Embed Size (px)
Citation preview

Hepatopancreaticobiliary pathology
Jemimah Denson

EXOCRINE PANCREAS

Specimen cut-up
• Margins :– Transection:
• Pancreatic• Bile duct (cystic, CHD, CBD) • Gastric and duodenal
– Dissection:• SMV• SMA• Posterior• CRM around CBD stump

Specimen cut-up
From RCPath dataset copyright Paul Brown St James’s University Hospital, Leeds

2906/11

Chronic pancreatitis
• Causes:– ETOH + smoking (act synergistically)– Obstruction– hereditary
• Macro– Diffuse or focal – mimic tumour on imaging– Shrunken and very hard– Dilated ducts with concretions.

Chronic pancreatitis
• Micro:– Acinar atrophy– Fibrosis– Pancreatic duct changes– Inflammation often mild– Islets remain– Enlarged peripheral nerves– Perineural invasion!!
• Complicatons – DM, pseudocyst, vascular

21269/13

Autoimmune pancreatitis
• Two types:
• Type 1 – part of IgG4 disease spectrum
• Type 2 – don’t have raised IgG4 & rarely develop extrapancreatic IgG4 disease. Requires tissue for diagnosis.

Autoimmune pancreatitis
• Macro– Usually diffuse but can be focal & mass
forming– Main PD is diffusely or segmentally narrowed
(cf other forms of pancreatitis)– 60% pancreatic head involved with narrowing
of CBD – May involved peripancreatic fat & enlarge LNs
– mimics Ca

Autoimmune pancreatitis
• Micro– Common to both types:
• Periductal lymphoplasmacytic inflammation• Inflammation of acinar parenchyma• Patchy distribution
– Type I• Storiform fibrosis• Obliterative phlebitis• Involvement of peripancreatic fat
– Type II• Granulocytic epithelial lesion (GEL)

AIP
Show 7728/12

IgG4
• What is positivity??• Depends on tissue and criteria• HISORt
– >10 positive cells per hpf– Better for biopsy material
• Boston– >50 positive cells per hpf AND IgG4:IgG >40%– Better for resection specimens
• Interpret with caution

Groove pancreatitis
• I have yet to see an example• Aka paraduodenal pancreatitis• Clinical history• Underlying cause is ectopic pancreatic tissue
within wall of duodenum – usually between ampulla of Vater and minor ampulla.
• Impaired drainage of pancreatic secretions leads to duct dilatation, cyst formation, rupture and inflammation.
• Worsened by ETOH

Groove pancreatitis
• Cysts in duodenal wall and pancratoduodenal groove
• Cystic spaces lined by flattened ductal epithelium or granulation tissue
• Acute and chronic inflammation
• Thickened duodenal MP with other foci of ectopic pancreas
• Brunner’s gland hyperplasia


Case history
• 25 year old female
• Abdominal and back pain, N&V, early satiety
• Imaging – large solid and cystic neoplasm in head of pancreas

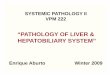
Microscopy

Microscopy

Solid pseudopapillary neoplasm
• Characteristically young females
• Low grade malignant but usually excellent prognosis
• Usually solitary
• Anywhere in pancreas
• Solid or cystic and anything in between, cyst is degenerative
• Usually encapsulated

Solid pseudopapillary neoplasm
• Poorly cohesive monomorphic cells
• Pseudopapillae
• Degnerative changes
• Cells:– Eosinophilic, foamy or vacuolated– Nucleus often indented or grooved– Eosinophilic globules

SPN immunohistochemistry
• Positive• Vimentin, CD10, β-catenin (nuclear and
cytoplasmic), PR, ORA beta, CD56, NSE• A1AT/A1ACT highlight eos. globules
• +/-• Synaptophysin, epithelial markers
• Negative• CK 7 & 19, chromogranin A, ORA alpha

1163/13

Pancreatic cystsNeoplastic epithelial:Serous cystic neoplasm
Mucinous cystic neoplasm
IPMN
SPN
Acinar cell cystadenoma
Cystic teratoma
Cystic ductal adenocarcinoma
Cystic pancreatoblastoma
Cystic mets
Nonneoplastic epithelial:Congenital cyst
Duplication
Choledochal cyst
Cystic hamartoma
Lymphoepithelial cyst
Retention cyst
Groove pancreatitis
Endometrial cyst
Neoplastic non-epithlieal:Lymphangioma
Haemangioma
Cystic schwannoma
Cystic degeneration in LMS
Cystic degeneration in GIST
Cystic degeneration in MPNST
Cystic degeneration in paraganglioma
Nonneoplastic non-epithelial:Pseudocysts
Parasitic cysts

