Embed Size (px)
Citation preview

HỒI SỨC NÃO SAU NGƯNG TIM
PGS.TS Cao Phi Phong
Cập nhật 2017

Câu hỏi thảo luận
1. Hội chứng não sau ngưng tim: cơ chế sinh lý bệnh
2. Hạ nhiệt độ bảo vệ chống lại các tổn thương thiếu máu như thế
nào?
3. Nêu chỉ định và chống chỉ định trong điều trị hạ nhiệt độ sau
ngưng tim
4. Khuyến cáo AHA 2010 và nghiên cứu lâm sàng ấn bản 2013 so
với khuyến cáo năm 2005 về đích nhiệt độ điều trị. (What is the
status of targeted temperature management (TTM)?)
5. Thực hành: nếu đoán trước dự hậu xấu, xác định tiêu chuẩn
thần kinh cho phép rút lui chăm sóc bn hôn mê sau ngưng tim
Hội chứng não sau ngưng tim (Post-cardiac arrest syndrome)

Bệnh sử:
BN nam 47 tuổi nhập cấp cứu vì đau ngực trong
3 ngày.Tiền sử: tăng huyết áp, hút thuốc lá
ECG: LVH (left ventricular hypertrophy.)
Cardiac markers: âm tính
CXR: bình thường

Khám
BN không theo dõi monitor
Mạch không bắt được, không đáp ứng
Không xác định thời gian ngưng tim
(Cardiac arrest when initial rhythm pulseless
VT or Vfib ?)

Các bước tiếp theo:
Xoa bóp tim ngoài lồng ngực ?
BN ROSC, hôn mê
Đặt nội khí quản ?
Đặt đường truyền TM ?
Điều trị hạ nhiệt ?

1. Hầu hết ngưng tim xảy ra người lớn,
2. Tỷ lệ sống sót cao nhất cho tất cả mọi lứa tuổi:
ngưng tim do rung thất hay nhanh thất không có mạch,
(arrest and a rhythm of VF or pulseless ventricular
tachycardia).
3. Hồi sức tim mạch đầu tiên là ấn ngực và phá
rung sớm (critical initial elements of CPR are chest
compressions and early defibrillation)
Giới thiệu

Thay đổi C-A-B
1. Ấn ngực thực hiện trước tiên
2. Thông khí thực hiện sau hoàn thành 30
ép ngực trong 18 giây.

1. Coi trọng và đưa động tác ép ngực
(Compressions) lên trên,
2. Trước khi thực hiện kiểm tra đường thở
(Airway) và hô hấp (Breathing).
Như vậy, thao tác mới được ghi trong
Guideline 2010 của AHA sẽ là C-A-B.
Theo Hiệp hội Tim Mạch hoa Kỳ (AHA), trong tài liệu 2010
American Heart Association Guidelines for Cardiopulmonary
Resuscitation and Emergency Cardiovascular Care, năm 2010,

AHA, thao tác ép ngực nên được bắt đầu
ngay lập tức.
Oxy sẽ cần phải có trong phổi và mạch
máu trong vòng vài phút đầu tiên.
Trước đây, bắt đầu với "A" (đường thở) thay
vì "C" (ép ngực) gây ra sự chậm trễ
(không cần thiết mất khoảng 30 giây quí giá)

1. Circulation(giúp máu lưu thông): ấn ngực, ấn hai
lần/giây hoặc 100 lần/phút.
- Sau 30 lần ấn ngực, ngữa đầu nâng cằm bn để thổi hơi.
- Bịt mũi nạn nhân, thổi 1 hơi trong 1 giây.
- Mỗi chu kỳ 30 lần ấn ngực và hai lần thổi hơi
2. Airway( thông đường thở): Mở đường thở bằng thủ
thuật ngửa đầu nâng cằm.
- Nếu nạn nhân không thở thực hiện ngay giúp thở
miệng-miệng hoặc miệng-mũi.
3. Breathing(thở): giúp thở miệng mũi, thực hiện ép
ngực.

Các hướng dẫn mới lần này cũng đề nghị trong
CPR, cứu hộ viên nên tăng tốc độ của ép ngực ít
nhất 100 lần một phút. Ngoài ra, ép phải sâu hơn
vào ngực, đến độ sâu ít nhất là 2 inch(# 5cm) ở
người lớn và 1,5 inch(# 4cm) ở trẻ.
Người thực hiện hô hấp nhân tạo cũng nên tránh tì
đè lên ngực bệnh nhân để nó có thể trở về vị trí bắt
đầu, và ép ngực nên được tiếp tục càng lâu càng
tốt mà không cần áp dụng tỉ lệ 5:1.



RL
Dịch tễ học ngưng tim
Ngưng tim ngoài bệnh viện • 64% trường hợp
• 2 - 9% sống sót ra viện
• 3-7% người sống sót có chức năng thần kinh trở lại bình thường
Ngưng tim trong bệnh viện • 36 % trường hợp
• 18% sống sót ra viện
ILCOR 2008 Circulation 2008; 118:2452-83
Hàng năm 350.000 ca ngưng tim ở Mỹ

• Chết do ngưng tim đột ngột
(Sudden Cardiac Death)
– Ước tính ở Mỹ số ca SCD /năm là 300.000
– Tần suất trên thế giới: 35-125/100.000 người, 25%
dưới 65 tuổi • Cobb JAMA 2002
• de Vreede-Swagemakers JACC 1997
– Nếu ROSC và nhập viện, trung bình sống sót và
xuất viện ở Mỹ 7.9% • Lloyd-Jones Circulation 2009
– Dự hậu tốt bn nhập viện 11-48%, phần lớn bn chết
và tổn thương thần kinh nặng vĩnh viễn • Becker Ann Emer Med 1993
Return of spontaneous circulation (ROSC): Tuần hoàn trở về bình thường
Phần lớn CPR thất bại:
Thiếu oxy (Anoxia)
Tổn thương tái tưới máu(Reperfusion injury)
Tổn thương thần kinh(Neurologic injury)
Khí đạo/ thở (Airway/Breathing)
Tuần hoàn(Circulation)
Biến chứng khác

• Refractory dysrhythmias (10%)
• Low cardiac output states (30%)
• Post-resuscitation Encephalopathy (40%)
Tại sao bn ROSC của chúng ta chết ?
(why do our ROSC patients die?)

