocilizumab in five phase III clinical trials from initial exposure of patients in each study through April 1, 2011, providing over 14,994 pt-years of safety data.
Study design
• Data on patients who received at least one dose of tocilizumab in five phase III trials (OPTION [TOcilizumab Pivotal Trial in Methotrexate Inadequate respONders], TOWARD [Tocilizumab in cOmbination With traditional DMARD therapy], RADIATE [Research on Actemra Determining efficacy after Anti-RNF FailurEs], AMBITION [Actemra versus Methotrexate double-Blind Investigative Trial In mONotherapy], LITHE [TociLIzumab safety and THE prevention of structural joint damage study]), in a clinical pharma-cology study, or in long-term extension studies were pooled and assessed.
• Data were presented from the first tocilizumab exposure until April 1, 2011 (all-exposed population).
• Adverse events (AEs) and serious adverse events (SAEs) are reported as rates per 100 pt-years and 95% CI.
• Individual case review and aggregate review were per-formed and, when appropriate, cases were adjudicated.
Key findings
• Patients (n = 4,009) who received one or more doses of tocilizumab up to the cutoff date of April 1, 2011 were pooled for analysis.
The study was based on the following phase III studies:
– IR to DMARDs (n = 3039): OPTION, TOWARD, LITHE;
– IR to tumour necrosis factor inhibitors (TNF) (n = 499); RADIATE;
– Monotherapy (n = 673): AMBITION;
– Clinical pharmacology study (n = 23);
– Long-term extensions (LTEs) of five pivotal studies.
• The mean (median [range]) treatment duration was 3.74 years (4.56 [0.0–5.8]).
• The total exposure to tocilizumab was 13,502.8 pt-years and total duration of observation was 14,994 pt-years.
• The overall rate of SAEs was 14.6/100 pt-years (95% CI, 14.0–15.3). (Figure 1)
Figure 1. Rate of SAEs over time
CI = confidence interval; Pt-years = patient-years; SAE = serious adverse event
0–12
n = 5573,471 Pt-years
n = 4313,028 Pt-years
n = 4332,766
n = 7725,729 Pt-years
16.114.2
15.7
13.5
13–24 25–36 >36
Time, months
SAEs
(95
% C
I) p
er 1
00 P
t-ye
ars
0
12
14
16
18
20
10
8
6
4
2
New Evidence in Rheumatology | January 2013 13
ACR/ARHP
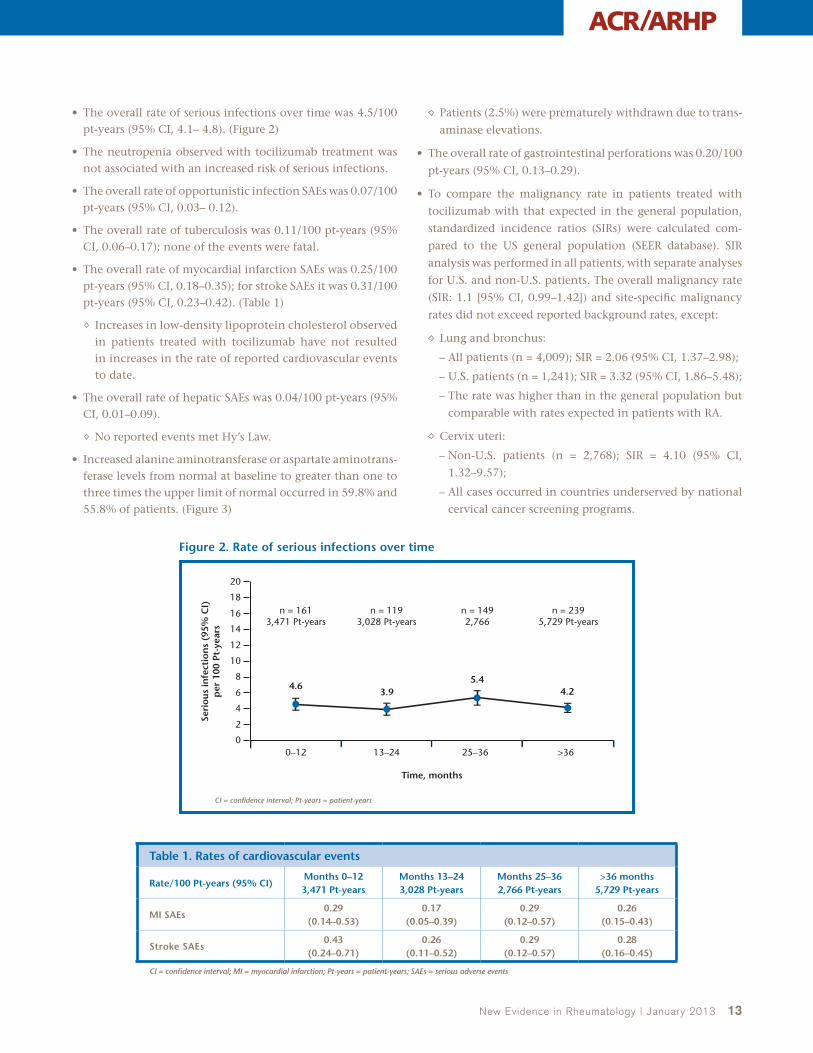
• The overall rate of serious infections over time was 4.5/100 pt-years (95% CI, 4.1– 4.8). (Figure 2)
• The neutropenia observed with tocilizumab treatment was not associated with an increased risk of serious infections.
• The overall rate of opportunistic infection SAEs was 0.07/100 pt-years (95% CI, 0.03– 0.12).
• The overall rate of tuberculosis was 0.11/100 pt-years (95% CI, 0.06–0.17); none of the events were fatal.
• The overall rate of myocardial infarction SAEs was 0.25/100 pt-years (95% CI, 0.18–0.35); for stroke SAEs it was 0.31/100 pt-years (95% CI, 0.23–0.42). (Table 1)
Increases in low-density lipoprotein cholesterol observed in patients treated with tocilizumab have not resulted in increases in the rate of reported cardiovascular events to date.
• The overall rate of hepatic SAEs was 0.04/100 pt-years (95% CI, 0.01–0.09).
No reported events met Hy’s Law.
• Increased alanine aminotransferase or aspartate aminotrans-ferase levels from normal at baseline to greater than one to three times the upper limit of normal occurred in 59.8% and 55.8% of patients. (Figure 3)
Patients (2.5%) were prematurely withdrawn due to trans-
aminase elevations.
• The overall rate of gastrointestinal perforations was 0.20/100
pt-years (95% CI, 0.13–0.29).
• To compare the malignancy rate in patients treated with
tocilizumab with that expected in the general population,
standardized incidence ratios (SIRs) were calculated com-
pared to the US general population (SEER database). SIR
analysis was performed in all patients, with separate analyses
for U.S. and non-U.S. patients. The overall malignancy rate
(SIR: 1.1 [95% CI, 0.99–1.42]) and site-specific malignancy
rates did not exceed reported background rates, except:
Lung and bronchus:
– All patients (n = 4,009); SIR = 2.06 (95% CI, 1.37–2.98);
– U.S. patients (n = 1,241); SIR = 3.32 (95% CI, 1.86–5.48);
– The rate was higher than in the general population but
comparable with rates expected in patients with RA.
Cervix uteri:
– Non-U.S. patients (n = 2,768); SIR = 4.10 (95% CI,
1.32–9.57);
– All cases occurred in countries underserved by national
cervical cancer screening programs.
Figure 2. Rate of serious infections over time
CI = confidence interval; Pt-years = patient-years
0–12
n = 1613,471 Pt-years
n = 1193,028 Pt-years
n = 1492,766
n = 2395,729 Pt-years
4.63.9
5.44.2
13–24 25–36 >36
Time, months
Seri
ous
infe
ctio
ns
(95%
CI)
per
100
Pt-
year
s
0
12
14
16
18
20
10
8
6
4
2
Table 1. Rates of cardiovascular events
Rate/100 Pt-years (95% CI)Months 0–12 3,471 Pt-years
Months 13–24 3,028 Pt-years
Months 25–36 2,766 Pt-years
>36 months 5,729 Pt-years
MI SAEs0.29
(0.14–0.53)0.17
(0.05–0.39)0.29
(0.12–0.57)0.26
(0.15–0.43)
Stroke SAEs0.43
(0.24–0.71)0.26
(0.11–0.52)0.29
(0.12–0.57)0.28
(0.16–0.45)
CI = confidence interval; MI = myocardial infarction; Pt-years = patient-years; SAEs = serious adverse events

14 New Evidence in Rheumatology | January 2013
Key conclusions
■ The safety profile of tocilizumab in the current analysis is consistent with that seen in previous tocilizumab analyses.1
• The safety profile remained stable over a mean treatment duration of 3.7 years.
• No new safety signals were identified.
■ SAE rates are consistent with those reported in the RA population, and the overall rate of malignancies does not exceed reported background rates (Surveillance Epidemiology and End Results [SEER] database).
Reference: 1. Genovese MC, Sebba A, Rubbert-Roth A, et al. Long-term safety of tocilizumab in patients with rheumatoid arthritis and a mean treatment duration of 3.7 years. ACR Annual Meeting Abstracts 2012;64:1640
Figure 3. ALT and AST elevations over time
0–12 37-48 61–7225–36 49–6013–24
Pati
ents
, %
Time, months
7.5
2.2
ALT >3 x ULN AST >3 x ULN
ALT = alanine aminotransferase; AST = aspartate aminotransaminase; ULN = upper limit of normal
0
3
6
9
12
15
3.5
1.2
3.3
1.0
2.9
0.9
2.6
0.6
1.6
0.61.1 1.2
ALT >3 × ULN, n 301/4,002 120/3,440 101/3,091 84/2,863 68/2,635 28/1,788
73–84
1/92
AST >3 × ULN, n 89/4,002 40/3,437 32/3,090 25/2,863 16/2,635 11/1,783 1/86
Burmester GR, et al. ACR 2012:2545
Safety and efficacy of subcutaneous tocilizumab versus intravenous tocilizumab in combination with traditional DMARDs in patients with moderate-to-severe rheumatoid arthritis
Background
Tocilizumab is an anti-interleukin-6 (IL-6) receptor
antibody that inhibits IL-6 signalling. Tocilizumab,
in combination with traditional disease-modifying
antirheumatic drugs (DMARDs) or as monotherapy, has
been demonstrated to be effective and well tolerated in
patients with rheumatoid arthritis who had an inad-
equate response (IR) to DMARDs.1 Since tocilizumab is
administered intravenously (iv), patients are required to be present in a medical facility. Having a subcutaneous (sc) formulation of tocilizumab would offer patients a convenient option that could be administered at home.
The objectives of this study were to assess the non-inferiority of tocilizumab sc to tocilizumab iv and to determine the safety of tocilizumab sc compared with tocilzumab iv.
New Evidence in Rheumatology | January 2013 15
ACR/ARHP
Study design
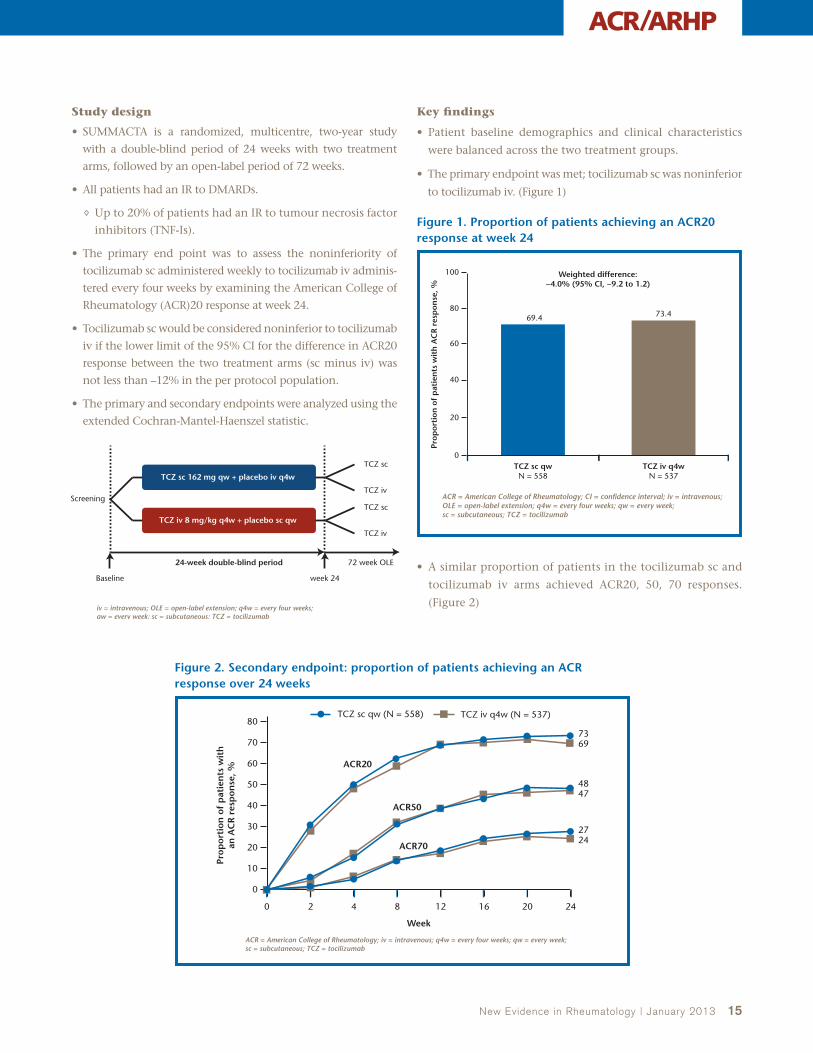
• SUMMACTA is a randomized, multicentre, two-year study
with a double-blind period of 24 weeks with two treatment
arms, followed by an open-label period of 72 weeks.
• All patients had an IR to DMARDs.
Up to 20% of patients had an IR to tumour necrosis factor
inhibitors (TNF-Is).
• The primary end point was to assess the noninferiority of
tocilizumab sc administered weekly to tocilizumab iv adminis-
tered every four weeks by examining the American College of
Rheumatology (ACR)20 response at week 24.
• Tocilizumab sc would be considered noninferior to tocilizumab
iv if the lower limit of the 95% CI for the difference in ACR20
response between the two treatment arms (sc minus iv) was
not less than –12% in the per protocol population.
• The primary and secondary endpoints were analyzed using the
extended Cochran-Mantel-Haenszel statistic.
Key findings
• Patient baseline demographics and clinical characteristics
were balanced across the two treatment groups.
• The primary endpoint was met; tocilizumab sc was noninferior
to tocilizumab iv. (Figure 1)
• A similar proportion of patients in the tocilizumab sc and
tocilizumab iv arms achieved ACR20, 50, 70 responses.
(Figure 2)
Figure 2. Secondary endpoint: proportion of patients achieving an ACR response over 24 weeks
TCZ iv q4w (N = 537)TCZ sc qw (N = 558)
Prop
orti
on o
f p
atie
nts
wit
han
AC
R r
esp
onse
, %
Week
0
80
70
60
50
40
30
20
10
ACR = American College of Rheumatology; iv = intravenous; q4w = every four weeks; qw = every week; sc = subcutaneous; TCZ = tocilizumab
24
ACR20
ACR50
7369
4847
2724
ACR70
16 208 120 2 4
Figure 1. Proportion of patients achieving an ACR20 response at week 24
69.4
20
0
40
60
80
100 Weighted difference:−4.0% (95% CI, −9.2 to 1.2)
73.4
TCZ sc qwN = 558
TCZ iv q4wN = 537
ACR = American College of Rheumatology; CI = confidence interval; iv = intravenous; OLE = open-label extension; q4w = every four weeks; qw = every week; sc = subcutaneous; TCZ = tocilizumab
Prop
orti
on o
f p
atie
nts
wit
h A
CR
res
pon
se, %
iv = intravenous; OLE = open-label extension; q4w = every four weeks; qw = every week; sc = subcutaneous; TCZ = tocilizumab
Screening
TCZ sc
TCZ iv
TCZ sc
TCZ iv
Baseline
TCZ iv 8 mg/kg q4w + placebo sc qw
TCZ sc 162 mg qw + placebo iv q4w
24-week double-blind period
week 24
72 week OLE
16 New Evidence in Rheumatology | January 2013
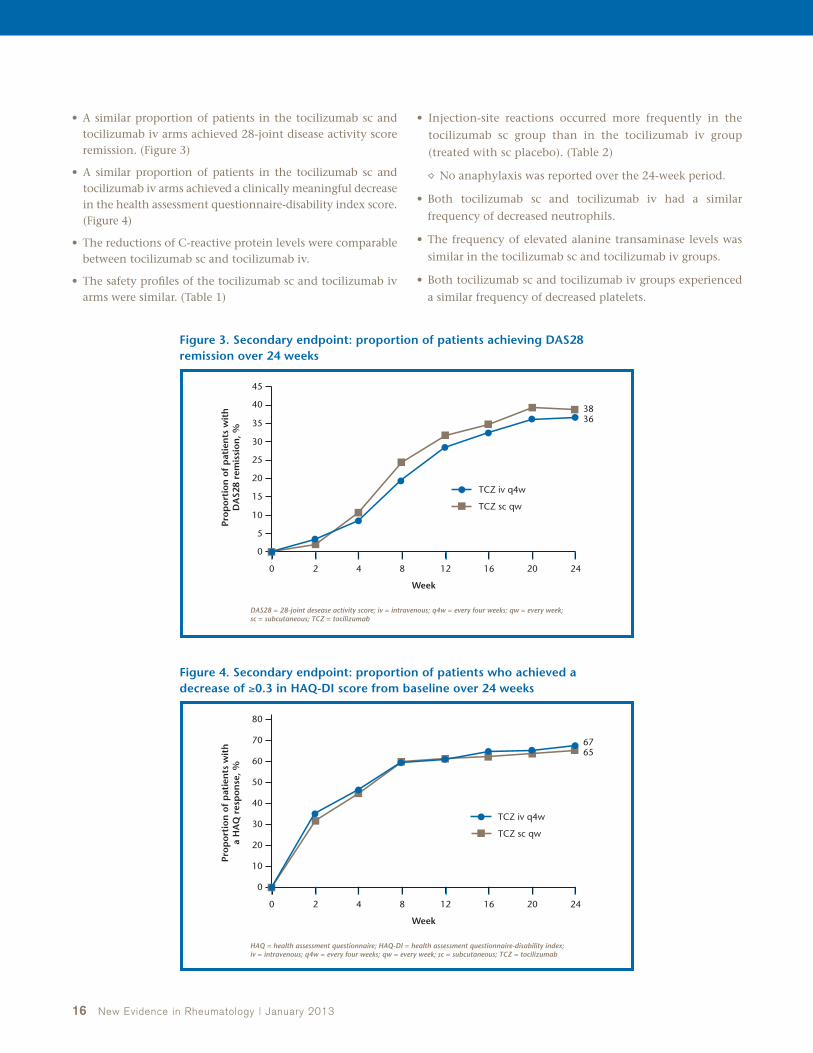
• A similar proportion of patients in the tocilizumab sc and tocilizumab iv arms achieved 28-joint disease activity score remission. (Figure 3)
• A similar proportion of patients in the tocilizumab sc and tocilizumab iv arms achieved a clinically meaningful decrease in the health assessment questionnaire-disability index score. (Figure 4)
• The reductions of C-reactive protein levels were comparable between tocilizumab sc and tocilizumab iv.
• The safety profiles of the tocilizumab sc and tocilizumab iv arms were similar. (Table 1)
• Injection-site reactions occurred more frequently in the
tocilizumab sc group than in the tocilizumab iv group
(treated with sc placebo). (Table 2)
No anaphylaxis was reported over the 24-week period.
• Both tocilizumab sc and tocilizumab iv had a similar
frequency of decreased neutrophils.
• The frequency of elevated alanine transaminase levels was
similar in the tocilizumab sc and tocilizumab iv groups.
• Both tocilizumab sc and tocilizumab iv groups experienced
a similar frequency of decreased platelets.
Figure 3. Secondary endpoint: proportion of patients achieving DAS28 remission over 24 weeks
Figure 4. Secondary endpoint: proportion of patients who achieved a decrease of ≥0.3 in HAQ-DI score from baseline over 24 weeks
TCZ sc qw
TCZ iv q4w
Prop
orti
on o
f p
atie
nts
wit
hD
AS2
8 re
mis
sion
, %
Week
0
45
40
30
25
20
15
10
5
DAS28 = 28-joint desease activity score; iv = intravenous; q4w = every four weeks; qw = every week; sc = subcutaneous; TCZ = tocilizumab
24
3836
16 208 120 2 4
35
TCZ sc qw
TCZ iv q4w
Pro
po
rtio
n o
f p
atie
nts
wit
ha
HA
Q r
esp
on
se, %
Week
0
80
70
60
50
40
30
20
10
HAQ = health assessment questionnaire; HAQ-DI = health assessment questionnaire-disability index; iv = intravenous; q4w = every four weeks; qw = every week; sc = subcutaneous; TCZ = tocilizumab
24
6765
16 208 120 2 4

New Evidence in Rheumatology | January 2013 17
ACR/ARHP
Key conclusions
■ Tocilizumab sc was confirmed to be noninferior to tocilizumab iv in the SUMMACTA study.
■ The efficacy of tocilizumab sc administered at 162 mg weekly was comparable to that of tocilizumab iv administered at 8 mg/kg every four weeks.
■ No new clinically meaningful safety signals for tocilizumab were identified with sc administration.
■ Tocilizumab sc could provide an additional administration option as well as at-home administration for patients with RA.
Reference: 1. Burmester GR, Rubbert-Roth A, Cantagrel A, et al. SUMMACTA: A randomized, double-blind, parallel group study of the safety and efficacy of tocilizumab SC versus tocilizumab IV in combination with traditional DMARDs in patients with moderate to severe RA. ACR Annual Meeting Abstracts 2012;64:2545.
Table 1. Adverse events and serious adverse events
TCZ sc 162 mg qw (N = 631) TCZ iv 8 mg/kg q4w (N = 631)
AEs
Total AEs, n 1,515 1,479
Patients with ≥1 AE, n (%) 481 (76.2) 486 (77.0)
Discontinuation due to AE, n (%) 30 (5) 41 (6.5)
SAEs
Total SAEs, n 33 41
Patients with ≥1 SAE, % 29 (4.6) 33 (5.2)
Deaths, n (%) 0 (0.0) 1 (<1)
AEs = adeverse events; iv = intravenous; q4w = every four weeks; qw = every week; SAEs = serious adverse events; sc = subcutaneous; TCZ = tocilizumab
Table 2. Injection site reactions and hypersensitivity
TCZ sc 162 mg qw (N = 631)
TCZ iv 8 mg/kg q4w (N = 631)
ISRs
Patients with ISRs, n (%) 64 (10.1) 15 (2.3)
ISR symptoms, n 168 94
Erythema, n (%) 28 (4.4) 5 (0.8)
Pain, n (%) 12 (1.9) 5 (0.8)
Pruritus, n (%) 14 (2.2) 0 (0.0)
Hematoma, n (%) 5 (0.8) 5 (0.8)
ISRs led to withdrawal, n 0 0
Hypersensitivity
Serious hypersensitivity, n (%) 2 (<1) 3 (<1)
ISRs = injection-site reactions; iv = intravenous; q4w = every four weeks; qw = every week; sc = subcutaneous; TCZ = tocilizumab

