Embed Size (px)
Citation preview

Recommendations for the Use of Genome‐Wide Sequencing for Undiagnosed Rare Genetic Diseases in Ontario
Page 1
FINAL REPORT
UseofGenome‐WideSequencingforUndiagnosedRareGeneticDiseasesinOntario
From the Working Group for the Use of Genome‐Wide Sequencing forUndiagnosed Rare Genetic Diseases in Ontario, commissioned by theGeneticTestingAdvisoryCommittee.
TheWorkingGrouprecommends:
1) The application of the herein criteria for the use of genome‐wide sequencing for undiagnosed rare genetic diseases inOntario.• Based on The clinical application of genome‐widesequencing for monogenic diseases in Canada: PositionStatement of the Canadian College ofMedical Geneticists(Boycottetal.JMedGenet2015)
2) That genome‐wide sequencing for undiagnosed rare geneticdiseases be publically funded inOntario, based on the hereinclinical criteria, testing recommendations and process for theevaluation of longer‐term patient outcomes supported by arobustdatacapturesystem.
December2016
Note:ThispublicationistechnicalinnatureandisavailableinEnglishonlyduetoitslimitedtargetedaudience.ThispublicationhasbeenexemptedfromtranslationundertheFrenchLanguageServicesAct.
Remarque:Cettepublicationestdenaturetechniqueetestdisponibleenanglaisuniquementenraisondesonpublicciblelimité.CettepublicationaétéexemptéedelatraductionenvertudelaLoisurlesservicesenfrançais.

Recommendations for the Use of Genome‐Wide Sequencing for Undiagnosed Rare Genetic Diseases in Ontario
Page 2
AboutTheGeneticTestingAdvisoryCommittee
New genetic tests are being rapidly developed and promoted as high tech tools toimprove diagnostic medicine and facilitate patient treatment. A formal evaluationprocessisrequiredtoassessthevalidityandeffectivenessofnewandexistinggeneticteststobettermanagehealthcarespending.
TheGeneticTestingAdvisoryCommittee(“GTAC”)wasestablishedinApril2014withathreeyearmandatetoreviewtheclinicalutilityandvalidityofgenetictestsandprovideadvice to theMinistryofHealthandLong‐TermCare (“ministry”)on theprovisionofgenetic tests inOntario. The creation of GTAC is in keepingwith the direction of theExcellentCare forAllAct and theOntarioActionPlan forHealthCare to promote thedelivery of high‐quality health care based on the best available scientific and clinicalevidence.
ThepurposeofGTACistoreviewandprovidereportsonexistingandnewgenetictests.These reports, in addition to other factors (e.g. implementation feasibility, availablefundingandresources,system level impacts,andsocialandethical factors)willguidetheministry’sdecision‐makingonpublicfundingofgenetictestsinOntario.
ReviewProcess
The evaluation process for a genetic test is determined by whether the test is to beprovidedinOntarioorthroughtheOut‐of‐Country(OOC)ProgramExceptionalAccessprocess.
GeneralStreamProcess:OntarioGeneticTests
1. Genetictestselection2. Evidence‐basedanalysis
a. Literature review of clinical and academic publications on thegenetictest
b. Referraltoanexpertsub‐committeec. GTACdeliberationoftheavailableevidence
3. DraftGTACreportandrecommendationprepared4. PostingdraftinOpenforComment5. Assessmentofstakeholder/publiccomments6. PostingoffinalizedGTACreportandrecommendations
ExceptionalAccessProcess:OOCGeneticTest
1.OOCgenetictestapplication/submission2.AssigntoappropriateGTACmemberforevaluationandrecommendation3.OOCResponsetorequestingphysician.
WebsiteEnglish:http://www.health.gov.on.ca/en/pro/programs/gtac/French:http://www.health.gov.on.ca/fr/pro/programs/gtac/default.aspx

Recommendations for the Use of Genome‐Wide Sequencing for Undiagnosed Rare Genetic Diseases in Ontario
Page 3
TableofContents
1. WorkingGroupObjectives...................................................................................................................4
2. ExecutiveSummary.................................................................................................................................5
3. DetailedRecommendations.................................................................................................................6
a. Recommendationsfordiagnosticassessment.....................................................................6
b. Pre‐testrecommendations...........................................................................................................8
c. Recommendationsforsecondaryfindings.........................................................................10
d. Clinicaltestingandresultsreportingrecommendations.............................................11
e. Post‐testrecommendations......................................................................................................13
f. Outcomemeasures........................................................................................................................14
AppendixI.Forms...........................................................................................................................................15
AppendixII.FrameworkforEvaluatingtheIntroductionofGenome‐WideSequencinginOntario.......................................................................................................................................16
AppendixIII.References..............................................................................................................................19
AppendixIV.WorkingGroupMembership.........................................................................................20

Recommendations for the Use of Genome‐Wide Sequencing for Undiagnosed Rare Genetic Diseases in Ontario
Page 4
1. WorkingGroupObjectives
ToassistGTACinthereviewoftheclinicalutilityandvalidityofagivengenetictestandafter a test prioritization process, GTAC convened a Working Group to developstandardized criteria to guide clinicians in the use of genome‐wide sequencing forundiagnosedraregeneticdiseasesinOntario.
The Working Group was tasked with taking the recommendations outlined in Theclinical application of genome‐wide sequencing for monogenic diseases in Canada:Position Statementof theCanadianCollegeofMedicalGeneticists (Boycott etal. JMedGenet 2015) and adapting them to provide implementation guidance, consideringfactors such as clinical care/pathway recommendations, diagnostic precision andclinical utility, cost, test sensitivity, test specificity, and the approach to secondaryfindings.
GTACwouldliketothanktheWorkingGroup(seeAppendixIV)fortheirdiligenceandhardworkincreatingthisreport.
The followingreportcaptures theworkinggroup’srecommendationsand itscontentshavebeenreviewedandapprovedbyGTAConSeptember16,2016.

