Embed Size (px)
Citation preview

GLOMERULONEFRITIS
Linda Armelia

Definisi dan Etiologi
Brenner and Rector's The Kidney. 8th ed. 2008Harrison’s Principles of Internal Medicine. 17th ed. 2008

Anatomy & Histology
Junqueira, Basic Histology. 11th ed. 2007

Glomerular Capillary
Marieb EN. Human Anatomy & Physiology. 7th ed.Junqueira, Basic Histology. 11th ed. 2007
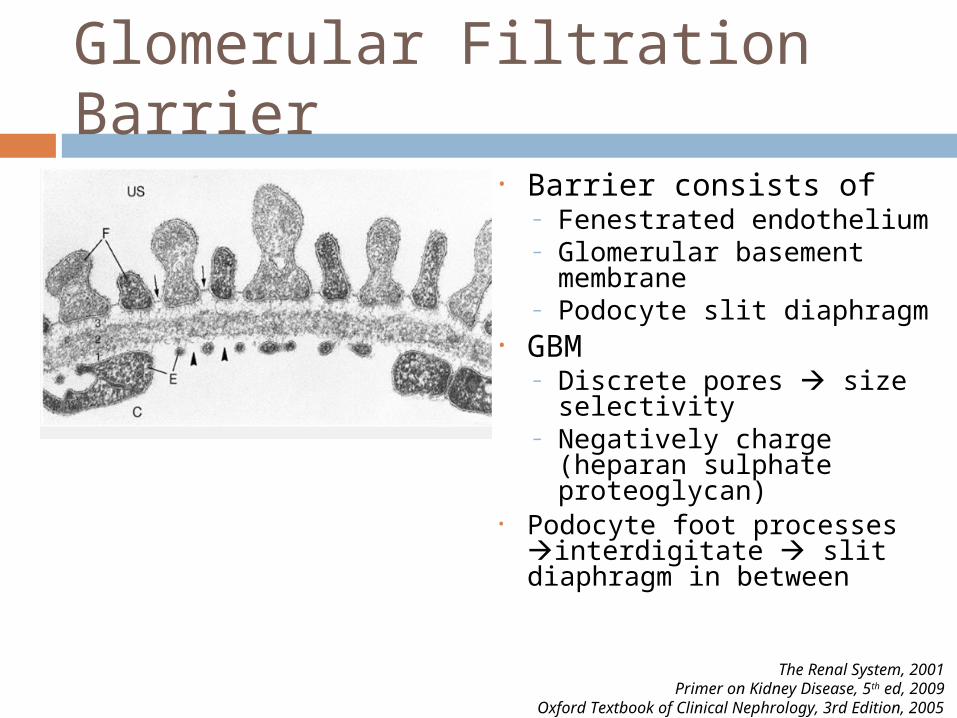
Glomerular Filtration Barrier• Barrier consists of
– Fenestrated endothelium– Glomerular basement
membrane– Podocyte slit diaphragm
• GBM – Discrete pores size
selectivity– Negatively charge
(heparan sulphate proteoglycan)
• Podocyte foot processes interdigitate slit diaphragm in between
The Renal System, 2001Primer on Kidney Disease, 5th ed, 2009
Oxford Textbook of Clinical Nephrology, 3rd Edition, 2005

