Embed Size (px)
Citation preview

Aditi Kapur et al
140
Factors leading to Nonhealing of severe Lip and Tongue Ulceration in a 10-month-old Infant with Spastic Quadriplegia1Aditi Kapur, 2Sudhir Bhandari, 3Ashima Goyal, 4Krishan Gauba, 5Manoj A Jaiswal
ABSTRACT
This paper reports a 10-month-old spastic quadriplegic male child presenting with severe ulceration of ventral surface of tongue and lower lip due to the presence of mandibular and maxillary primary central incisors. The patient was on antiepileptic medication since birth. The recent development of ulcers aggravated the already deficient dietary intake due to his compromised medical status. After considering various treatment modalities, a conservative approach to cover the mandibular teeth and gum pads with a splint made in a flexible denture material was decided. The appli-ance incorporated an extraoral wire component for prevention of risk of inadvertent ingestion and to aid in attaching retentive components as and when needed. The challenges faced by the clinicians and the pitfalls influencing the ultimate outcome with this intervention are described.
Keywords: Infant, Lip ulceration, Spastic quadriplegia.
How to cite this article: Kapur A, Bhandari S, Goyal A, Gauba K, Jaiswal MA. Factors leading to Nonhealing of severe Lip and Tongue Ulceration in a 10-month-old Infant with Spastic Quadriplegia. J Postgrad Med Edu Res 2017;51(3):140-143.
Source of support: Nil
Conflict of interest: None
INTRODUCTION
Tongue biting has frequently been associated with epi-lepsy1 and cerebral palsy.2,3 When it occurs in an infant, it manifests as a severe condition leading to panic and stress among the parents apart from discomfort to the
jpmer
CASe repOrT
1,2Associate Professor, 3Professor, 4Professor and Head 5Research Officer1Department of Paediatric and Preventive Dentistry, Oral Health Sciences Centre, Postgraduate Institute of Medical Education and Research, Chandigarh, India2Department of Prosthodontics, Oral Health Sciences Center Postgraduate Institute of Medical Education and Research Chandigarh, India3-5Department of Oral Health Sciences, Postgraduate Institute of Medical Education and Research, Chandigarh, India
Corresponding Author: Sudhir Bhandari, Associate Professor, Department of Prosthodontics, Oral Health Sciences Center, Postgraduate Institute of Medical Education and Research, Chandigarh, India, Phone: +919501866133, e-mail: [email protected]
10.5005/jp-journals-10028-1250
child. Treatment of such a condition has varied from very conservative methods, such as grinding the tooth surfaces,4 placement of composite on incisal edges of teeth,5 perform-ing formocresol pulpotomies and crown amputations,6 to more radical ones like extraction of the offending teeth.7,8 Placement of intraoral splints too has been successfully attempted,9,10 though retention, prevention of risk of inadvertent ingestion, and compliance of child always remain a challenge. To relieve the child of pain, extraction of teeth is usually the last alternative a clinician explores, especially in the absence of equally predictable results with other management strategies.11 This paper reports an attempt toward conservative management of a case of severe tongue and lip ulceration in a 10-month-old infant diagnosed with spastic quadriplegia soon after birth. It also highlights the pitfalls influencing the ultimate outcome of the attempted management strategy for this patient.
CASE REPORT
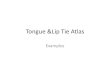
A 10-month-old male child was brought to the out-patient department of pediatric dentistry, with the chief complaint of pain and discomfort due to frequent injury to tongue from the lower front teeth during seizure epi-sodes for the past 2 to 3 weeks. The mother complained of inability of the child to take milk since the develop-ment of ulceration. The baby was observed to be under-weight and weak, weighing only 4.75 kg a week prior to the examination, as per hospital records. A detailed medical history revealed that the child was diagnosed with spastic quadriplegia and epilepsy soon after birth. He was the second born child to healthy parents and a normal sibling, and was on antiepileptic medication since birth. An intraoral examination revealed severe ulceration on the ventral surface of tongue with impressions of the erupting lower incisors (Fig. 1). The maxillary right primary central incisor, which had barely cut through the mucosa, had also led to ulceration of the lower lip (Fig. 2). The child was not breastfeeding and had been given milk with a spoon since birth. The intake of milk had remark-ably reduced since the appearance of ulcers. The frequent biting of the tongue and the lower lip during episodes of epileptic fit was attributed as the cause of his present condition. An increase in the dose of the antiepileptic medication, as advised by the pediatrician, was not successful in controlling it.

