Embed Size (px)
Citation preview

Low coverage genome-wide sequencing of cell-free DNA enables the detection, monitoring, and characterization of copy number alterations in patients with solid tumorsChristopher K. Ellison1*, Aaron M. Goodman2*, Sabine Riethdorf3, Amin R. Mazloom1, Lisa Tran2, Prachi Nakashe1, Erin McCarthy1, Tobias Gorges3, Alexander Stein4, Julia Quidde4, Daniel S. Grosu1, Mathias Ehrich1, Taylor J. Jensen1, Klaus Pantel3, Razelle Kurzrock2 1Sequenom, Laboratory Corporation of America® Holdings, San Diego, California, 2Department of Medicine, Division of Hematology/Oncology, and Center for Personalized Cancer Therapy, University of California, San Diego, Moores Cancer Center, San Diego, California, 3Department of Tumour Biology, University Medical Centre Hamburg-Eppendorf, Hamburg, Germany4Department of Internal Medicine, University Medical Centre Hamburg, Hamburg, Germany
5693
I. Introduction III. Results
IV. Conclusion
V. References
II. Methods
©2017 Laboratory Corporation of America® Holdings All rights reserved.
Circulating tumor DNA (ctDNA) has been detected in the blood of patients with a variety of cancer types and is thought to reflect the combined genetic profile of the primary tumor and metastases1. The majority of studies of noninvasive “liquid biopsies” have focused on detecting focal events, including single nucleotide variants, gene fusions, and copy number alterations (CNAs); however, these assays are limited to mutations occurring in targeted regions and require deep sequencing (>10,000x coverage) 2-4.
The objective of this study was to use low coverage, genome-wide sequencing of cell-free DNA (cfDNA) to evaluate the frequency, distribution, and persistence of genome-wide CNAs in the plasma of patients with solid tumors.
Low coverage whole-genome sequencing (median 0.3X) was performed for all 287 samples from 102 cancer patients and putative CNA events were iden-tified. cfDNA concentrations were determined for all samples and total cfDNA load was found to be significantly elevated in cancer patients relative to healthy controls. Although there was a poor correla-tion between total cfDNA load and the frequency and magnitude of CNAs across all patients, a strong correla-tion was observed within individual patients, suggesting that the CNAs detected in the cfDNA were derived from additional genetic material contributed by the tumor.
Low coverage, genome-wide sequencing of cfDNA from the plasma of cancer patients enables the detection of large CNAs. These data demonstrate the feasibility of detecting ctDNA in some cancer patients solely on the basis of CNA profiling and more specifically using a numerical quantifier, the GIN. Further, the nature of CNA events observed varied both between patients and across longitudinal samples from individu-al patients. These data suggest that GIN values derived from low-coverage sequencing track with clinical response in cases for which CNA events are detected. This study suggests that genome-wide CNA profiling may be useful alone or as a complement to standard variant detection strategies in the development of liquid biopsy technologies.
1.Bettegowda C, et al. Detection of circulating tumor DNA in early- and late-stage human malignancies. Sci Trans Med 6:224ra24.2.Pantel K, Alix-Panabières C. Liquid biopsy in 2016: Circulating tumour cells and cell-free DNA in gastrointestinal cancer. Nat Rev Gastroenterol Hepatol 2017 14:73-74.3.Wan JCM, et al. Liquid biopsies come of age: towards implementation of circulating tumour DNA. Nat Rev Cancer 2017. doi:10.1038/nrc.2017.74.Newman AM, et al. An ultrasensitive method for quantitating circulating tumor DNA with broad patient coverage. Nat Medicine 2014 20:548-554.5.Lefkowitz RB, et al. Clinical validation of a noninvasive prenatal test for genome-wide detection of fetal copy number variants. Am J Obstet Gynecol 2016 215:227.e1-227.e166.Ikeda S, et al. Metastatic basal cell carcinoma with amplification of PD-L1: exceptional response to anti-PD1 therapy. Nat Genomic Med 2017. doi:10.1038/npjgenmed.2016.37a
Whole blood (10 mL) was collected from 102 patients diagnosed with a variety of solid tumors, prior to the initiation of therapy, and processed to isolate plasma and white blood cells. For almost half of the patients (43/102), multiple collections were available (range: 2-17) to enable longitudinal monitoring of treatment response. In total, 287 aliquots of blood from multiple collaborative studies were used as part of this study.