Glomerular Filtration Barrier
Oxford Textbook of Clinical Nephrology, 3rd Edition, 2005
Harrison’s Principle of Internal Medicine 16th ed
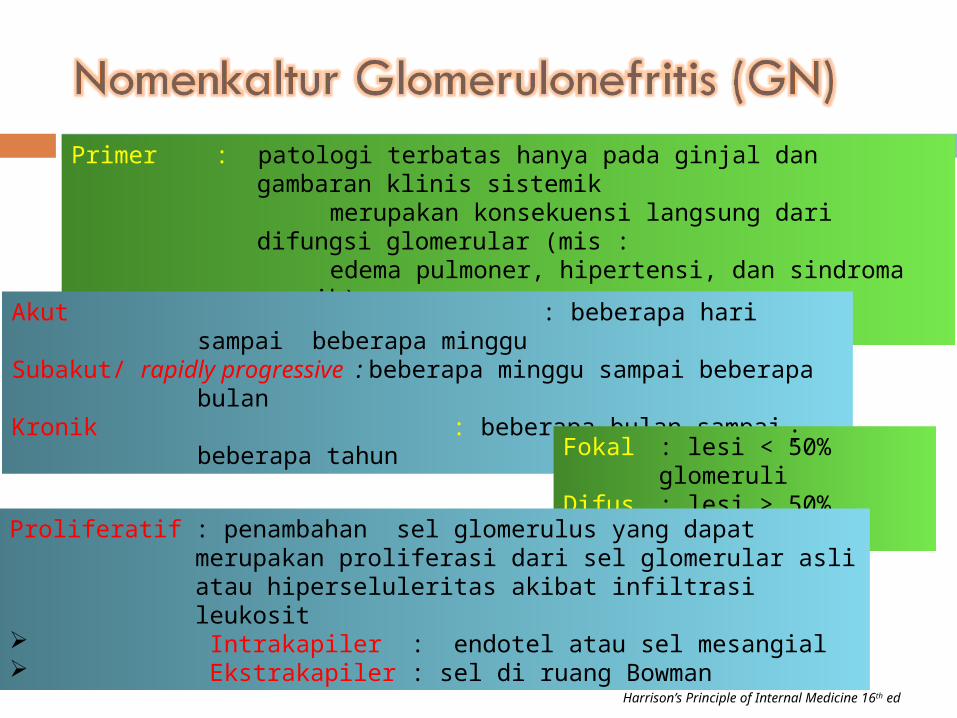
Primer : patologi terbatas hanya pada ginjal dan gambaran klinis sistemik merupakan konsekuensi langsung dari difungsi glomerular (mis : edema pulmoner, hipertensi, dan sindroma uremik)Sekunder : bagian dari kelainan multisistem
Akut : beberapa hari sampai beberapa minggu
Subakut/ rapidly progressive : beberapa minggu sampai beberapa bulanKronik : beberapa bulan sampai beberapa
tahunFokal : lesi < 50% glomeruliDifus : lesi > 50% glomeruli
Proliferatif : penambahan sel glomerulus yang dapat merupakan proliferasi dari sel glomerular asli atau hiperseluleritas akibat infiltrasi leukosit
Intrakapiler : endotel atau sel mesangial Ekstrakapiler : sel di ruang Bowman
:
Harrison’s Principle of Internal Medicine 16th ed
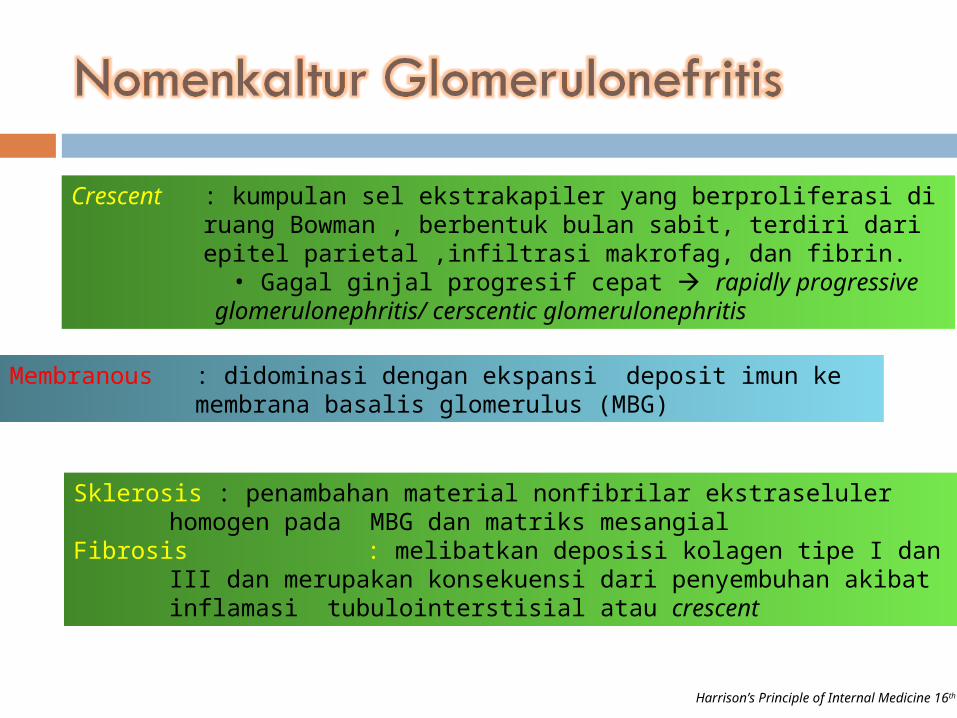
Crescent : kumpulan sel ekstrakapiler yang berproliferasi di ruang Bowman , berbentuk bulan sabit, terdiri dari epitel parietal ,infiltrasi makrofag, dan fibrin.
• Gagal ginjal progresif cepat rapidly progressive glomerulonephritis/ cerscentic glomerulonephritis
Membranous : didominasi dengan ekspansi deposit imun ke membrana basalis glomerulus (MBG)
Sklerosis : penambahan material nonfibrilar ekstraseluler homogen pada MBG dan matriks mesangial
Fibrosis : melibatkan deposisi kolagen tipe I dan III dan merupakan konsekuensi dari penyembuhan akibat inflamasi tubulointerstisial atau crescent
Patogenesis kerusakan glomerulus
• Otoimun• Genetik • Respon terhadap antigen asing • Pembentukan komplek imun • Identifikasi Antigen• Cell-mediated Immune Mechanisms• Mekanisme efektor: komplemen dan sel-sel
inflamasi
Comprehensive Clinical Nephrology, 2000

Patogenesis kerusakan glomerulus Otoimun
Comprehensive Clinical Nephrology, 2000
Self Reactive T and B cells are clonally deleted during fetal and neonatal life, but some survive
outside the thymusThese cells can be stimulated to generate response
to ‘self antigen’Infection altering host response to make them more immunogenic or by “molecular mimicry”
Certain bacteria act as “superantigen” can directly activate T-cell and cause monoclonal cell B
expansion

Patogenesis kerusakan glomerulus Genetik
• Respon terhadap antigen asing
Comprehensive Clinical Nephrology, 2000
Variations in HLA molecules and T-cell receptor are under strong genetic influence
Environmental events may have great importance, acting on genetic background in
inducing GN
Persistent antigenemia with circulating antigen-antibody complexes predispose to glomerular
injury classical example : chronic Hep B infection

Patogenesis kerusakan glomerulus• Pembentukan komplek imun
Identifikasi Antigen
Comprehensive Clinical Nephrology, 2000
In most cases of GN there is deposition of immune complex
Mechanisms of immune complex localization : “circulating immune complex” or “in situ
formation”
Regardless of the antigen origin, the spesific antigen involved remain largely unknown (except
anti-GBM, poststreptococcal GN)

Patogenesis kerusakan glomerulus Cell-mediated Immune Mechanisms
• Mekanisme efektor: komplemen dan sel-sel inflamasi
Comprehensive Clinical Nephrology, 2000
Certain glomerular disease develop primarily through cell-mediated immunity
Cresentic nephritis direct role of T cells in mediating proteinuria and crescent formation MCD permeability defects results from a
T-cell products
Complement : C5b-9 (membrane attack complex), and C5a (chemotactic factor)
Infiltrating cells are neutrophils, Tcells, or monocytes/macrophage
Intrinsic glomerular cells (epithelial, mesangial, and endothelial) may be activated by the injury and behave like
inflammatory cells

