Embed Size (px)
Citation preview

W358 AJR:203, October 2014
ent immediately after endograft placement or may result from hemodynamic stress incurred on the device over time. Proper surveillance re-lies on appropriate imaging protocols and in-terpretation. The initial procedure, secondary procedures that may be necessary to address complications, and surveillance scans expose patients to a significant radiation dose. Cumu-lative radiation risk is a concern as techniques and devices advance and patients live longer af-ter treatment. This article reviews post-EVAR surveillance imaging modalities and complica-tions that must be recognized and appropriate-ly reported by the interpreting physician.
Posttreatment SurveillanceCT angiography (CTA) is the current refer-
ence standard for surveillance and is the pri-mary imaging modality at most centers. CTA provides a sensitive evaluation for many im-portant complications, and patients will com-monly undergo numerous surveillance scans during their lifetime. However, CT may not be the ideal modality for surveillance primarily because of high accumulative radiation doses and the risk of contrast-induced nephropathy. Several studies show the benefits of alterna-tive ultrasound and MRI surveillance proto-cols. Each imaging modality has advantages and disadvantages that should be considered when developing a surveillance program.
CTCTA effectively detects migration, kink-
ing, structural failure, endoleak, infection, and aneurysm growth [3]. Surveillance CTA
Essentials of Endovascular Abdominal Aortic Aneurysm Repair Imaging: Postprocedure Surveillance and Complications
Andrew C. Picel1Nikhil Kansal2
Picel AC, Kansal N
1Department of Radiology, University of California San Diego, 200 W Arbor Dr, San Diego, CA 92103-8756. Address correspondence to A. C. Picel ([email protected]).
2Department of Vascular Surgery, St. Elizabeth’s Medical Center, Brighton, MA.
Vascular and Inter vent iona l Radiolog y • Review
WEB This is a web exclusive article.
AJR 2014; 203:W358–W372
0361–803X/14/2034–W358
© American Roentgen Ray Society
Endovascular abdominal aortic aneurysm repair (EVAR) con-sists of placing a stent-graft with-in the aorta to exclude the aneu-
rysm from arterial circulation and reduce the risk of rupture. The procedure may be per-formed with surgical groin exposure or by a totally percutaneous technique using vascu-lar closure devices. Detailed preprocedural anatomic evaluation is necessary to properly plan the EVAR procedure and reduce the risk of endograft failure and secondary complica-tions. Postprocedural surveillance is per-formed to evaluate for complications that may lead to aneurysm rupture and to help plan secondary treatments.
Complications after EVAR can be life threatening and necessitate prompt diagnosis and intervention. Overall complication rates are as high as 30%, and the rate of late com-plication requiring intervention is 2–3% [1, 2]. Effective surveillance should monitor for persistent aneurysm growth, new aneurysm formation, endoleak, device migration and kinking, graft thrombosis, infection, and ac-cess site complications. Patients who undergo EVAR often have complex disease, and sur-veillance must be effective in the presence of associated vascular pathology, such as dense aortic calcification, arterial stenosis, occlu-sions, and dissection.
Lifelong imaging surveillance is neces-sary to detect complications, which are of-ten asymptomatic. Early detection allows the potential to intervene and prevent aneurysm growth and rupture. Complications may pres-
Keywords: abdominal aortic aneurysm, endoleak, endovascular aortic aneurysm repair, EVAR complica-tions, imaging surveillance
DOI:10.2214/AJR.13.11736
Received October 18, 2013; accepted after revision May 29, 2014.
N. Kansal is a consultant for Endologix, Inc..
OBJECTIVE. Lifelong postprocedural imaging surveillance is necessary after endovas-cular abdominal aortic aneurysm repair (EVAR) to assess for complications of endograft placement, as well as device failure and continued aneurysm growth. Refinement of the sur-veillance CT technique and development of ultrasound and MRI protocols are important to limit radiation exposure.
CONCLUSION. A comprehensive understanding of EVAR surveillance is necessary to identify life-threatening complications and to aid in secondary treatment planning.
Picel and KansalPostprocedure Monitoring of Endovascular Abdominal Aortic Aneurysm Repair
Vascular and Interventional RadiologyReview
FOCU
S O
N:
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by C
olum
bia
Uni
vers
ity o
n 09
/29/
14 f
rom
IP
addr
ess
128.
59.2
22.1
2. C
opyr
ight
AR
RS.
For
per
sona
l use
onl
y; a
ll ri
ghts
res
erve
d

AJR:203, October 2014 W359
Postprocedure Monitoring of Endovascular Abdominal Aortic Aneurysm Repair
traditionally includes unenhanced, arterial phase (30-second delay), and delayed phase (120- to 300-second delay) sequences. Un-enhanced images are used to differentiate hyperdense calcifications from an endoleak that may appear on the arterial or delayed phase. The delayed phase is important to as-sess for a low-flow endoleak that may not be apparent on the earlier arterial phase images. A study using a dynamic CT technique with multiple early scan phases [4] found that the highest rate of endoleak detection occurred 27 seconds after reaching the preset bolus-tracking threshold. This finding suggests that the ideal timing for endoleak detection occurs at a time point between standard arte-rial phase and venous phase images [4].
CTA is more sensitive than conventional angiography for detecting endoleak. How-ever, angiography better determines the di-rectionality of blood flow and more accu-rately classifies the type of endoleak. Blood flowing out of the lumbar arteries or the in-ferior mesenteric artery (IMA) suggests a type I or type III endoleak. Inflow of blood through these vessels is consistent with a type II endoleak. The timing at which con-trast appears in the aneurysm sac is also im-portant for classification. A type I endoleak will be manifest as early contrast opacifica-tion along the stent-graft attachment sites, whereas a type II endoleak will appear on more delayed images [5–7].
For each surveillance study, CT size mea-surements should be precisely compared with prior measurements. A standardized measurement protocol helps limit interob-server variability. Measurements should be obtained in a plane perpendicular to the an-eurysm centerline with fine calipers using the outer aneurysm wall as the boundary (adventitia-to-adventitia) [8]. Advanced re-construction techniques should be used to ensure accurate measurements, including 2D multiplanar reformations, curved pla-nar reformations created on lumen center-line, and 3D reconstructions. In tortuous vessels, in the absence of multiplanar refor-matted images, measuring greatest diam-eters may be inaccurate. However, if com-pared with similar measurements on prior studies, interval change can be appropriate-ly assessed.
CT also provides the ability to calculate the aneurysm sac volume. Studies suggest that changes in aneurysm diameter and vol-ume may be discordant with calculated vol-umes providing a more accurate assessment
of aneurysm growth [6, 9, 10]. Volume cal-culations commonly require manual seg-mentation on a dedicated workstation, with postprocessing taking up to 45 minutes. A 2% volume increase is proposed as a thresh-old to identify endoleaks after EVAR [9]. Calculating volumes is more time consuming than simple diameter measurements and does not allow coregistration of interval studies. As automated reconstruction software is de-veloped, CT volumetry will become less time consuming and more practical for clinical use.
Contrast-induced nephropathy, cumulative radiation exposure, and cost are concerns in lifelong CTA surveillance. Traditional sur-veillance protocols consist of a baseline CT at 1 month after repair, followed by 6-month in-terval scans with a transition to yearly stud-ies in the absence of complications. Early an-eurysm sac shrinkage may be associated with fewer late complications after EVAR [11]. Therefore, it may be feasible to lengthen the interval to 1 year when the aneurysm sac is smaller than 5 cm or has decreased by 5 mm. When the sac size decreases to 4 cm, CT may then be obtained every 2–3 years [12]. Stud-ies also suggest that the surveillance interval can be lengthened in the absence of complica-tions on the 1-month posttreatment scan, and the 6-month follow-up scan may be eliminat-ed without adverse outcomes [13, 14].
Adjusting the CT scan technique can also reduce the radiation exposure. A tripha-sic CT scan may not be necessary for rou-tine surveillance. It is possible that the un-enhanced scan is needed on only the first surveillance examination and may be omit-ted thereafter in the absence of complica-tions. Routine delayed images may also be unnecessary, although a low-flow endoleak could be missed on the arterial phase study [15]. Others propose that eliminating the arterial phase would lead to reduced radia-tion exposure and still allow the detection of an endoleak on delayed images [16]. In ad-dition, a comparison of aortic volumes cal-culated from contrast-enhanced and unen-hanced sequences found no difference in volume measurements, with a significant re-duction in radiation exposure [17, 18]. This implies that unenhanced CT with volume analysis may be sufficient for follow-up in patients with contraindications to IV contrast agent administration or to limit the radiation exposure from multiple series. A change in the aneurysm sac volume would prompt an immediate contrast-enhanced study to evalu-ate for endoleak [19].
Several radiation dose–reduction tools are available on modern CT scanners and should be used for surveillance scans. Automatic exposure control adjusts the radiation dose according to patient size and tissue attenua-tion. Automatic exposure control modulation software can reduce the dose by up to 40–50% [20]. Iterative reconstruction loops can be used to reduce image noise and improve resolution, which results in the production of diagnostic-quality studies at a significantly lower dose [21]. Dual-energy CT allows si-multaneous acquisition of CT data with two different photon energy levels. Using this method, iodine can be subtracted and virtu-al unenhanced images can be created. Dual-phase dual-energy CT can reduce the radia-tion dose 19.5% compared with a standard triphasic CT examination [22].
Additional proposals to reduce radiation exposure include performing primary sur-veillance with ultrasound and radiography [18]. CTA would then be obtained to further examine a positive finding, such as expan-sion of the aneurysm sac [6, 23]. Some au-thors suggest that, in asymptomatic patients, it may be sufficient to abandon CT after 1 year of surveillance and follow diameter measurements and structural stability with ultrasound and abdominal radiographs [24].
RadiographyAnteroposterior and lateral radiographs
are often obtained with CTA to provide a global assessment of stent-graft position and integrity [23] (Fig. 1). Device migration, wire frame fracture, and kinking may be identi-fied. Radiographs should be consistently cen-tered to reduce geometric distortion. The po-sition of the stent-graft relative to anatomic landmarks is compared on serial radiographs. Oblique projections are acquired to improve the detection of wire frame fractures [6]. Ra-diographs should be obtained before the CTA examination to avoid contrast material in the urinary collecting system obscuring the en-dograft framework. Ultrasound and MRI provide a limited evaluation of stent-graft in-tegrity, and concurrent radiographs are re-quired for complete evaluation. The impor-tance of accurately describing the stent-graft appearance and position on radiographs may increase as radiation-sparing ultrasound and MRI protocols are developed and become more common in clinical practice. Radio-graphs do not provide an assessment of an-eurysm sac size and are not useful as a stand-alone screening modality.
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by C
olum
bia
Uni
vers
ity o
n 09
/29/
14 f
rom
IP
addr
ess
128.
59.2
22.1
2. C
opyr
ight
AR
RS.
For
per
sona
l use
onl
y; a
ll ri
ghts
res
erve
d

