Embed Size (px)
Citation preview

Journal of the Neurological Sciences xxx (2014) xxx–xxx
JNS-13145; No of Pages 4
Contents lists available at ScienceDirect
Journal of the Neurological Sciences
j ourna l homepage: www.e lsev ie r .com/ locate / jns
Short communication
Four novel connexin 32 mutations in X-linked Charcot–Marie–Toothdisease. Phenotypic variability and central nervous system involvement
Georgia Karadima ⁎, Georgios Koutsis, Maria Raftopoulou, Paraskewi Floroskufi,Karolina-Maria Karletidi, Marios PanasNeurogenetics Unit, 1st Department of Neurology, University of Athens Medical School, Eginition Hospital, Athens, Greece
⁎ Corresponding author at: Neurogenetics Unit, 1National & Kapodistrian University of Athens Medical SchSophias Ave., Athens 11528, Greece. Tel.: +30 21072891
E-mail address: [email protected] (G. Karadima).
http://dx.doi.org/10.1016/j.jns.2014.04.0070022-510X/© 2014 Published by Elsevier B.V.
Please cite this article as: Karadima G, et al, Fand central nervous system involvement, J N
a b s t r a c t
a r t i c l e i n f oArticle history:Received 9 December 2013Received in revised form 3 April 2014Accepted 5 April 2014Available online xxxx
Keywords:Charcot- Marie- ToothCMTXConnexin 32GJB1MutationCNS involvement
Charcot–Marie–Tooth (CMT) disease, the most common hereditary neuropathy, is clinically and geneticallyheterogeneous. X-linked CMT (CMTX) is usually caused by mutations in the gap junction protein b 1 gene(GJB1) coding for connexin 32 (Cx32). The clinical manifestations of CMTX are characterized by significantvariability, with some patients exhibiting central nervous system (CNS) involvement. We report four novelmutations in GJB1, c.191G N A (p.Cys64Tyr), c.508G N T (p.Val170Phe), c.778A N G (p.Lys260Glu) andc.300C N G (p.His100Gln) identified in four unrelated Greek families. These mutations were characterizedby variable phenotypic expression, including a family with the Roussy–Lévy syndrome, and three of themwere associated with mild clinical CNS manifestations.
© 2014 Published by Elsevier B.V.
1. Introduction
Charcot–Marie–Tooth (CMT) disease is a clinically and geneticallyheterogeneous group of hereditary motor and sensory neuropathiesthat cause progressive distal muscle weakness and atrophy, sensoryloss, and decreased or absent tendon reflexes [1]. X-linked CMT(CMTX) is usually caused by mutations in the gap junction protein b 1gene (GJB1) mapped to chromosome Xq13. It typically presentswith an earlier and more severe phenotype in males, while femalesare asymptomatic or oligosymptomatic. Electrophysiologically, itshows mixed features of demyelinating and axonal neuropathy [1].GJB1encodes connexin 32 (Cx32), which belongs to a highly conservedfamily of proteins that form gap junctions in vertebrates. Schwanncells and oligodentrocytes express Cx32, which plays an importantrole in the homeostasis of myelinated axons [2]. Since the first report[3], more than 300 different GJB1 mutations, predicted to affect allregions of the Cx32 protein, have been described [1]. In addition toperipheral neuropathy, several GJB1 mutations have been associatedwith asymptomatic central nervous system (CNS) involvement. Onoccasion, overt clinical symptoms from the CNS have been described [1].
st Department of Neurology,ool, Eginition Hospital, 74 Vas.
18; fax: +30 2107289289.
our novel connexin 32 mutateurol Sci (2014), http://dx.do
We report four novel mutations, c.191G N A, c.508G N T, c.778A N Gand c.300C N G of GJB1 in four Greek families with variable clinicalfeatures and mild clinical CNS manifestations in three of them.