Recommendations for the Use of Genome‐Wide Sequencing for Undiagnosed Rare Genetic Diseases in Ontario
Page 5
2. ExecutiveSummary
Genome‐wide sequencing, defined as any approach that analyzes and annotates DNAvariants on a genome‐wide scale, is an appropriate test to facilitate a diagnosis in apatientwithasuspectedrarediseaseincertaincircumstances.Approachesrelevanttotherecommendationsoutlinedhereinincludeclinomesequencing(verylargepanelthatincludes all genes listed in OMIM and associatedwith human disease), whole exomesequencing (WES; protein coding portions of the genome), and whole genomesequencing (WGS). Regardless of the approach, clinical genome‐wide sequencing, atthis time, should be used to interrogate the genome for nucleotide sequencevariants in genes known to cause disease; variants that are not relevant to thepatient’s primary indication for diagnostic evaluation, may also be identified.Nucleotidesequencevariantsingenesnotknowntobeassociatedwithdiseasewillnotbereported.
Recommendations include: (1) clinical genome‐wide sequencing is an appropriateapproach in the diagnostic assessment of a patient forwhom there is suspicion of asignificantmonogenicdiseasewhere thebaseline evaluationhasbeen completed andthe results will directly impact clinical decision‐making and care for the individualand/orfamilybeingtested;(2)giventhecomplexityofinterpretationandcounselling,clinicalgenome‐widesequencingshouldonlybeorderedbyphysicianswithsufficientexpertiseinuseofthetechnologyincludingprovisionofgeneticcounsellingandabilitytoobtain informed consent; (3)until thebenefitsof reporting secondary findings areestablished, the identification of secondary findings should follow guidelinesestablished by MOHLTC, using a consensus list of medically‐actionable genes that iscontinuouslyreviewed,updated,andinformedbyoutcomedata;(4)clinicalsequencing,interpretation, and reportingmust be performed in an accredited clinical laboratoryandfollowtherecommendationsoutlinedherein;(5)newdiagnoseswillbesharedwiththe patient alongside standard‐of‐care genetic counselling and all patients should begiven the option of having coded genome‐wide and phenotypic data deposited andstored in an international database to enable genomic discovery; and, (6) this testshouldbeintroducedintoclinicalcarealongsidearobustevaluativeprocesstooptimizethe quality and ensure appropriate use of genome‐wide sequencing. Finally, theserecommendationswillberoutinelyre‐evaluatedasknowledgeofdiagnosticandclinicalutilityofclinicalgenome‐widesequencingimproves.

Recommendations for the Use of Genome‐Wide Sequencing for Undiagnosed Rare Genetic Diseases in Ontario
Page 6
3. DetailedRecommendations
a. Recommendationsfordiagnosticassessment
1.1 Clinicalgenome‐widesequencing,atthistime,shouldbeusedtointerrogatethegenome for nucleotide sequence variants in genes known to cause disease.ClinicalWEScannotbeusedatthistimetoreliablydetectcopynumbervariantsor structural variation. Clinical WGS may be used to detect copy numbervariantsandstructuralvariationinadditiontosequencevariants, though it isnotcurrentlyafirsttiertestforsuchanalyses.
1.2 Given the complexity of interpretation and counselling, clinical genome‐widesequencing with open analysis should only be ordered by physicians withsufficientexpertiseinuseofthetechnologyasdefinedby:a. Abilitytodeterminewhetherclinicalgenome‐widesequencingisthetestof
choiceforthespecificclinical indication,takingintoaccountothergenomicavailable non‐genomic tests (such as microarray or metabolic tests) andmutationsthatwillnotbedetectedbythistechnology(suchastrinucleotiderepeats);and,
b. Abilitytoprovideadequatepre‐testcounseling,includinginformedconsentforprimaryandsecondaryfindings;and,
c. Ability to interpret the results of the clinical genome‐wide sequencing,includingsecondaryfindings,andprovideadequatepost‐testcounselling.
1.3 Clinical genome‐wide sequencing is considered medically necessary for aphenotypicallyaffected individualwhenALLthreeof the followingconditionsaremet:
a. Baseline evaluation has been completed (e.g. phenotyping, family history,pretestgeneticcounsellingandconsentand,where indicated, chromosomemicroarray,targetedtestingincludingbiochemicaltesting)
b. Results will directly impact clinical decision‐making and care for theindividual and/or family being tested. We assume that all diagnoses willprovide an opportunity for anticipatory guidance and enable access toservicesandsupport.Inaddition,resultsmustbeanticipatedtomeetoneormoreofthefollowingcriteria:i. Will likelypreclude further invasive diagnostic investigations, follow‐
up,orscreeningthatwouldberecommendedintheabsenceoftesting;ii. Provides specific and informed reproductive decision making and
familyplanning;or,iii. Willenable identificationofatrisk familymembers to identify if they
carry the causativemutation and facilitate early intervention or,willenabletheabilitytoruleoutrisktofamilymembers,thusavoidinglongtermmonitoring.
c. A genetic etiology is the most likely explanation for the phenotype,supportedbyaclinicalpresentationthatincludesanyoneofthefollowing:i. Moderatetoseveredevelopmentalorfunctionalimpairment;ii. Multisysteminvolvement;iii. Progressive clinical course which cannot be explained by another
cause;or,iv. Differential diagnosis includes two or more conditions (clinical and
genetic heterogeneity) that would require evaluation by separatepanels and therefore genome‐wide sequencing is the more cost‐effectiveapproachthanindividualgeneorgenepaneltesting.

Recommendations for the Use of Genome‐Wide Sequencing for Undiagnosed Rare Genetic Diseases in Ontario
Page 7
ANDthepatientdoesnotmeetanyofthefollowingexclusioncriteria:
a. The following clinical indications are NOT an indication for genome‐widesequencing:i. Isolatedmildintellectualdisabilityorlearningdisabilities;ii. Nonsyndromicautism;iii. Isolatedneurobehavioural disabilities (e.g. attentiondeficit disorder);
and,iv. Isolated neuropsychiatric conditions (e.g. schizophrenia, bipolar
disease,Tourettesyndrome)
b. Patient’sphenotypeishighlyspecifictoaknowngeneticconditionforwhichoptimized genetic testing (including genetic panel testing) exists; in thisinstance the targeted gene panel should be given priority if it is moresensitive (e.g. Noonan spectrum disorders). In addition, suspectedaneuploidy,methylationdefects,ortrinucleotiderepeatdisorderswouldnotqualifyforclinicalgenome‐widesequencing.
c. Previouscomprehensivepaneltestinghasbeencompletedinthelast3years(panel contained virtually all known genes for that clinical indication). Atthis time, clinical genome‐wide sequencing is not funded as a reflex testwhentheappropriatepanelhasnotyieldedamoleculardiagnosis.Ifapaneldidnotrevealadiagnosisinthepast3yearsbutthereisastrongargumenttobemade for clinicalgenome‐widesequencing, thisapplicationwouldbereviewed by an expert panel and justification must be made for the testindication.
d. Baseline evaluation (physical examination, investigations) has not beencompletedfortheclinicalindication[see1.3(a)].
e. A likely non‐genetic etiology has been identified to explain the symptoms(e.g.environmentalexposures,injury,orinfection).
1.4 Testing should always include the affected individual. In discussionwith theclinical laboratory, additional affected relatives or unaffected parents, ifavailable, may be analyzed concurrently to facilitate and improve variantinterpretation.Wesuggestthefollowingapproaches:o TriosarethepreferredstrategyforWESforundiagnosedpatientswithno
familyhistoryofsimilarlyaffectedindividuals.o Inthecontextofconsanguinity,asingletonapproachispreferred.o Inthecontextofpresumedrecessiveinheritance,oneaffectedindividual
and an unaffected parent OR two affected individuals is the preferredapproach.
o In the context of presumed dominant inheritance, the analysis ofadditional affected individuals may significantly reduce the number ofpotentially deleterious heterozygous variants; concurrent testing of themost distantly related and available affected family member shouldthereforebeconsidered..
o IfX‐linkedinheritance isclear,asingletonapproachwith filteringforX‐linkedvariantsispreferred.
o If a mitochondrial genome mutation is suspected, the mitochondrialgenome should be analyzed directly using alternate andmore sensitiveapproaches.
1.5 Limited evidence currently exists supporting the use of genome‐widesequencingintheprenatalsetting.Specificguidelinesforpre‐natalindicationsmustthereforebedevelopedwhensufficientevidencehasbecomeavailable.Intheinterim,requestsforclinicalgenome‐widesequencinginthissettingwouldrequireevaluationforappropriatenessbytheExceptionalAccessprocess.
1.6 Post‐mortem genome‐wide sequencing may be indicated if the affectedproband meets the inclusion/exclusion criteria outlined in this document,regardlessofageofdeath(prenatal,pediatric,oradult).

