Embed Size (px)
Citation preview

279
Genetic Epidemiology of Breast Cancer W. Douglas Thompson, Ph.D.
It has been recognized for some time that a family history of breast cancer is associated rather strongly with a wo- man’s own risk of developing the disease. Recent segrega- tion analyses of population-based data on familial pat- terns provide evidence for a rare autosomal dominant al- lele that increases a carrier’s susceptibility to breast can- cer. The estimated proportion of breast cancer patients who carry this allele declines sharply with age at diagno- sis. Empirical estimates of the risk associated with par- ticular patterns of family history of breast cancer indi- cate the following: (1) having any first-degree relative with breast cancer increases a woman’s risk of breast cancer 1.5-3-fold, depending on age, (2) having multiple first degree relatives affected is associated with particu- larly elevated risks, (3) having a second-degree relative affected increases the risk by approximately 50%, (4) affected family members on the maternal side and the pa- ternal side contribute similarly to the risk, (5) a family history of breast cancer is associated with bilateral dis- ease, and (6) breast cancer in males is associated with breast cancer in female relatives in much the same way as is breast cancer in women.
Ovarian cancer clearly has been shown to be associ- ated with breast cancer in families, and genetic linkage has provided strong evidence for a breast-ovarian cancer gene located somewhere on chromosome 17q. At the pop- ulation level, having a first degree relative with ovarian cancer may be at least as predictive of a woman’s risk for developing breast cancer as is having a second-degree relative with breast cancer. Considerably weaker evi- dence points to a possible familial relationship between breast and endometrial cancer and between breast cancer in women and prostatic cancer in males.
The clinical applications of the genetic epidemiology of breast cancer are complicated by uncertainty as to the efficacy of mammographic screening in women under the age of 50. For the vast majority of women with a positive family history, the epidemiologic evidence does provide the basis for offering considerable reassurance in that
Presented at the National Conference on Breast Cancer, Boston, Massachusetts, August 26-28, 1993.
From the Department of Applied Medical Sciences, School of Applied Science, University of Southern Maine, Portland, Maine.
Address for reprints: W. Douglas Thompson, Ph.D., Department of Applied Medical Sciences, School of Applied Science, University of Southern Maine, 96 Falmouth Street, Portland, ME 04103.
Accepted for publication January 31, 1994.
risks are not extremely high. For that rather small sub- group at exceptionally high risk, realistic estimates of the magnitude of absolute risk over the next 10-20 years may be more informative and less alarming than lifetime probabilities. Cancer 1994; 74979-87.
Key words: breast neoplasms, genetics, ovarian neo- plasms, prostatic neoplasms, endometrial neoplasms.
Breast cancer is by far the most frequently diagnosed type of malignant neoplasm among women, and it claims tens of thousands of lives annually in the United States. Despite extensive investigation into the etiology of breast cancer over the past several decades, the risk factors that have been identified to date account for only a minority of the disease in the population. Breast cancer in a first degree relative generally has been found to increase the risk of breast cancer two- to threefold.’ Having multiple affected first degree relatives may in- crease the risk sub~tant ia l ly .~ ,~
Awareness of family history as a risk factor leads to considerable concern on the part of many women who have affected family members, and some even seek pro- phylactic mastectomy. Clinicians also recognize the im- portance of family history as an indicator of risk and often query their female patients about the occurrence of breast cancer in family members. The use to which such information most appropriately should be put, however, is generally unclear.
This paper is not intended as an exhaustive review of the literature on the genetic epidemiology of breast cancer. Instead, its purpose is to present and synthesize some of the more recent data available on the subject and to evaluate those data from the perspective of pub- lic health and clinical decision making for individual patients.
Familial Aggregation of Breast Cancer
A number of case-control epidemiologic studies have examined the degree of familial aggregation of breast cancer. A large population-based study of this type is the Cancer and Steroid Hormone Study.4 In this study,

280 CANCER Supplement July 2, 2994, Volume 74, No. 1
Table 1. Numbers and Odds Ratios for Reported History of Breast Cancer in the Female Relatives of Breast Cancer Patients and Control Subjects, Age 20-44, Cancer and Steroid Hormone Study*
Occurrence of breast cancer in female relatives (N = 2080) (N = 2058) Odds ratio (95% CI)
No. of patients No. of control subjects
No first- or second-degree reported to
First-degree have been affected
Mother affected Sister affected Mother or sister with onset < 45 yr 2 or more affected
Second-degree
1459 1665 1.00 (referent)
191 57 93 19
70 21 30
1
3.11 (2.33-4.17) 3.10 (1 32-5.30) 3.54 (2.29-5.49)
21.68 (3.09-94.74)
Maternal grandmother or aunt affected 235 187 1.43 (1.16-1.77) Paternal grandmother or aunt affected 178 129 1.57 (1.23-2.01) 2 or more affected 66 34 2.22 (1.43-3.44)
CI: confidence interval. Excluded are 13 patients and 11 control subjects who did not provide information on the number of sisters they had had. The only second-degree relatives for
whom information was collected were grandmothers and aunts. Categories for first-degree relatives included women regardless of whether second-degree relatives were also affected; categories for second-degree relatives were restricted to women with no first-degree relative affected.
detailed family histories were collected from approxi- mately 4500 newly diagnosed breast cancer patients be- tween the ages of 20 and 54 and from a comparable number of age-matched control women from the gen- eral population. The initial findings were reported in 1 985,5 and extensive genetic and epidemiologic analy- ses have been conducted using these Here, I present some previously unpublished empirical esti- mates of the magnitude of the odds ratio (relative risk) for various patterns of family history of breast cancer among breast cancer cases versus controls in the Cancer and Steroid Hormone Study.