Nguyên nhân nào gây chết…?
Cause of Death in
OHCA
HIE
Cardiac
MOSF
Cause of death in IHCA
HIE
Cardiac
MOSF
Laver. Intensive Care Med 2004;30:2126
68%
9%
23% 51%
26%
23%
hypoxic-ischemic encephalopathy=HIE Multi-Organ System Failure=MOSF
Nội viện Ngoại viện

1. Chỉ có 10% bn ngưng tim đến bệnh viện
còn sống sót trở về nhà
2. 60% người sống sót sau ngưng tim phục
hồi ý thức
3. 1/3 mất nhận thức không hồi phục
Tại sao chúng ta cần phải cải thiện CPR ?

POST-CARDIAC ARREST SYNDROME
Hội chứng sau ngưng tim ?

Hội chứng sau ngưng tim
1. Tổn thương do thiếu oxy não
2. Rối loạn chức năng cơ tim liên hệ ngưng tim
- Giảm động toàn bộ, tăng áp suất cuối tâm trương
thất trái(LVEDP)
3. Thiếu máu hệ thống/đáp ứng tái tưới máu
- viêm nhiễm hệ thống, hoạt hóa dòng thác đông máu,
rối loạn điều hòa vận mạch, nguy cơ nhiễm trùng
Sau ngưng tim
Hậu quả về thần kinh
80% bn sau ngưng tim vẫn còn hôn mê
trên 1giờ sau hồi sức
dưới 50% có hồi phục thần kinh tốt
(clinical performance catergory 1 or 2)

Sinh lý bệnh
Trong thời gian ngưng tim, kết quả thiếu sót thần
kinh do:
+ giảm oxy não do tụt huyết áp, mất tưới máu
+ hypoxic não gây phù não và mất dẫn truyền thần kinh
+ tái tưới máu có thể gia tăng phù não, khởi đầu dòng
thác phá hủy hóa học và thay đổi đáp ứng viêm nhiễm
gây tổn thương mô
+ kết quả ảnh hưởng chức năng thần kinh sau hồi sức
tim mạch thành công
Sinh lý bệnh tổn thương do thiếu oxy
Liệt co mạch khởi đầu sự sung huyết
Kéo dài giảm tưới máu trong ngưng tim/CPR
Sau ROSC tổn thương tái tưới máu và tái
thêm oxy vào
dự trữ oxy trong não mất trong vài giây
dự trữ glucose/ATP mất trong 5 phút
đáp ứng viêm nhiễm, hoạt hóa nội mô, thâm nhiễm leukocyte
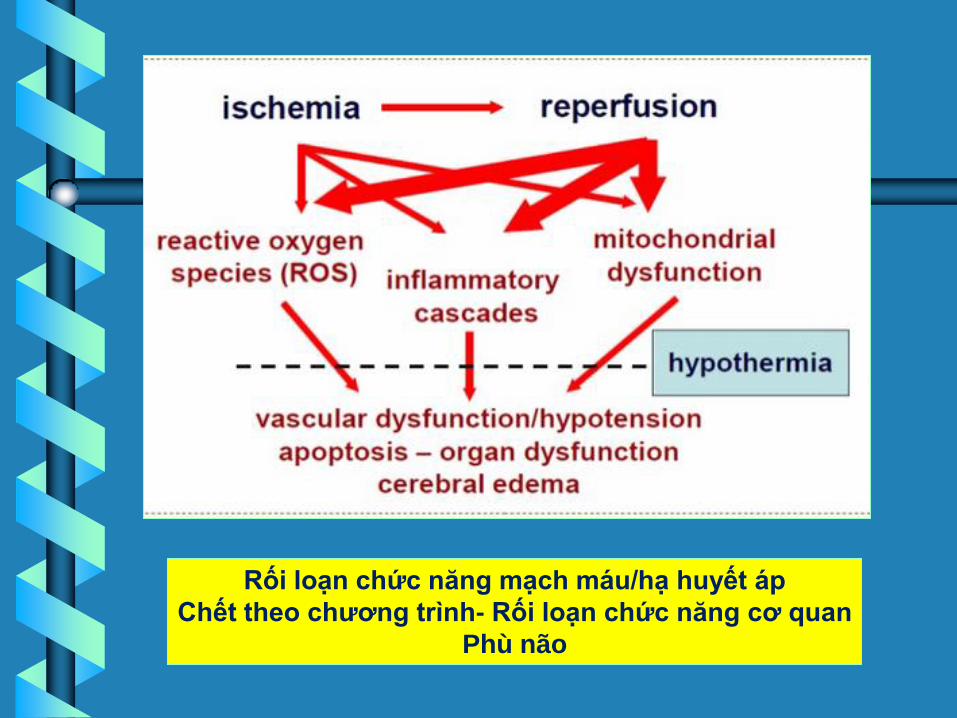
Rối loạn chức năng mạch máu/hạ huyết áp
Chết theo chương trình- Rối loạn chức năng cơ quan
Phù não

Mechanism of
anoxic-ischemic
injury to the brain

Reactive oxygen species (ROS): dạng oxygen phản ứng
- ROS được thành lập như dạng sản phẩm phụ tự nhiên trong biến
dưỡng bình thường của oxygen và có vai trò quan trọng tín hiệu tế
bào và cân bằng nội môi.
- Tuy nhiên trong môi trường stress(thí dụ tia cực tím hay tiếp xúc
nóng, ROS có thể gia tăng, làm tổn thương cấu trúc tế bào. Sự tích
lũy được biết như oxydative stress (sự suy yếu tế bào do chưa quá
nhiều nguyên tử oxy)
- ROS có thể tạo ra bởi nguồn ngoại sinh như ionizing radiation
Sự thành lập gốc tự do, tổn thương oxi hóa (oxidative)
Mất hàng rào máu não
Mất transmembrane chemical gradients
Phóng thích glutamate, tăng Ca++ nội bào, excitotoxic
chết tế bào
Làm trầm trọng hơn do phù não, mất tự điều hòa, giảm
huyết áp và thiếu oxy