18 New Evidence in Rheumatology | January 2013
Choquette D, et al. ACR 2012:1841
Lower than expected levels of DMARD acquisition immediately before and following biologic initiation in patients with rheumatoid arthritis
Background
Reports suggest that a large proportion of patients who acquire and use biologic disease-modifying antirheumatic agents (DMARDs) to treat patients with rheumatoid arthritis (RA) do not acquire or adequately consume traditional DMARDs.1 However, acquisition rates of biologics and DMARDs at the point of biologic initiation remain to be determined.
The primary objective of this study was to explore the level of DMARD acquisition in Canadian patients with RA in the six to 12 months immediately prior to and following biologic initiation, and to quantify the levels of biologic monotherapy versus biologic plus DMARD consumption.
Study design
• Concomitant biologic and DMARD therapy based on actual patient purchases was examined by tracking the records of a cohort of 1,652 anonymous patients with rheumatoid arthritis (RA) from public and private drug plans in Ontario and Quebec, via unique drug plan identifier numbers (third-party source).
• All patients who were initiated on a biologic between August 2009 and July 2010 were tracked for one year prior to and following their biologic initiation date.
• All cohort patients were compliant with the use of
biologics following initiation.
• The prescribing frequencies of RA therapies by
rheumatologists was assessed through randomly
recruited surveys (n = 100).
Key findings
• Among the cohort patients:
25% did not purchase any form of DMARDs
within the six months prior to starting a biologic
(41% for methotrexate); (Figures 1 and 2)
29% did not acquire DMARDs at any point in the
six months following biologic initiation (43% for
methotrexate);
22% did not acquire DMARDs for 12 months prior
to biologic initiation (37% for methotrexate);
26% did not acquire DMARDs 12 months following
biologic initiation (41% for methotrexate).
• Biologics without a DMARD were prescribed only
12% of the time.
• Prescriptions provided two to three months’ worth
of drug supplies.
Figure 1. Percent of patients not acquiring any methotrexate
37%
10
0
20
30
40
50 Pre biologic initiation
41%
12 months pre biologic 6 months pre biologic
Cohort of 1,652 patients with RA receiving a biologic analyzed six and 12 months prior to and following biologic initiation (RAM-Q, ODB, and ON and PQ private drug plan data)
DMARDs = disease-modifying antireheumatic drugs; ODB = Ontario Drug Benefit; ON = Ontario; PQ = Quebec; RA = rheumatoid arthritis; RAM-Q = Régie de l'assurance maladie du Québec
% p
atie
nts
not
acq
uiri
ng
met
hot
rexa
te
17%
43%
17%
41%
10
0
20
30
40
50 Post biologic initiation
6 months post biologic initiation 12 months post biologic initiation
% p
atie
nts
not
acq
uiri
ng
met
hot
rexa
te
% patients not acquiring methotrexate Physician frequency of not prescribing methotrexate post biologic initiation
Biologic initiation

New Evidence in Rheumatology | January 2013 19
ACR/ARHP
Kavanaugh A, et al. ACR 2012:772
Tocilizumab monotherapy compared with adalimumab monotherapy in patients with rheumatoid arthritis: results of a 24-week study
Background
Approximately one third of patients with rheumatoid arthritis (RA) treated with biologics receive them as monotherapy.1 Tocilizumab, an inhibitor of inter-leukin-6 (IL-6) receptor signalling, has been studied as monotherapy in six clinical trials but direct comparison
with a tumour necrosis factor (TNF) inhibitor such as
adalimumab has not previously been undertaken.
The objective of this study was to investigate the
efficacy and safety of tocilizumab versus adalimumab
monotherapy in patients with RA.
Figure 2. Percent of patients not acquiring any disease-modifying antirheumatic drugs
22%
10
0
20
30
40
50 Pre biologic initiation
25%
12 months pre biologic 6 months pre biologic
Cohort of 1,652 patients with RA receiving a biologic six and 12 months prior to and following biologic initiation (RAM-Q, ODB, and ON and PQ private drug plan data)
DMARDs = disease-modifying antireheumatic drugs; ODB = Ontario Drug Benefit; ON = Ontario; PQ = Quebec; RA = rheumatoid arthritis; RAM-Q = Régie de l'assurance maladie du Québec
% p
atie
nts
not
acq
uiri
ng
DM
AR
Ds
12%
29%
12%
26%
10
0
20
30
40
50 Post biologic initiation
6 months post biologic initiation 12 months post biologic initiation
% p
atie
nts
not
acq
uiri
ng
DM
AR
Ds
% patients not acquiring DMARDs Physician frequency of not prescribing DMARDs post biologic initiation (% biologic monotherapy)
Biologic initiation
Key conclusions
■ Many patients with RA who were treated with biologics (~29%) did not acquire any form of DMARD in the six to 12 months immediately following initiation of a first-line biologic, despite the observation that biologic monotherapy was prescribed by general physicians at a frequency of 12%.
• This suggests there was non-adherence by patients to physician-directed treatment regimens.
■ Many patients with RA who were treated with biologics (~one in four) did not acquire DMARDs in the six to 12 months immediately before a biologic was initiated for the first time.
• This may negatively influence compliance on DMARDs once a biologic is initiated.
■ Close monitoring of DMARD intake and/or management of patients on monotherapy is recommended .
• Nonetheless, patient education concerning adherence to treatment protocols is of prime importance.
Reference: 1. Choquette D, Thomas O, Arundine M. Lower than expected levels of DMARD acquisition immediately pre and post biologic initiation in rheumatoid arthritis patients. ACR Annual Meeting Abstracts 2012;64:1841.
20 New Evidence in Rheumatology | January 2013
Study design
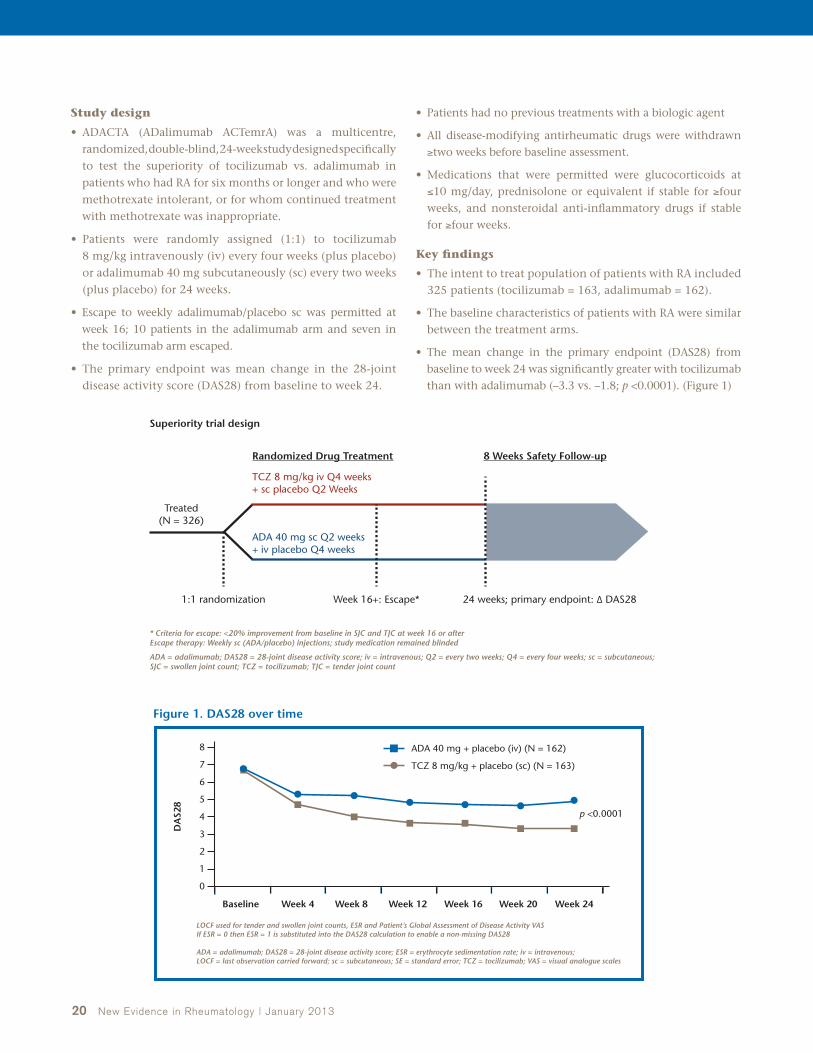
• ADACTA (ADalimumab ACTemrA) was a multicentre, randomized, double-blind, 24-week study designed specifically to test the superiority of tocilizumab vs. adalimumab in patients who had RA for six months or longer and who were methotrexate intolerant, or for whom continued treatment with methotrexate was inappropriate.
• Patients were randomly assigned (1:1) to tocilizumab 8 mg/kg intravenously (iv) every four weeks (plus placebo) or adalimumab 40 mg subcutaneously (sc) every two weeks (plus placebo) for 24 weeks.
• Escape to weekly adalimumab/placebo sc was permitted at week 16; 10 patients in the adalimumab arm and seven in the tocilizumab arm escaped.
• The primary endpoint was mean change in the 28-joint disease activity score (DAS28) from baseline to week 24.
• Patients had no previous treatments with a biologic agent
• All disease-modifying antirheumatic drugs were withdrawn ≥two weeks before baseline assessment.
• Medications that were permitted were glucocorticoids at ≤10 mg/day, prednisolone or equivalent if stable for ≥four weeks, and nonsteroidal anti-inflammatory drugs if stable for ≥four weeks.
Key findings
• The intent to treat population of patients with RA included 325 patients (tocilizumab = 163, adalimumab = 162).
• The baseline characteristics of patients with RA were similar between the treatment arms.
• The mean change in the primary endpoint (DAS28) from baseline to week 24 was significantly greater with tocilizumab than with adalimumab (–3.3 vs. –1.8; p <0.0001). (Figure 1)
* Criteria for escape: <20% improvement from baseline in SJC and TJC at week 16 or after Escape therapy: Weekly sc (ADA/placebo) injections; study medication remained blinded
ADA = adalimumab; DAS28 = 28-joint disease activity score; iv = intravenous; Q2 = every two weeks; Q4 = every four weeks; sc = subcutaneous; SJC = swollen joint count; TCZ = tocilizumab; TJC = tender joint count
Superiority trial design
Randomized Drug Treatment 8 Weeks Safety Follow-up
Treated(N = 326)
1:1 randomization
TCZ 8 mg/kg iv Q4 weeks + sc placebo Q2 Weeks
ADA 40 mg sc Q2 weeks + iv placebo Q4 weeks
Week 16+: Escape* 24 weeks; primary endpoint: ∆ DAS28
TCZ 8 mg/kg + placebo (sc) (N = 163)
p <0.0001
ADA 40 mg + placebo (iv) (N = 162)
DA
S28
Baseline Week 4 Week 8 Week 12 Week 16
0
8
7
6
5
4
3
2
1
LOCF used for tender and swollen joint counts, ESR and Patient’s Global Assessment of Disease Activity VASIf ESR = 0 then ESR = 1 is substituted into the DAS28 calculation to enable a non-missing DAS28
ADA = adalimumab; DAS28 = 28-joint disease activity score; ESR = erythrocyte sedimentation rate; iv = intravenous; LOCF = last observation carried forward; sc = subcutaneous; SE = standard error; TCZ = tocilizumab; VAS = visual analogue scales
Week 20 Week 24
Figure 1. DAS28 over time

New Evidence in Rheumatology | January 2013 21
ACR/ARHP
• A greater proportion of tocilizumab patients achieved American College of Rheumatology criteria (ACR)20, ACR50, and ACR70 than adalimumab patients (p <0.005). (Figure 2)
• The proportion of patients achieving clinical disease activity index remission (≤2.8 and ≤3.3) at week 24 was greater for the tocilizumab arm than the adalimumab arm (post-hoc analysis; p <0.05). (Figure 3)
• Incidences of adverse events (AEs), serious AEs, and serious infections were similar between arms (tocilizumab = 83%/21%/3%; adalimumab = 82%/23%/ 3%). (Table 1)
• Alanine transaminase and low-density lipoprotein elevations, and neutrophil count reductions were more common in patients in the tocilizumab arm. (Figures 4 and 5)
Figure 2. Secondary endpoints (proportions of patients with ACR20/50/70 response at week 24)
ACR20 ACR70ACR50
Pati
ents
(%
)
49.4
65.0*
27.8
47.2†
17.9
32.5*
0
10
50
20
30
40
70
60
ADA (N = 162) TCZ (N = 163)
*p <0.005 (vs. ADA) †p <0.0005 (vs. ADA) Significance was determined using a logistic regression analysis (covariates included treatment, region, and duration of RA)LOCF was used for missing TJC and SJC. If CRP was missing ESR was substitutedNon-responder imputation was used for missing data
ADA = adalimumab; CRP = C-reactive protein; DAS28 = 28-joint disease activity score; ESR = erythrocyte sedimentation rate; LOCF = last observation carried forward; SJC = swollen joint count; RA = rheumatoid arthritis; TCZ = tocilizumab; TJC = tender joint count
Remission(0 ≤2.8)
Low disease activity(2.8 <10)
Pati
ents
, %
9.3
17.2*
19.8
30.7†
0
5
25
10
15
20
35
40
30
ADA (n = 162) TCZ (n = 163)
*p = 0.0389, remission (unadjusted, no control for multiple testing) †p = 0.0211, low disease activity (unadjusted, no control for multiple testing) Proportions of patients were compared using Cochran-Mantel-Haenszel analysis stratified by region and duration of RA.Data collected after withdrawal/initiation of escape therapy were set to missing. LOCF was used for missing data.
ADA = adalimumab; AEs = adverse events; CDAI = clinical disease activity index; LOCF = last observation carried forward; RA = rheumatoid arthritis; TCZ = tocilizumab
Baseline week 4 week 8 week 12 week 16 week 20 week 24
Ab
solu
te m
ean
CD
AI,
%
0
5
25
10
15
20
35
40
45
50
30
Figure 3. CDAI: Remission, low disease activity, and mean CDAI score over time
Table 1. Adverse events (safety population)
ADA n = 162
TCZ n = 162
AEs 443 430
Patients with ≥1 AE, n (%) 134 (83) 133 (82)
SAEs 21 23
Patients with ≥1 SAE, n (%) 16 (10) 19 (12)
Infection AEs 106 113
Patients with ≥1 infection AE, n (%) 68 (42) 77 (48)
Infection SAEs 7 6
Patients with ≥1 infection SAE, n (%) 5 (3) 5 (3)
Deaths, n (%) 0 (0) 2 (1)*
Multiple occurrences of the same AE in one patient were counted only once*Deaths• 49-year-old woman on study day 3: illicit drug overdose (marijuana, benzodiazepines,
methadone in urine). Considered unrelated to study drug.• 56-year-old man “sudden death” on study day 93: cause unknown (autopsy not
performed). Considered possibly related to study drug. Comorbidities: peripheral vascular disease, hypertension, smoking, interstitial lung disease.
ADA = adalimumab; AEs = adverse events; SAEs = serious adverse events; TCZ = tocilizumab

22 New Evidence in Rheumatology | January 2013
62.3
20
0
40
60
100
80
TCZ (n = 162)ADA (n = 162)
24.7
72.2
30.9
1.95.6
1.2 1.2
Normal
ALT levels
Pati
ents
, %
>ULN–2.5× ULN >2.5–5× ULN >5–20× ULN
ADA = adalimumab; ALT = alanine aminotransferase; CTC = common toxicity criteria; TCZ = tocilizumab; ULN = upper limit of normal
20
0
40
60
100
80
TCZ (n = 162)ADA (n = 162)
75.9
90.7
4.3
10.5
1.2 1.93.7
11.1
0.0 0.6
Normal
Neutrophil level/mm3
Pati
ents
, %
<LLN–1500 <1000–500<1500–1000 <500
ADA = adalimumab; CTC = common toxicity criteria; TCZ = tocilizumab; LLN = lower limit of normal
Figure 5. Neutrophil levels by CTC grade (worst value) (safety population)
Figure 4. ALT levels by CTC grade (worst value) (safety population)
Key conclusions
■ Tocilizumab monotherapy was superior to adalimumab monotherapy in reducing the signs and symptoms of RA.
■ The overall AE profile was comparable between the two treatment arms.
■ The safety observed in the tocilizumab arm of the study was consistent with the known safety profile of tocilizumab, and no new or unexpected AEs were observed.
Reference: 1. Kavanaugh A, Emery P, van Vollenhoven RF, et al. Tocilizumab monotherapy compared with adalimumab monotherapy in patients with rheumatoid arthritis: results of a 24-week study. ACR Annual Meeting Abstracts 2012;64:772.

ACR/ARHP
Key conclusions
■ Tocilizumab monotherapy was superior to adalimumab monotherapy in reducing the signs and symptoms of RA.
■ The overall AE profile was comparable between the two treatment arms.
■ The safety observed in the tocilizumab arm of the study was consistent with the known safety profile of tocilizumab, and no new or unexpected AEs were observed.
Canadian perspective by Dr. Majed Khraishi
Tocilizumab is a very effective biologic used to treat patients with active rheumatoid arthri-tis (RA). We use tocilizumab in patients who have an inade-quate response to methotrexate and/or disease-modifying anti-rheumatic drugs (DMARDs), in patients who fail a tumour necrosis factor inhibitor (TNF-I), and occasionally in patients
who are naïve to biologics and have contraindications to methotrexate and/or DMARDs. While most biologics are comparable to each other in efficacy and safety, and are effective when given in combination with methotrexate, data suggest that tocilizumab use with (or without) methotrexate results in high remission rates. In addition, tocilizumab is effective and safe when given as monotherapy. The availability of two options that are effective provides physicians with greater flexibility when treating patients.
At ACR 2012, conference investigators presented studies on the long-term safety and efficacy of tocilizumab, efficacy of tocilizumab compared with adalimumab, as well as issues surrounding patient compliance with taking DMARDs while on biologic treatments.
Jones G et al. presented results from the long-term extension of the AMBITION study (Actemra versus Methotrexate double- Blind Investigative Trial In mONotherapy) in which the long-term efficacy of tocilizumab monotherapy in patients with RA previously methotrexate naïve or free for six months was analyzed. The study showed that tocilizumab continued to be very effective after long periods of therapy. Patients achieved high remission rates and the drug continued to work well over the 240 weeks (4.6 years). In addition, the safety profile of the drug remained stable over time with no new safety signals identified. Data from this study and others challenge the view that tocilizumab in combination with methotrexate is more effective than tocilizumab monotherapy. Additional studies on tocilizumab monotherapy in real-life settings as well as long-term radiological data will help to clarify this question.
The study by Kavanaugh et al. compared the efficacy and safety of tocilizumab monotherapy with adalimumab monotherapy. Not surprisingly, the study showed tocilizumab monotherapy to be more effective at standard doses for each agent. Clinicians usually give adalimumab in combination with methotrexate where it has demonstrated efficacy, but not as frequently as monotherapy. Overall, the key messages we can take from this study are that tocilizumab is a better option in patients when monotherapy is being considered, and that tocilizumab mono-therapy has a similar safety profile to adalimumab, a TNF-I widely used in the clinic.
The study by Genovese et al. addressed a number of concerns about the long-term safety of tocilizumab. These include cardiovascular effects, liver function, neutropenia, and bowel perforations. Overall, the safety profile of the drug was very good and specifically these adverse events (AEs) remained stable over the length of study period (3.7 years) with no alarming signals detected. Also, other long-term concerns such as infections and lymphomas did not seem to be more common with tocilizumab than with other biologics and their incidence did not increase over time.
The study by Burmester G et al. presented findings on the efficacy and safety of a subcutaneous (sc) formulation of tocilizumab. The study showed that the two forms were very effective, and it is clear that if a physician chooses tocilizumab sc over tocilizumab iv, efficacy would not be compromised by offering the sc route. The development of tocilizumab sc is significant because many patients prefer sc medications over iv. With the development of tocilizumab sc, patients now have a convenient choice and physicians have greater flexibility in treatment options. Based on these results, I consider tocilizumab iv and tocilizumab sc to be equally effective options. However, an important concern with moving away from the iv form of any medication to an sc form is whether patient noncompliance affects the safety and efficacy of the treatment. The advantages of the iv form of a drug are that the physician can be more certain of the number of doses a patient receives and that safety signals in the patient can be followed more carefully. A study that examines how safety and efficacy of a treatment is affected by switching from iv to sc forms of a drug would help clarify this question.
The study by Choquette D, et al. examined the extent of non-compliance in patients when taking DMARDs with and without biologics. Based on the study, the number of patients failing to take their DMARD prescriptions was higher than expected. There are significant consequences that result from DMARD noncompliance, the most significant of which is a failure to control disease progression. This causes physicians to change medications and expose patients to new and unnecessary treatments rather than optimize original treatments. The issue of noncompliance is difficult to deal with. A patient may simply refuse or stop a medication due to painful AEs. However, there are a number of ways to increase compliance. Improving communication between physicians and patients and between nurses (or other healthcare professionals) and patients is critical. We also need to better understand the effects of patient noncompliance on the efficacy and safety of treatments. It may be that some patients actually fair better with lower doses and thus reducing the dosage would be beneficial. A study that investigates the rate of noncompliance in patients who have undergone remission could help reveal ways to remedy this issue. Also, having biologic options that work well as mono-therapy, such as tocilizumab, may offer good options for patients with high non-compliance rates.
New Evidence in Rheumatology | January 2013 23
24 New Evidence in Rheumatology | January 2013
Investigator Commentary
New Evidence: What are the advantages of tocilizumab as a treatment for rheumatoid arthritis (RA)?
Dr. Genovese: Tocilizumab is a novel monoclonal antibody that competitively inhibits the binding of interleukin-6 (IL-6) to its receptor (IL-6R). Given its novel mechanism of action, tocilizumab provides an additional option for the management of RA. In addition, studies have shown tocilizumab to have good efficacy with a rapid onset of action, as well as a reasonable safety profile.
New Evidence: Please describe the withdrawal rate in your study.
Dr. Genovese: The withdrawal rate in our study was 1,473/4,009 patients (37%) after 72 months. This withdrawal rate is typical of that seen in clinical trials and is not in itself a reason for concern. Over time, patients often get tired of participating in clinical trials. Therefore, in a long-term study such as ours, it is typical to see withdrawal rates of this magnitude.
What is important when examining withdrawal rates is how these relate to reported adverse events (AEs). In our study, the rate of AEs leading to withdrawal was 5.0/100 patient years. Most of these withdrawals were related to infections, laboratory abnormalities, and neoplasms. However, the magnitude of the rate was not of concern in comparison with that seen with other treatments for RA and it decreased over time.
New Evidence: Did your study reveal any safety signals of concern?
Dr. Genovese: No new safety signals were detected in our study. The results of our study demonstrated that AE rates remained stable or decreased over time. In addition, AE rates reported in our study were similar to those shown in other studies examining the safety of tocilizumab.
The overall malignancy rate in our study was higher than that reported in the general population, but was no greater than that shown in patients with RA, as reported in the Surveillance Epidemiology and End Results (SEER) database. What is unclear is why the rate of certain cancers such as lung and bronchus, as well as cervical, was greater than that of others. Although we do not fully understand why the rate of malignancies is higher in patients with RA, it is possible that it has something to do with the body’s immune response to the inflammation.
At the ACR/ARHP 2012 Annual Scientific Meeting, New Evidence spoke with
Dr. Mark Genovese, Professor of Medicine and Co-Chief of the Division of
Immunology and Rheumatology at Stanford University Medical Center, about
the results of his study examining the long-term safety of tocilizumab in patients
with rheumatoid arthritis.
An Interview with Dr. Mark Genovese on the long-term safety of tocilizumab in patients with rheumatoid arthritis.

