Embed Size (px)
Citation preview

-507
THE FENESTRATION OPERATION FOROTOSCLEROSIS
By E. R. GARNETT PASSE, F.R.C.S., F.A.C.S.London
Since the discovery that the cause of deafnessin the majority of cases of otosclerosis was dueto ankylosis of the footplate of the stapes,various otologists in Europe and America havedevoted much of their lives endeavouring eitherto prevent the ankylosis or to restore by surgerythe natural path of sound waves. So far allattempts at preventing ankylosis of the foot-plate have been in vain; however, great strideshave been made with the second half of theproblem, which presented two main factors,namely, the establishment of a fistula into theperilymphatic space, which, despite the naturaltendency on the part of nature to close, wouldremain open indefinitely and, secondly, theselection of such cases which, when this wasaccomplished, would respond by a return ofhearing to a practical worthwhile level.The evolution of this operation, now known
as the Fenestration Operation, is of some con-siderable interest. Seventy-one years ago aGerman surgeon named Kessel discovered thatremoval of the stapes from its niche, in apatient suffering from deafness, restored thehearing for a short time. In i897 this was con-firmed by Passow. Again the improvementwas of short duration. From that timeonwards a number of otologists, e.g., Politzer,Birany, Rosey and Denker, found, uponcreating a fistula in the capsule of the labyrinth,that hearing was restored to patients deafenedby otosclerosis. Straaten stated that the sameresults would be obtained in cases whereadhesions tended to fix the. stapes in its ovalwindow. Many and various were the opera-tions devised, either for mobilizing the stapesor for producing a fistula into the labyrinth.
Jenkins in 1913 appears to have been thefirst in this country to treat cases of oto-sclerosis by opening the perilymphatic spacevia the semicircular canal. The hearing wasmarkedly improved for several days. In I923Holmgren of Stockholm operated on four casesof otosclerosis with the use of a binocular
dissecting microscope. He created a fistulaclose to the footplate of the stapes and thencovered it with a Thiersch graft. The hearingremained improved for several-months, butlater diminished. In I929 Sourdille of Nantesdescribed an operation performed in severalstages to achieve a permanent fistula coveredwith a cutaneous flap continuous with thetympanic membrane.From I936 to I939 I carried out a series of
thirty-six fenestration operations based uponthe Holmgren technique, the results of whichhave been published.The field of investigation, having been
broadened by otologists in Europe, thenmoved to the United States of America, wherethe chief exponents were I,empert, Sham-baugh and Campbell. Perhaps the mostzealous of these workers and the one to bringthe treatment to its modern degree of successwas Julius Lempert of New York, who alsodevised the endaural approach. Since thiswork was started in the United States ofAmerica some thousands of cases have beenoperated on and reports have been publishedin various journals concerning its successes andfailures, but a consensus of published reportsto date indicates that the fenestration operationhas at last taken its place as an accepted oto-logic procedure in certain cases of deafness dueto otosclerosis.From the practical standpoint the questions
which face the otologist who regularly practisesthe fenestration operation are:
(I) The classification or grouping of oto-sclerotics.
(2) The devising and carrying out of anefficient technique for the operation.
(3) The institution of a meticulous and rigidaseptic after treatment.
(4) The notation of follow up records basedon standard tests.
(5) Tinnitus in relation to otosclerosis andthe fenestration operation.
by copyright. on June 8, 2020 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.23.265.507 on 1 Novem
ber 1947. Dow
nloaded from

508 POST GRADUATE MEDICAL JOURNAL November i947
(6) Results of the fenestration operation andcomparison with those obtained by ahearing aid.
(7) The results of the fenestration opera-tion.
1. The Classification or Grouping ofOtoscleroticsThe ultimate aim is the selection of those
cases for whom, provided the operativetechnique is flawlessly carried out, we can say,beforehand that the result will be restorationof hearing to a permanent and useful level.This happy state has not yet been reached, butas the years go by we are approaching our goalmore and more closely.From the mass of literature which has
already been published on the subject, mainlyin the United States of America, and fromexamination of my own records, which includecareful examination of over 2,000 cases ofclinical otosclerosis, on more than 300 ofwhom I have operated, certain facts permit anaccurate classification of cases of clinical oto-sclerosis into one of three groups, each of whichmay have a certain expectancy of result.Group I. Those in whom clinical and audio-
metric examination for both pure tone andspeech establish beyond doubt that the reserveof cochlear nerve function is adequate. Inthis group I expect 8o to 90 per cent. of casesto be restored to the practical conversationallevel.