Table 1 gives data for breast cancer patients diag- nosed between the ages of 20 and 44 and control women in the same age group. Table 2 presents corre-
sponding data for women between the ages of 45 and 54. From Table 1, it can be seen that for women under the age of 45, the risk of developing breast cancer is increased approximately threefold if a mother or sister has been diagnosed with the disease (odds ratios, 3.1 1 and 3.10, respectively; 95% confidence intervals, 2.33- 4.17 and 1.82-5.30, respectively). Diagnosis of breast cancer before age 45 in either a mother or sister in- creases the risk somewhat more (odds ratio, 3.54; 95% confidence interval, 2.29-5.49). The risk is elevated par- ticularly in women who report that two or more of their first-degree female relatives have had breast cancer (odds ratio, 21.68; 95% confidence interval, 3.09- 94.74). Having an affected second-degree relative but not an affected first-degree relative increases the risk by
Table 2. Numbers and Odds Ratios for Reported History of Breast Cancer in the Female Relatives of Breast Cancer Patients and Control Subjects, Ages 45-54, Cancer and Steroid Hormone Study*
Occurrence of breast cancer in female relatives
No. of patients (N = 2614) (N = 2604) Odds ratio (95% CI)
No. of control subjects
No first- or second-degree reported to
First-degree have been affected
Mother affected Sister affected Mother or sister with onset < 45 yr 2 or more affected
Maternal grandmother or aunt affected Paternal grandmother or aunt affected 2 or more affected
Second-degree
1865
220 125 97 30
257 188
69
2100
132 64 39 5
186 134 35
1.00 (referent)
1.88 (1.49-2.36) 2.20 (1.60-3.07) 2.80 (1.92-4.08) 6.76 (2.49-19.84)
1.56 (1.27-1.9 1) 1.58 (1.25-2.00) 2.22 (1.44-3.42)
CI: confidence interval. * Excluded are 23 patients and 15 control subjects who did not provide information on the number of sisters they had had. The only second-degree relatives for whom information was collected were grandmothers and aunts. Categories for first-degree relatives included women regardless of whether second-degree relatives were also affected; cateeories for second-deeree relatives were restricted to women with no first-deeree relative affected.

Genetic Epidemiology of Breast Cancer/Thompson 281
approximately 50%, and the increase is of similar mag- nitude, regardless of whether the relative is on the ma- ternal or paternal side of the family.
For women between the ages of 45 and 54, Table 2 indicates an overall pattern similar to that observed for women between the ages of 20 and 44, except that the magnitude of the increase in risk associated with having an affected first-degree relative is somewhat smaller.
Other epidemiologic studies generally have found similar magnitudes of risk associated with family his- tory of breast c a n ~ e r . ~ , ~ , ' ~ - ' ~ Women with an affected first-degree relative are estimated to have a 1.5-3.0-fold increase in risk, with early age at onset in relatives often associated with a greater increase than late age at onset. An important qualification on the interpretation of many of these estimates, however, is the retrospective nature of the information collected in case-control in- vestigations. Because of their own recent diagnosis of breast cancer, case patients may be more knowledge- able than controls about cancer in their family mem- bers, and as a consequence, the relative risks reported in some studies may be inflated. Results presented in a recent report from the Nurses' Health Study" are not subject to this sort of distortion, because the informa- tion on family history was collected prospectively, be- fore the diagnosis of breast cancer in cohort members. In that study, a maternal history of breast cancer again was found to increase a woman's risk of breast cancer, with the magnitude of the increase related to age at di- agnosis of the mother's cancer. For women whose mother developed breast cancer before age 40, the mul- tivariate relative risk was 2.00 (95% confidence interval, 1.49-2.70), and for women whose mother developed the disease a t age 70 or later, the value was 1.46 (95% confidence interval, 1.01-2.11). Women with one or more affected sisters were found to be more than twice as likely as women with no affected sister to develop breast cancer. These estimates of relative risk, although of smaller magnitude than some of those obtained from case-control studies, indicate that the results from ret- rospective investigations of the familial aggregation of breast cancer are generally valid. Prospective data from a cohort of women in Iowa yielded a relative risk of 1.53 for any affected first-degree relative, but that study was restricted to women who were older than age 54 at the beginning of the follow-up period."
Application of segregation analysis to population- based data on breast cancer in families indicates a pat- tern consistent with inheritance of a rare autosomal do- minant allele.' The estimated proportion of breast can- cer patients who carry this allele declines sharply with increasing age a t diagnosis.
