Embed Size (px)
Citation preview

Pre-Malignant Lesions/conditionsLeukoplakia - chronic, white, verrucous plaque with
histologic atypiaSeverity linked to the duration and quantity of tobacco and alcohol
useOccur anywhere in the oral cavity Lip, tongue, or floor of the mouth lesions are prone for progression
to SCCErythroplakia - non-inflammatory erythematous plaque
Analagous to intra-oral erythroplasia of Queyrat or SCC in situBiopsies - severe dysplasia and areas of frank invasion

Pre-Malignant Lesions…Submucous fibrosis
generalized white discoloration of oral mucosa with progressive fibrosis, painful mucosal atrophy and restrictive fibrotic bands
individuals who chew betel quid, a concoction of tobacco, lime, areca nut and betel leaves
Ultimately leads to trismus, dysphagia and severe xerostomia
5 - 10 % progress to SCC

Cancerous lesion of Lips& Oral cavityLips –SCC, Melanoma, BCC(rare)Oral cavity: -- scc: 9/10 incidence --verrucous ca: <5% low grade, slow growing rarely
metastasizes with tendency to invade deep tissue.

Cancerous lesion of Lips& Oral cavityMinor salivary gland tumor: -in the glands lining the oral cavity -adenoidcystic ca, mucoepidermoid ca, adenocarcinoma.-Sarcoma

IncidenceGlobally >300,000 people diagnosed/yearEighth most common malignancyIndia –upto 40% of all malignanciesM>FRaising trend6-7th decadeMost of the people are dying because of ignorance

INCIDENCEDemographic and clinical profile of oral squamous
cell carcinoma patients: a retrospective study ( Shenoi R, Sharma BK, et.al, Indian J Cancer. 2012 Jan;49(1):21-6:
Most common site: mandibular alveolusMajor cause: tobacco chewingMajority of patients presented in stage IIIMajority presented within 6 months of onset

Risk FactorsTobacco: About 90% of people with oral cavity
and oropharyngeal cancer use tobacco Alcohol: Drinking alcohol strongly increases a
smoker's risk of developing oral cavity and oropharyngeal cancer.
Ultraviolet light: More than 30% of patients with cancers of the lip have outdoor occupations associated with prolonged exposure to sunlight.
Irritation: Long-term irritation to the lining of the mouth caused by poorly fitting dentures

Risk Factors Cont…Poor nutrition: A diet low in fruits and vegetables is
associated with an increased risk Mouthwash: Some studies have suggested that
mouthwash with a high alcohol content Human papillomavirus (HPV) infection: Immune system suppression:Age: The likelihood of developing oral and oropharyngeal
cancer increases with age, especially after age 35. Gender: Oral and oropharyngeal cancer is twice as
common in men as in women

How tobacco affectsTobacco smoke contains >4000 chemicals, at least 60
shown to be carcinogens.Smoke less tobacco: main form: chewing, snuff at least 28 carcinogens found in smokeless form

Relative Risk factors for Oral CancersHabit Relative Risk %NoneBetel nut ChewingSmoking onlyBetel chewing + Tobacco
chewingBetel chewing + SmokingBetel+Tobacco+smoking
1%4%3-6%8-15%
4-25%20%

How Alcohol affectsChronic alcohol exposure results in increased
cancer incidence in animal model.Acetaldehyde , reactive oxygen species- main
mutagenAcetaldehyde: directly binds to DNA, alters
methyl transfer leading to hypomethylation leading to alerted gene products
Alcohol promotes cytochrome P450- which increases activation of procarcinogens( tobacco, alcohol).
Alcohol can act as solvent facilitating entry of carcinogens into cells

Role of HPV in Oral SCCRole of human papilloma virus in the oral carcinogenesis: an
Indian perspective (Chocolatewala NM, et.al. J Cancer R Ther. 2009 Apr-Jun;5(2):7-17).
Association strongest for Oropharynx, specially cancer of tonsils followed by base of tongue.
High risk HPV-16 predominate type.Commonly affects younger age groups , male, non smokers.Better outcomes, more responsive to RT, higher survival rate.

INHERITED RISK FACTORSDefective DNA repair mechanism: xeroderma
pigmentosa, ataxia telangiectasia, bloom syndrome, fanconi syndrome
Tumor suppressor gene(p53) defect: Li Fraumeni syndrome.

INHERITED RISK FACTORSRelationship between ABO blood groups and oral
cancer (Jaleel BF, et. al. Indian J Dental Research 2012 Jan;23(1):7-10:
found that people with blood group A had 1.46 times higher risk of developing oral cancer as compared with other blood group.

