Embed Size (px)
Citation preview

FIBULA FREE FLAP MANDIBLE RECONSTRUCTION
DAVID A. HIDALGO, M.D.
MICROSURGERY 15:238-244 1994
Free flaps have many proven advantages in mandible re- construction. 1-3 Recently, the fibula has become a popular donor site choice for this purpose. It has many attractive features, is versatile, and has few drawback^.^-^ It provides up to 25 cm of bone, enough to reconstruct a mandible defect of any length. The bone has a consistent shape throughout its length, a feature that makes it ideal bone stock for shaping a mandible graft. The blood supply par- allels the course of the bone, an arrangement that guarantees adequate vascularity to all segments of a multiply osteoto- mized graft. The flexor hallucis longus muscle, largely ex- pendable, also courses with the bone and is conveniently located to fill in soft tissue loss adjacent to the bone, usually under the mandibular border. A skin island, based on a septocutaneous blood supply, is available in a size large enough to simultaneously reconstruct internal and external soft tissue defects. The skin blood supply, previously be- lieved to be tenuous, is actually reliable in 91.5% of pa- t i e n t ~ . ~ The fibula is located far enough from the head to allow a separate team to work simultaneously in each area without encroaching on one another. Positioning is not a problem because the fibula can be efficiently dissected in the supine patient. Finally, fibula donor site morbidity is low.
INDICATIONS The versatility of the fibula makes it the flap of choice
for the majority of mandible defects. It is equally well suited to short segment “bone-only’’ defects, anterior re- constructions requiring both external skin replacement as well as floor of mouth replacement, and hemimandible de- fects with adjacent lateral floor of mouth or buccal mucosa 1 0 ~ s . ~ Its only disadvantage is that the skin island is not reliable in every patient.
There are only two specific situations where another
~
From the Department of Surgery, Cornell University Medical College, and Plastic and Reconstructive Surgery Service, Memorial Sloan-Kettering Cancer Center, New York, NY.
Address repnnt requests to David A. Hidalgo, M.D , 1275 York Avenue, New York, NY 10021.
Received for publicahon January 4, 1994.
0 1994 Wiley-Liss, Inc.
flap type is better than the fibula. The first is a mandibular defect that has both massive internal and external soft tissue components. In these patients, the goal of an accurate bone reconstruction is usually secondary to that of achieving a healed wound. Both the esthetic and the functional results in this group of patients are generally poor. The extent of disease necessary to cause such a large defect usually im- plies limited survival. The priority in these patients is to have abundant soft tissue that is absolutely reliable. The scapula donor site is ideal for this application. The scapula is not otherwise popular because simultaneous flap prepa- ration and tumor ablation are not possible due to the donor site location. Much time is lost as a result. A second prob- lem with the scapula is that less bone is available compared to the fibula, and the bone that is available (14 cm) lacks a segmental blood s u p ~ l y . ~ * ~ This latter feature limits the number of osteotomies that can be safely made without jeopardizing the viability of the more distal bone segments.
The second situation where a flap other than the fibula is preferred is the case of a lesion of the retromolar trigone that extends to the oropharynx, soft palate, and base of tongue. The bone component is often limited in these cases and involves the angle of the mandible and a small portion of the adjacent ramus and body. The majority of the defect is soft tissue. The best type of replacement for this area is the thin, pliable skin available from the forearm donor site.””’ In this particular situation the limited unicortical bone available from the radius is not a disadvantage. The goal of the bony reconstruction is simply to restore man- dibular continuity in order to preserve tandem temporoman- dibular joint (TMJ) function and normal occlusion. The poor suitability of the radius for osseointegrated implants is not an issue with a bony defect so posterior. As with the specific instance cited for the use of the scapula above, this is another setting in which the soft tissue requirements are more specific and more important than the bone. The radius is not preferred for mandibular defects other than this, be- cause the bone quality is poor. Forearm donor site morbid- ity is higher than the fibula, and there frequently is a con- spicuous and poor appearance to the healed donor site.
The ilium is becoming a less popular donor site even though worldwide it is probably still the most commonly used free flap for mandible reconstruction. It was originally

Fibula Free Flap Mandible Reconstruction 239
attractive because it conveniently resembled a hemimandi- ble.12-16 However, there are a number of drawbacks to this donor site. First, the bone lacks a segmental blood supply. The modem concept of free flap mandible reconstruction calls for multiple graft osteotomies in order to achieve the optimal result. l7 As with the scapula, vascularity decreases in the more distal bone segments of a multiply osteotomized iliac graft. Although there is ample bone available at this donor site, the fixed configuration that originally was con- sidered an advantage is now considered a disadvantage. This is particularly true when trying to use the ilium for an anterior reconstruction. Unlike the straight, stick-like shape of the fibula, the ilium has an irregular shape. Although its shape can be changed with osteotomies, it.lacks the flexi- bility and precision that is characteristic of the fibula in this regard.