W360 AJR:203, October 2014
Picel and Kansal
Ultrasound ImagingDuplex ultrasound can be technically de-
manding in obese patients, as well as those with extensive arterial wall calcifications, but in many cases it can accurately reveal the proximal and distal fixation sites and deter-mine the aneurysm sac size [12] (Fig. 2). Ul-trasound measurements appear to be compa-rable to those obtained by CTA [25–27]. In certain cases, ultrasound dimensions may be more accurate because of overestimation on axial CT measurements. It is likely that ultra-sound diameters are equivalent to those mea-sured on reconstructed CT centerline of flow images [28]. A high degree of interobserv-er and intraobserver variability in diameter measurements suggests that ultrasound and CT should not be used interchangeably, but consistent use of an ultrasound or CT proto-col should be adopted for surveillance [28].
Color Doppler and spectral waveforms provide useful hemodynamic information. Endoleaks appear as pulsatile color-flow within or adjacent to the aneurysm sac. Bi-directional flow and lower peak systolic ve-locities are associated with spontaneous en-doleak closure [5, 29, 30]. A recent study suggests that 3D ultrasound can provide vol-ume estimation of the aortic sac with high technical success. Although 3D ultrasound is not currently used clinically, it may provide a sensitive measure of aneurysm growth, simi-lar to volumetric CTA [31, 32]. Ultrasound is limited in revealing kinking and migration of the stent-graft, and we suggest obtaining concurrent radiographs for surveillance.
Contrast-enhancement increases the sensi-tivity of ultrasound surveillance [33]. Several reports agree that contrast-enhanced ultrasound (CEUS) is at least as sensitive as CT for detect-ing endoleak, and there are instances of CEUS identifying endoleaks not seen on CT [34–37]. This may be because CEUS allows a dynam-ic scan time of several minutes compared with static CT images. It is possible that CEUS will detect endoleaks in cases of endotension that are not explained by CT. CEUS also provides improved endoleak classification because of the dynamic visualization of the direction of blood flow into the aneurysm sac [38, 39]. In addi-tion, a recent study described a 3D CEUS tech-nique that more effectively visualizes endoleak inflow vessels and may be more sensitive in de-tecting endoleak than 2D CEUS or CTA [40]. No major adverse effects have been found with ultrasound contrast agents [33].
Ultrasound-only surveillance protocols are under development, with some groups starting
as early as 6 months after intervention. Oth-ers initiate ultrasound surveillance depending on sac shrinkage at 1 year. Any suspicious ul-trasound finding is then evaluated with CTA [34]. Studies suggest that ultrasound can pro-vide surveillance comparable to CT and is sufficient to identify complications requir-ing intervention. However, 1- and 12-month postprocedural CT examinations may remain necessary to evaluate stent-graft position, in-tegrity, aneurysm morphologic features, and visceral vessel patency, which are not well evaluated by ultrasound [39]. Selective CTA would be performed in cases with endoleak detected on ultrasound, abdominal aortic an-eurysm diameter increase, migration on ra-diograph, or poor visibility of the stent-graft on ultrasound examination [27]. If ultra-sound-predominant surveillance is widely ac-cepted, it promises to significantly reduce ra-diation exposure and cost [41, 42].
MRIMR angiography (MRA) can detect lu-
minal patency, device positioning, and re-sidual sac flow. Nitinol stents are best suited for MRA, whereas stainless steel and co-balt-chromium-nickel alloy stents are ferro-magnetic and may result in significant arti-fact [5]. Several reports suggest that MRA is more sensitive than CTA in endoleak detec-tion [6, 7, 43–45]. In cases of endotension, the aneurysm sac increases in size without an appreciable endoleak on imaging. MRI should be considered in these cases because it is especially effective in identifying type II endoleaks that may otherwise be undetected and classified as endotension [45].
A typical MRA protocol consists of axial T1-weighted echo-gradient images and con-trast-enhanced MRA with arterial and late phase imaging. Late phase T1-weighted gado-linium-enhanced sequences are recommend-ed for detecting endoleak [7]. Time-resolved MRA and flow analysis show the evolution of contrast material in the aneurysm sac and may help classify the type of endoleak [6]. However, these sequences have inferior spa-tial resolution and are more sensitive to sus-ceptibility artifacts than T1-weighted con-trast-enhanced images [45]. Blood-pool MRI contrast agents have prolonged intravascular retention and have the potential to detect en-doleaks with slow flow rates that may be oc-cult on CT. MRI results in multiplanar im-ages with 3D reconstructions similar to CT but is limited by imaging artifacts from fer-romagnetic stents and coil material, relatively
high cost, and long examination times. MRI is ineffective in evaluating stent-graft integri-ty, and concurrent radiographs should be ob-tained for complete evaluation.
MRA avoids exposure to ionizing radiation and iodinated contrast material but is associ-ated with a potential for nephrogenic system-ic fibrosis resulting from exposure to gado-linium-based contrast material. Unenhanced MRI sequences provide an effective alterna-tive to avoid the risk of contrast material ad-ministration in patients with renal failure. One study suggests that a balanced morpho-logic true fast imaging with steady-state pre-cession (true-FISP) sequence is effective in imaging the aorta and its main branches and allows a sensitive evaluation for endoleak with a high negative predictive value [46]. Super-paramagnetic iron oxide particle–enhanced dynamic MRI may provide another useful imaging alternative in patients with renal in-sufficiency, with a recent small study showing excellent sensitivity for type II endoleak [47].
Pressure MeasurementAn investigational approach to surveil-
lance consists of monitoring the pressure within the aneurysm sac to predict negative outcomes. Pressure sensors implanted dur-ing endograft placement measure local pres-sures adjacent to the stent-graft limbs. Low pressure may indicate a shrinking aneurysm sac, and pulsatile high pressure suggests an enlarging aneurysm with possible endoleak [3, 48]. Remote pressure measurements have the potential to reduce or replace sur-veillance imaging, but further investigation is warranted before the devices are widely used. This technique does not evaluate stent-graft integrity and would not likely provide a stand-alone screening modality.
ConclusionLifelong imaging surveillance is manda-
tory to detect complications that may lead to aneurysm sac pressurization and rupture. CTA is the current reference standard for sur-veillance, but because of concerns of cumu-lative radiation exposure, several centers are investigating alternative imaging protocols. These protocols may consist of reduced-dose CT techniques or surveillance proto-cols based primarily on ultrasound or MRI. We currently perform a 1- to 2-month post-operative triple-phase CTA to evaluate for early complications and endograft position-ing. This is followed by a repeat CTA in 6 months. If no complications are detected and
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by C
olum
bia
Uni
vers
ity o
n 09
/29/
14 f
rom
IP
addr
ess
128.
59.2
22.1
2. C
opyr
ight
AR
RS.
For
per
sona
l use
onl
y; a
ll ri
ghts
res
erve
d

