Embed Size (px)
Citation preview

Journal of Clinical InvestigationVol. 45, No. 5, 1966
Hemodynamic Effects after Reversion from Atrial Fibril-lation to Sinus Rhythm by Precordial Shock *
THOMAS KILLIP t AND RALPH A. BAER
(From the Department of Medicine, Cornell University Medical College, New York, N. Y.)
Atrial fibrillation is the most common persistentarrhythmia in man. Since it was clinically recog-nized more than 50 years ago (1, 2), there hasbeen continued interest in the effect of atrial fibril-lation on cardiac performance. The increasedheart rate and tendency to excessive tachycardiaduring exercise, characteristic of untreated atrialfibrillation, have frequently clouded interpretationof the dynamic effects of change in rhythm. Manystudies in man have reported increases in cardiacoutput after reversion from fibrillation to sinusrhythm (3-5). Some workers have found no sig-nificant changes in a number of subjects (4-6).Interpretation of the data, however, has been tem-pered by the problem of separating the effects of achange in atrial pacemaker from the influences oftherapy. Heart rates have frequently variedgreatly. Quinidine or another drug has been ad-ministered in various dosages. Time lapse be-tween measurements has been different from onestudy and from one patient to another. The hemo-dynamic response to atrial fibrillation may vary indifferent forms of heart disease, yet most reportshave furnished scant functional and diagnosticdetails.The application of synchronized, direct current,
precordial shock for the reversion of arrhythmiasprovides a unique tool for the evaluation of hemo-dynamic changes that occur with change in rhythm(7). The technique appears to avoid the dis-advantages associated with previous studies. Sincereversion occurs at a predictable moment, studies
* Submitted for publication August 9, 1965; acceptedJanuary 6, 1966.
Supported by U. S. Public Health Service grants HE-07044 and FR-47, Division of General Medical Sciences,National Institutes of Health.
Presented in part at the National Meeting, AmericanFederation for Clinical Research, Atlantic City, N. J.,May 2, 1964.t Address requests for reprints to Dr. Thomas Killip,
Dept. of Medicine, Cornell University Medical College,525 E. 68th St., New York, N. Y. 10021.
may be arranged with a constant time lapse beforeand after application of the technique.We are reporting the effects of reversion from
atrial fibrillation to sinus rhythm on cardiac func-tion in 27 patients with heart disease. Six pa-tients who did not revert form a control group.The data show that in patients with valvular heartdisease there is a significant increase in cardiacoutput after conversion to sinus rhythm. In pa-tients with small hearts who do not have valvularheart disease, there is no significant change in car-diac output after sinus rhythm is induced. Datafor subjects at rest and during exercise are pre-sented and the implications discussed.
Methods
Twenty-seven patients with chronic atrial fibrillationwere hospitalized for at least 3 days before study (Ta-ble I). Seventeen patients had rheumatic heart disease.Six patients had no valvular abnormalities and normal toslightly enlarged hearts and are classified as "benign"fibrillators (8). None of these patients had angina orevidence of old or recent myocardial infarction. Thefour other patients included a single example of atrialseptal defect 48 months after operative closure, a myo-cardiopathy of unknown cause, a calcific aortic stenosis,and a bacteriologically cured endocarditis.For purposes of analysis the patients were divided into
four groups. Group I comprises six patients who re-mained in atrial fibrillation despite attempted reversionand serves as a control for the techniques of reversionand repeated hemodynamic study. Group II contains tenpatients with mitral valve dysfunction, six patients withpredominant mitral stenosis and four with predominantmitral regurgitation. Group III consists of five patientswith aortic valve deformity, and Group IV includes thepatients with benign fibrillation.
All patients were maintained on digitoxin. Neitherquinidine nor procaine amide nor any other antiarrhyth-mic drugs were administered until after the studies hadbeen completed. No sedation was given before the hemo-dynamic measurements.
After the patients had fasted overnight, hemodynamicstudies were performed. Patients were anesthetized lo-cally with procaine hydrochloride; a polyethylene no. 190catheter was then placed in the left median arm vein by
658
HEMODYNAMICS OF ELECTRICAL REVERSION FROM ATRIAL FIBRILLATION
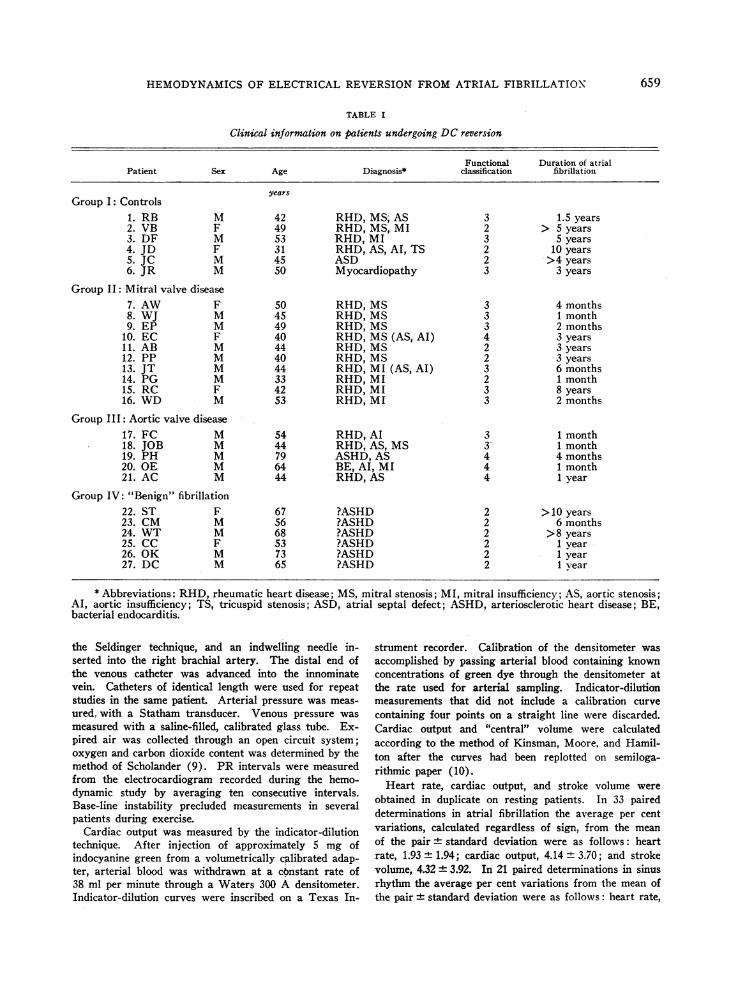
TABLE I
Clinical information on patients undergoing DC reversion
Functional Duration of atrialPatient Sex Age Diagnosis* classification fibrillation
yearsGroup I: Controls
1. RB M 42 RHD, MS; AS 3 1.5 years2. VB F 49 RHD, MS, MI 2 > 5 years3. DF M 53 RHD, MI 3 5 years4. JD F 31 RHD, AS, Al, TS 2 10 years5. JC M 45 ASD 2 >4 years6. JR M 50 Myocardiopathy 3 3 years
Group II: Mitral valve disease7. AW F 50 RHD, MS 3 4 months8. WJ M 45 RHD, MS 3 1 month9. EP M 49 RHD, MS 3 2 months
10. EC F 40 RHD, MS (AS, AI) 4 3 years11. AB M 44 RHD, MS 2 3 years12. PP M 40 RHD, MS 2 3 years13. JT M 44 RHD, MI (AS, AI) 3 6 months14. PG M 33 RHD, MI 2 1 month15. RC F 42 RHD, MI 3 8 years16. WD M 53 RHD, MI 3 2 months
Group III: Aortic valve disease17. FC M 54 RHD, AI 3 1 month18. JOB M 44 RHD, AS, MS 3- 1 month19. PH M 79 ASHD, AS 4 4 months20. OE M 64 BE, AI, MI 4 1 month21.AC M 44 RHD,AS 4 lyear
Group IV: "Benign" fibrillation22. ST F 67 ?ASHD 2 >10 years23. CM M 56 ?ASHD 2 6 months24. WT M 68 ?ASHD 2 >8 years25. CC F 53 ?ASHD 2 1 year26. OK M 73 ?ASHD 2 1 vear27. DC M 65 ?ASHD 2 1 vear
* Abbreviations: RHD, rheumatic heart disease; MS, mitral stenosis; MI, mitral insufficiency; AS, aortic stenosis;AI, aortic insufficiency; TS, tricuspid stenosis; ASD, atrial septal defect; ASHD, arteriosclerotic heart disease; BE,bacterial endocarditis.
the Seldinger technique, and an indwelling needle in-serted into the right brachial artery. The distal end ofthe venous catheter was advanced into the innominatevein. Catheters of identical length were used for repeatstudies in the same patient. Arterial pressure was meas-ured, with a Statham transducer. Venous pressure wasmeasured with a saline-filled, calibrated glass tube. Ex-pired air was collected through an open circuit system;oxygen and carbon dioxide content was determined by themethod of Scholander (9). PR intervals were measuredfrom the electrocardiogram recorded during the hemo-dynamic study by averaging ten consecutive intervals.Base-line instability precluded measurements in severalpatients during exercise.
