Embed Size (px)
Citation preview

7/28/2019 Heartbeat Classification
http://slidepdf.com/reader/full/heartbeat-classification 1/10
Available online at www.sciencedirect.com
Medical Engineering & Physics 30 (2008) 248–257
Assessment and comparison of different methodsfor heartbeat classification
I. Jekova a,∗, G. Bortolan b, I. Christov a
a Centre of Biomedical Engineering, Bulgarian Academy of Sciences, Sofia, Bulgariab Institute of Biomedical Engineering ISIB, CNR, Padova, Italy
Received 5 May 2006; received in revised form 5 February 2007; accepted 7 February 2007
Abstract
The most common way to diagnose cardiac dysfunctions is the ECG signal analysis, usually starting with the assessment of the QRScomplex as the most significant wave in the electrocardiogram. Many methods for automatic heartbeats classification have been applied and
reported in the literature but the use of different ECG features and the training and testing on different datasets, makes their direct comparison
questionable. This paper presents a comparative study of the learning capacity and the classification abilities of four classification methods –
K th nearest neighbour rule, neural networks, discriminant analysis and fuzzy logic. They were applied on 26 morphological parameters, which
include information of amplitude, area, interval durations and the QRS vector in a VCG plane and were tested for five types of ventricular
complexes – normal heart beats, premature ventricular contractions, left and right bundled branch blocks, and paced beats.
One global, one basic and two local learning sets were used. A small-sized learning set, containing the five types of QRS complexes
collected from all patients in the MIT-BIH database, was used either with or without applying the leave one out rule, thus representing the
global and the basic learning set, respectively. The local learning sets consisted of heartbeats only from the tested patient, which were taken
either consecutively or randomly.
Using the local learning sets the assessed methods achieved high accuracies, while the small size of the basic learning set was balanced by
reduced classification ability. Expectedly, the worst results were obtained with the global learning set.
© 2007 IPEM. Published by Elsevier Ltd. All rights reserved.
Keywords: Automatic heartbeat classification; K th nearest neighbour rule; Neural networks; Discriminant analysis; Fuzzy logic
1. Introduction
The most common way to study and diagnose cardiac dys-
functions is the ECG signal analysis usually starting with
the assessment of the QRS complex as the most significant
wave in the electrocardiogram. The normal ventricular com-
plexes (N) are provoked by the sinus node and are related
with regular conduction path through the ventricles, whichassures their normal narrow waveform. The existence of
ectopic centers, as well as, some blocked regions in the
ventricles, changes the path of propagation of the activa-
tion front and leads to generation of QRS complexes with
wide and bizarre waveforms related to premature ventric-
∗ Corresponding author at: Acad. G. Bonchev Str. bl. 105, 1113 Sofia,
Bulgaria. Tel.: +359 2 979 3631; fax: +359 2 723787.
E-mail address: [email protected] (I. Jekova).
ular contractions (PVC) and left and right bundle branch
blocks (LBBB, RBBB). Another type of ventricular com-
plexes, which feature with a particular QRS behavior are the
heartbeatsprovoked by pacemaker – the so-called paced beats
(PB). The automatic detection and classification of ventric-
ular beats considerably facilitates the analyses of long-term
ECG Holter recordings. Therefore, the accuracy of the auto-
matic heartbeat classification software is of great importancefor the precise cardiac dysfunctions diagnosis. It depends on
three basic factors – the used heartbeat feature set, the applied
classification method and the organization of the training
strategy.
Recently, a study compared the adequacy of morphologi-
cal and time-frequency ECG descriptors for classification of
the QRS complexes in five heartbeat classes [1]. An attempt
to estimate the influence of the applied classifier and the used
learning set on the classification accuracy was performed in
1350-4533/$ – see front matter © 2007 IPEM. Published by Elsevier Ltd. All rights reserved.
doi:10.1016/j.medengphy.2007.02.003

7/28/2019 Heartbeat Classification
http://slidepdf.com/reader/full/heartbeat-classification 2/10
I. Jekova et al. / Medical Engineering & Physics 30 (20 08) 248–257 249
[2], but it is limited only forN andPVC heart beats.Moreover,
one of the learning strategies in the latter work is applicable
only in the context of discrimination between N and PVC
complexes, since it relies on generation of artificial PVCs,
and cannot be applied for LBBB, RBBB and PB.