Recommendations for the Use of Genome‐Wide Sequencing for Undiagnosed Rare Genetic Diseases in Ontario
Page 8
b. Pre‐testrecommendations
2.1 Standard clinical assessment, including detailed phenotyping, must beundertakenanddocumentedprior to testing to facilitate interpretationof thegenome‐wide variants. Phenotyping should be documented using thestandardized nomenclature of Human Phenotype Ontology. Suchdocumentationmustbeforwardedtothelaboratoryintheformatpreferredbythe lab (laboratory specific requisition and/or software such as Phenotips(https://phenotips.org;Girdea,2013,etc.).
2.2 Priortotesting,geneticcounsellingforthepatient/familymustbeundertakenanddocumentedinthemedicalrecordbyaqualifiedhealthcareproviderwithathoroughunderstandingofclinicalgenome‐widesequencing,includingissuesunique to both pediatric and adult patients. Informed consent should beformally documented prior to testing, utilizing the program specific consentform.Thisconsentformshouldbecomepartofthepatientmedicalrecord.
2.3 Documentation of informed consent and preferences regarding secondaryfindingsmustbedocumentedonthelaboratoryrequisition.
2.4 Thecounsellingandconsentprocess should includebutnotbe limited to thefollowingitems:o Briefdescriptionofthetestandtherationaleforoffering,tailoredtothe
informationneedsofthepatient/family;o Informationregardingthelimitationsofthetestmethodology;o Informationregardingthepossibilityofsecondaryfindings.o Discussionofexpectedoutcomesandwhatwill,andwillnot,bereported
fromthetest,including:• variant classes (i.e. pathogenic, VUS, benign) related to genes
relevanttotheprimaryclinicalfindings;• Secondary findings and the choices pertaining thereto with
documentationofpatientpreferences;o Possible (or definite) need for unaffected parental or family member
samplesandthetypeofanalysisrequired;clinicalgenome‐wideanalysisor follow‐up Sanger testing. Unaffected family members should beinformed that if their sample is to undergo genome‐wide analysis it isonly to interpret the clinical significance of the variants in the probandpotentiallyrelatedtotheclinicalindication.Independentreportswillnotbe issued for unaffected family members and analysis for secondaryfindings will not be undertaken. Any follow‐up of secondary findingsidentified in the proband and possible impact on family membersrepresentdistincthealthcareinteractions;
o Potential implications of test results on issues such as medical care,possibleinsuranceanddiscrimination,impactforotherfamilymembers,recommendationsforcascadetestingforfamilymembers,etc;
o An explanation ofwhatwill happenwith data, including how long theywillbestoredaspertheguidelinesofthelaboratory;
o Potential for reinterpretation of variants or re‐analysis of data for theprimaryindication(shouldadiagnosisremainlacking)andhowthiswilloccur. Thiswould involve a new requisition and consent process at therequestofthehealth‐careprovider.
o Consentforclinicaltestingshouldfollowstandardguidelinesandincludesufficienttimetounderstandanddecidewhetherornottoproceedwithgenome‐widetesting.
2.5 All patients/families should be aware that they must opt out of havinganonymizedgenotypicandhigh‐levelphenotypicdatadepositedandstoredinaninternationaldatabasetoassistininterpretationofdisease‐causingvariants.

Recommendations for the Use of Genome‐Wide Sequencing for Undiagnosed Rare Genetic Diseases in Ontario
Page 9
2.6 Allpatients/familiesshouldbegiventheoptionofhavingcodedgenome‐wideand phenotypic data deposited and stored in an international database toenable genomic discovery. The release of genome‐wide sequencing data forsecondaryusewouldrequireadistinctconsentthatwouldwaivelaboratoriesofresponsibilitybeyondwhattheyhaveincludedintheirclinicalreport. Thisconsentwouldbeobtainedandprovidedbythereferringclinician/institution.
2.7 All patients/families should be given the opportunity to enroll in current orfutureresearchstudiestounderstandtherelationshipofgenome‐widevariantsfound in them and disease pathogenesis. The release of patientmaterials forfunctionalstudieswouldrequireadistinctconsentthatwouldbeobtainedandprovidedbythereferringclinician/institution.