There are other disadvantages of the ilium donor site. First, the skin island available with the bone has a tenuous blood supply and tends to be thick and block-like in most individuals. It therefore does not lend itself well to easy insetting within the oral cavity. Some advocates have used the internal oblique muscle to overcome this shortcoming." This enlarges the donor site defect considerably, however. This defect, even when limited as in a bone-only flap, poses a formidable closure task. Postoperative donor site morbid- ity includes delayed ambulation due to pain and the poten- tial for hernia formation.
PREOPERATIVE CONSIDERATIONS Angiography of the donor leg is not routinely canied
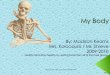
out. Specific radiographic studies are routinely obtained prior to surgery. Templates are made from these studies to aid in accurate shaping of the bone while it remains attached by its blood supply to the legi7 (Fig. 1). This minimizes the ischemia time and thereby eliminates a sense of time ur- gency during the crucial graft-shaping part of the procedure. A transverse plane CT scan reproduced in 1:l scale is used to make a template that shows the curve of the mandible in that plane. A lateral cephalogram is used to make a template that shows the shape in that view. Although providing in- formation in only two dimensions, these templates are the key to a precise reconstruction.
OPERATIVE TECHNIQUE When a hemimandible reconstruction is planned, the leg
on the same side of the lesion is selected, provided that either the internal or external jugular vein on the side of the lesion is available. The anatomy of the fibula is such that use of the ipsilateral leg is best. The flexor hallucis longus muscle lies conveniently under the fibula to fill in the soft tissue defect in the upper neck when the same side is used. The skin island can be easily rotated up and over the fibula to reach the oral cavity to reconstruct a mucosal defect.
Figure 1. Plastic templates are made from tracings of the lateral cephalogram (left) and a transverse plane CT scan reproduced full scale (right). These templates assist in the graft shaping process. (From Hidalgo DA: Aesthetic improvements in free flap mandible reconstruction. Plast Reconstr Surg 88:574, 1991.)
Flap Design Hemimandible reconstruction is planned so that the
pedicle enters the bone at the angle of the mandible graft (Fig. 2A). This arrangement maximizes pedicle length. In the case of an anterior reconstruction where the defect does not extend as far as the angle, the graft design is shifted more distally on the bone (Fig. 2B). The proximal part of the bone is removed in a subperiosteal plane, which effec- tively adds pedicle length. The periosteal component of the peroneal blood supply to the bone ensures viability of each segment.
When using the contralateral neck vessels, the contralat- eral leg is used as the fibula donor (Fig. 2C). Proximal bone is discarded, and the proximal end of the graft will abut the end of the mandible segment that is on the side of the recipient vessels. In the case of a hemimandible repair, the most distal part of the fibula will be angled anteriorly, when the bone is viewed in situ, to form the ramus of the man- dible.
The skin island is designed to run the length of the fibula in order to preserve all of its septal blood supply. The long axis of the skin island is centered over the posterior border of the fibula in order to capture the septal blood supply. This is routinely done even if a short skin island is all that is needed. The skin that is not used during insetting is deepithelialized but generally not excised.
Flap Dissection Dissection is performed from a lateral approach, and a
tourniquet is used. The skin is incised anteriorly, and the lateral compartment muscles are removed from the bone via electrocautery. A cuff of muscle only a few millimeters thick is left on the bone.

240 Hidalgo
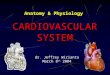
A
C
Figure 2. A: The bone design for a right hemimandible graft is shown drawn on the right leg. Note that the angle of the mandible graft is positioned at the point where the pedicle approximates the fibula. B: The bone design for an anterior graft requiring only partial right body replacement is shown drawn on the right leg. Note that the graft is shifted distally in order to increase pedicle length. C: The bone design for a right hemimandible graft in which the left side neck vessels will be used is shown drawn on the left leg.
