Embed Size (px)
Citation preview

EDUCATION EXHIBIT 417
Hypoxic-IschemicBrain Injury: ImagingFindings from Birth toAdulthood1
LEARNINGOBJECTIVESFOR TEST 2After reading thisarticle and takingthe test, the reader
will be able to:
� Discuss the factorsthat influence pat-terns of injury inhypoxic-ischemicbrain injury.
� Identify the variousUS, CT, and MRimaging features ofhypoxic-ischemicbrain injury.
� Describe the ap-propriate imagingwork-up for sus-pected hypoxic-isch-emic brain injury.
Benjamin Y. Huang, MD, MPH ● Mauricio Castillo, MD
Global hypoxic-ischemic injury (HII) to the brain is a significant causeof mortality and severe neurologic disability. Imaging plays an impor-tant role in the diagnosis and treatment of HII, helping guide casemanagement in the acute setting and providing valuable informationabout long-term prognosis. Appropriate radiologic diagnosis of HIIrequires familiarity with the many imaging manifestations of this in-jury. Factors such as brain maturity, duration and severity of insult,and type and timing of imaging studies all influence findings in HII.Severe hypoxia-ischemia in both preterm and term neonates preferen-tially damages the deep gray matter, with perirolandic involvementmore frequently observed in the latter age group. Less profound insultsresult in intraventricular hemorrhages and periventricular white matterinjury in preterm neonates and parasagittal watershed territory infarctsin term neonates. In the postnatal period, severe insults result in diffusegray matter injury, with relative sparing of the perirolandic cortex andthe structures supplied by the posterior circulation. Profound hypoxia-ischemia in older children and adults affects the deep gray matter nu-clei, cortices, hippocampi, and cerebellum. Because findings at con-ventional imaging may be subtle or even absent in the acute setting,particularly in neonates, magnetic resonance spectroscopy can helpestablish the diagnosis of HII. Promising new neuroprotective strate-gies designed to limit the extent of brain injury caused by hypoxia-isch-emia are currently under investigation.©RSNA, 2008
Abbreviations: ADC � apparent diffusion coefficient, ATP � adenosine triphosphate, CSF � cerebrospinal fluid, HII � hypoxic-ischemic injury,NAA � N-acetylaspartate, NMDA � N-methyl-d-aspartate, PVL � periventricular leukomalacia
RadioGraphics 2008; 28:417–439 ● Published online 10.1148/rg.282075066 ● Content Codes:
1From the Department of Radiology, University of North Carolina at Chapel Hill, 101 Manning Dr, CB 7510, Chapel Hill, NC 27599-7510. Pre-sented as an education exhibit at the 2006 RSNA Annual Meeting. Received April 5, 2007; revision requested June 13 and received July 30; acceptedAugust 3. Both authors have no financial relationships to disclose. Address correspondence to B.Y.H. (e-mail: [email protected]).
©RSNA, 2008
Note: This copy is for your personal, non-commercial use only. To order presentation-ready copies for distribution to your colleagues or clients, use the RadioGraphics Reprints form at the end of this article.
CME FEATURESee accompanying
test at http://www.rsna.org
/education/rg_cme.html
See last page
TEACHING POINTS

IntroductionHypoxic-ischemic injury (HII) to the brain is adevastating occurrence that frequently results indeath or profound long-term neurologic disabilityin both children and adults. Treatment of HIIconsists largely of supportive care, which doeslittle to prevent the ongoing injury that occurs inthe hours immediately following the causativeinsult. Promising new neuroprotective strategiesdesigned to limit the extent of brain injury causedby hypoxia-ischemia are under investigation.Many of these treatment strategies, including hy-pothermia and administration of excitatory aminoacid antagonists, have a limited window of effec-tiveness (in some cases as little as 6 hours), mak-ing early detection of injury critically important(1,2). Neuroimaging with ultrasonography (US),computed tomography (CT), and magnetic reso-nance (MR) imaging has become increasinglyvaluable in the work-up of patients with HII. Asmore effective treatment options become avail-able, imaging—particularly MR imaging—has thepotential to play a significant role in diagnosis andearly intervention in cases of HII. In addition,imaging studies performed in the subacute stagesof injury provide information on the severity andextent of injury and can be helpful in predictinglong-term outcome (3–6).
Imaging findings in HII are highly variable anddepend on a number of factors, including brainmaturity, severity and duration of insult, and typeand timing of imaging studies. Early imagingfindings can be subtle and are often overlooked.Therefore, it is essential to be familiar with themany patterns of injury that may be observed andto focus attention on areas that are most likely tobe injured when interpreting studies performedfor suspected HII.
In this article, we review the pathophysiologicfeatures of HII and the factors that influence thepattern of injury; review the specific imagingmanifestations of HII in term (�36 weeks gesta-tional age) and preterm (�36 weeks gestationalage) neonates, postnatal infants, children, andadults; describe the emerging role of proton MRspectroscopy in the evaluation of HII; and discussimaging choices for the evaluation of this injury.
Pathophysiologic Pro-cesses and Factors Influenc-
ing the Patterns of Injury in HII
Regardless of the specific cause of injury, thecommon underlying physiologic processes that
result in HII are diminished cerebral blood flow(ischemia) and reduced blood oxygenation (hy-poxemia). In general, infants and children aremore likely to suffer asphyxial events, which resultin hypoxemia and brain hypoxia. With prolongedhypoxemia, cardiac hypoxia occurs, leading todiminished cardiac output and, ultimately, tobrain ischemia. Thus, brain injury resulting fromasphyxia is the consequence of ischemia superim-posed on hypoxia. In fact, acute hypoxemia with-out superimposed ischemia is less likely to causeinjury, unless the hypoxic state is prolonged (7,8).On the other hand, adults more frequently sufferbrain ischemia as a result of cardiac arrest or cere-brovascular disease, with secondary hypoxia dueto reduced blood flow (8).
It is well known that global hypoxic-ischemicinsults do not affect all brain structures uni-formly. Rather, certain tissues in the brain aremore likely to be injured and are injured earlierthan others, a concept known as selective vulner-ability. Evidence suggests that the observed pat-terns of injury reflect dysfunction of selected exci-tatory neuronal circuits, which causes a complexcascade of deleterious biochemical events and,ultimately, selective neuronal death (7). Brainischemia results in a switch from oxidative phos-phorylation to anaerobic metabolism, which ishighly inefficient. This change causes rapid deple-tion of adenosine triphosphate (ATP), lactate ac-cumulation within cells, and eventual loss of nor-mal cellular membrane function. Depolarizationof presynaptic neuronal cell membranes causes amassive release of excitatory neurotransmitters—in particular, glutamate. In immature brains,glutamate binds predominantly to N-methyl-d-aspartate (NMDA) receptor–mediated calcium(Ca2�) channels. Activation of NMDA receptorsresults in an influx of Ca2� into postsynaptic neu-rons, which triggers a number of cytotoxic pro-cesses, including activation of membrane phos-pholipases and production of the oxygen freeradicals (such as nitric oxide) that damage cellmembranes and internal constituents. Damage tomitochondria may ensue, causing further loss ofATP production and, ultimately, energy deple-tion. Severe energy depletion results in rapid celldeath from necrosis. With lesser degrees of energydepletion, neurons may survive the initial insult,only to undergo a delayed form of programmedcell death known as apoptosis (Fig 1) (1,7–9).Apoptosis appears to play a significant role in in-jury to the immature brain.
From the model just described, we can drawthe following conclusions: (a) the areas of thebrain with the highest concentrations of gluta-
418 March-April 2008 RG f Volume 28 ● Number 2
TeachingPoint

mate or other excitatory amino acid receptors(primarily located in gray matter) are more sus-ceptible to excitotoxic injury that occurs as a re-sult of hypoxia-ischemia; (b) the areas of thebrain with the greatest energy demands becomeenergy depleted most rapidly during hypoxia-ischemia, and are therefore injured early on; and(c) because of delayed cell death from apoptosis,some injuries may not be evident until days afterthe initial insult has occurred. These factors helpto explain the relatively specific patterns of injurythat can be observed in patients with HII.
In any given patient, the sites in the brain thattend to be most vulnerable to hypoxic injury willbe determined largely by the maturity of thebrain, which, in turn, is a function of patient ageand, in infants, gestational age at birth. This iswhy HII in the perinatal period (up to 1 month ofage) differs from HII in adults or even in olderinfants and why the imaging appearance of HIIdiffers between term and preterm neonates. Onemust be cognizant of the degree of brain maturity
at the time of the insult when interpreting studiesfor suspected HII.
The severity of a hypoxic-ischemic insult alsoplays an important role in determining the distri-bution of injuries in the brain. Episodes of severehypoxia-ischemia result in a different injury pat-tern compared with less severe insults. Durationof insult also seems to be a key determinant of thepattern of injury in HII, since insults of short du-ration usually do not result in brain injury. It hasbeen suggested that, in the pediatric population,an arrest must typically last at least 15 minutes forbrain injury to occur (10).
HII in the Term NeonateHII continues to be a major cause of death andneurodevelopmental disability in term neonates,although its prevalence appears to be declining.The prevalence of HII is estimated to be between
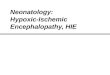
Figure 1. Diagram illustrates the cascade of events contributing to brain injury inhypoxia-ischemia. Brain ischemia results in a switch from oxidative phosphoryla-tion to anaerobic metabolism, causing rapid depletion of ATP, lactate accumula-tion within cells, and eventual loss of normal cellular membrane function. Depolar-ization of presynaptic neuronal cell membranes causes a massive release of gluta-mate, which binds to NMDA receptor–mediated Ca2� channels. Activation ofNMDA receptors results in an influx of Ca2� into postsynaptic neurons, triggeringa number of cytotoxic processes, including production of the oxygen free radicalsthat damage cell constituents (eg, mitochondria). Mitochondrial injury causes fur-ther loss of ATP production and energy depletion. In addition, depletion of ATPfurther perpetuates the cycle by inhibiting the activity of ATP-dependent glutamatereuptake pumps. Severe energy depletion results in rapid cell death by necrosis.Lesser degrees of energy depletion result in apoptosis.
RG f Volume 28 ● Number 2 Huang and Castillo 419