2. Patients and methods
2.1. Patients
Four unrelated Greek families with features suggestive of CMTXwere screened for mutations in GJB1. Family A had 2 affected members,amale proband (A1) and his mother. Family B also had 2 affectedmem-bers, a male proband (B1) and his mother (B2). Family C had 4 affectedmembers, a male proband (C1), his brother, daughter and mother.Family D had one affected member, a male proband (D1).
2.2. Electrophysiological investigation
The median, ulnar, peroneal and sural nerves were repeatedlyexamined with surface electrodes. Electromyography was performedwith concentric needle electrodes.
2.3. Molecular genetic analysis
The 1.4 Mb CMT1A duplication on chromosome 17p was excludedby a long PCR based test [4]. The coding region of GJB1 was screenedfor mutations according to established methods [3]. Sequences wereanalyzed on an ABI310 genetic analyzer. The AccI and BstNI restriction
ions in X-linked Charcot–Marie–Tooth disease. Phenotypic variabilityi.org/10.1016/j.jns.2014.04.007

Table 1Novel GJB1mutations identified in four unrelated Greek families with X-linked Charcot–Marie–Tooth disease.
Family Mutation Protein Domain dbSNP–Ensembl— 1000genomes-EVS
Polyphen-2/SIFTprediction
Frequencycontrols
Segregation withaffected status
Clinical features Variantstatus
A c.191G N A p.Cys64Tyr(p.C64Y)
EC1 Absent Probably damaging/damaging
Not Done Yes X-linked inheritance; Roussy–Lévysyndrome; intermediate CV;CNS involvement
Pathogenic
B c.508G N T p.Val170Phe(p.V170F)
EC2 Absent Benign/Tolerated 0/130 Yes X-linked inheritance; relativelysevere CMT; intermediate CV;CNS involvement
Probablypathogenic
C c.778A N G p.Lys260Glu(p.K260E)
C Absent Benign/Tolerated 0/130 Not checked X-linked inheritance; moderate CMT;intermediate CV
Probablypathogenic
D c.300C N G p.His100Gln(p.H100Q)
IC Absent Possibly damaging/Tolerated
Not Done Yes De novo mutation; moderate CMT;intermediate CV; CNS involvement
Probablypathogenic
EVS: exome variant server; CV: conduction velocities; CNS: central nervous system; CMT: Charcot–Marie–Tooth disease; EC1: first extracellular loop; EC2: second extracellularloop; C: C terminus; IC: intracellular loop.
2 G. Karadima et al. / Journal of the Neurological Sciences xxx (2014) xxx–xxx
enzymeswere used to confirm the c.508G N T and c.778A NGmutationsrespectively. The c.191G N A and c.300C N G mutations did not affect arestriction site.
3. Results
Table 1 summarizes the molecular and clinical characteristics ofthe novel mutations in Cx32 identified. More specifically, type andtopography of amino acid changes, presence in mutation databases,in-silico prediction of pathogenicity, frequency in controls, segregationwith affected status and most salient clinical features are displayed foreach novel mutation. Finally, based on all of the above, a likely variantstatus is attributed to each novel mutation. More detailed clinicalfeatures of each identified family are reported below.
3.1. Family A (c.191G N A, Cys64Tyr)
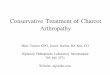
Family A is characterized by severe sensory involvement and whitematter hyperintensity on MRI. The 50 year-old proband reporteddisease onset in his teens with gait unsteadiness and frequent falls.Progression was slow. Examination revealed pes cavus, absent tendonreflexes, distal weakness and atrophy, bilateral foot drop and prominentsensory involvement with severely affected joint position sense,impaired hand use, Romberg sign positive and wide-based gait(Table 2). Electrophysiological findings compatible with severe mixeddemyelinating–axonal sensorimotor neuropathy with intermediatevelocities and absent sensory nerve action potentials (SNAPs) aredisplayed in the Supplementary Table. Brain MRI findings showingdiffuse white matter hyperintensity most prominent posteriorly andinvolving the splenium of the corpus callosum are shown in Fig. 1Aand D. There was no male-to-male transmission in the family. Theproband'smother developed later in life a prominent bilateral and sym-metric limb postural tremor. On examination, she had absent reflexes,prominent sensory involvement and extensor plantars (Table 2).