New Evidence in Rheumatology | January 2013 25
New Evidence: In which patients with RA treated with tocilizumab would monitoring be especially important?
Dr. Genovese: In all patients treated with tocilizumab it is important to monitor for typical safety signals
and treat accordingly. For example, in patients over 65 years with a history of diverticulitis and on oral
steroids, it is important to monitor closely for gastrointestinal (GI) perforations. In addition, in patients with
elevated low density lipoprotein levels, physicians may want to consider prescribing statins and monitoring for
cardiovascular events. In our study, we found no increase in AEs with the addition of statins during treatment
with tocilizumab.
New Evidence: Given the results of your study, how comfortable do you feel about the safety of tocilizumab?
Dr. Genovese: There do not appear to be any unique or new safety concerns appearing from this integrated safety
summary. We have followed the rate of AEs, serious AEs, infections, mortality, malignancies, GI perforations, and
laboratory abnormalities. Our study demonstrated that AEs reported with the use of tocilizumab remained stable
over time and were no greater than those seen in previous studies of this agent. In addition, the rate of AEs is
comparable in nature and frequency with that seen with other RA treatments.
Although these long-term results are reassuring, it would be helpful to have further data that could tell us which
patients should not be given particular agents. However, the benefit of giving tocilizumab in these patients outweighs
the cost and provides us with an additional option for treating this disease.
New Evidence: When in the treatment algorithm do you use tocilizumab?
Dr. Genovese: We use tocilizumab in patients who have failed tumor necrosis factor inhibitors as this was the
approved indication in the U.S. However, with the development of new labelling approvals in October, 2012,
we may use tocilizumab earlier in the treatment algorithm, such as in patients with an inadequate response to
disease-modifying antirheumatic drugs. I use tocilizumab monotherapy in 10% to 20% of my patients, as they
either cannot tolerate, or are inappropriate candidates for traditional small molecule therapies. Given the results
of our study, the safety of tocilizumab does not appear to be a barrier to using this agent earlier in the treatment
algorithm. However, cost and route of administration must also be considered when making treatment decisions.

26 New Evidence in Rheumatology | January 2013
Tumour necrosis factor inhibitors (TNF-Is) have proven to be very effective in patients who do not respond to traditional disease-modifying antirheumatic drugs.1 However, 20% to 40% of patients treated with TNF-Is either experience primary failure immediately or develop secondary failure over time. Treatment choices for patients experiencing TNF-I failure include switching to an alternative TNF-I, such as infliximab and etanercept, or to drugs with different underlying mechanism of action, such as rituximab and abatacept. Physicians faced with a choice between an alternative TNF-I and other drugs like rituximab and abatacept, make their decision based on factors that include efficacy, safety, mechanism of action and convenience of drug delivery, in addition to patient history and preference.
Rituximab is a chimeric monoclonal antibody against CD20 that has proven very effective in reducing the signs and symptoms of rheumatoid arthritis (RA).2,3 Rituximab is currently approved in Canada, the U.S., and Europe for treating patients with an inadequate response to one or more TNF-Is. Although the efficacy and safety of rituximab have been demonstrated in several randomized clinical trials, long-term data on safety, head-to-head comparisons with other biologics, and factors that help determine if rituximab is an appropriate alternative in patients who have failed treatment with a TNF-I failure are becoming clearer.
At ACR 2012, investigators presented studies on factors influencing the selection of rituximab treatments versus alternative TNF-Is in patients who failed one TNF-I, the efficacy of rituximab versus alternative therapies in patients who failed at least one TNF-I, and the long-term safety of rituximab in patients with RA.
The following is a report on five presentations given at ACR:
• A subanalysis of the SWITCH-RA study to determine reasons for the discontinuation of the initial TNF-I therapy and to identify factors that drive physicians to choose between rituximab and an alternative TNF-I in a subsequent therapy. Lack of efficacy was the main reason for discontinuation of an initial TNF-I, while safety profile and mode of administration were identified as important factors.
• A study examining the relationship of seropositivity status to efficacy of rituximab vs. alternative TNF-I therapies. Seropositive patients who were treated with rituximab achieved improved clinical efficacy compared with those who were treated with an alternative TNF-I.
• A 10-year follow-up study on the safety of rituximab in patients with RA. This study concluded that rituximab was well tolerated over time and multiple courses.
• A study evaluating the efficacy of rituximab in routine clinical practice in patients from the CORRONA (Consortium of Rheumatology Researchers of North America) registry. Data presented showed the use of rituximab in real-life settings to be as effective and safe as demonstrated in clinical trials.
• An evaluation of the relative efficacy of rituximab vs. abatacept in patients who had failed at least one TNF-I. The data suggest that in patients with RA who failed one or more TNF-Is, rituximab may result in better long-term survival than either abatacept or an alternative TNF-I.
Rituximab is More Effective than Abatacept and Alternative Tumour Necrosis Factor Inhibitors (TNF-Is) in Patients Who Have Failed TNF-Is
References: 1. Rubbert-Roth A, Finckh A. Treatment options in patients with rheumatoid arthritis failing initial TNF inhibitor therapy: a critical review. Arthritis Res Ther 2009;11 Suppl 1:S1. 2. Edwards JC, Szczepanski L, Szechinski J, et al. Efficacy of B-cell-targeted therapy with rituximab in patients with rheumatoid arthritis. N Engl J Med 2004;350:2572–81. 3. Buch MH, Smolen JS, Betteridge N, et al. Updated consensus statement on the use of rituximab in patients with rheumatoid arthritis. Ann Rheum Dis 2011;70:909–20.
Rituximab in Rheumatoid Arthritis Treatment

New Evidence in Rheumatology | January 2013 27
ACR/ARHP
Finckh A, et al. ACR 2012:456
Factors influencing choice of rituximab versus an alternative TNF inhibitor following TNF inhibitor failure in patients with rheumatoid arthritis: sub-analysis of a global, observational comparative effectiveness study
Background
Approximately 30% of patients with rheumatoid arthritis (RA) fail to achieve an American College of Rheumatology (ACR)20 response when treated with a tumour necrosis factor inhibitor (TNF-I).1 Over time, more patients either lose responsiveness or discontinue treatment due to adverse events. The options available to patients who have an inadequate response (IR) to TNF-Is include treatment with an alternative TNF-I and switching to a biologic therapy with a different mecha-nism of action. The factors associated with the selection of subsequent therapy, both from the physician and patient perspective, have not been evaluated in-depth.
The objective of this subanalysis of the SWITCH-RA study was to assess the reasons for discontinuation of the initial TNF-I therapy and to examine factors that drive physicians to choose between rituximab and an alternative TNF-I in a subsequent therapy.
Study design
• SWITCH-RA is a prospective, multicentre, global, observational study.
• Eligible patients were ≥18 years old and had started either rituximab or an alternative TNF-I following failure of a first TNF-I.
• Patients who had been treated with a second biologic therapy after a failure of one TNF-I for a period of up to four weeks were enrolled.
• Patients receiving a second biologic therapy within an RA clinical trial were excluded.
• The initial reasons for discontinuation of a first TNF-I and the physician’s rationale for subsequent therapy selection were recorded.
• The association between various factors and choice of rituximab or alternative TNF-I as a second biologic were analyzed using logistic regression with a stepwise method for variable selection.
The dependent variable was the type of second biologic (rituximab or alternative TNF-I).
Independent variables were medical rationale, characteristics of the new treatment, patient characteristics and physician characteristics.
Key findings
• A total of 1,111 patients were enrolled from 11 countries.
• Mean age and disease duration were approximately 55 and 8.3 years, respectively.
• Overall, 604 patients (54.4%) received rituximab and 507 (46.6%) received an alternative TNF-I as a second biologic.
• Most patients discontinued treatment due to inefficacy (74%): (Figure 1)
Primary inefficacy (40.8%);
Secondary inefficacy (59.2%);
Data were missing for 21 patients.
• Patients discontinued treatment due to intolerance (24%), which included allergic rash, pneumonia, and injection site reaction, and patient choice (2%).
• Factors most clearly associated with the selection of rituximab were generally related to the physician’s appreciation of treatment characteristics: (Figure 2)
Safety profile:
– No lymphoma risk;
– Low infection risk;
– Good long-term tolerance after infusion.
Administration profile:
– Low frequency of administration.
• Factors most clearly associated with the selection of an alternative TNF-I were related to:
Administration profile:
– Route of administration;
– Rapidity of action;
– Administration duration.
Patient characteristics:
– Treatment compatibility with professional life.

28 New Evidence in Rheumatology | January 2013
Figure 1. Reasons for discontinuation of initial TNF-I
Inefficacy* (n = 827)
* Primary inefficacy (n = 329, 40.8%), secondary inefficacy (n = 477, 59.2%), data were missing for 21 patients. Primary and secondary inefficacy assessed by individual investigators.
TNF-I = tumour necrosis factor inhibitor
74%
24%
2%
Primary40.8%
Secondary59.2%
Intolerance (n = 263)
Other reason (n = 21)
Figure 2. Factors associated with selection of rituximab versus an alternative TNF-I
Odds ratio (95% CI)
1.8 (1.3–2.4)
2.1 (1.5–3.0)
2.1 (1.5–2.9)
0.2 (0.1–0.3)
0.4 (0.2–0.8)
0.1 (0.1–0.2)
4.4 (2.9–6.6)
4.1 (2.4–7.1)
2.4 (1.5–3.9)
4.6 (2.3–9.5)
2.1 (1.2–3.5)
0.4 (0.3–0.7)
0.5 (0.4–0.8)
0.5 (0.3–0.9)
In favour ofrituximab
In favour ofalternative TNF-I
Medical rationale
RA disease (RF and CCP status)
Primary failure
New treatment characteristics
Efficient treatment after first TNF-I
Rapidity of action
Administration of duration
Route of administration
Low frequency of administration
Good long-term tolerance after infusion
Low infectious risk
No lymphoma risk
Well-organized treatment administration by MD
Patient characteristics
Compatible treatment with patient’s professional life
Patient’s option for treatment
Patient’s option for follow-up
Stepwise variable selection technique was used to obtain the selected set of explanatory factors that were used in the multivariate logistic regression.
CCP = cyclic citrullinated protein; CI =confidence interval; MD = medical doctor; RA = rheumatoid arthritis; RF = rheumatoid factor; TNF-I = tumor necrosis factor inhibitor
110100 0.1
New Evidence in Rheumatology | January 2013 29
ACR/ARHP
Key conclusions
■ The lack of efficacy of the initial TNF-I in the SWITCH-RA study, particularly over time, was the main reason for discontinuation of the initial TNF-I treatment.
■ Factors associated with the selection of rituximab over an alternative TNF-I tended to be associated with the physician’s appreciation of treatment characteristics related to the drug’s long-term safety profile and low frequency of administration.
■ Factors associated with the selection of an alternative TNF-I were primarily associated with drug administration and patient characteristics.
Reference: 1. Finckh A, Gottenberg J-E, Mpofu C, et al. Factors influencing choice of rituximab versus an alternative tumor necrosis factor inhibitor following tumor necrosis factor inhibitor failure in patients with rheumatoid arthritis: sub-analysis of a global, observational comparative effectiveness study. ACR Annual Meeting Abstracts 2012;64:456.
Rubbert-Roth A, et al. ACR 2012:467
Seropositive patients with rheumatoid arthritis who had an inadequate response to TNF inhibitors achieve improved clinical effectiveness after switching to rituximab versus switching to an alternative TNF inhibitor
Background
Tumor necrosis factor inhibitors (TNF-Is) are effective in
improving the signs and symptoms as well as slowing
or preventing structural damage in patients with
rheumatoid arthritis (RA).1 However, approximately
20% to 40% of patients experience an inadequate
response (IR) to TNF-I treatments. Recent evidence
indicates that following TNF-I failure, switching to
rituximab may be more effective than switching to an
alternative TNF-I. Patients who are seropositive have
been shown to achieve greater clinical responses to
rituximab than those who are seronegative.
The objective of the study was to compare the relative
effectiveness of rituximab versus an alternative TNF-I
according to serological status.
Study design
• SWITCH-RA, a global, multicentre, prospective,
observational, clinical trial, evaluated the relative
effectiveness of rituximab vs. an alternative TNF-I in
patients with an IR to a single previous TNF-I.
• The primary endpoint was the change from
baseline over six months in the 28-joint disease
activity score (DAS28) based on DAS28-3-erythrocyte
sedimentation factor (ESR).
• Eligible patients were ≥18 years old and had started either rituximab or an alternative TNF-I following an IR to a first TNF-I.
• Patients who had been treated with a second biologic therapy for a period of up to four weeks were enrolled.
• Patients who were rheumatoid factor (RF) positive and/or anticyclic citrullinated protein (CCP) positive were defined as seropositive.
• Analysis of covariance adjusted for unbalanced baseline characteristics was used for treatment cohort comparisons, with missing DAS28-3-ESR values imputed with nearest time point values.
Key findings
• Patients (n = 728) who completed six months of therapy with a second biologic were included in this analysis (rituximab = 405; TNF-I = 323).
• The proportion of patients who were seropositive was higher in the rituximab group compared with the alternative TNF-I group (RF = 82.7% vs. 67.0%; anti-CCP = 66.3% vs. 62.0%).
• The baseline DAS28-3-ESR scores in seropositive and seronegative patients at the time of switching were significantly higher in the rituximab group than in the alternative TNF-I group.

30 New Evidence in Rheumatology | January 2013
Figure 2. Changes in DAS28-3-ESR over six months, overall, and by reason for discontinuation of initial TNF-I in seropositive patients*
Mea
n c
han
ge
in D
AS2
8-3-
ESR
(SE
)
–1.6
–1.2
331n= 228
–2.0
–2.2
–2.4
–1.6
–0.2
–1.2
–0.8
–0.4
–1.8
–1.4
–1.0
–0.6
0.0
Alternative TNF-I
Overall
Rituximab
–1.9
–1.5
253 171
Switch due to inefficacy
–0.5 –0.5
74 51
Switch due to intolerance
p = 0.011 p = 0.021 p = 0.997
*Analyses adjusted for baseline value, propensity score, and other covariates found to be statistically significantly different between the two groups at baseline. DAS28-3-ESR least squares means.
DAS28 = 28-disease activity score based on DAS28-3 which excludes patient’s global health component; ESR = erythrocyte sedimentation rate; SE = standard error; TNF-I = tumour necrosis factor inhibitor.
• The mean duration of all previous TNF-I therapies were similar: 25.4 (standard deviation [SD] = 25.5) and 25.1 (SD = 26.5) months for patients treated with rituximab and patients treated with an alternative TNF-I, respectively.
• In patients who were seropositive, rituximab significantly reduced the DAS28-3-ESR score at six months compared with the alternative TNF-I treatment. (Figure 1)
There were no significant improvements in DAS28-3-ESR at six months in patients who were seronegative.
• Decreases in ESR (least square mean [standard error]) at six months were greater in patients who were seropositive and receiving rituximab than in those receiving an alternative TNF-I (–14.4 [4.5] vs. –7.3 [4.8], p = 0.006).
Corresponding results in patients who were seronegative were not statistically significant (–13.4 [8.3] vs. –10.4 [9.0], p = 0.582).
• The benefit of rituximab treatment varied in patients who were seropositive according to the reason for interrupting the previous TNF-I treatment. (Figure 2)
Patients who were seropositive who discontinued a first TNF-I treatment due to inefficacy achieved significantly better responses with rituximab compared with those receiving an alternative TNF-I.
Responses in patients who were seropositive who discontinued a first TNF-I treatment due to intolerance did not significantly differ between the two treatment groups.
Figure 1. Changes in DAS28-3-ESR over six months in seropositive and seronegative patients*
Mea
n c
han
ge
in D
AS2
8-3-
ESR
(SE
)–1.6
–1.2–1.3
–1.1
331n= 228 74 95
–2.0
–1.6
–0.2
–1.2
–0.8
–0.4
–1.8
–1.4
–1.0
–0.6
0.0
Alternative TNF-I
Seropositive
Rituximab
Seronegative
p = 0.011 p = 0.449
*Analyses adjusted for baseline value, propensity score, and other covariates found to be statistically significantly different between the two groups at baseline. DAS28(3)-ESR least squares means.
DAS28 = 28-disease activity score based on DAS28-3 which excludes patient’s global health component; ESR = erythrocyte sedimentation rate; SE = standard error; TNF-I = tumour necrosis factor inhibitor.
New Evidence in Rheumatology | January 2013 31
ACR/ARHP
Key conclusions
■ Patients who were seropositive who switched to rituximab after discontinuing their first TNF-I achieved significant improvements at six months compared with those who switched to an alternative TNF-I.
• Improvements were particularly evident in those discontinuing their initial TNF-I therapy due to inefficacy.
■ Over the six-month period of the study, no differences in efficacy between rituximab and an alternative TNF-I were seen in patients who were seronegative.
Reference: 1. Rubbert-Roth A, Finckh A, Sarzi-Puttini P, et al. Seropositive rheumatoid arthritis patients with an inadequate response to TNF inhibitors achieve improved clinical effectiveness after switching to rituximab versus switching to an alternative TNF inhibitor. ACR Annual Meeting Abstracts 2012;64:467.
van Vollenhoven RF, et al. ACR 2012:459
Long-term safety of rituximab: 10-year follow-up in the rheumatoid arthritis global clinical trial program
Background
The long-term safety of rituximab treatment in patients
with rheumatoid arthritis (RA) is continuing to be
established.1 The objective of this study was to evaluate
the long-term safety of rituximab in RA clinical trials.
Study design
• This was a pooled observed case analysis of safety
data in patients with moderate-to-severe active RA
treated with rituximab plus methotrexate that was
part of a global clinical trial program.
The global clinical trial program comprised eight
randomized clinical trials, two long-term open-label
extensions, and one open-label prospective study.
• Repeat treatments of rituximab were based on the
physician’s decision of clinical need and included
evidence of active disease (either swollen/tender joint
counts ≥eight or a 28-disease activity score of ≥2.6).
• Each course of rituximab consisted of two courses
of either 1,000 mg or 500 mg given intravenously
(iv) two weeks apart.
• Prior to each rituximab infusion, all patients
received methylprednisolone 100 mg iv; most patients
also received acetaminophen and an antihistamine.
• All patients received concomitant methotrexate at a
stable dose of 10 to 25 mg/week.
Key findings
• As of September 2011, 3,595 patients had received up
to 19 courses of rituximab over a period of 10 years.
• The number of patients available for analysis was:
Rituximab all-exposure: 3,595 (14,008 patient-
years [pt-years]);
Long-term population: 1,145 (7,716 pt-years);
Pooled placebo group: 818 (1,107 pt-years).
• Rates of adverse events (AEs) and serious AEs (SAEs)
were similar in the all-exposure, five-year follow-up,
and placebo populations.
• The rate of all AEs over time was highest during the
first six months after the first exposure to rituximab,
in part due to infusion-related reactions (IRRs),
which predominantly occurred with the first infusion
of the first course. (Figure 1)
Thereafter, rates of AEs and SAEs remained stable,
irrespective of the number of courses of treatment
received. (Figure 2, Table 2)
• The overall rates of all infections and serious infection
events (SIEs) were similar across the analysis of the
populations. (Table 1)
• The rate of confirmed malignancies (excluding
non-melanoma skin cancers) was similar to rates in
the general RA population.2,3,4 (Table 3)

32 New Evidence in Rheumatology | January 2013
Table 1. Summary of adverse events rates per 100 patient-years
RTX All-Exposure(n = 3,595)
RTX long-term ( >5 years) (n = 1,145)
Pooled placebo(n = 818)
Exposure (pt-years) 14,008 7,716 1,107
AE rate (95% CI) 249.34 (246.74–251.97) 237.25 (233.83–240.71) 315.43 (305.14–326.06)
SAE rate (95% CI) 14.03 (13.42–14.66) 12.25 (11.49–13.05) 13.82 (11.79–16.19)
Infection rate (95% CI) 78.60 (77.14–80.08) 75.10 (73.19–77.06) 90.39 (84.96–96.17)
SIE rate (95% CI) 3.8 (3.50–4.14) 2.76 (2.41–3.16) 3.79 (2.80–5.13)
AE = adverse event; CI = confidence interval; SAE = serious adverse event; SIE = serious infection event; RTX = rituximab
Figure 1. Incidence of infusion-related reactions by treatment course
Figure 2. Rates of adverse events over time: one-year increments (all-exposure population)
Course 1 Course 2 Course 3 Course 4 Course 5 Course 6 Course 7 Course 8 Course 9 Course 10
Pati
ents
wit
h a
ny
IRR
(%
)22
12
9 9
78
5 54 3 3
7
2
5
2
5
2
54
2
0
5
10
15
20
25First infusion
In courses 1–10, 17 patients reported 19 serious IRRs. The proportion of patients experiencing serious IRRs was 0.5% (17/3,595), with 11, 5, 0, 1, 1, 1, 0, 0, 0, and 0 events occurring per course, respectively.
3,595 2,750 1,744 1,471 1,202 906 709 502 323 1513,523 2,689 1,718 1,449 1,168 890 684 493 318 146
Second infusion
INF = infusion; IRR = infusion-related reactions
1st inf: n =2nd inf: n =
0–1 >1–2 >2–3 >3–4 >4–5
Time (years)
>5–6 >6–7 >7–8 >8–9
Rat
e o
f ev
ents
/100
pt-
year
s
0
100
200
300
400
500
3,496 3,086 2,278 1,788 1,368 799 529 408 136
Annual rate of adverse events
Annual rate of serious adverse events
pt-years = patient years
Total pt-yearsexposure