Cardiac output was measured by the indicator-dilutiontechnique. After injection of approximately 5 mg ofindocyanine green from a volumetrically calibrated adap-ter, arterial blood was withdrawn at a constant rate of38 ml per minute through a Waters 300 A densitometer.Indicator-dilution curves were inscribed on a Texas In-
strument recorder. Calibration of the densitometer wasaccomplished by passing arterial blood containing knownconcentrations of green dye through the densitometer atthe rate used for arterial sampling. Indicator-dilutionmeasurements that did not include a calibration curvecontaining four points on a straight line were discarded.Cardiac output and "central" volume were calculatedaccording to the method of Kinsman, Moore, and Hamil-ton after the curves had been replotted on semiloga-rithmic paper (10).Heart rate, cardiac output, and stroke volume were
obtained in duplicate on resting patients. In 33 paireddeterminations in atrial fibrillation the average per centvariations, calculated regardless of sign, from the meanof the pair ± standard deviation were as follows: heartrate, 1.93 ± 1.94; cardiac output, 4.14 + 3.70; and strokevolume, 4.32 + 3.92. In 21 paired determinations in sinusrhythm the average per cent variations from the mean ofthe pair + standard deviation were as follows: heart rate,
659
THOMAS KILLIP AND RALPH A. BAER
'000 V'Q -0 000 aUoei - C1 ("c0- I m
inf)0 t-=0 t- 00 m '000 mIc% 0% 00 0 (O00 00> 0
0000000000Q0000000000co0000O
~ "14 ) CIT CT CIT"I \4 '4' cN4cM
bC O DO0OOC
00000 o0o 00 00t-00 0\00 el'I) cl0% '0ll 'Or""
r"I- 4o'0% e14 00 - t 0 0%
t-C4 tsl--t mP m C\ "jo0\ u
I
000N 0Or"- to In - C\ 0% 0 C)
-o " oo n- \--4-- - tt 0_IIC (N 0' '000 C")0l
eq t- s o Ft C"oo on C
o0 0%ot- \ 000 0%C\
-00 Ch CN 0 00o ti 0%
" l)0110%*")0 V 1100 t
CNcm 14C1 mm C14 OoNm m
r4 - -4 -- -
00
44>C10N0 d1 00 It C\bo
td4) 00tU
*~~~~~
O0O C- NC4~om9 r0e me000%N 00 C4 0 C,4 " -4 -
m1cq 400 t"-0 C(r""t"-t-OO O 000 00t" 0%00 0%O C00
000000o0000O00l _I Cl _- 4_- - _I -_I
0 0 00 0 000dqoo toc r0- 00oo oo0 0oo00 00
U0Ceot C'v0 O4dmCl0% r-
00000 4 - CN CN _I _ 0"') t- 00C C~l cICl t"-.tk- 0%0
coo0 o0% co Cooo ooW41f) t- 00 0000 o00 Lo!) )'\0
000c Q0e \014 ti)' NO m Or-\"0 -1Ul t0 0 0% Cl 0% " " 00
cli cliv! 5e) cie3 l l
-.4 oo0 0\ I- tnU" oc
" 00 00 -4 '0Cl ClVt '- o
m o i 0\ cO 'I m 00Nof
0#) !)0i0 Cl -0o E)00
ooo4 on4 cI en eo0s
Cls# -- Cl0%t-0%~ONeq'0 0t-_1NC e M! nl Clq '0-- -- q-- "-4 -4 "-- T-C6 un cl) V)<9 (n
I- 0 '1)00 U1) t-
0o-00 --0-s000'000 "0
000 00000 00
00 00000 o0000)o000
t_O O O a 0t
U1)m- Cl 00 \0c"; v- CIT" s_
- --- ---\u, -.1
'000 U)" W4"U) '00 '0) ) '0>- i \'0
00' 00e bl) 0%eU
QCoo£ ) AoOr 2%0
00% 000 0%00 0 0
Cl \-4\0 CN 00C) 0%00- 0'0 00"W) 00- 0-
Z ) \!) C \ C\ ! en
c00 0% c!) e6C-e40
0'lo0-0- I4 C!
-o -_ - c-- -
00 -.4 C) Co00iI-
d14140Om0 114 114C00\0 0 0cq .- _ _s
¢T ¢z¢c u
5?
00 -C 00 0%.~~~~ot-*-t-
> ° i g
- U m v H U o
*-C
_cis >s
_ ce ,_
660
.S,-a
At
1-4 0 ?.4
'4Cb
c)
*e 0
o °~
"S
04)
0
co~
4C 4
-4)
a X._ 14
co
"0
cC X
PU
to
4)O~X
Uo X
*
._
C!) C\0% 0%
00
O) o
0%\ 00
o) O
000
00
c -
cl'0
C_
-s C
0000
U 0s
U)0
u) U)0% -
d-
.4 -
- Cl
C _
0%")
d.01.'C.
4i)
04)J
C,).0
q.9
Cd
*
HEMODYNAMICS OF ELECTRICAL REVERSION FROM ATRIAL FIBRILLATION
---- --
(Cl4C1')'0 000C tN-%, 0% C'01- 000 00
0C0 O0 00000ts0 000 0
400 00 0000000 00 00
-0m 0 C0 00 tl
0 CN C
'000% CI4 1\ Cl) (= ) CE)00C\ 00 00 0000% 0\0 0 00
'00 (N' C 000'-
14" --' 00 in- '0\-. \00
No --e - - - -
min'0\% 0%00
C14q
'000 t1- 0% 00 Nm 0M)1'Cl CE) (N 1')
---- - --
<U) VCl <CI) <C/)
ee e. T. .: ~~14~ . P<cn <Ncn-~C)<
\0' 01--\ 000 Cl4 1')0 Clo0 0O CNlO -:tM -)md
000 "t') C\ t-.C (I0C1C000%t- oo oOoo00 %O0 00C '
00000000000000000000 0000co8 CO CC) co com CC>
_q _~_Z _; _- _ _ _
_; _- _l _l
C) C) o N0000OC0000000000000000000000MONC0\0C1' U)00 00 OCE_l _. _; _; Z_- _;_4
0'04_ r1 I-0 0'0I_t 4\Nc
' 0'0o x '0- 0%'0 000%
C)C)\0 <Cl)r C\2C) <Cf
-td- CA ONCr 0\ 0 081 t- m\0:In 0d10 \ V- N0 00 CP
cq \ ou-d'\ om-X c14 0-o Nt\0 C7%\o cqm MOo \ot
C' c,4 e6 c'i C4 c'i e;c, e-3,
ooqd Cu) oo \0 I- 0\ X
C- cl C- cl 114C ci cli cl cli_
oCN 0oom00C4C \t to
O \ 00 00S:0\ +m ne
__l _4 _,- _,- r
<u) <: ¢uz <uu u
0
00 cis a , I-4.0-
-4.
-. L.. 4*
- cl. . .
w 4) H H un u
O
ei 0) (DI 0 -I 00 C1 e-
O- 0 0Cn4 e-4- - - -
In 00 t- \0 00 0 eq c00\ 0\ 00 00 00 00 C\ C\
too00000000 000000000o0 0u) 0o0 0 0 in 00 Od0 0vC -4O C U)_ 0 m 00 00c
(N - - N _
000000000000000000 go c'o 00 O0o 0
C0 0co t- 0\0 CO dC eCSm 000 OI
e 4 - - Ci - - 4 -
- 00ui in0 '00 \0oo00M -M ).tt\0d O (N00 000
If) '0 \0 \0 ' 0\%
0 00O 0% 0%C 00 0 00
I-.. d' 004 4 Cl Ln 0 t- O
'0 '0 ' 0 '0 \0 LO o '0\
N c 6 c c d C; e-i 6Ci6C0biC
k-t)-- 0%0 0\ 0 mm \d'000 t- - -'0-6.-.-~.-i.-*i....6
\00 10 eo 00 0% M q C1'
> 4 ~)rf) 0%t e1 U) \6 r' _1)(- cq (N C\ in0 M M MO c4)0 m eq0 00qCN
00 -tZ ooo6 sH d\ \
|0e roa s OrN4m It --(o eq -
CIN e Cl c CZ Cd C1 c
4) 4 V) V)0/\4 V) V C/ f UVH*: .H .i .~*i.H4 -H
)ooo N mvoa oo N>
1 0 0 +_U._
661
.Vbr^
l3
V 06
4)
4) 4
U) N
4)
.0
U U)
4)
4)
E4)
:$ N
4)
4)
4)
N IU
U 4)
3U
0 ij
Cl)
m
14
Clv
v
V
0.06
o
V
o0
to*
V
++
0
0
6
V
C/)c0. -4¢ x4
.0 0
-o 0
U4)
THOMAS KILLIP AND RALPH A. BAER
1.73 ± 4.19; cardiac output, 2.70 ± 2.77; and stroke vol-ume, 3.28 + 3.50.Measurements were made with subjects at rest and
during exercise. The exercise was a standardized bi-cvcling motion of the legs at a rate of 60 to 70 per min-ute performed while the patient was supine. The rateand the range of leg excursion were kept constant. Ve-nous and arterial pressure, heart rate, oxygen consump-tion, and cardiac output were obtained between the thirdand fifth minutes of exercise. The arterial pressure andelectrocardiogram were monitored for 10 minutes afterexercise, and a final indicator-dilution curve was ob-tained at that time.On the second day 24 hours after the control study,
reversion to sinus rhythm was attempted with synchro-nized DC precordial shock on patients under light thio-pental anesthesia, according to techniques previously de-scribed (11).On the third day, 24 hours after attempted reversion
and 48 hours after the first evaluation, the hemodynamicstudies were repeated exactly as on the first day.