The literature contains information about various classi-
fication rules, including linear discriminators [3,4], neuralnetworks [5–8], fuzzy adaptive resonance theory mapping
[9], self-organized maps [10], operation on vectors in the
multidimensional space [11,12], etc. The selection of an
appropriate classification rule depends greatly on the specific
application, in sense of the particularities of the estimated
ECG descriptors, available computational resources and
eventual real-time operation.
Taking into account the wide variations in the heart-
beat waveforms among the individual patients, some authors
[1–3,12,13] are paying attention to the organization of the
classifiers’ learning dataset, considering two main train-
ing strategies: global learning set (built from a large ECG
database) and local learning set (when it is customized tothe tested patient). The global learning set is preferable in
many commercial applications, which avoid the need for
time-consuming human expert annotations, associated with
manual editing of patient-specific ECG records. However,
the cited authors reported significant improvement in case of
a patient-adaptable local learning set. In this sense, specific
strategies are adopted for local learning in some arrhythmia
monitors, for example in intensive care rooms, where only
the normal or predominant beats are annotated/identified by
the cardiologist, and any irregular heartbeats, like premature
ventricular contractions, are classified automatically on the
basis of pattern differenceswith theannotated beats.It is obvi-ous that the size of the local learning set must be restricted
in terms of convenience, but there is not agreement in the
literature about its optimal size.
Manymethods for automatic heartbeatsclassificationhave
been applied and reported in the literature. However, the use
of different ECG feature sets, as well as, the training and
testing on different datasets, makes their direct comparison
questionable. In this paper, we present a comparative study of
the classification abilities of four classification methods—the
K th nearest neighbour classification rule (Knn), neural net-
works (NN),discriminant analysis (DA) and fuzzylogic (FL).
They were applied on the large collection of morphological
QRS descriptors used by Christov and Bortolan [5]. We have
tested the performance of the above-defined four classifica-
tion methods for five heartbeat classes, which feature with
particular QRS behavior (N, PVC, LBBB, RBBB and PB),
as well as in dependence of the content and the size of the
learning set.
2. Materials and methods
2.1. ECG signals
The study involved all 48 ECG recordings from the MIT-
BIH arrhythmia database. Each recording has a duration of
30 min and includes two leads—the modified limb lead II
and one of the modified leads V1, V2, V4 or V5 [14]. The
sampling frequency is 360Hz and the resolution is 200 sam-
ples per mV. The heartbeats were recognized by the fiducial
points in the database and the original database annotations
were accepted. The study was focused on the classification of
the five largest heartbeat classes in the MIT-BIH arrhythmiadatabase: (i) normal beats (N) – about 74820 cases; (ii) pre-
mature ventricular contractions (PVC) – about 6970; (iii) left
bundle branch blocks (LBBB) – about 8050; (iv) right bundle
branch blocks (RBBB) – about 7220; (v) paced beats (PB) –
about 7000. Table 1 shows the distribution of this heartbeat
types among the ECG recordings. In our study, we analyzed
the N, PVC, LBBB, RBBB and PB in the full-length MIT-
BIH files, without selection based on the quality of the signal.
Thus the analysis was applied even in the presence of artifacts
or noise in the ECG signal, which could result in accuracy
reduction.
2.2. Preprocessing
The preprocessing filtration was taken from Christov and
Bortolan [5] and the following procedures are realized:
• a notch filter for elimination of the power-line interfer-
ence, implemented by moving averaging of samples in one
period of the interference;
• a low-pass filter for suppression of the tremor noise,
realized by moving averaging of samples in 30 ms time-
interval, thus having a first zero at about 35 Hz;
• a high-pass recursive filter for drift suppression [15] with
cut-off frequency of 2.2 Hz.
Table 1
Distribution of the N, PVC, LBBB, RBBB and PB heartbeats among the ECG recordings
Heartbeat type ECG recordings containing the respective heartbeat types
N 100–106, 108, 112–117, 119, 121–123, 200–203, 205, 208–210, 212, 213, 215, 217, 219–223, 228, 230, 231, 233, 234
PVC 100, 102, 104–109, 111, 114, 116, 118, 119, 121, 123, 124, 200–203, 205, 207–210, 213–215, 217, 219, 221, 223, 228,
230, 231, 233, 234
LBBB 109, 111, 207, 214
RBBB 118, 124, 207, 212, 231, 232
PB 102, 104, 107, 217

7/28/2019 Heartbeat Classification
http://slidepdf.com/reader/full/heartbeat-classification 3/10
250 I. Jekova et al. / Medical Engineering & Physics 30 (2008) 248–257
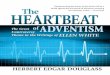
Fig.1. (a) Referencewaveformsfor thefive heartbeattypesunder classification(N, PVC,LBBB, RBBB, PB);(b andc) graphicalillustration of themorphological
descriptors extracted from ECG leads and VCG plane, respectively.