Group II. This comprises those who may beclassified as borderline cases. The clinical andaudiometric examination in these cases showthat the apparent extent of cochlear nervedamage is such that it will be necessary for themaximum improvement to be obtained if thepractical hearing level is to be reached. Inthis group success can be anticipated in onlyabout 20 to 40 per cent. of cases.Group III. Comprises those cases where the
cochlear nerve has so far deteriorated that thechances of improvement in hearing by thefenestration operation is practically nil. Ifthe cochlear nerve endings are not capable ofreceiving and transmitting a normal stimulusit is useless to create a new window. Occasion-ally, however, even in cases in Group III, Ihave been surprised by an apparently hopelesscase in whom the hearing was restored in the
low frequencies of 256 and 512 decibels to suchan extent as to enable spoken conversation tobe heard clearly, whereas they have previouslybeen stone'deaf to the loudest shout. Not onlyis it necessary for the fistula to remain opento obtain good hearing, but the cochlear nervemust be capable of receiving and transmittingsound impulses through the open fistula.During this last year, using a type of
fenestra that I described at a meeting of theOtological Section of the Royal Society ofMedicine in December, 1946, I have not had,in approximately I70 cases, one fistula whichhas closed as judged by the fistula sign. How-ever, one must bear in mind the fact that,although at last it may be possible to obtain afenestra which will remain open, there is thedifficulty of classifying and choosing suitablepatients for the operation. For this purpose Iemploy routine taking of history, clinicalexamination of the external, middle ears andthe upper respiratory tract to exclude infectiveand other diseased foci, together with carefulexamination of the receptive and conductivepower 'of the auditory apparatus by means ofthe audiometer, tuning forks and speech per-ception. I have frequently observed that somepatients whose hearing post-operatively hasreached only to 35-30 decibels have practicalhearing, while others whose auditory level isas high as 25 decibels have difficulty.
Several factors have become apparent whichare helpful in this estimation of hearingaccuracy. Rinne's tests are carried out withtuning forks of 5I2 and I,024 using masking.If they are both negative an improvement inhearing may be expected. If 2,048 is not heardat all by bone conduction the operation iscontraindicated.
Further, I have noticed that in determiningwhether a case is one of nerve deafness or oto-sclerosis, if the patient states that the sound'bursts' on them, as it were, e.g., if at 6odecibels the patient does not hear the note, butat 65-70 decibels the patient states that thenote is quite loud, then these cases are sufferingfrom a clinical nerve deafness and should notbe operated upon.
It has been said that the fenestrationoperation is of no value to people who have ahearing loss below 6o decibels, for below thisit has been stated that the hearing is not likely
by copyright. on June 8, 2020 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.23.265.507 on 1 Novem
ber 1947. Dow
nloaded from

November I947 PASSE: Fenestration Operation for Otosclerosis 5Q9
to recover to the practical level, i.e., the 30decibel or above. In my series many casesdisprove this observation and I have, in fact,several cases where the hearing gains have been55 decibels in practical frequencies. It hasalso been stated that, unless the hearing losscan be brought up to the 30 decibel level forthe frequencies of I,024 and 2,048, the patientcannot hear ordinary conversation. I haveobserved, however, many patients in whomimprovement to the 30 decibel level or abovehas been in the frequencies of 256 and 5I2 onlyand in whom I,024 and 2,048 have been belowthis level who hear ordinary conversation with-out undue straining. Patients who hear con-versation more readily after this operation arethose in whom the improvement has been overthe range 1,o24 to 2,048.
Whilst I have frequently stated that I do notconsider a 6o decibel loss in any frequency tomean that the hearing from this level cannot beraised to at least a 30 decibel level, I havefailed to raise an 8o decibel loss in any fre-quency to the practical level. However, if this80 decibel loss occurs only at 2,048, whilst1,024 and lower is above this level, then, otherthings being equal, it may still be possible togive the patient practical hearing for the low ormiddle registers as I have indicated. Further-more, in deciding whether the patient shouldhave the operation or not, one must considerthe fact that the operation in practically 90per cent, of cases appears to prevent furtherhearing loss, even if the improvement doesnot reach the practical level.
In choosing a patient as suitable for thisoperation one must bear in mind, of course,other factors such as the psychology of thepatient and, one may add, the degree of mentalintelligence possessed by the patient. Oneyoung patient upon whom I operated with asuccessful result developed an acute anxietystate following the operation. Furthermore,some types of hospital patient with a lowstandard of intelligence seem to be unable tomake the most of their restored hearing, orcomplain, because they cannot hear a watch atthree feet like some of their friends, that theoperation, though restoring conversationalhearing, is a failure to them.