Results
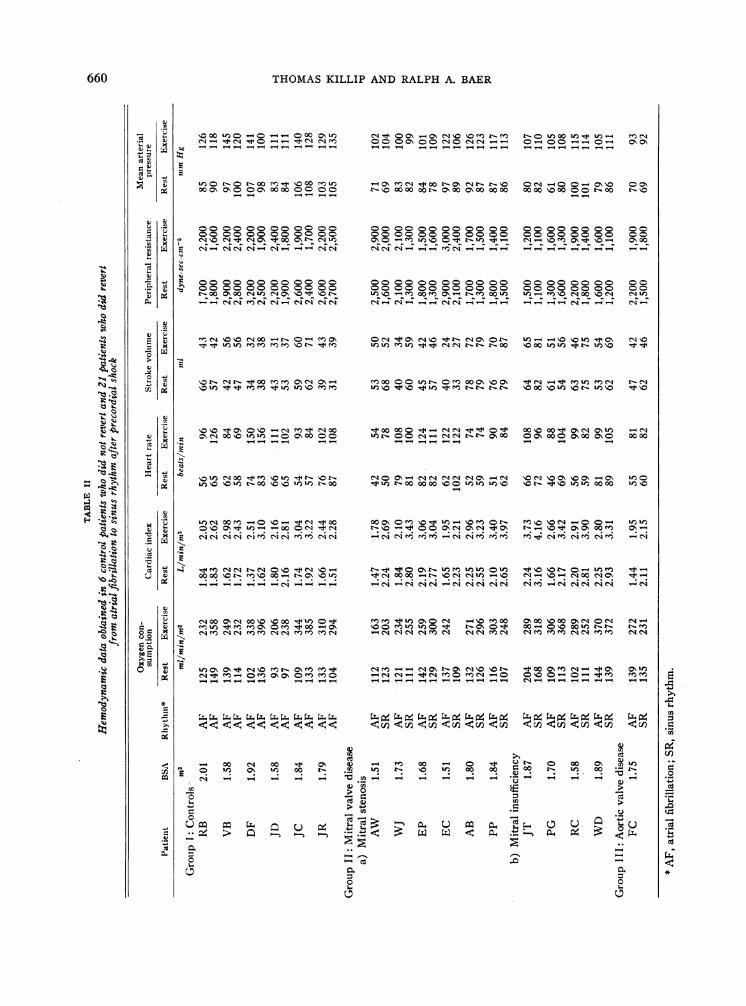
Hemodynamic data obtained in 27 patients atrest and during exercise before and after attemptedDC reversion to sinus rhythm are presented inTable II.
3.0PI
-J
X 2.00
~I.O0
REST |EXERCISECONT ROL
Rcst
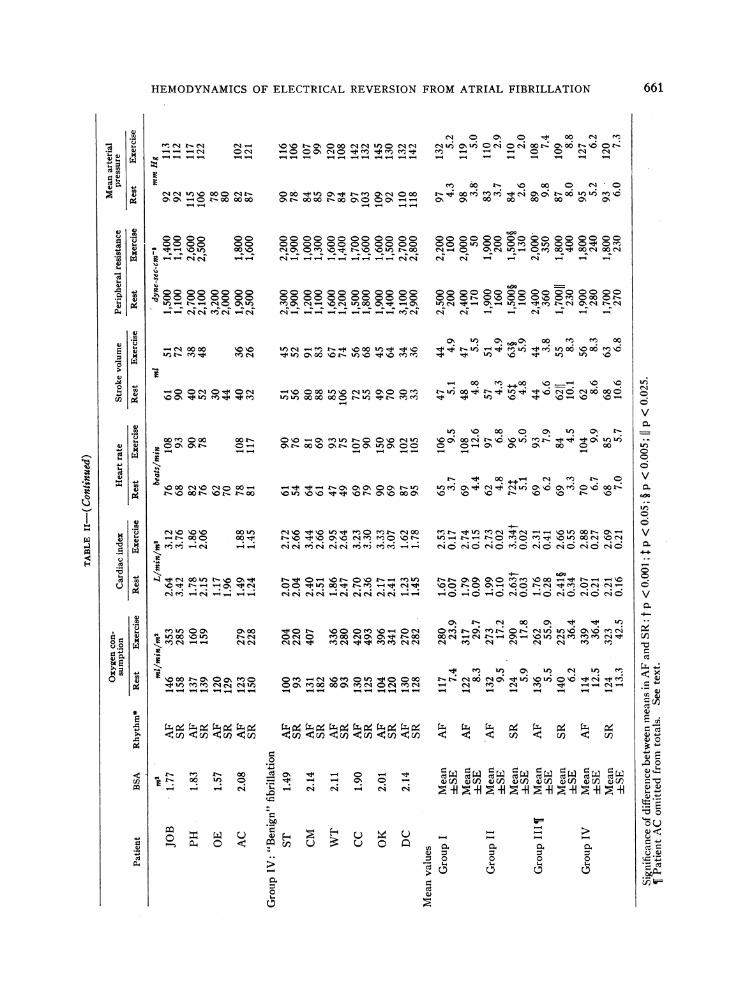
Group I. Control. The average age of the sixpatients in this group was 43 years, and the aver-age duration of atrial fibrillation Iwas more than 5years (Table I). There wnhere no significantchanges in any hemodynamic variables measuredbefore and after attempted reversion. Cardiac out-put averaged 7%S/ greater during the second study(Figure 1).Group II. Mitral stenosis (and mitral insuffi-
cicncy. Since the data for the patients wvith domi-nant mitral stenosis or insufficiency showed simi-lar trends, they are analyzed as a single group often patients. The average age tor the group was44 years, and atrial fibrillation had been presentfrom 1 month to 8 years (Table I).
Heart rate was greater after reversion in all butone patient. The mean heart rate in atrial fibril-lation was 62 beats per minute and increased to 72beats per minute in sinus rhythm (p < 0.025).AMean oxygen consumption was not significantlydifferent in the two studies, averaginig 132 ml per
p < .001
REST IEXERCISEMITRAL DISEASE
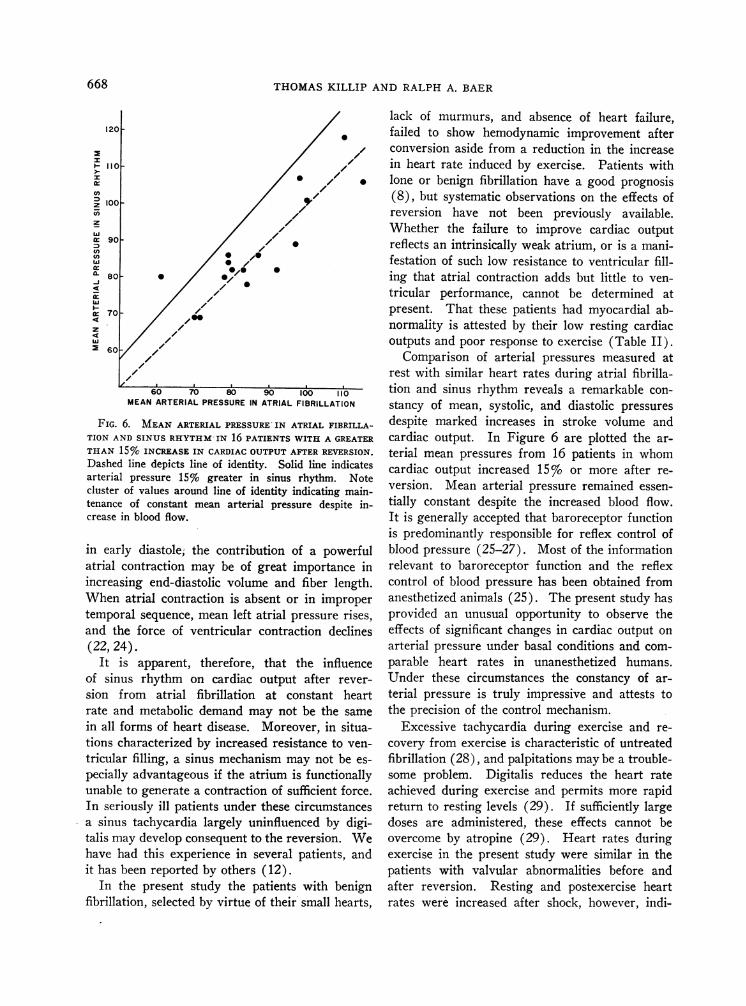
FIG. 1. EFFECT OF PRECORDIAL SHOCK AND REVERSION FRO-M ATRIAXI FIBRILLATION ( AF) TO
SINUS RHTYThIMA\ (SR) ON CARDIAC INDEX AT REST AND DURING EXERCISE. Control patients(left) who did not revert had Do significant changes in cardiac index at rest and during exer-
cise after precordial shock. In patients with mitral valve disease (middle) cardiac index in-creased 32%c (p <0.001) at rest and 22% (p <0.001) during exercise after reversion. In "be-
nign" fibrillators (right) cardiac index did not change significantly after reversion.
662
HEMODYNAMICS OF ELECTRICAL REVERSION FROM ATRIAL FIBRILLATION
minute per m2 before and 124 ml per minute per
m1 after reversion.The resting cardiac index was greater in all
patients after reversion. The mean cardiac indexduring atrial fibrillation for the group was 1.99 Lper minute per m2 and increased to 2.63 L per min-ute per m2 in sinus rhythm (p < 0.001). The in-crease ranged from 13%o to 52%o and averaged32% (Figure 1). The average increase in pa-
tients with dominant mitral stenosis was 32%; inthose with dominant mitral insufficiency it was
33%.Mean stroke volume increased from 57 ml per
beat to 65 ml per beat (p < 0.05) after reversiondespite the concomitant increase in heart rate.Arterial pressure remained remarkably constant.Calculated peripheral vascular resistance variedinversely with the cardiac output, falling in eachcase in sinus rhythm (p < 0.005) as cardiac out-put rose.
