Embed Size (px)
Citation preview

Aortic Aneurysm ScreeningWilly Pillay
Endovascular Surgeon

Doncaster Vascular Centre
Background
• AAA in 7.5% of Males > 65yr• 2% of all deaths in males > 65• 6800 AAA-related deaths/yr (Eng&Wales)• 7% risk of family member having AAA• 12% risk if index is female• 3.1% have peripheral aneurysms• 70% of peripheral aneurysms have AAA

Background on AAA
• Treatment when reaches 5.5cm size• Prevent rupture• Elective open surgery mortality – 7.5% in UK (Vascunet Data 2008)– AAA QIP to reduce mortality to 2.5%– 2012: 2.4% (DVC: 3.9%, Now 2.6%)
• Emergency open surgery mortality 40-50%• Elective EVAR mortality 2%• Emergency EVAR mortality ??? (IMPROVE trial)

Doncaster Vascular Centre
UK Small Aneurysm Trial
• 1998, Lancet• 1090 patients (age 60 – 76)• Asymptomatic AAA 4.0 – 5.5cm• Early surgery vs. ultrasound surveillance• Surgery if >5.5, increase> 1cm/yr, symptoms• US 6/12 (4.0-4.9), 3/12 (5.0-5.5)• Follow-up 4.6 year (mean)

Doncaster Vascular Centre
UK Small Aneurysm Trial
• Operative mortality was 5.8%• Hazard ratio 0.94 for early surgery (all-cause
mortality)• Mean survival 6.5 and 6.7 years• No increase mortality with delayed surgery• ¾ of surveillance group underwent surgery• ‘early surgery gives no significant survival advantage over
surveillance’ (…delayed surgery)

Doncaster Vascular Centre
UK Small Aneurysm Trial
• 2002, NEJM• Follow-up 8 yrs• 7.2% survival advantage in early surgery• Smoking cessation

Screening• Pro-active: Invite a target population• Opportunistic: e.g. HIV test at Antenatal Clinic• The condition
– An important health problem– Well understood epidemiology, disease progression, Latent period, risk factors– Implemented cost-effective primary prevention strategy
• The Test– Simple, safe, precise, and validated– Repeatable, reliable– Suitable cut-off levels defined and agreed– A further diagnostic test for positive results
• The Treatment– Effective, acceptable and available treatment for early detected disease– Early treatments lead to better outcomes– Clinical management should be optimised
• The Screening Programme– RCT shows that screening reduces mortality & morbidity– Clinically, ethically and socially acceptable to all– Benefit should outweigh physical or psychological harm

Doncaster Vascular Centre
MASSMulticentre Aortic Aneurysm Screening Study
• 2002, Lancet• 67800 males (65-74yr)• Invited for US screening or control• 3.0-4.4 annual/ 4.4-5.4 3mthly• Surgery >=5.5, symptoms, increase .1cm/yr• 4.9% incidence AAA (12% >=5.5cm)• Mortality elective 6%, emergency 37%• Follow-up 4.1 yrs (mean)

Doncaster Vascular Centre
MASS
• No difference in all-cause mortality (<3% of deaths)
• 42% RRR of mortality due to AAA (hazard ratio 0.58) (0.33 to 0.19)
• NNT = 710 screenings• 41% RRR of rupture of AAA (hazard ratio 0.59)
(0.41to 0.24)• £28 400/ life year gained

Doncaster Vascular Centre
MASS
• 2007, Annals Int Med• Follow-up 7 yrs (mean)• £12 000/life year gained• Hazard ratio 0.53
• 2012, BMJ• US<3.0cm rupture risk low• But AAA rupture in those with initial size 2.5-2.9cm
• ?women• ?2nd scan at 75yr if US<3.0cm

Doncaster Vascular Centre
Mass (2)

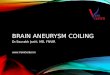
Final follow up of the Multicentre Aneurysm Screening Study (MASS) randomized trial of abdominal ‐aortic aneurysm screening
British Journal of SurgeryVolume 99, Issue 12, pages 1649-1656, 3 OCT 2012 DOI: 10.1002/bjs.8897http://onlinelibrary.wiley.com/doi/10.1002/bjs.8897/full#fig1

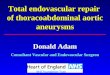
Final follow up of the Multicentre Aneurysm Screening Study (MASS) randomized trial of abdominal ‐aortic aneurysm screening
British Journal of SurgeryVolume 99, Issue 12, pages 1649-1656, 3 OCT 2012 DOI: 10.1002/bjs.8897http://onlinelibrary.wiley.com/doi/10.1002/bjs.8897/full#fig2

Screening
• Men on 65th birthday• Midline ultrasound AP measurement• >3.0cm Surveillance• >5.5cm Referred for treatment

Doncaster Vascular Centre
Workload impact
• Men age 65 = +/- 0.4% of population• Screening men > 65 yr– 4% have slight enlargement– 1% AAA > 4.0– 0.5 % > 5.5cm (i.e. 8 newly detected men with AAA/ 400
000, but screening planned only for men=65!)• Over 20 years (400 000 pop)– Elective ops increase from 61% to 94% of all AAA surgery– Increase 2.1 elective ops/month– Decrease 0.5 emergency ops/month– Increase 1.6 ops/month (after 20 yrs)

Doncaster Vascular Centre
A note on screening
• Screening is not fool-proof• Not every detected case will have a successful outcome• Minimum number of false +• Minimum number of false –• Quality assurance (Reproducibility)• Screening = risk reduction NOT diagnosis & cure• Possible harm:
– High M&M of subsequent treatment– Over detection of disease– Psychological effects– Genetic issues

Doncaster Vascular Centre
Men > 65Yr
• Self-referral will be incorporated into screening program
• Aorta <3.0cm = 0.54 rupture/ 10 000 person years

Doncaster Vascular Centre
Relatives < 65 yr
• Index case– Known AAA– Rupture– Screened case
• Referred to Vascular Surgeon for US/ counselling (outside of screening)

Doncaster Vascular Centre
Women
• 1.3% of women vs 7.6% men• Cochrane review AAA screening (2007)– No significant decrease in AAA-related mortality
(OR 2 vs 0.5 for men)– No significant decrease in in rupture (OR 1.5 vs 0.5
for men)– Surgery equally likely if screened or not
• Possibly screen those with family history?

To date
• NHSAAASP: guidance to measure aorta– AP and Longitudinal in Midline– Inner wall to inner wall
• Prevalence in NHSAAASP is 1.5% (2012)– Statins, Smoking
• Elective mortality has decreased to 2.4%