Recommendations for the Use of Genome‐Wide Sequencing for Undiagnosed Rare Genetic Diseases in Ontario
Page 10
c. Recommendationsforsecondaryfindings
Therecommendationssetouthereinrefertoanalysisofgenome‐widesequencingdatathat includes all clinically relevant genes (e.g.OMIM,Orphanet, other curated set), asdefinedbythelaboratory.Atpresent,thereportingofsecondaryfindings(alsoreferredto as incidental findings, additional findings) remains a controversial issue. This isprimarilyduetothelackofempiricknowledgeregardingthedownstreampsychosocialand clinical impact (i.e. potential benefits and risks) of gaining such knowledge forpatients/families and on the health care system as well as difficulty in interpretingthesevariantsintheabsenceofpersonalandfamilyhistoryofpotentiallyrelatedsignsand symptoms. Consequently, until the benefits of reporting secondary findings areestablished,acautiousapproachisrecommended.
3.1 The MOHLTC should support the development of a working group that willdevelop and maintain a consensus list of medically‐actionable genes to bereported by Ontario‐based laboratories. This review of this list will beinformedbydatacollectedandanalyzedaspartofSectionf(6.4).
3.2 Onlypathogenicandlikelypathogenicvariantsingenesfromthisconsensuslistwill be reported for secondary findings in the proband.Variants of uncertainsignificanceWILLNOTbereported.Genome‐widedatafromunaffectedfamilymembers generated for the purpose of interpreting variants identified in theproband will NOT be analyzed for secondary findings. Carrier status forconditionsunrelatedtotheprimarytestindicationWILLNOTbereported.
3.3 Follow‐up of secondary findings in the proband and at risk family memberswouldrepresentadistincthealthcareinteraction.
3.4 A process for obtaining informed consent and for communicating potentialsecondary findingsmustbe inplace(seeSectionb). Thereturnofsecondaryfindings,andtheoptionspertainingtheretoareasfollows:a. Competentaffectedindividualsshouldbegiventheoptionpriortotestingto
receive (or not receive) secondary findings unrelated to the primary testindication.
b. In children deemed not competent to participate in meaningful decisionmaking (i.e. too young or intellectually disabled), secondary results thatreveal risk for a highly‐penetrant condition that is medically‐actionableduring childhood should be reported to the parents. A child’s risk formedically‐actionable adult‐onset genetic conditions should not becommunicated unless: (1) the parents request such disclosure; AND, (2)disclosureofthe informationcouldpreventseriousharmtothehealthofaparentorfamilymember,asdeterminedonacase‐by‐casebasis.Thereisnoobligation to re‐contact pediatric patients as adults to let them know ofpotentially later onset monogenic diseases. However, parents/guardiansshouldbeencouragedtosharetestresultswiththeirchildrenatappropriatetimepoints.
c. For incompetent adults, results revealing a highly‐penetrant medically‐actionable condition should be reported to the legal representative, unlessthe incompetent adult explicitly refused to receive such actionable resultswhilestillcompetent.
3.5 Prior to disclosure of medically actionable secondary variants,patients/families should be given the opportunity to affirm or deny theirprevious decision to learn of secondary findings. Disclosure of secondaryvariantsshouldbestagedaccordingtothewishesofthepatient/family(i.e.atappointmentsubsequenttodiscussionofvariantsrelatedtoprimaryfindings);however, some discretionmust be undertaken by the clinician based on thepotentialurgencyofthesecondaryvariant.

Recommendations for the Use of Genome‐Wide Sequencing for Undiagnosed Rare Genetic Diseases in Ontario
Page 11
d. Clinicaltestingandresultsreportingrecommendations
4.1 Clinical sequencing, interpretation and reporting must be performed in aclinicallaboratorylicensedwithintheappropriatejurisdictiontoperformthesetests. Licensing and accreditationdetails should be includedon the report orreadilyavailablefromthelaboratorywebsite.
4.2 Requests for sequencing must be accompanied by relevant family history,detailed phenotypic information on the patient, in standardized HPO terms(collected by the laboratory requisition or software such as PhenoTips), anddetailsofanyrelevantpreviousgenetictesting.
4.3 Laboratoriesreportingresultsbasedongenome‐widesequencing,mustincludespecific information describing the sequencing methodology used (includingtest sensitivity, reagent kit version numbers, instrumentation used), theanalytical pipeline (including its limitations), and the approach to analysis.Supplemental information should include a reference to the list of genesexamined, and any relevant regions routinely not covered by the sequencingmethodologythathavenotbeenaddressedbySangersequencing.
4.4 Patientspecificcoverageforaparticulargene,orsetofgenes,mustbeavailableuponrequest.
4.5 Allreportsshouldclearlystate the testdescription;reason forreferral; result(Positive Negative, Inconclusive); DNA findings; interpretations;recommendation; background information (in relation to the reason forreferralandforotherDNAfindingsincludedonthereport);testmethodologies;and, references. Background information should includemode of inheritance,carrier status, risk toother familymembers,diseasepresentation/phenotype,asappropriate.
4.6 DNA findings above should include, at minimum, the cDNA position andnucleotide change (according toHGVSnomenclature)with the correspondingreference sequence version (NM number); the amino acid change; theclassification of the DNA variant (according to published guidelines, such asACMG2015);and,thezygosity.ThegDNApositionandnucleotidechangewiththe corresponding genome reference or build is optional. The significance ofalternative transcripts with multiple transcript designations must also beconsidered.
4.7 The laboratory report for clinical genome sequencing must include aninterpretation by a clinically trained and certified PhD or MD MolecularGeneticist; in Canada, this would typically be one with CCMG or ABMGcertification.When appropriate, consultation with the referring clinician onvariant interpretation in the context of the clinical presentation is stronglyadvised.
4.8 Interpretation of results should include assessment of current peer‐reviewedliterature,predictivesoftwareanddatabasesofknownvariation,andtakeintoaccounttheknownlimitationsoftheseresources.Interpretationshouldfollowstandardpublishedguidelines(Lerner‐Ellis,2015).
4.9 Ininstanceswhereunaffectedfamilialsamples(i.e.,parentsintrioanalysis)areanalyzedtohelp interpret thepatient’ssequencingdata,separatereportswillnotbegeneratedandsampleswillnotbeanalyzed individually forsecondaryfindings. Evidence ofmisassigned paternity, incest, etc., should be dealt withfollowingcurrentprinciplesandinstitutionalpolicies.
4.10 Secondaryfindings,ifpresent,shouldbeinaseparatesectionfromtheprimaryfindingsandindicatethereportingguidelinesbeingfollowed.

Recommendations for the Use of Genome‐Wide Sequencing for Undiagnosed Rare Genetic Diseases in Ontario
Page 12
4.11 Release of patient genome‐wide data for further analysis is case specific andsuchsecondaryuseofdatawillrequiresadistinctresearchconsentandthelabwillnotreleasedataunlessthereisdocumentationofthisconsentandaSOPinplacefordatatransfer.
4.12 The MOHLTC should enable a process for accreditation and external qualityassurance of Ontario labs conducting genome‐wide sequencing tests. Thisincludes,butisnotlimitedto,settingstandardsfor,andongoingevaluationof,technical performance characteristics, analytical quality, and reporting ofresults.