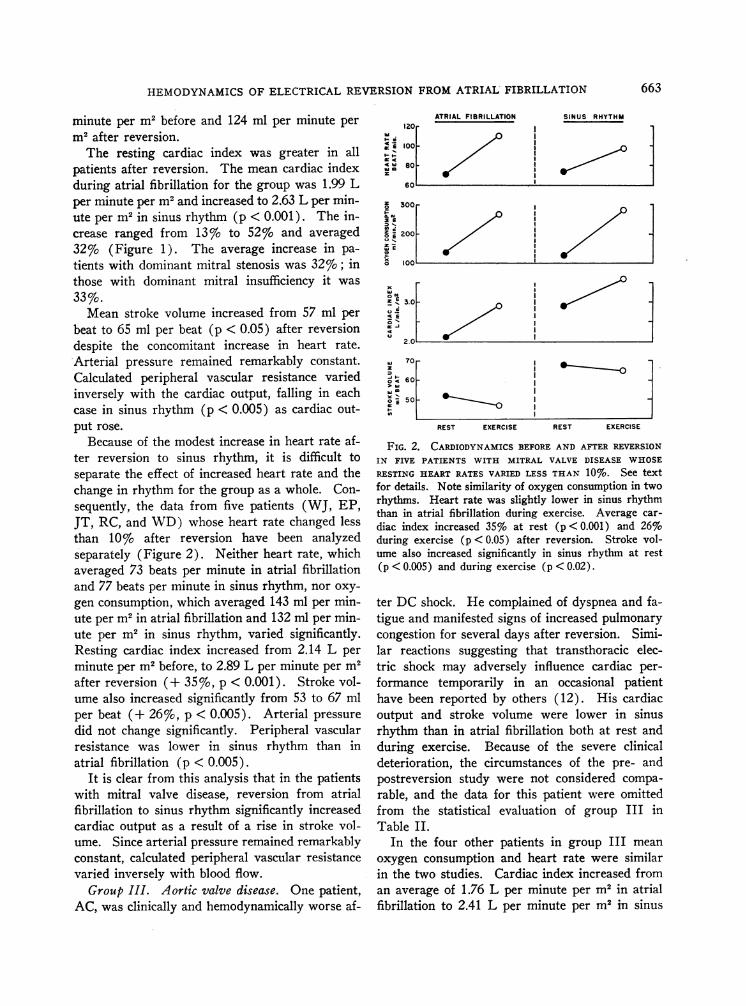
Because of the modest increase in heart rate af-ter reversion to sinus rhythm, it is difficult toseparate the effect of increased heart rate and thechange in rhythm for the group as a whole. Con-sequently, the data from five patients (WJ, EP,JT, RC, and WD) whose heart rate changed lessthan 10% after reversion have been analyzedseparately (Figure 2). Neither heart rate, whichaveraged 73 beats per minute in atrial fibrillationand 77 beats per minute in sinus rhythm, nor oxy-
gen consumption, which averaged 143 ml per min-ute per m2 in atrial fibrillation and 132 ml per min-ute per m2 in sinus rhythm, varied significantly.Resting cardiac index increased from 2.14 L per
minute per m2 before, to 2.89 L per minute per m2after reversion (+ 35%, p < 0.001). Stroke vol-ume also increased significantly from 53 to 67 mlper beat (+ 26%, p < 0.005). Arterial pressure
did not change significantly. Peripheral vascularresistance was lower in sinus rhythm than inatrial fibrillation (p < 0.005).
It is clear from this analysis that in the patientswith mitral valve disease, reversion from atrialfibrillation to sinus rhythm significantly increasedcardiac output as a result of a rise in stroke vol-ume. Since arterial pressure remained remarkablyconstant, calculated peripheral vascular resistancevaried inversely with blood flow.
Group III. Aortic valve disease. One patient,AC, was clinically and hemodynamically worse af-
4.
4
W:
120
100
80
z 300 _
2
200_
E
X) ^.
x
CZ tz E
e< Ei
la 70
' F 60
° E 50
ATRIAL FIBRILLATION SINUS RHYTHM
REST EXERCISE REST EXERCISE
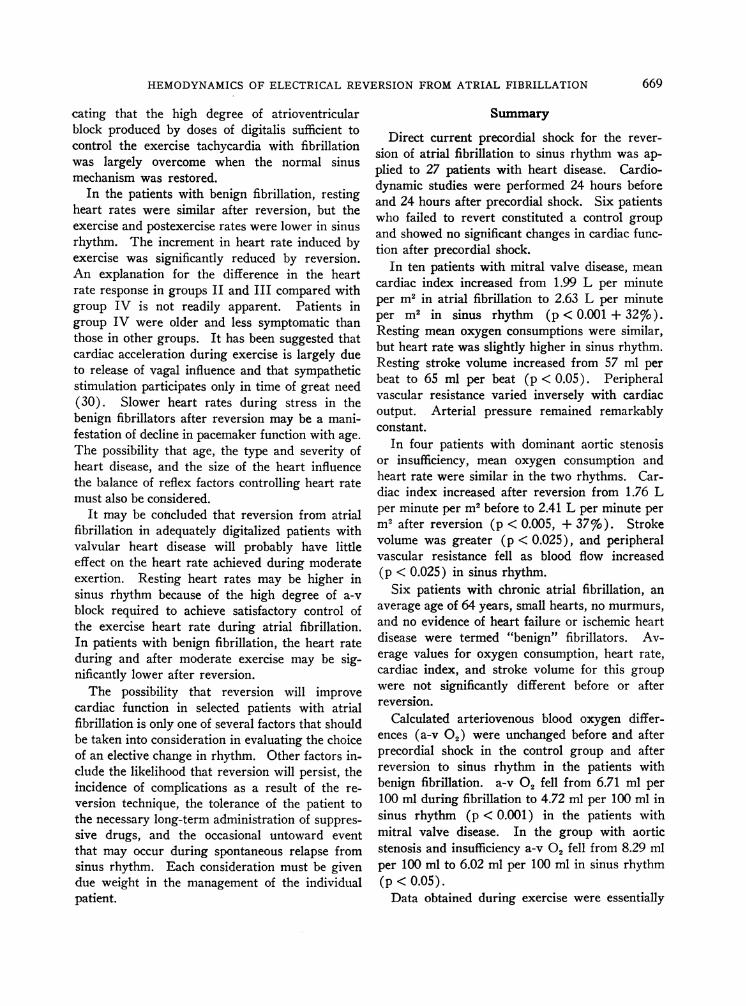
FIG. 2. CARDIODYNAMICS BEFORE AND AFTER REVERSION
IN FIVE PATIENTS WITH MITRAL VALVE DISEASE WHOSE
RESTING HEART RATES VARIED LESS THAN 10%0. See textfor details. Note similarity of oxygen consumption in tworhythms. Heart rate was slightly lower in sinus rhythmthan in atrial fibrillation during exercise. Average car-
diac index increased 35% at rest (p <0.001) and 26%during exercise (p < 0.05) after reversion. Stroke vol-ume also increased significantly in sinus rhythm at rest(p < 0.005) and during exercise (p < 0.02).
ter DC shock. He complained of dyspnea and fa-tigue and manifested signs of increased pulmonarycongestion for several days after reversion. Simi-lar reactions suggesting that transthoracic elec-tric shock may adversely influence cardiac per-
formance temporarily in an occasional patienthave been reported by others (12). His cardiacoutput and stroke volume were lower in sinusrhythm than in atrial fibrillation both at rest andduring exercise. Because of the severe clinicaldeterioration, the circumstances of the pre- andpostreversion study were not considered compa-
rable, and the data for this patient were omittedfrom the statistical evaluation of group III inTable II.
In the four other patients in group III mean
oxygen consumption and heart rate were similarin the two studies. Cardiac index increased froman average of 1.76 L per minute per m2 in atrialfibrillation to 2.41 L per minute per m2 in sinus
.0 - I
2.0
663
a
THOMAS KILLIP AND RALPH A. BAER
rhythm (37%o, p < 0.005). Mean stroke volumeincreased from 44 to 62 ml per beat (p < 0.025).Mean arterial pressure was essentially unchanged,and the calculated peripheral vascular resistancefell (p < 0.025).We concluded that in patients with symptomatic
aortic valve abnormalities, reversion from atrialfibrillation to sinus rhythm is associated with sig-nificant increase in cardiac output and stroke vol-ume.
Group IV. Benign' atrial fibrillation. The av-erage age in this group was 64 years. The dura-tion of fibrillation varied from 6 months to morethan 10 years (and in one patient was possibly aslong as 23 years) (Table I).
Average values for oxygen consumption, heartrate, cardiac index, and stroke volume were notsignificantly different in the two studies. In twopatients an increase in cardiac index greater thanencountered in group I was observed. In WTcardiac output increased 33% and stroke volume25%, whereas heart rate and oxygen consumptiondid not change. In patient DC oxygen consump-tion was unchanged, but heart rate increased from87 to 95 beats per minute, and cardiac ouput in-creased 18%o, whereas stroke volume increased10%o. Mean cardiac index for the group was 2.07
10.0
zwC)
Q
cc
wa.U,uJ
2-i0
0oil
L per minute in atrial fibrillation and 2.21 L perminute in sinus rhythm (+ 7%, Figure 1).