AJR:203, October 2014 W361
Postprocedure Monitoring of Endovascular Abdominal Aortic Aneurysm Repair
the aneurysm sac size is stable or decreased, then yearly surveillance is performed. Un-complicated cases are transitioned to yearly duplex ultrasound surveillance to follow the aneurysm sac size and evaluate for endoleak. Complications are typically followed with 6-month CT scans or go to catheter angiog-raphy for diagnosis and treatment.
Posttreatment ComplicationsSeveral complications detected on surveil-
lance imaging result in pressurization of the aneurysm sac and increase the risk of rupture. Because of postprocedural complications, re-peat interventions are necessary in 12–35% of cases [49, 50]. Most of these interventions are performed with endovascular techniques and require minimal additional hospitalization [49, 51]. The following complications detected on surveillance imaging may lead to repeat inter-vention and must be accurately recognized and described by the interpreting physician.
EndoleakAn endoleak results in blood flow outside
the stent-graft but within the aneurysm sac. Endoleaks occur in 15–25% of patients with-in the first 30 days after EVAR and are often asymptomatic [5, 52]. Lifelong imaging sur-veillance is required for detection. Endoleaks are classified according to the origin of blood flow (Table 1). Although CTA is superior for the detection of endoleak, catheter angiogra-phy better reveals the dynamics of blood flow critical for endoleak classification [53].
A type I endoleak results when blood en-ters the aneurysm sac from an attachment site and occurs after approximately 10% of EVAR procedures [54] (Fig. 3). There is di-rect communication with the arterial circula-tion, resulting in an increased risk of rupture. Landing zone characteristics that are beyond the device-specific instructions for use, such as a large, angulated, tapered, or calcified proximal neck, increase the risk of endoleak [6, 52, 55]. It is traditionally thought that ex-tensive thrombus results in a poor proximal seal and leads to a type I endoleak. Howev-er, recent reports suggest that neck thrombus may not lead to adverse outcomes in early and midterm results [56, 57].
CTA suggests the presence of a type I en-doleak when contrast material within the an-eurysm sac appears closely apposed to the proximal or distal attachment sites. Type I en-doleaks are subdivided as type Ia when the leak originates from the proximal attachment site and as type Ib from the distal attachment
site. Type Ic is a rare situation, with backfill-ing of the aneurysm sac resulting from failed embolization of the contralateral common iliac artery when an aortouniiliac device is placed in conjunction with a femoral-femoral bypass [5]. Type I endoleaks can appear in the immediate perioperative period or can present in a delayed fashion. Remodeling may result in mechanical or hemodynamic change, aor-tic neck dilation, iliac artery dilation, or in-creased iliac artery angulation that results in a delayed attachment site leak [58].
An adequate proximal seal is necessary to reduce the risk of type I endoleak. Stent-grafts were developed with hooks and barbs to help reduce migration and proximal en-doleak. Oversizing the endograft by 15–20% also helps achieve an adequate seal [52]. In cases of type I endoleak, early interven-tion is necessary to reduce the risk of rup-ture. Treatment typically consists of secur-ing the attachment sites with angioplasty balloons, stents, or endograft extensions [52, 59]. Treatment with coil embolization and glue has been successful in select cases. If the neck has expanded, placement of a fenes-trated graft or chimney grafts may prevent surgical conversion [60].
Advanced EVAR techniques, such as chimney or snorkel graft placement, require vigilant postprocedural surveillance. Varia-tions of this technique may be used when the main endograft device is positioned or ex-tended in such a manner to cover and pre-clude flow to the renal arteries, celiac artery, superior mesenteric artery (SMA), or inter-nal iliac arteries. In these cases, additional stents are placed parallel to the main stent-graft device. These additional stents extend beyond the sealing zone of the main endo-graft and provide a conduit to preserve flow to the otherwise covered aortic branches (Fig. 4). If the aorta is highly calcified, the chimney stents may not conform tightly to the aortic wall and result in a persistent type I endoleak that may require treatment. How-ever, type I endoleaks seen in the early post-procedural period may represent low flow in
the gutter formed around the chimney graft, and many resolve spontaneously. For the re-nal arteries, a literature review revealed type I endoleaks in 7% of cases after placement of a single chimney graft and in 15.6% of pa-tients receiving two grafts [61].
A type II endoleak is the most common type, occurring after 10–25% of cases [54]. This type of endoleak results from retrograde flow into the aneurysm sac from collateral vasculature, often the IMA or lumbar arter-ies (Fig. 5). Type II endoleaks are classified as type IIa when there is a single feeding vessel and as type IIb when there are multiple con-tributing vessels [5]. CT contrast agent found in an anterior location within the aneurysm sac suggests that the leak is from the IMA, and contrast agent in a posterolateral loca-tion is assumed to be from the lumbar arter-ies. One study suggests that a larger cross-sec-tional aortic diameter at the IMA ostium and a greater number of patent aortic side branches is associated with a higher incidence of type II endoleak [62]. Pre-EVAR coil embolization of the IMA may reduce the incidence of type II endoleak and aneurysm sac enlargement [63–66]. However, aortic side branch occlu-sion, particularly involving the lumbar arter-ies, is time consuming, often incomplete, and not routinely performed [67, 68].
The number of patent collateral vessels and the thickness and total circumference of mural thrombus correlate with the risk of developing a type II endoleak and aneurysm growth [59, 69–71]. Although it is suggested that lysis of thrombus within the aneurysm sac at the origin of collateral vessels may lead to a delayed type II endoleak, some studies also show a protective effect from thick cir-cumferential thrombus. The thickness and percentage circumference of aortic thrombus, particularly at lumbar artery and IMA ostia, may be inversely related to the formation of persistent type II endoleaks [72].
Up to 40% of type II endoleaks sponta-neously thrombose and immediate inter-vention is not always required [52]. Delayed type II endoleaks appear more than 1 year
TABLE 1: Endoleak Classification
Type of Endoleak Source of Blood Flow
Type I Stent-graft attachment sites
Type II Inflow from collateral vessels
Type III Structural stent-graft failure
Type IV Endograft material porosity
Type V Endotension
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by C
olum
bia
Uni
vers
ity o
n 09
/29/
14 f
rom
IP
addr
ess
128.
59.2
22.1
2. C
opyr
ight
AR
RS.
For
per
sona
l use
onl
y; a
ll ri
ghts
res
erve
d

W362 AJR:203, October 2014
Picel and Kansal
after EVAR and are often associated with increasing aneurysm size [73]. Treatment is often initiated because of the potential for increased sac pressure and rupture [74]. Al-though criteria are not evidence based, 5–10 mm of aneurysm sac expansion is often used as a threshold for intervention. However, there are reported cases of rupture without sac expansion, suggesting that a more ag-gressive approach to type II endoleak treat-ment may be warranted [75].
Endovascular treatment consists of embo-lization by a transarterial approach or direct translumbar puncture. The transarterial ap-proach consists of navigating microcathe-ters into the feeding or draining arteries and placing metallic coils to prevent retrograde flow. The IMA is catheterized through Rio-lan arcades from the SMA, and lumbar ar-teries are accessed through iliolumbar artery collaterals. The recurrence rate is high be-cause of the dynamic nature of multiple con-tributing vessels, similar to a vascular mal-formation [76]. After embolization, inflow tends to shift to other collateral vessels and the endoleak may persist. During treatment, occluding the inflow and outflow vessels re-duces the risk of recanalization, and short-term occlusion can be achieved if the embol-ic material reaches the aneurysm sac [52].
The translumbar approach is typically more effective than transarterial embolization, which tends to require multiple interventions [76, 77]. In the translumbar approach, the aneurysm sac is directly punctured under fluoroscopic or CT guidance for placement of coils and glue into the endoleak cavity and feeding vessels, if identified. By treating the endoleak cavity with embolization of the aneurysm sac itself, this technique is similar to treating the nidus of an arteriovenous malformation and eliminates the communication between aortic side-branches. It is suggested that transarterial embolization with microcatheter selection and embolization of the endoleak cavity, in addition to the feeding artery, has similar efficacy to translumbar embolization [78].
Secondary interventions for type II en-doleak are associated with high failure rates, and multiple treatments may be required, of-ten necessitating a combination of transarte-rial and translumbar approaches [77] (Fig. 6). Ethylene vinyl alcohol copolymer (Onyx, ev3) used as a secondary intervention for persistent type II endoleak is more success-ful than coil embolization alone [79]. Onyx is nonadhesive, which allows a slower pre-cise delivery. It shows predictable behavior
and is easily seen under fluoroscopy. One group achieved 73% success using Onyx as a transarterial embolic agent with improved results when Onyx reached the endoleak cav-ity [80]. Onyx may be used in combination with coils and plugs, which may protect from nontarget embolization and reduce the vol-ume of liquid embolic required [81].
Surveillance after endoleak treatment is complicated by beam-hardening artifact from coils and glue used as embolic material. The tantalum component of Onyx improves visibil-ity under fluoroscopy but results in CT streak artifact. This artifact may obscure fine detail, but measurement of aneurysm sac size to as-sess interval growth is often possible [82]. It is important to obtain an unenhanced CT series to differentiate high-density embolic material from enhancement that may be identified on the contrast-enhanced series and indicate the presence of a persistent or new endoleak.
A type III endoleak results from a structur-al stent-graft failure or disconnection between components, with an estimated incidence of 4% after 1 year [52]. CTA reveals contrast materi-al adjacent to the endograft but often not in the aneurysm sac periphery, as seen with a type II endoleak. Arterial pulsation and sac shrinkage may distort the device or lead to migration and result in a type III endoleak [6] (Fig. 7). A tear in the graft material is classified as type IIIa. Type IIIb is a junctional gap between modular components, and type IIIc refers to other causes of device failure, such as suture breakage [6]. Repair is emergent because of rapid arterial pressurization of the aneurysm sac and the po-tential for rupture. Endovascular repair often consists of placement of a stent-graft extension or cuff to cover the site of leakage.
Type IV endoleaks result from porosity in the graft material and are seen on angi-ography immediately after placement. They usually resolve when coagulation is normal-ized. Type IV endoleaks were seen primarily during placement of early-generation devices and are typically of no clinical consequence [5]. With production advances in the new-generation devices, this type of endoleak is now uncommonly seen [52].
A type V endoleak, also referred to as endotension, occurs when there is enlarge-ment of the aneurysm sac without a detect-able leak on imaging [5]. This may be due to ultrafiltration of blood across the stent-graft, with thrombus providing an ineffective bar-rier to pressure transmission, infection, sero-ma, or failure to detect the leak on imaging [6, 52]. A type V endoleak is a diagnosis of
exclusion. Imaging with additional modali-ties, such as ultrasound and MRA, should be attempted to exclude an alternate type of endoleak that was not detected on the initial surveillance study. Intervention, including conversion to open repair, may be necessary in the presence of increasing aneurysm size.
MigrationSurveillance imaging should be evalu-
ated for migration and compared with pri-or images; 5–10 mm of migration is gener-ally considered significant [6]. Landmarks, such as the SMA and renal arteries, can be used to measure migration and provide a standard for comparison. The risk of migra-tion depends on the type of device, neck di-ameter and configuration, and length of the landing zones [83]. The degree of stent-graft oversizing may also contribute to migration, with greater than 30% oversizing resulting in an inadequate proximal seal [84]. Neck enlargement or other changes in aneurysm morphologic features over time may lead to migration, whereas suprarenal fixation is as-sociated with a lower rate of migration [85]. Migration can result in endoleak, limb occlu-sion, and rupture. Extension cuffs are often placed for treatment. Long-term results are expected to yield lower rates of migration with new-generation devices.
Limb Kinking or ThrombosisStent-graft kinking may result from migra-
tion or decreasing aneurysm sac diameter and length. Kinking can lead to migration, throm-bosis, and type I or III endoleak. Excessive aortic neck angulation and a narrow distal aortic diameter predispose to kink formation [86]. The reported incidence varies depending on the degree of kinking but is in the range of 1.7–3.7% [52, 86]. It is possible that new low-profile devices will have higher rates of limb kinking and occlusion because of less radial force and columnar stent strength [87]. Addi-tional high-radial-force uncovered stents may be placed in an attempt to straighten kinks and avoid thrombosis.
Limb occlusion is often related to kinking of the metallic skeleton, extension of the stent-graft into tortuous or diminutive iliac arter-ies, or migration and dislocation of an endo-graft limb [88]. Excessive oversizing, resulting in folding of the graft material, and twisting of the limbs during deployment are two possible causes of thrombosis [58, 89]. The incidence of thrombosis is reported to be 0.5–11% [52]. In cases of diminutive iliac arteries, it may be
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by C
olum
bia
Uni
vers
ity o
n 09
/29/
14 f
rom
IP
addr
ess
128.
59.2
22.1
2. C
opyr
ight
AR
RS.
For
per
sona
l use
onl
y; a
ll ri
ghts
res
erve
d