Recommendations for the Use of Genome‐Wide Sequencing for Undiagnosed Rare Genetic Diseases in Ontario
Page 13
e. Post‐testrecommendations
5.1 The ordering clinician should review the report and place the findings intocontextwithotherrelevantmedicalconsiderationswhendiscussingtheresultswiththepatient/family.
5.2 The patient (and family when appropriate) must receive standard‐of‐caregeneticcounsellingandmanagementregardinganynewdiagnosis.
5.3 Thelaboratorymustprovideaccesstoexpertconsultationontheinterpretationofavariantifrequestedbythereferringclinician.
5.4 Thelaboratorymaysuggestthatadditionallaboratory‐baseddiagnosticfollowup is required to verify the genome‐wide sequencing findings (including atargetedtest;CNVtestormethylationspecifictest,inclusionofparentsorotherunaffectedoraffectedfamilymembers).
5.5 In the case in which the laboratory identifies multiple candidate variants,additional literature review, database searching, and phenotyping should beconsideredbytheorderingclinician.
5.6 Ifnopathogenicvariantisidentified,patientsshouldbecounselledthat:o DNA variant may still be present that was not detectable using the
sequencingmethod.o Further analysis might lead to a diagnosis at a later date when more
knowledge is available. This may involve re‐testing rather than re‐analysis, at the discretion of the laboratory.TheWG recommends thattheministryestablishcriteriaforboththefrequencyandfundingforthisre‐analysis. Requests forre‐analysisof thesequencingdatashouldbeinitiatedbyareferringphysician.Twotypesofre‐analysismayoccur:1)a single‐geneanalysismotivatedbyanovelgenediscoveryassociatedwith the phenotype or a new phenotypic finding that broadens thedifferentialdiagnosis; or, 2) a full re‐analysis. Thedecision to re‐analyzemustbebasedonexpansionofgeneticknowledgespecificforthedisease(pertinent to phenotype), time since last analysis, clinical presentation,andmanagementimplicationsforthepatientandfamily.
o Further analysis of the sequencing data through research may be anoption. Acleardistinctionshouldbemadebetweenclinicalandresearchanalysis, and explicit informed consent obtained for the latter, includingthat research test results would need to be confirmed in an approvedlaboratoryprior to being used to guidemedicalmanagement. If furtherresearch analysis is initiated the clinical laboratory will release theappropriatedataatthedirectionofthepatient;thedatamightbereleasedto thepatientora3rdpartyexplicitlydelegatedby thepatient (clinician,researcher,familymember,etc.).
5.7 Thelaboratorywillretainpatientdata(VCFfile)foraperiodofatleast3yearstoallowreanalysisorresearchinvestigation.

Recommendations for the Use of Genome‐Wide Sequencing for Undiagnosed Rare Genetic Diseases in Ontario
Page 14
f. Outcomemeasures
6.1 To optimize the quality and ensure appropriate use of genome‐widesequencing, it is essential to introduce this test into clinical care alongside arobust evaluative process. The proposed evaluation is characterized as aservice‐orientedqualityimprovementprocess.
6.2 Resources required to establish and sustain an outcomes‐oriented datainfrastructureshouldbeprovidedbyMOHLTC. Opportunities forMOHLTCtopartner with key stakeholders (e.g. Ontario Genomics Institute, GenomeCanada, Health Quality Ontario) to sustain and expand this infrastructureshouldbeactivelysought.
6.3 Theproposedevaluationprocess is framework‐drivenand is informedby the‘chainofevidence’concept,whichassistswithconnectingtheuseofthetesttoclinically important health or healthcare‐related outcomes (Appendix II).Fryback and Thornbury’s hierarchical model best articulates appropriateintermediate outcomes to evaluate genome‐wide sequencing by including‘diagnosticthinkingefficacy’and‘therapeuticefficacy’ascoredomains.
6.4 To capture these outcomes, a user‐friendly data collection tool should bedeveloped. The Efficacy Form (Appendix I) serves as an example of a datacollection tool thatcouldbeused tosupport theproposedevaluation. PartAwould be completed at the time that clinical genome‐wide sequencing isorderedandasksorderingclinicianstoindicatewhattheirdiagnosticcareplanfor the index casewouldbe if sequencingwasnotavailable.PartBwouldbecompleted following the disclosure of sequencing results to the index familyandasksclinicianstoindicate:(a)whattypeofsequencingresultwasidentifiedin the index case (i.e. Diagnosis, No Diagnosis, Partial Diagnosis, and/orSecondary Finding); (b) whether the sequencing result influenced diagnosticthinking;and,(c)howtheclinicalcareplanwasguidedbysequencingresult(s).PartAofthisformwouldtake<2minutestocompleteandPartBwouldtake<5minutestocomplete;cliniciansshouldbeincentivizedtocompletetheseforms.
6.5 The data collection tool should be centralized, electronic, andmandatory. Allclinical settings that participate in clinical genome‐wide sequencing shouldhave access to a shared external data capture portal and should enteroutcomes‐oriented data (defined by the data collection tool) on an ongoingbasis. Interim analyses should be conducted (annually) to recalibrate theprovincialgenomicsequencingstrategytooptimizeitsdelivery.
6.6Thisprocessandstructuredevelopedhereinshouldbesustainedandleveragedforfutureprovincial/nationalPrecisionMedicineinitiatives.

Recommendations for the Use of Genome‐Wide Sequencing for Undiagnosed Rare Genetic Diseases in Ontario
Page 15
AppendixI.Forms
Sectiona:RecommendationsforDiagnosticAssessment
Form1:PatientCriteriaforGenome‐WideSequencing
Sectionf:OutcomeMeasure
Form2:EfficacyForm

Recommendations for the Use of Genome‐Wide Sequencing for Undiagnosed Rare Genetic Diseases in Ontario
Page 16
AppendixII.FrameworkforEvaluatingtheIntroductionofGenome‐WideSequencinginOntario
A.TheEvaluationFrameworkA number of evaluation frameworks have been used for synthesizing the publishedevidence about the accuracy and utility of genetic tests. Some of these include: theEvaluation of Genomic Applications in Practice and Prevention frameworks (EGAPP),the Analytic validity; Clinical validity; Clinical utility; and Ethical, legal, and socialimplicationsframework(ACCEmodel),theFryback‐Thornburymodel,andtheUSPSTFframework for screening. All four frameworks cover three common domains ofevaluation: analytic validity, clinical validity, and clinical utility of the test. The ACCEframeworkand theFryback‐Thornburymodelextend todimensions that reflectuponcost and societal impact of the test (Figure 1: A comparison of key evaluationframeworks forclinical tests).Unliketheothermodels, theFryback‐Thornburymodelalsoattendstothenotionsofdiagnosticthinkingandtherapeuticefficacy.
Figure 1. A comparison of key evaluation frameworks for clinical tests