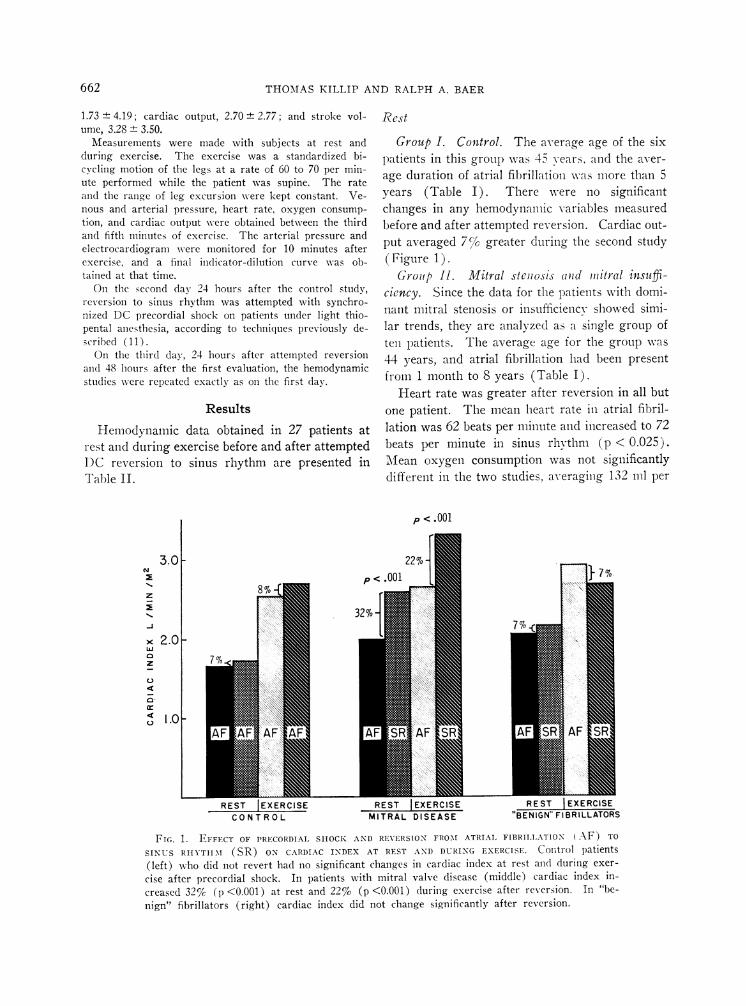
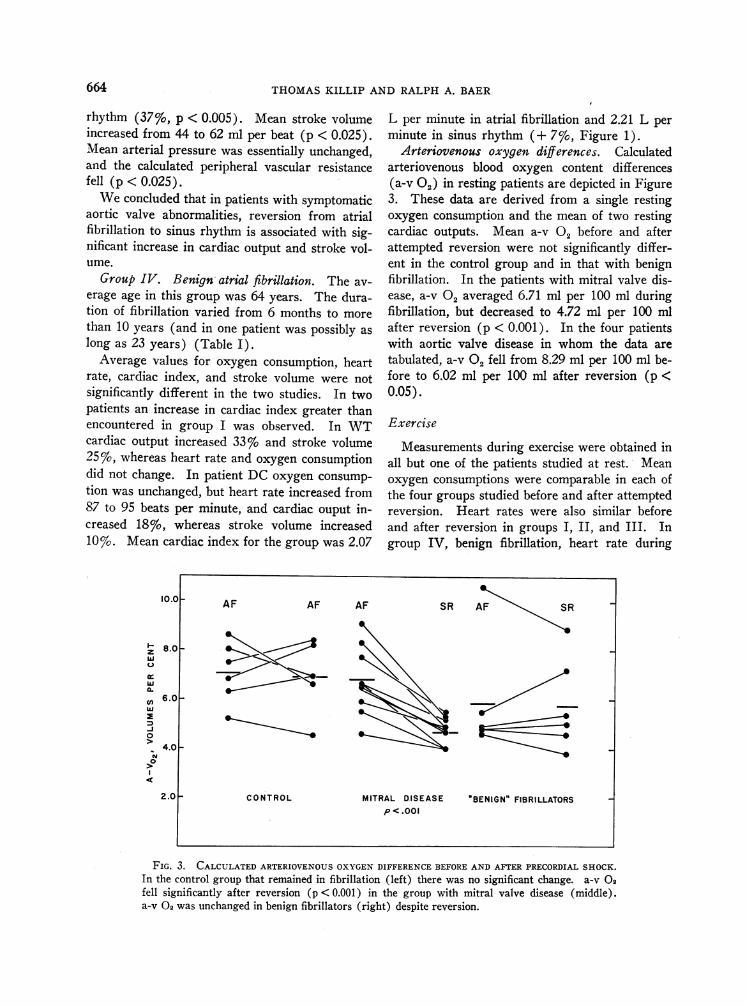
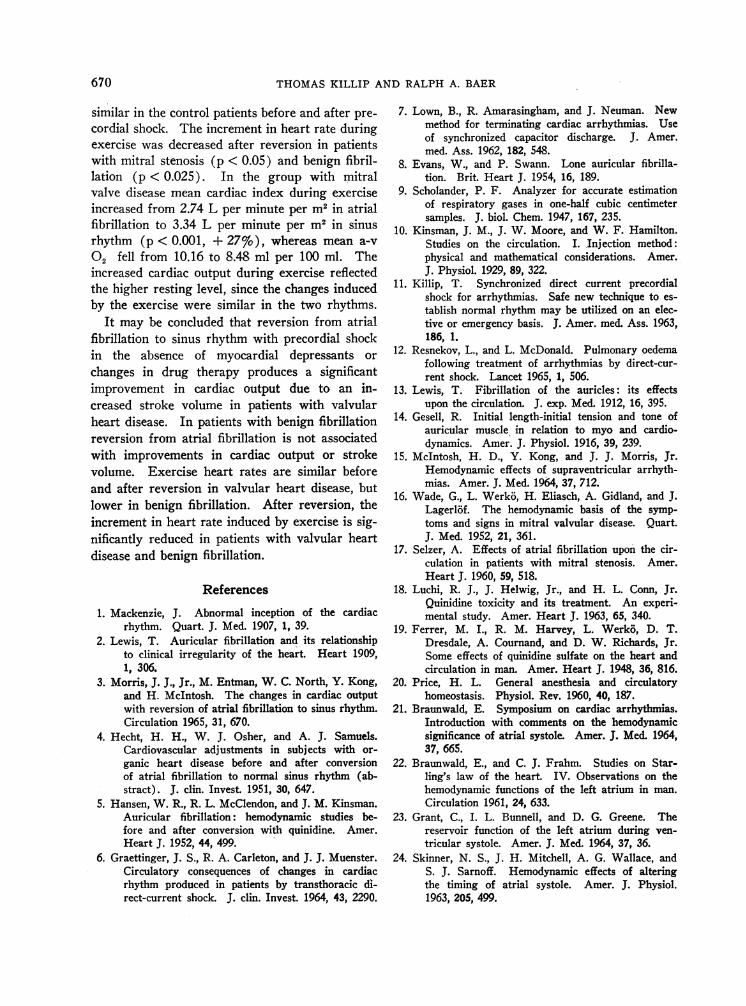
Arteriovenous oxygen differences. Calculatedarteriovenous blood oxygen content differences(a-v 02) in resting patients are depicted in Figure3. These data are derived from a single restingoxygen consumption and the mean of two restingcardiac outputs. Mean a-v 02 before and afterattempted reversion were not significantly differ-ent in the control group and in that with benignfibrillation. In the patients with mitral valve dis-ease, a-v 02 averaged 6.71 ml per 100 ml duringfibrillation, but decreased to 4.72 ml per 100 mlafter reversion (p < 0.001). In the four patientswith aortic valve disease in whom the data aretabulated, a-v 02 fell from 8.29 ml per 100 ml be-fore to 6.02 ml per 100 ml after reversion (p <0.05).
Exercise
Measurements during exercise were obtained inall but one of the patients studied at rest. Meanoxygen consumptions were comparable in each ofthe four groups studied before and after attemptedreversion. Heart rates were also similar beforeand after reversion in groups I, II, and III. Ingroup IV, benign fibrillation, heart rate during
SR AF SR
_'S
8.01-
6.0_
4.0 -
MITRAL DISEASEp <.001
BENIGN" FIBRILLATORS
FIG. 3. CALCULATED ARTERIOVENOUS OXYGEN DIFFERENCE BEFORE AND AFTER PRECORDIAL SHOCK.In the control group that remained in fibrillation (left) there was no significant change. a-v 02fell significantly after reversion (p < 0.001) in the group with mitral valve disease (middle).a-v 02 was unchanged in benign fibrillators (right) despite reversion.