Factors leading to Nonhealing of severe Lip and Tongue Ulceration
Journal of Postgraduate Medicine, Education and Research, July-September 2017;51(3):140-143 141
Jpmer
Management
As the first line of treatment, the edges of the erupting lower central incisor and the maxillary right central incisor were rounded off using a soflex disk (Sof, Lex, 3M ESPE). The parents were told to apply a chlorhexidine gluconate gel (1.0% w/v, Hexigel, ICPA, India) on the affected areas and were explained about the importance of gum pad cleaning. Four days following the intervention, there was a slight improvement in the lower lip ulceration but no perceptible change in the tongue ulceration. Two treat-ment options were hence, considered and discussed with parents: (1) Extraction of all erupted and erupting teeth and (2) fabrication of an appliance to cover the surfaces of teeth and also to separate the upper and lower arches in the event of clenching, and preventing the tongue to come in between. Keeping in view the overall condition of the child, the second treatment option was chosen as a more conservative way of managing the present condition. A preliminary impression of the mandibular arch, which was selected for appliance fabrication, was made by simply molding the polyvinyl siloxane putty
(Elite HD, Plus, Zhermack, Italy) on the arch, with the patient lying in a semi-reclined position in his mother’s lap. The impression was poured in dental stone (Fig. 3) and a special tray was fabricated in light cure acrylic resin (TRIAD® Transheet, Dentsply). This special tray was used for making another impression in polyvinyl silox-ane light body (Elite HD, Plus, Zhermack, Italy). A wax and wire framework was made on the final cast (Fig. 4) and the appliance was fabricated in flexible denture material (Valplast, USA). The final wire bending of the extraoral retentive component was done on the patient at the time of delivery of the appliance. The patient’s mother was instructed to place the appliance in the patient’s mouth daily, for as long as the child allowed, comfortably. A review of the patient 2 days later revealed that he did not adjust well to the appliance; the mother too conveyed her own inability and lack of persistence to place the appliance correctly. In addition, the mother had faced criticism from the elderly members of the family for forcing the plate on the child. The patient, however, looked very comfortable with the appliance, and showed no obvious sign of discomfort (Fig. 5). The parent was,
Figs 1A and B: Ulceration of ventral surface of the tongue with indentations of primary mandibular incisors
Fig. 2: Ulceration of the lower lip at presentation Fig. 3: Initial impression in putty and poured in stone
A B

Aditi Kapur et al
142
therefore, motivated to continue using the appliance and was reassured about the treatment. Three days later, the ulceration on the lower lip began to show some improvement with disappearance of the tooth indenta-tions, suggesting prevention of trauma from teeth (Fig. 6). The tongue ulceration, however, remained the same. The parents were unable to bring the child at 1 week for review, but telephonically conveyed a little improvement in the lip ulceration and a very slight improvement in the tongue ulceration. There was not much improvement in milk intake, the child was still unable to suck the nipple and had to be fed with a spoon. Ten days later, however, the patient developed fever, which was diagnosed as the fever of unknown origin, requiring hospitalization. The parents, however, took the child home against the physi-cian’s advice and did not report after that.
DISCUSSION
Self-injury to oral tissues in neonates, infants, and chil-dren can be seen in many disorders, each with a different
organic, functional, behavioral, or habitual etiology, such as Lesch–Nyhan syndrome, mental retardation, cerebral palsy, congenital indifference to pain, autism, epilepsy,1 Riga–Fede disease,7 or simply as a familial tendency.10 The broad term used for such a condition is self-injurious behavior (SIB) defined as any act causing intentional harm to self.1,3
The child in the present case was diagnosed with spastic quadriplegia soon after birth and was on anti-epileptic medication. He was weak and underweight and was unable to take proper feed. The condition had worsened after eruption of upper and lower primary incisors due to frequent tongue and lip biting during the episodes of seizure, leading to severe ulcerations. Grinding of the incisal edges of the primary mandibular and erupting maxillary incisors did not result in any relief from biting during an episode of seizure. Keeping in view the parental concerns and present condition of the child, extraction was ruled out as a treatment method as it required administration of general anesthesia. The second treatment option which involved fabrication of an appliance in a flexible denture material with an extraoral wire component for retention was attempted as a more conservative method. The various nonextraction methods that have been tried successfully in the literature are lip bumpers,12 lip shields,3 bite raising plates,9,11,13 tongue protectors,14 and occlusal splints15,16 made in acrylic or soft resin. Lee et al6 reported use of formocresol pulp-otomies and crown amputations as a more conservative method over extraction for management of such lesions in very young children. Clinicians, the world over, have successfully tried and reported innovative methods to improve the retention of soft resin occlusal splints, which is a challenging task to achieve in children aged less than 2 years with absence of a fully erupted primary dentition. Chen and Liu17 used head gears worn 24 hours a day to retain and stabilize splints for patients with severe SIB.
Fig. 4: Wax and wire framework Fig. 5: Child with the appliance
Fig. 6: Beginning of healing of the ulceration on lower lip

Factors leading to Nonhealing of severe Lip and Tongue Ulceration
Journal of Postgraduate Medicine, Education and Research, July-September 2017;51(3):140-143 143
Jpmer
Kozai et al14 used a tongue protector fabricated from soft denture relining material to manage tongue ulcers in a 22-month-old male child with Gaucher’s disease. Coyne and Montague8 fabricated an acrylic occlusal splint to be wired to the zygomatic arches for a 24-month-old boy with meningococcal septicemia, who developed lip and tongue biting in the recovery phase. The splint, however, could not be fit and eventually the ulcers healed following a “wait and see” approach. Suchak and Mars10 reported successful healing of severe tongue ulcerations along with interception of the habit in 10-month-old, medically healthy twin boys with a family history of self-mutilating behavior, using thermoplastic splints retained using denture adhesive.