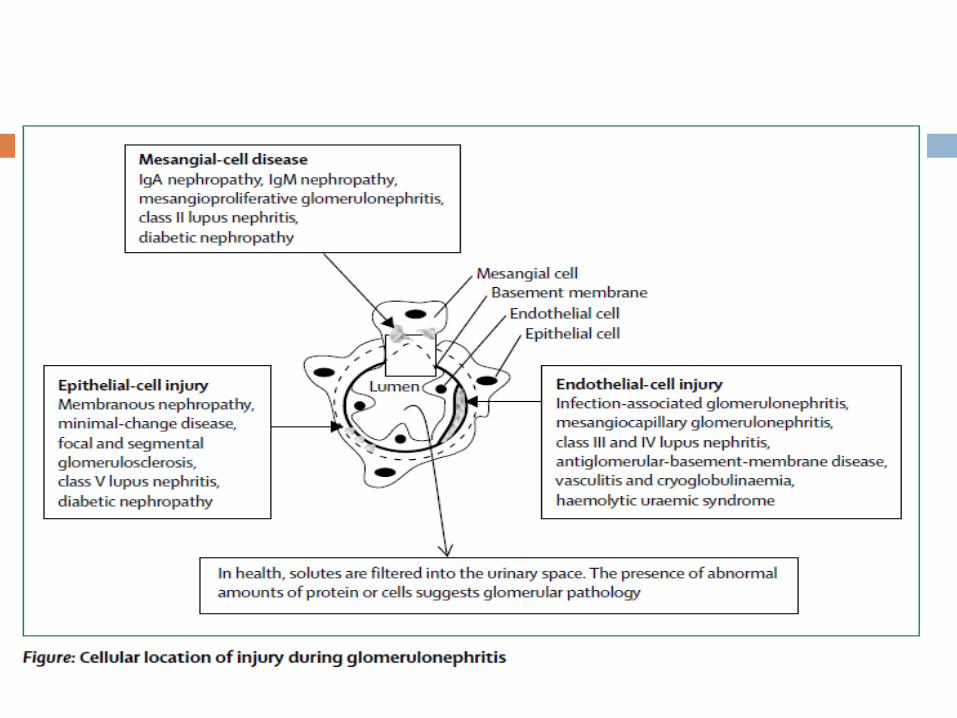
Patologi GN Berbagai perubahan patologis yg terjadi :
Proliferasi sel intrinsik (endotel, mesangial, epitelial) Infiltrasi lekosit Penumpukan matriks mesangial Perubahan membran basalis glomerular Scarring

Glomerulonephritis
Harrison’s Principles of Internal Medicine. 17th ed. 2008

Patogenesis kerusakan glomerulus
Oxford Textbook of Clinical Nephrology, 3rd Edition, 2005

Gambaran klinikAsymtomatic
Proteinuria 150mg-3g/dayHematuria > 2 red blood
cells/hpf in spun urine (usually dysmorphic)
Macroscopic HematuriaBrown/red painless
hematuria (no clots); typically coinsides with intercurrent infection
Asymptomatic hematuria + proteinuria between
attacks
Nephrotic syndromeProteinuria > 3,5 g/day
Hypoalbuminemia < 3,5g/dlEdema
HypercholesterolemiaLipiduria
Nephritic SyndromeOliguria
Hematuria : red cell castsProteinuria : usually < 3
g/dayEdema
HypertensionAbrupt onset, usually self
limiting
Rapidly Progressive Glomerulonephritis
Renal Failure over days/weeksProteinuria : usually < 3 g/day
Hematuria : red cell castsBlood pressure often normalMay have other features of
vasculitisChronic
GlomerulonephritisHypertension
Renal InsufficiencyProteinuria >3g/day
Shrunken smooth kidneyComprehensive Clinical Nephrology, 2000

Badr KF. Kidney Int 2005; 68: 1905–19.

Sindroma klinis penyakit glomerolus Hematuria asimtomatik dengan atau tanpa
proteinuria Sindroma Nefrotik Sindroma Nefritik RPGN Penyakit glomerular kronik
Glassock RJ. Clin Geriatr Med 2009; 25: 413–22.
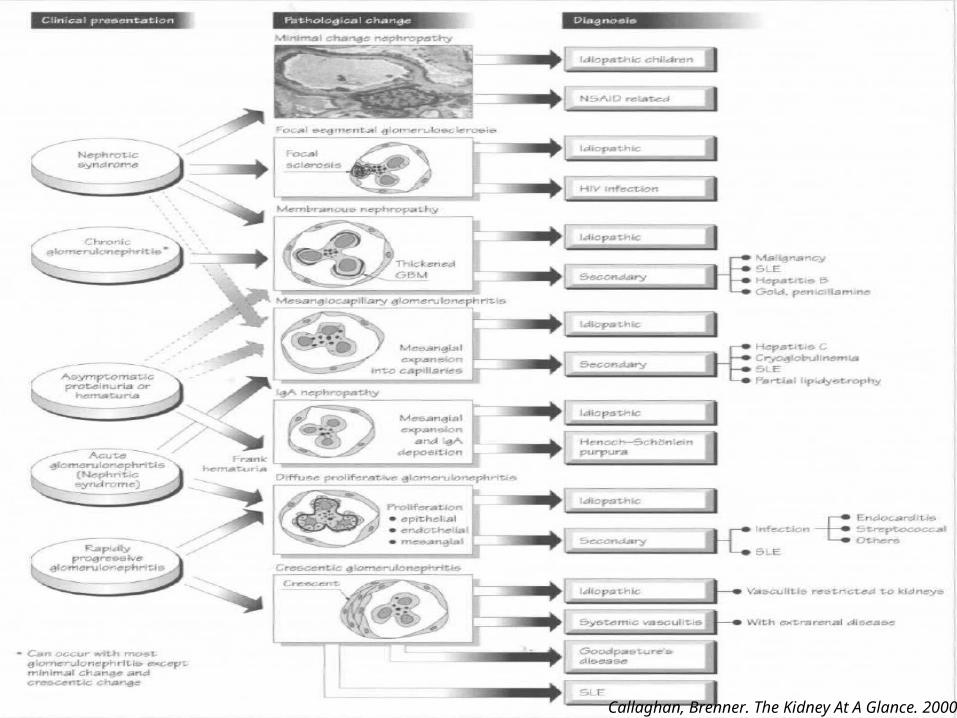
Callaghan, Brenner. The Kidney At A Glance. 2000