The septum between the lateral and anterior compart- ments is then incised, and these muscles are removed in the same fashion. The interosseous membrane is then incised and attention turned to the posterior dissection. The poste- rior skin island margin is incised, and the cleft between the soleus and flexor hallucis muscle is developed by blunt dissection. The soleus is then separated via electrocautery from the fibula and the intermuscular septum that extends to
Figure 3. The hemimandible graft shown (top) has a condyle graft attached. Typical miniplate placement in two planes is shown. An anterior graft viewed from underneath is shown below. Both body segments are left long and are shortened during insetting. Both hemimandible (lateral) and anterior grafts are fully shaped while at- tached by the pedicle at the donor site.
the skin island. No attempt is made to include a large por- tion of soleus with the bone. The transparent membrane that envelops the flexor hallucis longus muscle is incised pos- teriorly along the length of the muscle. Osteotomies are then performed. The proximal osteotomy is usually located just below the neck of the fibula and the distal osteotomy about 6 cm proximal to the lateral malleolus. The perineal vessels and the flexor hallucis longus muscle are divided distally. Traction on the bone near the distal osteotomy outward from the leg exposes the tibialis posterior muscle and its median raphe. The muscle is divided along the me- dian raphe via electrocautery in a distal-to-proximal direc- tion. As long as the muscle is divided along the raphe, neither the perineal vessels nor the posterior tibial vessels will be harmed. Proximally, however, care must be taken not to transect the pedicle near its origin as it crosses the raphe from medial to lateral just posterior to the muscle.
Graft Shaping The fibula is shaped as much as possible before the
pedicle is divided and the flap transferred to the head. This helps to minimize ischemia time. In general, the graft is

Fibula Free Flap Mandible Reconstruction 241
Figure 4. A: A lateral graft is shown following completion of the shaping process and just after division from the leg. B: The defect extends from the midramus to the midline and includes considerable intraoral soft tissue loss. C: The bone has been inset. Part of the skin
completely shaped, but its ends are left long (Figs. 3, 4A). The final osteotomies, which determine overall graft length, are performed during the insetting process. The goal of the graft shaping process is to duplicate precisely the contour of the inferior border of the mandible.
Several types of bone fixation are popular in mandible reconstruction. Miniplates are versatile and extremely easy to use.19 They provide enough rigidity to overcome the need for adjunctive forms of fixation postoperatively. Types with self-tapping screws require a minimum of instrumen- tation. Miniplates allow the graft to be shaped from segment to segment with a high degree of precision. They do not add significant bulk to the external surface of the graft, unlike reconstruction plates. They are the recommended form of furation for the fibula.
Lateral grafts. The shaping of lateral grafts begins with designing of the angle of the mandible graft to correspond to the point on the fibula where the pedicle first approximates the bone. This will maximize pedicle length and allow the
island is seen suspended from the mandibular border. D: In this more frontal view the skin island has been rotated over the mandible and into the oral cavity. After lengthwise folding it is used to resurface the lateral tongue and floor of the mouth.
microvascular anastomoses to be performed without the need for vein grafts. One osteotomy is performed to form the angle of the mandible in most patients. The templates allow the angle to be set with great accuracy. During fixa- tion of the angle, it must be kept in mind that the ramus diverges away laterally from the body at a small angle when the mandible is viewed from the front. The specimen is used as a reference to determine the amount of divergence needed. Miniplates are placed in two perpendicular planes to provide maximum rigidity. The external (lateral) aspect of the graft and the inferior border are used for plate place- ment (Fig. 3).
The ramus is usually finished before shaping the body. Posterior facial height is determined by the total height of the ramus and condyle. If the resection has been performed at or below the level of the midramus, the condyle and proximal ramus are left in situ as the specimen is removed. The final height of the graft ramus can be determined by measuring directly from the specimen. If the resection is to be performed higher than midramus, it is better to remove

242 Hidalgo
the entire ramus (including the condyle) with the specimen. The condyle is then cut from the specimen and bone scrap- ings from its end sent for frozen section. If there is no evidence of disease the condyle is then mounted onto the end of the graft ramus with miniplates (Fig. 3). It is critical to measure the total ramus height of the specimen prior to removing the condyle from it. This total height must be duplicated on the graft. The graft ramus is cut at the appro- priate length taking into consideration the height of the condyle segment that will be joined to it.20
The body of the graft usually requires one osteotomy. Both templates are used for reference because the body curves in the transverse plane and is usually angled either upward or downward in the lateral view at the same time. It is often helpful to refer to the specimen to help visualize what is needed at this midbody osteotomy. After fixation of this osteotomy, graft shaping at the donor site is complete. The end of the graft is purposefully left long with the final osteotomy performed during graft insetting.