AJR:203, October 2014 W363
Postprocedure Monitoring of Endovascular Abdominal Aortic Aneurysm Repair
necessary to place an aortouniiliac graft with a surgical bypass to avoid thrombosis. Throm-bectomy and stent placement may be attempt-ed to salvage a thrombosed limb. Otherwise, a femoral-to-femoral artery bypass may be re-quired to revascularize the limb supplied by the thrombosed segment (Fig. 8). In cases with an aneurysmal common iliac artery, snorkel stents or bifurcated iliac side branch devices may be used to preserve flow to the internal iliac artery. Surveillance imaging should carefully evaluate these devices for limb thrombosis, which may result in buttock claudication, especially when both internal iliac arteries are occluded.
InfectionEndograft infection is associated with high
mortality but is relatively uncommon, occur-ring in less than 1% of cases [90, 91]. Proce-dural contamination is the most likely cause of early infection. Although the stent-graft is protected by the intact aneurysm sac, remote sites of infection may lead to late colonization. Infection presents as leukocytosis, fever, and back pain. CT shows mesenteric inflammation adjacent to the stent-graft, perigraft fluid col-lections, abnormal enhancement, or air bubbles (Fig. 9). An aortoenteric fistula is a rare com-plication after EVAR that may lead to massive hemorrhage, endograft infection, and hypovo-lemic shock [92] (Fig. 10). Endoleaks resulting in aneurysm expansion may lead to erosion and aortoenteric fistula formation [93]. Endograft infection and placement in inflammatory aneu-rysms are other commonly proposed causes for fistula formation [94].
Treatment may consist of in situ repair with resection of the infected graft and placement of antibiotic-soaked polyester graft, auto-logous vein graft, or cryopreserved graft. Extraanatomic reconstruction is often per-formed in high-risk cases. Patients will first receive IV antibiotics and then be converted to an oral suppressive antibiotic regimen. The optimal duration of antibiotic therapy is not yet determined but may be lifelong in compli-cated cases [91].
Renal ComplicationsEVAR requires a minimum of 50–100
mL of iodized IV contrast material. The low-est possible dose of 50%/50% diluted isoos-molar contrast material should be used in pa-tients with renal insufficiency. Renal function declines after EVAR, with renal failure esti-mated to occur in 6.7% of cases [95]. A re-cent study suggests that patients who undergo EVAR have a greater continuous decline in re-
nal function over time compared with patients who undergo open aneurysm repair. This is likely due to contrast agent given during the initial procedure, secondary procedures to treat complications, and routine surveillance scans. Alternative unenhanced surveillance protocols should lessen the long-term risk of renal function impairment [96]. End-organ ischemia attributed to clot formation or em-bolic phenomena related to catheter manipula-tion in heavily diseased vessels may also result in ischemia and deteriorating renal function.
Patients should be well hydrated before and after the procedure. Pretreatment with so-dium bicarbonate reduces contrast-induced nephrotoxicity, and acetylcysteine is also fre-quently given despite limited evidence of its efficacy. Intravenous ultrasound can be used to evaluate the anatomy before treatment and assess the endograft after placement [97]. Us-ing intravenous ultrasound can significantly reduce the amount of IV contrast material ad-ministered during stent-graft placement [98].
Renal artery stenting may be performed be-fore EVAR in patients with renal artery steno-sis and marginal renal function. Stents placed in the proximal renal arteries extend a short distance into the aortic lumen and are flared to minimize kinking or fracture by the stent-graft [52]. If renal artery occlusion results from poor aortic endograft placement, attempts may be made to pull the device inferiorly and uncov-er the renal arteries. Patients with complicated proximal neck anatomy may require suprare-nal placement of the endograft and restricted blood flow to the kidneys. Chimney grafts or fenestrated grafts may be placed in these sit-uations [99]. Despite the administration of IV contrast material, EVAR is associated with im-proved short-term postoperative renal function compared with open repair [100].
Bowel IschemiaBowel ischemia is a serious but rare com-
plication after EVAR. Thrombotic deposits and atheroma in the suprarenal aorta may be dislodged during endograft placement and travel to the SMA, IMA, internal iliac arter-ies, and lower extremities. When involving the mesenteric circulation, microemboli may result in multifocal patchy bowel ischemia. Inadequate mesenteric collateral circulation is another proposed cause [52, 101]. Colonic ischemia is a strong independent predictor of postprocedural mortality. The incidence of colonic ischemia in EVAR is predicted to be lower than that of open repair, during which it occurs in 1–6% of cases [92, 102].
Device FailureStructural endograft failure is a rare compli-
cation that was more common with early-gen-eration devices [103]. It results from fatigue, corrosion, suture breakage, or graft fabric tear. Structural failures may occur in up to 5.5% of cases and result in ineffective attachment zone seal, migration, and endoleak [58]. Turbulent flow in the aneurysm sac due to an endoleak can contribute to early device fatigue and eventual failure [6]. It is possible that more device failures will be found as patients and devices age. A recent study found that metal-lic ring failure and suture breakage detected on 3D CTA correlate with the development of migration and type I and type III endoleaks, thus supporting the concept that fatigue deg-radation leads to delayed endoleaks [104]. Structural failures are often late occurrences, and vigilant long-term surveillance should be maintained for these complications [103].
Access Site ComplicationsEVAR is now commonly performed with
a totally percutaneous technique using arte-rial closure devices. Percutaneous EVAR is possible in 76–96% of patients with success rates depending on patient selection [105]. Percutaneous EVAR decreases the rate of wound complications, operative time, and length of hospital stay when compared with traditional open femoral access [105, 106]. Obesity, repeat groin access, larger sheath size, severe femoral artery calcification, ac-cess vessel size less than 5 mm, and lack of operator experience are associated with per-cutaneous EVAR failure and conversion to open femoral access [105, 107, 108]. A study suggests that femoral artery calcification in-volving greater than 50% of the anterior ves-sel wall increases the risk of closure device failure [106]. Ultrasound guidance allows proper puncture in the common femoral ar-tery and enables the operator to avoid areas with large anterior calcifications.
Access site complications occur in up to 3% of percutaneous EVAR procedures [92]. Several potential complications include arte-rial thrombosis, dissection, pseudoaneurysm formation, and local wound complications. The large delivery system and sheath size can result in dissection and avulsion of the access arteries. Arterial dissection may be repaired with stenting if it is discovered during the pro-cedure. Vessel rupture may occur when enter-ing small or heavily calcified vessels and may not become apparent until the vascular sheath is removed at the end of the procedure.
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by C
olum
bia
Uni
vers
ity o
n 09
/29/
14 f
rom
IP
addr
ess
128.
59.2
22.1
2. C
opyr
ight
AR
RS.
For
per
sona
l use
onl
y; a
ll ri
ghts
res
erve
d