New Evidence in Rheumatology | January 2013 33
ACR/ARHP
Key conclusions
■ No new safety signals were observed with increasing duration of exposure, including among patients with >five years of follow up.
■ Rituximab remains well tolerated over time as well as over multiple treatment courses.
■ IRRs predominantly occurred during the first infusion of the first course and were rarely serious.
■ Serious and non-serious infection rates were similar to previous analyses and did not increase over time or course.
■ The use of subsequent biologics, including tumour necrosis factor inhibitors, in patients with RA previously treated with rituximab, was not associated with an increased SIE rate.
■ Rates of myocardial infarctions and malignancies were consistent with those observed in epidemiological data from other RA cohorts.
■ Apart from IRRs, the overall safety profile of rituximab remains similar to that of the pooled placebo population as well as consistent with the published data of patients with moderate-to-severe RA.
References: 1. van Vollenhoven RF, Emery P, Bingham CO, et al. Long-term safety of rituximab: 10-year follow-up in the rheumatoid arthritis global clinical trial program. ACR Annual Meeting Abstracts 2012;64:459. 2. Mellemkjaer L, Linet MS, Gridley G, et al. Rheumatoid arthritis and cancer risk. Eur J Cancer 1996;32A(10):1753-1757. 3. Wolfe F. Michaud K. Biologic treatment of rheumatoid arthritis and the risk of malignancy: analyses from a large US observational study. Arthritis Rheum 2007;56(9):2886–2895. 4. Smitten A, Simon AT, Hochberg CM, et al. A meta-analysis of the incidence of malignancy in adult patients with rheumatoid arthritis. Arthritis Res Ther 2008;10(2):R45.
Table 2. SIEs rates before and after treatment with biologics and TNF-Is
All patients receiving any biologic following RTX treatment (n = 331)
Subset of patients receiving a TNF-I following RTX treatment (n = 268)
Before other biologic After other biologic Before TNF-I After TNF-I
Total exposure (pt-years) 593. 45 445.58 442.56 361.18
SIEs, n 29 19 23 13
SIEs/100 pt-years (95% Cl)
4.89(3.40–7.03)
4.26(2.72–6.69)
5.20(3.45–7.82)
3.60(2.09–6.20)
CI = confidence interval; pt-years = patient-years; RTX = rituximab; SIE = serious infection events; TNF-I = tumour necrosis factor inhibitor
Table 3. Rate of malignancy and incidence ratio for malignancy in rituximab all-exposure population and published data in adults with RA
Rate (per 100 pt-years)
Any site* Breast†
RTX (All-Exposure) (95% CI) 0.72 (0.59–0.87) 0.11 (0.07–0.18)
RA observational studies Danish Cancer Registry2
National Databank for Rheumatic Diseases3
1.171.30
0.130.21
Standardized incidence ratio
Any site* Breast†
Malignancy incidence in RTX-treated RAAll-exposure population‡ (95% CI)
1.01 (0.83–1.23) 0.64 (0.36–1.03)
Meta-analysis of malignancy incidence in adult patients with RA (95% CI)4
1.05 (1.01–1.09) 0.84 (0.79–0.90)
* Excluding non-melanoma skin cancer and non-malignant events† Only female patients‡ Surveillance Epidemiology and End Results database was used to obtain age- and sex-specific incidence ratio of malignancies for the U.S. general population for standardized incidence ratio calculations
CI = confidence interval; pt-years = patient-years; RA = rheumatoid arthritis; RTX = rituximab

34 New Evidence in Rheumatology | January 2013
Harrold L. et al. ACR 2012:464
Rituximab for the treatment of rheumatoid arthritis: treatment effectiveness in the CORRONA database
Background
In the U.S., rituximab in combination with methotrexate is approved for the treatment of moderate-to-severe active rheumatoid arthritis (RA) after failure of at least one tumour necrosis factor inhibitor (TNF-I). Although the efficacy and safety of rituximab in patients with RA have been demonstrated in two phase III studies, little is known regarding the efficacy of rituximab in adult patients with RA in routine clinical practice.1
The objective of this study was to evaluate the use of rituximab and assess its efficacy in routine clinical practice in the prospective CORRONA (Consortium of Rheumatology Researchers of North America) registry.
Study design
• The CORRONA registry is an independent, prospective, observational cohort with 34,269 patients with RA recruited in 39 states at more than 150 sites in the U.S.
• As of September 2012, data have been collected from both patients and rheumatologists, yielding 224,691 patient visits.
• Eligible patients were prior TNF-I users who had started on rituximab for the first time and who were not in remission at the time of rituximab initiation.
• The efficacy and safety outcomes of rituximab one year after rituximab initiation included clinical
disease activity index (CDAI), achievement of remission or low disease activity (LDA) based on CDAI, safety event rates, serious infections, and malignancies.
• Levels of disease activity were defined by CDAI (0–76.0), a composite index composed of swollen joint count (SJC; 0–28), tender joint count (TJC; 0–28), patient global disease activity (visual analog scale [VAS] = 0–10.0 cm) and physician global disease activity (VAS, 0–10.0 cm). The cutoff points for each disease activity level were:
Remission = CDAI ≤2.8;
LDA = 2.8 <CDAI ≤10;
Moderate disease activity = 10 <CDAI ≤22;
High disease activity = CDAI >22.
Key findings
• At the start of the study, approximately 72% of patients started rituximab in combination with one or more nonbiologic disease-modifying anti-rheumatic drug(s).
• Approximately 67% of patients were treated with multiple courses of rituximab and 33% of patients were not re-treated.
• At 12 months, approximately 11% of patients achieved CDAI remission, 33% achieved LDA, 28% achieved moderate disease activity, and 28% achieved high disease activity. (Figure 1)
Figure 1. Disease activity at baseline and 12 months among all patients who were initiated on rituximab
0
10.9%10
0
20
30
40
50
6012 monthsBaseline
17.7%
32.8%32.1%
27.9%
50.2%
28.3%
Remission (CDAI ≤2.8)
Disease activity
Low (CDAI ≤10) Moderate (CDAI ≤22) High (CDAI >22)
CDAI = clinical disease activity index`
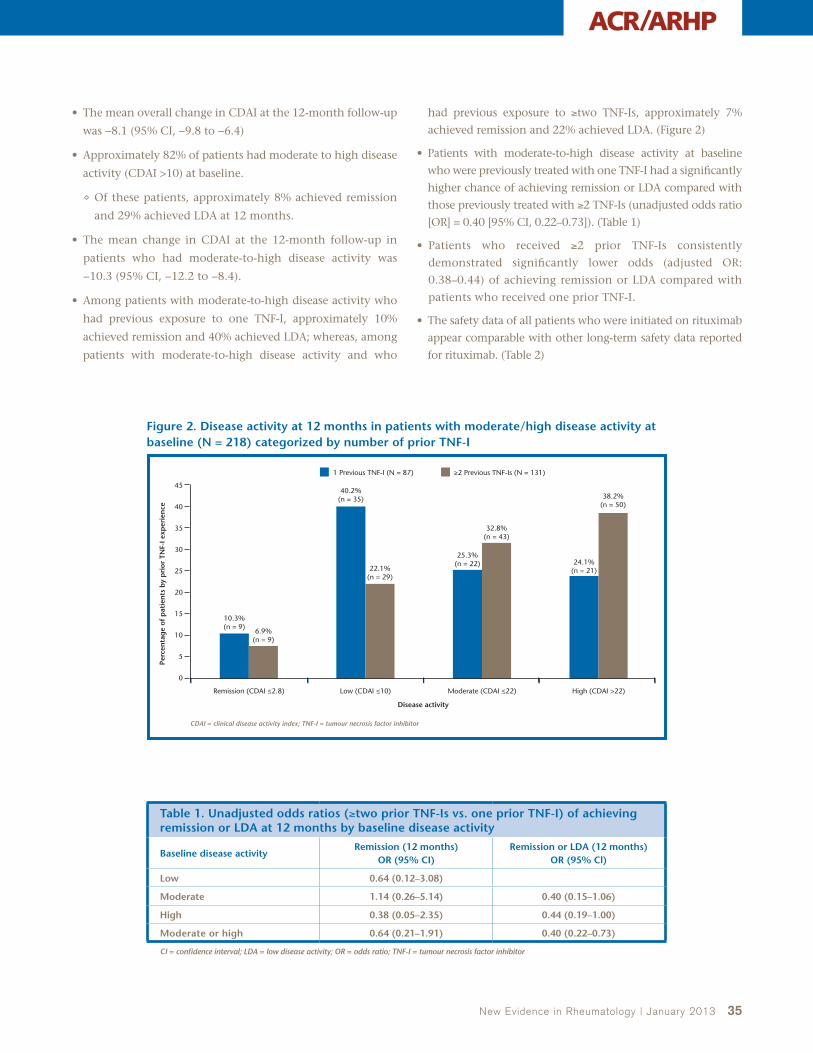
New Evidence in Rheumatology | January 2013 35
ACR/ARHP
• The mean overall change in CDAI at the 12-month follow-up
was −8.1 (95% CI, −9.8 to −6.4)
• Approximately 82% of patients had moderate to high disease
activity (CDAI >10) at baseline.
Of these patients, approximately 8% achieved remission
and 29% achieved LDA at 12 months.
• The mean change in CDAI at the 12-month follow-up in
patients who had moderate-to-high disease activity was
−10.3 (95% CI, −12.2 to −8.4).
• Among patients with moderate-to-high disease activity who
had previous exposure to one TNF-I, approximately 10%
achieved remission and 40% achieved LDA; whereas, among
patients with moderate-to-high disease activity and who
had previous exposure to ≥two TNF-Is, approximately 7%
achieved remission and 22% achieved LDA. (Figure 2)
• Patients with moderate-to-high disease activity at baseline
who were previously treated with one TNF-I had a significantly
higher chance of achieving remission or LDA compared with
those previously treated with ≥2 TNF-Is (unadjusted odds ratio
[OR] = 0.40 [95% CI, 0.22–0.73]). (Table 1)
• Patients who received ≥2 prior TNF-Is consistently
demonstrated significantly lower odds (adjusted OR:
0.38–0.44) of achieving remission or LDA compared with
patients who received one prior TNF-I.
• The safety data of all patients who were initiated on rituximab
appear comparable with other long-term safety data reported
for rituximab. (Table 2)
Figure 2. Disease activity at 12 months in patients with moderate/high disease activity at baseline (N = 218) categorized by number of prior TNF-I
6.9%(n = 9)
5
0
10
15
20
35
40
30
25
45
≥2 Previous TNF-Is (N = 131)1 Previous TNF-I (N = 87)
40.2%(n = 35)
10.3%(n = 9)
22.1%(n = 29)
25.3%(n = 22)
32.8%(n = 43)
24.1%(n = 21)
38.2%(n = 50)
Remission (CDAI ≤2.8)
Disease activity
Perc
enta
ge
of p
atie
nts
by
pri
or T
NF-
I exp
erie
nce
Low (CDAI ≤10) Moderate (CDAI ≤22) High (CDAI >22)
CDAI = clinical disease activity index; TNF-I = tumour necrosis factor inhibitor
Table 1. Unadjusted odds ratios (≥two prior TNF-Is vs. one prior TNF-I) of achieving remission or LDA at 12 months by baseline disease activity
Baseline disease activityRemission (12 months)
OR (95% CI)Remission or LDA (12 months)
OR (95% Cl)
Low 0.64 (0.12–3.08)
Moderate 1.14 (0.26–5.14) 0.40 (0.15–1.06)
High 0.38 (0.05–2.35) 0.44 (0.19–1.00)
Moderate or high 0.64 (0.21–1.91) 0.40 (0.22–0.73)
CI = confidence interval; LDA = low disease activity; OR = odds ratio; TNF-I = tumour necrosis factor inhibitor
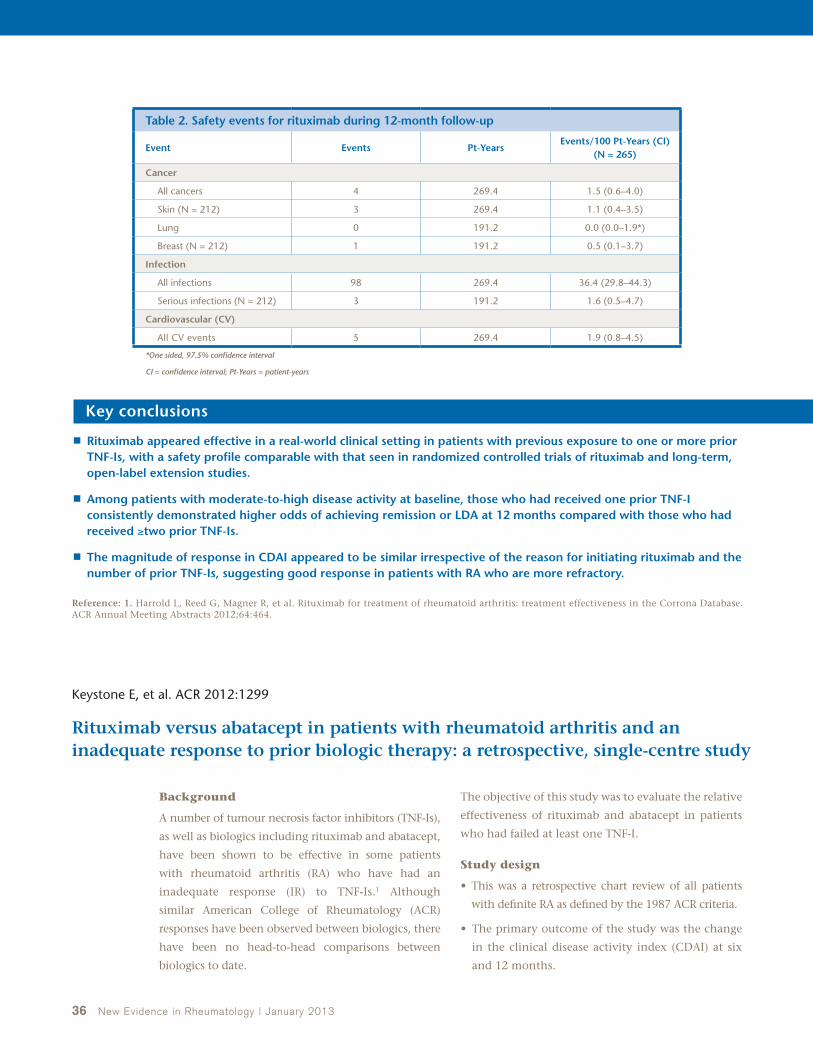
36 New Evidence in Rheumatology | January 2013
Reference: 1. Harrold L, Reed G, Magner R, et al. Rituximab for treatment of rheumatoid arthritis: treatment effectiveness in the Corrona Database. ACR Annual Meeting Abstracts 2012;64:464.
Key conclusions
■ Rituximab appeared effective in a real-world clinical setting in patients with previous exposure to one or more prior TNF-Is, with a safety profile comparable with that seen in randomized controlled trials of rituximab and long-term, open-label extension studies.
■ Among patients with moderate-to-high disease activity at baseline, those who had received one prior TNF-I consistently demonstrated higher odds of achieving remission or LDA at 12 months compared with those who had received ≥two prior TNF-Is.
■ The magnitude of response in CDAI appeared to be similar irrespective of the reason for initiating rituximab and the number of prior TNF-Is, suggesting good response in patients with RA who are more refractory.
Table 2. Safety events for rituximab during 12-month follow-up
Event Events Pt-Years Events/100 Pt-Years (CI)
(N = 265)
Cancer
All cancers 4 269.4 1.5 (0.6–4.0)
Skin (N = 212) 3 269.4 1.1 (0.4–3.5)
Lung 0 191.2 0.0 (0.0–1.9*)
Breast (N = 212) 1 191.2 0.5 (0.1–3.7)
Infection
All infections 98 269.4 36.4 (29.8–44.3)
Serious infections (N = 212) 3 191.2 1.6 (0.5–4.7)
Cardiovascular (CV)
All CV events 5 269.4 1.9 (0.8–4.5)
*One sided, 97.5% confidence interval
CI = confidence interval; Pt-Years = patient-years
Keystone E, et al. ACR 2012:1299
Rituximab versus abatacept in patients with rheumatoid arthritis and an inadequate response to prior biologic therapy: a retrospective, single-centre study
Background
A number of tumour necrosis factor inhibitors (TNF-Is),
as well as biologics including rituximab and abatacept,
have been shown to be effective in some patients
with rheumatoid arthritis (RA) who have had an
inadequate response (IR) to TNF-Is.1 Although
similar American College of Rheumatology (ACR)
responses have been observed between biologics, there
have been no head-to-head comparisons between
biologics to date.
The objective of this study was to evaluate the relative
effectiveness of rituximab and abatacept in patients
who had failed at least one TNF-I.
Study design
• This was a retrospective chart review of all patients
with definite RA as defined by the 1987 ACR criteria.
• The primary outcome of the study was the change
in the clinical disease activity index (CDAI) at six
and 12 months.

New Evidence in Rheumatology | January 2013 37
ACR/ARHP
• Rituximab or abatacept was initiated after failure of one or more TNF-Is.
• CDAI remission was defined as CDAI <2.8 and low disease state (LDAS) was defined as >2.8 <CDAI <10.
• Baseline differences between rituximab and abatacept with respect to tender joint count (TJC) and swollen joint count (SJC) were adjusted for demographics including age, sex, number of biologics, disease-modifying anti-rheumatic drug (DMARD) failures, and disease duration.
• The relative efficacy of rituximab and abatacept was evaluated by analyzing drug survival distribution.
• Kaplan-Meier survival curves were compared using the log rank test (p-values <0.05 indicated statistical significance).
Key findings
• The study cohort comprised 61 patients.
Of these patients, 37 were treated with rituximab and 24 with abatacept.
In the rituximab group, 10 patients received prior therapy with abatacept.
• Patients treated with rituximab had a higher disease activity compared with patients treated with abatacept (with or without prior abatacept treatment). (Tables 1 and 2)
• After excluding patients treated with rituximab who had
received prior abatacept, the survival rates of patients treated
with rituximab were generally better over time than those
treated with abatacept. (Figure 1, Table 3)
Overall, survival distribution was not significantly
different between the rituximab and abatacept groups
(p = 0.658); however, patients who were treated with
rituximab who also failed abatacept had significantly
reduced survival compared with those who were not
treated with abatacept (p = 0.015).
Table 1. Mean change of CDAI and SJC at different time points including abatacept failure
Subject group Month 6 Month 12
CDAI change ABA –4.4 (n = 18) –12.4 (n = 5)
CDAI change RTX –1.6 (n = 20) 1.7 (n = 13)
SJC change ABA –1.5 (n = 22) –3.2 (n = 6)
SJC change RTX –1.1 (n = 26) –1.2 (n = 17)
ABA = abatacept; CDAI = clinical disease activity index; RTX = rituximab; SJC = swollen joint count
Table 2. Mean change of CDAI and SJC at different time points excluding abatacept failure
Subject group Month 6 Month 12
CDAI change ABA –4.4 (n = 18) –12.4 (n = 5)
CDAI change RTX –0.75 (n = 20) 2.7 (n = 10)
SJC change ABA –1.5 (n = 22) –3.2 (n = 6)
SJC change RTX –0.7 (n = 26) –0.7 (n = 13)
ABA = abatacept; CDAI = clinical disease activity index; RTX = rituximab; SJC = swollen joint count
Figure 1. Rituximab versus abatacept survival analysis
RTX w/o ABA (n = 27)
All RTX (n = 37)
ABA (n = 24)
RTX prior ABA (n = 10)
All RTX vs ABA, p = 0.658RTX w/o ABA vs ABA, p = 0.226
RTX w/o ABA vs RTX with prior ABA, p = 0.015
Pro
po
rtio
n o
f su
bje
cts
rem
ain
ing
on
dru
g
Years
0.0
0.0 0.5 1.0 1.5 2.0 2.5 3.0 3.5 4.0
0.8
1.0
0.6
0.4
0.2
ABA = abatacept; RTX = rituximab; w/o = without
Table 3. Estimated survival rate of rituximab (n = 27) and abatacept (n = 24) at different time points excluding abatacept failure
Time (years) Rituximab (n = 27) Abatacept (n = 24)
0.5 0.92 0.83
1 0.79 0.74
1.5 0.74 0.54
2 0.68 0.54
3 0.68 0.54
4 0.68 0.41

38 New Evidence in Rheumatology | January 2013
Canadian Perspective by Dr. Janet Pope
Rituximab presents a good second-line biologic option for patients with rheumatoid arthritis (RA). In my clinic, I typically use rituximab after treatment with at least one tumor necrosis factor inhibitor (TNF-I) in patients with active RA. Although it shows a good response, particularly in patients with RA who are rheu-
matoid factor (RF)-positive and/or anti-cyclic citrullinated peptide (CCP)-positive, I do not restrict rituximab use to this population; my goal is to try to elicit a good response from most patients. However, preferentially, those with positive antibodies (RF and/or anti-CCP) are more likely to have a good response. I also use rituximab as a first-line biologic in patients who have a relative or absolute contraindication to TNF-Is, mainly in patients with a past history of lymphoma or high tuberculosis (TB) risk (such as latent TB infection) where isoniazid treatment is not tolerated or contraindicated, and in patients where there is a concern of developing multiple sclerosis (where TNF-Is may increase the risk slightly).
Some patients with RA treated with rituximab respond quite quickly and usually we know by eight to 12 weeks how well they will respond. In many patients, giving another course of rituximab leads to further improvement. Once patients achieve a low disease state or remission, we generally wait until they start flaring to retreat. After that we try to establish a treatment interval unique to each individual. Patients are usually comfortable with the treatment and time to response but are less comfortable in determining when they need to be retreated so we have to better train them. In cases where
the treatment interval has been determined, we should continue with that schedule (for example if a patient flares at 10 months after obtaining remission, then retreatment may be every nine months to prevent further flares).
Although there are many biologic options for patients with RA, rituximab is different in many aspects. Mechanistically, it depletes B cells. It is given intravenously, and while this is similar to other agents, such as abatacept or tocilizumab, rituximab is given as two doses followed by intermittent administration (six months or longer) as opposed to abata-cept and tocilizumab which are given as monthly infusions (although subcutaneous preparations of each are pending approval in Canada). Rituximab is a good treatment option, therefore, in patients who do not want to be treated frequent-ly and who are not comfortable with subcutaneous injections. Based on this, and for many other reasons, rituximab seems to be a patient-centred second-line biologic treatment. The benefit of rituximab is similar to other post-TNF-I approved drugs, but the safety profile is different in that a past history of tuberculosis and cancer (especially lymphoproliferative cancers) are not contraindicated, and while some patients do have infusion reactions, in general, these can be well managed.
With the various treatment choices now available for RA, it would be important to determine the long-term efficacy and safety of rituximab and when it is an appropriate option for treating patients with RA who have had an inadequate response (IR) to TNF-Is.
Finckh and colleagues examined the reasons for discon-tinuation of the initial TNF-I therapy and the factors that determined whether the subsequent therapy would be rituximab or an alternative TNF-I. The factors involved in
38 New Evidence in Rheumatology | September 2012
Reference: 1. Keystone E, Weber D, Xiong J, et al. Rituximab versus abatacept in rheumatoid arthritis patients with an inadequate response to prior biologic therapy: a retrospective, single-center study. ACR Annual Meeting Abstracts 2012;64:1299.
Key conclusions
■ Stratification of survival data according to the number of prior TNF-I failures indicated that rituximab (excluding patients who were treated with prior abatacept) was superior to abatacept among patients who failed three TNF-Is.
■ Survival was also numerically greater with rituximab vs. abatacept in patients who failed one prior TNF-I.
■ These results from real-life practice suggest that in patients with RA who failed one or more TNF-Is, rituximab may result in better long-term survival than either abatacept or an alternative TNF-I.
■ Prior abatacept treatment appears to reduce the efficacy of rituximab.
ACR/ARHP
the discontinuation of a TNF-I were mainly inefficacy, safety, and route of administration. These results were quite similar to what is seen in our Canadian clinical practice. The only caveat to what the Finckh study showed is that in registries, if patients stop a TNF-I due to safety reasons such as infusion reactions, or injection site reactions, or hospitalization due to pneumonia, they will have a high chance of a good response to the next biologic in terms of benefit and safety, generally irrespective of the next biologic used. The factors identified that drove physicians to select rituximab versus an alternative TNF-I reflected Canadian practice with some switching being data driven (patients who were RF positive, and/or with a poor response to an initial TNF-I, were more likely to be treated next with rituximab). The study was large and provided insight into how our colleagues think when making treatment changes, but it is unfortunate that it was not a randomized controlled trial which might have given us even more insight into the effectiveness and efficacy of the second biologic that patients will receive. It would be interesting to identify other factors, such as biomarkers in the blood, which would predict a better response of one drug over another within an individual. With the many choices available, we sometimes use drugs in RA based on the order of approval and comfort level. Consequently, a huge breakthrough in pharmacogenomics in the field could lead to better individualized treatment.
Rubbert-Roth and colleagues showed improved clinical efficacy in seropositive patients with an IR to TNF-Is who were then treated with rituximab versus those who were next treated with an alternative TNF-I. Studies using rituximab have consistently shown a better response (American College of Rheumatology [ACR]50 and ACR70 responses) in patients who are RF positive than in those who are RF negative. However, in some patients who are RF negative and who have tried different treatments that did not work adequately, I would consider using rituximab although the likelihood of achieving remission is less than in RF-positive patients.
I think the impact of this study will depend on the physician. For some, it will solidify the way they were thinking. They will move rituximab up on the scale and use it more often as a second biologic, particularly in seropositive patients; this will be especially true for clinicians who have easy access to rituximab. Others will probably keep it on the scale wherever it is, especially if it was working well for them within the treatment algorithm they have used.
Long term safety in patients with RA treated with multiple courses of rituximab was presented by van Vollenhoven et al. The study involved a large number of patients who received repeat infusions of rituximab for up to 10 years of follow-up. The safety results were very reassuring since no new safety issues occurred over time. One fear was that when immuno-globulin (Ig) (IgG and IgM) levels become low, patients might develop more infections, but the results showed a stable
serious infection (SI) rate in over 1,100 patients who had received more than five years of retreatment. Clearly, these patients were being retreated because they were benefitting from rituximab. Although it was a safety study and not dealing with efficacy and effectiveness, it was evident that some patients could be retreated repeatedly with ongoing efficacy. I think for clinicians who may have been hesitant about retreatment over time, this study helps to understand that the SI rates and infusion reactions were stable and not rising over time. It is also important to note that there did not seem to be any cancer signals with the rituximab treatment.
Harrold and colleagues evaluated the efficacy of rituximab in routine clinical practice using the CORRONA (Consortium of Rheumatology Researchers of North America) registry and found that it was effective and safe in patients who had received a prior TNF-I. Based on the study results, physi-cians can consider rituximab after one, two, or more TNF-Is and achieve a good response; whether it will be a sustained response is not clear because the CORRONA database has not followed patients long enough to answer that question. The safety results were also consistent with other studies and databases, which was reassuring. One finding in the study that may have been surprising to some clinicians was that one quarter of the patients were receiving rituximab as mono-therapy; rituximab is approved for use in combination with methotrexate. However, this goes hand in hand with what is done in the real-life setting with other drugs approved in combination with methotrexate.
Keystone and colleagues showed that rituximab treatment led to better long-term survival than abatacept in patients with RA who failed one or more TNF-I. It was also observed that prior abatacept treatment decreased rituximab efficacy. While the results were interesting, the trial was not randomized, was a single-site study with small numbers, and all the factors that led to prescribing one drug over the other were not known. We need to look at more databases and larger numbers to see whether the findings would be consistent among clinics. It would be useful to determine if the British Society for Rheu-matology Biologics Register, the Ontario Biologics Research Initiative, and other sites in Canada have similar data. It would also be important to have double-blind randomized controlled trials evaluating abatacept versus rituximab to determine the differences between both agents in terms of efficacy, durability of response, safety, and cost. The study showed a more durable response for rituximab versus abatacept. For clinicians who use rituximab as a second-line biologic, this will reinforce their behaviour. Rheumatologists who are undecided might consider both options as being reasonable but continue to wait for confirmatory data before they change their treatment algorithm, while probably favouring rituximab in patients who are RF positive as they might achieve a longer response.
New Evidence in Rheumatology | January 2013 39