664
-AF AF AF
0 ,
2-.0 _ CONTROL
HEMODYNAMICS OF ELECTRICAL REVERSION FROM ATRIAL FIBRILLATION
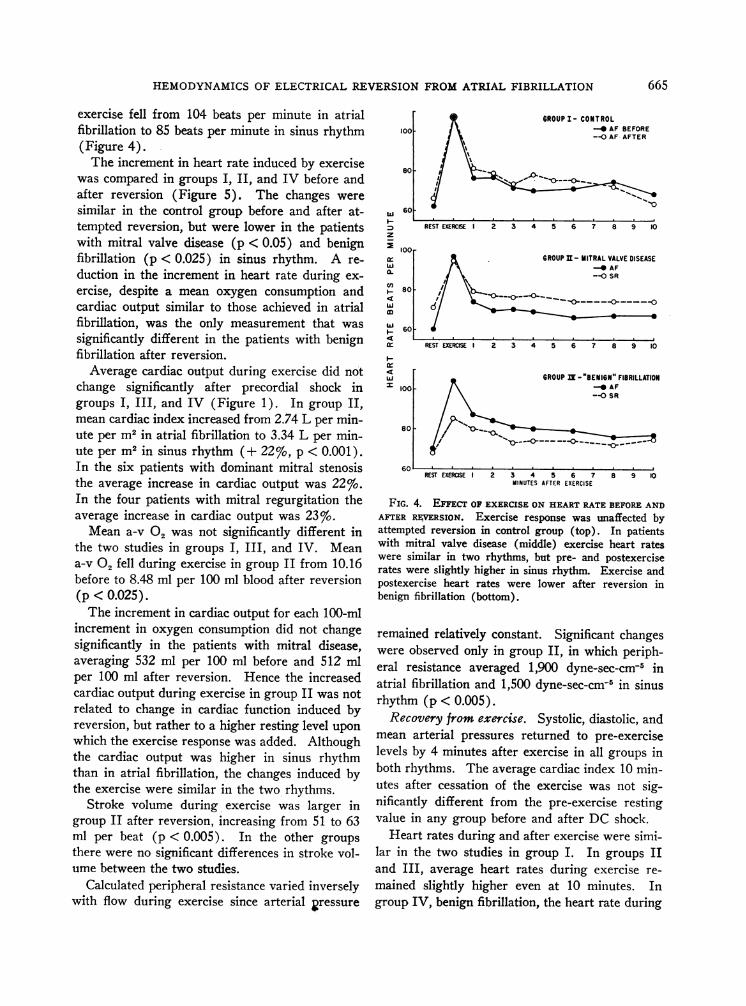
exercise fell from 104 beats per minute in atrialfibrillation to 85 beats per minute in sinus rhythm(Figure 4).The increment in heart rate induced by exercise
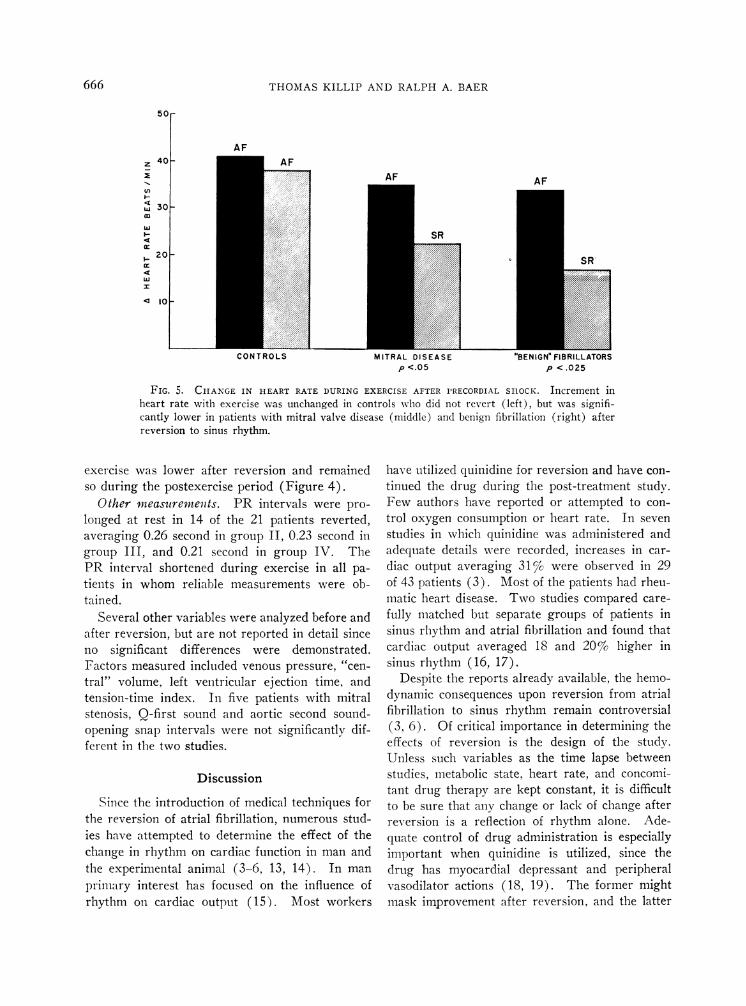
was compared in groups I, II, and IV before andafter reversion (Figure 5). The changes weresimilar in the control group before and after at-tempted reversion, but were lower in the patientswith mitral valve disease (p < 0.05) and benignfibrillation (p < 0.025) in sinus rhythm. A re-duction in the increment in heart rate during ex-ercise, despite a mean oxygen consumption andcardiac output similar to those achieved in atrialfibrillation, was the only measurement that wassignificantly different in the patients with benignfibrillation after reversion.Average cardiac output during exercise did not
change significantly after precordial shock ingroups I, III, and IV (Figure 1). In group II,mean cardiac index increased from 2.74 L per min-ute per m2 in atrial fibrillation to 3.34 L per min-ute per m2 in sinus rhythm (+ 22%, p < 0.001).In the six patients with dominant mitral stenosisthe average increase in cardiac output was 22%.In the four patients with mitral regurgitation theaverage increase in cardiac output was 23%.Mean a-v 02 was not significantly different in
the two studies in groups I, III, and IV. Meana-v 02 fell during exercise in group II from 10.16before to 8.48 ml per 100 ml blood after reversion(p <0.025).The increment in cardiac output for each 100-ml
increment in oxygen consumption did not changesignificantly in the patients with mitral disease,averaging 532 ml per 100 ml before and 512 mlper 100 ml after reversion. Hence the increasedcardiac output during exercise in group II was notrelated to change in cardiac function induced byreversion, but rather to a higher resting level uponwhich the exercise response was added. Althoughthe cardiac output was higher in sinus rhythmthan in atrial fibrillation, the changes induced bythe exercise were similar in the two rhythms.
Stroke volume during exercise was larger ingroup II after reversion, increasing from 51 to 63ml per beat (p < 0.005). In the other groupsthere were no significant differences in stroke vol-ume between the two studies.
Calculated peripheral resistance varied inverselywith flow during exercise since arterial 2ressure
w
z
ir
CII(n
w
4
Ir-4
=Id
100
80
60
GROUP I- CONTROL-_ AF BEFORE--OAF AFTER
REST EXERCISE I 2 3 4 5 6 7 8 9 10
100-GROUP I - MITRAL VALVE DISEASE
- AF-0SR
80 0 0
60 -
REST EXERCISE I 2 3 4 5 6 7 8 9 10
GROUP N -"BENIGN" FIBRILLATION100 - -O AF
--0 SR
80so- =
60REST EXERCISEI 2 3 4 5 6 7 8 9 10
MINUTES AFTER EXERCISE
FIG. 4. EFFECT OF EXERCISE ON HEART RATE BEFORE ANDAFTER RAVERSION. Exercise response was unaffected byattempted reversion in control group (top). In patientswith mitral valve disease (middle) exercise heart rateswere similar in two rhythms, but pre- and postexerciserates were slightly higher in sinus rhythm. Exercise andpostexercise heart rates were lower after reversion inbenign fibrillation (bottom).
remained relatively constant. Significant changeswere observed only in group II, in which periph-eral resistance averaged 1,900 dyne-sec-cm-5 inatrial fibrillation and 1,500 dyne-sec-cm-8 in sinusrhythm (p < 0.005).Recovery from exercise. Systolic, diastolic, and
mean arterial pressures returned to pre-exerciselevels by 4 minutes after exercise in all groups inboth rhythms. The average cardiac index 10 min-utes after cessation of the exercise was not sig-nificantly different from the pre-exercise restingvalue in any group before and after DC shock.
Heart rates during and after exercise were simi-lar in the two studies in group I. In groups IIand III, average heart rates during exercise re-mained slightly higher even at 10 minutes. Ingroup IV, benign fibrillation, the heart rate during
665
THOMAS KILLIP AND RALPH A. BAER
MlIIKAML U5LMA5Lp <.05
pCtIUN <l.02LL5 IUK5
P <.025
FIG. 5. CHANGE IN HEART RATE DURING EXERCISE AFTER PRECORDIAL SHOCK. Increment inheart rate with exercise was unchanged in controls who did not revert (left), but was signifi-cantly lower in patients with mitral valve disease (middle) and benign fibrillation (right) afterreversion to sinus rhythm.
exercise was lower after reversion and remainedso during the postexercise period (Figure 4).
Other measuremeits. PR intervals were pro-
longed at rest in 14 of the 21 patients reverted,averaging 0.26 second in group II, 0.23 second ingroup III, and 0.21 second in group IV. ThePR interval shortened during exercise in all pa-
tients in whom reliable measurements were ob-tained.
Several other variables were analyzed before andafter reversion, but are not reported in detail sinceno significant differences were demonstrated.Factors measured included venous pressure, "cen-tral" volume, left ventricular ejection time, andtension-time index. In five patients with mitralstenosis, Q-first sound and aortic second sound-opening snap intervals were not significantly dif-ferent in the two studies.
Discussion
Since the introduction of medical techniques forthe reversion of atrial fibrillation, numerous stud-ies have attempted to determine the effect of thechange in rhythm on cardiac function in man andthe experimental animal (3-6, 13, 14). In man
primary interest has focused on the influence ofrhythm on cardiac output (15). Most workers
have utilized quinidine for reversion and have con-
tinued the drug during the post-treatment study.Few authors have reported or attempted to con-
trol oxygen consumption or heart rate. In seven
studies in which quinidine was administered andadequate details were recorded, increases in car-
diac output averaging 31% were observed in 29of 43 patients (3). Most of the patients had rheu-matic heart disease. Two studies compared care-
fully matched but separate groups of patients insinus rhythm and atrial fibrillation and found thatcardiac output averaged 18 and 20% higher insinus rhythm (16, 17).
Despite the reports already available, the hemo-dynamic consequences upon reversion from atrialfibrillation to sinus rhythm remain controversial(3, 6). Of critical importance in determining theeffects of reversion is the design of the study.Unless such variables as the time lapse betweenstudies, metabolic state, heart rate, and concomi-tant drug therapy are kept constant, it is difficultto be sure that any change or lack of change afterreversion is a reflection of rhythm alone. Ade-quate control of drug administration is especiallyimportant when quinidine is utilized, since thedrug has myocardial depressant and peripheralvasodilator actions (18, 19). The former mightmask improvement after reversion, and the latter
AF40H
20h
z
US
Cl)
w
w
wx
666
5OF
30F
10~
HEMODYNAMICS OF ELECTRICAL REVERSION FROM ATRIAL FIBRILLATION
might enhance ventricular function under certaincircumstances.The present study was designed to control as
many variables as possible. No antiarrhythmicdrugs were administered. Digitalis was maintainedat constant dosage, and resting ventricular ratesduring atrial fibrillation were well controlled. Pre-cordial shock was utilized for conversion and wasapplied with barbiturate analgesia 24 hours afterthe first study and 24 hours before the secondstudy. The effects of the reversion and the influ-ences of repeated studies on the hemodynamicfunctions measured were analyzed in a controlgroup of patients who remained in atrial fibrilla-tion despite precordial shock.We conclude from the present data that rever-
sion to sinus rhythm from atrial fibrillation en-hances stroke volume and therefore cardiac outputat rest in patients with mitral or aortic valve dis-ease. Although the outputs are higher during ex-ercise after reversion, the increment induced by!exercise remains relatively fixed in the tworhythms.Our data may be compared with the results re-
ported by Graettinger, Carleton, and Muenster(6) and Morris and co-workers (3) in which DCshock was also used for reversion. Graettingerstudied 16 patients of whom 10 had rheumaticheart disease. Premedication consisted of barbi-turates and meperidine. The postconversion datawere obtained 1 and 2 hours after patients hadawakened from thiopental anesthesia. No changein oxygen consumption occurred, but heart ratedecreased significantly, falling more than 15 beatsper minute in 6 patients at rest. Small increasesin cardiac output and decreases in a-v O2 wereobserved, but since similar changes occurred in 4patients who did not revert and also in a controlgroup of 14 patients with chronic heart diseasesubjected to repeated studies, the authors con-cluded that reversion had little effect on cardiacfunction unless the ventricular rate fell sharply.Neither the type of heart disease, the rhythm, northe sedation, if any, was described for the 14"control" patients.