two and four per 1000 live term births (10). Be-tween 15% and 20% of infants suffering HII dieduring the neonatal period, and an additional25% develop permanent neurologic deficits (2).Potential risk factors for the development of neo-natal HII can be separated into antepartum, in-trapartum, and postpartum factors. In most cases,HII in term neonates is associated with antepar-tum risk factors alone (including maternal hypo-tension, infertility treatment, multiple gestation,prenatal infection, and thyroid disease) or ante-partum factors in combination with intrapartumfactors. Intrapartum factors alone (including for-ceps delivery, breech extraction, umbilical cordprolapse, abruptio placentae, tight nuchal cord,and maternal fever) are responsible for a smallminority of cases of HII. Only 10% of cases ofHII in term neonates are associated with postna-tal complications such as severe respiratory dis-tress, sepsis, or shock (11,12).
Clinical signs and symptoms of neonatal HIIcan be nonspecific at birth and usually evolve overa period of days (11), but data suggest that infantsat highest risk for having suffered severe HII canbe identified with reasonable reliability on thebasis of a constellation of clinical findings. Thesefindings include evidence of intrapartum distress(eg, fetal heart rate abnormality), severe func-tional depression (indicated by a low 5-minuteApgar score), need for resuscitation in the deliv-ery room, severe fetal acidemia, an abnormalearly neurologic examination, and an abnormalelectroencephalogram (1). In the first hours fol-lowing a severe insult, neonates may demonstratedepressed consciousness, periodic breathingwith apnea, or bradycardia. Hypotonia may bepresent, particularly if there has been injury to thecortical regions, and seizures may occur in casesof severe injury (11). Infants who survive a severehypoxic insult typically go on to develop quadri-paresis, choreoathetosis, severe seizure disorders,or mental retardation. Patients with moderateinjuries invariably develop spastic diplegia orquadriplegia (often falling under the umbrellaterm cerebral palsy) (10). In cases of mild HII, pa-tients may recover completely or be mildly devel-opmentally delayed.
The imaging characteristics of HII in termneonates can be subdivided based on the severityof injury (severe versus mild to moderate [partial]asphyxia). This subdivision is somewhat simplis-tic, since HII comprises a continuous range ofinsults that vary in both severity and duration.Hence, features of both severe and partial as-phyxia may be seen in any given patient.
Transfontanelle cranial US is usually the firstneuroimaging study to be performed in neonateswith suspected HII. Although abnormalities canbe detected at US, the sensitivity of this modalityis low; therefore, a negative study should not beinterpreted as definitive evidence that no injuryhas occurred. If clinical suspicion for HII re-mains, MR imaging should be performed toevaluate for the presence and severity of injury. Itis important to keep in mind that the histologicand biochemical features of injured tissue evolveover time, so that the results of a study performedhours after an anoxic episode can differ signifi-cantly from those of a study performed severaldays later.
Severe AsphyxiaSevere asphyxial events in term neonates result ina primarily central pattern of injury involving thedeep gray matter (putamina, ventrolateral thal-ami, hippocampi, dorsal brainstem, and lateralgeniculate nuclei) and occasionally the perirolan-dic cortex. These areas of the brain are activelymyelinating (an energy-intensive process) or con-tain the highest concentrations of NMDA recep-tors at term (4,13) and are, therefore, the mostsusceptible to neonatal HII. The remainder of thecerebral cortex is generally spared or shows mildinsults, since it is generally less metabolically ac-tive in the immediate perinatal period; however,with more prolonged insults, the remaining cortexwill become involved, a finding that generally por-tends a worse neurologic outcome (10).
Cranial US performed in the 1st week of life interm neonates has a fairly low sensitivity (�50%)for detecting abnormalities due to HII (14,15),but its sensitivity increases when it is performedafter 7 days. Early US findings include a globalincrease in cerebral echogenicity and obliterationof the cerebrospinal fluid (CSF)–containingspaces, suggesting diffuse cerebral edema. In-creased echogenicity in the basal ganglia, thalami,and brainstem can also be seen in the 1st weekbut is more readily apparent after 7 days (15,16).The presence of thalamic echogenicity generallysuggests a more severe injury and correlates witha poorer outcome (17). Late findings includeprominence of the ventricles and extraaxial CSF-containing spaces, likely due to atrophy. The useof cerebral arterial Doppler US during US evalua-tion performed in the first few days of life mayimprove sensitivity and specificity for brain injury,since the presence of diminished resistive indexes(�60) in the anterior and middle cerebral arterieshas been associated with a poor clinical outcome,even in the absence of other US abnormalities(14).
420 March-April 2008 RG f Volume 28 ● Number 2

MR imaging is an accurate modality for evalu-ating neonatal HII. Diffusion-weighted imaging issensitive for the detection of injury in the first 24hours, during which time conventional T1- andT2-weighted images may appear normal. Diffu-sion-weighted images will demonstrate increasedsignal intensity in the region of the ventrolateralthalami and basal ganglia (particularly the poste-rior putamina), in the perirolandic regions, andalong the corticospinal tracts (Fig 2). It should benoted that diffusion-weighted MR imaging per-formed during this period will often lead to un-derestimation of the ultimate extent of injury(18,19); indeed, normal findings at diffusion-weighted imaging performed in the first 24 hours,although uncommon, have been reported (18). Itis believed that the prominent role of apoptosis inneonatal HII may explain why diffusion-weightedimaging in the acute setting leads to underestima-tion of injury. Abnormalities seen at diffusion-weighted imaging generally peak at 3–5 days andsubsequently “pseudonormalize” by about theend of the 1st week (4,6,10,20), although de-creased ADC values can persist in injured regions
into the 2nd week (18,20). It should be notedthat, although diffusion-weighted images seem-ingly improve and appear relatively normal by theend of the 1st week, this finding does not implythat there has been improvement or reversal ofunderlying disease. Hence, we use the termpseudonormalization to indicate the apparent reso-lution of signal intensity abnormalities on diffu-sion-weighted images. Because of the (admittedlyunlikely) possibility of a false-negative diffusion-weighted MR imaging study early in neonatal life,a negative MR imaging study performed for HIIin the first 24 hours should prompt either repeatMR imaging at 2–4 days, when diffusion abnor-malities are expected to be greatest, or evaluationwith proton MR spectroscopy.
Conventional T1- and T2-weighted MR im-ages obtained on day 1 are frequently normaland are therefore less useful than diffusion-weighted images obtained for the diagnosis of HIIin the acute setting. By day 2, injured areas may
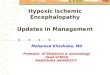
Figure 2. Severe neonatalHII in a 2-day-old term infantwho suffered severe birth as-phyxia. (a, b) Diffusion-weighted MR images showincreased signal intensity inthe ventrolateral thalami (ar-rows in a) and perirolan-dic cortex (arrows in b).(c, d) Corresponding appar-ent diffusion coefficient(ADC) maps show low signalintensity in the ventrolateralthalami (arrows in c) and peri-rolandic cortex (arrows in d).
RG f Volume 28 ● Number 2 Huang and Castillo 421

demonstrate hyperintensity on both T1- and T2-weighted images (Fig 3). Signal intensity changescan also be seen in the dorsal brainstem and hip-pocampi (13). T2 shortening subsequently devel-ops in the thalami and posterior putamina, usu-ally by the 2nd week after insult (19). T1 shorten-ing in the thalami, basal ganglia, and perirolandiccortex may persist for several months (13). Theexact cause of the observed signal intensitychanges seen at conventional MR imaging duringthe 1st week remains unclear. Suggested possiblecauses of T1 shortening include hemorrhage, cal-cification, lipid release from myelin breakdown,and even the paramagnetic effects of free radicals(13,21). Some investigators discount hemorrhageas a potential cause of early T1 shortening basedon the observation that T2 shortening does notoccur until several days after the initial T1changes have occurred (19). One histologic study
has reported clusters of mineralized neurons inthe globus pallidus and thalamus in asphyxiatedinfants, findings that suggest mineralization as thecause of specific signal intensity changes on T1-and T2-weighted images (22), but this remainscontroversial. Furthermore, some controversyexists regarding the timing of signal intensitychanges in the basal ganglia at T2-weighted imag-ing, with some authors reporting that T2-weighted images are usually normal during the1st week, with T2 shortening appearing after7–10 days (23). This discrepancy may be due tothe inherently high water content of the neonatalbrain, which may make subtle changes associatedwith edema in the acute stages of injury difficultto appreciate on T2-weighted images. In general,conventional T1- and T2-weighted images aremost diagnostically useful at the end of the 1stweek, when abnormalities at diffusion-weightedimaging have pseudonormalized (Fig 3). In thechronic stage of injury, atrophy of the injured
Figure 3. Severe neonatalHII in a 7-day-old term infant.(a) Axial T1-weighted MRimage obtained at the level ofthe basal ganglia shows in-creased signal intensity in thelentiform nuclei (*) and ven-trolateral thalami (arrows).(b) T2-weighted MR imageshows decreased signal inten-sity in the posterior aspects ofthe putamina (arrowheads)and ventrolateral thalami (ar-rows). (c) Diffusion-weightedMR image shows a relativelack of hyperintensity in thelocations cited in b, findingsthat represent pseudonormal-ization. Only the left globuspallidus shows high signal in-tensity. (d) CorrespondingADC map shows hypointen-sity in the posterior putamina(arrowheads) and ventrolateralthalami (arrows).
422 March-April 2008 RG f Volume 28 ● Number 2
TeachingPoint

structures will be seen along with T2 hyperinten-sity, particularly in the ventrolateral thalami, pos-terior putamina, and corticospinal tracts (Fig 4)(13).
When bilateral basal ganglia lesions are seen ina neonate, the primary differential diagnostic con-siderations are underlying inborn errors of metab-olism—especially mitochondrial disorders, whichshould be suspected when (a) there is little clini-cal evidence for intrapartum hypoxia-ischemia;and (b) unusual imaging findings such as hetero-topia, atrophy, or localized white matter abnor-malities are seen (24).
Partial AsphyxiaLess severe insults result in a different pattern ofinjury. Experiments performed in animal modelshave demonstrated that episodes of prolongedfetal hypoxia result in shunting of blood to vitalbrain structures, such as the brainstem, thalami,basal ganglia, hippocampi, and cerebellum, at theexpense of less metabolically active structures,namely, the cerebral cortex and white matter
(25). Therefore, the brainstem, cerebellum, anddeep gray matter structures are generally sparedfrom injury in mild to moderate hypoxic-ischemicinsults, since autoregulatory mechanisms are ableto maintain perfusion to these areas of the brain.In neonates, moderate insults of short durationcause little or no injury to the brain (10); how-ever, more prolonged insults result in injury to theintervascular boundary (watershed) zones, whichare relatively hypoperfused as a result of thisshunting. Affected patients tend to present withseizures or hypotension. Neurologic examinationmay eventually demonstrate proximal extremityweakness or spasticity (10).
Cranial US is of limited use in the detection ofcortical and subcortical watershed zone injuries,given their location relative to the calvaria. There-fore, MR imaging is the modality of choice interm infants who experience partial asphyxialevents. Again, diffusion-weighted images are theearliest to change, usually within the first 24
Figure 4. Severe neonatal HII in a5-day-old term infant who sufferedprofound birth asphyxia. (a, b) AxialT1-weighted MR images show hy-perintensity in the ventrolateral thal-ami (arrowheads in a), basal ganglia(arrows in a), and perirolandic cor-tex (arrows in b). (c, d) Axial T2-weighted MR images obtained ap-proximately 7 months later showdiffuse atrophy as well as hyperinten-sity (gliosis) in the ventrolateral thal-ami (arrowheads in c), posterior pu-tamina (arrows in c), and perirolan-dic regions (arrows in d).
RG f Volume 28 ● Number 2 Huang and Castillo 423