Serous cystic neoplasms
• Serous cystadenoma or cystadenocarcinoma (very rare)
• Microcystic (more♀) or macrocystic (more ♂) • Solid serous adenoma• Often asymptomatic – incidentally detected• Characteristic imaging for microcystic with
‘starburst’ pattern• Associations – minority vHL & NETs

Serous cystadenoma• Macro
– Microcystic mostly body/tail. Sponge like with stellate scar
– Macrocystic mostly head. Few thin walled cysts with watery fluid
– Don’t usually communicate with duct system.
• Micro– Single layer cuboidal cells with clear cystoplasm
• ICC and ∆∆• Malignancy diagnosed on clinical behaviour

Show 3847/13

Mucinous cystic neoplasms
• Classification– Premalignant
• Low-grade, intermediate & high-grade dysplasia.
– Malignant i.e. invasive carcinoma
• Mostly female• Mean age 45• Most in body or tail• Solitary – uni or multilocular• Don’t communicate with duct system• Lined by tall, columnar, mucin-producing cells
with characteristic ovarian-type stroma

2283/13

Intraduct papillary mucinous neoplasia
• Grossly and radiologically visible papillary mucin forming lesion arising from main PD or its branches
• Classification:– Premalignant
• Low to high grade dysplasia
– Malignant
• Mean 65 yrs, ♂:♀ = 1.5:1• Associations ??P-J & FAP. Synchronous &
metachronous extrapancratic malignancies in 10-40%

IPMN
• Further subtyped into:– Main duct type, branch duct type or mixed– Epithelial subtype:
• Gastric (BD > MD)• Intestinal (MD > BD)• Pancreaticobiliary (BD > MD)• Oncocytic (BD > MD)
• Gastric type most likely to be LG, rest more likely to be HG

PanIN
• Precursor lesion for pancreatic ca• Classification
– PanIN 1A = mucinous (pyloric) metaplasia, flat lesion
– PanIN 1B = papillary architecture– PanIN 2 = atypical hyperplasia (LG dysplasia)– PanIN 3 = HG dysplasia
• Microscopic diagnosis• ∆∆• Show 29021/13

Ductal adenocarcinoma
• Risk factors– Age– Sex– Race– Chronic pancreatitis– Smoking– Familial/inheritied (10%)
• FAMMM• BRCA2• Peutz-Jeghers• HNPCC & FAP

Ductal Adenocarcinoma
• Site– Distal BD, ampulla, pancreas
• Epithelial subtypes– Pancreaticobiliary, intestinal, clear cell, foamy cell
etc..
• Mixed tumours/variants– Adenosquamous (squame at least 30%)– Colloid (mucin pools at least 80%)– Signet ring, Medullary, hepatoid, undifferentiated etc– MANEC (both at least 30%)

Show 29683/13

Acinar cell carcinoma
• Mostly adults, mean 60 yrs, but account for 15% of paediatric exocrine pancreatic neoplasms.
• May get lipase hypersecretion syndrome
• 50% present with mets
• Macro – large, well circumscribed or encapsulated tumours. Pushing border. Occur anywhere in pancreas.

Acinar cell carcinoma
• Lobules of cellular tumour sep’d by fibrous bands.
• Acinar pattern, solid or trabecular• Granular eosinophilic cytoplasm• Prominent nucleoli• Zymogen granules PAS/D positive• ICC:
– Trypsin, chymotrypsin, lipase, (amylase)– Bcl10, A1AT, AE1/AE3

Show 32345/13

Other pancreatic tumours
• Non-epithelial– Very rare <1% of pancreatic neoplasms– More often spread from extrapancreatic
primary
• Paediatric
• Mets– Lung, kidney, breast, colon and MM most
common

LIVER

Classification
• Hepatocellular
• Biliary
• Other

7060/12

7060/12

Focal nodular hyperplasia• Young women• Aetiology ?abnormal blood flow• Can have more than 1 lesion• Characteristic macroscopic appearance
with central scar• Large, thick walled vessels within fibrous
septae• Bile ductules at periphery• Features of cholestasis• Bland, normal appearing hepatocytes