40 New Evidence in Rheumatology | January 2013
Investigator Commentary
New Evidence: What is the rationale for using rituximab in patients with rheumatoid arthritis (RA) who have an inadequate response (IR) to tumour necrosis factor inhibitor (TNF-I) therapy?
Dr. Keystone: The rationale for using rituximab in patients with RA with an IR to TNF-I therapy is its superiority which has been demonstrated in open-label studies where it was shown to have a better outcome than using a second TNF-I. When patients experience primary failure with TNF-I therapy, it has been recommended to move directly to a therapy with a different mechanism of action (MoA), one of which is B-cell depletion through the use of rituximab.
New Evidence: Please comment on the efficacy in your study.
Dr. Keystone: In our study, which was a retrospective chart review of patients with RA who had failed TNF-Is, we wanted to determine whether abatacept or rituximab would achieve a better response. The rituximab group consisted of 37 patients, 10 of whom had previously received abatacept, while the abatacept group included 24 patients. When comparing the entire rituximab group with the abatacept group, rituximab did not seem to be performing well. However, removing the 10 patients previously treated with abatacept from the analysis showed that rituximab was superior to abatacept in terms of survival particularly after failure of three TNF-Is. As the number of TNF-I failures decreased, the difference became less pronounced, likely owing to the small sample sizes. Therefore, based on our results, the higher the number of TNF-I failures, the more efficacious rituximab appeared to be.
New Evidence: Why do you think prior abatacept treatment reduced rituximab efficacy in patients with RA?
Dr. Keystone: One reason why rituximab was less efficacious in patients with RA previously treated with abatacept was probably related to the number of biologic failures these patients had experienced. Interestingly, abatacept inhibits cell-cell interaction and rituximab is involved in a similar MoA in that it depletes cells. These are the only two biologics that work by inhibiting cells in RA, while all the other agents are cytokine inhibitors (TNF-I, IL-6 inhibitors). Therefore, it is also possible that the decreased rituximab efficacy after abatacept treatment was due to these patients already failing the MoA involving cell-cell interaction. Consequently, introducing rituximab, an agent with a similar MoA, was not able to help.
At the ACR/ARHP 2012 Annual Scientific Meeting, New Evidence spoke with Dr. Edward Keystone, Professor of Medicine, University of Toronto, and Director of The Rebecca MacDonald Centre for Arthritis and Autoimmune Disease and The Division of Advanced Therapeutics in Arthritis, about the results of his study that examined the performance of rituximab versus abatacept in patients with rheumatoid arthritis who had failed at least one tumour necrosis factor inhibitor.
An Interview with Dr. Edward Keystone on his retrospective single-centre study comparing rituximab with abatacept in patients with rheumatoid arthritis who had an inadequate response to prior biologic therapy
New Evidence in Rheumatology | January 2013 41
New Evidence: Were there any correlations between the reason of TNF-I failure and rituximab efficacy?
Dr. Keystone: Yes there were correlations between the reason for biologic failure and rituximab efficacy. When comparing the rituximab group (without including the abatacept-treated patients) with the abatacept group, rituximab performance was slightly better than abatacept (not statistically significant) when TNF-I failure occurred as a result of efficacy, while there were no differences between both groups when failure occurred due to adverse events (AE). It is important to keep in mind that the patient numbers were small and a bigger sample size may be necessary to confirm these results.
New Evidence: Were there any safety concerns with rituximab in your study?
Dr. Keystone: I did not do any safety analysis in this study but, based on my clinical practice using rituximab, there was nothing of concern in terms of AEs. Physicians sometimes worry about B-cell depletion, but serious infection rates and malignancy rates show that, to date, there are no differences between using rituximab and the other biologics. Although meta-analysis data suggest the possibility that abatacept may have less serious infections, the effectiveness of rituximab after multiple TNF-I failures makes me more likely to use it first. In the past, we would use abatacept first followed by rituximab, and that was mainly due to concerns about progressive multifocal leukoencephalopathy (PML). Nowadays, I have changed my practice because I know that PML is not much of an issue.
New Evidence: Describe the limitations of your study.
Dr. Keystone: The main limitations of the study were that it was a retrospective review, the patient numbers were small, and there were differences in the number of biologics used among patients. Another limitation is that we looked predominantly at the outcome being the survival rate. We did look at efficacy in terms of response (swollen joint count and clinical disease activity index), but the problem was that patients were treated on a regular basis with abatacept while rituximab treatment was periodic (treatment coverage was dependent on active disease), making it hard to be definitive about differences in the outcomes.
New Evidence: Do you think rituximab should be given systematically to treat patients with RA?
Dr. Keystone: Ethically, I would want to give rituximab as soon as patients start to feel sick and not wait until they have active disease with more swollen joints. Again, however, it may be challenging to do so because sometimes financial coverage, particularly by provincial payers, is dependent on active disease.
New Evidence: What conclusions can be made based on this study and how will they affect clinical decisions?
Dr. Keystone: My data suggest that rituximab is superior to abatacept in patients who fail TNF-Is, particularly in those who fail multiple TNF-Is. If I have a very sick patient who is not responsive to initial TNF inhibition, rituximab would be my treatment choice. I would use it early especially given the current data. In less responsive patients in better health, I might consider abatacept first, but I am still more likely to treat with rituximab until we have results that determine whether the decreased effectiveness of rituximab after abatacept was due to the number of biologics used or the exhaustion of the cell-cell interaction MoA.
New Evidence: Which agent is more cost-effective, abatacept or rituximab?
Dr. Keystone: While treatment with abatacept occurs monthly, rituximab is given only at the time when the patient flares, so it is periodic. Patients could go for 40 to 50 weeks before being retreated. Based on that, rituximab is more cost-effective.
New Evidence: Do you recommend rituximab in cases of failure to TNF-Is in patients with RA?
Dr. Keystone: I absolutely recommend it and I am moving it forward in my practice to after primary failure with a TNF-I. A few years ago, I used to be concerned about using rituximab because of PML, but I am much less worried now because in the last couple of years, there have been no new cases of PML despite a significant number of patients with RA being treated with rituximab. In the past, I used to generally give rituximab after two TNF-Is, but my preliminary data suggest that rituximab may be better than a second TNF-I, particularly in a primary failure. These data are consistent with other studies in the field; however, these studies do not specify whether the improved response to rituximab was after primary or secondary TNF-I failure, which is important to know. I will be addressing this question in my future studies. So, I am moving rituximab up the ladder in terms of therapeutic strategies, and although abatacept is still a reasonable alternative, my experience and data so far suggest that rituximab might be superior.

42 New Evidence in Rheumatology | January 2013
Juvenile idiopathic arthritis (JIA) is a heterogeneous group of arthritic diseases that affect children under the age of 16 years. Included within this grouping are systemic JIA (sJIA) and polyarticular JIA (pJIA).1 sJIA is characterized by systemic features such as fever, skin rash, joint inflammation and, often, significant growth abnormalities. pJIA is characterized by inflammation in five or more joints. Until recently, patients with JIA were limited to disease-modifying antirheumatic drugs (DMARDs) as first-line treatment and tumour necrosis factor inhibitors (TNF-Is) as second-line treatment. Patients who experienced an inadequate response to second-line treatments had limited options.
In 2012, tocilizumab became the first drug approved by Health Canada for the treatment of children with sJIA.2 The phase III TENDER trial, which formed a significant basis for the approval of tocilizumab in Canada, showed tocilizumab to be very effective in patients with sJIA.3 While the study demonstrated clear efficacy and safety results, the effects of treatment on patient growth were still unknown. Now, two-year data from the TENDER trial have clarified this question by showing significant catch-up growth in patients treated with tocilizumab.4 The promising results of tocilizumab in sJIA have been followed with the CHERISH study in which the efficacy and safety of tocilizumab were tested in patients with pJIA.5 Given the heterogeneous nature of the diseases under the JIA classification and the treatment challenges that arise as a consequence, the availability of additional
treatment options, such as tocilizumab, marks a significant step towards improved JIA management.
At ACR 2012, investigators presented data on how tocilizumab treatment affects catch-up growth in patients with sJIA, efficacy of tocilizumab treatment in patients with pJIA, progress in identifying risk factors for the development of uveitis, and a new tool for quantifying visual function in uveitis. The following is a report on four presentations given at ACR:
• Long-term growth responses of children with sJIA treated with tocilizumab from the TENDER trial. The study found that treatment with tocilizumab in patients with sJIA led to catch-up growth and improvements in the growth-hormone axis.
• A phase III trial summarizing the efficacy and safety of tocilizumab treatment in patients with pJIA. The trial met its primary endpoint of significant reduction in flares compared with placebo.
• A study characterizing the epidemiology and clinical outcomes of children with JIA-uveitis and idiopathic uveitis. Race, age of arthritis onset, and subtype of JIA were identified as possible risk factors in the development of uveitis.
• A study validating a new measure of visual function — the Effects of Youngsters’ Eyesight (EYE) on Quality of Life (QOL) (EYE-Q), in children with uveitis. The study concluded that EYE-Q is a valid new measure of visual function in children with uveitis.
Tocilizumab Therapy is Effective in Systemic Juvenile Idiopathic Arthritis and polyarticular JIA
References: 1. Martini A, Lovell DJ. Juvenile idiopathic arthritis: state of the art and future perspectives. Ann Rheum Dis 2010;69:1260–1263. 2. Hoffmann-La Roche. PrACTEMRA® (tocilizumab) Product Monograph. January 19, 2012. 3. De Benedetti F, Brunner H, Ruperto N, et al. Efficacy and safety of tocilizumab (TCZ) in patients with systemic juvenile idiopathic arthritis (sJIA): 2-year data from TENDER, a phase 3 clinical trial. EULAR Annual Meeting 2012:FRI0328. 4. De Benedetti F, Ruperto N, Espada G, et al. Catch-up growth during tocilizumab therapy for systemic juvenile idiopathic arthritis: 2-year data from a phase 3 clinical trial. ACR Annual Meeting Abstracts 2012;64:760. 5. Brunner HI, Ruperto N, Zuber Z, et al. Efficacy and safety of tocilizumab in patients with polyarticular juvenile idiopathic arthritis: data from a phase 3 trial. ACR Annual Meeting Abstracts 2012;64:1597.
Juvenile Idiopathic Arthritis
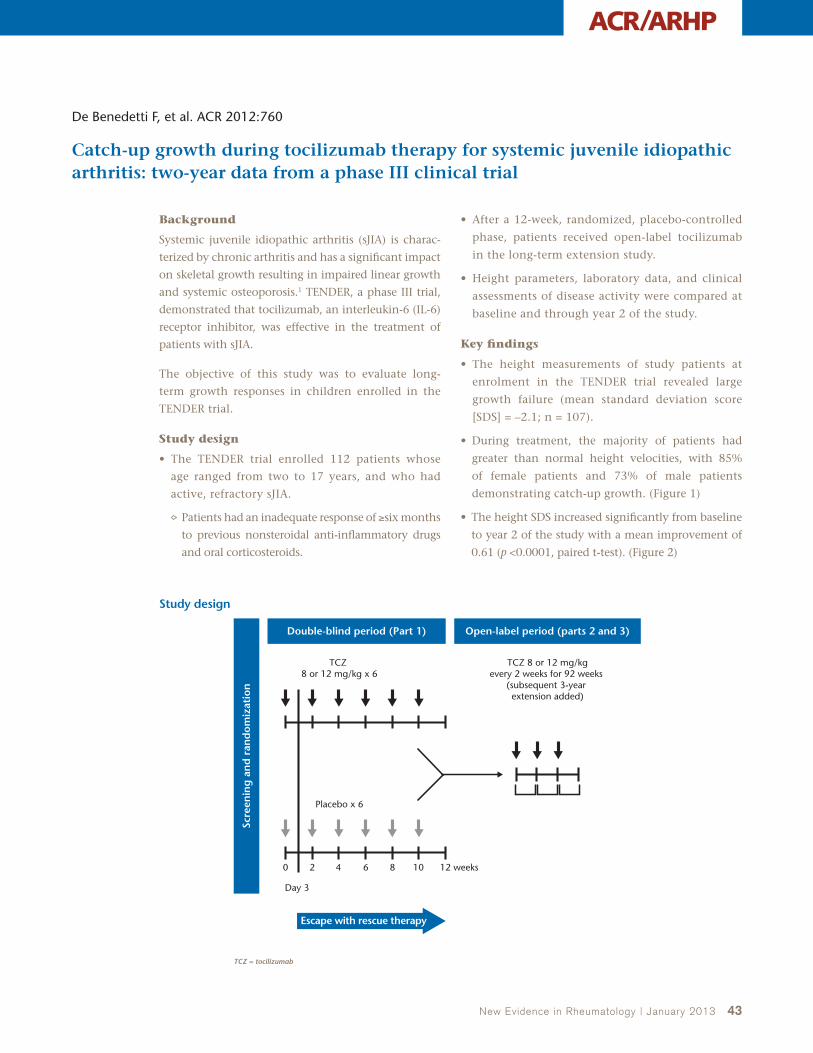
New Evidence in Rheumatology | January 2013 43
ACR/ARHP
De Benedetti F, et al. ACR 2012:760
Catch-up growth during tocilizumab therapy for systemic juvenile idiopathic arthritis: two-year data from a phase III clinical trial
Background
Systemic juvenile idiopathic arthritis (sJIA) is charac-
terized by chronic arthritis and has a significant impact
on skeletal growth resulting in impaired linear growth
and systemic osteoporosis.1 TENDER, a phase III trial,
demonstrated that tocilizumab, an interleukin-6 (IL-6)
receptor inhibitor, was effective in the treatment of
patients with sJIA.
The objective of this study was to evaluate long-
term growth responses in children enrolled in the
TENDER trial.
Study design
• The TENDER trial enrolled 112 patients whose
age ranged from two to 17 years, and who had
active, refractory sJIA.
Patients had an inadequate response of ≥six months
to previous nonsteroidal anti-inflammatory drugs
and oral corticosteroids.
• After a 12-week, randomized, placebo-controlled
phase, patients received open-label tocilizumab
in the long-term extension study.
• Height parameters, laboratory data, and clinical
assessments of disease activity were compared at
baseline and through year 2 of the study.
Key findings
• The height measurements of study patients at
enrolment in the TENDER trial revealed large
growth failure (mean standard deviation score
[SDS] = –2.1; n = 107).
• During treatment, the majority of patients had
greater than normal height velocities, with 85%
of female patients and 73% of male patients
demonstrating catch-up growth. (Figure 1)
• The height SDS increased significantly from baseline
to year 2 of the study with a mean improvement of
0.61 (p <0.0001, paired t-test). (Figure 2)
Study design
TCZ = tocilizumab
Day 3
0 2 4 6 8 10 12 weeks
Placebo x 6
TCZ 8 or 12 mg/kg x 6
TCZ 8 or 12 mg/kgevery 2 weeks for 92 weeks
(subsequent 3-year extension added)
Double-blind period (Part 1)
Escape with rescue therapy
Open-label period (parts 2 and 3)
Scre
enin
g a
nd
ran
do
miz
atio
n

44 New Evidence in Rheumatology | January 2013
• Although the mean corticosteroid dose was higher in the
first year (0.13 mg/kg/day compared with 0.05 mg/kg/day
in the second year), mean height velocities in the first and
second years of the study were comparable at 5.8 and 6.3 cm/
year, respectively (p = 0.32, paired t-test). (Figure 2)
• During tocilizumab treatment, a significant increase in
insulin-like growth factor 1 (IGF-1) levels was observed,
suggesting a normalization of the growth hormone axis
function (mean baseline IGF-1 SDS of –1.1 [n = 95],
compared with year 2 mean IGF-1 SDS of 0.0 [n = 91]; p <0.0001, paired t-test). (Figure 3)
• The osteocalcin/c-telopeptide of type 1 collagen ratio increased significantly (p = 0.0045, paired t-test), suggesting an increase in osteoblast activity relative to osteoclast activity.
• Patients with greater improvement in the Juvenile Arthritis Disease Activity Score in 71 joints (JADAS-71) during the first year had greater height velocities during that year (r = –0.35, p = 0.0002; mean decrease in JADAS-71 of 29.2 [n = 107]). (Figure 4)
Figure 1. 2-year height velocity vs. baseline age
Figure 2. Height velocity and height SD score
For each sex, the curve represents the expected height velocity based on WHO norms for height
WHO = World Health Organization; yr = year
Females
18108 14 16122 64
Age, yr
Hei
gh
t ve
loci
ty, c
m/y
r
–2
14
10
6
4
2
0
8
12
Males
18108 14 16122 64
Age, yr
Hei
gh
t ve
loci
ty, c
m/y
r
–2
14
10
6
4
2
0
8
12
Pre-Tx, n = 36; baseline, n = 81; year 1, n = 81; year 2, n = 71.Patients with ≥1 year of TCZ who had Tanner stage <4 at baseline.*Comparisons made between pre-Tx and year 1 and year 2 using paired t-tests; all p <0.0001
SD = standard deviation; TCZ = tocilizumab; Tx = treatment; yr = year
pre-Tx year 1 year 2 Baseline year 1 year 2
Hei
gh
t ve
loci
ty, c
m/y
r
10
6
4
2
0
8
dashed line at 0:expected change in height SD score for normal is 0
dashed lines mean normal expected height velocities
Hei
gh
t SD
sco
re
-5
1
-1
-3
-4
-2
0
*
*
**
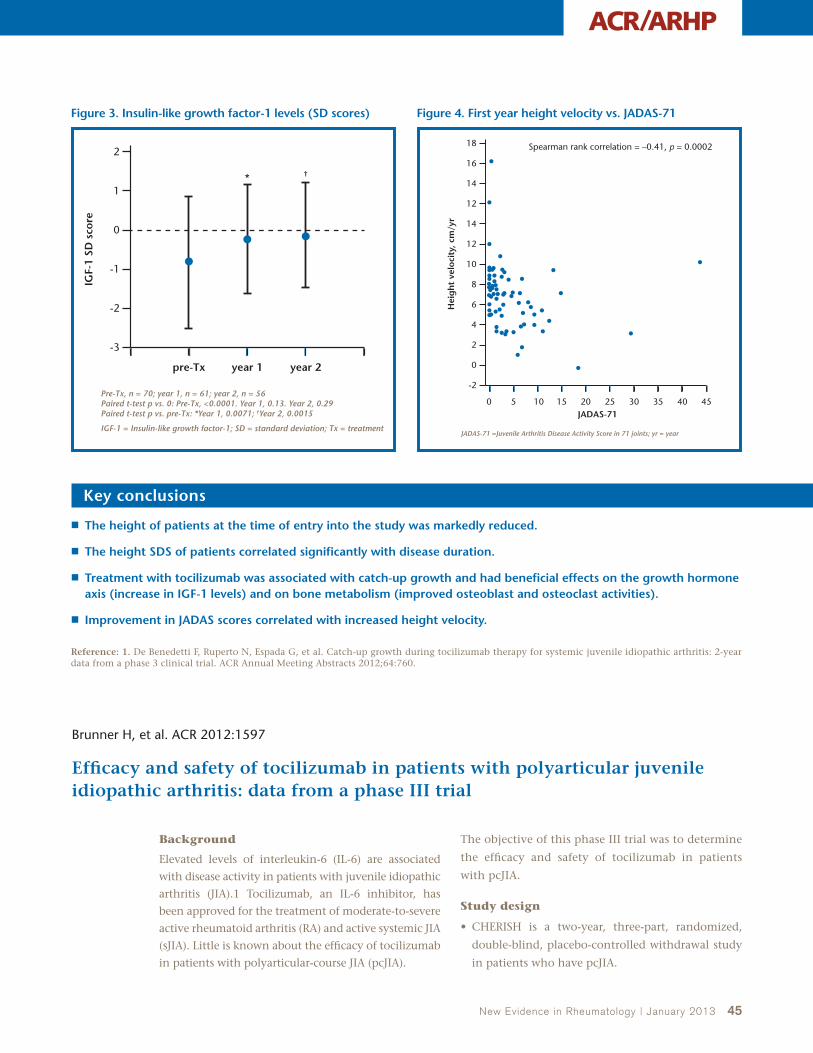
New Evidence in Rheumatology | January 2013 45
ACR/ARHP
Key conclusions
■ The height of patients at the time of entry into the study was markedly reduced.
■ The height SDS of patients correlated significantly with disease duration.
■ Treatment with tocilizumab was associated with catch-up growth and had beneficial effects on the growth hormone axis (increase in IGF-1 levels) and on bone metabolism (improved osteoblast and osteoclast activities).
■ Improvement in JADAS scores correlated with increased height velocity.
Reference: 1. De Benedetti F, Ruperto N, Espada G, et al. Catch-up growth during tocilizumab therapy for systemic juvenile idiopathic arthritis: 2-year data from a phase 3 clinical trial. ACR Annual Meeting Abstracts 2012;64:760.
Figure 3. Insulin-like growth factor-1 levels (SD scores) Figure 4. First year height velocity vs. JADAS-71
Pre-Tx, n = 70; year 1, n = 61; year 2, n = 56 Paired t-test p vs. 0: Pre-Tx, <0.0001. Year 1, 0.13. Year 2, 0.29 Paired t-test p vs. pre-Tx: *Year 1, 0.0071; †Year 2, 0.0015
IGF-1 = Insulin-like growth factor-1; SD = standard deviation; Tx = treatment
pre-Tx year 1 year 2
IGF-
1 SD
sco
re
2
0
-1
-2
-3
1* †
JADAS-71 =Juvenile Arthritis Disease Activity Score in 71 joints; yr = year
402015 30 35 45250 105JADAS-71
Hei
gh
t ve
loci
ty, c
m/y
r
-2
14
10
6
4
2
0
8
12
14
12
Spearman rank correlation = –0.41, p = 0.000218
16
Brunner H, et al. ACR 2012:1597
Efficacy and safety of tocilizumab in patients with polyarticular juvenile idiopathic arthritis: data from a phase III trial
Background
Elevated levels of interleukin-6 (IL-6) are associated
with disease activity in patients with juvenile idiopathic
arthritis (JIA).1 Tocilizumab, an IL-6 inhibitor, has
been approved for the treatment of moderate-to-severe
active rheumatoid arthritis (RA) and active systemic JIA
(sJIA). Little is known about the efficacy of tocilizumab
in patients with polyarticular-course JIA (pcJIA).
The objective of this phase III trial was to determine
the efficacy and safety of tocilizumab in patients
with pcJIA.
Study design
• CHERISH is a two-year, three-part, randomized,
double-blind, placebo-controlled withdrawal study
in patients who have pcJIA.