2.3. Morphological descriptors
The method for calculation of the large collection of mor-
phological descriptors was applied to all QRS complexes
annotated as N, PVC, LBBB, RBBB or PB in the MIT-
BIH arrhythmia database (see the reference waveforms in
Fig. 1a). An isoelectric, baseline segment is searched for
by starting from the QRS fiducial point back on the time
axis up to 120 ms. The segment is found if eight successive
differences between adjacent samples are less than a preset
value [16] and the difference between the end samples of
the segment is lower than the same value. The earliest sam-
ple of this segment is defined as an isoelectric point. The
QRS pattern recognition technique [16] identified the onset
and the offset of the QRS complex by simultaneous analysis
of the two ECG leads. Then a number of 26 morphological
descriptors representing information of the amplitude, area,
specific interval durationsand measurementsof theQRS vec-
tor in the vectorcardiographic(VCG) planewere calculated as
follows:
• Eleven descriptors were extracted by individual assess-
ment of each lead (their total number is 22 considering the
two leads):
(1) Pp: maximal amplitude of the positive peak.
(2) Pn: maximal amplitude of the negative peak.
(3) ArP: area of the positive samples in the identified
pattern.
(4) ArN: area of the negative samples in the identified
pattern.
(5) Ar: area of the QRS complex—the sum of the abso-
lute values of the ECG samples in the identified
pattern (Ar = ArP + ArN).
(6) Av: sum of the absolute values of the velocities in the
pattern interval.
(7) No: number of samples crossing a threshold of 70%
of the highest peak amplitude.
(8) Ima: time-interval from the QRS complex onset to
the maximal positive peak.
(9) Imi: time-interval from the QRS complex onset to
the maximal negative peak.
(10) S1: QRS slope velocity calculated for the time-
interval between the QRS complex onset and the first
peak.
(11) S2: QRS slope velocity calculated for the time-
interval between the first peak and the second peak.
• One descriptor representing the time-interval between the
onset and the offset of the ventricular contraction was
derived by the simultaneous leads analysis—Width.
• Three descriptors were calculated from the single-plane
VCG formed by the two leads:
• VCGamp: maximal amplitude of the VCG vector.
• VCGsin: sine component of the angle of the maximal
amplitude vector.
• VCGcos: cosine component of the angle of the maximal
amplitude vector.
Illustration of all morphological parameters is pre-
sented in Fig. 1b and c.
2.4. Classification methods
2.4.1. Kth nearest neighbour rule
This classification rule operates on vectors in a multi-
dimensional space [17,18]. In our case the heartbeats were
represented by 26-dimensional vector x = {Width, Pp1, Pn1,
Ar1, ArP1, ArN1, Av1, No1, Ima1, Imi1, S11, S21, Pp2, Pn2,
Ar2, ArP2, ArN2, Av2, No2, Ima2, Imi2, S12, S22, VCGam,
VCGsin, VCGcos}.
Initially, the reference set of the classification rule (called
learning set in our study) was formed to contain vectors of all

7/28/2019 Heartbeat Classification
http://slidepdf.com/reader/full/heartbeat-classification 4/10
I. Jekova et al. / Medical Engineering & Physics 30 (20 08) 248–257 251
analyzed heartbeat classes – N, PVC, LBBB, RBBB, and PB.
Each vector was previously labelled as belonging to one of
the five classes by the accompanying database annotations.
During the first iteration, clusters were formed by group-
ing together those beats that belong to the same class at an
Euclidean distance from each other smaller than 10% of the
range of each data dimension. Thus, a number of separateclusters for each class were formed in the multidimensional
space. During the next iterations, every remaining vector,
independently of its class, was assigned to the cluster whose
centroid had the closest Euclidean distance. The class label
of each cluster was defined by the class of the constituent
vectors. If a cluster contained vectors belonging to differ-
ent classes, it was called mixed cluster. The mixed clusters
accepted the class label of the dominant vectors, if there was
a dominance of at least three elements. Otherwise the clus-
ter was not considered. The distances between the centroids
of all possible couples of clusters were checked. When two
clusters labelled with the same class had closer Euclidean
distance than 30% of the range of each data dimension, theywere merged. If theadjacentcouples were of differentclasses,
the smaller was removed from the cluster list and its vec-
tors became ‘free’ (unclustered). During this process, the free
vectors were assigned to the existing clusters with the above
described procedures. All these iterations continued until the
mean cluster vectors remained unchanged or the number of
iterations exceeded a predefined value (200 iterations in our
case).