Paracusis Willisii or the power of hearingmore clearly in noisy surroundings, such as a
train or motor car, is another point that oneshould observe most carefully before selecting apatient as suitable for the operation. Absenceof this sign usually indicates that a clinicalnerve deafness, either primary or secondary, ispresent. If the patients volunteer that theyhear better in a quiet room, then, as a rule,they are unsuitable for the fenestration opera-tion. Those patients who had paracusisWillisii in the past but no longer have it alsofall into this class.
In my experience I have occasionally foundimproved bone conduction in the operated earin successful cases, but, as one might expect, Ihave also frequently found the reverse. Thislatter observation has been confirmed experi-mentally by Lowry. I have, however,: foundimproved air conduction in the opposite earsome short time after a successful fenestrationoperation. Possibly bone conduction in itselfdoes not give a direct indication of the acousticnerve function, for other observers have foundthat bone conduction has improved after asuccessful fenestration operation. I haveoperated many times and produced successfulresults on patients where bone conduction for1,024 and 2,048 has been below the 30 decibellevel, bringing the air conduction hearing lossto the 30 decibel level or above for these fre-quencies. In the early days of the fenestrationoperation Lempert and others stated that theydid not think it worth while operating wherethe loss of bone conduction in the speech zoneamounted to more than 30 decibels, but this isno longer true. It' may be, of course, thatthe bone conduction does not give such a goodindication of the condition of the acousticnerve as was at first thought. Owing toimproved technique, I feel we must lower thebone conduction limit from 30 decibels to 35or 40 in frequencies of I,024 and 2,o48, butretain it at 30 decibels for 512.
Concerning age and the operation in general,young people have the greatest restoration ofhearing, possibly owing to a better state of thecochlear nerve endings. I have two youngpatients who show upon repeated examinationthat the hearing level has been restored to zeroin one frequency. On the other hand, I haveelderly'patients in the sixties, and even in theseventies, who have regained the practical con-versational level with improvements of as much
by copyright. on June 8, 2020 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.23.265.507 on 1 Novem
ber 1947. Dow
nloaded from

5Io POST GRADUATE MEDICAL JOURNAL November I947Noeme1'4
as 40 to 50 decibels in various frequencies.Furthermore, in none of my elderly patientshas the fenestra appeared to close. This maybe, of course, owing to the fact that bony re-growth in the elderly is naturally retarded.
In the fenestration operation the vascularcirculation of the internal ear is considerablyaltered by the extensive removal of the peri-osteal layer of bone from the capsule in theregion of the vestibule, lateral, superior andposterior canals. This may in part beresponsible for the fact that the operationappears to retard the otosclerotic process sofar as one can judge by cochlear function. Thishas been repeatedly confirmed by Lempert,Sourdille and Frazer.X-ray investigation does not give much
assistance bther than to show whether themastoid is pneumatized or sclerosed. If it issclerosed, then possibly the diagnosis is oneof a chronic adhesive process and not of oto-sclerosis. However, sclerosis does not contra-indicate the operation. The proof of stapedialfixation can only be truly ascertained duringthe operation, by palpation of the stapes itself.Excellent results have also been obtained incases where the stapes proved to be entirelysurrounded by dense bands of fibrous tissue.
Routine examination of the eustachian tubesis carried out in all cases and it is surprisinghow seldom complete obstruction is found. Iam not speaking, of course, of children withlirge masses of adenoids. I have not seen onecase of bilateral adult deafness where theeustachian tubes were both blocked byadenoids, though I have seen several in whomadenoidectomy has resulted in partial cohesionof what remains of the cushions of the.eustachian tubes, but rarely is this deafnessbilateral or of the increasing type. One patientpresenting deafness of an unilateral natureappeared on examination to have a growth inthe eustachian orifice, which on section provedto be an epithelioma.
Patients, especially the young, who state thattheir hearing reached its present level ofdeterioration in a matter of weeks or a fewmonths, since when, and it may be years, thehearing has not deteriorated further, usuallybut not always prove to have severe nerve deaf-ness. There appear to be a larger number ofyoung people suffering from clinical nerve
deafness, the etiology of which is apparentlyas obscure as that of otosclerosis, than oneformerly suspected, and they present a widefield for future research.We now realize that otosclerosis may cause
deafness by other mechanisms than the onewhich causes stapedial ankylosis and until wecan be certain that the latter change is the onlyone present we are bound to meet a percentageof failures. Similarly, there is no reason why acase which has remained successfully cured fora number of years may not suddenly begin tolose the hearing owing to a focus of otosclerosisdeveloping in another vital region. For-tunately, otosclerotic foci causing deafness byattacking the otitic capsule elsewhere thanadjoining the oval window are rare,-but theprognosis must necessarily be guarded to thisextent and, in all fairness, the patient warnedof such a possibility.To sum up the important question of
selection:(I) Bone conduction, whilst not a decisive
criterion for the state of the acousticnerve, is certainly a great help,; theformer guiding level of 30 decibels forfrequencies I,024 and 2,048 may nowbe lowered to 40 decibels.