Hematuria Eritrosit dismorfik atau silinder eritrosit pada
urinalisa lesi di glomerolus Hematuria > 2 eritrosit/LPB Gross hematuria
Glomerular Proteinuria > 3 gram / 24 jam Perubahan pada sifat “size selektif” GBM
molekul dgn BM > 70 kd ( protein ) ikut terfiltrasi
Perubahan pada sifat “charge selektif” GBM ultrafiltrasi molekul bermuatan negatif seperti albumin

Evaluation of Hematuria and/or Proteinuria
Harrison’s Principles of Internal Medicine. 17th ed. 2008

Nefrotik VS Nefritik
Proteinuria > 3.5 grm/1.73 m2/24 jam
Hipoalbuminemia Edema Hiperlipidemia Lipiduria
Hematuria Silinder eritrosit Proteinuria Insufisiensi renal Retensi garam
( hipertensi nefropati dan edema )
Sindroma Nefrotik Sindroma Nefritik
Current Diagnosis & Treatment: Nephrology & Hypertension. 2009

Differentiation Between Nephrotic and Nephritic Syndrome
Typical Featues Nephrotic NephriticOnset Insidous AbruptEdema ++++ ++Blood Pressure Normal RaisedJugular Venous Pressure
Normal/low Raised
Proteinuria ++++ ++Hematuria May/ may not occur +++Red-cell casts Absent PresentSerum Albumin Low Normal/Slightly
Reduced
Comprehensive Clinical Nephrology, 2000

Sindroma nefrotik• Primer nefropati membranosa, FSGS,
minimal changes, MPGN• Sekunder DM, SLE, amiloidosis, leukemia• Penyakit glomerolus mempengaruhi “charge
or size selectivity” dinding kapiler glomerolus peningkatan permeabilitas glomerolus proteinuria
• Komplikasi hiperlipidemia, trombosis, defisinsi vitamin D, hipokalsemia, infeksi, malnutri, anemia

Sindroma nefritik• Primer post infectious GN, Nefropati Ig-A,
nefritis lupus• Patogenesis Inflamasi di Glomerolus
a. Antibodi di sirkulasi b. Komplek imun di sirkulasi c. Antigen yang mengaktivasi komplemen
• Komplikasi edema, hipertensi, anemia, ESRD,

Nachman PJ, dkk. Brenner: Brenner and Rector's The Kidney. 8th ed.
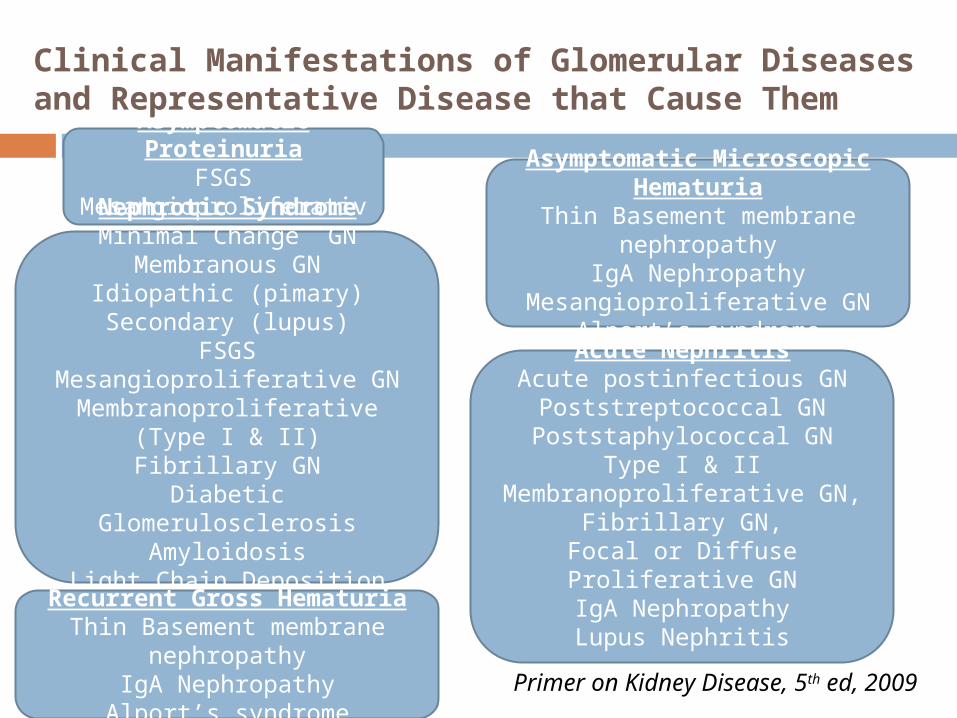
Clinical Manifestations of Glomerular Diseases and Representative Disease that Cause ThemAsymptomatic
ProteinuriaFSGS
Mesangioproliferative GNNephrotic Syndrome
Minimal Change GNMembranous GN
Idiopathic (pimary)Secondary (lupus)
FSGSMesangioproliferative GN
Membranoproliferative (Type I & II)
Fibrillary GNDiabetic Glomerulosclerosis
AmyloidosisLight Chain Deposition
Disease
Asymptomatic Microscopic Hematuria
Thin Basement membrane nephropathy
IgA NephropathyMesangioproliferative GN
Alport’s syndrome
Recurrent Gross HematuriaThin Basement membrane
nephropathyIgA Nephropathy
Alport’s syndrome
Acute NephritisAcute postinfectious GN
Poststreptococcal GNPoststaphylococcal GN
Type I & II Membranoproliferative GN,
Fibrillary GN,Focal or Diffuse Proliferative
GNIgA NephropathyLupus Nephritis
Primer on Kidney Disease, 5th ed, 2009

