Embed Size (px)
Citation preview
8/8/2019 Ged Test Accom App Adhd
http://slidepdf.com/reader/full/ged-test-accom-app-adhd 1/7
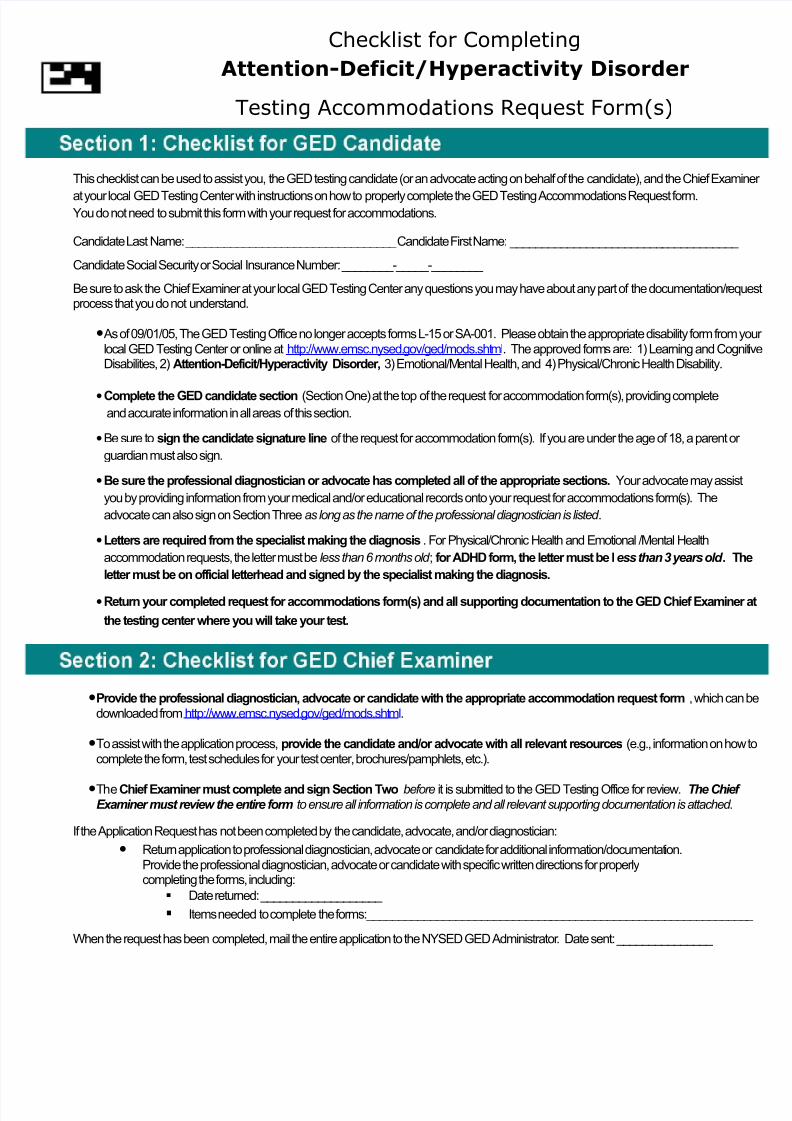
Checklist for Completing
Attention-Deficit/Hyperactivity Disorder
Testing Accommodations Request Form(s)
This checklist can be used to assist you, the GED testing candidate (or an advocate acting on behalf of the candidate), and the Chief Exami
at your local GED Testing Center with instructions on how to properly complete the GED Testing Accommodations Request form.You do not need to submit this form with your request for accommodations.
Candidate Last Name: _________________________________ Candidate First Name: ____________________________________
Candidate Social Security or Social Insurance Number: ________-_____-________
Be sure to ask the Chief Examiner at your local GED Testing Center any questions you may have about any part of the documentation/requprocess that you do not understand.
•As of 09/01/05, The GED Testing Office no longer accepts forms L-15 or SA-001. Please obtain the appropriate disability form from ylocal GED Testing Center or online at http://www.emsc.nysed.gov/ged/mods.shtml. The approved forms are: 1) Learning and CognDisabilities, 2) Attention-Deficit/Hyperactivity Disorder, 3) Emotional/Mental Health, and 4) Physical/Chronic Health Disability.
•Complete the GED candidate section (Section One) at the top of the request for accommodation form(s), providing completeand accurate information in all areas of this section.