hours following injury, and typically demonstratecortical and subcortical white matter restriction,most pronounced in the parasagittal watershedterritories (Fig 5). It should be noted that abnor-malities on diffusion-weighted images can be ex-tremely subtle, with images even appearing nor-mal (19), since areas of restricted diffusion can bemasked by the intrinsically high T2 values of theneonatal brain, which is mostly unmyelinated.Therefore, diffusion-weighted images of the neo-natal brain should always be reviewed in conjunc-tion with their corresponding ADC maps (onwhich true areas of restriction should be apparentas areas of low signal intensity) or with calculatedADC values (19).
T1- and T2-weighted images may appear nor-mal in the first 24 hours (18), but by day 2, T2-weighted images will often demonstrate corticalswelling with loss of differentiation between graymatter and white matter and hyperintensity in thecortex and subcortical white matter, predomi-nantly in the parasagittal watershed zones butoccasionally involving the hemispheres diffusely(4). The deep gray matter structures are typicallyspared in these patients. In the chronic stage,
there is atrophy with cortical thinning and dimin-ished white matter volume, predominantly in theparasagittal watershed zones.
HII in the Preterm NeonateHII is more common in preterm neonates than interm neonates. At least 5% of infants born before32 weeks gestational age and up to 19% of infantsborn before 28 weeks develop cerebral palsy. Fur-thermore, although preterm neonates make up arelatively small proportion of all live births, ap-proximately 50% of cases of cerebral palsy occurin individuals born prematurely (26). The riskfactors for the development of HII in pretermneonates are similar to those seen in term neo-nates, but injury is more likely to occur in prema-ture patients because of both an increased fre-quency of events potentially causing hypoperfu-sion (including respiratory distress syndrome,pneumothorax, patent ductus arteriosus, andneonatal sepsis) and the relatively poor autoregu-latory capacity of the premature brain (10,26).
HII in preterm infants, particularly those ofvery low birth weight, is difficult to diagnose clini-cally early on because signs may be lacking ormistaken to result from developmental immatu-rity. For instance, preterm infants normally have
Figure 5. Partial neonatal HII in a2-day-old term infant who experi-enced seizures shortly after birth.(a, b) Axial T1-weighted (a) andT2-weighted (b) MR images appearessentially normal. (c, d) Diffusion-weighted MR image (c) and corre-sponding ADC map (d) show re-stricted diffusion in the cortex andsubcortical white matter in a para-sagittal watershed distribution.
424 March-April 2008 RG f Volume 28 ● Number 2
TeachingPoint

decreasedmuscletonecomparedwithtermin-fants (11), and transient neurologic abnormalitiesare especially common in preterm infants who donot go on to develop long-term neurologic deficits(26). Therefore, imaging can be particularly use-ful in establishing the diagnosis of HII in preterminfants.
The imaging manifestations of HII in pretermneonates differ from those seen in term neonates,due primarily to the relative immaturity of thepreterm neonatal brain. Despite these differences,the observed patterns of HII in preterm neonatescan still be subdivided based on the severity of the
in preterm neonates manifest predominantly asdamage to the deep gray matter structures andbrainstem. Events of mild to moderate severity inthis population typically manifest as either germi-nal matrix–intraventricular hemorrhages or peri-ventricular white matter damage (also referred toas periventricular leukomalacia [PVL]) (19,27).
Severe AsphyxiaThe injury pattern observed in preterm neonatesfollowing brief but severe hypoxic-ischemic in-sults is similar in several respects to the patterndescribed for term neonates who suffer similarinsults, but there are also characteristic differ-ences (27). Injury to the thalami, basal ganglia,hippocampi, cerebellum, and corticospinal tractscan be seen, with the thalami, anterior vermis,and dorsal brainstem being most frequently in-volved. Although basal ganglia injury is frequentlyencountered in this group, involvement of thesestructures is less severe compared with involve-ment of the thalami, particularly among neonatesborn at less than 32 weeks gestation (27). Wheninvolved, the basal ganglia tend to cavitate andshrink without scarring. In addition, the periro-landic cortex is more likely to be spared in prema-
ture neonates than in term neonates (4,27). Ger-minal matrix hemorrhages and periventricularwhite matter injury may also be seen.
The comparative resistance of the basal gangliato damage in preterm neonates has been attrib-uted in part to their relatively late myelinationcompared with the thalami (27). Pathologic stud-ies have shown that the thalamus and globuspallidus myelinate at 24–25 weeks gestation,whereas the corpus striatum (caudate nucleus andputamen) does not myelinate until 35–36 weeks(28). The areas of most advanced myelination inthe brain generally correspond to the areas ofgreatest metabolic activity. Consequently, theseare the areas that are expected to be most suscep-tible to damage in the setting of oxygen depriva-tion. This hypothesis may also explain the relativesparing of the perirolandic cortex, which also doesnot myelinate until 35–36 weeks (28).
In general, because the likelihood of brain in-jury is high among preterm neonates and the neu-rologic examination is often difficult to interpret,most of these patients undergo cranial US, whichcan easily be performed at the patient’s bedside inthe intensive care unit. US of the brain in pretermneonates with HII may demonstrate increasedechogenicity in the thalami by 48–72 hours fol-lowing an insult but may also be normal, particu-larly in the first 2 days.
MR imaging is generally the next imagingstudy performed after US in preterm neonateswith suspected brain injury. As with asphyxiatedterm neonates, conventional MR imaging per-formed within the 1st day after injury may benormal or show only subtle abnormalities. Diffu-sion abnormalities are usually evident in the thal-ami within 24 hours (Fig 6). After 2 days, T2 pro-longation can be seen in the thalami and basalganglia. By the 3rd day following injury, T1
Figure 6. Severe asphyxia in a prema-ture neonate (34 weeks gestation) who suf-fered an episode of prolonged apnea andsubsequent seizures at 1 week of life. Dif-fusion-weighted MR image (a) and corre-sponding ADC map obtained the followingday (b) show restricted diffusion in theventrolateral thalami (arrows). The T1-and T2-weighted images were normal.
RG f Volume 28 ● Number 2 Huang and Castillo 425
TeachingPoint
hypoxic event. Profound hypoxic-ischemic events

shortening will be seen in the injured areas. Diffu-sion-weighted abnormalities are most apparentaround days 3–5 following insult and subse-quently begin to pseudonormalize (10,19). T2shortening develops in the injured areas at ap-proximately 7 days, and T1 shortening persistsinto the chronic stage.
Mild to Moderate Asphyxia:Intraventricular HemorrhageThe overall prevalence of intraventricular hemor-rhage in preterm neonates weighing less than2000 g is approximately 25%, and in the majorityof cases this bleeding occurs within the first 24hours of life (29,30). Prevalence is inversely re-lated to gestational age and weight at birth; there-fore, infants who are very premature with a verylow birth weight are at highest risk for developingintraventricular hemorrhage. The majority of in-traventricular hemorrhages in preterm neonatesare associated with germinal matrix hemorrhages.The germinal matrix is a zone of cells lining thewalls of the lateral ventricles in fetal life and ulti-mately gives rise to the neurons and glia of thebrain (10,29). It is generally most active during
the latter half of the 1st trimester and throughoutthe 2nd trimester (10). The germinal matrix be-comes less active by the end of the 2nd trimesterand gradually involutes over the 1st half of the3rd trimester. By approximately 34 weeks gesta-tion, the germinal zones have nearly completelyinvoluted, which explains why germinal matrixhemorrhages are infrequent after this time. Thelast portion of the germinal matrix to involute, anarea known as the ganglionic eminence, is locateddeep to the ependyma in the caudothalamicnotch, a groove between the head of the caudatenucleus and the thalamus, and it is here that mostgerminal matrix hemorrhages originate.
The pathogenesis of germinal matrix hemor-rhage is believed to be related to the vascularproperties of the germinal matrix. Germinal ma-trix capillaries are unusual in that they are largerthan normal systemic capillaries but are lined onlywith simple endothelium without the muscular orcollagenous support normally seen in larger ves-sels (29). In addition, pathologic studies havedemonstrated a greater degree of vascularity inthe germinal matrix than in other portions of thebrain (31). Finally, the large number of mito-chondria seen within cells of the capillary walls
Figure 7. Intraventricular hemor-rhage. Coronal transfontanelle cra-nial US images obtained in four dif-ferent preterm neonates show thetypes of intraventricular hemorrhageassociated with prematurity. Ingrade I hemorrhage (a), small sub-ependymal hemorrhages are seen ashyperechoic foci in the region of thecaudothalamic grooves (arrows).There is no intraventricular exten-sion. Grade II hemorrhage (b) isseen in the caudothalamic grooves(arrows) with blood extending intothe lateral ventricles (arrowhead).The ventricles are not enlarged. Ingrade III hemorrhage (c), intraven-tricular extension of hemorrhage isagain seen, in this case involvingboth lateral ventricles (arrowheads)and the third ventricle (arrow).Marked ventriculomegaly is alsonoted. In grade IV hemorrhage (d),there is hemorrhage originating inthe periventricular white matter (ar-row) and extending into the ven-tricles.
426 March-April 2008 RG f Volume 28 ● Number 2