Clinical Manifestations of Glomerular Diseases and Representative Disease that Cause Them
Rapidly Progressive GNCresentic GNAnti GBM GN
Immune Complex GNANCA GN
Pulmonary-Renal Vasculitic Syndrome
Goodpasture’s (anti GBM) syndrome
Immune complex vasculitisLupus
ANCA VasculitisMicroscopic Polyangitis
Wegener’s granulomatosisChurg-strauss Syndrome
Chronic Kidney DiseaseChronic sclerosing GN
Primer on Kidney Disease, 5th ed, 2009

Minimal Change Disease (MCD)
= nil (Nothing-In-Light microscopy lesion) disease• Penyebab terbanyak penyebab sindroma nefrotik
pada anak , pada orang dewasa 10-15%.• Biopsi ginjal (penting pad dewasa)
– Normal/minimal changes pada mikroskop cahaya– Negative immunofluorescent microscopy– Podocyte foot process effacement pada mikroskop
elektron• Mayoritas idiopathic , tetapi bisa juga timbul
sekunder.
Waldman M, et al. Clin J Am Soc Nephrol 2007; 2:445-53. Saha TC, Singh H. Minimal Change Disease: A Review. 2006 Southern Medical Association

Minimal Change Disease
Abnormal T-cell
Function and
immune mediated defects
Inhibits sulfate
incorporation to GBM
Vasc Endothelial
Growth Factor
Diminished negative charge
Increased permeability to
protein
Toxic Epithelial Cell Injury
Foot process fusion and epithelial
detachmentPrimer on Kidney Disease, 5th ed, 2009Comprehensive Clinical Nephrology, 2000

Minimal Change Disease (MCD)Neoplasma Limfoma, leukemia, timoma, renal cell
carcinoma, colon carcinoma , pancreatic carcinoma
Obat-obatan NSAIDs, trimethadion, paramethadione, lithium, interferon, methimazole, tamoksifen
Infeksi Sifilis, HIV , mikoplasma, skistosomiasisAtopi Pollen, susu sapi, debu rumah, sengatan
lebahSuperimposed dengan penyakit ginjal lainnya
IgA nefropati, SLE, DM tipe 1, Polisitik kidney, HIV associated nefropati
Lainnya Sklerosing cholangitism sclerosing mesentricm GBS, MG, renal artery stenosis, partial lipodistropi
Glasssock RJ . Secondary minimal change disease. Nephrol Dial Transplant 2003

Biopsi histopatologi
UNC kidney center
Mikroskop cahaya glomerolus yang tampak normal GBM tipis, tanpa adanya hiperselularitas
dan expansi matriks mesangial

Electron microscope foot process effacement
UNC kidney center

Tatalaksana MCD• Terapi non-immunosupresif:
– Diuretik– ACE inhibitor/ARB– Statin
• Terapi immunosupresif :Prednisone (drug of choice)– Pada dewasa prednison 1 mg/kgBB/hari selama
8–16 minggu kemudian di–tappering off secara perlahan selama 6 bulan
Nakayama M, et al. Am J Kidney Dis 2002; 39:503Saha TC, Singh H. Minimal Change Disease: A Review. 2006 Southern Medical Association
.

Minimal Change Disease : Treatment
MCNS Patients
Children and AdultsSecond-line TherapyCyclophosphamide
Mycophenolate mofetilCyclosporine/
tacrolimus
AdultsSecond-line
TherapyCyclophosphamide
Mycophenolate mofetil
Cyclosporine/tacrolimus
Frequent relapsesSteroid
dependencySteroid
toxicity (30%
Frequent relapses
No steroid toxicity (30%)
Infrequent Relapses
(30%)
No Further Relapses
(10%)
Primer on Kidney Disease, 5th ed, 2009

Respons terapi Remisi komplit ekskresi protein urin < 300/hari
atau 3 hari berturut-turut dgn menggunakan dipstik, didapatkan prroteinuria (-).
Remisi parsial didapatkan penurunan kadar ≥50% (ekskresi protein urin antara 300-3500 mg/hari).
Relaps ekskresi urin> 3500 mg/hari setelah sebelumnya tercapai remisi komplit atau parsial.
Waldman M, et al. Clin J Am Soc Nephrol 2007; 2:445-53.

Steroid resisten dan Relaps Cyclophosphamide 2 mg/kg/hari Chlorambucil 0.15 mg/ kg/hari Cyclosporine 5 mg/kg/hari 6 - 12 months
ditappering 25% tiap 2 bulan MMF dan azatriophine steroid resisten Diagnosisnya mungkin bukan MCD tetapi
Focal Segmental Glomerulosclerosis (FSGS)
12 minggu
Beck LH, et al. Prim Care Clin Office Pract 2008; 35: 265–96.