Results from several studies indicate that having a relative with bilateral breast cancer may put a woman
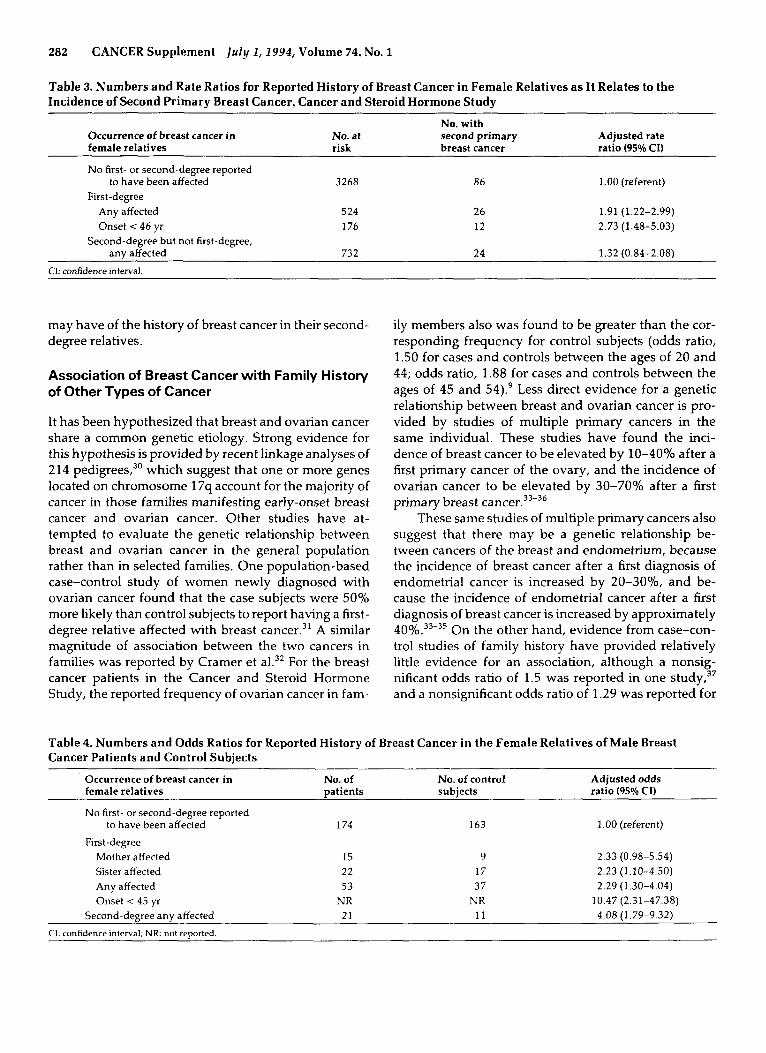
at a particularly high risk of developing breast can- cer, 14~17-25 although other studies do not.3,5,26,27 Retro- spective collection of family history data may be partic- ularly problematic when the women providing the his- tory are asked to differentiate between unilateral and bilateral disease. Recently, prospective population- based interview data addressing this issue have been published.2' Selected results are summarized in Table 3. For that study, the breast cancer cases from the Cancer and Steroid Hormone Study, who were diagnosed with breast cancer between 1980 and 1982 and interviewed about their family history shortly thereafter, were fol- lowed through 1986 via the Surveillance, Epidemiology and End Results Program of the National Cancer Insti- tute to monitor the occurrence of a second primary breast cancer in the contralateral breast. As the results in the table indicate, women who have had a first pri- mary breast cancer are more likely to develop a contra- lateral second primary breast cancer if they have a fam- ily history of breast cancer than if they do not. In addi- tion, the magnitude of the rate ratio (relative risk) is greater if a first-degree relative was diagnosed with breast cancer before age 45 than if she was diagnosed with breast cancer at a later age.
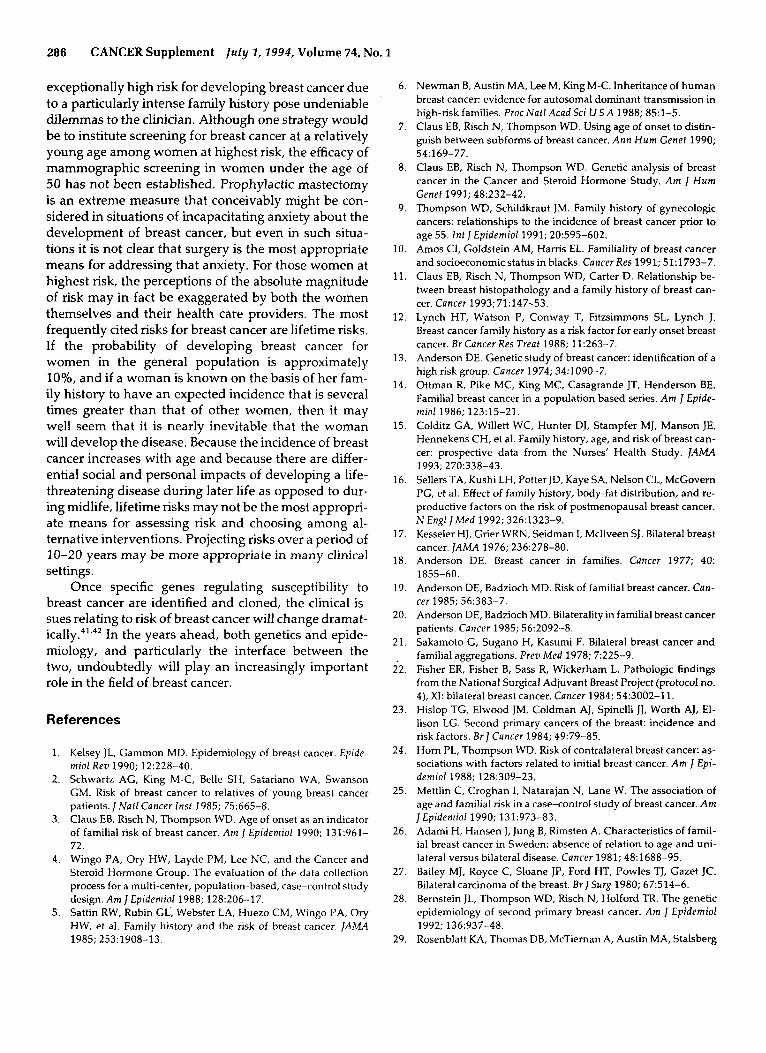
Several of the pedigrees reported in the literature as illustrative of families with an extremely high rate of occurrence of breast cancer have been remarkable in that they include instances of male breast cancer, which in the general population is extremely rare. Therefore, it would seem that the presence of male breast cancer in a family may be a particularly powerful indicator that female family members are at high risk for developing breast cancer. A recent population-based study, how- ever, indicates that the familial association between male and female breast cancer is not strikingly stronger than the corresponding association for female breast cancer within families.29 Table 4 presents selected re- sults from that study. Having a mother affected with breast cancer is found to increase the risk of male breast cancer 2.33-fold, and having an affected sister is found to increase the risk 2.23-fold. These estimates are close to the corresponding figures of 1.97 and 2.25 obtained from a metaanalysis of five studies of female breast can- cer. The table also indicates that male breast cancer may be related particularly strongly to early-onset breast cancer in female first-degree relatives, but the confi- dence interval around the estimate of 10.47 is wide. The finding of a 4.08-fold increase in risk associated with having an affected second-degree female relative makes little genetic or epidemiologic sense in the context of the estimates for first-degree relatives; it may reflect insta- bility due to small numbers or systematic bias due to case-control differences in the knowledge that men
282 CANCER Supplement ju ly I , 1994, Volume 74, No. 1
Table 3. Numbers and Rate Ratios for Reported History of Breast Cancer in Female Relatives as It Relates to the Incidence of Second Primary Breast Cancer, Cancer and Steroid Hormone Study