3.2. Family B (c.508G N T, Val170Phe)
Family B is characterized by a relatively severe neuropathy, whitematter hyperintensity on MRI and mild clinical CNS involvement. The32 year-old proband reported disease onset in childhood with gaitdisturbance and frequent falls. There was significant deteriorationduring adolescence necessitating surgical intervention to correct footdeformity. Examination revealed pes cavus, reduced tendon reflexes,severe distal weakness and atrophy, bilateral foot drop, distal sensoryinvolvement and bilateral extensor plantar reflexes (Table 2). Electro-physiological findings compatible with severe mixed demyelinating–axonal sensorimotor neuropathy with intermediate velocities andabsent SNAPs are displayed in the Supplementary Table. BrainMRIfind-ings showing diffuse white matter hyperintensity most prominentposteriorly and involving the splenium of the corpus callosum are
Please cite this article as: Karadima G, et al, Four novel connexin 32 mutatand central nervous system involvement, J Neurol Sci (2014), http://dx.do
shown in Fig. 1B,E and F. There was no male-to-male transmissionin the family. The proband's mother was oligosymptomatic. On ex-amination, she had pes cavus and reduced tendon reflexes (Table 2).Electrophysiological findings revealed a mixed demyelinating–axonal sensorimotor neuropathy with intermediate velocities(Supplementary Table).
3.3. Family C (c.778A N G, Lys260Glu)
Family C is characterized by amoderate neuropathywith no specificdistinguishing features. The 39 year-old proband reported disease onsetin childhood with gait unsteadiness and frequent falls. Examinationrevealed pes cavus, reduced tendon reflexes, distal weakness and at-rophy and mild distal sensory involvement (Table 2). He could notheel-walk but could manage toe walking with some difficulty.Electrophysiological findings compatible with a mixed demyelinating–axonal sensorimotor neuropathy with intermediate velocities aredisplayed in the Supplementary Table. Brain MRI was not performed.There was no male-to-male transmission in the family. The proband'smother had a similar clinical picture, whereas the brother was moreseverely affected. Neither was available for examination. The proband'sdaughter reportedly had gait disturbance.
3.4. Family D (c.300C N G, His100Gln)
Family D is characterized by a moderate neuropathy with whitematter hyperintensity on MRI and mild clinical CNS involvement. The16 year-old proband reported disease onset in his early teens withgait unsteadiness. Examination revealed pes cavus, mildly increasedtendon reflexes, mild distal weakness and atrophy, mild sensory in-volvement and bilateral extensor plantars (Table 2). Electrophysiologi-cal findings compatible with a mixed demyelinating–axonalsensorimotor neuropathy with intermediate velocities are displayedin the Supplementary Table. Brain MRI showing diffuse white matterhyperintensity most prominent posteriorly is shown in Fig. 1C. Theproband's parents were asymptomatic and normal on neurologicaland electrophysiological examinations.
4. Discussion
Cx32 is a member of the connexin protein family, which formsintercellular channels through which ions and small molecule metabo-lites pass between cells. Cx32 crosses themembrane four times and hasboth its amino and carboxyl-termini on the cytoplasmic aspect of thechannel. Extracellular loops are structurally conserved, with threecysteines in each loop. Mutations predicted to affect all regions of theCx32 protein have been described. To date, all exonic amino acid chang-ing mutations, with one exception, are thought to be pathogenic [1,5].Studies in cell culture and transgenic mice show that GJB1 mutationscan cause a loss of channel function, gain of toxic effects or both on
ions in X-linked Charcot–Marie–Tooth disease. Phenotypic variabilityi.org/10.1016/j.jns.2014.04.007

3G. Karadima et al. / Journal of the Neurological Sciences xxx (2014) xxx–xxx
myelinating Schwann cells, with resulting peripheral nerve degenera-tion [6]. Expression studies in paired Xenopus oocytes support thehypothesis that CMTX is a disease that arises due to either partial orcomplete loss of function of Cx32 [7].