(three to five times more than in systemic capillar-ies) suggests that germinal matrix capillaries havehigh oxidative metabolic requirements and are,therefore, particularly susceptible to changes inoxygen concentration (29). It is believed that hyp-oxia-ischemia initially causes damage to the endo-thelial cells of the germinal matrix capillaries, re-sulting in loss of normal capillary integrity. Witheventual brain reperfusion caused by resuscitationof the patient, hemorrhage ensues.
Germinal matrix hemorrhages have classicallybeen subdivided into four grades, reflecting thelocation of hemorrhage and the presence or ab-sence of ventriculomegaly (Table). Grade I–IIIhemorrhages arise from the germinal matrix, withvariable extension into the lateral ventricles.Grade IV hemorrhages are not true germinal ma-trix hemorrhages, but rather are believed to repre-sent hemorrhagic venous infarcts that subse-quently extend into the ventricular system.Higher-grade hemorrhages correlate with a higherperinatal mortality rate and a higher prevalence oflong-term neurologic sequelae (10). Intraventric-ular hemorrhage in neonates can generally beevaluated adequately with cranial US (Fig 7). MR
imaging is generally necessary only to detect con-comitant injuries in this group, such as periven-tricular white matter injury or deep gray matterinjury.
Cerebellar hemorrhages have also been re-ported at autopsy in up to 25% of preterm infantswith very low birth weight. With the increasinguse of posterior fontanelle US, a number of theseposterior fossa hemorrhages—which were prob-ably underdiagnosed in the past, since they areoften clinically silent—are being seen in preterminfants. It has been hypothesized that these hem-orrhages are in fact germinal matrix hemorrhagesarising from germinal zones known to exist withinthe external granule cell layer of the cerebellarhemispheres and in the subependymal layer of theroof of the fourth ventricle (32).
Cerebellar hemorrhages may be missed at USperformed through the anterior fontanelle but areeasily seen with a posterior fontanelle approach.These hemorrhages are usually lentiform or cres-centic and are located peripherally in the dorsalaspects of the cerebellar hemispheres (Fig 8) (32).
Figure 8. Cerebellar germinal matrix hemorrhage in a preterm neonate born at 24 weeks gestation. (a, b) Coronal(a) and sagittal (b) US images obtained in the 1st week of life demonstrate an area of echogenicity (arrow) in the leftcerebellar hemisphere, a finding that is compatible with hemorrhage. (c) On a coronal US image obtained approxi-mately 2 weeks later, the area of interest is hypoechoic (arrow), a finding that suggests liquefaction of the hemor-rhage.
Grades of Germinal Matrix–Intraventricular Hemorrhage
Grade Description
I Subependymal hemorrhage with no or minimal intraventricular extensionII Hemorrhage extending from the germinal matrix into the ventricles without ventricular enlargementIII Hemorrhage extending from the germinal matrix into the ventricles with ventricular enlargementIV Periventricular parenchymal hemorrhagic infarction (not a true germinal matrix hemorrhage; rather,
thought to be due to hemorrhage within a venous infarction)
RG f Volume 28 ● Number 2 Huang and Castillo 427

Mild to Moderate Asphyxia:Periventricular LeukomalaciaPeriventricular leukomalacia (PVL), also referredto as white matter injury of prematurity, is a com-mon occurrence among premature infants. Theprevalence of injury appears to be inversely re-lated to gestational age at birth. Previously, thepathogenesis of PVL was believed to be relatedto ischemia in watershed zones existing in theperiventricular white matter of immature brains(33). It was postulated that white matter in theimmature fetal brain is supplied by ventriculope-tal arteries penetrating inward from the brain sur-face, making the deep white matter most suscep-tible to decreases in perfusion; as the brain ma-tures in the 3rd trimester, “ventriculofugal”arteries were believed to develop, shifting the wa-tershed zone out toward the cortex. The existenceof ventriculofugal arteries has come into question(34), but a recent postmortem anatomic seriesshowed low cerebral white matter vascularity un-til after 32 weeks gestational age, a finding thatsuggests that relative hypovascularity of theperiventricular white matter does, in fact, play arole in the development of PVL (31).
It is now believed that PVL is probably relatedto the selective vulnerability of cells of oligoden-drocyte lineage to changes of hypoxia-ischemia.Prior to the onset of myelination and during theperiod of highest risk for PVL, the cerebral whitematter is populated predominantly by late oligo-dendrocyte precursors known as preoligodendro-cytes (35). Compared with early oligodendrocyteprecursors and mature oligodendrocytes, preoli-godendrocytes are more susceptible to oxidativeand excitotoxic injuries occurring as a result ofhypoxia (9,36). This theory is supported by theobservation that the declining prevalence of PVLafter approximately 32 weeks gestation coincideswith oligodendrocyte maturation in the periven-tricular white matter (35). In addition, damage to
subplate neurons—cells that play a role in normalfetal thalamocortical development and that beginto regress late in fetal development—may play arole in the development of PVL (9).
PVL is most frequently observed adjacent tothe trigones of the lateral ventricles and adjacentto the foramina of Monro (33,37). Motor andvisual impairment are the most common long-term neurologic sequelae of white matter injury inpremature infants, due to the fact that the motorand visual pathways pass through the most com-monly injured regions of white matter (10). Spas-tic diplegia, in which motor impairment is greaterin the legs than in the arms, is a common neuro-logic sequela of PVL and more commonly devel-ops in preterm infants than in term infants withHII (26).
At histologic analysis, the lesions of PVLevolve in a characteristic pattern. Initially, there isnecrosis, often progressing to cavitation and thedevelopment of porencephalic cysts. Over time,these cysts collapse, eventually resulting in gliosisand significant reduction in white matter volumein the periventricular regions (33,37).
Four stages of PVL have been described at US(38). Initially, there is congestion, which mani-fests as globular areas of increased echogenicity(sometimes referred to as “flares”) in the periven-tricular regions in the first 48 hours. These find-ings are followed by a transient period of relativenormalization, usually by the 2nd–4th weeks oflife. Periventricular cyst development then occursat approximately 3–6 weeks of life (Fig 9). Fi-nally, by 6 months of age, end-stage PVL results,with resolution of cysts and associated ventricularenlargement (38,39).
Although increased periventricular echogenic-ity should raise suspicion for white matter injury,this finding is far from sensitive or predictive,since initial US studies may be normal in neo-nates who go on to develop PVL and, conversely,increased periventricular echogenicity may be
Figure 9. PVL in a preterm infant.(a) Coronal head US image obtained inthe 1st week of life shows increased echo-genicity in the periventricular white matter(arrows). (b) Follow-up US image ob-tained 2 months later shows developmentof cystic changes in these regions and dila-tation of the adjacent lateral ventricles,findings that are consistent with PVL.
428 March-April 2008 RG f Volume 28 ● Number 2

seen in healthy neonates (33). In one study, serialcranial US examinations performed over the first6 weeks of life in premature neonates with verylow birth weight showed that the presence of pro-longed (�7 days) periventricular echogenicityhad a sensitivity of only 26% and a positive pre-dictive value of only 36% for the detection ofwhite matter injury compared with MR imaging(40). Serial US performed during this periodfared considerably better in detecting subsequentcystic change (sensitivity � 75%, specificity �100%). Therefore, the primary role of US is indetecting germinal matrix hemorrhages duringthe immediate postnatal period and cysticchanges of PVL later in perinatal life.
MR imaging generally allows better visualiza-tion of periventricular white matter abnormalitiesat an earlier stage than does US, particularlyamong infants with noncystic areas of echogenic-ity at US (41). At MR imaging, early white matterinjury will manifest as periventricular foci of T1shortening (without corresponding T2 shorten-ing) within larger areas of T2 prolongation (40).These foci are usually evident by 3–4 days, subse-quently giving way to mild T2 shortening at 6–7
days (Fig 10) (10). In contrast, hemorrhage (re-ported to be present in 64% of cases of PVL [41])initially manifests with much lower signal inten-sity on T2-weighted images. It is believed that theabnormalities seen at MR imaging represent reac-tive astrogliosis. Focal mineralization may ac-count for the areas of T1 hyperintensity (22).
Head CT provides little additional informationin the early stages of PVL and should probably beavoided in neonates, given the associated ionizingradiation exposure. However, CT can be useful inconfirming findings of end-stage PVL later in life.End-stage PVL has a characteristic appearance atCT and MR imaging, with reduction in the vol-ume of periventricular white matter and centrasemiovale, ventriculomegaly with dilatation of thetrigones, and an irregular ventricular outline. T2-weighted MR imaging will also demonstrate ab-normal periventricular white matter hyperinten-sity, most frequently in the peritrigonal regions(Fig 11) (37,42). Thinning of the corpus callo-sum, particularly in the posterior body and sple-nium, may also be seen (42).
Figure 11. End-stage PVL in a 9-year-old child who presented with motor andcognitive delay and seizures. The patientwas born at 32 weeks gestational age. Ax-ial fluid-attenuated inversion recoveryMR images demonstrate increased signalintensity and a few tiny cysts in the im-mediate periventricular white matter. Inb, there is enlargement of the atria of thelateral ventricles with a decrease in volumeof the adjacent white matter, and the wallsof the lateral ventricles have a wavy appear-ance.
Figure 10. PVL in a preterm neonate.Axial T1-weighted (a) and T2-weighted(b) MR images obtained on day 4 of lifedemonstrate T1 hypointensity and T2 hy-perintensity in the periventricular whitematter. Note the punctate foci of high sig-nal intensity on the T1-weighted image(arrows in a). These foci should be distin-guished from foci of hemorrhage, whichwould demonstrate greater T2 shorteningon the corresponding T2-weighted image.
RG f Volume 28 ● Number 2 Huang and Castillo 429

HII in PostnatalInfants and Young Children
Hypoxic-ischemic injuries in infants and youngchildren are usually the result of drowning, chok-ing, or nonaccidental trauma (4). Certain differ-ences exist between the patterns of injury ob-served in neonates and those seen in older infants;these differences are probably related to rapidbrain maturation during the perinatal period. Asmyelination nears completion by about 2 years ofage, injuries similar to the pattern seen in adultsbegin to appear.
Severe AsphyxiaSevere insults to infants between 1 and 2 years ofage result in injuries to the corpora striata, lateralgeniculate nuclei, hippocampi, and cerebral cor-tex (particularly the anterior frontal and parieto-occipital cortex), with relative sparing of the thal-ami and perirolandic cortex (13). Injuries occur-ring after the immediate perinatal period butbefore 1 year of age can demonstrate features ofboth birth asphyxia and later infantile asphyxia,with involvement of the basal ganglia (predomi-nantly posteriorly), lateral thalami, and dorsalmidbrain, as well as cortical injury. The reasonsfor the differences between injury patterns seen inneonates and those seen in older infants are notentirely clear. It has been suggested that relativesparing of the thalami in older infants may be dueto redistribution of blood flow from the anteriorcirculation to the posterior circulation followingasphyxia, but this phenomenon would not explainthe relative resistance of the perirolandic cortex inthese patients (13). It is likely that some of the
observed differences are due to physiologic andbiochemical changes that occur with brain matu-ration, which result in different patterns of activ-ity and, thus, different regional energy require-ments (10).
Cranial US ceases to be a practical imagingoption in infants once the anterior fontanelle hasclosed, which occurs as early as 4 months of age(43). Once US is no longer feasible, CT becomesthe initial imaging study of choice. Early CT per-formed within 24 hours of an insult may be nega-tive or may demonstrate only subtle hypoattenua-tion of the deep gray matter structures (13). Sub-sequent CT will demonstrate diffuse basal gangliaabnormalities along with diffuse cerebral edema,manifesting as cortical hypoattenuation, loss ofnormal “gray-white” differentiation, and cisternaland sulcal effacement (13,44,45). There may berelative sparing of the perirolandic regions (13).Hemorrhagic infarctions of the basal ganglia maybe evident by 4–6 days (45). Imaging in thechronic phase will demonstrate diffuse atrophywith sulcal and ventricular enlargement (44,45).
Within the first 24 hours, a small number ofthese patients may demonstrate the “reversalsign,” in which there is reversal in the normal CTattenuation of gray matter and white matter (Fig12a). It has been proposed that this finding is dueto the distention of deep medullary veins second-ary to partial obstruction of venous outflow fromthe elevated intracranial pressure caused by dif-fuse edema (46). The end result is that the cere-bral white matter is of higher attenuation than thecortical gray matter. Another well-known CT signof severe HII is the “white cerebellum sign” (Figs12b, 13a, 13b) (47), which has been described inat least one study as a component of the reversalsign (48) and in which there is diffuse edema andhypoattenuation of the cerebral hemispheres with
Figure 12. Reversal sign in a 4-month-old victim of nonaccidental trauma.(a) Unenhanced CT scan shows diffusecortical swelling and hypoattenuation inthe white matter relative to areas of pre-served cortex, a finding that is referred toas the reversal sign and generally portendsa poor prognosis. A small amount of ex-traaxial hemorrhage adjacent to the leftfrontal lobe is also seen (arrow). (b) Unen-hanced CT scan demonstrates the whitecerebellum sign. The cerebellar hemi-spheres (*) are hyperattenuating relative tothe supratentorial structures, which arehypoattenuating due to edema.
430 March-April 2008 RG f Volume 28 ● Number 2