Occurrence of breast cancer in female relatives
No. with No. at second primary Adjusted rate risk breast cancer ratio (95% CI)
No first- or second-degree reported
First-degree to have been affected
Any affected Onset < 46 yr
any affected Second-degree but not first-degree,
3268
524 176
732
86
26 12
24
1.00 (referent)
1.91 (1.22-2.99) 2.73 (1.48-5.03)
1.32 (0.84-2.08)
C1: confidence interval.
may have of the history of breast cancer in their second- degree relatives.
Association of Breast Cancer with Family History of Other Types of Cancer
It has been hypothesized that breast and ovarian cancer share a common genetic etiology. Strong evidence for this hypothesis is provided by recent linkage analyses of 214 pedigree^,^' which suggest that one or more genes located on chromosome 17q account for the majority of cancer in those families manifesting early-onset breast cancer and ovarian cancer. Other studes have at- tempted to evaluate the genetic relationship between breast and ovarian cancer in the general population rather than in selected families. One population-based case-control study of women newly diagnosed with ovarian cancer found that the case subjects were 50% more likely than control subjects to report having a first- degree relative affected with breast cancer.31 A similar magnitude of association between the two cancers in families was reported by Cramer et aL3’ For the breast cancer patients in the Cancer and Steroid Hormone Study, the reported frequency of ovarian cancer in fam-
ily members also was found to be greater than the cor- responding frequency for control subjects (odds ratio, 1.50 for cases and controls between the ages of 20 and 44; odds ratio, 1.88 for cases and controls between the ages of 45 and 54).9 Less direct evidence for a genetic relationship between breast and ovarian cancer is pro- vided by studies of multiple primary cancers in the same individual. These studies have found the inci- dence of breast cancer to be elevated by 10-40% after a first primary cancer of the ovary, and the incidence of ovarian cancer to be elevated by 30-70% after a first primary breast ~ a n c e r . ~ ~ - ~ ~
These same studies of multiple primary cancers also suggest that there may be a genetic relationship be- tween cancers of the breast and endometrium, because the incidence of breast cancer after a first diagnosis of endometrial cancer is increased by 20-30%, and be- cause the incidence of endometrial cancer after a first diagnosis of breast cancer is increased by approximately 4 0 Y 0 . ~ ~ - ~ ~ On the other hand, evidence from case-con- trol studies of family history have provided relatively little evidence for an association, although a nonsig- nificant odds ratio of 1.5 was reported in one and a nonsignificant odds ratio of 1.29 was reported for
Table 4. Numbers and Odds Ratios for Reported History of Breast Cancer in the Female Relatives of Male Breast Cancer Patients and Control Subjects
Occurrence of breast cancer in No. of No. of control Adjusted odds female relatives patients subjects ratio (95% CI)
No first- or second-degree reported
First-degree
to have been affected 174 163 1 .OO (referent)
Mother affected 15 9 2.33 (0.98-5.54) Sister affected 22 17 2.23 (1.10-4.50) Any affected 53 37 2.29 (1.30-4.04) Onset < 45 yr NR NR 10.47 (2.31-47.38)
Second-degree any affected 21 11 4.08 (1.79-9.32)