(2) Paracusis Willisii, if present, is a mostimportant guide to the possibility ofoperation. If absent it definitely ex-cludes the patient from this operation.
(3) The duration of the increasing deafnessit not very significant.
(4) Whilst the greatest acuity may beexpected after operation in youngpersons, successful results may alsobe obtained in the elderly.
2. The Evolution and Execution of anEfficient Technique in theFenestration OperationThe rationale of operation is now based on a
technique which has proved experimentally togive the best results. (Lindsay, Shambaughand Juers.)As might be expected with an operation of
this nature in which technique is all important,progress has been made by various methods,the good ones being retained and improved andthe poor discarded. Endeavour has so far beendirected into two main channels:
by copyright. on June 8, 2020 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.23.265.507 on 1 Novem
ber 1947. Dow
nloaded from

November i 947 PASSE : Fenestration Operation for Otosclerosis 511
Cr:):id~~'"~"'":::....i:~!`.`.̀``~`~.~!~ii~`~. `` ``~!~~i~i~.`~;~!~iiii~:~;iii;i~~iri·ai ~.~...!· .~< z~. ,···:4.,............
·i~w i~I'.~' .,".~
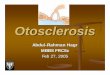
FIG. I. FIG. 2. FIG. 3.FIG. I.-Cross section of lateral semicircular canal. FIG. 2.--Periosteal bone removed down to
endosteal bone over a large area. FIG. 3.-Endosteal bone thinned down until the roofis finally removed
.. ...... ...:ii :.iiil;ii ~ ~ ·.::.~::* ·*;
... .II
rAX.
5i~4 ;
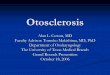
FIG 4 ·Fic S.FIG 6
FIG. 4-The old type of fenestra made for use with the cartilage stopple. FIG. 5.-Lateral viewof the fenestra in roof of vestibule and canal showing fenestra seated on top of a ridge.FIG. 6.-Skin flap in situ. Note that it is in contact with the membranous canal.
(I) To establish a fistula in the perioticcapsule which will remain perman-ently open and so allow mobilizationof the perilymph.
(2) To provide some form of covering forthis opening which will transmit airwaves with a maximum of efficiency.
The foundations of the present-day tech-nique have been well laid by Julius Lempert ofNew York, who performed much experimentalwork in devising a method of keeping open thefenestra. Many ingenious methods of pre-venting bony regeneration were used fromeburnation of the edges of the bone to theintroduction of foreign substances of variouskinds. Many successes have been obtainedwith the introduction of an autogenous carti-lage graft or stopple. My second series of Ioocases were performed this way, but I use it nolonger, as it did not fulfil its early promise.Shambaugh in 1946 gave an account of 822fenestration operations performed under con-tinuous irrigation and reported that in 88 percent. of cases of more than two years' durationa h'earing improvement of io decibels or overhas been fully maintained. It was he whoevolved the technique of enchrondralization of
the fenestra; by this means the periotic layersof bone are removed until only the osteo-genetically inert enchrondral layer of the bonylabyrinthine capsule remains in the area inwhich he makes his fenestra.As mentioned previously in December, 1946,
I described a modification of this fenestra inwhich I performed a more extensive removal ofthe periosteal layer of bone around the canaland domed vestibule, leaving only a thin egg-shell layer of the endosteal bone extendingfrom the dome of the vestibule' anteriorly tothe downward bend of the lateral semi-circular canal posteriorly. On top of this ridgeof bone the fenestra is then made. The maindifference between my ienestra and that ofShambaugh is that my fenestra is much longerand more of the endosteal bone is exposed.By using this method I have been able toobtain a fenestra' in some cases almost a centi-metre in length. Great care must be taken notto injure the membranous canal in such a longfenestra as it tends to float out of the canal.By using the binocular microscope and irriga-tion, all bone fragments and dust particles arecarefully removed as soon as they are madefrom the region of the fenestra and on the
by copyright. on June 8, 2020 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.23.265.507 on 1 Novem
ber 1947. Dow
nloaded from

512 POST GRADUATE MEDICAL JOURNAL November I947
\I=ncIs IO
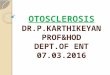
FIG. 7.-Single 'S '-shaped incision cutting 'tongue'of skin.