The four novel missense GJB1 mutations identified either affectidentical codons (p.Cys64Tyr, and p.His100Gln) or are closely located(p.Val170Phe, and p.Lys260Glu) to other known mutations associatedwith CMTX [8–11]. They also co-segregate with affected family mem-bers in 3 of the 4 families and are not known polymorphisms(Table 1). Furthermore, two (p.Val170Phe, and p.Lys260Glu) werefound to be absent from controls. The remaining two that couldnot be checked in controls (p.Cys64Tyr, and p.His100Gln) had CNSwhite matter involvement known to characterize CMTX, as had thep.Val170Phe mutation [12]. Similar diffuse white matter changes havebeen previously reported in CMTX patients [13–15]. The posteriorpredominance of the hyperintensity and the specific involvement ofthe corpus callosum have also been previously noted in CMTX [16].Furthermore, clinical features that suggest the pathogenicity of thefour novel mutations include, beyond the characteristic CMT phenotype(all families) and MRI findings (families A, B and D), the evidence ofX-linked inheritance (families A, B and C), the finding of mixeddemyelinating–axonal neuropathy with intermediate conductionvelocities on nerve conduction studies (all families) and the signsof pyramidal tract involvement (families A, B and D). Therefore,given all of the above, despite the in-silico prediction of a tolerable-benign nature for two of the mutations (p.Val170Phe, p.Lys260Glu),there is substantial evidence that all four novel mutations are causa-tive of the CMTX phenotype in our patients.
In family A, the G to A transition in codon 64 results in an amino acidsubstitution (Cys64Tyr) in the first extracellular loop of connexin 32.The substitution of the small in size cysteine by the hydrophobic,aromatic and bigger in size tyrosine, possibly results in reduced mem-brane stability and modified channel function. This family had two
Table 2Summary of examination findings in Greek patients with novel GJB1mutations.
Family (mutation) A (c.191G N A, Cys64Tyr) B (c.508G N
Patient A1a A2b B1a
Age at examination (yrs) 50 66 32Pescavus Yes Yes YesHammer toes Yes Yes YesTendon reflexesUpper limbsLower limbs (knee/ankle)
−−
−−
++/−
Weakness upper limbsProximalDistal
−++
−−
−+++
Weakness lower limbsProximalDistal
−+++
−−
−+++
Atrophy upper limbsProximalDistal
−++
−+
−+++
Atrophy lower limbsProximalDistal
−++
−+
−+++
Sensory involvement upper limbsPinprickVibrationPosition sense
++++++
+++++
−−−
Sensory involvement lower limbsPinprickVibrationPosition sense
++++++++
+++++++
−++−
Plantar response Flexor Extensor ExtensorPostural upper limb tremor − +++ −Romberg's sign Yes Yes –
Wide-based gait Yes Yes –
−: absent; +: mild (in the case of tendon reflexes, reduced); ++: moderate (in the case of tea Proband.b Proband's mother.
Please cite this article as: Karadima G, et al, Four novel connexin 32 mutatand central nervous system involvement, J Neurol Sci (2014), http://dx.do
intriguing features. Firstly, the clinical presentation suggestive of theRoussy–Lévy syndrome, particularly in the mother, a finding that hasonly rarely been reported with other GJB1 mutations [17]. Secondly,the CNS involvement on brain MRI, which has not been reported inprevious mutations affecting the same codon [9,11].
In family B, the G to T transversion in codon 170 resulted in an aminoacid exchange (Val to Phe) in the second extra cellular domain of theprotein. The bigger size of the phenylalanine and its aromatic sidechain may provoke dysfunction of the extracellular loop bindinginvolvement. The intriguing features about this family were the rela-tively severe clinical picture of the proband requiring surgical interven-tion, and the CNS involvement that was both seen on MRI and detectedon neurological examination (extensor plantars). It is interesting thatthe only reported exonic polymorphism in GJB1was in the same nucle-otide position (c.508G N A, p.Val170Ile) [1,5]. The authors supporteda non-pathogenic status for this variant based on non-segregationwith disease status (present in the proband's healthy, both clinicallyand electrophysiologically, father), on in-silico prediction and onthe stereochemical similarity of the wild-type and mutated aminoacids (Val to Ile) [5]. However, it is noteworthy that the c. 508G N Apolymorphism was not present in 200 controls and has not beenreported in variation databases.