Cơ chế tổn thương não do ngưng
tuần hoàn
• Tổn thương nguyên phát:
– “suy năng lượng (Energy failure)” do thiếu ATP
• Tổn thương thứ phát:
– Mất gradients điện giải qua tế bào
• Ca+, Na+, Cl- vào, K+ thoát ra tế bào
• Nước theo Na+ vào tế bào gây cytotoxic edema
– Lipid peroxidases tổn thương màng tế bào
– Phóng thích Neurotransmitter gây excitotoxicity
– Hoạt hóa apoptotic pathways
– Microvascular thrombosis
– Tổn thương Reperfusion
6-72h

• Tổn thương thứ phát khác
- Cơn động kinh không kiểm soát
- Hypotension, hypoperfusion – Postresuscitation syndrome
– ICP crisis
– Autoregulatory failure
- Sốt
- Tái ngưng tim
- Thiếu oxy
- Rối loạn biến dưỡng glucose
Neurology 2008;72:744

• “không tuần hoàn (No flow)” ảnh hưởng phần lớn các vùng hoạt động của não
– Cortex
– Basal ganglia
– Cerebellum
• “tuần hoàn kém (Low flow”) ảnh hưởng vùng giáp ranh giữa các mạch máu (watershed areas )
Cardiac arrest associated brain injury “CAABI”


Hạ nhiệt bảo vệ tổn thương thiếu máu như thế nào?

Điều trị hypothermia hồi phục chức năng thần
kinh trong bệnh nhân nguy cơ cao sau ngưng tim

Cơ chế
ischemia
glutamate release
oxygen-free radicals
calcium shifts
mitochondrial dysfunction
reperfusion
excitotoxicity
inflammatory cascades
cell death
blood brain barrier disruption & cerebral edema
hypothermia
lower metabolic rate
less oxygen consumption
Geocadin RG, Koenig MA, Jia X et al. Management of brain injury after
resuscitation from cardiac arrest. Neurol Clin. 2008;22:487-506.
Hypothermia làm chậm tổn thương thần kinh
do thiếu oxy sau ngưng tim
• Cơ chế:
– giảm tỷ lệ biến dưỡng não (cerebral metabolic rate:
CMRO2)
– ức chế sản xuất gốc tự do (free radical )
– ức chế phóng thích amino acid kích thích (excitatory amino acid)
– ức chế sự tràn vào của calcium (calcium shifts)

Điều trị hypothermia có tác dụng bảo vệ thần
kinh sau ngưng tim
Chưa thật sự hiểu hết
Giảm nhu cầu năng lượng sau ngưng tim

Điều trị hypothermia có tác dụng bảo vệ thần kinh
sau ngưng tim
Chưa thật sự hiểu hết
Giảm nhu cầu năng lượng sau ngưng tim
Hiệu quả điều trị hạ nhiệt
• Hạ nhiệt (Cooling) trong 24 giờ và làm ấm
chậm hạn chế ảnh hưởng thiếu oxy não và tái
tưới máu
• Hypothermia làm chậm biến dưỡng não (↓O2 consumption by 6% for each degree in body
temperature reduction)
• Hypothermia hạn chế chết tế bào não và giảm
bớt phù não

Phòng ngừa sốt
83% bệnh nhân ngưng tim có sốt trong 48
giờ sau ngưng tim
Phòng ngừa sốt trong 72 giờ sau hồi sức
giảm dự hậu thần kinh
Lịch sử
1. Hypothermia đã được báo cáo ở Egyptians, Greeks & Romans
2. Hippocrates – đắp nước đá và tuyết lên vết thương bn làm giảm
chảy máu
3. Napoleon’s surgeon Genral Baron Larrey quan sát người lính bị
thương và nhiệt độ thấp và đặt họ gần lửa, chết nhanh hơn người
còn nhiệt độ thấp


A randomized controlled trial



50
Therapeutic hypothermia improves
outcome after cardiac arrest
HACA trial - Austria
* External cooling device (time 0: hospital admission)
*
THE HYPOTHERMIA AFTER CARDIAC ARREST STUDY GROUP

51
Therapeutic hypothermia improves
outcome after cardiac arrest
Bernard’s trial - Australia
* Ice packs (time 0: ambulance)
*

52
• 109 comatose patients with OHCA – Swiss tertiary university hospital
• 54 treated with standard resuscitation + normothermia
• 55 treated with standard resuscitation + therapeutic hypothermia
• End-points – Feasibility
– Safety
– Outcome
Crit Care Med, 2006;34(7):1865
Khả thi
An toàn
Dự hậu

32
33
34
35
36
37
38
0 3 6 12 18 24 36 48
NORMOTHERMIA (n=54)
HYPOTHERMIA (n=55)
T°C
Time (hrs)
Therapeutic hypothermia : 3 phases
induction
maintenance
rewarming


55
Điều trị hạ nhiệt sau ngưng tim
sự thành công từ lý thuyết đến lâm sàng
(a successful translation from bench to bedside)
> 500 patients studied
* * * * * *
% g
oo
d o
utc
om
e

56
Hypothermia (HT) vs. Normothermia (NT)
21st century
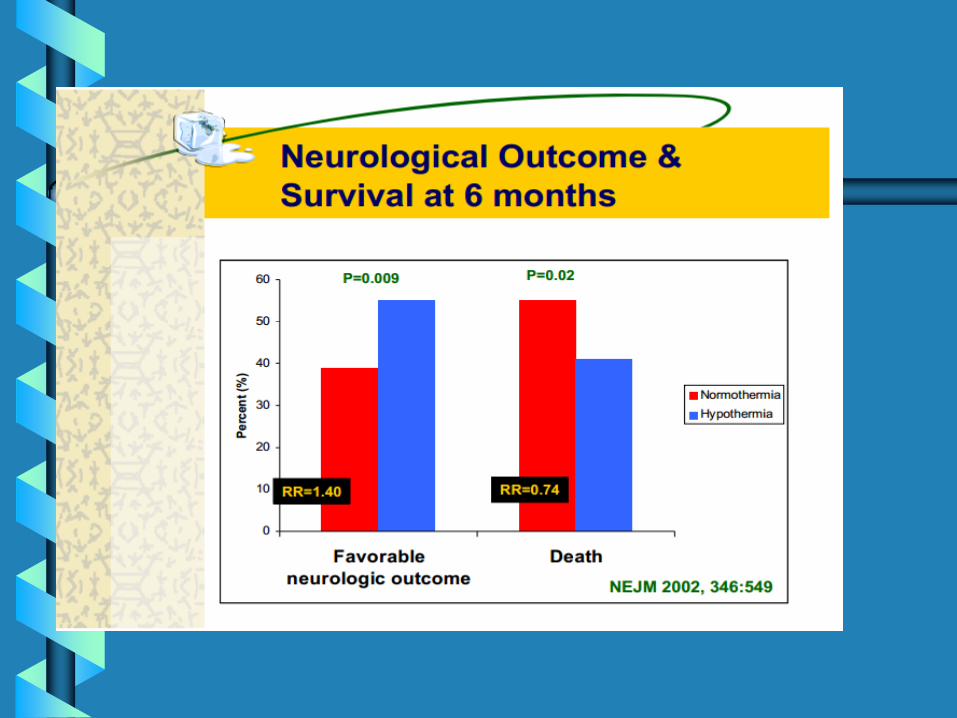
• VF, no shock (rung thất, không shock) – HACA trial 2002 (275 pts)
• Good outcome TH 55% vs. NT 39% P<0.05
– Bernard 2002 (77 pts)
• Good outcome TH 49% vs. NT 26% P<0.05
– Oddo 2006 (109 pts)
• Good outcome TH 56% vs. NT 26% P<0.05
– Busch 2006 (61 pts)
• Good outcome TH 59% vs. NT 32% P<0.05
– Belliard 2007 (68 pts)
• Good outcome TH 56% vs. NT 36% P<0.05