According to the K -nearest neighbours rule, a new vector
x (belonging to an unknown class) was classified on the basis
of the nearest mean vector. The distance between vector x
and the centroid of the jth cluster z j
was computed as theEuclidean distance:
d j =
ni=1
(xi−norm − zj i )
2,
where j is the cluster index, i the parameter index, and n is
number of the parameters used. Vector x was classified to the
class of the cluster z j at which d j had a minimum.
All parameters used in this equation must be previously
normalized with respect to the standard deviation, because
their different magnitudes or variances might cause unequal
weighting in the calculation of d j
with inappropriate effects.
The normalization was defined by
xi−norm =xi
(1/N r)N r
j =1(xj i − xi)
2
where N r is the number of all reference vectors and xi is the
mean value of the ith parameter.
2.4.2. Fuzzy logic
The method, which was applied for the classification of
QRS complexes, used a partition of the feature space in five
classes with a fuzzy clustering and a consequent fuzzy clas-
sification [19–22]. In this way a Sugeno-type fuzzy inference
system whose membership function parameters were tuned
using a fuzzy clustering with the least squares type method
was developed. In particular, a dynamic algorithm performed
the partition using decreasing rate of the influence of cluster
center (from 50% of the width of the input data space from
10%). Bell shape (Gaussian) membership functions had beenused. Every QRS complex had a membership value in the
five classes: N, PVC, LBBB, RBBB or PB. The tested QRS
was assigned to the class, with the corresponding maximal
membership function.
2.4.3. Linear discriminant analysis
Linear discriminant analysis (DA) is a classical statistical
approach for classifying samples of unknown classes, based
on training samples with known classes [3]. It is assumed that
the features have normal distributions,althoughthe violations
of the normality assumption are not fatal as long as non-
normality is caused by skewness and not by outliers [23].
For each of the below described learning sets the 26
morphological descriptors were subjected to standard linear
discriminant analysis. Equal a priori classification prob-
abilities were used for all heartbeat classes. All cases,
which produced outliers in the parameters distributions,
were excluded from analysis. The outliers were defined as
data points, which are out of the range of the mean value
±3× standard error. Thus, five linear discriminant functions
of the n-dimensional vector x were generated by the software
package Statistica and were used to differentiate between N,
PVC, LBBB, RBBB and PB beats:
F j
(x) =
w
j
i xi + aj
Here j changes between 1 and 5, i changes between 1 and
the number of the parameters (26 in our case), x i the ith
parameter, and wj i and a j are the discriminant coefficients
and constants, which are calculated to maximize the distance
between the means of the different classification groups. In
thetesting phase, thefive discriminant functions( j = 1, . . .,5),
were calculated for the assessed heart beat and it was labeled
as corresponding to the class, which has maximal value of F j.
2.4.4. Neural networks
From the 26 morphological descriptors, appropriate neu-ral network architecture was testedfor theclassification of the
five classes of QRS complexes [5–8,24–26]. Multiple feed-
forward neural networks were used and the back-propagation
learning phase with an approximation of a second-order algo-
rithm, based on Levenberg–Marquardt method, was applied
for improving the speed of convergence. One input layer ( X ),
one hidden layer with five nodes and one output layer with
five output nodes (corresponding to N, PVC, LBBB, RBBB
or PB) are used. The output vector (Y k ) can be expressed at
iteration k as
Y k = f (X,W k)

7/28/2019 Heartbeat Classification
http://slidepdf.com/reader/full/heartbeat-classification 5/10
252 I. Jekova et al. / Medical Engineering & Physics 30 (2008) 248–257
and the network weights are upgraded as follow:
W k+1 = W k − [J T J + μI ]−1J T e
where J is the Jacobian matrix with first derivatives of
the network errors (e) with respect to the weights and
μ is a dynamic parameter. A standard normalization pro-
cedure was performed on the input data and the mean
square error was used as error function. The NN train-
ing was terminated after a fixed number of iterations
(100).