•Be sure to sign the candidate signature line of the request for accommodation form(s). If you are under the age of 18, a parent or
guardian must also sign.
•Be sure the professional diagnostician or advocate has completed all of the appropriate sections. Your advocate may assist
you by providing information from your medical and/or educational records onto your request for accommodations form(s). The
advocate can also sign on Section Three as long as the name of the professional diagnostician is listed .
•Letters are required from the specialist making the diagnosis . For Physical/Chronic Health and Emotional /Mental Health
accommodation requests, the letter must be less than 6 months old ; for ADHD form, the letter must be less than 3 years old . Th
letter must be on official letterhead and signed by the specialist making the diagnosis.
•Return your completed request for accommodations form(s) and all supporting documentation to the GED Chief Examine
the testing center where you will take your test.
•Provide the professional diagnostician, advocate or candidate with the appropriate accommodation request form , which candownloaded from http://www.emsc.nysed.gov/ged/mods.shtml.
•To assist with the application process, provide the candidate and/or advocate with all relevant resources (e.g., information on howcomplete the form, test schedules for your test center, brochures/pamphlets, etc.).
•TheChief Examiner must complete and sign Section Two before it is submitted to the GED Testing Office for review. The Chief Examiner must review the entire form to ensure all information is complete and all relevant supporting documentation is attached .
If the Application Request has not been completed by the candidate, advocate, and/or diagnostician:
• Return application to professional diagnostician, advocate or candidate for additional information/documentation.Provide the professional diagnostician, advocate or candidate with specific written directions for properlycompleting the forms, including:
Date returned: ___________________
Items needed to complete the forms:____________________________________________________________
When the request has been completed, mail the entire application to the NYSED GED Administrator. Date sent: _______________

8/8/2019 Ged Test Accom App Adhd
http://slidepdf.com/reader/full/ged-test-accom-app-adhd 2/7
8/8/2019 Ged Test Accom App Adhd
http://slidepdf.com/reader/full/ged-test-accom-app-adhd 3/7
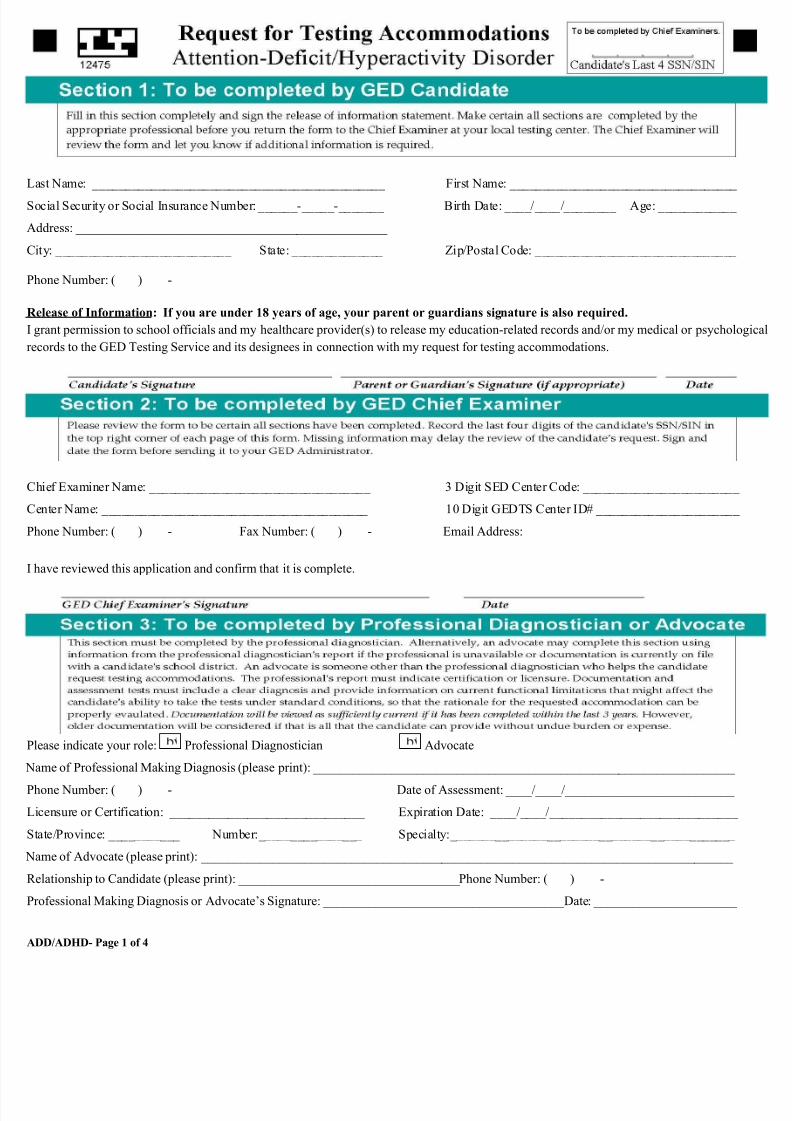
Last Name: _____________________________________________ First Name: ___________________________________
ocial Security or Social Insurance Number: ______-_____-_______ Birth Date: ____/____/________ Age: ____________
Address: ________________________________________________
City: ___________________________ State: ______________ Zip/Postal Code: _______________________________
Phone Number: ( ) -
Release of Information: If you are under 18 years of age, your parent or guardians signature is also required.