sparing of the cerebellum and brainstem, result-ing in apparent high attenuation of the cerebel-lum and brainstem relative to the cerebral hemi-spheres. It has been suggested that this finding isdue to the redistribution of blood to the posteriorcirculation that occurs during anoxic events (47).Both the reversal sign and the white cerebellumsign indicate severe injuries and portend a poorneurologic outcome (46–48).
MR imaging is frequently performed in chil-dren with HII. Diffusion-weighted images willusually be abnormal within the first 12–24 hours,initially demonstrating bright signal intensity inthe posterolateral lentiform nuclei (Fig 13c); tha-lamic involvement (when present) will usuallyinvolve the ventrolateral nuclei (4). Over the next48 hours, there is typically significant progressionof involvement to include the remainder of thebasal ganglia and the cortex (4). ConventionalT1- and T2-weighted images obtained in the first24 hours are often normal (13) and may appear
so for up to 2 days (21). By 48 hours, T2-weighted images will usually demonstrate diffusebasal ganglia and cortical signal intensity abnor-mality (Fig 13d), a finding that probably repre-sents edema (4,21). Again, there may be relativesparing of the perirolandic cortex and thalami(13).
Other entities to consider when bilateral basalganglia abnormalities are seen include inborn er-rors of metabolism, hypoglycemia, osmotic myeli-nolysis, hemolytic uremic syndrome, encephalitis,and toxic exposures (carbon monoxide and cya-nide) (49).
Mild to Moderate AsphyxiaAs in term neonates, milder anoxic events in olderinfants will generally result in watershed zone in-juries involving the cortex and subcortical white
Figure 13. Severe HII in a 6-year-old child. (a) Unenhanced CT scanobtained at the level of the basal gan-glia after cardiopulmonary arrestthat lasted 30 minutes is essentiallyunremarkable. (b) On an unen-hanced CT scan obtained just in-ferior to but contemporaneouslywith a, the cerebellum appearsslightly hyperattenuating relative tothe rest of the brain. This finding isanother example of the white cere-bellum sign as an early CT indicatorof HII. (c, d) Diffusion-weighted (c)and T2-weighted (d) MR imagesobtained 4 days later show high sig-nal intensity with corresponding T2abnormalities in the caudate nuclei(white arrows), lentiform nuclei(black arrows), and occipital lobes(* in c).
RG f Volume 28 ● Number 2 Huang and Castillo 431

matter (Fig 14). White matter lesions are morecommon in children under 1 year of age (5).Relative sparing of the periventricular white mat-ter will be seen (42).
HII in Older Children and AdultsAs stated earlier, HII in adults is more often aresult of cardiac arrest or cerebrovascular disease,with secondary hypoxemia. Drowning and as-phyxiation remain common causes of HII in olderchildren. Mild to moderate global ischemic in-sults to the brain usually result in watershed zoneinfarcts. Severe HII in this population primarily
Figure 15. HII in a 53-year-oldman who experienced a prolonged,severe hypotensive episode followingliver transplantation. (a, b) AxialT2-weighted MR images show hy-perintensity in the globi pallidi (ar-rowheads in a) and cerebellum (ar-rows in b). (c, d) Correspondingdiffusion-weighted MR images showassociated high signal intensity in theglobi pallidi (arrowheads in c) andcerebellum (arrows in d).
Figure 14. Mild to moder-ate HII in a 2-year-old childwho suffered a hypoxic-isch-emic event 5 days after under-going a Fontan procedure.(a) Unenhanced head CTscan shows bilateral corticaland subcortical hypoattenua-tion in the parasagittal water-shed regions. (b) Diffusion-weighted MR image obtainedat the same level shows corre-sponding high-signal-intensityareas compatible with water-shed infarcts.
432 March-April 2008 RG f Volume 28 ● Number 2

affects the gray matter structures: the basal gan-glia, thalami, cerebral cortex (in particular thesensorimotor and visual cortices, although in-volvement is often diffuse), cerebellum, and hip-pocampi (50,51). This predominance of graymatter injury is related to the fact that gray mattercontains most of the dendrites where postsynapticglutamate receptors are located and are, there-fore, the sites most susceptible to the effects ofglutamate excitotoxicity. As a result of synapticactivity, gray matter is also more metabolicallyactive than white matter. Although cerebellar in-jury can be seen in neonates, it tends to be morecommon in older patients. The reason for thispredilection is not entirely clear, but it has beensuggested that the relative immaturity of Purkinjecells (which are normally exquisitely sensitive toischemic damage) in neonates somehow protectsthe cerebellar cortex (52).
In older patients, CT is generally the initialimaging study performed when brain injury issuspected. CT findings include diffuse edemawith effacement of the CSF-containing spaces,decreased cortical gray matter attenuation withloss of normal gray-white differentiation, and de-creased bilateral basal ganglia attenuation (50).As in young children, the reversal sign and thewhite cerebellum sign may be seen in adults andindicate severe injury with a poor prognosis (53).
Diffusion-weighted MR imaging is the earliestimaging modality to become positive, usually
within the first few hours after a hypoxic-ischemicevent. During the first 24 hours, diffusion-weighted imaging may demonstrate increasedsignal intensity in the cerebellar hemispheres,basal ganglia, or cerebral cortex (in particular, theperirolandic and occipital cortices) (Fig 15) (51).The thalami, brainstem, or hippocampi may alsobe involved (5,51,54). As in younger patients,conventional T1- and T2-weighted images are of-ten normal or demonstrate only very subtle abnor-malities. In the early subacute period (24 hours–2 weeks), conventional T2-weighted images typi-cally become positive and demonstrate increasedsignal intensity and swelling of the injured graymatter structures, although these findings may besubtle. As mentioned earlier, diffusion-weightedimaging abnormalities usually pseudonormalizeby the end of the 1st week (4,6,10,20). Gray mat-ter signal intensity abnormalities at conventionalMR imaging may persist into the end of the 2ndweek. In the chronic stage, T2-weighted imagesmay demonstrate some residual hyperintensity inthe basal ganglia, and T1-weighted images mayshow cortical necrosis (Fig 16), which is seen asareas of high signal intensity in the cortex (51,54).
Delayed White Matter Injury(Postanoxic Leukoencephalopathy)
Postanoxic leukoencephalopathy is an uncom-mon syndrome of delayed white matter injury,usually occurring weeks after a hypoxic-ischemicevent. This process occurs in approximately2%–3% of patients following a global hypoxicinsult (most commonly in association with carbonmonoxide intoxication) and is characterized by aperiod of relative clinical stability or even im-provement, followed by an acute neurologic de-cline, usually 2–3 weeks after the initial insult.Patients may experience delirium, personalitychanges, intellectual impairment, movement dis-orders, or, rarely, seizures (55–57). Approxi-mately 75% of patients go on to complete ornear-complete recovery over the next 6–12months. In the remaining patients, there may beresidual dementia. Rarely, the condition mayprogress to paresis, a vegetative state, or death(57).
In typical cases of postanoxic leukoencepha-lopathy, conventional and diffusion-weightedMR imaging performed immediately followingthe causative insult fail to demonstrate signifi-cant cerebral white matter abnormalities, but
Figure 16. Cortical necrosis in a35-year-old patient who had experi-enced an ischemic event severalweeks earlier. Axial T1-weightedMR image shows bilateral serpigi-nous high signal intensity in the cor-tex of the occipital lobes (greater onthe left side), a finding that is com-patible with cortical necrosis.
RG f Volume 28 ● Number 2 Huang and Castillo 433

diffusion-weighted imaging performed during theperiod of delayed neurologic decline demon-strates diffuse confluent areas of restricted diffu-sion throughout the cerebral white matter (Fig17) (51,54,55,58–60). Corresponding hyperin-tensity on T2-weighted images is also seen. Al-though classically a delayed process, the leukoen-cephalopathy can also manifest as progressivedeterioration without an intervening lucid period.In these cases, white matter signal intensitychanges can be seen within the 1st week (55). Inyoung children, postanoxic white matter injuryoccurs sooner and can be observed by as early as2 days. Clinical findings of diffuse white matterinjury may not be readily apparent or may bequite subtle in very young children and infants,with abnormal MR imaging findings being theearliest evidence of white matter injury (4).
Clinical improvement appears to be associatedwith a decrease in the extent of signal intensityabnormalities (60), but residual abnormalities canpersist beyond 18 months (61). Surviving patientsmay go on to develop diffuse atrophy at follow-upimaging.
The exact mechanism for delayed white matterinjury following anoxia is not known. It has beensuggested that the findings may represent a pro-cess similar to wallerian degeneration (51). It isalso conceivable that apoptotic cell death mayplay a role in the pathogenesis of this entity.
Role of Proton MR Spec-troscopy in the Evaluation of HII
Proton MR spectroscopy has become a valuabletool in the evaluation of HII, particularly in theperinatal period. Indeed, MR spectroscopy anddiffusion-weighted MR imaging are the mostsensitive imaging modalities for detecting HIIin the acute period (19,62), and MR spectroscopyis perhaps more sensitive to injury and more in-dicative of the severity of injury in the first 24hours after a hypoxic-ischemic episode, whenconventional and diffusion-weighted MR imag-ing may yield false-negative findings or lead tosignificant underestimation of the extent of injury(10,18,19). MR spectroscopy will demonstratesubstantial lactate elevation (appearing as a dou-blet centered at 1.3 ppm at 1.5 T) in the deepgray nuclei, parieto-occipital region, or whitematter of the parasagittal watershed zones by asearly as 2–8 hours (19,62,63). A glutamine-gluta-mate peak may also be detected at 2.3 ppm (62),probably reflecting the release of glutamate thatoccurs in HII (Fig 18).
Two lactate elevations are believed to occurduring the acute to subacute period of HII. Inanimal models, lactate levels increase almost im-mediately following a hypoxic-ischemic insult,probably as a result of hypoxemia and ensuinganaerobic glycolysis, only to fall back nearly tobaseline over the next few hours as a result of re-stored perfusion. Over the following 24–48hours, a second increase takes place that is
Figure 17. Postanoxic leukoencephalopathy in an adult patient who had experienced respiratory arrest 2 weeksearlier. (a, b) Axial T2-weighted (a) and diffusion-weighted (b) MR images show diffuse white matter hyperinten-sity. (c) On the corresponding ADC map, the white matter is hypointense, a finding that indicates restricted diffu-sion.
434 March-April 2008 RG f Volume 28 ● Number 2
TeachingPoint