Focal Segmental Glomerulosclerosis (FSGS)
Penyebab utama kejadian sindroma nefrotik pada dewasa berisiko tinggi terjadi ESRD ( 50% ) dalam 5-10 thn
FSGS primer dan sekunder Manifestasi asimtomatik proteinuria VS
sindroma nefrotik Hematuria, HT, azotemia 15-30% pasien Gold standar histopatologi biopsi
Chun MJ . Focal segmental glomerulosklersosis in neprotic adults: presentation, prognosis and respon theraphy.J am Soc nephrol 2004


Klasifikasi FSGS
Brenner and Rector's The Kidney. 8th ed. 2008
Terapi• Steroid prednisone 1 mg/kg BB/ hari ( max
60-80 mg/hari selama 6-8 bulan • Terapi adjuvant - Diet dan diuretik- ACE-I dan ARB- Kontrol lipid statin - Vitamin E- Plasmaferesis

Respon terapi • Respons komplit prednison dilanjutkan
sampai 1–2 minggu tappering off dalam 2–3 bulan.
• Respons parsial tappering off dalam 6–9 bulan.
• Steroid–dependent dan steroid–resistant a) Siklosporin dan prednison dosis rendahb) Siklofosfamidc) Mycophenolate mofetil
Beck LH, dkk. Prim Care Clin Office Pract 2008; 35: 265–96.

Membranous Nephropathy (MN) Istilah MN perubahan histologi
Penebalan membran basal glomerular Frekuensi lebih sering terjadi pada laki-laki,
dewasa dekade 4-5 Penyebab tersering sindrom nefrotik pada
pasien non-diabetes Primer VS sekunder ( SLE, hepatitis B,
hepatitis C, NSAID, penisilamin, kanker kolon)
Ponticelli C. Jnephrol 2007; 20: 268–87. Clin J Am Soc Nephrol 3: 905-919, 2008

Mikroskop cahaya pada MNPenebalan difuse pada Glomerular Basement Membrane pada seluruh glomerolus
Clin J Am Soc Nephrol 3: 905-919, 2008

Immunofluoresence pada MNDiffuse granular pattern dari Ig-G di sepanjang membran basal glomerular
Clin J Am Soc Nephrol 3: 905-919, 2008

Miroskop elektron pada MNElectron dense deposits are present in the subepithelial space across the glomerular basement membrane and under the epithelial cells

Mikroskop Cahaya dengan pewarnaan perak pada MN
•Spike appearance
•Menggambarkan membran basal yang tumbuh di antara subephitelial immune deposits
UpToDate 18.2, 2010

Klasifikasi MN• Stage I:
Subepithelial dense deposits (arrow)
• Stage II:Projections of basement membrane
• Stage III: Deposits surrounded by basement membrane
• Stage IV:Thickened basement membrane
Brenner and Rector's The Kidney. 8th ed. 2008

Manifestasi Klinis MN Sindrom nefrotik (80%) Proteinuria asimptomatik Hematuria mikroskopik (50%) Tekanan darah dan GFR normal pada
70% pasien
Ponticelli C. Jnephrol 2007; 20: 268–87.

Algoritma tatalaksana pada MN
Cattran D. J Am Soc Nephrol 2005; 16: 1188–94.

Membranous Nephropathy : Treatment
Mild Proteinuria (<4g/day)
Normal GFR
Maintain BP
below 130/80ACEI
Monitor
Moderate Proteinuri
a (4-8 g/day) Normal
GFR
Maintain BP below 130/80
ACEIMonitor
progress for 6 mo
Persistent (>4g/day)
Cytotoxic + steroids or
Cyclosporine
Heavy Proteinuria
(>8g/day) with or without
diminished GFR
Maintain BP below 130/80
ACEI, consider low protein diet
Monitor progress for < 6 mo (may initiate therapy early if renal function deteriorates
Persistent (> 8g/day) with or
without diminished GFR
Cyclosporine or cytotoxic +steroidsPrimer on Kidney Disease, 5th ed, 2009

Membranoproliferative GN (MPGN)
Terbagi atas 3 tipe MPGN tipe I, II, III Dicirikan adanya difus proliferasi sel
mesangial dan penebalan dinding kapiler glomerolus
Primer >>> , sekunder ( monoclonal immunoglobulin, SLE, chronic thrombotic microangiopathies, infeksi kronik hepatitis C)
Alchi B, Jayne D. Pediatr Nephrol (2010) 25:1409–1418

Klasifikasi MPGN 3 types on MPGN:
Type I: discrete immune deposits in the mesangium and subendothelial space
Type II: continuous, dense ribbon-like deposits along the basement membranes
Type III: immune complex disease, similar to type I. However, subepithelial deposits are prominent in type III
Brenner and Rector's The Kidney. 8th ed. 2008
MPGN tipe I Subendotelial, dan mesangial dense deposit MPGN bentuk terbanyak Aktivasi komplemen jalur klasik Secondary to a chronic or subacute infectious process:
Hepatitis C virus (HCV) Slowly progressive course to ESRD in 40-50% of cases Long-term treatment with high-dose alternate-day
prednisone 120 mg of prednisone every other day For 12 to 16 weeks tappering
Alchi B, Jayne D. Pediatr Nephrol (2010) 25:1409–1418 Beck LH, et al. Prim Care Clin Office Pract 2008; 35: 265–96

MPGN Tipe II Intra membranous dense deposit Berhubungan dengan C3 nephritic factor
aktivasi jalur alternatif Sindrom nefrotik Prognosis buruk sebagian besar
pasien mengalami ESRD setelah 7 tahun Jarang remisi spontan
Beck LH, et al. Prim Care Clin Office Pract 2008; 35: 265–96. Alchi B, Jayne D. Pediatr Nephrol (2010) 25:1409–1418Gerald BA et all. J Am Soc Nephrol 2005 :16: 1392–1404

