Embed Size (px)
Citation preview

British Journal of Ophthalmology, 1985, 69, 443-445
Frontalis sling: a modified simple techniqueS M BETHARIA
From Dr Rajendra Prasad Centre for Ophthalmic Sciences, Ansari Nagar, New Delhi 110029, India
SUMMARY A modified simple technique of brow suspension by using 4-0 Supramid (non-absorbable thread) suture and only one skin incision is described in 25 eyes of 15 cases of ptosis,including cases of congenital and mechanical ptosis and ptosis with Marcus Gunn phenomenon.This technique avoids the use of any special instruments such as the Reese ptosis knife and Wrightneedle.
A sling operation is by far the easiest of all ptosisoperations to perform. Though it may have im-portant disadvantages, such as the risk of lagophthal-mos and lid lag in down gaze, it is the operation ofchoice for certain cases of gross bilateral ptosis withpoor levator function as seen in the blepharophimosissyndrome, cases of mechanical ptosis, and in severeunilateral ptosis covering the pupillary area to pre-vent amblyopia before a definitive levator operationcan be carried out.
Various kinds of material have been used for slingsurgery, including skin muscle flaps, non-absorbablesutures, preserved sclera, reconstituted collagen,Silastic bands, and fascia lata. Bodian' used strips ofhuman sclera successfully, whereas Iliff advocatedthe use of reconstituted collagen. Helveston andWilson3 used strips of sclera woven with 4-0 Supramidfor passing the sling. Tillet and Tillet4 used a siliconesling, and Callahan' used a Silastic band for frontalissuspension. Crawford6 and Fox7 advocated the use offascia lata.Methods of passing the sling have been des-
cribed.' The slings were rhomboidal or pentagonalin shape, and multiple incisions were made during theoperation. Most of these methods are tedious andrequire special instruments such as a fascia latastripper, a Wright needle, and a Reese ptosis knifefor the operation, and they leave ugly scars.
Materials and methods
A modified simple technique of brow suspension isdescribed below which has been carried out success-fully on 25 eyes in 15 cases of blepharophimosis withgross ptosis, mechanical ptosis, and ptosis associatedCorrespondence to Dr S M Betharia, Dr Rajendra Prasad Centre forOphthalmic Sciences, New Delhi 110029, India.
with the Marcus Gunn phenomenon after disinser-tion of levator muscle from the tarsal plate (Table 1).
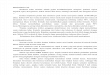
SURGICAL PROCEDUREThe operation is carried out under general anaes-thesia. The first step is to lift the lid with the help ofthe index finger just medial to the centre of the upperlid and observe the contour of the lid margin inrelation to the limbus. This gives an approximate ideaof the place from which the needle has to be passed.A 5 mm wide bite is taken about 4mm away from thelid margin by using a 15 mm curved cutting needlecarrying 4-0 Supramid suture. This bite is takenthrough the orbicularis and the pretarsal tissue(Fig. 1). The needle is taken out and re-enteredthrough the same point from which it has emergedand carried upwards through the plane between theorbicularis and the levator and through the singleincision made above the brow (Figs. 2, 3). The otherarm of the suture is similarly carried through by usinga similar needle which enters through the initialopening made by the needle and is then brought outthrough the incision above the brow (Figs. 4, 5). Asingle knot is first tied, the lid is lifted, and thecontour of the lid margin in relation to the limbusis observed. The tension on the two arms of the
Table 1 Distribution ofcases
Diagnosis No. of Operation donecases
Blepharophimosis syndrome 10 Bilateral slingCongenital ptosis with Marcus 2 Unilateral sling afterGunn phenomenon disinsertion of the
laevatorMechanical ptosis (haemangioma 3 Unilateral slingand neurofibroma)
443
on January 7, 2021 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.69.6.443 on 1 June 1985. Dow
nloaded from

SM Betharia
Fig. 3
Figs. 1 to 8 Steps ofthe modifiedfrontalis sling operation.
Fig. 8
444
Fig. 5 Fig. 6
on January 7, 2021 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.69.6.443 on 1 June 1985. Dow
nloaded from

Frontalis sling: a modified simple technique
operation.
suture is so adjusted that there is no central notchingor ectropion (Fig. 6). Three square knots are tied,and the skin incision is closed with 5-0 black silk(Fig. 7). A modified Frost suture is finally made(Fig. 8).
Results and discussion
Of 15 cases operated upon so far by this techniqueonly one had suture granuloma and infection. The lidlag, which was quite marked at the beginning, wasmuch reduced after three months. The lagophthal-mos was minimal. A good symmetrical lift with agood lid fold was obtained (Figs. 9 to 14). All thecases were followed up postoperatively for three tonine months, average six months.
This method employs only one skin incision asagainst six in Crawford's technique6 of doublerhomboids and five in Fox's method,7 thereby reduc-ing the possibility of scar marks. The central 5 mmbite through the orbicularis and pretarsal tissueeliminates the central notching, while the peripheralparts of the lid on the medial and lateral sides arelifted properly, and the contour of the lid can be
Fig. 11 Showing marked lid lag inearly postoperativeperiod.
Fig. 14 Postoperative photographafter three months showinggoodcorrection in primary gaze.
correctly adjusted by pulling on the two arms of thesuture. A good lid fold and symmetry were achievedby this technique. The lid lag, which was marked inthe initial postoperative period, was reduced to aminimum, and there was minimal lagophthalmos.This method is extremely simple and required nospecial instruments.
References
1 Bodian M. Repair of ptosis using human sclera. AmJ Ophthalmol1968; 65: 352-8.
2 Iliff CE. Surgical management ofptosis. Somerville, NJ: Ethicon,1963: 9-12.
3 Helveston EM, Wilson DL. A suture reinforced scleral sling.Arch Ophthalmol 1975; 93: 643-5.
4 Tillet CW, Tillet GM. Silicone sling in correction of ptosis. Am JOphthalmol 1963; 62: 521-3.
5 Callahan A. Correction of unilateral blepharoptosis with bilateraleyelid suspension. Am J. Ophthalmol 1972; 74: 321-6.
6 Crawford JS. Repair of ptosis using frontalis muscle and fascialata. TransAm Acad Ophthalmol Otolaryngol 1956; 60: 672-8.
7 Fox SA. Complications of frontalis sling surgery. Am J Ophthal-mol 1967; 63: 758-62.
8 Friedenwald JS, Guyton JS. A simple ptosis operation: utilizationof the frontalis by means of a simple rhomboid shaped suture.Am J Ophthalmol 1948; 31: 411-4.
Fig. 9 Preoperative photograph ofacase ofblepharophimosis syndrome.Note the arching ofbrows and wrinkleson theforehead suggestingfrontalisoveraction.
Fig. 12 Showing reduction in the lidlag after three months.
Fig. 10 Early postoperativephotograph showing a goodsymmetrical correction with good lidfold.
Fig. 13 Showing very minimallagophthalmos after the modified sling
445
on January 7, 2021 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.69.6.443 on 1 June 1985. Dow
nloaded from