periosteal surface of the meatal flap. Com-plete haemostasis is most essential and is,obtained by diathermy, fibrin foam or oxycel.It has been my practice in recent months to' float' the flap into place in a bed of Ringer'sSolution. The flap is fixed in position by waxplugs placed in a groove prepared especiallyabove the fenestra and great care is taken toprevent pressure on the flap over the actualfenestra by the subsequent dressing. The flapis firmly adherent to the bone in 48 to 56 hours.This was proved by a case in which at thecommencement of preparing the fenestra myelectric drill broke down and I had to leave theflap over the prepared area of the vestibule andsemicircular canal whilst the engine was beingrepaired. Forty-eight hours later, on raisingthe flap to complete the fenestra, I found thatit was firmly adherent by vascular granulationtissue to the bony bed. Plastic surgeons haveconfirmed this observation since.At present I am working with solutions of
anti-histamine agents to endeavour to preventsome of the traumatic post-operative labyrinth-itis supposedly due to histamine liberationfrom the under surface of the flap. It is tooearly yet to state any results, but so far theyhave been most encouraging. Other methods
Edgfdge of floap
vI?
FIG. 8.-Showing tongue of skin tucked upwards andbackwards into mastoid cavity.
of preventing post-operative labyrinthitis areby absorbent sponges or self-absorbent cellu-lose. Immobilization in a head frame for48 hours post-operatively as recommended byShambaugh has, I believe, a definite use.
Since I gave up using the cartilage stoppleand employed the above means in an endeavourto lessen post-operative labyrinthitis I havenoticed that a greater number of patients havestated that their hearing improved the, dayafter operation, and also that the post-operativeperiod of lessened hearing is reduced in manycases by several days. Nor does the nausea andvomiting appear to be so great nor so prolongedas it did in my earlier cases. Patients are nowquite willing to get out of bed on the fourthday, whilst formerly it was often a week beforethey could be persuaded to do so. The amountofgiddiness and nausea following the operationappears to have an individual characteristic inthat patients who are readily seasick appear tobe affected more severely than those who donot suffer from this malady.The flap I use is formed of the anterior
meatal wall. It is always possible to cover thedome of the vestibule and the ampulla of thelateral canal with this very thin skin, but itdoes not always prove possible to cover the
by copyright. on June 8, 2020 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.23.265.507 on 1 Novem
ber 1947. Dow
nloaded from

November 1947 PASSE: Fenestration Operation for Otosclerosis 513
prolongation of the fenestra around the bend ofthe lateral canal with the anterior meatal wall.Results may be much better using this thinskin in covering the fenestra, though it is alsoapparent that the epidermal lining of the cavityin this region invariably becomes paper thinwithin 9 to I2 months unless infectionsupervenes. This, then, appears to be thetechnique of choice at the present day.
It has not been necessary to carry outrevision in any of my cases performed duringthe last I2 months, though it was necessary inapproximately io to 15 per cent. of casesperformed during the previous I2 monthswhen I employed the cartilage stopple in-sertion. In each case of revision performed inthese cases the cartilage stopple was found to beimmobilized or even extruded by fibroustissues and not by bony growth, though bonewas found on section embedded in the fibroustissue.
Should damage occur to the endolymphaticsystem during the operation, escape of endo-lymph occurs and leads to a reduction in theamount of hearing gained, though it by nomeans prevents partial restoration of hearing.I feel, however, in these cases that in duecourse fibrous tissue is more likely to fill thecanal and cause further deterioration of hear-ing than if the membranous endolymphaticsystem remains intact and unites with theunder-surface of the flap. On the other hand,cases of Meniere's disease treated by extractionof the lateral and superior membranous canals,after sealing off the utricular ends by dia-thermy, did not result in a further reduction ofthe patient's already somewhat lessenedhearing.
Concerning the risks of the operation, Ihave had no deaths or serious complicationsin my 300 cases. There has been no case ofpersistent dizziness-sufficient to be incom-moding-lasting more than four months.There has been one case of internal saphenousphlebitis. This was probably due to theanaesthetic, for I perform the operation underintermittent intravenous pentothal injectedinto one of the veins of the legs or feet.