Recommendations for the Use of Genome‐Wide Sequencing for Undiagnosed Rare Genetic Diseases in Ontario
Page 17
B.LevelsofEfficacy
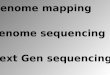
Table 1. Fryback and Thornbury hierarchical model of efficacy~ ·
Level 1: Technical Efficacy In the laboratory setting, does the test measure what it purports to measure?
Level 2: Diagnostic Accuracy Efficacy
What are the medical test characteristics of the test (e.g ., sensitivity, specificity)?
Does the test result distinguish patients with and without the ta rget disorder among patients in whom it is clinically reasonable to suspect that the disease is present?
Level 3: Diagnostic Thinking efficacy Does the medical test help cl inicians come to a diagnosis?
Does the test change clinician's pretest estimate of the probability of a specific disease?
Level 4: Therapeutic Efficacy Does the medical test aid in planning treatment?
Does the medical test change or cancel planned treatments?
Level 5. Patient Outcome Efficacy Do patients benefit from the use of the test?
Do patients who undergo this medical test fare better than similar patients who are not tested?
Level 6. Societal Efficacy Cost- benefit and cost-effectiveness
• Level1:TechnicalEfficacy(i.e.analyticvalidity) refers to theabilityofgenome‐widesequencingtoaccuratelyandreliablymeasurethecharacteristicitisintendedtomeasure(e.g.,thepresenceofagenemutation).Analyticvalidityisafunctionofmanyfactors,suchasanalyticaccuracy,precision,analyticsensitivityandspecificity,reportable range of test results for the test system, reference range, or normalvalues. These performance parameters will be monitored by participatinglaboratoriesinaccordancewithstandardlaboratoryprocedures.
• Level2:DiagnosticEfficacy (i.e.clinicalvalidity) refers to the abilityofCGES topredict the presence of absence of a clinical condition or predisposition. Thisperformance parameter will be monitored by participating laboratories inaccordance with standard laboratory procedures. As per published literature, adiagnostic rate of 30%will be applied as our provincial benchmark (Yang, 2014;Yang,2015;Lee,2014;Soden,2014).
• Levels 3: Diagnostic Thinking Efficacy. In the clinical context, patients’ healthoutcomescannotbeaffectedbyagenetictestresultunlesstheattendingclinicianisled todosomethingdifferent thanwouldhavebeendonewithout the informationprovided by the test (i.e. decisional impact). Similarly, the clinician’s choice ofmanagement should not change unless something has changed in the diagnosticthinking,allother thingsequal.Asanalternative todecisional impact, genetic testresult may have non‐decisional but still important impact by changing thedifferential diagnosis, strengthening an existing hypothesis, or reassuring theclinician that a speculated diagnosis has or has not been confirmed. An empiricapproach to ascertaining diagnostic thinking efficacy forWES is presented in theEfficacy Form (Appendix I). Benchmarks cannot be predetermined. This processwillassistindefiningbenchmarksgoingforward.
• Level 4: Therapeutic efficacy (i.e. clinical utility). A genetic test result mayinfluencetheclinician’sdiagnosticthinkingandsubsequently,haveanimpactonthepatient’sclinicaltrajectoryofcare.Theintentofthecareplanwilltypicallybetiedtothetypeofgenetictestresult.Whenadiagnosticvarianthasbeenidentified,careplansmaybe tailored to suitprognoses thatarebetterdefined (e.g. sub‐specialistreferrals, imaging or surveillance plans, medication implications, family membertesting, reproductive planning,). When no variant or a variant of uncertaindiagnosticsignificancehasbeenidentified,careplansmaybetailoredtowardsmoreextensivediagnosticinvestigations(e.g.musclebiopsies,additionalgeneticanalyses,family member testing). For the purpose of the proposed evaluation process, apre/post test design will enable a description of care plans triggered by WEScomparedtostandardcare(EfficacyForm).Benchmarkscannotbepredetermined.Thisprocesswillassistindefiningbenchmarksgoingforward.

Recommendations for the Use of Genome‐Wide Sequencing for Undiagnosed Rare Genetic Diseases in Ontario
Page 18
• Levels5:PatientOutcomeEfficacy‘Improvedhealth’canbedefinedandmeasuredinmanydifferentways(e.g.reducedmorbidity,increasedlifeexpectancy,improvedquality of life, reduced pain, reduced number of invasive procedures). Patientoutcomesresearchenablesadeterminationofthewaysinwhichtheexpectedcostofanintervention(i.e.genetictest)canbeweightedagainstexpectedbenefits(e.g.improvedqualityoflife,reducednumberofinvestigations)andassuch,canbeusedasarationalguideforpayers,clinicians,andpatientstodecideaboutwhetherornotto reimburse,order,orpursue (respectively)aparticular intervention (i.e. genetictest)inthefirstplace.PatientoutcomesresearchisoutofscopeforthepurposeoftheproposedWESevaluation,butthedatainfrastructurethat iscreatedshouldbeforward thinking and flexible in order to accommodate such research in the nearfuture.Benchmarks:N/Aatthistime
• Level6:SocietalEfficacy.Thequestionofsocietalefficacygoesbeyondthequestionof individual risks and benefits. It poses questions of acceptability and resourceallocation.Itaskswhetherthecostfortheuseofagivengenetictestisacceptable–to society as awhole ‐ even though individual patientsmaybenefit. Questionsofbenefit‐risk trade‐offs, ethical considerations, and resource allocation featureherein. Whilesocietalefficacywillbean implicitconsiderationover thecourseofthe proposedWES evaluation process, fulsome consideration of this elementwilloccuratalaterstage.Benchmarks:N/Aatthistime.
D.Limitations• The trajectory of care that is captured by this process will reflect a projected
trajectory; it will not reflect actual resources consumed (i.e. health care dollarsspent).
• Thetrajectoryofcarethatiscapturedwillreflectuponaprospectivewindowof6‐12months as this is the characteristic follow‐up period for childrenwho receiveroutinecare fromtertiarycaregeneticscentres. Itwillnotcapturerecommendedservicesforthelongerterm.
• Health/functional outcomes will not be captured by this tool; only intermediateoutcomesrelatedtodiagnosticandtherapeuticefficacywillbecapturedatthispointintime.
E.Deliverables• Aconceptualmodeltailoredtotheevaluationofgenomediagnostics.• Acentralized,datacapturesystemanddatacollectionprotocolsuitedtolong‐term
evaluationandensuringqualityofgenomediagnosticsinOntario.Thisprocessandstructureshouldbesustainedandleveragedforfutureprovincial/nationalPrecisionMedicineinitiatives.
• Preliminary evidence that reflects upon the technical, diagnostic and therapeuticefficacyofgenome‐widesequencingasadiagnostic tool for raregeneticdisordersandwillbeusedtoinformtheimplementationofclinicalgenome‐widesequencinginOntario.
• Ateamoflaboratoryscientists,clinicians,andevaluationscientistswell‐positionedto expand the proposed evaluation concept and design to other provincial andnationalcentresforthepurposeofongoingqualityimprovementandresearch.