The assessed heartbeat is labeled as belonging to the class
with the highest output component.
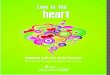
Fig. 2. Statistical assessment (mean value (·), ±standard error () and ±standard deviation (I)) of the morphological descriptors in groups defined by the
different heartbeat classes.

7/28/2019 Heartbeat Classification
http://slidepdf.com/reader/full/heartbeat-classification 6/10
Table 2
Sensitivity (Se), specificity (Sp), positive predictive value (PPV) and negative predictive value (NPV) obtained with the different classification methods. Learningeach patient record; L2 local, 33.3(3)% randomly selected QRS complexes of each patient record
Knn FL DA NN
Se (%) Sp (%) PPV (%) NPV (%) Se (%) Sp (%) PPV (%) NPV (%) Se (%) Sp (%) PPV (%) NPV (%)
Learning set G
N 87.19 81.52 92.31 71.43 87.33 80.61 91.98 71.43 83.97 90.79 95.87 68.99
PVC 68.83 83.64 23.55 97.34 78.79 84.99 27.76 98.21 57.56 88.99 27.67 96.63
LBBB 18.84 95.31 25.15 93.35 24.76 94.03 25.77 93.72 27.42 89.33 17.70 93.63
PB 2.14 99.32 18.54 93.37 18.47 99.52 73.32 94.42 48.24 99.63 90.30 96.39
RBBB 43.23 97.11 52.70 95.82 27.87 98.47 57.54 94.82 31.54 94.43 29.69 94.87
Learning set B
N 94.80 95.31 98.09 87.83 94.33 85.56 94.33 85.56 88.84 94.93 97.81 76.97
PVC 88.80 94.63 54.79 99.14 85.30 95.62 58.78 98.89 70.96 97.63 68.65 97.87
LBBB 58.10 98.32 74.36 96.56 64.26 96.97 63.93 97.01 85.56 91.16 44.76 98.69 PB 74.50 99.23 78.49 98.18 65.16 99.65 93.10 97.54 80.52 99.81 96.78 98.61
RBBB 88.50 98.23 78.86 99.13 75.93 99.39 90.24 98.23 81.38 98.19 76.28 98.66
Learning set L1
N 98.40 98.00 99.19 96.05 97.01 98.36 99.33 92.95 99.67 98.92 99.57 99.17
PVC 90.73 98.77 84.83 99.29 91.96 97.70 75.20 99.38 94.81 99.76 96.80 99.60
LBBB 99.98 100 99.95 100 100 99.91 98.95 100 100 100 99.97 100
PB 100 99.93 99.02 100 99.82 99.92 98.96 99.99 99.98 99.93 99.11 100
RBBB 100 99.98 99.70 100 99.12 99.99 99.84 99.94 99.92 99.98 99.74 100
Learning set L2
N 99.91 99.54 99.82 99.76 99.85 99.37 99.75 99.62 96.64 98.46 99.37 92.01
PVC 97.76 99.92 98.96 99.84 97.40 99.89 98.47 99.81 96.94 97.27 72.29 99.77
LBBB 99.98 99.98 99.81 100 99.91 99.97 99.69 99.99 99.98 99.98 99.81 100
PB 99.98 100 99.96 100 99.96 99.99 99.91 100 95.92 99.99 99.91 99.71
RBBB 99.96 99.99 99.90 100 99.65 99.99 99.88 99.97 98.45 100 99.94 99.88

7/28/2019 Heartbeat Classification
http://slidepdf.com/reader/full/heartbeat-classification 7/10
254 I. Jekova et al. / Medical Engineering & Physics 30 (2008) 248–257
2.5. Learning sets
The wide variations in the heartbeat waveforms among
the individual patients make the selection of the learning set
a critical choice. For this fact, two main training strategies are
considered: global learning set, independent from the tested
patient and built from a large ECG database, and the local
learning set, in case it is customized to the tested patient.
Consequently, in order to study the effects and the influ-
ence of the content and the size of the learning set on the
classification accuracy, we formed one global learning set,
and three local learning sets, defined as follows:
Fig. 3. Statistical indices (Se, Sp) estimated with the Knn, FL, DA and NN classification methods for the defined five heartbeat classes and four different
learning sets.