46 New Evidence in Rheumatology | January 2013
• The study examined patients aged between two and 17 years and who had active pcJIA JIA for ≥six months with a failure on methotrexate.
• The primary efficacy endpoint was the proportion of patients with JIA American College of Rheumatology (ACR)30 flares on tocilizumab vs. placebo in part two of the study (weeks 16–40).
• Patients in the study had JIA (International League of Associations for Rheumatology criteria) with ≥five joints with active arthritis.
The study included patients with rheumatoid factor (RF)-positive polyarticular JIA, RF-negative polyarticular JIA, and extended oligoarticular JIA.
• Patients were given a stable dose of methotrexate and non-steroidal anti-inflammatory drugs.
• The maximum stable dose of oral corticosteroids was 10 mg/day or 0.2 mg/kg/day (whichever weight was lower).
Key findings
• Patients who received tocilizumab 8 mg/kg (<30 kg body weight) showed weaker improvements in JIA ACR 30/50/70/90 criteria than the other two groups in part one of the study. (Figure 1)
• The number of patients treated with tocilizumab and who developed JIA ACR30 flares was significantly lower than the number of patients treated with placebo in part two of the study. (Figure 2)
• Patients receiving tocilizumab maintained JIA responses at week 40. (Figure 3)
• The overall rate of adverse events (AE) in patients treated with tocilizumab was 480/100 patient-years (pt-years). (Table 1)
• The overall rate of serious AEs (SAEs) in patients treated with tocilizumab was 12.5/100 pt-years.
• AE and SAE rates in patients treated with tocilizumab were similar to those treated with placebo in part two of the study. (Table 2)
TCZ (n = 82)
Placebo (n = 81)
Escape to TCZ (JIA ACR30 flare)
Open-labellead-in (n = 188)
Double-blindWithdrawal (n = 166)
Open-labelextension (n = 160)
Weight ≥30 kg TCZ 8 mg/kg q4wks
Weight <30 kgTCZ 8 mg/kg or 10 mg/kg q4wks
Weight ≥30 kg TCZ 8 mg/kg q4wks
Weight <30 kgTCZ 8 mg/kg or 10 mg/kg q4wks
Part 1 Part 2 Part 3
16 weeks 24 weeks 64 weeks
58 centres in 15 countries
CHERISH: A 3-part, randomized withdrawal study in pcJIA
ACR= American College of Rheumatology; JIA = juvenile idiopathic arthritis; pcJIA = polyarticular-course JIA; q4wks = every four weeks; TCZ = tocilizumab
Figure 1. Juvenile idiopathic arthritis ACR 30/50/70/90 responses
JIA ACR30 JIA ACR50 JIA ACR70 JIA ACR90
AC
R r
esp
onse
, % p
atie
nts
41
24
31
25
63
87
80
7168
9389
77
0
30
20
10
70
40
50
60
80
90
100
TCZ 8 mg/kg <30 kg BW TCZ 10 mg/kg <30 kg BW TCZ 8 mg/kg ≥30 kg BW
Patients who withdrew or for whom the endpoint could not be determined were classified as nonresponders
ACR = American College of Rheumatology; BW = body weight; JIA = juvenile idiopathic arthritis; TCZ = tocilizumab

New Evidence in Rheumatology | January 2013 47
ACR/ARHP
Figure 2. Patients with juvenile idiopathic arthritis ACR30 flare
All placebo(N = 81)
Adjusted difference in means = –0.21 (95% CI, –0.35 to –0.08); p = 0.0024
All TCZ(N = 82)
JIA
AC
R30
fla
re r
elat
ive
to w
eek
16,
% p
atie
nts
26
48
0
30
20
10
40
50
60
ACR = American College of Rheumatology; CI = confidence interval; JIA = juvenile idiopathic arthritis; TCZ = tocilizumab
Figure 3. Maintenance of JIA response over 40 weeks
JIA ACR30 JIA ACR50 JIA ACR70 JIA ACR90
AC
R r
esp
on
ses,
% p
atie
nts
0
10
20
30
60
40
80
50
100
70
90
Patients who withdrew or escaped to open-label TCZ or for whom the endpoint could not be determined are classified as nonresponders in part two of the analyses
ACR = American College of Rheumatology; JIA = juvenile idiopathic arthritis; TCZ = tocilizumab
74 73
65
All TCZ
45
Table 1. Overall rate of adverse events in patients treated with tocilizumab
System order class AE rate/100 pt-years
Overall TCZ exposure 184 pt-years 480
Infections and infestations 163.7
Gastrointestinal disorders 71.0
Musculoskeletal and connective tissue disorders
53.1
Respiratory, thoracic, and mediastinal disorders
36.9
Skin and subcutaneous tissue disorders 33.1
Nervous system disorders 28.7
Injury, poisoning, and procedural complications
22.2
AE = adverse events; pt-years = patient-years; TCZ = tocilizumab
Table 2. AE and SAE rates in patients treated with tocilizumab in part two of the study
All placebo N = 81
All TCZN = 82
Duration of follow-up (pt-years) 27.41 32.33
Total patients with ≥1 AE 60 58
Total number of AEs 141 147
AE rate per 100 pt-years 514.4 454.7
Total patients with ≥1 SAE 3 3
Total number of SAEs 3 3
SAE rate per 100 pt-years 10.9 9.3
A comparable number of patients experienced at least one AE or SAE in each treatment group
AE = adverse event; pt-years = patient-years; SAE = serious adverse event; TCZ = tocilizumab
Key conclusions
■ CHERISH met its primary endpoint with a significant reduction of flares compared with placebo.
■ Tocilizumab was highly effective and resulted in a meaningful improvement of pcJIA.
■ The response of patients to tocilizumab was maintained for 40 weeks.
■ The suggested doses of tocilizumab for patients with pcJIA are 8 mg/kg for those with a body weight of ≥30 kg, and 10 mg/kg for those with a body weight of <30 kg.
■ The safety profile of tocilizumab in patients with pcJIA is consistent with that seen in other diseases treated with tocilizumab.
Reference: 1. Brunner H, Ruperto N, Zuber Z, et al. Efficacy and safety of tocilizumab in patients with polyarticular juvenile idiopathic arthritis: data from a phase 3 trial. ACR Annual Meeting Abstracts 2012;64:1597.

48 New Evidence in Rheumatology | January 2013
Table 1. Mean scores on patient reported quality of life and function measures
JIAN = 104
JIA-UN = 19
I-UN = 9
p-value
EYE-Q (range 0–4)† 3.64 ± 0.44 3.49 ± 0.49 3.33 ± 0.72 0.063
EYE-Q new (range 0–4) 3.52 ± 0.46 3.28 ± 0.48 3.10 ± 0.70 0.008*
CHAQ (range 0–3)‡ 0.61 ± 0.61 0.58 ± 0.68 0.11 ± 0.25 0.021*
PedsQL physical scale (range 0–100)† 70.4 ± 23.7 71.1 ± 24.5 86.5 ± 13.1 0.045*
PedsQL psychosocial scale 74.3 ± 18.5 71.0 ± 19.8 76.2 ± 21.7 0.674
PedsQL total scale 72.9 ± 19.0 71.0 ± 20.0 79.8 ± 17.4 0.347
ANOVA, *p <0.05†Greater scores indicate better QOL; ‡Greater scores indicate worse QOL
Note: The sample size in each group varies by scoring tool
ANOVA = analysis of variance; CHAQ = Childhood Health Assessment Questionnaire; EYE-Q = Effects of Youngsters’ Eyesight on QOL; I-U = idiopathic uveitis; JIA = juvenile idiopathic arthritis; JIA-U = juvenile idiopathic arthritis-associated uveitis; PedsQL = Pediatric Quality of Life Inventory; QOL = quality of life
Angeles-Han S, et al. ACR 2012:2005
Clinical course and outcomes of children with juvenile idiopathic arthritis-associated uveitis and idiopathic uveitis
Background
Uveitis is a condition characterized by the inflammation
of the middle layer of the eye and can lead to vision loss
and blindness. The number of studies that have focused
on the outcomes of children with both juvenile idio-
pathic arthritis-associated uveitis (JIA-U) and idiopathic
uveitis (I-U) have been few.1 Identifying these risk factors
is important when examining the long-term outcomes
in children afflicted with JIA-U.
The objective of this study was to characterize the
epidemiology and clinical outcomes of children with
JIA-U and I-U in a cohort of children in an urban
tertiary care centre in southeastern U.S.
Study design
• Children (n = 151) with JIA, JIA-U, and I-U were
included in the study.
• Rheumatology and ophthalmology medical records
of all participants were reviewed.
• Questionnaires were completed on overall quality of
life (QOL) (Pediatric QOL Inventory [PedsQL]), physical
function (Childhood Health Assessment Questionnaire
[CHAQ]), and visual function (Effects of Youngsters’
Eyesight on QOL [EYE-Q]).
Key findings
• Of the 151 patients in the study, most were female (72%), non-Hispanic (90%), and Caucasian (71%).
• Compared with children with JIA, children with JIA-U were more frequently African American, diagnosed with oligoarticular extended and poly-articular rheumatoid factor negative (RF[–]) JIA, and had a younger age of arthritis onset.
• No significant differences in sex, antinuclear anti-body (ANA), RF (−), or human leukocyte antigen (HLA-B27) were seen.
• Children with uveitis were RF negative.
• Children with I-U had worse visual acuity (p = 0.004), and ocular complications — band keratopathy (p = 0.008), cystoid macular edema (p = 0.004), and synechiae (p = 0.005).
• Significant differences were seen in the EYE-Q scores in children with uveitis compared with those with JIA (p = 0.008).
• There were significant differences in the CHAQ and PedsQL physical scale scores in children with arthritis compared with I-U (p = 0.021, p = 0.045).
• Among all groups, there were no differences in total PedsQL and psychosocial QOL scores. (Table 1)

New Evidence in Rheumatology | January 2013 49
ACR/ARHP
Key conclusions
■ Children with I-U may have a poorer visual outcome compared with those with JIA-U.
■ Race, ethnicity, age of arthritis onset, and JIA subtype are important risk factors for developing uveitis, whereas sex, ANA, and HLA-B27 need further investigation.
■ Children with JIA-U have more components of disability compared with children with JIA alone and I-U.
• As expected, visual disability was worse with uveitis, and physical disability was worse in those with arthritis.
Reference: 1. Angeles-Han ST, Yeh S, McCracken C, et al. Clinical course and outcomes of children with juvenile idiopathic arthritis-associated uveitis. ACR Annual Meeting Abstracts 2012;64:2005.
Angeles-Han S, et al. ACR 2012:1155
A new measure of visual function for children with juvenile idiopathic arthritis-associated uveitis
Background
Studies on outcomes of children with juvenile idio-
pathic arthritis-associated uveitis (JIA-U) have focused
primarily on arthritis and secondarily on clinical
ocular examination and physical disability.1 This
assessment could improve by including measures
of the impact of uveitis on daily life. Until recently,
however, instruments to measure visual function in
patients with JIA-U have been unavailable.
The objective of this study is to validate a measure
of visual function, the Effects of Youngsters’ Eyesight
(EYE) on Quality of Life (QOL) (EYE-Q), in children
with uveitis.
Study design
• Focus groups were held to modify the old EYE-Q for
children with uveitis.
The new EYE-Q contains items specific to uveitis.
A parent-proxy version was also developed.
• Children with JIA, JIA-U, and idiopathic uveitis (I-U)
were included.
• Ophthalmology and rheumatology records were
reviewed.
• Questionnaires were completed on overall QOL (Pediatric QOL Inventory [PedsQL]), physical func-tion (Childhood Health Assessment Questionnaire [CHAQ]), and visual function (EYE-Q).
Key findings
• Patients (n = 104) with JIA were included, 29 with JIA-U, and 18 with I-U.
• Significant differences were seen in the child and parent EYE-Q, CHAQ, and PedsQL physical scores in children with uveitis compared with children with JIA. (Table 1)
• For the child report, there were weak correlations between EYE-Q scores and logmarVA (r = −0.20) and moderate correlations with the PedsQL (r = 0.48) and CHAQ (r = −0.49). (Table 2)
Similar results were found with the parent report.
• Correlations between the parent and child EYE-Q (r = 0.82), the old and new versions of the EYE-Q for the child report (r = 0.97), and the parent report (r = 0.80) were robust.
• Cronbach’s α for the old EYE-Q child and parent reports was 0.90. Cronbach’s α for the new EYE-Q child and parent reports was 0.91.

50 New Evidence in Rheumatology | January 2013
Key conclusions
■ The new EYE-Q, with items specific to uveitis, is a valid measure of visual function in children with uveitis. ■ Given that there were differences in child and parent perceptions of disease, including both perspectives in disease
assessment is important. ■ The EYE-Q may be an important measure in the assessment of outcomes in patients with uveitis, and may also be a
better measure than either the clinical exam or arthritis-specific measures alone.■ Longitudinal studies examining the performance of the EYE-Q in children with JIA-U and I-U are ongoing.
Reference: 1. Angeles-Han ST, Yeh S, McCracken C, et al. A new measure of visual function for children with juvenile idiopathic arthritis-associated uveitis. ACR Annual Meeting Abstracts 2012;64:1155
Table 1. Mean scores on standard quality of life and function measures in JIA
JIAN = 104
JIA-UN = 29
I-UN = 18
p-value
Child reports*
EYEQ (range 0−4)‡ 3.64 ± 0.44 3.49 ± 0.49 3.33 ± 0.72 0.063
EYEQ new (range 0−4)‡ 3.52 ± 0.46 3.28 ± 0.48 3.10 ± 0.70 0.008†
CHAQ (range 0−3)§ 0.61 ± 0.61 0.58 ± 0.68 0.11 ± 0.25 0.021†
PedsQL physical scale (range 0−100)‡ 70.4 ± 23.7 71.1 ± 24.5 86.5 ± 13.1 0.045†
PedsQL psychosocial scale 74.3 ± 18.5 71.0 ± 19.8 76.2 ± 21.7 0.674
PedsQL total scale 72.9 ± 19.0 71.0 ± 20.0 79.8 ± 17.4 0.347
Parent reports
EYEQ (range 0−4)‡ 3.79 ± 0.37 3.58 ± 0.5 3.15 ± 0.92 <0.001†
EYEQ new (range 0−4)‡ 3.66 ± 0.39 3.27 ± 0.5 3.01 ± 0.82 <0.001†
CHAQ (range 0−3)§ 0.56 ± 0.63 0.41 ± 0.56 0.14 ± 0.22 0.014†
PedsQL physical scale (range 0−100)‡ 69.3 ± 25.3 72.9 ± 24.4 92.0 ± 12.1 0.003†
PedsQL psychosocial scale 76.4 ± 20.1 73.7 ± 20.5 79.0 ± 21.4 0.699
PedsQL total scale 73.8 ± 20.4 73.5 ± 20.8 73.8 ± 20.4 0.185
* data are missing†ANOVA p <0.05‡Greater scores indicate better QOL; §Greater scores indicate worse QOL
ANOVA = analysis of variance; CHAQ = Childhood Health Assessment Questionnaire; EYEQ = Effects of Youngsters’ Eyesight on QOL; JIA = juvenile idiopathic arthritis; PedsQL = Pediatric Quality of Life Inventory; QOL = quality of life
Table 2. Correlations of the EYEQ with standard measures of quality of life and function in JIA
R (95% CI)† p-value
EYEQ child report
LogmarVA –0.20 (–0.45 to 0.08) 0.150
CHAQ –0.49 (–0.63 to [–0.32]) <0.0001*
PedsQL total scale 0.48 (0.31 to 0.61) <0.0001*
EYEQ parent 0.82 (0.75 to 0.88) <0.0001*
New EYE-Q 0.97 (0.95 to 0.98) <0.0001*
EYEQ parent report
LogmarVA –0.35 (-0.53 to [–0.13]) 0.002
CHAQ score –0.29 (–0.43 to [–0.13]) <0.001*
PedsQL total 0.34 (0.19 to 0.48) <0.001*
New EYEQ 0.80 (0.73 to 0.85) <0.001*
Spearman’s correlation coefficients, *p <0.05†Mild correlations: r <0.3; moderate correlations: r = 0.3−0.7; strong correlation: r >0.7
CHAQ = Childhood Health Assessment Questionnaire; CI = confidence interval; EYE-Q = Effects of Youngsters’ Eyesight on QOL; JIA = juvenile idiopathic arthritis; LogmarVA = logmar visual acuity; PedsQL = Pediatric Quality of Life inventory; QOL = quality of life