thought to be the result of a process known as“secondary energy failure,” in which neurons thatsurvived the initial insult develop delayed energydepletion, probably as a result of mitochondrialfailure. This process probably explains in partwhy initial diffusion-weighted imaging leads tounderestimation of injury in the acute setting.Injury due to secondary energy failure will resultin elevated cerebral lactate after 24 hours at MRspectroscopy and carries a grave prognosis (63).In general, the finding of elevated lactate in thefirst few days of life portends a poor neurologicoutcome (3,63).
Premature infants normally have higher lactatepeaks and lower N-acetylaspartate (NAA) peaksthan do term infants, which may make interpreta-tion of the spectra of premature infants difficult.Lactate diminishes and NAA increases as thebrain matures, but trace amounts of lactate maybe evident even in the spectra of healthy term in-fants (63,64). Therefore, it helps to be aware ofan infant’s gestational age at birth when interpret-ing an MR spectroscopic study to avoid a false-positive result (3). The lactate-NAA ratio may bea useful measure when interpreting MR spectro-scopic studies performed in preterm neonates.Penrice et al (63) reported the mean lactate-NAAratio in the thalami of control neonates (gesta-tional age, 29–42 weeks) to be 0.25 (SD � 0.11).Asphyxiated infants (both term and preterm)tended to have lactate-NAA ratios greater than0.4, and infants with severe injuries generally hadlactate-NAA ratios greater than 0.5. Further-
more, lactate-NAA ratios above 95% confidencelimits were associated with death or major impair-ment at 1 year (63).
In addition, some investigators have describeddecreased levels of NAA, centered at 2.0 ppm, inthe spectra of asphyxiated infants imaged sub-acutely, a finding that also correlates with apoorer neurologic outcome (3,65). It should benoted that NAA is usually normal acutely in HIIand does not significantly decline until approxi-mately 48 hours after the acute injury (3,63).
In older children, abnormal spectroscopic find-ings include lactate elevation, glutamine-gluta-mate elevation, and reduced NAA. The finding ofabnormal MR imaging spectra correlates with avery poor outcome (persistent vegetative state ordeath) (21). A normal MR spectroscopic exami-nation combined with normal findings at routineMR imaging generally correlates with a good out-come, although injury cannot be ruled out untilday 3–4 (4).
Imaging Choicesin Evaluating HII
A number of factors must be taken into accountwhen choosing the most appropriate imagingstudy for evaluating suspected HII. These factorsinclude, but are certainly not limited to, patientage, patient condition, and concerns about ioniz-ing radiation exposure. A simplified algorithm for
Figure 18. Neonatal asphyxia in a term neonate. Short-echo-time (30 msec) (a) and long-echo-time (135msec) (b) MR spectroscopic images obtained on day 1 of life with a voxel positioned in the right basal gangliashow a lactate (Lac) doublet centered at 1.3 ppm in a and an inverted lactate doublet in b. There is also el-evated glutamine-glutamate (Glx) in a and low NAA in b. Cho � choline, Cr and Cr2 � creatine resonances(3.0 ppm and 3.9 ppm, respectively).
RG f Volume 28 ● Number 2 Huang and Castillo 435

imaging patients with suspected HII is shown inFigure 19.
Neonates with suspected HII are usually criti-cally ill and hemodynamically unstable, makingpatient transport to fixed scanners often impracti-cal in the acute setting. Therefore, cranial US isthe screening examination of choice for these pa-tients, since it is noninvasive, involves no ionizingradiation exposure, and can be performed at thepatient’s bedside. The major limitations of US areits operator dependence and its relatively low sen-sitivity for injury, particularly over the cerebralconvexities (66). Although US performed in theacute setting is helpful when it demonstrates dis-ease, a negative US study does not rule out injury,and an alternative imaging study is often neces-sary.
We do not routinely advocate the use of CT inthe evaluation of neonatal HII because it involvesionizing radiation exposure. Furthermore, CT isno more sensitive for detecting nonhemorrhagicinjury in neonates than is US, due in part to thenormally high water content of the neonatal brain(66). Therefore, MR imaging is the next imagingstudy of choice after US. Although MR imaging isoften logistically more difficult to perform (due toissues of patient transport, sedation, and monitor-ing), it is more sensitive for the evaluation of HII.MR imaging protocols should include, at a mini-mum, axial T1- and T2-weighted sequences, dif-fusion-weighted sequences, and an ADC map. At
our institution, we use spin-echo T1-weighted(repetition time msec/echo time msec � 600/12)and turbo spin-echo T2-weighted (6860/125)sequences. For diffusion-weighted imaging, weuse a single-shot echoplanar technique with a bvalue of 1000 sec/mm2. The optimal b value fordiffusion-weighted images is controversial andvaries among institutions. Most authors reportusing b values of 700–1000 sec/mm2, althoughsome authors report using b values as high as1500 sec/mm2 (4). If there is a concern for hem-orrhage, we include an axial gradient-echo T2-weighted sequence (705/15, 20° flip angle), whichis more sensitive to the presence of deoxyhemo-globin and methemoglobin than are standardturbo spin-echo T2-weighted sequences. Fluid-attenuated inversion recovery images can be use-ful in evaluating adults and older children but areof limited use in detecting edema in newborns.
If MR imaging performed in the first 24 hoursis negative, a repeat examination performed at2–4 days may help rule out the possibility of de-layed injury, given that MR imaging may occa-sionally produce a false-negative result in theacute period (4). In addition, proton MR spec-troscopy could be performed in the acute stage.Although some institutions routinely perform MRspectroscopy for suspected neonatal brain injury,we reserve this modality for situations in whichdiffusion-weighted imaging findings are normalbut the clinical suspicion for HII remains high. Inthese situations, we perform long-echo-time (135msec) and short-echo-time (30 msec) spectros-
Figure 19. Diagram illustrates a suggested algorithm for the imaging of suspected HII.
436 March-April 2008 RG f Volume 28 ● Number 2

copy with voxels positioned in the basal gangliaand centra semiovale. If subtle abnormalities arenoted at MR imaging performed in the acute set-ting, follow-up imaging performed at the end ofthe 1st week of life may be helpful in defining pro-gression and overall extent of injury (4).
In adults and children who are not candidatesfor cranial US owing to closure of the anteriorfontanelle, unenhanced head CT is the initialscreening test of choice. If the study is positive, noadditional imaging is usually necessary, althoughone might consider performing additional MRimaging to assess the overall extent of injury. Anegative CT study should prompt further evalua-tion with MR imaging because, as mentioned ear-lier, CT is relatively insensitive for detecting in-jury in the acute setting. As in neonates, repeatimaging in the subacute setting in infants andyoung children may be helpful in determining theultimate extent of damage due to delayed tissueinjury.
Currently, MR perfusion imaging does notplay a role in the evaluation of brain injury due toglobal hypoxia-ischemia, although MR perfusionimaging of hypoxia-ischemia has been performedin animal models. In a rat model, Dijkhuizen et al(67) demonstrated luxury perfusion at dynamicgadolinium-enhanced MR perfusion imaging im-mediately following resuscitation from HII, fol-lowed by a state of mild hypoperfusion in corticaland striatal areas that persisted for several hours.By 24 hours, there was hyperemia in the caudatenucleus. Qiao et al (68) demonstrated increasedregional cerebral blood flow in infarcted tissue 24hours following hypoxia-ischemia in 4-week-oldrats but not in 1-week-old rats, possibly reflectingthe poorer ability of the newborn rats to mount acompensatory cerebrovascular response to hypox-ia-ischemia. Although these data are of academicinterest, it remains to be seen whether MR perfu-sion imaging will play a significant clinical role inthe evaluation of HII in the future.
ConclusionsHII can pose a difficult diagnostic problem from aneuroimaging standpoint, especially in newborns.Observed injury patterns are highly variable anddepend on brain maturity, severity and length ofinsult, and type and timing of imaging. Makingthe diagnosis of HII at US, CT, and MR imagingrequires a clear understanding of the various im-aging patterns that can result. By focusing on thespecific regions that are most likely to be injured
due to selective vulnerability, one can avoid false-negative interpretations caused by overlookingsubtle findings in an otherwise normal-appearingbrain. Diffusion-weighted MR imaging and pro-ton MR spectroscopy are the most sensitive imag-ing modalities in the early hours following injury,but diffusion-weighted imaging often leads to un-derestimation of the true extent of injury in veryyoung children. Therefore, delayed imaging inthe subacute phase may be helpful in determiningthe overall extent of injury and long-term progno-sis, particularly in the pediatric population.
References1. Shalak L, Perlman JM. Hypoxic-ischemic brain
injury in the term infant: current concepts. EarlyHum Dev 2004;80:125–141.
2. Vannucci RC, Perlman JM. Interventions for peri-natal hypoxic-ischemic encephalopathy. Pediatrics1997;100:1004–1014.
3. Barkovich AJ, Baranski K, Vigneron D, et al. Pro-ton MR spectroscopy for the evaluation of braininjury in asphyxiated, term neonates. AJNR Am JNeuroradiol 1999;20:1399–1405.
4. Grant PE, Yu D. Acute injury to the immaturebrain with hypoxia with or without hypoperfusion.Radiol Clin North Am 2006;44:63–77, viii.
5. Christophe C, Fonteyne C, Ziereisen F, et al.Value of MR imaging of the brain in children withhypoxic coma. AJNR Am J Neuroradiol 2002;23:716–723.
6. Wijdicks EF, Campeau NG, Miller GM. MR im-aging in comatose survivors of cardiac resuscita-tion. AJNR Am J Neuroradiol 2001;22:1561–1565.
7. Johnston MV, Trescher WM, Ishida A, NakajimaW. Neurobiology of hypoxic-ischemic injury in thedeveloping brain. Pediatr Res 2001;49:735–741.
8. Biagas K. Hypoxic-ischemic brain injury: advance-ments in understanding of mechanisms and poten-tial avenues for therapy. Curr Opin Pediatr 1999;11:223–228.
9. McQuillen PS, Ferriero DM. Selective vulnerabil-ity in the developing central nervous system. Pedi-atr Neurol 2004;30:227–235.
10. Barkovich AJ. Brain and spine injuries in infancyand childhood. In: Barkovich AJ, ed. Pediatricneuroimaging. 4th ed. Philadelphia, Pa: Lippin-cott Williams & Wilkins, 2005; 190–290.
11. Ferriero DM. Neonatal brain injury. N Engl J Med2004;351:1985–1995.
12. Nelson KB. The epidemiology of cerebral palsy interm infants. Ment Retard Dev Disabil Res Rev2002;8:146–150.
13. Barkovich AJ. MR and CT evaluation of profoundneonatal and infantile asphyxia. AJNR Am J Neu-roradiol 1992;13:959–972.
RG f Volume 28 ● Number 2 Huang and Castillo 437