CI. confidence interval: NR: not reoorted.

Genetic Epidemiology of Breast Cancer/Thompson 283
women between the ages of 20 and 44 in the Cancer and Steroid Hormone Study.' The strongest evidence to date for a familial association between breast cancer and endometrial cancer comes from the prospective evaluation of second primary breast cancer in the Can- cer and Steroid Hormone Study.28 Based on family his- tories collected shortly after the diagnosis of first pri- mary breast cancer, a family history of endometrial can- cer was associated significantly with the subsequent development of a second primary breast cancer (rate ra- tio, 2.13 for one or more affected first-degree relatives; 95% confidence interval, 1.04-4.35).
Two recent studies also have suggested that the in- cidence of breast cancer in women may be associated with a history of prostate cancer in male relatives. An- derson and Badzioch3' found that, within a group of families ascertained through an index patient with male breast cancer, the occurrence of breast cancer in women was 3.7-fold higher if there was a history of prostate cancer within the family. A recent record linkage study in Iceland yielded a relative risk of 1.4 for the familial association of prostate cancer and female breast can- ~ e r . ~ ~ Further studies are needed to elucidate the nature and magnitude of the familial association between these two cancers.
Population-wide Perspective on Familial Risks
There clearly is a familial component to breast cancer that is likely to represent genetic transmission and that accounts for some proportion of the incidence of the disease in the population. The precise magnitude of that proportion, and therefore the importance of genetic transmission in the etiology of breast cancer at the pop- ulation level, has not yet been established. Therefore, to put the genetic epidemiology of breast cancer into clearer public health perspective, I have conducted some multivariable analyses of familial risks in the Can- cer and Steroid Hormone Study4 and have attempted to quantify the implications of these risks at the popula- tion level.
The first step in this process is the fitting of logistic regression models4' to the family histories of the breast cancer cases and controls to estimate the multiplicative factor by which each component of family history con- tributes to the incidence of breast cancer. The models provide for the possibility that the contribution of each component may differ in magnitude for women be- tween the ages of 20 and 44 for those between the ages of 45 and 54. Results are given in Table 5. Because nei- ther a family history of endometrial cancer nor the dis- tinction between unilateral and bilateral breast cancer in family members was found to be associated with the incidence of breast cancer, these factors are not in-
Table 5. Computation of a Woman's Relative Risk for Breast Cancer Development Based on Data from the Cancer and Steroid Hormone Study+
History of cancer in female relatives
Multiplicative factor for increased risk
Breast cancer in one or more first- degree relatives
Breast cancer with onset younger than age 45 in one or more first. degree relatives
Breast cancer in two or more first- degree relatives
Breast cancer in one or more second-degree relatives
Breast cancer in two or more second-degree relatives
2.22 or 1.47t
1.38
3.83
1.36
1.49 Ovarian cancer in one or more first-
degree relatives 1.59 The baseline group was women with no breast cancer in first- or second-de-
gree relatives and no ovarian cancer in first-degree relatives. Estimates were based on logistic regression analysis. t The value of 2.22 was used for women age 20-44 yr, and the value of 1.47 was used for women age 45-54 vr.
cluded in the table. The only component of family his- tory found to differ significantly with age in terms of its impact on the incidence of breast cancer is having one or more first-degree relatives affected with breast can- cer. The odds ratio (i.e., relative risk or multiplicative factor for the increase in risk) for this component is es- timated to be 2.22 for women between the ages of 20 and 44 and 1.47 for women between the ages of 45 and 54. Having a second-degree relative with ovarian can- cer was not found to be associated significantly with breast cancer in this study.
Using the estimates in Table 5, one can calculate the risk of developing breast cancer for a woman having a particular pattern of family history relative to that for a woman with no breast cancer in first- and second-de- gree relatives and no ovarian cancer in first-degree rel- atives. Because the control subjects in the Cancer and Steroid Hormone Study were selected randomly from defined geographic areas, they provide useful informa- tion on the frequency with which various patterns of family history occur in the general population. Tables 6 and 7 give, separately for the two age groups, the rela- tive risk for each distinct pattern of family history that occurred at least once in the control group. The relative risks are obtained by multiplying together the bracketed factors for each component of family history that ap- plies to a particular woman. Thus, in Table 6 the value of 4.51 is calculated by multiplying 2.22 X 1.36 X 1.49 to obtain the relative risk for developing breast cancer among women who are between the ages of 20 and 44 and who have one first-degree relative affected with breast cancer (age at onset of 45 or older), two or more

284 CANCER Supplement July 1,1994, Volume 74, No. 3
Table 6. Relative Risk of Breast Cancer According to History of Cancer of the Breast and Ovary in Female Relatives Age 20-44
Family history of breast cancer
First-degree
Onset < 45 yr cancer in first-degree Relative in population Second-degree Family history of ovarian Representation
I+ (2.22). 11.38) 2'13.831 1+[1.36] 2'11.49) relative [1.59] risk (per 1000)
1 .oo 803 X 1.36 128
X 1.59 6 X X 2.03 17 X X 2.17 2
X 2.22 20 X X 3.03 8 X X 3.06 1 1 X X X 4.16 2 X X X 4.51 1 X X X X 6.21 1 X X X X 6.62 < l X X X X 15.96 < I
Total 1.17 1000
Numbers in brackets are the multiplicative factors for increase in risk as listed in Table 5.