3, The Institution of a Meticulous andRigidly Aseptic After-treatmentThe success of the operation does not
depend only on the technique employed in theactual operation. It also depends to a verylarge extent upon obtaining a dry cavitysoundly healed in a minimum of time. As Iemploy the endaural approach entirely, one ofthe problems which early manifested itselfwas the prevention of stenosis of the externalmeatus which occurred in a small percentage ofcases. In order to avoid this, I devised amodification of the Lempert endaural incision,which provides me with a flap of skin hingedpostero-superiorly, which at the end of theoperation is folded back into the meatus andheld up against the lower border of the tem-poralis muscle by .means of a suture passedthrough the flap and through the skin of thepost-auricular groove. This also provides astarting point for epithelialization in thisregion and by this means the external meatusis covered by skin for five-sixths of its circum-ference and no skin is wasted as in the Lempertendaural incision. (See diagram.)The first dressing is performed on the sixth
day under pentothal anaesthesia, the secondon the fourteenth day and the subsequent onesonce a week until the cavity is dry, without, ofcourse, any further anaesthesia.
I am now using an absorbable cellulbsepacking which as it liquefies can be sucked outof the cavity on the tenth day and so avoids ananaesthetic. From first to last the operationneed give no pain whatever. After the cavityis cleaned one of the sulpha drugs is insufflatedin powder form. All dressings are performedin 'the early stages by myself, and I cannotadvocate too strongly the necessity for this.All dressings used are sterilized by autoclave.It was found in female patients that the hairwas a great source of infection; in order toavoid this in the early days I insisted on thepatient wearing a bandage for four weeks andI am convinced that this has done more toreduce post-operative infection than any othersingle factor. The rate of healing appears tobe an individual matter and no hard and fastrule can be laid down; it may take any timefrom four weeks to six months. Recentexperiments with the above cellulose soaked ina 2 per cent. Benadryl solution have givengreat promise of a rapid epithelization of thecavity, but it is too soon to pass judgmenton this.
by copyright. on June 8, 2020 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.23.265.507 on 1 Novem
ber 1947. Dow
nloaded from

514 POST GRADUATE MEDICAL JOURNAL November I947
4. The Notation of Follow-up RecordsBased upon Standard TestsIf progress is to be made in this.operation,
then complete records should be kept, notonly of the results, but of the minute technicaldetails as to shape and size and position of thefenestra, condition of membranous canal, typeof dressings, shape and position of flap, typeof dressing employed, etc., so that by com-parison of these details a technique offering thebest results may be evolved.
Careful records of audiometric tests takenat intervals of one month, three months, sixmonths, one year and then yearly for o ormore years for both air and bone conductionof both ears is also necessary to'appraise thevalue of the operation. To this I add aquestionnaire to be answered yearly as towhether the patient regards the results assatisfactory. In my series of over 300 cases Ihave only one patient (who subsequent to theoperation developed frequent attacks of acuteotitis media) who has stated that the operationwas not worth while.
If otologists practising this operation wouldco-operate and compare their results basedupon some practical classification of patients assuggested above, together with the minutedetails of technique employed, I feel that pro-gress would be made more rapidly than byindependent workers. I am using a standardperforated record card which rapidly showsthe results of any particular item in the history,selection, operation and after-treatment of each'case.
5. Tinnitus in Relation to Otosclerosisand the Fenestration OperationApproximately go per cent. of all cases of
deafness whom I have examined in the lasttwo years complain of tinnitus in one or bothears, or 'in the head.' 6o per cent. of theseclaim that the tinnitus is of a pulsatingcharacter synchronous with the heart beat andmade worse by exertion. The tinnitus amongthese people is nearly always of the 'hissing'or 'steam' or 'booming' variety. In theother type the noise is continuous, not affectedby the heart beat or exertion, and is usually of ahigh-pitched or continuous bell or clangingvariety. Many patients complain of an ex-
plosive sound in the ear, usually as they areabout to drop off to sleep. Pre-operativeaudiometry of patients with tinnitus presents aslight added difficulty which can be overcomewith patience. One of the questions asked bymost patients is what effect the operation willhave on their noises. Here the answer isunpredictable, but examination of my recordsshow that in approximately 25 per cent. thenoises are either relieved or greatly reduced.In a further 60 to 70 per cent. the noises remainunaltered in intensity, but may be altered intone. In a small percentage they may evenbecome worse for a short time and make thehearing tests post-operatively extremely diffi-cult. I believe that tinnitus which is syn-chronous with the heart beat is due to reflexvascular spasm.