MPGN tipe III Deposit di subendotel, mesangial dan
subepitelial Alternative pathway ( C5 convertase)

Gambaran klinis Sindroma nefrotik(40–70%) Sindroma nefritik (20–30%) proteinuria asimtomatik dan hematuria
(20–30%) gross hematuria (10–20%). Lab kadar C3 dan C4 yang rendah, C3
nephritic factor (+)
Alchi B, Jayne D. Pediatr Nephrol (2010) 25:1409–1418Gerald BA et all. J Am Soc Nephrol 2005 :16: 1392–1404

Alchi B, Jayne D. Pediatr Nephrol (2010) 25:1409–1418Lenvin A. Management of membarnoproliferative glomerulonephritis:Evidence based recommendation. Kidney international 1999 ; 55(70)
Algoritme Tatalaksana MPGN

Immunoglobulin A Nephropathy (IgAN) = Berger’s Diseases th 1968 oleh Dr Berge Berger’s
disease Prevalensi tersering pada ras Asian dan
Kaukasian Penyebab utama primary GN Klinis gross hematuria disertai infeksi
saluran nafas bagian atas Lab eritrosit dismorfik dan silinder
eritrosit pada urinalisa, proteinuria (+)Beck LH, et al. Prim Care Clin Office Pract 2008; 35: 265–96 Donadio JV, Grande JP. IgA Nephropathy. N Eng J Med 2001;347(10): 738-48.

Patogenesis Immunoglobulin A Nephropathy
Donadio JV, Grande JP. IgA Nephropathy. N Eng J Med 2001;347(10): 738-48

Histopatologi
Mikroskop cahaya:Peningkatan matrik
mesangial dan selularita
Mikroskop elektron:
Deposit IgA di daerah mesangial
Immunofluoresence:
Deposit Ig-ADi mesangial
Tumlin JA, et al. Clin J Am Soc Nephrol 2004; 2: 1054–61.

Tatalaksana
Proteinuria ringan < 500 mg/hari, fungsi ginjal normal, tekanan darah normal observasi, monitor tiap 6 bulan.
Fungsi ginjal normal, proteinuria 500-1000 mg/hari, tekanan darah meningkat ACE-Inhibitor/ARB
Glukokortikoid: Sindrom nefrotik episode akut Progresif aktif
Prognosis: stable disease atau progresif lambat
Alexopoulos, E. Kidney Int 2004; 65:341Donadio JV, Grande JP. IgA Nephropathy. N Eng J Med 2001;347(10): 738-48

Poststreptococcal GN (PSGN) Etiologi Streptococcus ( grup A dan C),
Staphylococcus aureus , Staphylococcus epidermidis, Salmonella typhi dan parathyphi, Treponema pallidum, Brucella abortus
GN terjadi 2-3 minggu setelah faringitis atau infeksi kulit
Peningkatan titer Anti-streptolysin O (ASO) Hypocomplementemia CH50 dan C3
berkurang, C4 normal
Beck LH, et al. Prim Care Clin Office Pract 2008; 35: 265–96.
Poststreptococcal GN (PSGN) Klinis Nefritik sindrom hematuria
gross / mikroskopik, hipertensi, edema, oligouria 2 minggu
4% massive proteinuria masif, azotemia progresif dan cresentic glomerulonefritis

Tatalaksana Sindrom nefritik self limiting terapi
simtomatik (edema dan hipertensi) meliputi kontrol tekanan darah (ACEI/ ARB) dan diet rendah garam
Infeksi streptococcal 1.2 juta unit benzathine penisiline dosis tunggal atau 4x250 mg eritromisin oral selama 7-10 hari
Beck LH, et al. Prim Care Clin Office Pract 2008; 35: 265–96.

Rapidly Progressive GN (RPGN) Sindroma klinis ditandai onset yang tiba tiba
dari hematuria, proteinuria dan anemia yang berkembang secara cepat menjadi gagal ginjal dalam hitungan minggu atau bulan
3 tipe kelainan berdasarkan imunofluorosen: Tipe I : Anti–GBM antibodies Tipe II : Immune complex glomerulonephritis Tipe III : Pauci–immune glomerulonephritis ( ANCA
associated crecentic GN) paling sering (>50%).
Jennette JC.Rapidly progresive crescentic glomerulonephritis. Kidney International, Vol. 63 (2003), pp. 1164–1177

Tampilan RPGN
Penurunan fungsi ginjal yang sangat cepat ( penurunan GFR>50% dalam 3 bulan)
Ukuran ginjal normal atau membesar Sindroma nefritik ( proteinuria, eritrosit
dismorfik, silinder eritrosit) Ditemukan glomerular cresent pada
pemeriksaaan imunoflurosense Tidak pernah remisi spontas

Brenner and Rector's The Kidney. 8th ed. 2008

Tipe I (Anti–GBM antibodies) Antibodi anti-GBM yang patogen terhadap domain
NCI dari rantai α-3 kolagen tipe IV yang mrpk komponen dari membran basalis glomerolus dan alveolus
Klinis: edema, hipertensi, uremia , oligouria, hematuria, hemoptisis dan sesak
Lab: hematuria, proteinuria, anti GBM antibodi, peningkatan ureum dan kreatinin,
Bila disertai dengan perdarahan pulmoner Goodpasture Syndrome
Biopsi nekrosis segmental, kebocoran darah masuk ke bowman’s space dan terbentuknya cresent

Lupus Nephritis Lupus nephritis involved deposition of
preformed immune complexes, initially in the mesangial interstices with eventual spillover into subendothelial space, which initiates progressive stages of inflammation as well as mesangial and endocapillary proliferative disease
Circulating nuclear remnants from excessive apoptotic breakdown bound to capillary glomerular sites binding to autoantibodies
Primer on Kidney Disease, 5th ed, 2009