Table 7. Relative Risk of Breast Cancer According to History of Cancer of the Breast and Ovary in Female Relatives Age 45-54
Family history of breast cancer
First -degree Second -degree Family history of ovarian Representation
I + Onset <45 yr 2+ I+ 2+ cancer in first-degree relative Relative in population (1.47]* (1.381 (3.831 (2.361 (1.491 (1.591 risk (per 1000)
X
X
X
X
X
X
X
X
X
X
X
X
X X
X
X
X X
X
X
X
X
X X
Total
X
X
X
X
1 .oo 1.36 1.47 1.59 2.00 2.02 2.03 2.16 2.34 2.76 2.99 3.22 4.11 5.64 7.76
16.81 1.15
797 105 4 6
8 12 1 1 13
< 1 < I
2 2
< I I 1 1
< l 1000
Numbers in brackets are the multiolicative factors for increase in risk as listed in Table 5.
second-degree relatives with breast cancer, and no first- degree relative with ovarian cancer. This risk is ex- pressed relative to the risk for women between the ages
of 20 and 44 who have no first- or second-degree rela- tive with breast cancer and no first-degree relative with ovarian cancer. The final column in Tables 6 and 7 is

Genetic Epidemiology of Breast Cancer/ Thompson 285
calculated from the control group and indicates the es- timated number of women per 1000 in the general pop- ulation that has the particular pattern of family history.
The estimates given in Tables 6 and 7 indicate that, although certain patterns of family history are associ- ated with substantial elevations in the risk of breast can- cer, these high risk patterns occur only infrequently in the general population. Even among those women who do have some history of breast cancer in first- or second- degree relatives and/or some history of ovarian cancer in first-degree relatives, the majority have a level of risk that is less than 50% higher than that for women with- out a family history. The last figure given in the final column of each table is an estimate of the magnitude of the incidence for the population as a whole divided by the incidence in the subgroup that has no history of breast cancer in either first- or second-degree relatives and has no history of ovarian cancer in first-degree rel- atives. It is obtained by taking a weighted average of the relative risks listed in that table, with the weights being the proportion of the population having the particular pattern of family history. This estimate can be used to calculate the approximate percentage of all breast can- cer in the population that is attributable to family his- tory. For women between the ages of 20 and 44, this percentage is (1.17-1.00)/1.17, 14.5%, and for women between the ages of 45 and 54, it is (1.15-1.00)/1.15,
These percentages are considerably larger than the recently published and widely cited figure of 2.5% based on prospective data from the Nurses’ Health Study.I5 That figure, however, was obtained from erro- neous calculations, and the appropriate figure is 6.0% (GA Colditz, M.B.B.S. personal communication, 1993). A major basis for the discrepancy between the estimates from the Cancer and Steroid Hormone Study and the estimate of 6.0% from the Nurses’ Health Study is that the latter value is based only on first-degree relatives. It is evident from Tables 6 and 7, however, that although the relative risk is greater when a first-degree relative is affected with breast cancer than when only a second- degree relative is affected, more women in the popula- tion have an affected second-degree relative than have an affected first-degree relative. Consequently, failure to consider the contribution of affected second-degree relatives can lead to substantial underestimation of the total contribution of family history to the incidence of breast cancer in the population as a whole. When infor- mation on only first-degree family members is consid- ered in the Cancer and Steroid Hormone Study, the es- timated percentage is, in fact, close to the figure of 6.0% from the Nurses’ Health Study (7.1% for women be- tween the ages of 20 and 44; 5.3% for women between
13.0 yo.
the ages of 45 and 54). Data from the prospective study by Sellers et a1.16 yield an estimate of 6.1%.
It also should be noted that rather little of the breast cancer occurring in the population is attributable to ovarian cancer in first-degree relatives, because only a small proportion of women in the population have that risk factor. For those women who do, in fact, have such a history, however, it seems to be at least as strong a predictor of breast cancer as is having a second-degree relative affected with breast cancer.
If further studies support the reported familial as- sociation between prostate cancer in males (which is a common cancer) and breast cancer in females, then con- sideration of a family history of prostate cancer may yield estimates appreciably higher than 13.0-14.5?40 for the total percentage of breast cancer that is explicable in terms of family history of cancer. Additionally, some women in the Cancer and Steroid Hormone Study ap- parently underreported breast cancer in second-degree relative^,^ so that the true proportion of women with an affected second-degree relative is probably greater than that indicated in Tables 6 and 7. The true contribution of breast cancer in second-degree relatives to the inci- dence of breast cancer in the population therefore is probably greater than what I have estimated, unless the extent of underreporting of breast cancer in second-de- gree relatives differs for case and control subjects, and the estimates of relative risk used for the calculations thereby have been inflated.