W364 AJR:203, October 2014
Picel and Kansal
Angioplasty can be attempted to allow ac-cess through severely stenotic vessels. A sur-gically placed retroperitoneal iliac artery con-duit provides another option for access in patients with small, tortuous, or heavily calci-fied iliofemoral vessels [92]. A 10-mm poly-ester fiber (Dacron, DuPont) graft is com-monly used for the conduit, which is placed to provide large-vessel access. The conduit is often attached to the common iliac artery near the terminal bifurcation [107]. Distal placement is necessary to preserve the land-ing zone for the endograft device. At the end of the procedure, the conduit may be ligated near its origin or closed and left in place for future access.
Abdominal Aortic Aneurysm RuptureDelayed abdominal aortic aneurysm rup-
ture after EVAR is rare, reported to occur in 0.5% of cases per year [59]. Treatment con-sists of endovascular revision or open surgical conversion. Ruptures may occur in patients without evidence of increasing aneurysm size on surveillance. This is likely due to sudden pressurization of the aneurysm sac from a type I or III endoleak [59]. Mortality rates are significantly higher for secondary procedures performed after abdominal aortic aneurysm rupture. Detailed imaging evaluation to deter-mine the cause of the endograft failure assists in surgical planning for either endovascular or open repair [50]. Endovascular therapy to treat the underlying failure will likely involve graft extensions within the proximal or distal landing zones or within the stent-graft com-ponents to adequately seal the rupture.
ConclusionEVAR depends on imaging for prepro-
cedural treatment planning and detection of postprocedural complications. As devices continue to advance, more patients will be-come amenable to endovascular repair. Re-finement in the surveillance CT technique and the development of ultrasound and MRI protocols are important to limit radiation and contrast material exposure. Proper EVAR surveillance requires close collaboration be-tween imagers and interventionalists to en-sure that appropriate and safe screening is performed and for prompt notification when urgent intervention is required. A comprehen-sive understanding of EVAR surveillance and associated complications is necessary for the interpreting physician to create a detailed and clinically useful imaging report and assist in the care of these complex patients.
References 1. d’Audiffret A, Desgranges P, Kobeiter DH, Bec-
quemin JP. Follow-up evaluation of endoluminally
treated abdominal aortic aneurysms with duplex
ultrasonography: validation with computed tomog-
raphy. J Vasc Surg 2001; 33:42–50
2. Kranokpiraksa P, Kaufman JA. Follow-up of endo-
vascular aneurysm repair: plain radiography, ultra-
sound, CT/CT angiography, MR imaging/MR an-
giography, or what? J Vasc Interv Radiol 2008;
19:S27–S36
3. van der Vliet JA, Kool LJ, van Hoek F. Simplifying
post-EVAR surveillance. Eur J Vasc Endovasc
Surg 2011; 42:193–194
4. Lehmkuhl L, Andres C, Lucke C, et al. Dynamic
CT angiography after abdominal aortic endovascu-
lar aneurysm repair: influence of enhancement pat-
terns and optimal bolus timing on endoleak detec-
tion. Radiology 2013; 268:890–899
5. Shah A, Stavropoulos SW. Imaging surveillance
following endovascular aneurysm repair. Semin
Intervent Radiol 2009; 26:10–16
6. Stavropoulos SW, Charagundla SR. Imaging tech-
niques for detection and management of endoleaks
after endovascular aortic aneurysm repair. Radiol-
ogy 2007; 243:641–655
7. Alerci M, Oberson M, Fogliata A, Gallino A, Vock
P, Wyttenbach R. Prospective, intraindividual
comparison of MRI versus MDCT for endoleak
detection after endovascular repair of abdominal
aortic aneurysms. Eur Radiol 2009; 19:1223–1231
8. Cayne NS, Veith FJ, Lipsitz EC, et al. Variability
of maximal aortic aneurysm diameter measure-
ments on CT scan: significance and methods to
minimize. J Vasc Surg 2004; 39:811–815
9. Kauffmann C, Tang A, Therasse E, et al. Measure-
ments and detection of abdominal aortic aneurysm
growth: accuracy and reproducibility of a segmen-
tation software. Eur J Radiol 2012; 81:1688–1694
10. Wever JJ, Blankensteijn JD, Th M Mali WP, Eikel-
boom BC. Maximal aneurysm diameter follow-up
is inadequate after endovascular abdominal aortic
aneurysm repair. Eur J Vasc Endovasc Surg 2000;
20:177–182
11. Bastos Gonçalves F, Baderkhan H, Verhagen HJ,
et al. Early sac shrinkage predicts a low risk of late
complications after endovascular aortic aneurysm
repair. Br J Surg 2014; 101:802–810
12. Back MR. Surveillance after endovascular abdomi-
nal aortic aneurysm repair. Perspect Vasc Surg En-
dovasc Ther 2007; 19:395–400
13. Go MR, Barbato JE, Rhee RY, Makaroun MS. What
is the clinical utility of a 6-month computed tomog-
raphy in the follow-up of endovascular aneurysm
repair patients? J Vasc Surg 2008; 47:1181–1187
14. Kirkpatrick VE, Wilson DE, Williams RA, Gordon
IL. Surveillance computed tomographic arterio-
gram (CTA) does not change management before
three years in patients who have a normal post-
EVAR study. Ann Vasc Surg 2014; 28:831–836
15. Iezzi R, Cotroneo AR, Filippone A, et al. Multide-
tector CT in abdominal aortic aneurysm treated
with endovascular repair: are unenhanced and de-
layed phase enhanced images effective for endole-
ak detection? Radiology 2006; 241:915–921
16. Macari M, Chandarana H, Schmidt B, Lee J, Lam-
parello P, Babb J. Abdominal aortic aneurysm: can
the arterial phase at CT evaluation after endovascu-
lar repair be eliminated to reduce radiation dose?
Radiology 2006; 241:908–914
17. Nambi P, Sengupta R, Krajcer Z, Muthupillai R,
Strickman N, Cheong BY. Non-contrast computed
tomography is comparable to contrast-enhanced
computed tomography for aortic volume analysis
after endovascular abdominal aortic aneurysm re-
pair. Eur J Vasc Endovasc Surg 2011; 41:460–466
18. Bley TA, Chase PJ, Reeder SB, et al. Endovascular
abdominal aortic aneurysm repair: nonenhanced
volumetric CT for follow-up. Radiology 2009;
253:253–262
19. Bobadilla JL, Suwanabol PA, Reeder SB, Pozniak
MA, Bley TA, Tefera G. Clinical implications of
non-contrast-enhanced computed tomography for
follow-up after endovascular abdominal aortic an-
eurysm repair. Ann Vasc Surg 2013; 27:1042–1048
20. Raman SP, Johnson PT, Deshmukh S, Mahesh M,
Grant KL, Fishman EK. CT dose reduction appli-
cations: available tools on the latest generation of
CT scanners. J Am Coll Radiol 2013; 10:37–41
21. Willemink MJ, Leiner T, de Johg PA, et al. Itera-
tive reconstruction techniques for computed to-
mography. Part 2. Initial results in dose reduction
and image quality. Eur Radiol 2013; 23:1632–1642
22. Flors L, Leiva-Salinas C, Norton PT, Patrie JT,
Hagspiel KD. Endoleak detection after endovascu-
lar repair of thoracic aortic aneurysm using dual-
source dual-energy CT: suitable scanning protocols
and potential radiation dose reduction. AJR 2013;
200:451–460
23. Harrison GJ, Oshin OA, Vallabhaneni SR, Bren-
nan JA, Fisher RK, McWilliams RG. Surveillance
after EVAR based on duplex ultrasound and ab-
dominal radiography. Eur J Vasc Endovasc Surg
2011; 42:187–192
24. Dias NV, Riva L, Ivancev K, Resch T, Sonesson B,
Malina M. Is there a benefit of frequent CT follow-
up after EVAR? Eur J Vasc Endovasc Surg 2009;
37:425–430
25. Wolf YG, Johnson BL, Hill BB, Rubin GD, Fog-
arty TJ, Zarins CK. Duplex ultrasound scanning
versus computed tomographic angiography for
postoperative evaluation of endovascular abdomi-
nal aortic aneurysm repair. J Vasc Surg 2000;
32:1142–1148
26. Raman KG, Missig-Carroll N, Richardson T, Mu-
luk SC, Makaroun MS. Color-flow duplex ultra-
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by C
olum
bia
Uni
vers
ity o
n 09
/29/
14 f
rom
IP
addr
ess
128.
59.2
22.1
2. C
opyr
ight
AR
RS.
For
per
sona
l use
onl
y; a
ll ri
ghts
res
erve
d