I endeavoured in a series of cases to alleviatethis by destroying Jacobson's nerve and vesselsas they pass over the promontory by means ofcoagulation diathermy during the operation, aprocedure later described as a separate opera-tion by Lempert. The results of this have beenmost disappointing, and this is understandableif tinnitus is due to spasm of branches of theinternal auditory artery as well as branches ofthe tympanic. Bearing this in mind, I havefound that severance of the preganglionicfibres of T. i and 2 produces instantaneous andcomplete cessation of the pulsating type oftinnitus, thereby ' clearing the head' andgreatly improving the aural acuity. Furtherwork is being done on this question and alsoits relation to the aetiology of treatment of earlyotosclerosis, and when sufficient material isavailable it will be presented. One patientsuffering from early otosclerosis upon whoma stellectomy was performed, showed a markedgain in hearing with complete cessation of thetinnitus after operation, although the hearingstill continues to deteriorate and the tinnitus topersist on the unoperated side.
It is still questionable whether it is desirableto perform a sympathectomy on both sides ornot. The innervation of the internal auditoryartery may or may not be by fibres from boththoracic chains. It is yet to be proved that it isnecessary to operate on both sides to producethe effect on one ear only. Up to now mostof the work on the -sympathetic supply of thevessels to the ear has been done on the superior
by copyright. on June 8, 2020 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.23.265.507 on 1 Novem
ber 1947. Dow
nloaded from

November I947 PASSE: Fenestration Operationfor Otosclerosis 515
or inferior cervical ganglion, but this neglectsthe branches to the vertebral artery which aremost important. Possibly the operation ofchoice would be periarterial sympathectomy ofthe internal auditory artery. This producesthe same excellent result, but is a moreformidable operation. I am convinced thatresection of the plexus promontorium is onlyof use in cases of tinnitus which may be due toirritation of this plexus by inflammation. Manypatients complain during the first five or sixdays of severe noises in the operated ear, whichsubside within the next few weeks. This maybe an example of tinnitus due to irritation ofthe plexus promontorium.
6. The Results of the FenestrationOperation and Comparison withthose obtained by Hearing AidThe testimony obtained by Shambaugh in
his questionnaire to 853 patients who hadundergone the fenestration operation revealsthat' many patients who have had the fenestra-tion operation and who regard the results assatisfactory assert without qualification thatthey hear better now than they did with theiraid, and without the distortion, the nuisanceand the upkeep expense of an aid.'Time and time again the same feelings have
been expressed to me by patients, not one ofwhom has-stated that they prefer the hearingobtained with an aid. Without exception theyappear only too relieved to be able to do with-out it.
The Results of the FenestrationOperationPossibly in this operation more than.in any
other one must state that the results dependupon the individual care in selection and theskill of the operator. In discussing the resultsof the fenestration operation it is necessary todivide the results into groups, namely: (I)those in whom the hearing has been restoredto the practical conversational level; (2) thosein whom the hearing loss was very great and inwhom, although the hearing has not beenrestored completely to the conversational level,yet it has been materially improved to theextent that the patient is now able to use ahearing aid of a smaller, less powerful and moreconvenient type; and (3) those cases of boththe above groups in whom the hearing losshas been prevented from further deteriorationfor an indefinite period. Whether or not theoperation in successful cases arrests or preventsthe usual nerve degeneration of otosclerosiscannot yet be answered with certainty owingto the limited duration of results so far avail-able. In the U.S.A., surgeons who haveresults of longer duration than myself statethat a further nerve degeneration in theoperated ear of successful cases has rarely beenobserved. From my own present series of twoyears' duration I can report a similar result.If the hearing is not improved although thefenestra remains open, are we justified inassuming that further degeneration of thecochlear nerve will not take place ? This also
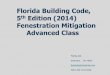
INTERIM RESULTS
Hearing improved Hearing improvedSeries. Total No. of Hearing never but improvement Hearing and fully
cases. improved. lost later. worse. maintained.
1936/39 36 5 28 I Two of eightyears' duration.
1945/46 with coch- 53 of one to twolear stopple 100oo 7 36 3 years' duration.
1946/47 enchrondral- 153 during lastized fistula. i66 I x 2. None twelve months.
FIG., 9.
by copyright. on June 8, 2020 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.23.265.507 on 1 Novem
ber 1947. Dow
nloaded from

5I6. POST GRADUATE MEDICAL JOURNAL November x947
remains unanswered. Much has been said oflate concerning improvement of hearing ob-tained in the unoperated ear in those cases inwhom the fenestration operation has resultedin improved hearing in the operated ear. Care-ful examination of the unoperated ear in alarge percentage of cases has shown that someslight improvement does occur up to io or 15decibels, but that this improvement is purelytemporary in nature and in not any of mycases has it persisted over more than sixmonths. This phenomenon may account forthe facility with which some patients hear thenurse or the surgeon during the first 24 to 48hours after the operation, for the operated earis packed with a dressing and bandaged, thusmaking hearing for ordinary speech impossible,as I have proved experimentally on myself.Conversely, in one case in which I performedthe fenestration operation on the second ear,it was noted by the patient that the hearing inthe operated ear markedly deteriorated duringthe period of post-operative labyrinthitis, butrecovered again as this subsided.