The patient is placed in intermaxillary fmation to ensure normal occlusion as the graft is inset. The border of the mandible from its cut end past the midline to the opposite (normal) side is exposed prior to insetting the graft. This allows visualization of the curve of the mandible and pro- vides room for the miniplates. The condyle, if present on the graft, is inset into the glenoid fossa. A nonresorbable suture is placed to close partially the capsule around the condyle if possible. &or to performing the last graft os- teotomy, total graft length is checked, comparing it to the total length measured from the specimen.
It is important to establish symmetry between the angles of the mandible from side to side. During insetting, each must be at an equal distance from the midsagittal plane and on an equal transverse plane as well. Significant deviation from this will result in facial asymmetry.
Anterior grafts. Shaping of anterior grafts also begins with planning pedicle position. The graft design is generally shifted more distally on the leg compared to lateral grafts. Enough proximal fibula is resected (and discarded) in a subperiosteal plane to at least match the amount of body length that remains on the side on which the microvascular anastomoses will be performed. This is done so that when the graft is inset the part of the pedicle that originally ap- proximated the bone is located at the angle of the mandible. This is a simple and effective method of providing maxi- mum pedicle length in the case of anterior grafts.
Anterior grafts consist of a central segment and two body segments. Experience has shown that central segment length should be approximately 2 cm. The location of the central segment on the distal fibula is determined after pedi- cle length requirements have been considered. An osteot- omy site is marked at each end of the central segment.
Figure 5. A: An anterior graft is shown following division of the pedi- cle. Note the unequal length body segments. B: The postoperative view shows how the skin has been used to replace the floor of the mOUth.
These osteotomies are angled in two planes because the body segments will diverge away from the central segment in two directions (upward and backward). It is important to maintain the anterior face of the central segment in a ver- tical plane as the body segments are attached to it.” Miniplates are placed in two planes for fixation (Fig. 3).
The body segments are left long, and their final length is determined during insetting (Fig. 5A). If the body seg- ment on one side extends almost to the angle, then a mid- body osteotomy will be needed. This is performed in the manner described for lateral grafts and is the last part of graft shaping process at the donor site.
Insetting an anterior graft is more difficult than insetting a lateral graft. First, there are usually few teeth left on the mandible. This precludes the use of intermaxillary fixation and makes the entire insetting process less precise. The only reliable landmarks are the maxillary arch and the midline. Second, the remaining lateral mandibular segments are mo- bile in many planes, which makes it difficult to maintain their normal spatial orientation during insetting.

Fibula Free Flap Mandible Reconstruction 243
Figure 6. A: A typical postoperative result following hemimandible reconstruction is shown. A small intraoral skin island was used. B: The panorex shows the graft with its miniplate fixation. A condyle graft was not used in this patient.
It is important to refer to the specimen and to make sure that the curve of the graft matches it. The total length of the graft should be the same as the specimen once the ends of the graft have been shortened for insetting. The straight-line distance between the two ends of the graft body segments (an indirect measure of the angle of divergence of the body segments from the central segment) should also be the same as on the specimen. Care must be taken to avoid creating retrognathia, prognathism, or a twist in the mandible during insetting. Correct interarch distance must be maintained, and the mandibular arch should parallel the maxillary arch. This will facilitate dental reconstruction later. The graft is fixed to the lateral mandibular segments with miniplates placed in two planes.
POSTOPERATIVE CARE Graft monitoring is not precise. If an intraoral skin is-
land is present, its color and capillary refill can be followed by direct observation. The peroneal artery (and often the vein) can be monitored by conventional doppler exam. Bone scans are not routinely obtained.
Figure 7. A: A typical postoperative result followng reconstmction of an anterior defect. The anterior floor of the mouth was replaced with a skin island. B: The panorex shows the graft. Note that the inferior border of the mandible is symmetric and that the body segments are of different lengths.
Intermaxillary fixation is released after 5 days if the condyle has not been reconstructed. If the condyle has been transplanted, fixation is discontinued after 10 days. Ambu- lation is encouraged as soon as after 5 days in those not requiring a skin graft donor site closure. Patients with a donor site skin graft do not ambulate for 3 weeks. Donor site symptoms tend to be mild and transient. Edema and episodic pain are most common and generally resolve with time. Inability to flex the hallux is permanent. Ankle insta- bility is extremely rare and usually responds to strengthen- ing exercises.