57
Tác dụng phụ của điều trị hạ nhiệt
Study Arrhythmia Pneumonia Sepsis Bleeding
Bernard, 1997 Yes No No No
Yanagawa, 1998 No Yes*p<0.05 No
Zeiner, 2000 Yes No No No
Nagao, 2000 Yes Yes
Felberg, 2001 Yes Yes Yes
Idrissi, 2001 No No No No
Holzer, 2002 No No No Yes
HACA, 2002 Yes Yes Yes Yes
Bernard, 2002 No No No No
Bernard, 2003 No No No No
Oddo, 2006 No No No No
THE HYPOTHERMIA AFTER CARDIAC ARREST STUDY GROUP: HACA

• Điều trị hạ nhiệt là chăm sóc chuẩn mực ở bn hôn mê sau ngưng tim do rung thất
• Chúng ta có thể điều trị hạ nhiệt cho tất cả bn hôn mê sau ngưng tim ?
– VF và shock tuần hoàn
– Non-VF
Chỉ định và chống chỉ định
trong điều trị hạ nhiệt độ
sau ngưng tim

Ai sẽ cần điều trị (củ)?
1. Trên 18 tuổi
2. Ngưng tim không do chấn thương do rung
thất hay nhịp nhanh thất vô mạch
3. Tuần hoàn trở về tự phát không hồi phục
thần kinh hoàn toàn(hôn mê)

1. Adult >18 years
2. Witnessed out-of-hospital cardiac arrest when initial
rhythm pulseless VT or Vfib; consider inPEA or
asystole; consider after in-hospital cardiac arrest
3. ROSC within 60 minutes from start of CPR
4. Unconscious with GCS < 8 after ROSC
5. Endotracheal intubation with mechanical ventilation
6. Initial temperature > 30°C
Inclusion Criteria (mới)

Ai sẽ không điều trị (củ)?
1. Phụ nữ có thai
2. Shock tim nặng
3. Bệnh lý đông máu nguyên phát
4. Tình trạng không hồi sức(DNR)
5. Hôn mê không do ngưng tim
6. CPR trên 45 phút
7. Ngưng tim mà không do VF nguyên phát
hay V tach
Exclusion Criteria(mới)
1. Patients who were comatose prior to cardiac arrest
(head injury, drug overdose, status epilepticus,
suspected intracranial hemorrhage)
2. Uncontrolled GI bleeding
3. Patients who are terminally ill/DNR order
4. Patient not intubated
5. Rapidly improving neurological status

Exclusion Criteria(mới)
6. Temperature < 30◦C after cardiac arrest
7. MAP < 60 mmHg despite fluids and vasopressors
8. Variability continues in who receives TH
(Camp-Rogers TR, et al. An observational study of patient
selection criteria for post-cardiac arrest therapeutic hypothermia.
[Review].Resuscitation 2013;84:1536-9.)

1. Làm hạ quá mức không chủ tâm <32°C - Ventricular arrhythmias
- Very little risk at temperatures greater than 30°C
- Below 30°C defibrillation may not be effective
2. Di chuyển Potassium - Potassium shifts into the cells due to cooling
- As the patient is rewarmed, potassium shifts back into the
intravascular space
- Need to be cautious if replacing potassium during cooling
process!

3. Co mạch và lợi tiểu
Vascular volume is decreased and patient may need fluid
replacement during rewarming
4. Tăng nguy cơ nhiễm trùng
Macrophage / leukocyte function is slowed
If patient is cooled for less than 24 hours, the effects are minimal
5. Chảy máu có thể gia tăng khi nhiệt độ dưới
35°C Clotting factor reactions are slowed
6. Gây kiềm chuyển hóa(metabolic alkalosis)
7. Lạnh có thể tác động vài loại thuốc dùng sau
ngưng tim
8. Giảm nhu động đường tiêu hóa và biến
dưỡng gan
9. Run rẩy (Shivering) - gia tăng nhu cầu biến dưỡng
- khó chịu
- tăng nhiệt độ

Sự khác biệt không ý nghĩa thống kê

Hypothermia có thể không gia tăng tổng số
người sống sót nhưng gia tăng chất lượng
sống người sống sót
Hiện nay, dự hậu xấu thần kinh thường gặp
và trung bình chỉ 3-4% bn trở về chức năng
bình thường

ĐiỀU TRỊ HẠ NHIỆT

Điều trị như thế nào ?
1. Hạ nhiệt 32-34 độ C
2. Theo dõi nhiệt độ mỗi 1 giờ
3. HATB 60-80mmHg
4. Nằm đầu cao 30 độ
5. Duy trì pO2 90-100mmHg
6. pH trong giới hạn bình thường
7. Bắt đầu nuôi ăn qua đường ruột
8. Tái ấm lại thụ động sau 24 giờ hạ nhiệt đã
hoàn thành