grant permission to school officials and my healthcare provider(s) to release my education-related records and/or my medical or psycholo
ecords to the GED Testing Service and its designees in connection with my request for testing accommodations.
Chief Examiner Name: __________________________________ 3 Digit SED Center Code: ________________________
Center Name: _________________________________________ 10 Digit GEDTS Center ID# ______________________
Phone Number: ( ) - Fax Number: ( ) - Email Address:
have reviewed this application and confirm that it is complete.
Please indicate your role: Professional Diagnostician Advocate
Name of Professional Making Diagnosis (please print): _________________________________________________________________
Phone Number: ( ) - Date of Assessment: ____/____/__________________________
Licensure or Certification: ______________________________ Expiration Date: ____/____/_____________________________
tate/Province: ___________ Number:________________ Specialty:____________________________________________
Name of Advocate (please print): __________________________________________________________________________________
Relationship to Candidate (please print): __________________________________Phone Number: ( ) -
Professional Making Diagnosis or Advocate’s Signature: _____________________________________Date: ______________________
ADD/ADHD- Page 1 of 4
8/8/2019 Ged Test Accom App Adhd
http://slidepdf.com/reader/full/ged-test-accom-app-adhd 4/7
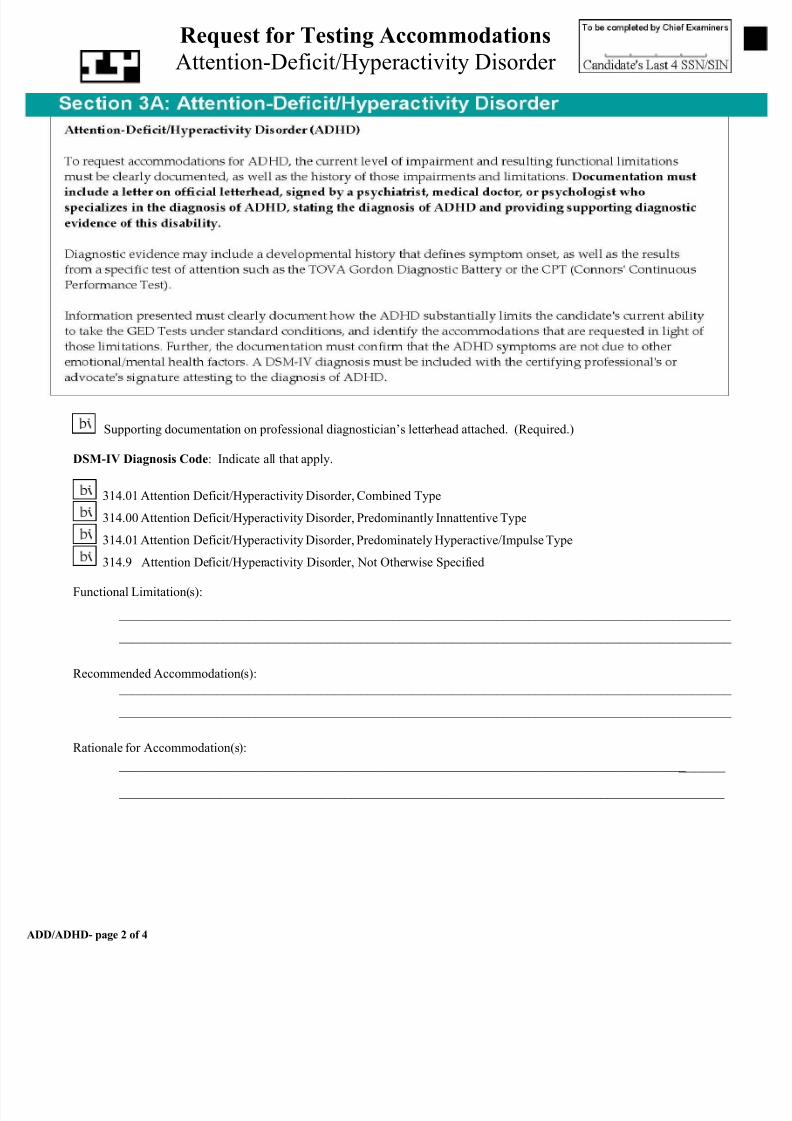
Request for Testing Accommodations
Attention-Deficit/Hyperactivity Disorder
Supporting documentation on professional diagnostician’s letterhead attached. (Required.)