ACR/ARHP
Canadian perspective by Dr. Earl Silverman
The recent approval of the inter-leukin-6 (IL-6) receptor inhibitor tocilizumab was a major break-through for patients with systemic juvenile idiopathic arthritis (sJIA). It is currently being tested in other types of JIA including polyarticular course JIA (pcJIA). Previously, the treatment of sJIA was mainly dependent on prednisone for control of inflammation. However,
prednisone led to impairment of other functions such as major growth problems. The phase III trial (TENDER), a double-blind randomized placebo controlled trial in sJIA, showed that tocilizumab was effective in the treatment of patients with sJIA, leading to its current indication for use in these patients. This was momentous for patients and physicians as there was now a treatment that was not only efficacious but also safe in treating such a serious disease.
In the study by Benedetti et al., which was a sub-study within the bigger TENDER trial, tocilizumab was shown to control sJIA and improve growth in patients. An increase in insulin-like growth factor 1 levels was observed, providing a biochemical evidence of growth normalization. Prednisone has been previously shown to impair the osteoblasts and osteoclast activities important for bone growth, remodelling and repair. In this study, treatment with tocilizumab resulted in a significant increase in the serum levels of osteocalcin/c-telopeptide of type 1 collagen (a marker of bone formation/resorption) (p = 0.0045, paired t-test). The disease activity measure Juvenile Arthritis Disease Activity Score-1 (JADAS-1) also improved with tocilizumab because patients got better and their disease was under control. The JADAS-1 improvement correlated with better growth.
Currently, tocilizumab is accessible to patients with sJIA who need it as it has the indication in Canada and is now covered by several provinces and private insurers. The main issue is that the treatment requires infusions every two weeks. This becomes very inconvenient for patients living outside big cities. Few infusion centres will give the drug to very young children because of the potential for infusion reactions and the need to have a pediatrician present at the time of treatment.
It is currently believed that there are two groups of patients with sJIA, one whose disease is driven by IL-6 and another by IL-1. Both IL-6 and IL-1 inhibitors are important new treatments for patients with sJIA but, at the moment, we do not know how to differentiate which patients will respond to which drug. Biomarker studies are required to identify patients responsive to IL-1 but not IL-6 inhibition and vice versa in order to better treat these patients.
From healthcare and scientific points of view, I would consider treating patients with tocilizumab or IL-1 inhibitors at an early stage of the disease. With the current approval for tocilizumab, we can start treatment early and withdraw it when patients are in remission. Currently, half the patients with sJIA will go into remission and will be able to stop medications between six and 12 months. If remission occurred on an IL-6 or IL-1 inhibitor, then we could stop the drug without having to give prednisone
to patients. The net result would be remission without the adverse events (AE) associated with prednisone. As half of the patients with sJIA have a much more prolonged and/or severe disease course, we are hoping that early treatment will put more patients into long-term remission before the disease settles in.
While tocilizumab is now approved for the treatment of sJIA, its role in pcJIA is currently being explored and the results seem promising. In pcJIA, when methotrexate and leflunomide fail, the only licensed drugs available are tumor necrosis factor inhibitors (TNF-Is) and abatacept. TNF-Is are safe, show good results, and are mainly used as a first biologic treatment. However, the challenge is that not all patients respond well to them. After TNF-I failure, physicians will treat patients with another TNF-I or an agent with a different mode of action, mainly abatacept, or rituximab if the patients are rheumatoid factor (RF) positive. Despite the current options, there are still patients who are nonresponders, hence the need for new drugs. Tocilizumab was shown to work in adult patients with rheumatoid arthritis (RA), and since pcJIA has clinical similarities to RA, it could be beneficial for children with pcJIA.
In the Brunner et al. study (CHERISH), tocilizumab was found to be effective and safe in patients with pcJIA. The study included patients with pcJIA: RF-positive polyarticular JIA (pJIA), RF-negative pJIA, and extended oligoarticular JIA. The dose was based on the patient’s weight: those weighing more than 30 kg received the same dose per kg as adults; those weighing less than 30 kg received a slightly higher dose per kg. The lack of initial pharmacokinetic studies to determine the correct dose to use, particularly for those patients weighing less than 20 kg, was a limitation as these young patients may have been underdosed, especially since young patients are known to require a higher dose per kg than adults. The study had an open label lead-in phase without a placebo followed by a double-blind withdrawal phase. As a result of this study design, only responders from the first part entered into the double-blind phase, therefore, the study could not provide any efficacy data but only effectiveness results. The rationale for the study was that it was thought children could not be recruited to double-blind studies, however the TENDER study demonstrated that placebo-controlled studies can be performed in JIA. The current study results showed that tocilizumab was effective as it significantly reduced flares with 26% of patients on tocilizumab developing JIA American College of Rheumatology (ACR) 30 flare versus 48% of those who were on placebo. Tocilizumab was also found to be safe with no unexpected AEs. However, more informative data could have been obtained in a randomized placebo-controlled trial.
We were happy with how patients responded to tocilizumab; we enrolled patients from our centre who had significantly active disease and who had failed one and sometimes two TNF-Is, and they responded very well to the treatment. I believe that if the final assess-ment of the results of this trial support the data presented at the ACR 2012 meeting, and the paper passes peer review, then tocilizumab should receive its indication for pcJIA. The next step would then be to determine where tocilizumab would fit within the pcJIA treatment algorithm. Long-term safety studies are very important but there were no safety signals to suggest that it would not be safe in the long run in children and adolescents.
New Evidence in Rheumatology | January 2013 51
52 New Evidence in Rheumatology | January 2013
Antineutrophil cytoplasmic antibody (ANCA)-associated vasculitis is an autoimmune disease characterized by small blood vessel inflammation. It includes granulomatosis with polyangiitis (GPA) (Wegener’s), microscopic polyangiitis (MPA), and the Churg-Strauss syndrome with the majority of these patients being ANCA positive. The conventional treatment for patients with ANCA-associated vasculitis is cyclophosphamide and glucocorticoids for induction of remission followed by azathioprine for maintenance. Recently two pivotal studies (RAVE [Rituximab in ANCA-Associated Vasculitis] and RITUXVAS [Rituximab versus cyclophosphamide in ANCA-associated vasculitis]) showed that rituximab had a similar efficacy to conventional treatment in inducing remission.1,2 This finding led to the approval of rituximab for remission induction by the Food and Drug Administration and Health Canada. However, the rate of adverse events (AEs) was found to be similar between rituximab and conventional treatment and relapses continue to be a major concern.1,3-5 For now, however, rituximab remains an alternative for adult patients with GPA or MPA with severe, active disease and who are ANCA positive.
At ACR 2012, studies were presented that evaluated the efficacy of rituximab in the induction of remission, its long-term efficacy, as well as its role in the maintenance of remission in ANCA-associated
vasculitis. This section reports on three presentations
given at ACR:
• Long-term efficacy and risks of rituximab when
used alone or in combination with another
immunosuppressive agent other than steroids.
Rituximab was very effective in inducing remission
and the rate of relapse-free survival was higher in
patients who received a second immunosuppressive
agent. There were no differences in serious AEs.
• Role of rituximab in the maintenance of remission
after cyclophosphamide induction in comparison
with the conventional maintenance using
azathioprine. Results showed a low relapse rate
with rituximab compared with azathioprine. No
differences were observed in AEs, but there were
more dropouts in the azathioprine arm than in the
rituximab arm, and three deaths occurred in the
azathioprine arm but none in the rituximab group.
• A meta-analysis evaluating the clinical benefits of
rituximab in ANCA-associated vasculitis. Ritux-
imab was found to be efficacious in inducing
remission when compared with control in a meta-
analysis that combined data from De Menthon et al.
(Infliximab versus Rituximab in Systemic Necrotizing
Vasculitides), RAVE and RITUXVAS studies.
The Multifaceted Role of Rituximab in ANCA-Associated Vasculitis: From Induction to Maintenance
References: 1. Stone JH, Merkel PA, Spiera R, et al. Rituximab versus cyclophosphamide for ANCA-associated vasculitis. N Engl J Med
2010;363:221–32. 2. Jones RB, Tervaert JW, Hauser T, et al. Rituximab versus cyclophosphamide in ANCA-associated renal vasculitis.
N Engl J Med 2010;363:211–20. 3. Pagnoux C, Mahr A, Hamidou MA, et al. Azathioprine or methotrexate maintenance for ANCA-
associated vasculitis. N Engl J Med 2008;359:2790–803. 4. Holle JU, Gross WL, Latza U, et al. Improved outcome in 445 patients with
Wegener’s granulomatosis in a German vasculitis center over four decades. Arthritis Rheum 2011;63:257-66. 5. Jayne D, Rasmussen N,
Andrassy K, et al. A randomized trial of maintenance therapy for vasculitis associated with antineutrophil cytoplasmic autoantibodies.
N Engl J Med 2003;349:36–44.
Vasculitis

New Evidence in Rheumatology | January 2013 53
ACR/ARHP
Azar L, et al. ACR 2012:1544
Long-term outcome of patients with granulomatosis with polyangiitis (Wegener’s) treated with rituximab
Background
Rituximab is an efficacious alternative to cyclophos-phamide for the treatment of granulomatosis with polyangiitis (GPA). However, relapses have been observed, long-term efficacy is unknown, and strategies to reduce the risk of relapse after rituximab-induced remission are just beginning to be explored.
At ACR 2012, Azar and colleagues presented findings from a study that evaluated the long-term efficacy and risks of rituximab when used alone or in combination with another immunosuppressive agent other than steroids.1
Study design
• The study was a single centre retrospective review that included patients with GPA who fulfilled the 1990 American College of Rheumatology criteria and were treated with at least one course of rituximab.
• Subset analysis included the effect of receiving a second immunosuppressive agent, other than steroids.
• Remission was defined as Birmingham vasculitis activity score (BVAS)/Wegener’s granulomatosis (WG) = 0.
Key findings
• A total of 110 patients (56 females, 54 males) were enrolled in the study.
Patients received 211 courses of rituximab.
The mean age at the first rituximab treatment (rituximab 1) was 50.
Indications for rituximab were: new onset (n = 5), relapsing (n = 85), persistent disease (n = 15), and remission maintenance (n = 5).
At the time of rituximab 1, median BVAS/WG was 4 (range 1–11).
Median follow-up after rituximab 1 was 23 months (interquartile range [IQR] 10–50).
In the past, 82% of the patients were antineutrophil-associated cytoplasmic antibody positive.
Clinical features at any time during disease course prior to rituximab 1 are presented in Table 1.
• In 77% of the cases, two infusions of 1 g were given two weeks apart, and apart from three
patients with worsening or persistent lung involvement, complete remission was achieved in 99/102 patients with active disease and available information.
• Post rituximab 1, 49 patients experienced 78 relapses with the median time to relapse being 13 months (IQR 7–20.5); at the time of relapse 42.2% of patients were B-cell depleted in peripheral blood (data from 45 relapses in 31 patients).
• Among 92 patients who achieved remission and did not receive subsequent pre-emptive ritux-imab treatments, 49 patients had been started or continued on a second immunosuppressive agent after rituximab 1; 43 patients did not receive a second immunosuppressive agent after rituximab 1. The second agents used were:
Azathioprine (29 patients, median 150 mg/day); Methotrexate (12 patients, median 22.5 mg/week); Mycophenolate mofetil (eight patients, median 2 g/day).
Table 1. Clinical manifestations prior to rituximab 1 (%)
Clinical Manifestations %
Constitutional symptoms 38
Arthralgia/arthritis 70.4
Cutaneous involvement 26.6
Eye involvement 42
Ear, nose, and throat involvement 96.1
Pulmonary involvement Nodules or cavitiesOther infiltrateEndobronchial involvementAlveolar hemorrhageRespiratory failure
82.856.125.713.321.96.6
Renal involvementHematuria without RBC castsRBC castsRise in creatinine >30% or GFR fall >25%Median GFR (IQR)
58.025.728.529.5
82 (62–96)
Nervous system involvement Cranial nerve palsySensory peripheral neuropathyMotor mononeuritis multiplex
25.77.611.45.7
GFR = glomerular filtration rate; IQR =interquartile range; RBC = red blood cell

54 New Evidence in Rheumatology | January 2013
• Baseline characteristics of the two groups are shown in Table 2.
• Rate of relapse-free survival was significantly higher in patients who received a second agent (p = 0.04). (Figure 1)
HR of relapse in patients receiving a second agent compared with patients who did not was 0.54 (95% CI 0.30–0.99).
The median prednisone dose at the endpoint was 0 mg and 5 mg in the two groups, respectively (p = 0.23).
• Of the 16 patients who were relapse free at two years
after rituximab 1 and observed beyond that time, eight
remained in remission for up to six years.
• Serious adverse events (SAEs) did not differ between the
groups. Serious infections occurred after rituximab 1 in
4.1% (second agent) and 7% (no second agent) patient
subsets, respectively (p = 0.66).
Table 2. Baseline characteristics of the two groups
Baseline characteristicsSecond
immunosuppressive agent after RTX1
No second immunosuppressive
agent after RTX1p value
Age at first RTX (year) median (IQR) 49 (39–61) 43 (35–65) 0.69
Women (%) 40.8 65.1 0.02
New onset disease (%) 4.1 2.3 0.99
Disease duration before RTX (months) 44 (17–108) 53 (20–108) 0.61
Number of prior relapses 3 (2–4) 3 (1–4) 0.54
BVAS/WG at initial diagnosis 8 (6–10) 7.5 (4–10) 0.38
Received CYC in the past (%) 78.7 92.9 0.06
Duration of CYC use (months) 10 (5–30) 6 (3.5–12) 0.067
Past ANCA PR3/MPO positive (%) 69.8/4.7 70.3/13.5 0.31
Clinical manifestations at time of RTX1 (%)Ear, nose, and throat involvementPulmonary involvementRenal involvementGFR (mL/min/1.73 m2)
53.153.132.7
75 (49–91)
44.255.830.2
77.5 (49–100)
0.400.790.800.56
BVAS/WG at time of RTX1 3 (2-6) 4 (1–5) 0.74
RTX regimen used: 1 g intravenous x 2 (%) 75.5 72.1 0.90
ANCA = antineutrophil cytoplasmic antibody; BVAS = Birmingham vasculitis activity score; CYC = cyclophosphamide; GFR = glomerular filtration rate; IQR = interquartile range; MPO = myeloperoxidase; PR3 = proteinase-3; RTX = rituximab; RTX1: rituximab 1 (first rituximab treatment); WG = Wegener’s granulomatosis
Figure 1. Relapse-free survival with steroids and rituximab only vs. an additional immunosuppressive agent
0 6 12 18 24 30 36 42 48 54 60 66 72 78
24N = 49 10 4 4 2
18N = 43 6 4 1 0
Months
% R
elap
se f
ree
Kaplan-Meier analysis: Relapse-free survival of patients treated with steroids and rituximab only vs. an additional immunosuppressive agent (p = 0.04)
0
10
20
30
40
50
60
70
80
90
100
With additional agent
No additional agent

New Evidence in Rheumatology | January 2013 55
ACR/ARHP
Key conclusions
■ Rituximab is a very effective remission-inducing agent for GPA: 97% of treated patients achieved remission. ■ The use of a second immunosuppressive agent in conjunction with rituximab diminished the likelihood of relapse and
did not result in a greater number of SAEs. ■ Within subsets of patients who were relapse free at two years after one rituximab treatment, remissions endured for
two to six years in eight out of 16 patients.
Reference: 1. Azar L, Springer J, Xu M, et al. Long-term outcome of patients with granulomatosis with polyangiitis (Wegener’s) (GPA) treated with rituximab.
ACR Annual Meeting Abstracts 2012;64:1544.
Guillevin L, et al. ACR 2012:1652
Rituximab versus azathioprine for maintenance in ANCA-associated vasculitis
Background
Rituximab has been shown to be as effective as cyclophosphamide at inducing remission of anti-neutrophil cytoplasmic antibody (ANCA)-associated vasculitides. However, one major issue in treating ANCA-associated vasculitides is how to prevent the frequent relapses that occur in these patients.1-3
At ACR 2012, the results of a prospective, randomized, controlled trial of rituximab versus azathioprine to maintain ANCA-associated vasculitis remission were reported (MAINRITSAN [RITuximab in Systemic ANca-associated vasculitides] trial).4
Study design
• The inclusion criteria for the study were:
ANCA-associated vasculitides: granulomatosis with polyangiitis (GPA)(Wegener’s), microscopic polyan-giitis (MPA), and kidney-limited disease (systematic GPA or MPA with Five Factor Score ≥ 1);
Patients had to be older than 18 years but younger than 75 years;
Patients must have experienced remission after a first flare or relapse.
• Once remission was obtained with a conventional regimen, patients with newly diagnosed ANCA- associated vasculitides (two thirds of the enrol-ment) or relapsing ANCA-associated vasculitides
(one third of the enrolment) were randomly
assigned to receive a 500-mg rituximab infusion
on days 1 and 15, then at 5.5 months, and then
every six months for a total of five infusions over
18 months, or azathioprine for 22 months at the
initial dose of 2 mg/kg/day.
• The primary objective was to evaluate rituximab’s
efficacy in maintaining remission of ANCA-associated
vasculitis after obtaining remission of a first flare or
relapse. The secondary objectives were to:
Assess the safety of rituximab vs. azathioprine;
Evaluate the predictive value of ANCA appearance
and/or CD19 for relapses (ANCA and CD19 not
yet analyzed).
• Evaluation criteria were:
Primary endpoint: Number of major relapses at 28
months after inclusion (18 months for rituximab or
22 months for azathioprine plus 10 or six months).
Secondary endpoint: Number of adverse effects
(AEs) in each group, number of minor relapses,
mortality in each group, and the number of
ANCA-positive patients in each group.
• The hypothesis was that the relapse rate with
azathioprine would be 40% compared with 15%
with rituximab.

56 New Evidence in Rheumatology | January 2013
Key findings
• Patients (n = 117) were part of the study with 59 in the azathioprine arm (47 first flares and 12 relapses) and 58 in the rituximab arm (46 first flares and 12 relapses).
• The main clinical manifestations at diagnosis or last relapse included kidney, lung, or ear, nose, and throat involvement. (Figure 1)
• Patient dropout in the azathioprine arm was 21/59 (35.6%; there were several causes for the same patient) with the reasons leading to dropout outlined below.
There were 15 major relapses (25.4%)
Four patients had severe AEs (6.7%).
Seven patients stopped treatment for other reasons (11.8%).
• Patient dropout in the rituximab arm was 6/58 (10.3%; there were several causes for the same patient) with the reasons leading to dropout outlined below.
There were three major relapses (5.2%).
One patient was lost to follow-up.
Three patients stopped treatment for other reasons.
CS 1 mg/kg/day
20 mg at3 months
10 mg at6 months
Induction treatment
Maintenance treatment
R = 500 mg of rituximab
2 weeks 5 months+
2 weeks
6 months 6 months Endpoint28 months
R R R R R
MPS15 mg/kg
MPS15 mg/kg
MPS15 mg/kg
pCYC Day 0 0.6 g/m2
pCYC Day 14 0.6 g/m2
pCYC Day 28 0.6 g/m2
pCYC S 49 0.7 g/m2
pCYC Day 70 0.7 g/m2
pCYC Day 91 0.7 g/m2
Azathioprine 2 mg/kg/daythen tapered
22 months
CS = corticosteroids; MPS = methylprednisolone; R = rituximab; pCYC = pulse cyclophosphamide

New Evidence in Rheumatology | January 2013 57
ACR/ARHP
• Severe AE rates were comparable in both groups: (Table 1)
In the azathioprine arm, 37 in 30 patients (50.8%);
In the rituximab arm, 32 in 27 patients (50%).
• Deaths during follow-up were observed in 3/117 patients (2.5%), all of whom were in the azathioprine arm; there were no deaths in the rituximab arm.
One patient developed septicemia five months after inclusion. This occurred at the time of relapse when treatment was intensified.
One death due to pancreatic cancer occurred at 24 months after inclusion.
One death resulted from bowel ischemia, 30 months after randomization and at the time of relapse.
• Both event-free survival and overall survival were better in the rituximab group than in the azathioprine group. (Figure 2) (Figure 3)
Figure 1. Main clinical symptoms in the study population
Rituximab
Azathioprine
Total
% Patients
0 50 100
ENT
Lungs
Kidneys
ENT = ear, nose, and throat
Table 1. Severe adverse events in the azathioprine and rituximab groups
Severe Adverse Event Azathioprine Rituximab Outcome
Infections
Lung Infections 4 3 recovery
GI Infections 1 3 recovery
Herpes zoster 2 1 recovery
Septicemia 1 death
Tuberculosis, mycobacteria 1 1 recovery
Pneumocystis 0 1 recovery
Drug Intolerance and Miscellaneous
Hepatitis 3 0 recovery
Lymphopenia 1 1 recovery
Neutropenia 2 0 recovery
Anemia 2 0 recovery
GI ischemia (30 months) 1 0 death
Chills fever 0 3 recovery
Cancers
Skin cancer (basocellular) 2 0 surgery
Prostate cancer 0 1 medical treatment
Pancreatic cancer 1 0 death
Cardiovascular
Atrial fibrillation 1 0 treatment
Venous thrombosis 1 1 recovery
Aortic dissection 1 0 recovery
Endocarditis 1 0 recovery
Metabolic and other disorders
Diabetes 4 5 treatment
Hip osteonecrosis 1 1 surgery
Cataract 6 3 surgery
GI = Gastrointestinal

58 New Evidence in Rheumatology | January 2013
Figure 2. Event-free survival in azathioprine- and rituximab-treated groups
Figure 3. Overall survival in azathioprine- and rituximab-treated groups
0 6 12 18 24
Time from inclusion (months)
Surv
ival
, %
0
20
40
60
80
100
Azathioprine
Rituximab
0 6 12 18 24
Time from inclusion (months)
Surv
ival
, %
0
20
40
60
80
100
Azathioprine
Rituximab
References: 1. Jayne D, Rasmussen N, Andrassy K, et al. A randomized trial of maintenance therapy for vasculitis associated with antineutrophil cytoplasmic autoantibodies. N Engl J Med 2003;349:36–44. 2. Pagnoux C, Mahr A, Hamidou MA, et al. Azathioprine or methotrexate maintenance for ANCA-associated vasculitis. N Engl J Med 2008;359:2790–803. 3. Stone JH, Merkel PA, Spiera R, et al. Rituximab versus cyclophosphamide for ANCA-associated vasculitis. N Engl J Med 2010;363:221–32. 4. Guillevin L, Pagnoux C, Karras A, et al. Rituximab versus azathioprine for maintenance in ANCA-associated vasculitis. ACR Annual Meeting Abstracts 2012;64:1652.
Key conclusions
■ Rituximab is superior to azathioprine in maintaining remission in ANCA-associated vasculitides.
■ A 500-mg dose of rituximab every six months is sufficient to maintain remission. Relapses observed with this regimen are rare.
■ Treatment tolerance was good with a limited number of AEs that were mainly transient.

New Evidence in Rheumatology | January 2013 59
ACR/ARHP
Figure 1. Clinical remission within six months
0.01 0.1
Favours Rituximab
1 10
Favours control
100
Chi2 = chi-squared test; CI = Confidence interval; df = degrees of freedom; M-H = Mantel-Haenszel; RAVE-ITN = Rituximab in ANCA-associated Vasculitis-Immune Tolerance Network; RITUXVAS = Rituximab versus cyclophosphamide in ANCA-associated vasculitis
Study or Subgroup
De Menthon 2011
RAVE-ITN
RITUXVAS 2010
Total (95% CI)
Total events
Heterogeneity: Chi2 = 0.66, df = 2 (p = 0.72); I2 = 0%
Test for overall effect: Z = 1.52 (p = 0.13)
Events
2
29
3
34
Rituximab Control
Total
8
99
33
140
Total
9
98
11
118
Events
5
37
1
43
Weight (%)
10.8
85.7
3.5
100.0
Risk RatioM-H, Fixed, 95% CI
0.45(0.12–1.71)
0.78(0.52–1.15)
1.00 (0.12–8.65)
0.75 (0.51–1.09)
Risk RatioM-H, Fixed, 95% CI
Mejia C, et al. ACR 2012:1543
Rituximab for ANCA-associated vasculitis: a meta-analysis of randomized trials
Background
Over the past 40 years, combination therapy with
cyclophosphamide and glucocorticoids has been the
standard regimen for remission induction in anti-
neutrophil cytoplasmic antibody (ANCA)-associated
vasculitis. Although a major advance in the treatment
of these entities and a superior regimen to the
glucocorticoid monotherapy regimens that preceded
it, nonresponders and the potential for significant
adverse effects (AEs) have been major drawbacks.
The search for new therapeutic options has led to
the investigation of anti-B-cell therapies. Rituximab,
an anti-CD20 monoclonal antibody, has compared
favourably with cyclophosphamide-based regimens
in remission induction in clinical trials, leading to
formal approval by the Food and Drug Adminis-
tration for this indication. It has also been able to
maintain remission for many months of follow-up
without the need for medication-based maintenance
regimens such as azathioprine which is standard in
cyclophosphamide-based regimens.
At ACR 2012, Meija et al presented a meta-analysis that evaluated the clinical benefits of rituximab in ANCA-associated vasculitis.1
Study design
• All randomized controlled trials of rituximab involving patients with ANCA-associated vascu-litis were searched for in PubMed, EMBASE, and Cochrane databases during June 2012.
• Significant nonrandomized controlled trials were also reviewed for a separate analysis.
• Data were extracted by two reviewers and analyzed using RevMan 5 software.
Key findings
• Based on the search, three randomized controlled trials were found.
• Rituximab was shown to be more efficacious in achieving remission and decreasing ANCA titres when analyzing the combined data. (Figure 1) (Figure 2)
• A trend favouring rituximab in achieving remission was also found in nine nonrandomized studies that were analyzed separately. (Figure 3)