AJR:203, October 2014 W365
Postprocedure Monitoring of Endovascular Abdominal Aortic Aneurysm Repair
sound scan versus computed tomographic scan in
the surveillance of endovascular aneurysm repair. J
Vasc Surg 2003; 38:645–651
27. Nyheim T, Staxrud LE, Rosen L, Slagsvold CE,
Sandbaek G, Jorgensen JJ. Review of postopera-
tive CT and ultrasound for endovascular aneurysm
repair using Talent stent graft: can we simplify the
surveillance protocol and reduce the number of CT
scans? Acta Radiol 2013; 54:54–58
28. Han SM, Patel K, Rowe VL, Perese S, Bond A,
Weaver FA. Ultrasound-determined diameter mea-
surements are more accurate than axial computed
tomography after endovascular aortic aneurysm
repair. J Vasc Surg 2010; 51:1381–1387
29. Parent FN, Meier GH, Godziachvili V, et al. The inci-
dence and natural history of type I and type II endole-
ak: a 5-year follow-up assessment with color duplex
ultrasound scan. J Vasc Surg 2002; 35:474–481
30. Arko FR, Filis KA, Siedel SA, et al. Intrasac flow
velocities predict sealing of type II endoleaks after
endovascular abdominal aortic aneurysm repair. J
Vasc Surg 2003; 37:8–15
31. Bredahl K, Long A, Taudorf M, et al. Volume esti-
mations of the aortic sac after EVAR using 3-D ul-
trasound: a novel, accurate, and promising tech-
nique. Eur J Vasc Endovasc Surg 2013; 45:450–455
32. Arsicot M, Lathelize H, Martinez R, Marchand E,
Picquet J, Enon B. Follow-up of aortic stentgrafts:
comparison of the volumetric analysis of the aneu-
rysm sac by ultrasound and CT. Ann Vasc Surg
2014 [Epub ahead of print]
33. Mirza TA, Karthikesalingam A, Jackson D, et al.
Duplex ultrasound and contrast-enhanced ultra-
sound versus computed tomography for the detec-
tion of endoleak after EVAR: systematic review
and bivariate meta-analysis. Eur J Vasc Endovasc
Surg 2010; 39:418–428
34. Bakken AM, Illig KA. Long-term follow-up after
endovascular aneurysm repair: is ultrasound alone
enough? Perspect Vasc Surg Endovasc Ther 2010;
22:145–151
35. Ten Bosch JA, Rouwet EV, Peters CT, et al. Con-
trast-enhanced ultrasound versus computed tomo-
graphic angiography for surveillance of endovas-
cular abdominal aortic aneurysm repair. J Vasc
Interv Radiol 2010; 21:638–643
36. Cantisani V, Ricci P, Grazhdani H, et al. Prospec-
tive comparative analysis of colour-Doppler ultra-
sound, contrast-enhanced ultrasound, computed
tomography and magnetic resonance in detecting
endoleak after endovascular abdominal aortic an-
eurysm repair. Eur J Vasc Endovasc Surg 2011;
41:186–192
37. Gürtler VM, Sommer WH, Meimarakis G, et al. A
comparison between contrast-enhanced ultrasound
imaging and multislice computed tomography in
detecting and classifying endoleaks in the follow-
up after endovascular aneurysm repair. J Vasc Surg
2013; 58:340–345
38. Millen A, Canavati R, Harrison G, et al. Defining a
role for contrast-enhanced ultrasound in endovas-
cular aneurysm repair surveillance. J Vasc Surg
2013; 58:18–23
39. Iezzi R, Cotroneo AR, Basilico R, Simeone A,
Storto ML, Bonomo L. Endoleaks after endovascu-
lar repair of abdominal aortic aneurysm: value of
CEUS. Abdom Imaging 2010; 35:106–114
40. Abbas A, Hansrani V, Sedgwick N, Ghosh J, Mc-
Collum CN. 3D contrast enhanced ultrasound for
detecting endoleak following endovascular aneu-
rysm repair (EVAR). Eur J Vasc Endovasc Surg
2014; 47:487–492
41. Beeman BR, Doctor LM, Doerr K, McAfee-Ben-
nett S, Dougherty MJ, Calligaro KD. Duplex ultra-
sound imaging alone is sufficient for midterm en-
dovascular aneurysm repair surveillance: a cost
analysis study and prospective comparison with
computed tomography scan. J Vasc Surg 2009;
50:1019–1024
42. Chaer RA, Gushchin A, Rhee R, et al. Duplex ul-
trasound as the sole long-term surveillance method
post-endovascular aneurysm repair: a safe alterna-
tive for stable aneurysms. J Vasc Surg 2009;
49:845–850
43. Pitton MB, Schweitzer H, Herber S, et al. MRI ver-
sus helical CT for endoleak detection after endo-
vascular aneurysm repair. AJR 2005; 185:1275–
1281
44. van der Laan MJ, Bartels LW, Viergever MA,
Blankensteijn JD. Computed tomography versus
magnetic resonance imaging of endoleaks after
EVAR. Eur J Vasc Endovasc Surg 2006; 32:361–
365
45. Habets J, Zandvoort HJ, Reitsma JB, et al. Mag-
netic resonance imaging is more sensitive than
computed tomography angiography for the detec-
tion of endoleaks after endovascular abdominal
aortic aneurysm repair: a systematic review. Eur J
Endovasc Surg 2013; 45:340–350
46. Resta EC, Secchi F, Giardino A, et al. Non-contrast
MR imaging for detecting endoleak after abdomi-
nal endovascular aortic repair. Int J Cardiovasc
Imaging 2013; 29:229–235
47. Ichihashi S, Marugami N, Tanaka T, et al. Prelimi-
nary experience with superparamagnetic iron oxide-
enhanced dynamic magnetic resonance imaging and
comparison with contrast-enhanced computed to-
mography in endoleak detection after endovascular
aneurysm repair. J Vasc Surg 2013; 58:66–72
48. Ellozy SH, Carroccio A, Lookstein RA, et al. Ab-
dominal aortic aneurysm sac shrinkage after endo-
vascular aneurysm repair: correlation with chronic
sac pressure measurement. J Vasc Surg 2006; 43:2–7
49. Becquemin JP, Kelley L, Zubilewicz T, Desgrang-
es P, Lapeyre M, Kobeiter H. Outcomes of second-
ary interventions after abdominal aortic aneurysm
endovascular repair. J Vasc Surg 2004; 39:298–
305
50. Mehta M, Sternbach Y, Taggert JB, et al. Long-
term outcomes of secondary procedures after endo-
vascular aneurysm repair. J Vasc Surg 2010;
52:1442–1449
51. Elkouri S, Gloviczki P, McKusick MA, et al. Peri-
operative complications and early outcome after
endovascular and open surgical repair of abdominal
aortic aneurysms. J Vasc Surg 2004; 39:497–505
52. Liaw JV, Clark M, Gibbs R, Jenkins M, Cheshire
N, Hamady M. Update: complications and man-
agement of infrarenal EVAR. Eur J Radiol 2009;
71:541–551
53. Stavropoulos SW, Clark TW, Carpenter JP, et al.
Use of CT angiography to classify endoleaks after
endovascular repair of abdominal aortic aneu-
rysms. J Vasc Interv Radiol 2005; 16:663–667
54. Veith FJ, Baum RA, Ohki T, et al. Nature and sig-
nificance of endoleaks and endotension: summary
of opinions expressed at an international confer-
ence. J Vasc Surg 2002; 35:1029–1035
55. Aburahma AF, Campbell JE, Mousa AY, et al.
Clinical outcomes for hostile versus favorable neck
anatomy in endovascular aortic aneurysm repair
using modular devices. J Vasc Surg 2011; 54:13–
21
56. Bastos Gonçalves F, Verhagen HJ, Chinsakchai K,
et al. The influence of neck thrombus on clinical
outcome and aneurysm morphology after endovas-
cular aneurysm repair. J Vasc Surg 2012; 56:36–44
57. Wyss TR, Dick F, Brown LC, Greenhalgh RM. The
influence of thrombus, calcification, angulation,
and tortuosity of attachment sites on the time to the
first graft-related complication after endovascular
aneurysm repair. J Vasc Surg 2011; 54:965–971
58. Hellinger JC. Endovascular repair of thoracic and
abdominal aortic aneurysm: pre- and postprocedural
imaging. Tech Vasc Interv Radiol 2005; 8:2–15
59. Becquemin JP, Allaire E, Desgranges P, Kobeiter
H. Delayed complications following EVAR. Tech
Vasc Interv Radiol 2005; 8:30–40
60. Arko FR 3rd, Murphy EH, Boyes C, et al. Current
status of endovascular aneurysm repair: 20 years of
learning. Semin Vasc Surg 2012; 25:131–135
61. Moulakakis KG, Mylonas SN, Avgerinos E, et al.
The chimney graft technique for preserving vis-
ceral vessels during endovascular treatment of aor-
tic pathologies. J Vasc Surg 2012; 55:1497–1503
62. Güntner O, Zeman F, Wohlgemuth WA, et al. Infe-
rior mesenteric arterial type II endoleaks after endo-
vascular repair of abdominal aortic aneurysm: are
they predictable? Radiology 2014; 270:910–919
63. Ward TJ, Cohen S, Fischman AM, et al. Preopera-
tive inferior mesenteric artery embolization before
endovascular aneurysm repair: decreased incidence
of type II endoleak and aneurysm sac enlargement
with 24-month follow-up. J Vasc Interv Radiol
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by C
olum
bia
Uni
vers
ity o
n 09
/29/
14 f
rom
IP
addr
ess
128.
59.2
22.1
2. C
opyr
ight
AR
RS.
For
per
sona
l use
onl
y; a
ll ri
ghts
res
erve
d