1. Thần kinh và tim mạch thích hợp
hypothermia nhẹ - 89.6 – 95°F (32 - 35°C)
2. Biến chứng gia tăng với nhiệt độ thấp hơn
hypothermia trung bình - 82.4 – 89.5°F (28 - 32°C)
và hypothermia nặng - < 82.4°F (<28°C)
Có thể gây dysrhythmias, bradycardia, vấn đề đông
máu và gia tăng nguy cơ nhiễm trùng.
• 30 to 40 mL/kg cooled to 4˚C infused over 30 min
reduces core temperature 2˚C - 2.5˚C
• Decreases time to therapeutic temperature (32 - 34˚C)
• Simple, safe, inexpensive, and effective in lowering
body temperature
• Patient continues to cool after rate decreased
(overshoot goal temperature)
Cold Intravenous Fluids

Bernard et al. Resuscitation 2003 30ml/kg 4C RL reduced temp 35.5 to 33.8C.
Initiated in ED.
Kim et al. Circulation 2005 2L 4C NS reduced temp by 1.4C in 30 min.
Polder man et al. Crit Care Med 2005 2 Liters 4C NS bolus (+) Cooling blanket
Reduced temp from 36.9 to 32.9 in one hour
No complications in either study were reported.
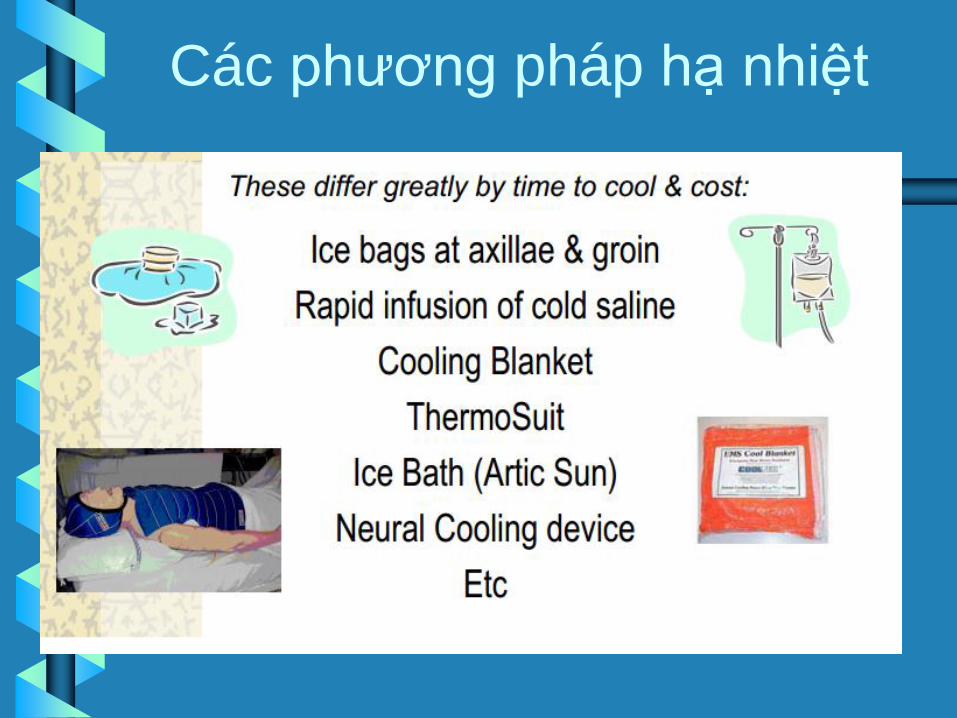
Các phương pháp hạ nhiệt

External (ngoài)
- Cooling blankets, ice packs
- Cooling helmet (mũ chụp)
Internal (trong)
- Cold saline/fluids
- Endovascular/Intravascular heat exchange device
- Intranasal
- Cardiopulmonary bypass

Internal methode
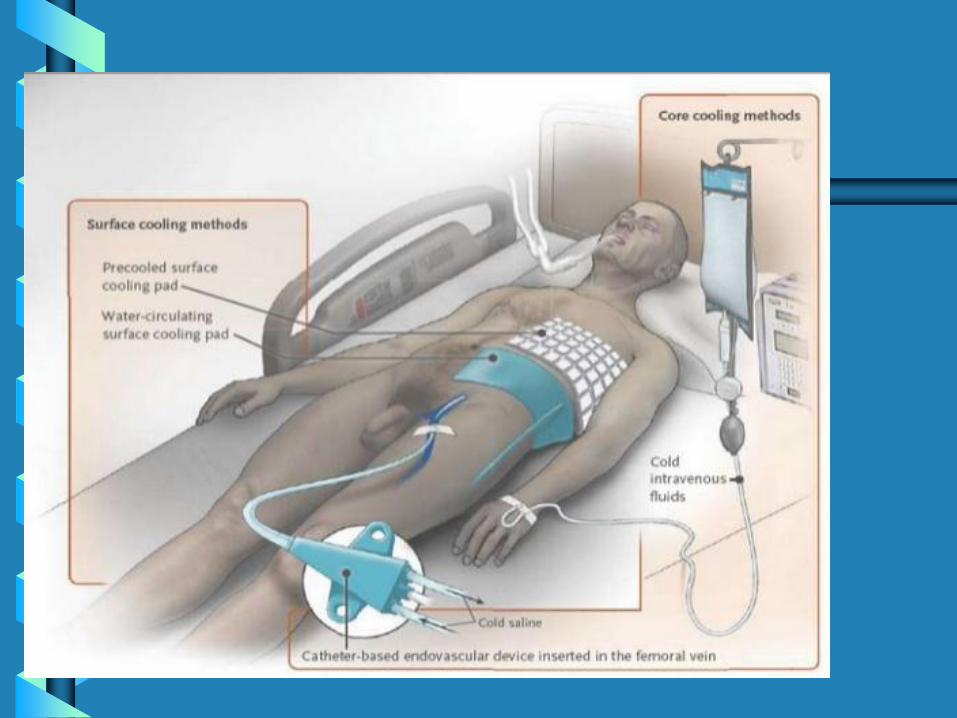

External mefhode




83
Khuyến cáo quốc tế
• July 2003: ILCOR Advisory statement – Điều trị hạ nhiệt được khuyến cáo sau
• Người chứng kiến ngưng tim
• Do rung thất (ventricular fibrillation)
• Sau hồi sức không có shock tuần hoàn
The International
Liaison
Committee on
Resuscitation
(ILCOR) was
formed in 1992
(ủy ban liên lạc
hồi sức quốc tế)