60 New Evidence in Rheumatology | January 2013
Figure 2. Decrease in ANCA titres within six months
Figure 3. Clinical remission up to six months (data from non-randomized studies)
0.01 0.1
Favours Rituximab
1 10
Favours control
100
ANCA = antineutrophil associated antibody; Chi2 = chi-squared test; CI = Confidence interval; df = degrees of freedom; M-H = Mantel-Haenszel; RAVE-ITN = Rituximab in ANCA-associated Vasculitis-Immune Tolerance Network; RITUXVAS = Rituximab versus cyclophosphamide in ANCA-associated vasculitis
Study or Subgroup
De Menthon 2011
RAVE-ITN
RITUXVAS 2010
Total (95% CI)
Total events
Heterogeneity: Chi2 = 2.56, df = 2 (p = 0.28); I2 = 22%
Test for overall effect: Z = 3.67 (p = 0.0002)
Events
1
53
0
54
Rituximab Control
Total
5
99
33
137
Total
11
98
10
119
Events
3
75
2
80
Weight (%)
2.3
93.0
4.7
100.0
Risk RatioM-H, Fixed, 95% CI
0.73 (0.10–5.42)
0.70 (0.56–0.87)
0.06 (0.00–1.25)
0.67 (0.54–0.83)
Risk RatioM-H, Fixed, 95% CI
0.01 0.1
Favours Rituximab
1 10
Favours control
100
Chi2 = chi-squared test; CI = Confidence interval; df = degrees of freedom; M-H = Mantel-Haenszel
Study or Subgroup
Briyahe 2007
Eriksson 2005
Henes 2007
Keogh 2005
Keogh 2006
Rachel 2009
Seo 2008
Smith 2006
Stasi 2006
Total (95% CI)
Total events
Heterogeneity: Chi2 = 15.86, df = 8 (p = 0.04); I2 = 50%
Test for overall effect: Z = 9.54 (p < 0.00001)
Events
4
0
1
0
0
16
3
0
1
25
Rituximab Control
Total
8
9
6
11
10
65
8
11
10
138
Total
8
9
6
11
10
65
8
11
10
138
Events
8
9
6
11
10
65
8
11
10
138
Weight (%)
6.0
6.7
4.6
8.1
7.4
46.0
6.0
8.1
7.4
100.0
Risk RatioM-H, Fixed, 95% CI
0.53 (0.27–1.04)
0.05 (0.00–0.79)
0.23 (0.06–0.97)
0.04 (0.00–0.66)
0.05 (0.00–0.72)
0.25 (0.17–0.38)
0.41 (0.18–0.95)
0.04 (0.00–0.66)
0.14 (0.03–0.64)
0.21 (0.15–0.29)
Risk RatioM-H, Fixed, 95% CI

ACR/ARHP
Reference: 1. Mejia C and Lozada C. Rituximab for ANCA-associated vasculitis: a meta-analysis of randomized trials. ACR Annual Meeting Abstracts 2012; 64:1543.
Key conclusions
■ Rituximab has been shown to be an effective alternative for achieving remission in ANCA-associated vasculitis when compared with control in this meta-analysis.
■ The notion of having a therapy that allows better disease control and fewer AEs over a long period of time for the treatment of ANCA-associated vasculitis is promising and more randomized control trials are needed.
Canadian perspective by Dr. Christian Pagnoux
In Canada, the conventional treatment for antineutrophil cytoplasmic antibody (ANCA)- associated vasculitis is cyclo- phosphamide in combination with corticosteroids for remis-sion induction, followed by azathioprine or methotrexate for maintenance. The major problems that may result from this conventional treatment
are infections, infertility and, when given for years, an increased risk of cancers such as basal cell skin carcinoma or lymphoma. Moreover, despite this staged induction-maintenance strategy, our group and others have shown a relapse rate of about 50% at five years.1-3 Owing to these challenges with the current treatment, there was a need for a new therapy.
Rituximab, an anti-CD20 chimeric monoclonal antibody, was introduced in the early 1990s to treat lymphoma and later on received its indication for RA treatment in 2006. In the early 2000s, rituximab was shown to induce remission in patients with refractory or relapsing ANCA-associated vasculitis in some cohort studies and case series. Following the findings of RITUXVAS (Rituximab versus cyclophosphamide in ANCA- associated vasculitis) and RAVE (Rituximab in ANCA-Associated Vasculitis) randomized trials, rituximab was approved for remission induction by the Food and Drug Administration in 2011 and Notice of Compliance was received from Health Canada in the same year.4-6
RITUXVAS was a prospective multicentre trial that included newly diagnosed patients who had renal involvement. The trial showed that induction therapy with rituximab, in combination with two initial cyclophosphamide pulses, had similar efficacy to the conventional staged treatment with corticosteroids and cyclophosphamide for induction followed by azathioprine for
maintenance. The RAVE trial, a noninferiority trial, showed that induction with rituximab alone (one infusion of 375mg/m2 every week for a total of four infusions) or the conventional staged and sequential treatment was noninferior. However, while we were hoping to see a better safety profile with rituximab, the results showed the same rate of adverse events (AEs) in both arms. As a result, rituximab could only be recommended as an alternative to the conventional treatment. There were no major differences among any of the patient subgroups except that patients who relapsed (RAVE trial enrolled patients with new or relapsing disease) responded more often and better to rituximab than those who were newly diagnosed. This finding suggested that in patients who relapsed and who were treated originally with cyclophosphamide, it may be better to switch them to rituximab at the time of their relapse.
Rituximab being noninferior to cyclophosphamide in inducing remission in ANCA-associated vasculitis was an important finding, but with its expensive cost, it could not be seen as more than just an alternative. Currently in Ontario and in Canada, rituximab along with corticosteroids is only approved for the induction treatment of adult patients with granulomatosis with polyangiitis (GPA) or microscopic polyantiitis (MPA) with severe, active disease and who are ANCA positive, and public coverage is offered only according to these indications. Ontario’s criteria specify that rituximab is an alternative for a specific population that cannot be treated with cyclophosphamide such as those at risk of developing cancer and those who need to preserve fertility. In addition, rituximab cannot be used as a first-line treatment. Those who have already received a total dose of cyclophosphamide greater than 25 g (a dose associated with a higher risk of cancer) are also candidates for rituximab induction. It is unfortunate, however, that treatment is limited to ANCA-positive patients as data have shown that ANCA- negative patients can achieve remission with rituximab.7 I certainly would like to be able to treat these patients in my clinic.
New Evidence in Rheumatology | January 2013 61

Other groups may benefit from rituximab such as those who relapsed who received less than 25 g of cyclophosphamide in the past as well as children. Although I treat elderly patients with limited doses of cyclophosphamide, it would be useful to have rituximab as an option for this population in case of relapse. More studies are needed to determine the full capacity of rituximab in vasculitis treatment beyond its current indications in order for it to be approved in other patient populations. Moreover, as shown by the RAVE trial, relapses still occurred after rituximab-based induction therapy at a non-negligible rate. Studies on rituximab addressing long-term efficacy and relapse are therefore very important.
The study by Azar and colleagues from the Cleveland Clinic was retrospective and looked at the long-term efficacy and risks of rituximab. More precisely, the aim was to study whether con-tinuing an immunosuppressant other than corticosteroids after rituximab induction was useful and lowered the relapse rate. The study group consisted of 110 patients with GPA who had received at least one course of rituximab; some of them had repeated courses because they were relapsing or had persistent lingering manifestations. After achieving remission with rituximab, some continued or received maintenance with azathioprine, metho-trexate, or mycophenolate mofetil, whereas the remainder did not receive any other immunosuppressive treatment. Patients who did not receive any maintenance therapy relapsed more often than the ones who did (65% versus 42% after a median of two years; p = 0.006). Based on this study, it is probably better to give an additional agent when using rituximab for induction. However, these results are in contrast to the data from Jones and colleagues (the David Jayne group). They did not observe any differences in the relapse rates of their patients with refractory or relapsing ANCA-associated vasculitis who were given, after rituximab-induction treatment, azathioprine or methotrexate compared with those who were not. Until now, I was proposing azathioprine (or methotrexate) for maintenance after rituximab induction treatment only for patients who were anxious about not continuing any therapy; however, with these new results, I may consider more seriously maintenance with azathioprine (or methotrexate) for my patients until better options become available. Indeed, 42% is still a high relapse rate, so it remains important to investigate different treatment strategies, including perhaps maintenance with rituximab.
As previously mentioned, treatment of ANCA-associated vasculitis requires an induction as well as a maintenance phase. While rituximab has been approved for the induction of remission, its role in maintenance needs to be explored. In a retrospective study published recently by the David Jayne group, patients with refractory or relapsing ANCA-associated vasculitis were either induced with rituximab then systematically infused with rituximab at 1 g every six months for at least two years or they did not receive any further systematic treatment.8 The results showed 73% relapse in the patients who were not
receiving systematic rituximab treatment compared with only 12% relapse in the patients who did. In France, we have tried different regimens of rituximab infusions for maintenance and have seen a decrease in the relapse rate to 7% but these results still require confirmation by means of randomized controlled trials.
To this end, our MAINtenance of remission using RITuximab in Systemic ANca associated vasculitides (MAINRITSAN) study aimed to determine whether systematic rituximab reinfusions could be used as treatment for maintenance in comparison with the conventional approach that included azathioprine, metho-trexate or, less frequently, mycophenolate mofetil. It was an open-label randomized study that included 117 adult patients with severe GPA or MPA who had achieved remission with cyclo-phosphamide but not rituximab because it was not the first-line therapy (with the findings of the RAVE trial, we know now that rituximab is not superior to cyclophosphamide). Two thirds of the patients had a new diagnosis and the remaining third had relapsed. At randomization, all patients were in remission. Consequently, for those randomized to rituximab, we went with a lower dose of rituximab (500 mg per infusion) for maintenance, given on days 1 and 14 then every six months until month 18. Patients in the azathioprine arm received treatment for a slightly longer time than the patients in the rituximab arm (22 months versus 18 months) since the effect of rituximab would probably last longer than that of azathioprine after administering the last dose. We waited until month 28 to assess response because we thought that most of the relapses may happen after treatment cessation. Our results showed an impressive difference in the rate of major relapses between patients in the azathioprine arm compared with those in the rituximab arm (25% versus 5%). There were no significant differences in the rate of AEs; however there were three deaths in the azathioprine arm but none in the rituximab arm. A cost-effectiveness analysis still needs to be done, but the results are really obvious.
At present, the optimal regimen and duration of maintenance treatment are still not well known and some adjustments may be needed when using rituximab. One could decide to wait for early signs of relapse before giving rituximab again, and thus treat as needed only, which can be hazardous. One could follow B-cell status and ANCA titres (this will be the topic of the MAINRITSAN 2 trial) and treat accordingly. Finally, one could give systematic rituximab infusions; this is what we would recommend now based on our MAINRITSAN study data. We think that rituximab can be recommended for maintenance after cyclophosphamide induction, and likely also for patients induced with rituximab. We believe that giving a moderate dose every six months will be beneficial for patients as well as cost-effective. In France, following the MAINRITSAN trial, we are now suggesting an infusion with rituximab at a dose of 500 mg every six months for two years and then potentially moving to a yearly infusion of 1 g for several additional years.
62 New Evidence in Rheumatology | January 2013

ACR/ARHP
A new international study Rituximab Vasculitis Maintenance
Study (RITAZAREM) will start soon. This is an international
randomized trial comparing rituximab versus azathioprine as
maintenance therapy, but only in patients who have relapsed,
who have ANCA-associated vasculitis and after rituximab-based
induction therapy (based on the RAVE trial, rituximab is superior
to cyclophosphamide for induction in this patient subset). It will
involve several centres around the world. In Canada, we plan
to enrol at least eight patients, four in Toronto and four in
Hamilton. Patients will be induced with corticosteroids and
rituximab and if disease is stable at four months, they will be
randomized to receive either azathioprine until month 27 or
rituximab at 1 g every four months. It is anticipated that the
study will be completed in 2016.
New Evidence in Rheumatology | January 2013 63
Reference: 1. Pagnoux C, Mahr A, Hamidou MA, et al. Azathioprine or methotrexate maintenance for ANCA-associated vasculitis. N Engl J Med 2008;359:2790-803. 2. Sanders JS, Slot MC, Stegeman CA. Maintenance therapy for vasculitis associated with antineutrophil cytoplasmic autoanti-bodies. N Engl J Med 2003;349:2072-3. 3. Holle JU, Gross WL, Latza U, et al. Improved outcome in 445 patients with Wegener’s granulomatosis in a German vasculitis center over four decades. Arthritis Rheum 2011;63:257-66. 4. Cartin-Ceba R, Fervenza FC, Specks U. Treatment of antineutrophil cytoplasmic antibody-associated vasculitis with rituximab. Curr Opin Rheumatol 2012;24:15-23. 5. Jones RB, Tervaert JW, Hauser T, et al. Rituximab versus cyclophosphamide in ANCA-associated renal vasculitis. N Engl J Med 2010;363:211-20. 6. Stone JH, Merkel PA, Spiera R, et al. Rituximab versus cyclophosphamide for ANCA-associated vasculitis. N Engl J Med 2010;363:221-32. 7. Jones RB, Ferraro AJ, Chaudhry AN, et al. A multicenter survey of rituximab therapy for refractory antineutrophil cytoplasmic antibody-associated vasculitis. Arthritis Rheum 2009;60:2156-68. 8. Smith RM, Jones RB, Guerry MJ, et al. Rituximab for remission maintenance in relapsing antineutrophil cytoplasmic antibody-associated vasculitis. Arthritis Rheum 2012;64:3760-9.
64 New Evidence in Rheumatology | January 2013
Investigator Commentaries
New Evidence: Why is there a need to find alternatives for azathioprine and methotrexate for maintenance
therapy in ANCA-associated vasculitis?
Dr. Pagnoux: The conventional treatment to induce remission in patients with ANCA-associated vasculitis
is cyclophosphamide in combination with corticosteroids. Patients are then given either azathioprine or
methotrexate for maintenance, both of which have similar efficacy and safety. However, the rate of relapse
with these treatments can reach over 50% at five years. Therefore, improvements in available treatments for
maintenance are needed to reduce relapse rates.
New Evidence: What were the advantages of using rituximab for maintenance therapy in your study?
Dr. Pagnoux: The main advantage to using rituximab as maintenance therapy in our study was the
increased efficacy of this agent compared with azathioprine, in terms of prevention of major relapses. Of
those patients treated with azathioprine, 25% relapsed compared with 5% treated with rituximab after
28 months of follow-up. This was a significant difference with only three patients out of a total of 58 in the
rituximab arm experiencing major relapses; we were very happy with these results as we were looking for a
clear difference due to cost concerns.
At the ACR/ARHP 2012 Annual Scientific Meeting, New Evidence spoke with Dr. Christian Pagnoux, faculty member of the Division of Rheumatology at Mount Sinai Hospital, Toronto, about the results of the RITuximab in Systemic ANca associated vasculitis (MAINRITSAN) study in which he was coprimary investigator with Dr. Loïc Guillevin. The study examined rituximab systematic reinfusion treatment for maintenance in ANCA-associated vasculitis compared with conventional treatment.
An Interview with Dr. Christian Pagnoux on the MAINRITSAN study that examined the efficacy and safety of rituximab compared with azathioprine for maintenance in antineutrophil cytoplasmic antibodies (ANCA)-associated vasculitis

New Evidence in Rheumatology | January 2013 65
New Evidence: What were the limitations of your study?
Dr. Pagnoux: One of the study limitations was the age restriction in the patient population as it consisted only of adults between the ages of 18 and 75 years; therefore, the results cannot be applied to younger or older patients. The study population was also slightly heterogeneous, as we enrolled those who relapsed and newly diagnosed patients but we stratified them at enrolment according to these categories, 1/3 and 2/3, respectively. Conversely, one advantage of this heterogeneity is that the results obtained can be applicable to both patient populations. We are also planning to conduct some more subtle subgroup analyses.
Another limitation includes the study being open label; however, the difference in the relapse rate between both groups was so overt that it is unlikely due only to the open-label design. As for it being multicentric, this should not be seen as a limitation or source of heterogeneity, especially since the criteria for inclusion and treatment protocols were clear and the study was closely monitored.
New Evidence: What is the rationale for having patients with different diagnoses as part of your study and did you stratify them based on these subgroups?
Dr. Pagnoux: Our patient population is typical of an ANCA-associated vasculitis study and we did not do any stratification based on diagnoses. We had 88 patients with granulomatosis with polyangiitis, 24 patients with micropolyangiitis, and five patients with kidney-limited disease. At present, these patients are often combined in therapeutic studies because they are all treated the same way, and there is no definite evidence yet to change or adjust the treatment based on the different diagnoses.
New Evidence: What dose of rituximab was given to the patients in this study and why?
Dr. Pagnoux: We used 500 mg on days 1 and 14, then every six months with the last infusion treatment at 18 months. We based our decision on the fact that the patients were in remission, B-cell depleted, and no longer had active disease and, therefore, did not require the higher doses given for induction. We decided on the six-month time point based on the duration of B-cell depletion and the occurrence of relapses in previous case series, including some of our French group series.
New Evidence: Were there any significant differences in the adverse events (AEs) observed between both study arms?
Dr. Pagnoux: There were no significant differences in the AEs observed in both arms. There were, however, more dropouts in the azathioprine arm due to AEs such as gastrointestinal intolerance, hepatitis, and cytopenia. This was not observed with the rituximab arm. There were also three deaths in the azathioprine arm but none in the rituximab arm.
New Evidence: Were there any safety concerns with using rituximab in maintenance therapy?
Dr. Pagnoux: There were no major safety concerns with using these repeated infusions of rituximab for maintenance until month 18. However, one patient developed pulmonary pneumocystosis. It is, therefore, important to administer prophylactic treatment with cotrimoxazole (trimethoprim-sulfamethoxazole) to avoid this complication. An extremely rare complication with rituximab treatment is progressive multifocal leukoencephalopathy but there have been no such cases reported to date for patients with vasculitis treated with rituximab. However, a few cases have been observed with the conventional treatment; so it can be caused by any immunosuppressant.
New Evidence: Did you do any biomarker analysis in your study?
Dr. Pagnoux: We know that 40% to 50% of patients relapse with the conventional treatment but we still have no means of detecting them early with sufficiently sensitive and specific biomarkers. In our MAINRITSAN study, we did systematic and serial serum collections but no analyses have yet been performed. We will be analyzing CD19 lymphocyte counts and ANCA titres and will likely study other potential biomarkers. Identifying biomarkers predictive of relapse may help determine which patients require maintenance and which ones do not really need it or only for a shorter time.

66 New Evidence in Rheumatology | January 2013
New Evidence: Do you feel the study results are strong enough to change current clinical practice or are additional analyses needed to assess the efficacy and safety of rituximab as maintenance therapy?
Dr. Pagnoux: I believe that the results are strong enough to plead for a change in our clinical practice. I am confident that rituximab is a better treatment for maintenance than azathioprine as our results show high efficacy with rituximab and no differences in the safety profile. For patients who achieve remission, we should now seriously consider the possibility of using rituximab at a moderate dose as a maintenance regimen. We will also continue to do subgroup analysis to determine whether certain groups may be better candidates for receiving rituximab rather than conventional drugs like azathioprine.
New Evidence: What is the duration of maintenance treatment with rituximab that you propose?
Dr. Pagnoux: As three quarters of the relapses occur after the cessation of the maintenance treatment when using conventional therapy, it is possible that patients may need maintenance for years if not for life, even when using rituximab for induction. Long-term follow-up of our patients in the MAINRITSAN study is important and ongoing. Importantly, treatment will need to be balanced against the AEs. Based on our current results, I would propose using rituximab at 500 mg every six months up to 18 months.
New Evidence: Would you use rituximab for maintenance in your clinical practice?
Dr. Pagnoux: I would love to use rituximab for maintenance in my clinical practice but it is not possible in Canada at the moment as it is only approved for induction treatment. However with the data obtained from this randomized controlled trial, along with evidence from other previous open and retrospective studies supporting these results, we may try, perhaps in collaboration with some official therapeutic committees in Canada, to apply for coverage for patients in Ontario first, and if successful, we will extend our efforts to all of Canada.

New Evidence in Rheumatology | January 2013 67
New Evidence: What was the rationale for your study hypothesis?
Dr. Guillevin: Our hypothesis was that 40% of the patients in the azathioprine arm will relapse and this was based on previous trials. As for the 15% relapse rate in the rituximab arm, the number was chosen arbitrarily because we were the first to try this treatment. Our choice had also a financial basis because we thought that rituximab should demonstrate a very clear improvement in the relapse rate for it to be of interest. If rituximab were to have a similar efficacy to azathioprine or if it were to be even slightly better, it would still not be interesting enough especially since it is an expensive drug.
New Evidence: What were the reasons for using a low dose of rituximab for maintenance?
Dr. Guillevin: We had many discussions about the appropriate dose to be used in our study especially in light of higher doses being used by other groups. However, we decided to use a lower dose for two reasons: the first being that our patients were in full remission and secondly, to minimize the risk of adverse effects (AEs) including infections. Finally, from an economic perspective, using 500 mg every six months was a reasonable option.
New Evidence: Did you have any information on the B-cell status of the patients who relapsed?
Dr. Guillevin: We haven’t analyzed ANCA titres and CD19 expression yet but we have collected this information. Our new trial — MAINRITSAN 2 (MAINtenance of remission using RITuximab in Systemic ANca associated vasculitis) — will adapt the infusion of rituximab according to the different biological parameters including CD19 levels.
In the MAINRITSAN 2 trial, one arm will be MAINRITSAN 1 (the current study) and in the other arm we will monitor CD19, clinical manifestations, and ANCA titres. If we observe any changes in the clinical manifestations, or any increases in ANCA titres and CD19 expression, we will pulse with rituximab; otherwise we will wait another three months.
At the ACR/ARHP 2012 Annual Scientific Meeting, New Evidence spoke with Dr. Loïc Guillevin, Professor of Medicine and Therapeutics, Head of the Department of Internal Medicine, Cochin Hospital, University of Paris Descartes, Sorbonne Paris Cité. The discussion focused on the results of his study that examined rituximab systematic reinfusion treatment for maintenance in ANCA-associated vasculitis versus the conventional treatment.
An Interview with Dr. Loïc Guillevin on the MAINRITSAN study that examined the efficacy and safety of rituximab compared with azathioprine for maintenance in antineutrophil cytoplasmic antibodies (ANCA)-associated vasculitis

68 New Evidence in Rheumatology | January 2013
New Evidence: Do you think more studies are needed to improve the relapse rate you observed in your study?
Dr. Guillevin: I am not sure whether more studies looking at rituximab for maintenance will show a better relapse rate than the one we observed. RITAZAREM (rituximab vasculitis maintenance study) — is being planned in which it is proposed that 1 g be given every four months and with a longer follow-up. However, I believe there will be more AEs with this high dose. In my opinion, it is much better to give a low dose of rituximab and reinfuse if needed.
New Evidence: Do you think the use of rituximab in maintenance is more important than its use in induction?
Dr. Guillevin: For maintenance we are clearly at a time when we need to change the standard of care and rituximab could or would become the main treatment. For remission induction, we have alternatives since both the conventional treatment and rituximab were shown to have similar efficacy and safety profiles.
New Evidence: Why was there a high dropout rate in the azathioprine arm?
Dr. Guillevin: The high dropout rate in the azathioprine arm was mainly due to AEs that included intolerance, hepatitis, and skin cancers among others. The treatment regimen was not very well tolerated.
New Evidence: Do you think rituximab should be the standard treatment for maintenance based on the results of this study or do you think there is a need for further studies?
Dr. Guillevin: I think rituximab could become the standard treatment for maintenance in ANCA-associated vasculitis. Usually it is much better to have another confirmatory trial but this one is very convincing, and the difference between both arms is very large. These are not the complete results yet, but we are aiming to have the full analysis completed within the first three months of 2013.
New Evidence: In your practice in France do you use rituximab as a maintenance treatment?
Dr. Guillevin: We have used it in the study protocol. Importantly, we have a meeting in the near future to publish the guidelines for the French practice during which I will be recommending rituximab as a maintenance treatment.