Unfortunately, the Cancer and Steroid Hormone Study4 included only case and control subjects under the age of 55. It would be important to conduct compa- rable multivariable analyses in datasets that include older women.
Clinical Implications
Current knowledge concerning the genetic epidemiol- ogy of breast cancer indicates that, for a sizable minority of the breast cancers that occur in the population, some sort of genetically transmitted susceptibility contributes to their etiology. At the same time, a positive history of breast cancer or certain other malignant neoplasms in family members should not lead to especially great worry on the part of most women and their health care providers. For the majority of women with a family his- tory of breast cancer in first- or second-degree relatives, the elevation in risk is less than 50% higher than the risk for women without a family history. All women, irrespective of their family history, are at a high enough risk for developing breast cancer that screening via mammography and physical examination of the breast should be conducted at appropriate intervals.
The small subgroup of women who are, in fact, at
286 CANCER Supplement July 1, 2994, Volume 74, No. 1
exceptionally high risk for developing breast cancer due to a particularly intense family history pose undeniable dilemmas to the clinician. Although one strategy would be to institute screening for breast cancer at a relatively young age among women at highest risk, the efficacy of mammographic screening in women under the age of 50 has not been established. Prophylactic mastectomy is an extreme measure that conceivably might be con- sidered in situations of incapacitating anxiety about the development of breast cancer, but even in such situa- tions it is not clear that surgery is the most appropriate means for addressing that anxiety. For those women at highest risk, the perceptions of the absolute magnitude of risk may in fact be exaggerated by both the women themselves and their health care providers. The most frequently cited risks for breast cancer are lifetime risks. If the probability of developing breast cancer for women in the general population is approximately lo%, and if a woman is known on the basis of her fam- ily history to have an expected incidence that is several times greater than that of other women, then it may well seem that it is nearly inevitable that the woman will develop the disease. Because the incidence of breast cancer increases with age and because there are differ- ential social and personal impacts of developing a life- threatening disease during later life as opposed to dur- ing midlife, lifetime risks may not be the most appropri- ate means for assessing risk and choosing among al- ternative interventions. Projecting risks over a period of 10-20 years may be more appropriate in many clinical settings.
Once specific genes regulating susceptibility to breast cancer are identified and cloned, the clinical is- sues relating to risk of breast cancer will change dramat- i ~ a l l y . ~ ' , ~ ~ In the years ahead, both genetics and epide- miology, and particularly the interface between the two, undoubtedly will play an increasingly important role in the field of breast cancer.
References
1.
2.
3.
4.
5.
Kelsey JL, Gammon MD. Epidemiology of breast cancer. Epide- miol Rev 1990; 12:228-40. Schwartz AG, King M-C, Belle SH, Satariano WA, Swanson GM. Risk of breast cancer to relatives of young breast cancer patients. / Naf l Cancer I n s f 1985; 75:665-8. Claus EB, Risch N, Thompson WD. Age of onset as an indicator of familial risk of breast cancer. A m / Epidemiol 1990; 131:961- 72. Wingo PA, Ory HW, Layde PM, Lee NC, and the Cancer and Steroid Hormone Group. The evaluation of the data collection process for a multi-center, population-based, case-control study design. Am J Epidemiol 1988; 128:206-17. Sattin RW, Rubin GL, Webster LA, Huezo CM, Wingo PA, Ory HW, et al. Family history and the risk of breast cancer. ] A M 1985; 25311908-13.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
Newman B, Austin MA, Lee M, King M-C. Inheritance of human breast cancer: evidence for autosomal dominant transmission in high-risk families. Proc Natl Acad Sci U S A 1988; 85:l-5. Claw EB, Risch N, Thompson WD. Using age of onset to distin- guish between subforms of breast cancer. A n n Hum Genet 1990;