Hướng dẫn điều trị hạ nhiệt của AHA
1. Bn mất ý thức với ROSC sau OHCA sẽ điều trị hạ nhiệt
32-34 độ từ 12-24 giờ khi nhịp bắt đầu là rung thất
2. Hạ nhiệt có thể ích lợi cho nhịp khác hay IHCA

2005 khuyến cáo AHA và ILCOR
Khuyến cáo gây và duy trì 12-24 giờ,
điều trị hạ nhiệt (33 độ C) sau ROSC
BN bị OHCA còn hôn mê sau hồi sức,
khởi đầu nhịp tim là rung thất

2005

2005

1. Bên cạnh việc hấp thụ O2 việc thải CO2 là một chức
năng quan trọng của hô hấp do đó thành phần CO2
trong khí thở ra có liên quan mật thiết đến các quá trình
sinh lý trong cơ thể.
2. Giá trị và sự biến thiên của tỷ lệ CO2 trong khí thở có ý
nghĩa quan trọng trong việc đánh giá tình trạng bệnh
nhân và giúp quá trình điều trị có hiệu quả.
3. Đường biểu diễn sự thay đổi tỷ lệ CO2 trong khí thở theo
thời gian gọi là capnogram. Thông thường người ta hiển
thị áp lực riêng phần của CO2 hoặc nồng độ CO2.
Capnography
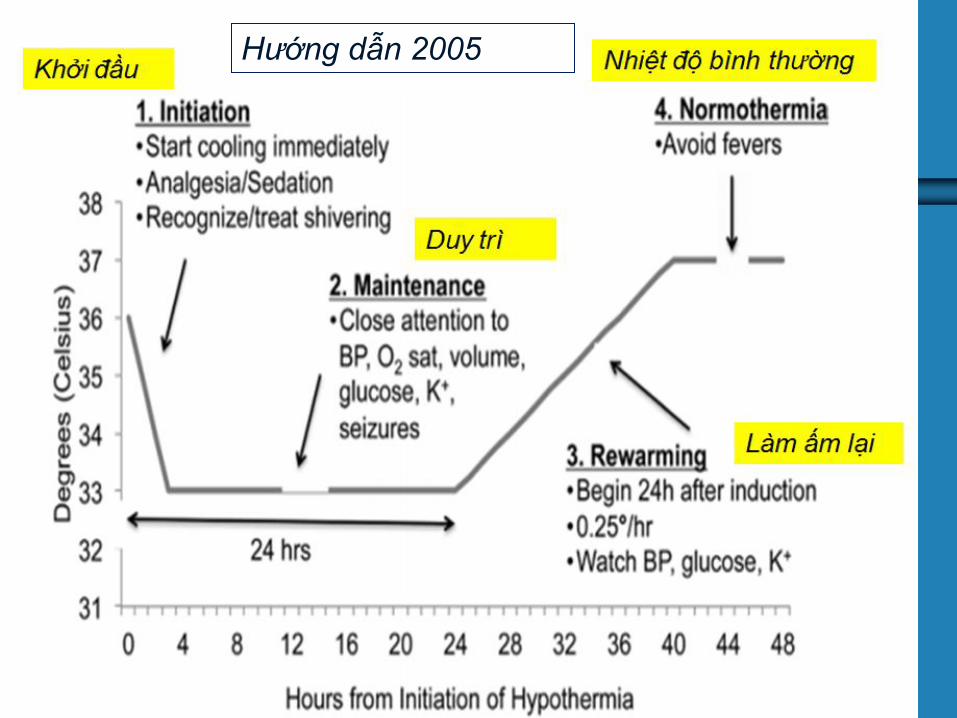
Hướng dẫn 2005

Khuyến cáo AHA 2010 so với khuyến
cáo năm 2015 về đích nhiệt độ điều trị.
(What is the status of targeted
temperature management (TTM)?)

1. The 2010 Guidelines strongly advised induced
hypothermia (32ºC to 34ºC) for the subgroup of
patients with out-of-hospital VF/pulseless ventricular
tachycardia (pVT) cardiac arrest and post-ROSC
coma (the absence of purposeful movements), and
encouraged that induced hypothermia be considered
for most other comatose patients after cardiac arrest.
2. Precise duration and optimal temperature targets
were unknown, and the Guidelines recommended 12
to 24 hours at 32ºC to 34ºC based on the regimens
studied in prior trials
Hướng dẫn 2010

The TTM after a cardiac arrest clinical trial published in
2013 included patients with both shockable and
nonshockable rhythms experiencing out-of-hospital
cardiac arrest.
The TTM trial showed that hypothermia at a targeted
temperature of 33° C did not confer a benefit as compared
with a targeted temperature of 36° C in the first 24 hours
and both groups did not differ in complication rates.
Hướng dẫn 2013
Đích hạ 33 độ C không ích lợi so
36 độ C trong trong 24 giờ đầu
It is left at the discretion of the hospital policy to use
either 36 or 33° C pending further guidance. It is
important to highlight that 36° C in this trial was not
intended to represent the normothermia arm but rather
the TTM arm.
Maintaining this temperature target still requires similar
active interventions as the induced hypothermia
Dùng cả 2 36 hay33° C trong
khi chờ đợi, quan trọng 36° C

The 2015 ILCOR systematic review identified multiple
new randomized controlled trials testing different target
temperatures and different timing for initiation of
temperature control after cardiac arrest.52
Reflecting that a variety of temperature targets are now
used, the term targeted temperature management
(TTM) has been adopted to refer to induced
hypothermia as well as to active control of temperature
at any target.
Hướng dẫn 2015
TTM thông qua gây hạ nhiệt tác động
tốt ở bất cứ đích nào

Guidelines Update for Cardiopulmonary Resuscitation
and Emergency Cardiovascular Care
(+ based on an extensive evidence review process that was begun
by the International Liaison Committee on Resuscitation (ILCOR)
after the publication of the 2010 International Consensus on
Cardiopulmonary Resuscitation and Emergency Cardiovascular Care
Science With Treatment Recommendation
+ completed in February 2015)
The recommendations in the 2015
American Heart Association (AHA)