INHERITED RISK FACTORSAllergies and risk of head and neck cancer
(Michaud DS, et.al. Cancer Causes Control. 2012 Aug;23(8):1317-22. Epub 2012 Jun 19).
Case control studyAllergies have heightened Th2 immunityHad a 19% lower risk of HNSCC.Statistically significant for oropharyngeal cancer.HPV status does not confound or modify
associations with [email protected]

MOLECULAR BIOLOGYCytogenetic : chromosomes 3,5,8,11,17,18.Tumor suppressor genes inactivation: p16,p21,p53,RB
gene.Proto-oncogene activation: cyclinD1/PRADD1.Growth factors /receptors overexpression: EGF,EGF-
R,TGF- ,HER-2/neu,FGF,FGF-R,PDGF).ɑ

MOLECULAR BIOLOGYRAS family oncogene.Telomeres, telomerase, cell senescenceTumor immunology(role of TIL, CTL, IL-2/4/6)Tumor invasion and metastasis:(endothelial
proliferation:PGE2,TGFβ,FGF,VEGF),MMP

MOLECULAR PROGRESSION MODEL OF HNSCC CARCINOGENESIS
Normal squamous mucosaEGF, EGFROverexpression
Squamous hyperplasia Telomerase activation p16 inactivation
DysplasiaPRAD-1 amplification 3p deletion
p53 inactivation Carcinoma in-situ
4q, 5q, 8p, 13qdeletion
Invasive carcinomaMatrix metalloproteinaseOver-expression
Metastasis

DNA changesP53, p16, Ki67 immunoexpression in oral scc
( Dragomir LP, et.al, Rom jo morph embry 2012; 53(1)89-93:
positivity index- increased for p16 tumor invasion- identified with p53, Ki67.Study highlights value of immunostain for p16 in
identifying dysplastic lesionPredictive importance of p53, Ki16 markers in
identifying aggressive form of tumour.

DNA CHANGESImmunohistochemical p53, Ki16, hTERT in oral
scc( Abraho AC et.al.Brazil oral research 2011 Jan-Feb;25(1):34-41:
p53 positivity in 93.3% of PMD, 43.3% of OSCC, 80% OEH.

Site of oral cavity Tongue : 35%Floor of mouth: 30%Lower alveolus: 15%Buccal mucosa: 10%Upper alveolus/hard palate: 8%RMT: 2%Lips: lower-93%, upper-5%, commissure- 2%

Symptomsa sore in the mouth that does not heal (most
common symptom) pain in the mouth that doesn't go away (also
very common) a persistent lump or thickening in the cheek a persistent white or red patch on the gums,
tongue, tonsil, or lining of the mouth a sore throat or a feeling that something is
caught in the throat that doesn't go away Increased salivation

More Symptomsdifficulty chewing or swallowing difficulty moving the jaw or tongue swelling of the jaw that causes dentures to fit
poorly or become uncomfortable loosening of the teeth or pain around the teeth or
jaw voice changes a lump or mass in the neck weight loss persistent bad breath

Patient WorkupInvestigations : Primary: photographs incisional biopsy FNAC Orthopantogram CXR ECG Routine blood investigations

Patient Workup Investigations: for staging - CT face + neck ± CT chest - MRI - USG of neck or primary ± USG guided FNAC of suspicious lymphadenopathy - PET

INVESTIGATIONS FOR RECONSTRUCTIONAllen’s test of vascular supply to hand if a radial forearm
flap anticipated.MRA of leg vessels if composite fibula reconstruction
anticipated.Colour Doppler of chest , abdomen if DCIA(deep
circumflex iliac artery) free flap anticipatedDental impression for all maxillary tumours

STAGING OF THE DISEASEAmerican joint committee on cancer: T , N , M Tx- primary tumour cannot be assessed T0- No evidence of primary tumour T1- ≤ 2cm in greatest dimension T2- 4cm < 2cm> in greatest dimension T3- > 4cm in greatest dimension

STAGING OF THE DISEASE T4a- Oral cavity: tumour invades through cortical bone, into deep(extrinsic) muscle of tongue, maxillary sinus or skin. Lips: cortical bone, inferior alveolar nerve, floor of mouth, skin i.e. chin or nose.
T4b- involves masticator space, pterygoid plates, skull base and/or encases internal carotid artery

STAGING OF THE DISEASEN stage: Nx- regional lymph nodes can not be assessed. N0- no regional lymph node metastasis. N1- metastasis in a single ipsilateral lymph node ≤ 3cm in greatest dimension. N2a- metastasis in a single ipsilateral LN > 3cm but < 6cm in greatest dimension.

STAGING OF THE DISEASE N2b- metastasis in multiple ipsilateral LNs, none > 6cm in greatest dimension. N2c- metastasis in B/L or C/L LNs, none > 6 cm. N3- metastasis in a LN > 6 cm in greatest dimension
M stage: Mx- cannot be assessed, M0- no distant metastasis, M1- distant metastasisi.