Claus EB, Risch N, Thompson WD. Genetic analysis of breast cancer in the Cancer and Steroid Hormone Study. A m / Hum Genet 1991; 48932-42. Thompson WD, Schildkraut JM. Family history of gynecologic cancers: relationships to the incidence of breast cancer prior to age 55. Int J Epidemiol 1991; 20595-602. Amos CI, Goldstein AM, Harris EL. Familiality of breast cancer and socioeconomic status in blacks. Cancer Res 1991; 51:1793-7. Claus EB, Risch N, Thompson WD, Carter D. Relationship be- tween breast histopathology and a family history of breast can- cer. Cancer 1993;71:147-53. Lynch HT, Watson P, Conway T, Fitzsimmons SL, Lynch J. Breast cancer family history as a risk factor for early onset breast cancer. Br Cancer Res Treat 1988; 11:263-7. Anderson DE. Genetic study of breast cancer: identification of a high risk group. Cancer 1974; 34:1090-7. Ottman R, Pike MC, King MC, Casagrande JT, Henderson BE. Familial breast cancer in a population based series. A m J Epide- miol 1986; 123:15-21. Colditz GA, Willett WC, Hunter DJ, Stampfer MJ, Manson JE, Hennekens CH, et al. Family history, age, and risk of breast can- cer: prospective data from the Nurses' Health Study. JAMA
Sellers TA, Kushi LH, Potter JD, Kaye SA, Nelson CL, McCovem PG, et al. Effect of family history, body-fat distribution, and re- productive factors on the risk of postmenopausal breast cancer. N EnglJMed 1992; 326:1323-9. Kesseler HJ, Crier WRN, Seidman I, Mcllveen SJ. Bilateral breast cancer. J A M A 1976; 236:278-80. Anderson DE. Breast cancer in families. Cancer 1977; 40:
Anderson DE, Badzioch MD. Risk of familial breast cancer. Cnn- cer 1985; 56:383-7. Anderson DE, Badzioch MD. Bilaterality in familial breast cancer patients. Cancer 1985; 56:2092-8. Sakamoto G , Sugano H, Kasumi F. Bilateral breast cancer and familial aggregations. Prev Med 1978; 7:225-9. Fisher ER, Fisher B, Sass R, Wickerham L. Pathologic findings from the National Surgical Adjuvant Breast Project (protocol no. 4), XI: bilateral breast cancer. Cancer 1984; 54:3002-11. Hislop TG, Elwood JM, Coldman A], Spinelli JJ, Worth A], El- lison LG. Second primary cancers of the breast: incidence and risk factors. Br J Cancer 1984; 49:79-85. Horn PL, Thompson WD. Risk of contralateral breast cancer: as- sociations with factors related to initial breast cancer. A m J Epi- demiol 1988; 128:309-23. Mettlin C, Croghan I, Natarajan N, Lane W. The association of age and familial risk in a case-control study of breast cancer. Am J Epidemiol 1990; 131:973-83. Adami H, Hansen J, Jung B, Rimsten A. Characteristics of famil- ial breast cancer in Sweden: absence of relation to age and uni- lateral versus bilateral disease. Cancer 1981; 48:1688-95. Bailey MJ, Royce C, Sloane JP, Ford HT, Powles TJ, Gazet JC. Bilateral carcinoma of the breast. Br JSurg 1980; 67:514-6. Bernstein JL, Thompson WD, Risch N, Holford TR. The genetic epidemiology of second primary breast cancer. Am J Epidemiol
Rosenblatt KA, Thomas DB, McTiernan A, Austin MA, Stalsberg
54: 169-77.
1993; 270:338-43.
1855-60.
1992; 136:937-48.

Genetic Epidemiology of Breast Cancer/Thompson
H, Stemhagen A, et al. Breast cancer in men: aspects of familial aggregation. ] Natl Cancer Inst 1991; 83:849-54. Easton DF, Bishop DT, Ford D, Crockford GP, and the Breast Cancer Linkage Consortium. Genetic linkage analysis in familial breast and ovarian cancer: results from 214 families. Am ] Hum Genet 1993; 52:678-701.
31. Schildkraut JM, Thompson WD. Relationship of epithelial ovar- ian cancer to other malignancies within families. Genet Epidemiol
32. Cramer DW, Hutchison GB, Welch WR, Scully RE, Ryan KJ, De- terminants of ovarian cancer risk, 1: reproductive experiences and family history. ] Natl Cancer lnst 1983; 71:711-6.
33. Curtis RE, Hoover RN, Kleinerman RA, Harvey EB. Second can- cer following cancer of the female genital system in Connecticut, 1935-82. Nut2 Cancer Inst Monogr 1985; 68:113-37.
34. Storm HH, Ewertz M. Second cancer following cancer of the fe- male genital system in Denmark, 1943-80. Natl Cancer Inst Mo- nogr 1985; 68:331-40.
35. Harvey EB, Brinton LA. Second cancer following cancer of the breast in Connecticut, 1935-82. N a f l Cancer lnst Monogr 1985;
30.
1988; 5~355-67.
68199-112.
287
36. Ewertz M, Mouridsen HT. Second cancer following cancer of the female breast in Denmark, 1943-80. Natl Cancer Inst Monogr
37. Kelsey JL, Fischer DB, Holford TR, LiVolsi VA, Mostow ED, Goldenberg IS, et al. Exogenous estrogens and other factors in the epidemiology of breast cancer. ] Natl Cancer Inst 1981; 67:
38. Anderson DE, Badzioch MD. Breast cancer risks in relatives of male breast cancer patienfs. ]Nut1 Cancer Inst 1992; 84:1114-7.
39. Tulinius H, Eglsson V, Olafsdbttir GH, Signvaldason H. Risk of prostate, ovarian, and endometrial cancer among relatives of women with breast cancer. BM] 1992; 305:855-7.
40. Hosmer D, Lemeshow S. Applied logistic regression. New York: Wiley, 1989.
41. King M-C, Rowel1 S, Love SM. Inherited breast and ovarian can- cer: what are the risks? what are the choices? ] A M 1993; 269:
42. Biesecker BB, Boehnke M, Calzone K, Market DS, Garber JE, Col- lins FS, et al. Genetic counseling for families with inherited sus- ceptibility to breast and ovarian cancer. ] A M 1993; 269:
1985; 68~325-9.
327-33.
1975-80.
1970-4.