Targeted temperature management
(TTM), formally known as “therapeutic
hypothermia,”

2015 Recommendations - Updated
1. We recommend that comatose (ie, lack of
meaningful response to verbal commands) adult
patients with ROSC after cardiac arrest have TTM
(Class I, LOE B-R for VF/pVT OHCA; for non-
VF/pVT (ie, “nonshockable”) and in-hospital
cardiac arrest). (Class I, LOE C-EO)
(C
2. We recommend selecting and maintaining a
constant temperature between 32ºC and 36ºC
during TTM. (Class I, LOE B-R)

2015 Recommendations - Updated
3. It is reasonable that TTM be maintained for at
least 24 hours after achieving target temperature.
(Class IIa, LOE C-EO)

Củ-2010
Comatose (ie, lacking of meaningful response to
verbal commands) adult patients with ROSC after
out-of-hospital VF cardiac arrest should be cooled to
32°C to 34°C for 12 to 24 hours.
Induced hypothermia also may be considered for
comatose adult patients with ROSC after IHCA of any
initial rhythm or after OHCA with an initial rhythm of
pulseless electrical activity or asystole.

Tại sao ?
1. Initial studies of TTM examined cooling to temperatures
between 32°C and 34°C compared with no well-defined
TTM and found improvement in neurologic outcome for
those in whom hypothermia was induced. (không xác định,
ghi nhận cải thiên nhóm hạ nhiệt)
2. A recent high-quality study compared temperature
management at 36°C and at 33°C and found outcomes
to be similar for both. (so sánh điều trị ở 36 và 33 độ, dự hậu
tương tự cả 2)

3. Taken together, the initial studies suggest that TTM is
beneficial, so the recommendation remains to select
a single target temperature and perform TTM.
4. Given that 33°C is no better than 36°C, clinicians can
select from a wider range of target temperatures.
5. The selected temperature may be determined by
clinician preference or clinical factors

Tiếp tục quản lý nhiệt độ sau 24 giờ
(Continuing Temperature Management
Beyond 24 Hours)

2015 ( mới):
Tích cực phòng ngừa sốt bn hôn mê sau TTM là hợp lý
(Actively preventing fever in comatose patients after TTM is
reasonable)
Tại sao?
In some observational studies, fever after rewarming
from TTM is associated with worsened neurologic
injury, although studies are conflicting. Because
preventing fever after TTM is relatively benign and
fever may be associated with harm, preventing fever is
suggested.
Sốt sau khi làm ấm lại làm tổn
thương thần kinh

Mục tiêu huyết động học sau hồi sức (Hemodynamic Goals After Resuscitation)
2015 (mới): có thể hợp lý tránh và hạ áp tức khắc trong
chăm sóc sau ngưng tim(HATT<90, HATB<65)
(It may be reasonable to avoid and immediately correct hypotension
(systolic blood pressure less than 90 mm Hg, mean arterial pressure
less than 65 mm Hg) during post–cardiac arrest care.)

Tại sao?
+ sau ngưng tim, HATT< 90 mmHg, HATB<65mmHg :tử
vong cao và giảm hồi phục chức năng
+ trong khi HATT>100mmHg hồi phục tốt

Dự hậu sau ngưng tim
(Prognostication After Cardiac Arrest)
2015 (mới):
Thời gian sớm nhất dự hậu thần kinh xấu qua khám lâm
sảng bn không TTM là 72 giờ sau ngưng tim, nhưng có
thể lâu hơn nếu bn dùng an thần hay liệt
(The earliest time to prognosticate a poor neurologic outcome using
clinical examination in patients not treated with TTM is 72 hours after
cardiac arrest, but this time can be even longer after cardiac arrest if
the residual effect of sedation or paralysis is suspected to confound
the clinical examination.)

2015 ( cập nhật:
Bn điều trị TTM, an thần hay liệt có làm lẩn lộn thăm
khám lâm sàng, chờ đợi 72 giờ sau khi nhiệt độ trở
lại bình thường trước khi tiên lượng dự hậu
(In patients treated with TTM, where sedation or paralysis
could confound clinical examination, it is reasonable to wait
until 72 hours after return to normothermia before predicting
outcome.)

2010 (củ):
không có khuyến cáo về thời gian dự hậu
(While times for usefulness of specific tests were identified, no
specific overall recommendation was made about time to
prognostication.)

Tại sao ?
+ Clinical findings, electrophysiologic modalities,
imaging modalities, and blood markers are all useful for
predicting neurologic outcome in comatose patients, but
each finding, test, and marker is affected differently by
sedation and neuromuscular blockade.
+ In addition, the comatose brain may be more sensitive
to medications, and medications may take longer to
metabolize after cardiac arrest.

+ No single physical finding or test can predict
neurologic recovery after cardiac arrest with 100%
certainty.
+ Multiple modalities of testing and examination used
together to predict outcome after the effects of
hypothermia and medications have been allowed to
resolve, are most likely to provide accurate prediction
of outcome

Ích lợi lâm sàng kết hợp dự hậu
thần kinh xấu (Useful Clinical Findings That Are Associated
With Poor Neurologic Outcome*)

+ Absence of pupillary reflex to light at 72 hours or more
after cardiac arrest
+ Presence of status myoclonus (different from isolated
myoclonic jerks) during the first 72 hours after cardiac
arrest
+ Absence of the N20 somatosensory evoked potential
cortical wave 24 to 72 hours after cardiac arrest or after
rewarming
+ Presence of a marked reduction of the gray-white ratio
on brain CT obtained within 2 hours after cardiac arrest

+ Extensive restriction of diffusion on brain MRI at 2
to 6 days after cardiac arrest
(hạn chế khuếch tán trên MRI não)
+ Persistent absence of EEG reactivity to external
stimuli at 72 hours after cardiac arrest
+ Persistent burst suppression or intractable status
epilepticus on EEG after rewarming
Absent motor movements, extensor posturing, or myoclonus should
not be used alone for predicting outcome.
*Shock, temperature, metabolic derangement, prior sedatives or
neuromuscular blockers, and other clinical factors should be
considered carefully because they may affect results or interpretation
of some tests.