Lupus Nephritis
Comprehensive Clinical Nephrology, 2010

Lupus Nephritis : Classification, ISN 2004Designation DescriptionClass I : Minimal Mesangial LGN Near-normal glomeruli dy LM; mesangial deposits are
present by IF and/or EMClass II : Mesangial Proliferative GN Mesangial Hypercellularity and matrix expansion, with
mesangial deposits by IF and EMClass III : Focal LGN < 50% of glomeruli display active or inactive
segmental (<50% of the tuft) or global (>50% of the tuft) endocapillary proliferation or sclerosis; predominantly mesangial and subendothelial deposits are present on IF and EM
Class IV : Diffuse LGN
Class IV-S : Segmental diffuse LGN Class IV-G : Global diffuse LGN
>50% of glomeruli have endocapillary or extracapillary glomerulonephritis; predominantly mesangial and subendothelial deposits are present on IF and EM; two subsets are defined>50% of affected glomeruli have segmental lessions
>50% of affected glomeruli have global lessionsClass V : Membranous LGN Capillary loop thickening in association with
predominantly subepithelial deposits by IF and EMClass VI : Advanced Sclerosis >90% of glomeruli are obsolescent, with substatial
activity in remaining glomeruli
Primer on Kidney Disease, 5th ed, 2009
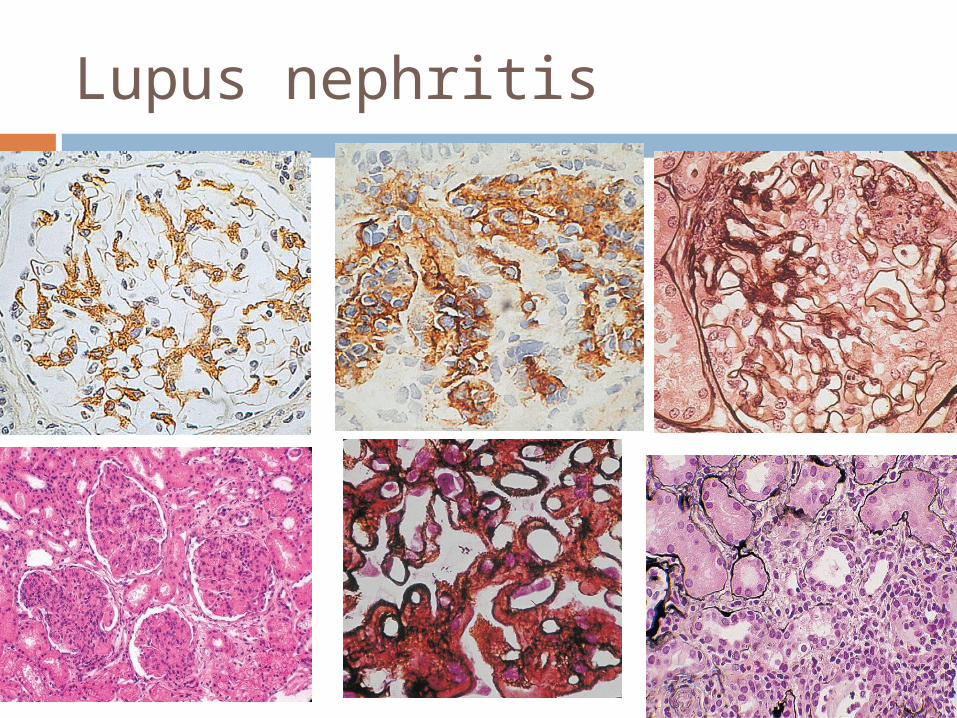
Lupus nephritis

Lupus Nephritis : Treatment Remission criteria :
a reduction in proteinuria below 0.5 g/24 h or urine protein to creatinine ratio below 0.5 g/g absence of glomerular hematuria or red cell casts, and Normalization or at least stabilization of GFR.
Flare : isolated increase in proteinuria, typically at least doubling and
above 1 g/24 h, as a proteinuric flare; or appearance of glomerular hematuria or red cell casts with
proteinuria, with or without hypertension and a decline in GFR, as a nephritic flare
In general, patients assigned to ISN class I and class II need no therapy directed at the kidney
active proliferative LN into an induction phase and a maintenance phase
Comprehensive Clinical Nephrology, 2010

Lupus Nephritis : Treatment
Comprehensive Clinical Nephrology, 2010

Lupus Nephritis : Treatment
Comprehensive Clinical Nephrology, 2010

Lupus Nephritis : Treatment
Comprehensive Clinical Nephrology, 2010

Overt SN No hipertention No hematuria Normal renal function Normal complex imun
MCD

Nephrotic syndrome Hipotensi Associated with myeloma Hamotura (-) Renal function insuficiensi
Amyloidosis

Nephrotic syndrome Non selection
proteinuria Microhematuria Hypertension GFR ↓ Complement normal
FSGS
Heavy proteinuria Microhematuria Hypertension
(normal) Slowly GFR ↓ Tromboemboli
MGN

NS-Nephritic Hypertension Minimal or rapidly decreases of renal
function Low complement Hematuria
MPGN

Hematuria after URI Reccent of
proteinuria/microhematuria
Proteinuria (minimal to moderate neprotic range)
Hipotension Normal complement IgA
nephropathy
Acute onset of edema
Non nephrotic proteinuria
Hypertension GFR low Low complement Acute post
streptococal GN

Nephrotic rane Oliguria Rapid progressive loss of renal function Lack system respon (Anti GM
nonAb/coplement) Anti GBM

Steroid responsiveness MCD FSGS IgM Mesangial proliperatif