Sounds like FNH??
• Nodular regenerative hyperplasia– Hyperplastic hepatocytes form small nodules,
without fibrous tissue. More diffuse, part of a process of disorder blood flow in liver
• Partial nodular transformation– Very rare, nodule at the hilum, similar to NRH
• Macroregenerative nodule– At least 8mm diam. Usually a large nodule of
cirrhosis. May be pre-neoplastic (see later)

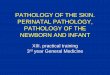
3717/13

Hepatocellular adenoma
• Steatotic– HNF1α mutated – usually somatic but can be inherited –
association with hereditary DM, multiple colonic adenomas– Least associated with malignancy
• Inflammatory (telangiectatic)– OCP association and obesity, fatty liver, ETOH excess– Present with inflammatory syndrome
• Β-catenin activated– More often male– More malignancy risk, may be precursor lesion– ??FAP association
• Other

Hepatocellular adenoma
• General features– Occur in non-cirrhotic liver– Often unencapsulated– Bland hepatocytes, 2-3 cell thick plates, retained retic
network.– No bile ducts although ductules may be seen.
• Specific features– Steatotic– Β-cat mutated may show mild atypia & rosettes– Inflammatory – inflamed portal tracts with no
veins/BDs, thick walled vessels, ductular reaction, sinusoidal dilatation & peliosis

Hepatocellular adenoma
• Special stains– No specific marker– Reticulin– Steatotic
• LFABP negative (cf normal liver and other HCA types)
– β-catenin activated• Nuclear β-cat & GS positive
– CD34– Serum amyloid A

Premalignant/early malignant lesions
• Macroscopic lesions– Large regenerative nodule = MRN– Dysplastic nodule – low and high grade– Early HCC <2cm
• Microscopic features– Large cell change - ?if premalignant or not– Small cell change - premalignant– Dysplastic foci = <1mm diameter
• Definition of HCC = stromal invasion

33469/13


HCC
• Liver disease
• Environment
• Geographical
• Unless patient is being screened it often presents late
• Pt may have raised serum AFP

HCC
• Macroscopic– Classic appearance = ……– Usually soft tumour
• Microscopic– Varied but classically:
• pseudoglandular/trabecular growth• cells look like hepatocytes• Bile production• Various inclusions esp eosinophilic globules

Diagnosing HCC
• Hopefully characteristic macro and microscopic appearances
• On biopsy can be very difficult to ∆∆ low-grade HCC from dysplastic nodule or even adenoma.
• Histochemistry– Reticulin, DPAS
• ICC

HCC ICC
• Malignant or not?– CD34, glypican 3, HSP70, glutamine
synthetase all more +ve in HCC– CK7/19 can help differentiate between true or
pseudo invasion (+ve ductular reaction in pseudo)
• HCC vs non-hepatic– HepPar 1, AFP, TTF-1, CD10, pCEA
Show ICC & 21521/13

2478/10

Fibrolamellar HCC
• Younger patients
• Not associated with chronic liver disease/cirrhosis
• Better prognosis
• Polygonal eosinophilic cells within abundant fibrous stroma

22567/13

Benign biliary tumours
• Von Myenburg complex
• Bile duct adenoma
• Bile duct cyst
• Ciliated hepatic foregut cyst
• Intraductal papillary neoplasms & biliary papillomatosis
• Mucinous cystic neoplasm (hepatobiliary cystadenoma)

260/12

Cholangiocarcinoma
• Intrahepatic vs hilar vs extrahepatic• Aetiology less clear than HCC• Increased risk in chronic biliary dx,
cirrhosis, parasitic infections (SE Asia), mucinous cystic neoplasm, biliary papillomatosis
• Diagnostic difficulties:– Intrahepatic CC vs met adenocarcinoma– HCC vs CC or mixed tumour

Mixed HCC-CC
• Peripheral mass forming intrahepatic CC thought likely to have a hepatic progenitor cell origin which may explain mixed tumours (which tend to behave like CC)

Non-epithelial liver lesions
• Vascular– Haemangiomas, epithelioid
haemangioendothelioma
• Other mesenchymal– Inflammatory pseudotumour– angiomyolipoma
• Leukaemias & lymphomas