Stage Grouping
Stage 0 Tis N0 M0 Stage I T1 N0 M0Stage II T2 N0 M0Stage III T1, T2 N1 M0
T3 N0, N1 M0Stage IV A T1, T2, T3 N2 M0
T4a N0, N1, N2 M0Stage IV B Any T N3 M0
T4b Any N M0Stage IV C Any T Any N M1

TREATMENTTreatment goals: to eradicate primary tumor and LN
metastasis, to maintain function, cosmetic reconstruction
Factors affecting choice of treatment: tumor factor patient factor resource factor

Treatment Goals forCancer of the Oral Cavity• Cure of cancer• Preservation or restoration of form and
function• Avoid or minimize sequelae of treatment• Prevent second primary cancersPalliationRestore cosmesisMinimise morbidity and mortality

TUMOR FACTORS AFFECTING TREATMENT• Site• Size (T stage)• Location• Multiplicity• Proximity to bone• Pathological features• Histology, grade, depth of invasion, tumortype• Status of cervical lymph nodes• Previous treatment

TREATMENTPatient factors: age, general medical condition, performance status, occupation, lifestyle(smoking/drinking)
socioeconomic considerations previous treatment

TREATMENTPhysician factors: surgery, radiotherapy, chemotherapy nursing & rehabilitation services,
dental, prosthetics, support services

Treatment Surgery Radiotherapy Chemotherapy ImmunotherapyTargeted therapyGene therapy

Treatment of ChoiceStage I , II: single modality treatment is effective and
preferable.Stage III , IV: multimodal therapy is essential

TREATMENTSURGERY:
Early stage T1/2No tumor: Wide excision +/ - NDHigh risk of locoregional recurrent (40%)
Management of No Neck:High incidence of occult metastasis in the clinically No Neck (15-43%)Controversy : Observation or Surgery/RadiationDepend on primary site. Should be have minimal morbidityELND if risk of occult meta >20%. (SND/SOHND).
Locally advanced tumor: Combined modality treatment

Classification of ND1991 Classification:RNDModified RNDSelective ND:
SupraomohyoidLateralPosterolateralAnterior
Extended ND
2001 Classification:RNDModified RNDSelective ND (SND):
SND (L.I-III/IV)SND (L.II-IV)SND (L.II-V)SND (L.VI)
Extended ND
Proposed by American HN Society and AAOHNS

Standard treatment options for management of lymph node:Radiation therapy alone or neck dissection:
N1 (0–2 cm).N2b or N3; all nodes smaller than 2 cm. (A combined surgical and radiation therapy approach should also be considered.)
Radiation therapy and neck dissection:N1 (2–3 cm), N2a, N3.
Surgery followed by radiation therapy, indications for which are as follows:
Multiple positive nodes.Contralateral subclinical metastases.Invasion of tumor through the capsule of the lymph node.N2b or N3 (one or more nodes in each side of the neck, as appropriate, >2 cm).
Radiation therapy prior to surgery:Large fixed nodes.

SURGICAL APPROACHES Trans-oral approach Lower cheek approach Upper cheek approach mandibulotomy Visor flap

Surgical approach depends on• Tumor size• Tumor site• Tumor location• Proximity to mandible or maxilla• Need for neck dissection• Need for reconstructive surgery

Factors predicting positive marginLarge tumour.Perineural spread.Vascular permeation.Noncohesive invasive frontCervical metastasis

Carcinoma tonguePathological types1. nonhealing ulcer2. proliferative growth with everted edge3. indurated variety with frozen tongue4. fissure variety

Carcinoma tongue - clinicalBleeding ulcerPainAnkyloglossiaDysarticulationDysphagiaFetor orisNeck nodes

Carcinoma tongue- surgeryWide local excision – CISPartial glossectomyHemiglossectomyTotal glossectomyNeck dissectionFlap reconstruction- PMMC/DP/FREE ALT/FRFF

Oral competenceDeglutitionArticulationExpression of emotionSymbol of beauty
Lip Function

EPIDEMIOLOGY
It is one of most common malignant tumor affecting
head & neck
Squamous cell Carcinoma is most common in India
Factors affecting are:
1. Solar radiation
2. Tobacco smoking
3. Viruses
LIP CANCER

Male:female ratio – 14:1
Lower lip > upper lip (solar radiation)
90% : lower lip
6%: oral commissure
4%: upper lip

1. Lip should have sensation, motion, prevent drooling, permit speech & resonable cosmetic appearance.
2. Full thickness skin flaps used whenever possible3. It should provide sufficient mucosa contiguous to
commisure to avoid contracture
Principles of lip repair