14. Stark JE, Seibert JJ. Cerebral artery Doppler ultra-sonography for prediction of outcome after perina-tal asphyxia. J Ultrasound Med 1994;13:595–600.
15. Babcock DS, Ball W Jr. Postasphyxial encepha-lopathy in full-term infants: US diagnosis. Radiol-ogy 1983;148:417–423.
16. Hertzberg BS, Pasto ME, Needleman L, KurtzAB, Rifkin MD. Postasphyxial encephalopathy interm infants: sonographic demonstration of in-creased echogenicity of the thalamus and basalganglia. J Ultrasound Med 1987;6:197–202.
17. Connolly B, Kelehan P, O’Brien N, et al. Theechogenic thalamus in hypoxic ischaemic en-cephalopathy. Pediatr Radiol 1994;24:268–271.
18. Robertson RL, Ben-Sira L, Barnes PD, et al. MRline-scan diffusion-weighted imaging of term neo-nates with perinatal brain ischemia. AJNR Am JNeuroradiol 1999;20:1658–1660.
19. Barkovich AJ, Westmark K, Partridge C, Sola A,Ferriero DM. Perinatal asphyxia: MR findings inthe first 10 days. AJNR Am J Neuroradiol 1995;16:427–438.
20. Forbes KP, Pipe JG, Bird R. Neonatal hypoxic-ischemic encephalopathy: detection with diffu-sion-weighted MR imaging. AJNR Am J Neurora-diol 2000;21:1490–1496.
21. Dubowitz DJ, Bluml S, Arcinue E, Dietrich RB.MR of hypoxic encephalopathy in children afternear drowning: correlation with quantitative pro-ton MR spectroscopy and clinical outcome. AJNRAm J Neuroradiol 1998;19:1617–1627.
22. Felderhoff-Mueser U, Rutherford MA, SquierWV, et al. Relationship between MR imaging andhistopathologic findings of the brain in extremelysick preterm infants. AJNR Am J Neuroradiol1999;20:1349–1357.
23. Dietrich RB. Anoxic ischemic injury in children.In: Orrison WW Jr, ed. Neuroimaging. Philadel-phia, Pa: Saunders, 2000; 1685–1703.
24. Gire C, Girard N, Nicaise C, Einaudi MA, Mont-fort MF, Dejode JM. Clinical features and neuro-radiological findings of mitochondrial pathology insix neonates. Childs Nerv Syst 2002;18:621–628.
25. Ashwal S, Majcher JS, Vain N, Longo LD. Pat-terns of fetal lamb regional cerebral blood flowduring and after prolonged hypoxia. Pediatr Res1980;14:1104–1110.
26. O’Shea TM. Cerebral palsy in very preterm in-fants: new epidemiological insights. Ment RetardDev Disabil Res Rev 2002;8:135–145.
27. Barkovich AJ, Sargent SK. Profound asphyxia inthe premature infant: imaging findings. AJNRAm J Neuroradiol 1995;16:1837–1846.
28. Hasegawa M, Houdou S, Mito T, Takashima S,Asanuma K, Ohno T. Development of myelina-tion in the human fetal and infant cerebrum: a my-elin basic protein immunohistochemical study.Brain Dev 1992;14:1–6.
29. Volpe JJ. Intraventricular hemorrhage in the pre-mature infant: current concepts—I. Ann Neurol1989;25:3–11.
30. Paneth N, Pinto-Martin J, Gardiner J, et al. Inci-dence and timing of germinal matrix/intraventricu-lar hemorrhage in low birth weight infants. Am JEpidemiol 1993;137:1167–1176.
31. Ballabh P, Braun A, Nedergaard M. Anatomicanalysis of blood vessels in germinal matrix, cere-bral cortex, and white matter in developing in-fants. Pediatr Res 2004;56:117–124.
32. Merrill JD, Piecuch RE, Fell SC, Barkovich AJ,Goldstein RB. A new pattern of cerebellar hemor-rhages in preterm infants. Pediatrics 1998;102:E62.
33. Flodmark O, Roland EH, Hill A, Whitfield MF.Periventricular leukomalacia: radiologic diagnosis.Radiology 1987;162:119–124.
34. Nelson MD Jr, Gonzalez-Gomez I, Gilles FH.The search for human telencephalic ventriculofu-gal arteries. AJNR Am J Neuroradiol 1991;12:215–222.
35. Back SA, Luo NL, Borenstein NS, Levine JM,Volpe JJ, Kinney HC. Late oligodendrocyte pro-genitors coincide with the developmental windowof vulnerability for human perinatal white matterinjury. J Neurosci 2001;21:1302–1312.
36. Back SA, Han BH, Luo NL, et al. Selective vul-nerability of late oligodendrocyte progenitors tohypoxia-ischemia. J Neurosci 2002;22:455–463.
37. Flodmark O, Lupton B, Li D, et al. MR imagingof periventricular leukomalacia in childhood. AJRAm J Roentgenol 1989;152:583–590.
38. Dubowitz LM, Bydder GM, Mushin J. Develop-mental sequence of periventricular leukomalacia:correlation of US, clinical, and nuclear magneticresonance functions. Arch Dis Child 1985;60:349–355.
39. Bowerman RA, Donn SM, DiPietro MA,D’Amato CJ, Hicks SP. Periventricular leukoma-lacia in the pre-term newborn infant: sonographicand clinical features. Radiology 1984;151:383–388.
40. Inder TE, Anderson NJ, Spencer C, Wells S,Volpe JJ. White matter injury in the prematureinfant: a comparison between serial cranial sono-graphic and MR findings at term. AJNR Am JNeuroradiol 2003;24:805–809.
41. Sie LT, van der Knapp MS, van Wezel-Meijler G,Taets van Amerongen AH, Lafeber HN, Valk J.
438 March-April 2008 RG f Volume 28 ● Number 2

Early MR features of hypoxic-ischemic brain in-jury in neonates with periventricular densities onsonograms. AJNR Am J Neuroradiol 2000;21:852–861.
42. Barkovich AJ, Truwit CL. Brain damage fromperinatal asphyxia: correlation of MR findingswith gestational age. AJNR Am J Neuroradiol1990;11:1087–1096.
43. Aisenson MR. Closing of the anterior fontanelle.Pediatrics 1950;6:223–226.
44. Taylor SB, Quencer RM, Holzman BH, NaidichTP. Central nervous system anoxic-ischemic in-sult in children due to near-drowning. Radiology1985;156:641–646.
45. Fitch SJ, Gerald B, Magill HL, Tonkin ILD. Cen-tral nervous system hypoxia in children due tonear-drowning. Radiology 1985;156:647–650.
46. Bird CR, Drayer BP, Gilles FH. Pathophysiologyof “reverse” edema in global cerebral ischemia.AJNR Am J Neuroradiol 1989;10:95–98.
47. Harwood-Nash DC. Abuse to the pediatric centralnervous system. AJNR Am J Neuroradiol 1992;13:569–575.
48. Han BK, Towbin RB, De Courten-Myers G,McLaurin R, Ball WS Jr. Reversal sign on CT:effect of anoxic/ischemic cerebral injury in chil-dren. AJNR Am J Neuroradiol 1989;10:1191–1198.
49. Ho VB, Fitz CR, Chuang SH, Geyer CA. Bilateralbasal ganglia lesions: pediatric differential consid-erations. RadioGraphics 1993;13:269–292.
50. Kjos BO, Brant-Zawadzki M, Young RG. EarlyCT findings of global central nervous system hy-poperfusion. AJR Am J Roentgenol 1983;141:1227–1232.
51. Arbelaez A, Castillo M, Mukherji S. Diffusion-weighted MR imaging of global cerebral anoxia.AJNR Am J Neuroradiol 1999;20:999–1007.
52. Castillo M. Selective vulnerability and the cerebel-lum in neonates. AJNR Am J Neuroradiol 2007;28:20–21.
53. Vergote G, Vandeperre H, DeMan R. The rever-sal sign. Neuroradiology 1992;34:215–216.
54. Takahashi S, Higano S, Ishii K, et al. Hypoxicbrain damage: cortical laminar necrosis and de-layed changes in white matter at sequential MRimaging. Radiology 1993;189:449–456.
55. Roychowdhury S, Maldjian JA, Galetta SL, Gross-man RI. Postanoxic encephalopathy: diffusion MRfindings. J Comput Assist Tomogr 1998;22:992–994.
56. Bass E. Cardiopulmonary arrest: pathophysiologyand neurologic complications. Ann Intern Med1985;103:920–927.
57. Moore DP, Jefferson JW. Delayed postanoxic leu-koencephalopathy. In: Moore DP, Jefferson JW,eds. Handbook of medical psychiatry. 2nd ed.Philadelphia, Pa: Elsevier Mosby, 2004; 372–373.
58. Kim JH, Chang KH, Song IC, et al. Delayed en-cephalopathy of acute carbon monoxide intoxica-tion: diffusivity of cerebral white matter lesions.AJNR Am J Neuroradiol 2003;24:1592–1597.
59. Custodio CM, Basford JR. Delayed postanoxicencephalopathy: a case report and literature re-view. Arch Phys Med Rehabil 2004;85:502–505.
60. Chang KH, Han MH, Kim HS, Wie BA, HanMC. Delayed encephalopathy after acute carbonmonoxide intoxication: MR imaging features anddistribution of cerebral white matter lesions. Radi-ology 1992;184:117–122.
61. Inagaki T, Ishino H, Seno H, Umegae N, AoyamaT. A long-term follow-up study of serial magneticresonance images in patients with delayed en-cephalopathy after acute carbon monoxide poison-ing. Psychiatry Clin Neurosci 1997;51:421–423.
62. Hanrahan JD, Sargentoni J, Azzopardi D, et al.Cerebral metabolism within 18 hours of birth as-phyxia: a proton magnetic resonance spectroscopystudy. Pediatr Res 1996;39:584–590.
63. Penrice J, Cady EB, Lorek A, et al. Proton mag-netic resonance spectroscopy of the brain in nor-mal preterm and term infants, and early changesafter perinatal hypoxia-ischemia. Pediatr Res1996;40:6–14.
64. Leth H, Toft PB, Pryds O, Peitersen B, Lou HC,Henriksen O. Brain lactate in preterm and growth-retarded neonates. Acta Paediatr 1995;84:495–499.
65. Groenendaal F, Veenhoven RH, van der Grond J,Jansen GH, Witkamp TD, De Vries LS. Cerebrallactate and N-acetyl-aspartate/choline ratios inasphyxiated full-term neonates demonstrated invivo using proton magnetic resonance spectros-copy. Pediatr Res 1994;35:148–151.
66. Barkovich AJ. The encephalopathic neonate:choosing the proper imaging technique. AJNRAm J Neuroradiol 1997;18:1816–1820.
67. Dijkhuizen RM, Knollema S, van der Worp HB,et al. Dynamics of cerebral tissue injury and perfu-sion after temporary hypoxia-ischemia in the rat:evidence for region-specific sensitivity and delayeddamage. Stroke 1998;29:695–704.
68. Qiao M, Latta P, Foniok T, et al. Cerebral bloodflow response to a hypoxic-ischemic insult differsin neonatal and juvenile rats. MAGMA 2004;17:117–124.
RG f Volume 28 ● Number 2 Huang and Castillo 439
This article meets the criteria for 1.0 credit hour in category 1 of the AMA Physician’s Recognition Award. To obtaincredit, see accompanying test at http://www.rsna.org/education/rg_cme.html.