W366 AJR:203, October 2014
Picel and Kansal
2013; 24:49–55
64. Axelrod DJ, Lookstein RA, Guller J, et al. Inferior
mesenteric artery embolization before endovascu-
lar aneurysm repair: technique and initial results. J
Vasc Interv Radiol 2004; 15:1263–1267
65. Alerci M, Giamboni A, Wyttenbach R, et al. Endo-
vascular abdominal aneurysm repair and impact of
systematic preoperative embolization of collateral
arteries: endoleak analysis and long-term follow-
up. J Endovasc Ther 2013; 20:663–671
66. Burbelko M, Kalinowski M, Heverhagen JT,
et al. Prevention of type II endoleak using the AM-
PLATZER vascular plug before endovascular aneu-
rysm repair. Eur J Endovasc Surg 2014; 47:28–36
67. Sheehan MK, Hagino RT, Canby E, et al. Type 2
endoleaks after abdominal aortic aneurysm stent
grafting with systematic mesenteric and lumbar coil
embolization. Ann Vasc Surg 2006; 20:458–463
68. Gould DA, McWilliams R, Edwards RD, et al.
Aortic side branch embolization before endovascu-
lar aneurysm repair: incidence of type II endoleak.
J Vasc Interv Radiol 2001; 12:337–341
69. Fan CM, Rafferty EA, Geller SC, et al. Endovascu-
lar stent-graft in abdominal aortic aneurysms: the
relationship between patent vessels that arise from
the aneurysmal sac and early endoleak. Radiology
2001; 218:176–182
70. Aburahma AF, Mousa AY, Campbell JE, et al. The
relationship of preoperative thrombus load and lo-
cation to the development of type II endoleak and
sac regression. J Vasc Surg 2011; 53:1534–1541
71. Ward TJ, Cohen S, Patel RS, et al. Anatomic risk
factors for type-2 endoleak following EVAR: a ret-
rospective review of preoperative CT angiography
in 326 patients. Cardiovasc Intervent Radiol 2014;
37:324–328
72. Brountzos E, Karagiannis G, Panagiotou I, Tzavara
C, Efstathopoulos E, Kelekis N. Risk factors for the
development of persistent type II endoleaks after
endovascular repair of infrarenal abdominal aortic
aneurysms. Diagn Interv Radiol 2012; 18:307–313
73. Nolz R, Tuefelsbauer H, Asenbaum U, et al. Type
II endoleak after endovascular repair of abdominal
aortic aneurysms: fate of the aneurysm sac and
neck changes during long-term follow-up. J Endo-
vasc Ther 2012; 19:193–199
74. Zhou W, Bley E Jr, Varu V, et al. Outcome and
clinical significance of delayed endoleaks after en-
dovascular aneurysm repair. J Vasc Surg 2014;
59:915–920
75. Sidloff DA, Stather PW, Choke E, Bown MJ, Say-
ers RD. Type II endoleak after endovascular aneu-
rysm repair. Br J Surg 2013; 100:1262–1270
76. Baum RA, Carpenter JP, Golden MA, et al. Treat-
ment of type 2 endoleaks after endovascular repair
of abdominal aortic aneurysms: comparison of
transarterial and translumbar techniques. J Vasc
Surg 2002; 35:23–29
77. Nevala T, Biancari F, Manninen H, et al. Type II
endoleak after endovascular repair of abdominal
aortic aneurysm: effectiveness of embolization.
Cardiovasc Intervent Radiol 2010; 33:278–284
78. Stavropoulos SW, Park J, Fairman R, Carpenter J.
Type 2 endoleak embolization comparison: trans-
lumbar embolization versus modified transarterial
embolization. J Vasc Interv Radiol 2009; 20:1299–
1302
79. Abularrage CJ, Patel VI, Conrad MF, Schneider
EB, Cambria RP, Kwolek CJ. Improved results us-
ing Onyx glue for the treatment of persistent type 2
endoleak after endovascular aneurysm repair. J
Vasc Surg 2012; 56:630–636
80. Müller-Wille R, Wolhlgemuth WA, Heiss P, et al.
Transarterial embolization of type II endoleaks af-
ter EVAR: the role of ethylene vinyl alcohol copo-
lymer (Onyx). Cardiovasc Intervent Radiol 2013;
36:1288–1295
81. Khaja MS, Park AW, Swee W, et al. Treatment of
type II endoleak using Onyx with long-term imag-
ing follow-up. Cardiovasc Intervent Radiol 2014;
37:613–622
82. Stavropoulos SW, Marin H, Fairman RM, et al. Re-
current endoleak detection and measurement of
aneurysm size with CTA after coil embolization of
endoleaks. J Vasc Interv Radiol 2005; 16:1313–
1317
83. Sampaio SM, Panneton JM, Mozes G, et al. An-
euRx device migration: incidence, risk factors, and
consequences. Ann Vasc Surg 2005; 19:178–185
84. Sternbergh WC 3rd, Money SR, Greenberg RK,
Chuter TA; Zenith Investigators. Influence of en-
dograft oversizing on device migration, endoleak,
aneurysm shrinkage, and aortic neck dilation: re-
sults from the Zenith Multicenter Trial. J Vasc Surg
2004; 39:20–26
85. Resch T, Ivancev K, Brunkwall J, Nyman U, Ma-
lina M, Lindblad B. Distal migration of stent-grafts
after endovascular repair of abdominal aortic aneu-
rysms. J Vasc Interv Radiol 1999; 10:257–264
86. Fransen GA, Desgranges P, Leheij RJ, Harris PL,
Becquemin JP; EUROSTAR Collaborators. Fre-
quency, predictive factors, and consequences of
stent-graft kink following endovascular AAA re-
pair. J Endovasc Ther 2003; 10:913–918
87. Early H, Atkins M. Technical tips for managing
difficult iliac access. Semin Vasc Surg 2012;
25:138–143
88. Maleux G, Koolen M, Heye S, Nevelsteen A. Limb
occlusion after endovascular repair of abdominal
aortic aneurysms with supported endografts. J Vasc
Interv Radiol 2008; 19:1409–1412
89. Lalka S, Dalsing M, Cikrit D, et al. Secondary in-
terventions after endovascular abdominal aortic
aneurysm repair. Am J Surg 2005; 190:787–794
90. Cernohorsky P, Reijnen MM, Tielliu IF, van Ster-
kenburg SM, van den Dungen JJ, Zeebreqts CJ.
The relevance of aortic endograft prosthetic infec-
tion. J Vasc Surg 2011; 54:327–333
91. Fatima J, Duncan AA, de Grandis E, et al. Treat-
ment strategies and outcomes in patients with in-
fected aortic endografts. J Vasc Surg 2013;
58:371–379
92. Maleux G, Koolen M, Heye S. Complications after
endovascular aneurysm repair. Semin Intervent Ra-
diol 2009; 26:3–9
93. Ruby BJ, Cogbill TH. Aortoduodenal fistula 5
years after endovascular abdominal aortic aneu-
rysm repair with the Ancure stent graft. J Vasc
Surg 2007; 45:834–836
94. Saratzis N, Saratzis A, Melas N, Ktenidis K, Kiski-
nis D. Aortoduodenal fistulas after endovascular
stent-graft repair of abdominal aortic aneurysms:
single-center experience and review of the litera-
ture. J Endovasc Ther 2008; 15:441–448
95. Wald R, Waikar SS, Liangos O, Pereira BJ, Cher-
tow GM, Jaber BL. Acute renal failure after endo-
vascular vs open repair of abdominal aortic aneu-
rysm. J Vasc Surg 2006; 43:460–466
96. Antonello M, Menegolo M, Piazza M, Bonfante L,
Gergo F, Frigatti P. Outcomes of endovascular an-
eurysm repair on renal function compared with
open repair. J Vasc Surg 2013; 58:886–893
97. Murphy EH, Arko FR. Technical tips for abdomi-
nal aortic endografting. Semin Vasc Surg 2008;
21:25–30
98. Belenky A, Atar E, Orron DE, et al. Endovascular
abdominal aortic aneurysm repair using transve-
nous intravascular US catheter guidance in patients
with chronic renal failure. J Vasc Interv Radiol
2014; 25:702–706
99. Coscas R, Kobeiter H, Desgranges P, Becquemin
JP. Technical aspects, current indications, and re-
sults of chimney grafts for juxtarenal aortic aneu-
rysms. J Vasc Surg 2011; 53:1520–1527
100.Donas KP, Torsello G, Bisdas T, Osada N, Schone-
feld E, Pitoulias GA. Early outcomes for fenes-
trated and chimney endografts in the treatment of
pararenal aortic pathologies are not significantly
different: a systemic review with pooled data anal-
ysis. J Endovasc Ther 2012; 19:723–728
101. Dadian N, Ohki T, Veith FJ, et al. Overt colon
ischemia after endovascular aneurysm repair: the
importance of microembolization as an etiology. J
Vasc Surg 2001; 34:986–996
102. Perry RJ, Martin MJ, Eckert MJ, Sohn VY, Steele
SR. Colonic ischemia complicating open vs endo-
vascular abdominal aortic aneurysm repair. J Vasc
Surg 2008; 48:272–277
103. Rutherford RB. Structural failures in abdominal
aortic aneurysm stentgrafts: threat to durability
and challenge to technology. Semin Vasc Surg
2004; 17:294–297
104. Ueda T, Takaoka H, Petrovitch I, Rubin GD. De-
tection of broken sutures and metal-ring fractures
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by C
olum
bia
Uni
vers
ity o
n 09
/29/
14 f
rom
IP
addr
ess
128.
59.2
22.1
2. C
opyr
ight
AR
RS.
For
per
sona
l use
onl
y; a
ll ri
ghts
res
erve
d