Recommendations for the Use of Genome‐Wide Sequencing for Undiagnosed Rare Genetic Diseases in Ontario
Page 19
AppendixIII.References
GirdeaM,DimitriuS,FiumeM,BowdinS,BoycottKM,ChenierS,ChitayatD,FaghfouryH,Meyn,MS,RayPN,SoJ,StavropoulosDJ,BrudnoM.PhenoTips:PatientPhenotypingSoftwareforClinicalandResearchUse.HumMutat2013;34:1057‐65.
GreenRC,BergJS,GrodyWW,KaliaSS,KorfBR,MartinCL,McGuireAL,NussbaumRL,O'Daniel JM,OrmondKE,RehmHL,WatsonMS,WilliamsMS,BieseckerLG,AmericanCollege of Medical Genetics and Genomics. ACMG recommendations for reporting ofincidental findingsinclinicalexomeandgenomesequencing.GenetMed2013;15:565‐74.
Lee H, Deignan JL, Dorrani N, Strom SP, Kantarci S, Quintero‐Rivera F, Das K, Toy T,HarryB,YourshawM,FoxM,FogelBL,Martinez‐AgostoJA,WongDA,ChangVY,ShiehPB,PalmerCG,DippleKM,GrodyWW,VilainE,NelsonSF.ClinicalexomesequencingforgeneticidentificationofrareMendeliandisorders.JAMA2014;312:1880‐7.
Lerner‐Ellis J,WangM,White S, LeboMS;CanadianOpenGeneticsRepositoryGroup.CanadianOpenGeneticsRepository (COGR):Aunifiedclinicalgenomicsdatabaseasacommunityresourceforstandardisingandsharinggeneticinterpretations.JMedGenet2015;52:438‐45.
SodenSE,SaundersCJ,WilligLK,FarrowEG,SmithLD,PetrikinJE,LePichonJB,MillerNA, Thiffault I, Dinwiddie DL, Twist G, Noll A, Heese BA, Zellmer L, Atherton AM,AbdelmoityAT,SafinaN,NypSS,ZuccarelliB,Larson IA,ModrcinA,HerdS,CreedM,Zhaohui Y, Yuan X, Brodsky RA, Kingsmore SF. Effectiveness of exome and genomesequencingguidedbyacuityof illness fordiagnosisofneurodevelopmentaldisorders.SciTranslMed2014;6:265ra168.
Sun F, Bruening W, Erinoff E, Schoelles KM. Addressing Challenges in Genetic TestEvaluation. Evaluation Frameworks and Assessment of Analytic Validity. MethodsResearchReport(PreparedbytheECRIInstituteEvidence‐basedPracticeCenterunderContractNo.HHSA290‐2007‐10063‐I.)AHRQPublicationNo.11‐EHC048‐EF.Rockville,MD: Agency for Healthcare Research and Quality. June 2011. Available at:www.effectivehealthcare.ahrq.gov/reports/final.cfm.
YangY,MuznyDM,ReidJG,BainbridgeMN,WillisA,WardPA,BraxtonA,BeutenJ,XiaF,NiuZ,HardisonM,PersonR,BekheirniaMR,LeducMS,KirbyA,PhamP,ScullJ,WangM, Ding Y, Plon SE, Lupski JR, Beaudet AL, Gibbs RA, Eng CM. Clinical whole‐exomesequencingforthediagnosisofmendeliandisorders.NEJM2013;369:1502‐11.
YangY,MuznyDM,XiaF,NiuZ,PersonR,DingY,WardP,BraxtonA,WangM,BuhayC,VeeraraghavanN,HawesA,ChiangT,LeducM,BeutenJ,ZhangJ,HeW,ScullJ,WillisA,LandsverkM,CraigenWJ,BekheirniaMR,Stray‐PedersenA,LiuP,WenS,AlcarazW,CuiH,WalkiewiczM,Reid J, BainbridgeM, PatelA, BoerwinkleE, BeaudetAL, Lupski JR,Plon SE, Gibbs RA, Eng CM.Molecular Findings Among Patients Referred for ClinicalWhole‐ExomeSequencing.JAMA2014;312:1870‐9.

Recommendations for the Use of Genome‐Wide Sequencing for Undiagnosed Rare Genetic Diseases in Ontario
Page 20
Remarque: Cette publication est de nature technique et est disponible en anglais uniquement en raison de son public cible limité. Cette publication a été exemptée de la traduction en vertu de la Loi sur les services en français.
Note: This publication is technical in nature and is available in English only due to its limited targeted audience. This publication has been exempted from translation under the French Language Services Act.
AppendixIV.WorkingGroupMembership
Dr.KymBoycott,Children’sHospitalofEasternOntario(Chair)Dr.SarahBowdin,HospitalforSickChildrenDr.DennisBulman,Children’sHospitalofEasternOntarioDr.PraneshChakraborty,Children’sHospitalofEasternOntarioDr.JordanLerner‐Ellis,MtSinaiHospitalDr.RobinHayeems,HospitalforSickChildrenDr.SharanGoobie,LondonHealthSciencesCentreDr.PeterRay,HospitalforSickChildrenMs.CherylShuman,HospitalforSickChildren

vR.1
December 2016 Form 1: Patient Criteria for Genome‐Wide Sequencing
MOHLTC Process for Approval of Whole‐Exome Sequencing
Background: Whole‐exome sequencing (WES) is a useful diagnostic test in a number of clinical scenarios for patients with known or suspected genetic disease. The Genetic Testing Advisory Committee (GTAC) to the Ontario Ministry of Health and Long‐term Care was tasked with taking the recommendations outlined in The clinical application of genome‐wide sequencing for monogenic diseases in Canada: Position Statement of the Canadian College of Medical Geneticists (Boycott et al. J Med Genet 2015) and providing implementation guidance for the province of Ontario, considering factors such as diagnostic precision, cost, test sensitivity, test specificity, and ultimate impact on health outcomes. Guidelines were developed on the basis of evidence to facilitate clinical translation of this technology and contribute to best practices in Ontario. The clinical indications we outline here will evolve over time as more data are generated and at this time the following criteria for approval should be considered provisional. Data will be requested regarding outcomes of the test for your patient and your cooperation in providing this information will contribute to these evolving best practices.
Approval Process:
• The accompanying form was developed to reflect the developed guidelines for approval of clinical WES. This form must be completed and accompany the application to the MOHTLC.
• If the OOC health services are received without written prior approval from the ministry, then the services are not eligible for reimbursement and all costs associated with these services will be the sole responsibility of the patient.
• If the approval criteria are not met for a particular patient, the case will be reviewed by the Exceptional Access Committee of GTAC and additional information will be requested for this deliberation.
• At this time WES is NOT funded as a reflex test when the appropriate genetic panel has not yielded a molecular diagnosis. If a panel test was negative in the past 3 years but there is a strong argument to be made for WES at this time, please attach a letter justifying the need for WES and this will be reviewed by the Exceptional Access Committee of GTAC.
Laboratory and Analysis Approach: Testing should always be done on the affected individual.
Additional affected relatives or unaffected parents, if available, may be analyzed concurrently to facilitate and improve variant interpretation. We suggest the following approaches:
• Trios are the preferred strategy for WES for undiagnosed patients with no family history of similarly affected individuals.
• In the context of consanguinity, a singleton approach is preferred.
• In the context of recessive inheritance, one affected individual and an unaffected parent OR two affected individuals is the preferred approach.
• If X‐linked inheritance is clear, a singleton approach with filtering for X‐linked variants is preferred.
• If a mitochondrial genome mutation is suspected, the mitochondrial genome should be analyzed directly using alternate and more sensitive approaches.
Options if WES is Unrevealing: If the clinical presentation of your patient is not explained after clinical WES you can consider the following:
• Request re‐analysis of the data in 1 years time.
• With appropriate consent, share your patient’s phenotypic data, candidate gene and/or WES data with one of the many global sharing initiatives for unsolved rare diseases (e.g. PhenomeCentral; www.phenomecentral.org).
At this time WGS is NOT funded by the MOHLTC as either a primary or reflex test.