7/28/2019 Heartbeat Classification
http://slidepdf.com/reader/full/heartbeat-classification 8/10
I. Jekova et al. / Medical Engineering & Physics 30 (20 08) 248–257 255
(1) Global learning set (G): it contains five types of QRS
complexes collected from all patients in the MIT-BIH
database. From each record we selected 1 QRS complex
of each available type in the record. A total of 91 QRS
complexes were collected as a basic learning dataset. In
the training process, the leave one out rule (LOO) was
applied in order to achieve an independent learning fromthe tested patient (global learning). This means that in
the classification process of one ECG recording, only
heartbeats in G from the remaining 47 ECG recordings
were used.
(2) Basic learning set (B): it contains five types of QRS
complexes collected from all patients in the MIT-BIH
database. From each record we selected 1 QRS complex
of each available type in the record. Thus, 91 QRS com-
plexes were used as a basic learning dataset (it is similar
to G, but with no use of LOO rule).
(3) Local learning set (L1): it consists of the first 30% of the
selected record.
(4) Local learning set (L2): it consists of 33.3(3)% randomlyselected QRScomplexes from therecord. We shouldnote
that the heart beats were randomly selected once and
further used for training of all the four methods.
G may be considered in the strategy of global learning
sets, while the remaining sets B, L1 and L2 are local learning
sets.
3. Results
The statistical distributions of the morphological descrip-
tors for the different heartbeat classes are represented in
Fig. 2. In terms of space-saving, the parameters measured
for the two ECG leads are shown only for ECG Lead1.
The classification abilities of the four classification meth-
ods, applied on the morphological ECG descriptors are
estimated for the four learning sets described above by pro-
cessing all heartbeats from MIT-BIH arrhythmia database,
which were not used for learning and belong to the selected
heartbeat classes. Four statistical indices were calculated for
each heartbeat class i (i = N, PVC, LBBB, PB, RBBB): sensi-
tivity (Sei), specificity (Spi), positive predictive value (PPVi)
and negative predictive value (NPVi). They are computed
according to the following relations [27]:
Spi =TNi
TNi + FPi
, PPVi =TPi
TPi + FPi
,
NPVi =TNi
TNi + FNi
, Sei =TPi
TPi + FNi
TPi (true positives) is the number of heartbeats of the ith
class, which are correctly classified (e.g. N classified as N);
TNi (true negatives) is the number of heartbeats not belong-
ing to the ith class and not classified in the ith class (e.g.
PVC, LBBB, RBBB and PB not classified as N); FPi (false
positives) is the number of heartbeats classified erroneously
in the ith class (e.g. PVC, LBBB, RBBB and PB classified as
N); FNi (false negatives) is the number of heartbeats of class
i, classified in a different class (e.g. N not classified as N).
The results are listed in Table 2 and their graphical repre-
sentation is illustrated in Fig. 3.
4. Discussion and conclusion
The performances of Knn, FL, DA and NN, which were
applied for heartbeat classification in five classes, depend
on the used learning set. Fig. 3 illustrates the graphical
representations of the sensitivities and specificities for all
learning sets. The results obtained by training all methods
with the global learning set (G) were unreliable, especially
for PB processed with Knn (Se = 2.14%) and for LBBB
and RBBB processes with NN (Se = 5.13% and Se = 8.38%,
respectively). However, the low accuracies for these three
heartbeat types were prospective, since the MIT-BIH arrhyth-
mia database contains only four patients with PB, fourpatients with LBBB and five patients with RBBB, which are
quite insufficient for collection of a reliable global learning
set. All methods showed limited results with B, due to its
small size, and significantly better accuracies with L1 and
L2. The disadvantage of L1 and L2 is that they do not con-
tain all analyzed heartbeat types but only these, which are
typical for the ECG recording of the respective patient. Thus,
the classification methods do not have the possibility to rec-
ognize correctly heartbeats, which appear accidentally and
such ventricular complexes are fated to be classified wrongly
by default when using L1 or L2. The performances of Knn,
NN and FL methods are the best with L2. Generally the betterlearning capacity of L2 is dueto thefact that they comprise the
variations of morphology waveforms of the QRS complexes,
which appear in the ECG recording of one patient. Such kind
of learning sets may be obtained by random manual edit-
ing of the ECG recording. Since the DA method achieved
the best accuracy with the L1 learning set, it can be specu-
lated that the variations in the morphology parameters lead
to unstable discriminant functions and lower classification
accuracies.