Bone healing is followed by periodic panorex studies. Patients proven free of disease can have osseointegrated implants placed 6 months to 1 year after reconstruction. Miniplates that lie in the region of implant placement are first removed as a separate procedure. The fibula has suf- ficient thickness in all dimensions to support implants.*l Case studies are shown in Figures 4-7.
CONCLUSIONS The fibula has many anatomic features that make it
widely applicable for composite mandibular defects. It is easy to shape, and the blood supply to all osteotomized

244 Hidalgo
segments is uniform. A skin island is available in at least 91% of patients, and the flexor hallucis longus muscle can be used for soft tissue replacement under the mandible. The fibula is compatible with miniplates for fixation as well as osseointegrated implants for dental reconstruction. Donor site morbidity is low. The esthetic and functional results of mandible reconstruction with the fibula are excellent.
1.
2.
3.
4.
5.
6.
7.
8.
Duncan MJ, Manktelow RT, Zuker RM, et al.: Mandibular recon- struction in the radiated patient: The role of osteocutaneous free tissue transfers. Plasr Reconstr Surg 76829-840, 1985. Rosen IB, Manktelow RT, Zuker RM, et al.: Application of microvas- cular free osteocutaneous flaps in the management of post-radiation recurrent oral caucer. Am J Surg 150474-479, 1985. Silverberg B, Banis JC, Acland RD: Mandibular reconstruction with microvascular bone transfer. Am J Surg 150440-446, 1985. Flemming AFS, Brough MD, Evans ND, et al.: Mandibular recon- struction using vascularized fibula. Br J Plasr Surg 43:403-409, 1990. Hidalgo DA: Fibula free flap: A new method of mandible reconstruc- tion. P h r Reconsrr Surg 84:71-79, 1989. Lyberg T The vascularized fibular flap for mandibular reconstruction. JCranio-Max-Fac Surg 19:113-118, 1991. Schustennan MA, Reece GP, Miller MJ, et al.: The osteocutan~us free fibula flap: Is the skin paddle reliable? P h r Reconstr Surg 90:
Sullivan MJ, Baker SR, Crompton R, et al.: Free scapular osteocu- taneous flap for mandibular reconstruction. Arch Orolaryngol Head Neck Surg 115:1334-1340, 1989.
787-793, 1992.
9. Swartz WM, Banis JC, Newton ED, et al.: The osteocutaneous scap- ular flap for mandible and maxillary reconstruction. Plmr Reconstr
10. Soutar DS, Scheker LR, Tanner NSB, et al.: The radial forearm flap: A versatile method for intra-oral reconstruction. Br J Plasr Surg 36:
11. Soutar DS, Widdowson W P Immediate reconstruction of the mandi- ble using a vascularized segment of radius. Head Neck Surg 8:232- 246, 1986.
12. David DJ, Tan E, Katsaros J, et al.: Mandibular reconstruction with vascularized iliac crest: A 10-year experience. P h t Reconstr Surg
13. Jewer DD, Boyd JB, Manktelow RT, et al.: Orofacial and mandibular reconstruction with the iliac crest free flap: A review of 60 cases and a new method of classification. Plasr Reconsrr Surg 84391-403, 1989.
14. Taylor GI: Reconstruction of the mandible with free composite iliac bone grafts. Ann Plasr Surg 9:361-376, 1982.
15. Urken M L Composite free flaps in oromandibular reconstruction. Arch Orolaryngol Head Neck Surg 117:724-732, 1991.
16. Urken ML, Weinberg H, Vickery C, et al.: Ommandibular recon- struction using microvascular composite free flaps. Arch Otolaryngol Head Neck Surg 117:733-744, 1991.
17. Hidalgo DA: Aesthetic improvements in free-flap mandible recon- struction. Plast Reconstr Surg 88574-585, 1991.
18. Urken ML, Vickery C, Weinberg H, et al.: The internal oblique-iliac crest osseomyocutaneous free flap in oromandibular reconstruction. Arch Otolaryngol Head Neck Surg 115:339-349, 1989.
19. Hidalgo D A Titanium miniplate fixation in free flap mandible recon- struction. Ann Plmt Surg 23:498-507, 1989.
20. Hidalgo D A Condyle transplantation in free flap mandible recon- struction. P h t Reconsrr Surg (in press).
21. Zlotolow IM, Hurn JM, Piro JD, et al.: Osseointegrated implants and functional prosthetic rehabilitation in microvascular fibula free flap reconstructed mandibles. Am J Surg 164:677-681, 1992.
Surg 77530-545, 1986.
1-8, 1983.
82792-801, 1988.