Hypothermia in the
Prehospital Setting - Updated

2015 Recommendation - New
We recommend against the routine prehospital
cooling of patients after ROSC with rapid infusion of
cold intravenous fluids. (Class III: No Benefit, LOE A)
Không hạ nhiệt thường quy trước
bệnh viện bn sau ROSC với truyền
nhanh TM dung dịch lạnh
Other Neurologic Care - Updated
1. Brain injury is a common cause of morbidity and
mortality in post–cardiac arrest patients.
2. Brain injury is the cause of death in 68% of patients
after out-of-hospital cardiac arrest and in 23% after in-
hospital cardiac arrest. 87
3. The pathophysiology of post–cardiac arrest brain injury
involves a complex cascade of molecular events that
are triggered by ischemia and reperfusion and then
executed over hours to days after ROSC.
Other Neurologic Care - Updated
4. Events and conditions in the post–cardiac arrest period
have the potential to exacerbate or attenuate these
injury pathways and impact ultimate outcomes.
5. Clinical manifestations of post–cardiac arrest brain
injury include coma, seizures, myoclonus, various
degrees of neurocognitive dysfunction (ranging from
memory deficits to persistent vegetative state), and
brain death.88

The 2010 Guidelines emphasized advanced
neurocritical care for patients who have brain injury
after cardiac arrest, including :
+ electroencephalography (EEG) phát hiện cơn động
kinh và nhanh chóng điều trị.
+ The 2015 ILCOR systematic review considered
detection and treatment of seizures.

Seizure Management - Updated
1. An EEG for the diagnosis of seizure should be
promptly performed and interpreted, and then
should be monitored frequently or continuously in
comatose patients after ROSC. (Class I, LOE-LD)
2. The same anticonvulsant regimens for the
treatment of status epilepticus caused by other
etiologies may be considered after cardiac arrest.
(Class IIb, LOE C-LD)

Neuroprotective Drugs
The routine use of coenzyme Q10 in patients treated
with hypothermia is uncertain. (Class IIb, LOE B)
Few neuroprotective drugs have been tested in clinical trials, and only
one published randomized trial was performed in which a
neuroprotective drug was combined with therapeutic hypothermia. No
neuroprotection benefit was observed when patients (without
hypothermia) were treated with thiopental, glucocorticoids,
nimodipine, lidoflazine, diazepam, and magnesium sulfate. One trial
using coenzyme Q10 in patients receiving hypothermia failed to show
improved survival with good neurological outcome

Trong thực hành
1. Ở Mỹ bn hôn mê sau ngưng tim được theo dõi bs
thần kinh (hospitalist or neurointensivist).
2. Châu Âu nghiên cứu gần đây cho thấy liên hệ bs
thần kinh 25% về dự hậu thần kinh và quyết định
mức độ chăm sóc và điều tri
3. Nếu dự hâu xấu xác định tiêu chuẩn thần kinh “rút
lui chăm sóc”
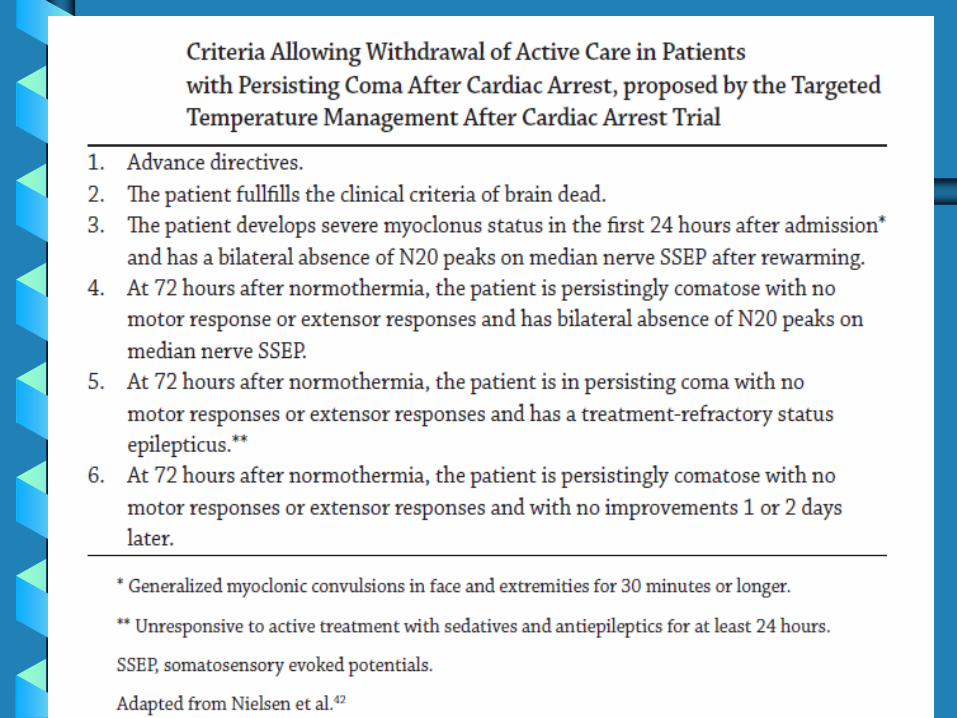
The most recent (and reasonable) proposal has come
from the Targeted Temperature Management After
Cardiac Arrest trial but it remains a difficult judgment
call which cannot be simplified as a few rules


Kết luận và tương lai
1. Lĩnh vực chăm sóc sau ngừng tim gia tăng chiều sâu
nhanh chóng trong thập kỷ qua
2 Các nghiên cứu can thiệp tương lai thiết kế lý tưởng,
giải trình sự đa dạng của bệnh nhân và tiêu điểm can
thiệp trong các nhóm chuyên biệt có thể lợi ích nhất
3. Bằng can thiệp đáp ứng sinh lý và bệnh tật, cơ hội
tồn tại sự sống lớn hơn, điều trị đúng sẽ mang lại ích
lợi cho bệnh nhân

Câu hỏi ?





























![VIETNAMESE - Hepatitis...• đi đến phòng khám sức khỏe Tình dục • Tới một phòng khám xét nghiệm nhanh được gọi là a[TesT] (chỉ khi quý vị là đàn](https://img.dokumen.tips/doc/110x75/5ece37b3ad894a6137715ba3/vietnamese-hepatitis-a-i-n-phng-khm-sc-khe-tnh-dc.jpg)