Although a lot of studies dealing with heartbeat classifi-
cation are present in the literature, a strict comparison with
the results of the present work is difficult to perform, since
different heartbeat categories were used and different ECG
datasets were considered. Several studies are concerning
the discrimination between premature ventricular contrac-
tion (PVC) and Normal beats (N). For example Hamand Han
[9] obtained sensitivity and specificity in the classification
of PVC of 97% and 99% considering 6 MIT-BIH records,
whereas Moraes et al. [11] obtained 90.7 and 96.6% with 44
MIT-BIH records. However, aiming to set a bench mark for
the fiveheartbeat types considered in this study, we compared
our results with the clustering ability reported by Lagerholm
et al. [10], where they processed all 48 MIT-BIH recordings
for clustering ECG complexes using Hermit functions and

7/28/2019 Heartbeat Classification
http://slidepdf.com/reader/full/heartbeat-classification 9/10
256 I. Jekova et al. / Medical Engineering & Physics 30 (2008) 248–257
Table 3
Sensitivity (Se) and specificity (Sp) obtained by the four analysed classification methods (Knn, FL and NN with the local learning set L2 and DA with the local
learning set L1) compared to the statistical indices achieved by Lagerholm et al. [10]
Beat type Lagerholm et al. [10] Knn with L2 FL with L2 DA with L1 NN with L2
Se (%) Sp (%) Se (%) Sp (%) Se (%) Sp (%) Se (%) Sp (%) Se (%) Sp (%)
N 99.79 99 99.91 99.54 99.85 99.37 99.67 98.92 99.88 99.57
PVC 95.79 97.86 97.76 99.92 97.40 99.89 94.81 99.76 97.99 99.90LBBB 99.83 98.39 99.98 99.98 99.91 99.97 100 100 99.93 99.98
PB 98.97 97.69 99.98 100 99.96 99.99 99.98 99.93 99.96 100
RBBB 98.01 98.66 99.96 99.99 99.65 99.99 99.92 99.98 99.92 100
self-organizing maps. Some differences are present in the two
studies:
• In [10] a proper QRS detector was used, excluding from
analysis about 0.3% of the N, RBBB and PVC beats and
0.2% of the LBBB and PB beats while in the present study
the annotation of the MIT-BIH database was used, and all
heartbeats were analyzed.• In [10] all the ECG recordings were clustered in 15 classes
based on the dominant class, while in the present study a
learning setand a testing setwere used forthe classification
of 5 classes.
Although the problem of clustering is different from the
classification process, we computed the corresponding sen-
sitivity and specificity indices for the five considered classes
considering the clustering table in [10]. The results are
reported in Table 3, in comparison to the best results obtained
by the Knn, FL, DA and NN methods with the different
learning sets.
The performances of Knn, NN and FL trained with L2
for PVC, LBBB, RBBB and PB are better than the results
in [10] and the accuracies for N beats achieved in both stud-
ies are comparable. The Se value for PVC beats achieved
with DA (trained with L1) is lower than the reported in [10]
but it is balanced with higher Sp value. This may be due to
the large variety of bizarre PVC waveforms, which results
in relatively wide and skewed distributions of some of the
morphological parameters (see Fig. 2). For all other heart-
beat types the DA assures reliable results, comparable to or
higher than the reported in [10].
Theresults of the performed study could be used for selec-
tion of both the most suitable classification method and fordetermining the best strategy for learning set collection, tak-
ing into account the predefined requirements for heartbeat
classification.
Acknowledgments
This study was supported by a joint project between
the Italian National Research Council (ISIB-CNR) and the
Bulgarian Academy of Sciences (Center of Biomedical
Engineering-BAS).
References
[1] Christov I, Gomez-Herrero G, Krasteva V, Jekova I, Gotchev
A, Egiazarian K. Comparative study of morphological and time-
frequency ECG descriptors for heartbeat classification. Med Eng Phys
2006;28:876–87.
[2] Bortolan G, Jekova I, Christov I. Comparison of four methods for pre-
mature ventricular contractions and normal beats clustering. Comput
Cardiol 2005;32:921–4.
[3] Chazal P, O’Dwyer M, Reilly RB. Automatic classification of heart-
beats using ECG morphology and heartbeat interval features. IEEE
Trans Biomed Eng 2004;51:1196–206.
[4] Jekova I, Bortolan G, Christov I. Pattern recognition and optimal
parameter selection in premature ventricular contraction classification.