AJR:203, October 2014 W367
Postprocedure Monitoring of Endovascular Abdominal Aortic Aneurysm Repair
in AneuRx stent-grafts by using three-dimensional
CT angiography after endovascular abdominal
aortic aneurysm repair: association with late en-
doleak development and device migration. Radiol-
ogy 2014 [Epub ahead of print]
105. Bensley RP, Hurks R, Huang Z, et al. Ultrasound-
guided percutaneous endovascular aneurysm re-
pair success is predicted by access vessel diameter.
J Vasc Surg 2012; 55:1554–1561
106. Manunga JM, Gloviczki P, Oderich GS, et al.
Femoral artery calcification as a determinant of
success for percutaneous access for endovascular
abdominal aortic aneurysm repair. J Vasc Surg
2013; 58:1208–1212
107. Minion DJ, Davenport DL. Access techniques for
EVAR: percutaneous techniques and working with
small arteries. Semin Vasc Surg 2012; 25:208–216
108. Mousa AY, Campbell JE, Broce M, et al. Predictors
of percutaneous access failure requiring open femo-
ral surgical conversion during endovascular aortic
aneurysm repair. J Vasc Surg 2013; 58:1213–1219
A CB
D
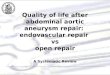
Fig. 1—68-year-old man who underwent endovascular abdominal aortic aneurysm repair (EVAR) and experienced device migration and structural failure. A, CT maximum-intensity-projection (MIP) image obtained 1 month after EVAR shows stent-graft positioned just below most inferior renal artery (arrow).B, Abdominal radiograph obtained 2 years later suggests increased angulation of proximal portion of stent-graft as well as stent fracture (arrow).C and D, Interval surveillance scout radiograph (C) and CT MIP image (D) show increased angulation of stent-graft as well as migration. Stent-graft is now 2.5 cm inferior to left renal artery (arrow, D).E, Postoperative radiograph was obtained after failed endovascular repair. Proximal portion of stent-graft was resected and aorta repaired with polyester fiber (Dacron, DuPont) graft.
E
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by C
olum
bia
Uni
vers
ity o
n 09
/29/
14 f
rom
IP
addr
ess
128.
59.2
22.1
2. C
opyr
ight
AR
RS.
For
per
sona
l use
onl
y; a
ll ri
ghts
res
erve
d

W368 AJR:203, October 2014
Picel and Kansal
AFig. 2—71-year-old man who underwent ultrasound surveillance after endovascular abdominal aortic aneurysm repair. A, Sagittal gray-scale ultrasound image identifies stent-graft (arrow) and accurately measures maximal aortic diameter.B, Sagittal color ultrasound image shows blood flow entering proximal neck of stent-graft (arrow) without evidence of endoleak.
B
A
Fig. 3—77-year-old woman with type I endoleak. A, Axial CT image shows contrast material outside stent-graft but within aneurysm sac (arrow) indicating endoleak near proximal landing zone.B, Sagittal reformatted CT image shows contrast material within region of proximal attachment site (arrow) consistent with type Ia endoleak.
B
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by C
olum
bia
Uni
vers
ity o
n 09
/29/
14 f
rom
IP
addr
ess
128.
59.2
22.1
2. C
opyr
ight
AR
RS.
For
per
sona
l use
onl
y; a
ll ri
ghts
res
erve
d

AJR:203, October 2014 W369
Postprocedure Monitoring of Endovascular Abdominal Aortic Aneurysm Repair
A
Fig. 4—75-year-old man with chimney grafts placed to preserve flow to renal arteries. A, Unenhanced axial CT image shows bilateral chimney stents (arrows) running parallel to aortic stent-graft.B, Coronal maximum-intensity-projection CT image shows renal chimney stents (arrows) extending proximal to covered portion of aortic stent-graft to preserve flow to renal arteries.
B
A
Fig. 5—81-year-old man with type II endoleak. A and B, Axial (A) and oblique sagittal reformatted (B) CT images show contrast material within aneurysm sac adjacent to patent inferior mesenteric artery (arrow) consistent with type II endoleak. In type II endoleak, contrast material will often appear in periphery of aneurysm sac.
B
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by C
olum
bia
Uni
vers
ity o
n 09
/29/
14 f
rom
IP
addr
ess
128.
59.2
22.1
2. C
opyr
ight
AR
RS.
For
per
sona
l use
onl
y; a
ll ri
ghts
res
erve
d

W370 AJR:203, October 2014
Picel and Kansal
AFig. 6—86-year-old man with type II endoleak. A, Axial CT image shows contrast material within periphery of aneurysm sac (arrow). Contrast material was also seen anteriorly in aneurysm sac adjacent to inferior mesenteric artery (IMA). This patient has type II endoleaks supplied by both IMA and lumbar arteries.B, Fluoroscopic image obtained during transarterial therapy. Microcatheter was navigated from superior mesenteric artery through collateral vessels and into IMA. Coils were placed (arrow) to occlude IMA and treat type II endoleak. Coil embolization was also performed of contributing lumbar artery.C, Endoleak persisted and translumbar therapy was performed. Axial CT image shows percutaneous placement of needle (arrow) to directly access aneurysm sac.D, Contrast material injection through percutaneous access shows type II endoleak supplied by left L4 lumbar artery (arrow). Embolization was performed with metallic coils and ethylene vinyl alcohol copolymer (Onyx, ev3).E, Posttreatment sagittal CT image shows metallic artifact (arrow) and high-density material within aneurysm sac from coils placed during endoleak treatment.
CB
D E
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by C
olum
bia
Uni
vers
ity o
n 09
/29/
14 f
rom
IP
addr
ess
128.
59.2
22.1
2. C
opyr
ight
AR
RS.
For
per
sona
l use
onl
y; a
ll ri
ghts
res
erve
d

AJR:203, October 2014 W371
Postprocedure Monitoring of Endovascular Abdominal Aortic Aneurysm Repair
AFig. 7—78-year-old man with stent-graft migration and type III endoleak. A, Axial CT image shows separation of proximal portion of stent-graft resulting in large type III endoleak with immediate risk of rupture.B, Coronal CT reconstructed maximum-intensity-projection image shows disassociation of endograft main body from proximal cuff (arrow).C, Repair was accomplished by placement of additional stent-graft component (arrow) to seal large type III endoleak.
CB
AFig. 8—88-year-old woman with limb occlusion. A and B, Axial (A) and oblique sagittal reformatted (B) CT images show occlusion of left iliac limb (arrow) extending proximally to bifurcation of endograft.C, Three-dimensional reconstructed CT image shows femoral-to-femoral artery bypass (arrow) placed to salvage endovascular repair and perfuse left lower extremity. Left external iliac artery fills in retrograde fashion from surgical bypass.
CB
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by C
olum
bia
Uni
vers
ity o
n 09
/29/
14 f
rom
IP
addr
ess
128.
59.2
22.1
2. C
opyr
ight
AR
RS.
For
per
sona
l use
onl
y; a
ll ri
ghts
res
erve
d

W372 AJR:203, October 2014
Picel and Kansal
A
Fig. 9—62-year-old man with endograft infection. A, Axial CT image shows inflammatory reaction (arrow) near proximal attachment of infected stent-graft.B, Axial CT image at level of stent-graft limbs shows perigraft inflammation and gas (arrow) consistent with infection. Bacteremia persisted after several weeks of IV antibiotic therapy. Infected endograft was removed, and aortobiiliac bypass graft was placed.
B
A
Fig. 10—77-year-old man with aortoenteric fistula.A and B, Axial (A) and sagittal (B) unenhanced CT images show air and oral contrast material (arrow) adjacent to endograft within aneurysm sac, consistent with aortoenteric fistula due to erosion of endograft into duodenum.
B
F O R Y O U R I N F O R M A T I O N
The reader is directed to a related article, titled “Essentials of Endovascular Abdominal Aortic Aneurysm Repair Imaging: Preprocedural Assessment,” which begins on page W347.
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by C
olum
bia
Uni
vers
ity o
n 09
/29/
14 f
rom
IP
addr
ess
128.
59.2
22.1
2. C
opyr
ight
AR
RS.
For
per
sona
l use
onl
y; a
ll ri
ghts
res
erve
d