Morris studied 12 patients just before and 2hours after DC shock (3). Six had rheumaticheart disease with mitral valve abnormalities. Nomedications other than the anesthesia for the shockwere employed. An increase in cardiac output,
predominantly a reflection of stroke volume, oc-curred in 7 of 11 patients at rest and in all 5 pa-tients exercised.The design of the present study is such that it is
unlikely that the techniques of cardiac reversionor anesthesia significantly influenced the results.In the study of Graettinger and associates, how-ever, because of the short time interval betweenstudy and therapy and the rapid ventricular ratesin many of the patients, factors other than thechange in rhythm may have played a significantrole, including sedation, precordial shock, changesin heart rate, and anesthesia. Thiopental may in-fluence cardiac function, and the effect may lastseveral hours (20). The effects of DC shock onmyocardial function in man are insufficientlyunderstood. Ventricular arrhythmias, atrioven-tricular dissociation, and transient ST segmentelevations may be due in part to direct effects ofthe shock, although digitalis has been implicated.Although serum glutamic oxalacetic transaminasedoes not increase significantly after DC shock(11), the possibility that some degree of myo-cardial injury occurs is not ruled out.
Another consideration is the effect of sustainedventricular arrhythmia on cardiac function (15).Recovery from ventricular or supraventriculartachycardias may not be immediate after a pre-cordial shock. Conceivably, long-established atrialfibrillation may adversely affect atrial functionwith slow recovery after reversion. Atrial wavesof small amplitude have been observed immediatelyafter electric reversion (6, 21). They may re-flect intrinsic myocardial abnormality or the effectof anesthesia and shock or be a functional conse-quence of a long-standing arrhythmia. Serial ob-servations on atrial function after DC shock wouldbe of considerable interest.The atrial pulse pressure and presumably the
force of atrial contraction may be greater thannormal in patients with left ventricular and mitralvalve disease (22, 23). It is probable that thecontribution of atrial contraction to the subse-quent stroke output will depend to a considerableextent upon the impedance to ventricular filling.If there is little diastolic resistance, inflow willoccur predominantly in the first portion of dias-tole, and atrial contraction may be expected toadd but little. If the ventricle or the mitral valveoffers significant resistance to ventricular filling
667
THOMAS KILLIP AND RALPH A. BAER
110 _
/- //M 100 /a)~~~~~~~U,9ZIQ
//,W~~~~~~~~
/
290 /
a 68070
I-
~70
260
60 70 90 100 110
MEAN ARTERIAL PRESSURE IN ATRIAL FIBRILLATION
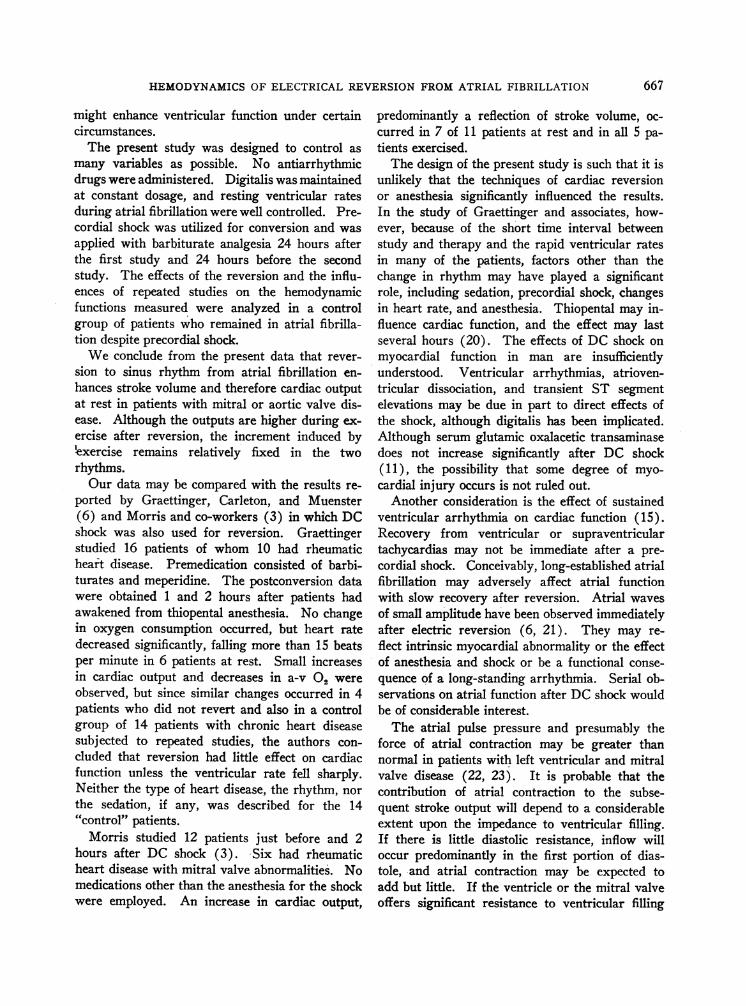
FIG. 6. MEAN ARTERIAL PRESSURE IN ATRIAL FIBRILLA-TION AND SINUS RHYTHM IN 16 PATIENTS WITH A GREATERTHAN 15%6 INCREASE IN CARDIAC OUTPUT AFTER REVERSION.Dashed line depicts line of identity. Solid line indicatesarterial pressure 15% greater in sinus rhythm. Notecluster of values around line of identity indicating main-tenance of constant mean arterial pressure despite in-crease in blood flow.
in early diastole, the contribution of a powerfulatrial contraction may be of great importance inincreasing end-diastolic volume and fiber length.When atrial contraction is absent or in impropertemporal sequence, mean left atrial pressure rises,and the force of ventricular contraction declines(22, 24).
It is apparent, therefore, that the influenceof sinus rhythm on cardiac output after rever-
sion from atrial fibrillation at constant heartrate and metabolic demand may not be the samein all forms of heart disease. Moreover, in situa-tions characterized by increased resistance to ven-
tricular filling, a sinus mechanism may not be es-
pecially advantageous if the atrium is functionallyunable to generate a contraction of sufficient force.In seriously ill patients under these circumstancesa sinus tachycardia largely uninfluenced by digi-talis may develop consequent to the reversion. Wehave had this experience in several patients, andit has been reported by others (12).
In the present study the patients with benignfibrillation, selected by virtue of their small hearts,
lack of murmurs, and absence of heart failure,failed to show hemodynamic improvement afterconversion aside from a reduction in the increasein heart rate induced by exercise. Patients withlone or benign fibrillation have a good prognosis(8), but systematic observations on the effects ofreversion have not been previously available.Whether the failure to improve cardiac outputreflects an intrinsically weak atrium, or is a mani-festation of such low resistance to ventricular fill-ing that atrial contraction adds but little to ven-tricular performance, cannot be determined atpresent. That these patients had myocardial ab-normality is attested by their low resting cardiacoutputs and poor response to exercise (Table II).
Comparison of arterial pressures measured atrest with similar heart rates during atrial fibrilla-tion and sinus rhythm reveals a remarkable con-stancy of mean, systolic, and diastolic pressuresdespite marked increases in stroke volume andcardiac output. In Figure 6 are plotted the ar-terial mean pressures from 16 patients in whomcardiac output increased 15% or more after re-version. Mean arterial pressure remained essen-tially constant despite the increased blood flow.It is generally accepted that baroreceptor functionis predominantly responsible for reflex control ofblood pressure (25-27). Most of the informationrelevant to baroreceptor function and the reflexcontrol of blood pressure has been obtained fromanesthetized animals (25). The present study hasprovided an unusual opportunity to observe theeffects of significant changes in cardiac output onarterial pressure under basal conditions and com-parable heart rates in unanesthetized humans.Under these circumstances the constancy of ar-terial pressure is truly impressive and attests tothe precision of the control mechanism.
Excessive tachycardia during exercise and re-covery from exercise is characteristic of untreatedfibrillation (28), and palpitations may be a trouble-some problem. Digitalis reduces the heart rateachieved during exercise and permits more rapidreturn to resting levels (29). If sufficiently largedoses are administered, these effects cannot beovercome by atropine (29). Heart rates duringexercise in the present study were similar in thepatients with valvular abnormalities before andafter reversion. Resting and postexercise heartrates were increased after shock, however, indi-
668
HEMODYNAMICS OF ELECTRICAL REVERSION FROM ATRIAL FIBRILLATION
cating that the high degree of atrioventricularblock produced by doses of digitalis sufficient tocontrol the exercise tachycardia with fibrillationwas largely overcome when the normal sinusmechanism was restored.
In the patients with benign fibrillation, restingheart rates were similar after reversion, but theexercise and postexercise rates were lower in sinusrhythm. The increment in heart rate induced byexercise was significantly reduced by reversion.An explanation for the difference in the heartrate response in groups II and III compared withgroup IV is not readily apparent. Patients ingroup IV were older and less symptomatic thanthose in other groups. It has been suggested thatcardiac acceleration during exercise is largely dueto release of vagal influence and that sympatheticstimulation participates only in time of great need(30). Slower heart rates during stress in thebenign fibrillators after reversion may be a mani-festation of decline in pacemaker function with age.The possibility that age, the type and severity ofheart disease, and the size of the heart influencethe balance of reflex factors controlling heart ratemust also be considered.