Comput Cardiology 2004;31:357–60.
[5] Christov I, Bortolan G. Ranking of pattern recognition parameters for
premature ventricular contraction classification by neural networks.
Physiol Meas 2004;25:1281–90.
[6] Gomez-Herrero G, GotchevA, ChristovI, EgiazarianK. Heartbeatclas-
sificationusing independent component analysisand matchingpursuits.
In: IEEE Int. Conf. Acoustics, Speech and Signal Processing, vol. 4.
Philadelphia, USA: ICASSP; 2005. p. 725–8.
[7] Al-Nashash H. Cardiacarrhythmia classificationusingneuralnetworks.
Technol Health Care 2000;8:363–72.[8] Maglaveras N, Stamkopoulos T,Diamantaras K, Pappas C, Strintzis M.
ECGpatternrecognitionand classificationusingnon-linear transforma-
tions andneuralnetworks: a review. IntJ MedInform1998;52:191–208.
[9] Ham FM, Han S. Classification of cardiac arrhythmias using fuzzy
ARTMAP. IEEE Trans Biomed Eng 1996;43(4):425–30.
[10] Lagerholm M, Peterson G, Braccini G, Edenbrandt L, Sornmo L. Clus-
tering ECGcomplexusingHermitefunctions andself-organizingmaps.
IEEE Trans Biomed Eng 2000;47(7):838–48.
[11] Moreas JCTB, Seixas MO, Vilani FN, Costa EV. A real time QRS
complex classification method using Mahalanobis distance. Comput
Cardiol 2002;29:201–4.
[12] Christov I, Jekova I, Bortolan G. Premature ventricular contrac-
tion classification by the K th nearest neighbours rule. Physiol Meas
2005;26:123–30.
[13] Hu YH,PalreddyS, TompkinsWJ. A patient-adaptable ECGbeat clas-sifier using a mixture of experts approach. IEEE Trans Biomed Eng
1997;44(9):891–900.
[14] Mark R, Moody G. MIT-BIH Arrhythmia database directory. Cam-
bridge: Massachusetts Institute of Technology; 1988.
[15] Daskalov IK, Dotsinsky IA, Christov I. Developments in ECG acquisi-
tion, preprocessing, parameter measurement and recording. IEEE Eng
Med Biol 1998;17:50–8.
[16] Daskalov IK, Christov I. Electrocardiogramsignal preprocessing
for automatic detection of QRS boundaries. Med Eng Phys
1999;21(1):37–44.
[17] Fukunaga K. Introduction to statistical pattern recognition. New York:
Academic Press; 1972.
[18] Kissiov VT, Hadjitodorov ST. A fuzzy version of the K –NN method.
Fuzzy Sets Syst 1992;49:323–9.

7/28/2019 Heartbeat Classification
http://slidepdf.com/reader/full/heartbeat-classification 10/10
I. Jekova et al. / Medical Engineering & Physics 30 (20 08) 248–257 257
[19] Pedrycz W, Bortolan G, Degani R. Classification of electrocardio-
graphic signals: a fuzzy pattern matching approach. Artif Intell Med
1991;3:31–46.
[20] Jang JSR. ANFIS: adaptive-network-based fuzzy inference systems.
IEEE Trans Syst Man Cybern 1993;23(3):665–85.
[21] Chiu S. Fuzzy model identification based on cluster estimation. J Intell
Fuzzy Syst 1994;2(3):267–8.
[22] Sugeno M. Industrial applications of fuzzy control. North Holland:
Elsevier Science Publishers; 1985.
[23] Tabachnick BG, Fidell LS. Using multivariate statistics. New York:
Harper Collins College Publishers; 1996.
[24] XueQ, Hu YH,TompkinsWJ. Neural-network-based adaptive matched
filtering for QRS detection. IEEE Trans Biomed Eng 1992;39:
317–29.
[25] Yang TF, Devine B, Macfarlane PW. Artificial neural networks for
the diagnosis of atrial fibrillation. Med Biol Eng Comput 1994;32:
615–9.
[26] SilipoR, Bortolan G, Marchesi C. Designof hybrid architectures based
on neural classifier and RBF pre-processing for ECG analysis. I. J
Approx Reason 1999;21:177–96.
[27] Michaelis J, Wellek S, Willems JL. Reference standards for software
evaluation. Methods Inform Med 1990;29:289–97.