In family C, the A to G transition in codon 260 resulted in anamino acid exchange (Lys260Glu) in the C-terminus domain. Lysine ispositively charged instead of glutamic acid that is negatively charged.Thismutationmay change the overall charge of Cx32 and possibly affectthe ability of gap junctions to regulate the intracellular signalingcascades that favor the survival and myelination of axons. There wereno specific distinguishing clinical features in this family. The possibilityof sub-clinical CNS involvement was not further investigated.
In family D, the C to G transversion in codon 100 resulted in anamino acid exchange (His to Gln) in the second intra cellular domain.A basic amino acid, histidine, is substituted by the polar amino acid
T, Val170Phe) C (c.778A N G, Lys260Glu) D (c.300C N G, His100Gln)
B2b C1 D151 39 16Yes Yes YesYes Yes –
++/−
++/−
++++++
−−
−+
−−
−−
−+
−+
−−
−++
−+
−−
−++
−+
−−−
−−−
−−−
−−−
++−
−+−
Flexor Flexor Extensor− − −– – –
– – –
ndon reflexes, normal); +++: severe (in the case of tendon reflexes, increased).
ions in X-linked Charcot–Marie–Tooth disease. Phenotypic variabilityi.org/10.1016/j.jns.2014.04.007

Fig. 1. BrainMRI of patients with novel GJB1mutations and asymptomatic CNS involvement. A–C: Axial FLAIR or T2 sequences at the level of the centrum semiovale of probands with thec.191G N A (A), the c.508G N T (B) and the c.300C N G(C) mutations demonstrating diffuse white matter hyperintensity, most prominent posteriorly. D, E: Sagittal T2 sequences ofprobands with the c.191G N A (D) and the c.508G N T (E) mutations demonstrating hyperintensity at the splenium of the corpus callosum. F: Axial T2 sequence of the proband withthe c.508G N T mutation also demonstrating hyperintensity at the splenium of the corpus callosum.
4 G. Karadima et al. / Journal of the Neurological Sciences xxx (2014) xxx–xxx
glutamine. The alteration of the protein's charge may affect the forma-tion of functional gap junctions. The intriguing feature about this familywas the CNS involvement that, as in family B, was both seen on brainMRI and detected on neurological examination (extensor plantars).This has not been previously reported in mutations affecting the samecodon [8,10].
In conclusion, four novel Cx32mutations are presented, which causea spectrum of clinical manifestations more or less characteristic ofCMTX, including polyneuropathy of varying severity, Roussy–Lévysyndrome, and mild clinical CNS manifestations in three families. Thisspectrum of mutations and phenotypes is compatible with the geneticand clinical heterogeneity that characterizes CMTX and may contributeto the elucidation of the pathogenetic pathways involved in the disease.Furthermore, the identification of new CMTX causing mutations is acrucial step for carrier detection and pre-symptomatic diagnosis.
Supplementary data to this article can be found online at http://dx.doi.org/10.1016/j.jns.2014.04.007.
Conflict of interest
None.
References
[1] Reilly MM, Murphy SM, Laurá M. Charcot–Marie–Tooth disease. J Peripher Nerv Syst2011;16:1–14.
[2] Abrams CK, Freidin MM, Verselis VK, Bennett MV, Bargiello TA. Functionalalterations in gap junction channels formed by mutant forms of connexin 32:evidence for loss of function as a pathogenic mechanism in the X-linked form ofCharcot–Marie–Tooth disease. Brain Res 2001;900:9–25.
[3] Bergoffen J, Scherer SS,Wang S, Scott MO, Bone LJ, Paul DL, et al. Connexinmutationsin X-linked Charcot–Marie–Tooth disease. Science 1993;262:2039–42.