The appliance used in this child was made with an aim to separate the upper and lower arches, in order to relieve the traumatic influence of the offending teeth on tongue and lower lip. Flexible denture base material was chosen over a rigid heat cure denture base material as it was presumed that flexible material would dissipate forces during seizure without causing injury to soft tissues. The appliance used an extraoral wire framework to prevent the risk of ingestion and also for facilitating attachments to aid in retention after the initial settling in phase. The child’s biting on the flexible denture plate further added to its retention. The appliance was of “preventive nature” and the length of time it would have to be in use could not be predicted. A strong retentive component was, therefore, needed.
Considering the age of the child, the wire framework adapted well to cheeks and did not make the child uncom-fortable. The child was uneasy at the time of placement of the appliance, but appeared comfortable once it was in its intended position. The parents, though not very edu-cated and farmers by occupation, were appreciative of the effort, unlike the grandparents, as a mild improvement in the ulceration was evident within a week’s time. The overall success of the appliance, however, was doubtful, as the patient did not report for follow-up after probably being explained about the poor prognosis of the child’s present medical condition by the physician.
CONCLUSION
We attempted a conservative method of managing trau-matic ulceration in a 10-month-old male child with spastic quadriplegia using a splint made in flexible denture material. In addition to child’s age being a major limit-ing factor in the overall success of the intervention, his medical status, lack of parent’s motivation, and prevailing notions among the elderly in the family were some of
the reasons responsible for suboptimal results. However, considering the overall scenario, the approach described is most conservative and may prove to be more success-ful in a situation where the aforementioned factors are more favorable.
REFERENCES
1. Romer M, Dougherty N, Fruchter M. Alternative therapies in the treatment of oral self-injurious behavior: a case report. Spec Care Dentist 1998 Mar-Apr;18(2):66-69.
2. Sonenberg EM. Treatment of self induced trauma in a patient with cerebral palsy. Spec Care Dentist 1990 May;10(3):89-90.
3. Zemnick CB, Richard KY, Chussid S, Soleimani K. Labial protection device for a child patient with cerebral palsy: a case report. J Implant Adv Clin Dent 2009 Aug;1(5):71-77.
4. Baghdadi ZD. Riga Fede disease: report of a case and review. J Clin Pediatr Dent 2001 Spring;25(30):209-213.
5. Goho C. Neonatal sublingual traumatic ulceration (Riga-Fede disease): reports of cases. ASDC J Dent Child 1996 Sept-Oct;63(5):362-364.
6. Lee JH, Berkowitz RJ, Choi BJ. Oral self-mutilation in the Lesch-Nyhan syndrome. ASDC J Dent Child 2002 Jan-Apr;69(1):66-69.
7. Padmanabhan MY, Pandey RK, Aparna R, Radhakrisnnan V. Neonatal sublingual traumatic ulceration – case report & review of the literature. Dent Traumatol 2010 Dec;26(6): 490-495.
8. Coyne BMC, Montague T. Teeth grinding, tongue and lip biting in a 24-month-old boy with meningococcal septicemia. Report of a case. Int J Pediatr Dent 2002 Jul;12(4):277-280.
9. Fardi K, Topouzelis N, Kotsanos N. Lesch-Nyhan syndrome: a preventive approach to self-mutilation. Int J Pediatr Dent 2003 Jan;13(1):51-56.
10. Suchak A, Mars M. Case report: a unique presentation of severe tongue biting in 10 month-old twins with a novel approach to management. Eur Arch Pediatr Dent 2010 Jun;11(3):149-150.
11. Arhakis A, Topouzelis N, Kotsiomiti E, Kotsanos N. Effective treatment of self injurious oral trauma in Lesch-Nyhan syn-drome: a case report. Dent Traumatol 2010 Dec;26(6):496-500.
12. Cauwels RGEC, Martens IC. Self-mutilation behavior in Lesch-Nyhan syndrome. J Oral Pathol Med 2005 Oct;34(9):573-575.
13. Fenton SJ. Management of oral self-mutilation in neuro-logically impaired children. Spec Care Dentist 1982 Mar-Apr;2(2):70-73.
14. Kozai K, Okamoto M, Nagasaka N. New tongue protector to prevent decubital lingual ulcers caused by tongue thrust with myoclonus. ASDC J Dent Child 1998 Nov-Dec;65(6):474-477.
15. Jeong TS, Lee JH, Kim S, Kim JH, Tootla RG. A preventive approach to oral self mutilation in Lesch-Nyhan syndrome: a case report. Pediatr Dent 2006 Jul-Aug;28(4):341-344.
16. Rasmussen P. The congenital insensitivity to pain syndrome (analgesia congentia): report of a case. Int J Pediatr Dent 1996 Jun;6(2):117-122.
17. Chen LR, Liu JF. Successful treatment of self-inflicted oral mutilation using an acrylic splint retained by a head-gear. Pediatr Dent 1996 Sept-Oct;18(5):408-410.