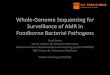
cfDNA from the plasma of each sample was extracted using a bead-based method and genomic DNA was extracted from white blood cells using a standard silica membrane-based protocol (Qiagen) for use as a germline control. Total cfDNA load was quantified using a single-locus ddPCR assay for each plasma sample. All DNA samples were subjected to optimized library preparation for low-coverage next-generation sequencing (Illumina, San Diego, CA). Genome-wide CNA profiles were generated for each sample and CNA events were detected using an algorithm originally developed for noninvasive prenatal testing5. CNAs present in paired cfDNA and white blood cell samples were considered to be derived from the germline and thus removed from further anal-ysis. A genomic instability number (GIN) representing the cumulative deviation from expectation of all autosomal CNAs was calculated. The GIN metric is an unbounded positive value in which higher numbers represent more significant CNAs in both magnitude and abundance; example values with associated genome profiles are shown in Figure 1.
Figure 1. Illustrative genome-wide profiles and associat-ed GIN values for patients without detected CNAs (above) and with extensive CNA events detected (below). Each data point represents the relative number of cfDNA fragments derived from a 50kbp contiguous segment of the genome.
In total, 35.9% (103/287) of blood samples showed evidence of one or more genome-wide CNA in cfDNA and 47.1% (48/102) of patients in this study showed similar evidence in at least one sample. Among patients with longitudinal monitoring, 41.8% (18/43) of individuals showed evidence of CNAs at the initial sampling time point and 37.2% (16/43) of individuals showed similar evidence at the most recent sampling point. Collectively, multiple CNAs were detected on all autosomes and overlapped 94% of the addressable genome, suggesting that genome-wide profiling is necessary to fully assess CNA distributions. Figure 3 shows the distributions of CNAs detected across all autosomes.
Figure 2. A correlation of cfDNA load and CNA events was observed for individual samples (right) but not for all data collectively (left).
Figure 3. CNA events in cancer patients were detected ge-nome-wide and were not constrained to a pre-defined set of gene targets. Blue segments represent high confidence duplication events and pink represents deletion events.
Measures of CNA frequency alone may be informative, but fail to ad-equately capture changes in magnitude of detected CNAs. We devised a metric that quantified the level of genomic instability as inferred through CNA frequency and magnitude. This metric, termed the genomic instability number (GIN) was associated with the number of CNAs detected in a patient. Figure 4 shows the relationship between the count of CNA events and the GIN metric across all subjects. In patients capable of longitudinal monitoring, GIN values were observed concomitant with therapeutic response or disease progression and may provide information earlier than standard imaging-based methods. Figures 5-8 show whole genome profiles and GIN values for three such patients.
Figure 8. GIN profile for patient with squamous cell carcinoma of the tonsil under treatment with Nivomulab exhibiting rapid disease progression. cfDNA (GIN metric) detected disease progression approximately four months prior to imaging confirmation.
Figure 7. GIN profile for patient with squamous cell carcinoma of the skin under treatment with Pembrolizumab exhibiting a clinical response through the period of longitudinal sampling.
Figure 6. Liquid biopsy whole genome profiles from a basal cell carcinoma patient under treatment with Nivolumab. Amplification of region containing PD-L1 (9p24.3 - 9p22.2) and other CNAs were not detected post-treatment, consistent with observed complete response. Scan images from Ikeda et al. (2017)6.
Figure 5. Longitudinal liquid biopsy whole genome profiles (left) and GIN values (right) from a single patient with colorectal cancer and liver metastases under treatment with FOLFOXIRI and Cetuximab; data are consistent with a clinical response.
Figure 4. Genome Instability Number (GIN) is strongly correlated with the number of CNA events detected in a given patient.