DSM-IV Diagnosis Code: Indicate all that apply.
314.01 Attention Deficit/Hyperactivity Disorder, Combined Type
314.00 Attention Deficit/Hyperactivity Disorder, Predominantly Innattentive Type
314.01 Attention Deficit/Hyperactivity Disorder, Predominately Hyperactive/Impulse Type
314.9 Attention Deficit/Hyperactivity Disorder, Not Otherwise Specified
Functional Limitation(s):
______________________________________________________________________________________________
______________________________________________________________________________________________
Recommended Accommodation(s): ______________________________________________________________________________________________
______________________________________________________________________________________________
Rationale for Accommodation(s):
_______________________________________________________________________________________ ______
______________________________________________________________________________
ADD/ADHD- page 2 of 4

8/8/2019 Ged Test Accom App Adhd
http://slidepdf.com/reader/full/ged-test-accom-app-adhd 5/7
Request for Testing Accommodations
Attention-Deficit/Hyperactivity Disorder
Extended Time (please specify): 1 ½ times 2 times Other:_____________________________________
Audiocassette (tone-indexed) (requires extended testing time, generally double time)
2 times Other: ____________
The use of this accommodation requires practice. Candidates should have an opportunity to practice using an Official G Practice Test, Audiocassette Version prior to the scheduled testing date.
Braille
Scribe
Calculator for Part II
Talking Calculator for entire mathematics test.
Private room
Supervised Breaks (specify in minutes):
Uninterrupted testing time:________ minutes, break time:________ minutes
Other_ _______________________________________________________________________________________
_____________________________________________________________________________________________
_____________________________________________________________________________________________
_____________________________________________________________________________________________
_____________________________________________________________________________________________
_____________________________________________________________________________________________
_____
General Educational Development (GED) Testing Service will not discriminate against candidates for testing on the basis of any legally
rotected characteristic, including, but not limited to, race, color, religion, sex, sexual orientation, pregnancy, marital status, physical or me
isability, age, veteran status, and national origin.
ADD/ADHD – page 3 of 4

8/8/2019 Ged Test Accom App Adhd
http://slidepdf.com/reader/full/ged-test-accom-app-adhd 6/7
Approved for:
Extended Time (please specify): 1 ½ times 2 times Other: ________
Audiocassette (tone indexed) (requires extended testing time, generally double time)
2 times Other: ________
The use of this accommodation requires practice. Candidates should have an opportunity to practice using an
Official GED Practice Test, Audiocassette Version prior to the scheduled testing date.
Braille
Scribe
Calculator for Mathematics part II
Talking calculator for entire Mathematics Test
Private Room
Supervised Breaks (specify in minutes):
Uninterrupted testing time:________ minutes, breaks time:________ minutes
Other__________________________________ __________________________________ _______________
Returned for more information. Date Returned: ____/____/________
Reasons for returning request:
_________________________________________________________________________________________________
_________________________________________________________________________________________________
_________________________________________________________________________________________________
Request forwarded to GEDTS for review (explain reasons below) Date Forwarded: ____/____/________
Reasons for forwarding request to GEDTS for review:
_________________________________________________________________________________________________
_________________________________________________________________________________________________
_________________________________________________________________________________________________
_____________________________ _(518) 474-2801___ __________________
GED Administrator's Signature Telephone Number Date
ADD/ADHD page 4 of 4

8/8/2019 Ged Test Accom App Adhd
http://slidepdf.com/reader/full/ged-test-accom-app-adhd 7/7