FIGURE 2. Direct excision and repair of lower l ip lesions. Lesions up to one half of the l ip can be excised and repair primarily.Small lesions can be excised using the "V" excision, and can be angled to blend into the chin-lip crease. Larger lesions can beexcised using a "W" pattern. The "W" avoids crossing the chin-lip crease and retains an adequate margin of tissue around thelesion inferiorly. The largest lesions can be excised as a rectangle and incisions made in the chin-lip crease to allow advancementof lateral lip tissue for [email protected]

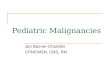
FIGURE 6. Abbe cross lip flap. (A)"V"-shaped incision diagramed around lowerlip lesion and proposed upper lip flap outlined.(B) Lesion removed, flap rotated and suturedinto defect. Flap is designed with height 1 to 2mm greater than defect to be reconstructed

FIGURE 6. Estlander cross lip flap. (A)"V"-shaped incision diagramed around lowerlip lesion and proposed upper lip flap outlined.(B) Lesion removed, flap rotated and suturedinto defect. Flap is designed with height 1 to 2mm greater than defect to be reconstructed.

Karapandzic flap, (A) Lower lip defect after resection of carcinoma. Proposed incisions outlined. (B) Incisions madethrough skin. Buccal branches of facial nerve and labial artery branches preserved to greatest extent possible. (C) Tissueadvanced and defect closed.

RADIOTHERAPYApplications: - Radical : early tongue cancer - palliative : advanced total control not possible: 20Gy
x5 daily fractions x 1 week. -combined therapy. -preoperative. -postoperative.

POST-OP RTIndications:-presence of nodal disease with exptracapsular spread.-presence of involved surgical margin-excision margin less than 5mm.-stage III/IV.-perineural or vascular invasion.-poor differentiation.-oral cavity primary.-multicentric primary.->4 nodes positive.-soft tissue invasion.-dysplasia or carcinoma insitu at resection margin.

IMMUNOTHERAPYHPV Vaccines
Estimated that 25% of HNSCC are HPV associated Tend to arise in younger patients Lingual and palatine tonsils Occur predominantly in non smoker/drinker Associated with a more favorable prognosis
HPV viral oncogenes E6 and E7 are consistently expressed in HPV associated cancers Thought to integrate into the host DNA, and when expressed, bypass
the regulation of cell proliferationBoth protein and DNA vaccines targeting HPV DNA are currently
in phase I and phase II trials

TARGETED THERAPYTargeted therapy in head and neck cancer: state
of the art 2007 and review of clinical applications( Langer CJ. Cancer 2008 Jun 15;112(12):2635-45:
-anti-EGFR monoclonal antibody(MoAb) cetuximab first targeted therapy to be developed
-single agent cetuximab confer clinical benefits in patient with cisplatin refractory metastatic disease.

TARGETED THERAPYMolecular targeted therapies in head and neck cancer - An
update of recent developments(Martin Goerner, et.al, Head & Neck Oncology 2010, 2:8):
-anti-EGFR MoAbs :cetuximab , pantimumab, zalutumumab -EGFR targeted tyrosine kinase inhibitors: gefitinib, erlotinib - EGFR & HER-2 combined tyrosine kinase inhibitors: lapatinib, BIBW-2992. - VEGFR inhibitor: bevacicumab, sorafenib, sunitinib.

GENE THERAPYGene therapy for oral squamous cell carcinoma: An
overview( TR Saraswathi, et.al, Indian J Dent Res. 2007 Jul-Sep;18(3):120-3)
STRATEGIES: -genegene addition therapytherapy: reconstitution of wild type p-53 function
with p-53 expressing adenovirus-> led to inhibition of SCC cell lines.
- antisense RNA therapy: introducing a remedial gene that prevents expression of a specific defective gene: potential target E6 & E7 genes of HPV.
- suicide gene therapy: introduction of a gene into a cell inabling a prodrug to be activated into an active cytotoxic drug.

Recurrent lips & oral cavity cancerSurgery is preferred, if radiation was used initially.Surgery, radiation or combination if surgery used
initially.Chemotherapy , but no increase in survival
demonstrated.Other novel therapy method

PROGNOSISLocation/thickness/depth of primary tumorStagingType of histologyGradingPresence of perineural spreadMandibular invasionLn extension (Level, size, exptracapsular)Molecular markers (?)

What happens after Treatment?Speech and Swallowing Therapy Follow-up tests Chemoprevention Watch for new symptoms General health considerations

SummaryRisk factorsPremalignant lesionsSign and symptomsInvestigationsTNM staging and diagnosisTreatment plan SurgeryRadiotherapyChemotherapyFollow up