Form 1: Patient Criteria for Genome‐Wide Sequencing December 2016
vR.1
PRIVATE & CONFIDENTIAL
Please complete this eligibility form and the pre‐test form and send it along with your application for OOC funding requesting clinical WES.
RE: patient Information sticker here
Please confirm that clinical WES is indicated and appropriate for your patient.
Patient must meet one or more from Clinical Presentation AND Management Impact (check all that apply) Clinical Presentation:
Moderate to severe developmental or functional impairment Multisystem involvement Progressive clinical course Differential diagnosis includes two or more conditions that would be evaluated in separate panels
Management Impact: Will limit further invasive diagnostic investigations Results allow for specific and informed reproductive decision making Will enable identification of at risk family members and facilitate early intervention
AND
I confirm that: o Detailed phenotypic characterization (physical examination, investigations) has occurred and is
documented. o Pretest genetic counseling and consent has been completed. o Chromosomal microarray has been completed and does NOT explain the patient’s phenotype (for
patients with developmental delay, intellectual disability, multiple congenital anomalies, dysmorphic features).
o Other causative circumstances (e.g. environmental exposures, injury, and infection) do NOT explain the patient’s clinical presentation.
o Previous targeted testing unrevealing (*if specific monogenetic disorder suspected). o Previous comprehensive panel testing has NOT been in completed in the last 3 years (panel contained
virtually all known genes for that clinical indication).
I confirm that the patient does NOT have: o Isolated mild intellectual disability or learning disabilities; o Nonsyndromic autism; o Isolated neurobehavioural disabilities (e.g. attention deficit disorder). o A phenotype highly specific to a known genetic condition for which optimized genetic panel testing exists.
If so, then the targeted gene panel should be given priority assuming it is more sensitive (e.g. Noonan spectrum disorders).

Form 1: Patient Criteria for Genome‐Wide Sequencing December 2016
vR.1
__________________________________________
______________________________________________
_____________________________ ___________________________
__ __ __ __ __ __
I am requesting: Singleton and rationale
Trio and rationale
I confirm that I am a physician in Ontario practicing in Medical Genetics with: 1. Expertise in performing a clinical genetics evaluation including family history, genetic‐focused medical
history and physical examination, and have a critical understanding of prior genetic evaluations. 2. Expertise in determining whether clinical WES is the test of choice for the specific clinical indication,
prioritizing other available tests as appropriate. 3. Expertise in providing adequate pre‐test counseling, including informed consent for primary and
incidental findings. 4. Ability to interpret the results of the clinical WES and provide adequate post‐test counseling.
I confirm that I will participate in the evaluation strategy of clinical WES for my patient by completing the outcomes data collection form at the time the results are shared with my patient/family.
Physician Signature: Date:
CSN #

December 2016 Form 2: Efficacy Form_vR.1
Part A: Complete at time of WES request
Q1. Patient’s diagnostic care plan Check all tests that
have been
performed
Check all tests that
you would request
if WES was not
available at this
point
Laboratory tests:
Cytogenetic testing (specify):
Molecular testing (specify):
Metabolic testing (specify):
Medical imaging:
MRS (specify):
MRI (specify):
CT (specify):
U/S (specify):
X‐Ray (specify):
Skeletal Survey:
Bone Age:
Echo:
Other (specify):
Invasive procedures:
Skin biopsy
Muscle biopsy
Nerve biopsy
Other (specify):
Other:

Form 2: Efficacy Form_vR.1 December 2016
_______________________________
PART B: Post‐WES care plan
Q1. WES result Diagnosis No diagnosis
Partial Diagnosis
Secondary Finding
(check all that apply)
Q2. Diagnostic thinking efficacy (Check all that apply)
Yes No
WES result helped to establish a diagnosis
WES result helped to establish prognosis
WES identified new risks for the patient
WES halted the diagnostic odyssey
WES altered differential diagnosis
WES result ruled out potential diagnoses
(that were previously hypothesized to be
the cause)
WES result indicated that further dx
investigations were required
Other:

Form 2: Efficacy Form_vR.1 December 2016
Q3. WES result altered the patient’s care plan by prompting
(select all that apply):
Primary
Diagnosis
Secondary
Finding
Sub‐specialist referral(s)
Allergy/Immunology
Cardiology
Chronic Pain
Dentistry
Dermatology
Developmental Peds
Endocrinology
ENT
Gastroenterology
General Surgery
Gynecology
Hematology
Metabolic
Nephrology
Neurology
Neurosurgery
Oncology
Ophthalmology
Orthopedics
Pharmacology
Physical Medicine & Rehab
Plastics
Psychiatry/Addiction Medicine
Respirology
Rheumatology
Sports Medicine
Thoracic Surgery
Urology
Vascular Surgery
Other:
Allied health referrals
Audiology
Dietetics/Nutrition
Occupational Therapy
Physiotherapy

Form 2: Efficacy Form_vR.1 December 2016
Q3. WES result altered the patient’s care plan by prompting
(select all that apply):
Primary
Diagnosis
Secondary
Finding
Speech Language Therapy
Genetic Counselling
Psychology
Other:
Medical imaging
MRS:
MRI (specify):
CT (specify):
U/S (specify):
X‐Ray (specify):
Skeletal survey:
Bone age:
Echo:
Other:
Laboratory investigations
Genetic (specify):
Biochemical (specify):
Cytogenetic (specify):
Other:
Medication implications
A new medication
A medication change (i.e. stoppage, dosage change)
Identification of a medication sensitivity
Other:
Procedures (specify):
Discontinuation of specific health services (specify):
Genetic counselling for family members
related to recurrence risk
related to cascade family testing
related to prenatal testing options
related to prenatal care
Research opportunities for the patient/family (specify):
Other