It may be concluded that reversion from atrialfibrillation in adequately digitalized patients withvalvular heart disease will probably have littleeffect on the heart rate achieved during moderateexertion. Resting heart rates may be higher insinus rhythm because of the high degree of a-vblock required to achieve satisfactory control ofthe exercise heart rate during atrial fibrillation.In patients with benign fibrillation, the heart rateduring and after moderate exercise may be sig-nificantly lower after reversion.The possibility that reversion will improve
cardiac function in selected patients with atrialfibrillation is only one of several factors that shouldbe taken into consideration in evaluating the choiceof an elective change in rhythm. Other factors in-clude the likelihood that reversion will persist, theincidence of complications as a result of the re-version technique, the tolerance of the patient tothe necessary long-term administration of suppres-sive drugs, and the occasional untoward eventthat may occur during spontaneous relapse fromsinus rhythm. Each consideration must be givendue weight in the management of the individualpatient.
Summary
Direct current precordial shock for the rever-sion of atrial fibrillation to sinus rhythm was ap-plied to 27 patients with heart disease. Cardio-dynamic studies were performed 24 hours beforeand 24 hours after precordial shock. Six patientswho failed to revert constituted a control groupand showed no significant changes in cardiac func-tion after precordial shock.
In ten patients with mitral valve disease, meancardiac index increased from 1.99 L per minuteper m2 in atrial fibrillation to 2.63 L per minuteper m2 in sinus rhythm (p < 0.001 + 32%).Resting mean oxygen consumptions were similar,but heart rate was slightly higher in sinus rhythm.Resting stroke volume increased from 57 ml perbeat to 65 ml per beat (p < 0.05). Peripheralvascular resistance varied inversely with cardiacoutput. Arterial pressure remained remarkablyconstant.
In four patients with dominant aortic stenosisor insufficiency, mean oxygen consumption andheart rate were similar in the two rhythms. Car-diac index increased after reversion from 1.76 Lper minute per m2 before to 2.41 L per minute perm2 after reversion (p < 0.005, + 37%o). Strokevolume was greater (p < 0.025), and peripheralvascular resistance fell as blood flow increased(p < 0.025) in sinus rhythm.Six patients with chronic atrial fibrillation, an
average age of 64 years, small hearts, no murmurs,and no evidence of heart failure or ischemic heartdisease were termed "benign" fibrillators. Av-erage values for oxygen consumption, heart rate,cardiac index, and stroke volume for this groupwere not significantly different before or afterreversion.
Calculated arteriovenous blood oxygen differ-ences (a-v 02) were unchanged before and afterprecordial shock in the control group and afterreversion to sinus rhythm in the patients withbenign fibrillation. a-v 02 fell from 6.71 ml per100 ml during fibrillation to 4.72 ml per 100 ml insinus rhythm (p < 0.001) in the patients withmitral valve disease. In the group with aorticstenosis and insufficiency a-v °2 fell from 8.29 mlper 100 ml to 6.02 ml per 100 ml in sinus rhythm(p < 0.05).Data obtained during exercise were essentially
669
THOMAS KILLIP AND RALPH A. BAER
similar in the control patients before and after pre-cordial shock. The increment in heart rate duringexercise was decreased after reversion in patientswith mitral stenosis (p < 0.05) and benign fibril-lation (p < 0.025). In the group with mitralvalve disease mean cardiac index during exerciseincreased from 2.74 L per minute per m2 in atrialfibrillation to 3.34 L per minute per m2 in sinusrhythm (p < 0.001, + 27%o), whereas mean a-v02 fell from 10.16 to 8.48 ml per 100 ml. Theincreased cardiac output during exercise reflectedthe higher resting level, since the changes inducedby the exercise were similar in the two rhythms.
It may be concluded that reversion from atrialfibrillation to sinus rhythm with precordial shockin the absence of myocardial depressants orchanges in drug therapy produces a significantimprovement in cardiac output due to an in-creased stroke volume in patients with valvularheart disease. In patients with benign fibrillationreversion from atrial fibrillation is not associatedwith improvements in cardiac output or strokevolume. Exercise heart rates are similar beforeand after reversion in valvular heart disease, butlower in benign fibrillation. After reversion, theincrement in heart rate induced by exercise is sig-nificantly reduced in patients with valvular heartdisease and benign fibrillation.
References
1. Mackenzie, J. Abnormal inception of the cardiacrhythm. Quart. J. Med. 1907, 1, 39.
2. Lewis, T. Auricular fibrillation and its relationshipto clinical irregularity of the heart. Heart 1909,1, 306.
3. Morris, J. J., Jr., M. Entman, W. C. North, Y. Kong,and H. McIntosh. The changes in cardiac outputwith reversion of atrial fibrillation to sinus rhythm.Circulation 1965, 31, 670.
4. Hecht, H. H., W. J. Osher, and A. J. Samuels.Cardiovascular adjustments in subjects with or-ganic heart disease before and after conversionof atrial fibrillation to normal sinus rhythm (ab-stract). J. clin. Invest. 1951, 30, 647.
5. Hansen, W. R., R. L. McClendon, and J. M. Kinsman.Auricular fibrillation: hemodynamic studies be-fore and after conversion with quinidine. Amer.Heart J. 1952, 44, 499.
6. Graettinger, J. S., R. A. Carleton, and J. J. Muenster.Circulatory consequences of changes in cardiacrhythm produced in patients by transthoracic di-rect-current shock. J. clin. Invest. 1964, 43, 2290.
7. Lown, B., R. Amarasingham, and J. Neuman. Newmethod for terminating cardiac arrhythmias. Useof synchronized capacitor discharge. J. Amer.med. Ass. 1962, 182, 548.
8. Evans, W., and P. Swann. Lone auricular fibrilla-tion. Brit. Heart J. 1954, 16, 189.
9. Scholander, P. F. Analyzer for accurate estimationof respiratory gases in one-half cubic centimetersamples. J. biol. Chem. 1947, 167, 235.
10. Kinsman, J. M., J. W. Moore, and W. F. Hamilton.Studies on the circulation. I. Injection method:physical and mathematical considerations. Amer.J. Physiol. 1929, 89, 322.
11. Killip, T. Synchronized direct current precordialshock for arrhythmias. Safe new technique to es-tablish normal rhythm may be utilized on an elec-tive or emergency basis. J. Amer. med. Ass. 1963,186, 1.
12. Resnekov, L., and L. McDonald. Pulmonary oedemafollowing treatment of arrhythmias by direct-cur-rent shock. Lancet 1965, 1, 506.
13. Lewis, T. Fibrillation of the auricles: its effectsupon the circulation. J. exp. Med. 1912, 16, 395.
14. Gesell, R. Initial length-initial tension and tone ofauricular muscle, in relation to myo and cardio-dynamics. Amer. J. Physiol. 1916, 39, 239.
15. McIntosh, H. D., Y. Kong, and J. J. Morris, Jr.Hemodynamic effects of supraventricular arrhyth-mias. Amer. J. Med. 1964, 37, 712.
16. Wade, G., L. Werko, H. Eliasch, A. Gidland, and J.Lagerl6f. The hemodynamic basis of the symp-toms and signs in mitral valvular disease. Quart.J. Med. 1952, 21, 361.
17. Selzer, A. Effects of atrial fibrillation upon the cir-culation in patients with mitral stenosis. Amer.Heart J. 1960, 59, 518.
18. Luchi, R. J., J. Helwig, Jr., and H. L. Conn, Jr.Quinidine toxicity and its treatment. An experi-mental study. Amer. Heart J. 1963, 65, 340.
19. Ferrer, M. I., R. M. Harvey, L. Werko, D. T.Dresdale, A. Cournand, and D. W. Richards, Jr.Some effects of quinidine sulfate on the heart andcirculation in man. Amer. Heart J. 1948, 36, 816.
20. Price, H. L. General anesthesia and circulatoryhomeostasis. Physiol. Rev. 1960, 40, 187.
21. Braunwald, E. Symposium on cardiac arrhythmias.Introduction with comments on the hemodynamicsignificance of atrial systole. Amer. J. Med. 1964,37, 665.
22. Braunwald, E., and C. J. Frahm. Studies on Star-ling's law of the heart. IV. Observations on thehemodynamic functions of the left atrium in man.Circulation 1961, 24, 633.
23. Grant, C., I. L. Bunnell, and D. G. Greene. Thereservoir function of the left atrium during ven-tricular systole. Amer. J. Med. 1964, 37, 36.
24. Skinner, N. S., J. H. Mitchell, A. G. Wallace, andS. J. Sarnoff. Hemodynamic effects of alteringthe timing of atrial systole. Amer. J. Physiol.1963, 205, 499.
670
HEMODYNAMICS OF ELECTRICAL REVERSION FROM ATRIAL FIBRILLATION
25. Heymans, C., and E. Neil. Reflexogenic Areas ofthe Cardiovascular System. Boston, Little,Brown, 1958.
26. Ead, H. W., J. H. Green, and E. Neil. A compari-son of the effects of pulsatile and non-pulsatileblood flow through the carotid sinus on the reflexo-genic activity of the sinus baroceptors in the cat.J. Physiol. (Lond.) 1952, 118, 509.
27. Bronk, D. W., and G. Stella. Afferent impulses inthe carotid sinus nerve. I. The relation of thedischarge from single end organs to arterial bloodpressure. J. cell. comp. Physiol. 1932, 1, 113.
28. Blumgart, H. The reaction to exercise of the heartaffected by auricular fibrillation. Heart 1924, 11,49.
29. Modell, W., H. Gold, and H. H. Rothendler. The useof digitalis to prevent exaggerated acceleration ofthe heart during physical exercise in patients withauricular fibrillation. J. Amer. med. Ass. 1941,116, 2241.
30. Gasser, H. S., and W. J. Meek. A study of themechanisms by which muscular exercise producesacceleration of the heart. Amer. J. Physiol. 1914,34, 48.
SPECIAL NOTICE TO SUBSCRIBERS
The Post Office will not forward the Journal when you move.Please send your new address, including the zip code, to TheJournal of Clinical Investigation, Business Office, 10 StoughtonStreet, Boston, Mass. 02118.
671





