Concerning the permanency of the hearingimprovement the final answer is yet to beobtained. In the early days of this operation,bony closure almost invariably occurred withrecurrence of deafness to at least the pre-operative level. As a result of the introductionof the enchrondralized type of fenestra it hasbeen affirmed that cases operated on andfollowed up for more than six years show acessation of osteogenesis tending to close thefenestra once healing is completed. In orderto be on the safe side an arbitrary time of twoyears has been chosen as a reasonable time forosteogenesis to come to an end, and the hearingimprovement maintained for two years may beregarded as almost certainly permanent. Inmy opinion the critical period is six months,though, as I have stated before in my seriesfor last year, in no case has the fistula closed.In only two cases in which an improvement inhearing* has occurred has there been up to dateany marked deterioration in hearing. I havefound that a slight depreciation of 5 to Io
* 9i per cent. of Group I showed an improvementin their hearing.
decibels may occur from time to time, depend-ing upon the patient's state of health andwhether they are tired, overworked or areunder undue nervous strain, etc. There stillremains a small percentage of cases who,though apparently suitable in every way forthe operation, give an unpredictable result.The reason for this has not yet been deter-mined so that failures do still occur, althoughpre-operative indications are satisfactory andthe operative and post-operative techniques asperfect as possible. It must be rememberedthat the hearing is never restored to normal.In my whole series I have only two patients inwhom the hearing has been restored to thenormal line and then only for one frequency ineach case. As the amount of work being per-formed in this country is increasing, I feel itwould be of considerable help if a standardcomplete and adequate record of all cases werekept over a period of at least ten years, so thatnot only may the results be tabulated, but thetechnique and incidents of the operation notedand faithfully recorded. It is only by thesemeans that a final evaluation of this operationcan be formed.
BIBLIOGRAPHYIHOLMGREN, G. (I939), Acta Otolaryngologica, 27, 338.HOLMGREN, G. (I94I), Acta Otolaryngologica, 29, 99.HOLMGREN, G. (I946), Practica oto-rhino-laryngologica, 8, 44I.JENKINS, G. T. (1913), Tr. Internal Congr. med. sect., I6, 609.KESSEL, J. (I874), Archiv far Ohrenheilkunde, 8, 23I.LEMPERT, J. (I938), Archives of Otolaryngology, 28, 42.LEMPERT, J. (I940), Archives of Otolaryngology, 31, 7II.LEMPERT, J. (I942), Archives of Otolaryngology, 36, 473.LEMPERT, J. (I945), Archives of Otolaryngology, 41, I.LEMPERT, J. (I946), Archives of Otolaryngology, 43, 199.LEMPERT, J., and WOLFF, D. (I945), Archives of Otolaryngology,
42, 339.PASSE, E. R. G. (I9g9), Journal of Laryngology, 54, 567.PASSE, E. R. G. (I946), Proceedings of Roy. Soc. Med., Vol. XL,
No. 4, 319-320.PASSE, E. R. G. (I947), Lancet, Feb. I.SI-AMBAUGH, G. C. (I940), Archives of Otolaryngology, 32, 927.SHAMBAUGH, G. C. (I946), Kansas City Med. Yournal, March-
Apiil.SHAMBAUGH, G. C. (1946), Archives of Otolaryngology, 43, 549.SHAMBAUGH, G. C. (I942), J.A.M.A., 119, 243.SHAMBAUGH, G. C. (1942), Annals of Otology, 5I, 817.SHAMBAUGH, G. C. (I945), Quarterly Bulletin, Univers. med.
school, Chicago, N. 4, 19, 259.SHAMBAUGH, G. C. (I945), Archives of Otolaryngology, 41, 189.SHAMBAUGH, G. C. (I944), The American Acad. of Ophthalm. and
Otology. Graduate Lecture 65.SHAMBAUGH, G C. (I946), J.A.M.A., 130, 999.SHAMBAUGH, G. C. (I947), Surg. Gynec. and Obstet., 'The
Fenestration operation; an evaluation of its present status,"84, 825.
SOURDILLE, M. (I935), Sociite Fran§aise de Laryngologie, Oct.SOURDILLE, M. (1930), Journal of Laryngology, 45, 6o0.
by copyright. on June 8, 2020 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.23.265.507 on 1 Novem
ber 1947. Dow
nloaded from