RG Volume 28 • Volume 1 • March-April 2008 Huang and Castillo
Hypoxic-Ischemic Brain Injury: Imaging Findings from Birth to Adulthood
Benjamin Y. Huang, MD, MPH and Mauricio Castillo, MD
Page 418 Imaging findings in HII are highly variable and depend on a number of factors, including brain maturity, severity and duration of insult, and type and timing of imaging studies. Page 422 In general, conventional T1- and T2-weighted images are most diagnostically useful at the end of the 1st week, when abnormalities at diffusion-weighted imaging have pseudonormalized (Fig 3). Page 424 Abnormalities on diffusion-weighted images can be extremely subtle, with images even appearing normal (19), since areas of restricted diffusion can be masked by the intrinsically high T2 values of the neonatal brain, which is mostly unmyelinated. Therefore, diffusion-weighted images of the neonatal brain should always be reviewed in conjunction with their corresponding ADC maps (on which true areas of restriction should be apparent as areas of low signal intensity) or with calculated ADC values (19). Page 425 Profound hypoxic-ischemic events in preterm neonates manifest predominantly as damage to the deep gray matter structures and brainstem. Events of mild to moderate severity in this population typically manifest as either germinal matrix–intraventricular hemorrhages or periventricular white matter damage (also referred to as periventricular leukomalacia [PVL]) (19,27). Page 434 MR spectroscopy and diffusion-weighted MR imaging are the most sensitive imaging modalities for detecting HII in the acute period (19,62).
RadioGraphics 2008; 28:417–439 ● Published online 10.1148/rg.282075066 ● Content Codes:

RadioGraphics 2008 This is your reprint order form or pro forma invoice
(Please keep a copy of this document for your records.)
Author Name _______________________________________________________________________________________________ Title of Article _______________________________________________________________________________________________ Issue of Journal_______________________________ Reprint # _____________ Publication Date ________________ Number of Pages_______________________________ KB # _____________ Symbol RadioGraphics Color in Article? Yes / No (Please Circle) Please include the journal name and reprint number or manuscript number on your purchase order or other correspondence. Order and Shipping Information Reprint Costs (Please see page 2 of 2 for reprint costs/fees.) ________ Number of reprints ordered $_________ ________ Number of color reprints ordered $_________ ________ Number of covers ordered $_________ Subtotal $_________ Taxes $_________ (Add appropriate sales tax for Virginia, Maryland, Pennsylvania, and the District of Columbia or Canadian GST to the reprints if your order is to be shipped to these locations.) First address included, add $32 for each additional shipping address $_________
TOTAL $_________
Shipping Address (cannot ship to a P.O. Box) Please Print Clearly Name ___________________________________________ Institution _________________________________________ Street ___________________________________________ City ____________________ State _____ Zip ___________ Country ___________________________________________ Quantity___________________ Fax ___________________ Phone: Day _________________ Evening _______________ E-mail Address _____________________________________ Additional Shipping Address* (cannot ship to a P.O. Box) Name ___________________________________________ Institution _________________________________________ Street ___________________________________________ City ________________ State ______ Zip ___________
Country _________________________________________ Quantity __________________ Fax __________________ Phone: Day ________________ Evening ______________ E-mail Address ____________________________________ * Add $32 for each additional shipping address
Payment and Credit Card Details Enclosed: Personal Check ___________ Credit Card Payment Details _________ Checks must be paid in U.S. dollars and drawn on a U.S. Bank. Credit Card: __ VISA __ Am. Exp. __ MasterCard Card Number __________________________________ Expiration Date_________________________________ Signature: _____________________________________ Please send your order form and prepayment made payable to: Cadmus Reprints P.O. Box 751903 Charlotte, NC 28275-1903 Note: Do not send express packages to this location, PO Box.
FEIN #:541274108
Invoice or Credit Card Information Invoice Address Please Print Clearly Please complete Invoice address as it appears on credit card statement Name ____________________________________________ Institution ________________________________________ Department _______________________________________ Street ____________________________________________ City ________________________ State _____ Zip _______ Country ___________________________________________ Phone _____________________ Fax _________________ E-mail Address _____________________________________ Cadmus will process credit cards and Cadmus Journal
Services will appear on the credit card statement. If you don’t mail your order form, you may fax it to 410-820-9765 with
your credit card information. Signature __________________________________________ Date _______________________________________ Signature is required. By signing this form, the author agrees to accept the responsibility for the payment of reprints and/or all charges described in this document.
Reprint order forms and purchase orders or prepayments must be received 72 hours after receipt of form either by mail or by fax at 410-820-9765. It is the policy of Cadmus Reprints to issue one invoice per order.
Please print clearly.
Page 1 of 2 RB-9/26/07

RadioGraphics 2008 Black and White Reprint Prices
Domestic (USA only) # of
Pages 50 100 200 300 400 500
1-4 $221 $233 $268 $285 $303 $323 5-8 $355 $382 $432 $466 $510 $544 9-12 $466 $513 $595 $652 $714 $775
13-16 $576 $640 $749 $830 $912 $995 17-20 $694 $775 $906 $1,017 $1,117 $1,22021-24 $809 $906 $1,071 $1,200 $1,321 $1,47125-28 $928 $1,041 $1,242 $1,390 $1,544 $1,68829-32 $1,042 $1,178 $1,403 $1,568 $1,751 $1,924
Covers $97 $118 $215 $323 $442 $555
International (includes Canada and Mexico) # of
Pages 50 100 200 300 400 500
1-4 $272 $283 $340 $397 $446 $506 5-8 $428 $455 $576 $675 $784 $884 9-12 $580 $626 $805 $964 $1,115 $1,278
13-16 $724 $786 $1,023 $1,232 $1,445 $1,65217-20 $878 $958 $1,246 $1,520 $1,774 $2,03021-24 $1,022 $1,119 $1,474 $1,795 $2,108 $2,42625-28 $1,176 $1,291 $1,700 $2,070 $2,450 $2,81329-32 $1,316 $1,452 $1,936 $2,355 $2,784 $3,209
Covers $156 $176 $335 $525 $716 $905 Minimum order is 50 copies. For orders larger than 500 copies, please consult Cadmus Reprints at 800-407-9190. Reprint Cover Cover prices are listed above. The cover will include the publication title, article title, and author name in black. Shipping Shipping costs are included in the reprint prices. Domestic orders are shipped via UPS Ground service. Foreign orders are shipped via a proof of delivery air service. Multiple Shipments Orders can be shipped to more than one location. Please be aware that it will cost $32 for each additional location. Delivery Your order will be shipped within 2 weeks of the journal print date. Allow extra time for delivery.
Color Reprint Prices
Domestic (USA only) # of
Pages 50 100 200 300 400 500
1-4 $223 $239 $352 $473 $597 $719 5-8 $349 $401 $601 $849 $1,099 $1,3499-12 $486 $517 $852 $1,232 $1,609 $1,992
13-16 $615 $651 $1,105 $1,609 $2,117 $2,62417-20 $759 $787 $1,357 $1,997 $2,626 $3,26021-24 $897 $924 $1,611 $2,376 $3,135 $3,90525-28 $1,033 $1,071 $1,873 $2,757 $3,650 $4,53629-32 $1,175 $1,208 $2,122 $3,138 $4,162 $5,180
Covers $97 $118 $215 $323 $442 $555
International (includes Canada and Mexico)) # of
Pages 50 100 200 300 400 500
1-4 $278 $290 $424 $586 $741 $904 5-8 $429 $472 $746 $1,058 $1,374 $1,6909-12 $604 $629 $1,061 $1,545 $2,011 $2,494
13-16 $766 $797 $1,378 $2,013 $2,647 $3,28017-20 $945 $972 $1,698 $2,499 $3,282 $4,06921-24 $1,110 $1,139 $2,015 $2,970 $3,921 $4,87325-28 $1,290 $1,321 $2,333 $3,437 $4,556 $5,66129-32 $1,455 $1,482 $2,652 $3,924 $5,193 $6,462
Covers $156 $176 $335 $525 $716 $905 Tax Due Residents of Virginia, Maryland, Pennsylvania, and the District of Columbia are required to add the appropriate sales tax to each reprint order. For orders shipped to Canada, please add 7% Canadian GST unless exemption is claimed. Ordering Reprint order forms and purchase order or prepayment is required to process your order. Please reference journal name and reprint number or manuscript number on any correspondence. You may use the reverse side of this form as a proforma invoice. Please return your order form and prepayment to: Cadmus Reprints P.O. Box 751903 Charlotte, NC 28275-1903 Note: Do not send express packages to this location, PO Box. FEIN #:541274108 Please direct all inquiries to:
Rose A. Baynard 800-407-9190 (toll free number) 410-819-3966 (direct number) 410-820-9765 (FAX number)
[email protected] (e-mail)
Reprint Order Forms and purchase order or prepayments must be received 72 hours after receipt of form.
Page 2 of 2