Please cite this article as: Karadima G, et al, Four novel connexin 32 mutatand central nervous system involvement, J Neurol Sci (2014), http://dx.do
[4] Stronach EA, Clark C, Bell C, Lofgren A, McKay NG, Timmerman V, et al. Novel PCR-based diagnostic tools for Charcot–Marie–Tooth type 1A and hereditary neuropathywith liability to pressure palsies. J Peripher Nerv Syst 1999;4:117–22.
[5] Brozková D, Mazanec R, Haberlová J, Sakmaryová I, Subrt I, Seeman P. Six new gapjunction beta 1 gene mutations and their phenotypic expression in Czech patientswith Charcot–Marie–Tooth disease. Genet Test Mol Biomark 2010;14:3–7.
[6] Kleopa KA, Abrams CK, Scherer SS. How do mutations in GJB1 cause X-linkedCharcot–Marie–Tooth disease? Brain Res 2012;1487:198–205.
[7] Weber PA, Chang HC, Spaeth KE, Nitsche JM, Nicholson BJ. The permeability of gapjunction channels to probes of different size is dependent on connexin compositionand permeant-pore affinities. Biophys J 2004;87:958–73.
[8] Bone LJ, Deschenes SM, Balice-Gordon RJ, Fischbeck KH, Scherer SS. Connexin32 andX-linked Charcot–Marie–Tooth disease. Neurobiol Dis 1997;4:221–30.
[9] Bort S, Nelis E, TimmermanV, Sevilla T, Cruz-Martínez A,Martínez F, et al.Mutationalanalysis of the MPZ, PMP22 and Cx32 genes in patients of Spanish ancestry withCharcot–Marie–Tooth disease and hereditary neuropathy with liability to pressurepalsies. Hum Genet 1997;99:746–54.
[10] Sorour E, Upadhyaya M. Mutation analysis in Charcot–Marie–Tooth disease type 1(CMT1). Hum Mutat Suppl 1998;1:S242–7.
[11] Young P, Grote K, Kuhlenbäumer G, Debus O, Kurlemann H, Halfter H, et al. Mutationanalysis in Chariot–Marie Tooth disease type 1: point mutations in theMPZ gene andtheGJB1 gene cause comparable phenotypicheterogeneity. J Neurol 2001;248:410–5.
[12] Scherer SS, Kleopa KA. X-linked Charcot–Marie–Tooth disease. J Peripher Nerv SystSuppl 2012;3:9–13.
[13] Panas M, Karadimas C, Avramopoulos D, Vassilopoulos D. Central nervous systeminvolvement in four patients with Charcot–Marie–Tooth disease with connexin 32extracellular mutations. J Neurol Neurosurg Psychiatry 1998;65:947–8.
[14] Kassubek J, Bretschneider V, Sperfeld AD. Corticospinal tract MRI hyperintensity inX-linked Charcot–Marie–Tooth disease. J Clin Neurosci 2005;12:588–9.
[15] Mazzeo A, Di Leo R, Toscano A, Muglia M, Patitucci A, Messina C, et al. Charcot–Marie–Tooth type X: unusual phenotype of a novel CX32 mutation. Eur J Neurol2008;15:1140–2.
[16] Paulson HL, Garbern JY, Hoban TF, Krajewski KM, Lewis RA, Fischbeck KH, et al.Transient central nervous system white matter abnormality in X-linked Charcot–Marie–Tooth disease. Ann Neurol 2002;52:429–34.
[17] Senderek J, Hermanns B, Bergmann C, Boroojerdi B, BajboujM, HungsM, et al. X-linkeddominant Charcot–Marie–Tooth neuropathy: clinical, electrophysiological, andmorphological phenotype in four families with different connexin32 mutations. JNeurol Sci 1999;167:90–101.
ions in X-linked Charcot–Marie–Tooth disease. Phenotypic variabilityi.org/10.1016/j.jns.2014.04.007