Embed Size (px)
Citation preview
Epstein-Barr Virus: Cancer and Immunosuppression
Jeffrey I. Cohen
Head, Medical Virology Section
Laboratory of Clinical Infectious Diseases
NIH
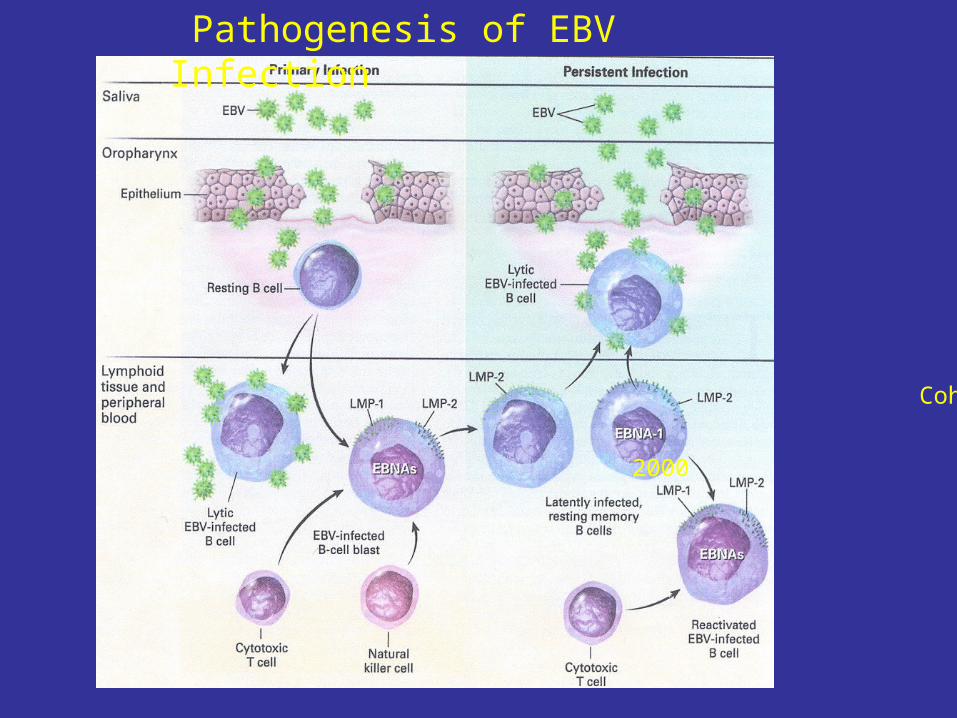
Pathogenesis of EBV Infection
Cohen
NEJM 2000

Early IM: NK cells
non-HLA specific CTLs
Late IM: HLA-restricted CTLs (CD8 and CD4):
Lytic epitopes - up to 40% of CD8 cells
Latent epitopes - up to 2% of CD8 cells
Healthy EBV seropositive persons:
Latent epitopes- 4% of CD8 cells
Lytic epitopes- 0.1 to 5% of CD8 cells
Cellular Immune Responses Are Critical For Control of EBV

EBV Transforms B Cells In Vitro and the Cells Express Limited Viral and Cellular Proteins
Rickinson and Kieff, Fields Virology
EBV LCLs EBV Latency Proteins Cell Genes Induced

EBV Latency Proteins
Cohen NEJM 2000

Oncogene Expression in transgenic mice leads to B cell lymphoma; expression in fibroblasts leads to tumors in nude mice
B Cell Proliferation Upregulates adhesion molecules, CD23, CD40, IL-6, IL-10, etc. Activates NF-B
Inhibits apoptosis
Upregulates Bcl-2, A20, Mcl-1
LMP-1 is the EBV Oncogene
LMP-1
H & E
(Kulwichit et al PNAS 1998)
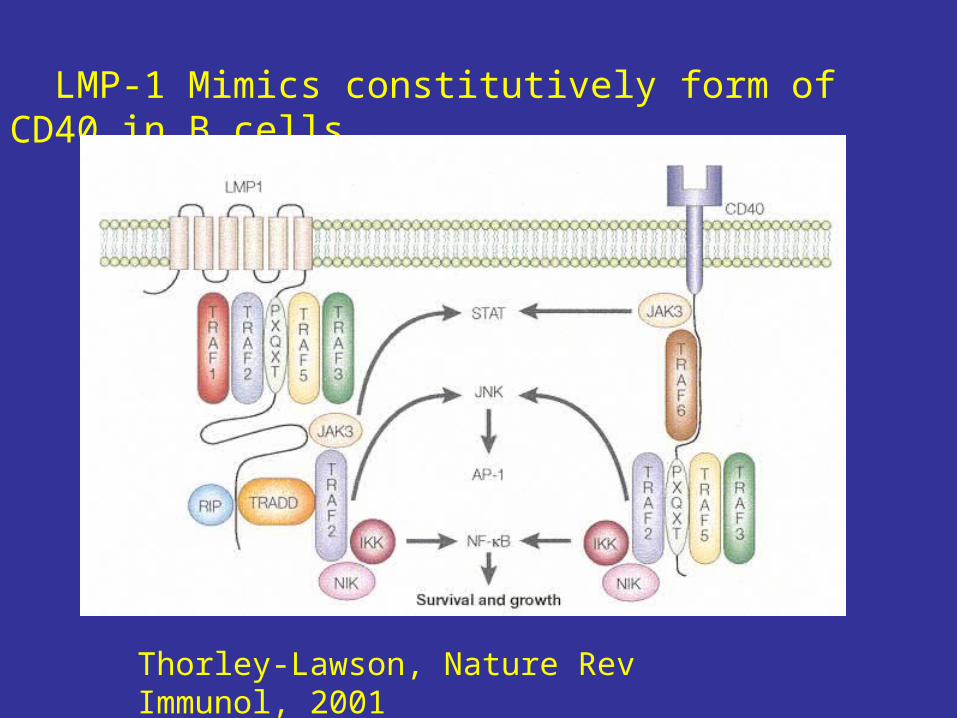
LMP-1 Mimics constitutively form of CD40 in B cells
Thorley-Lawson, Nature Rev Immunol, 2001

Liebowitz NEJM 1998
Activation of NF-B in Tumor from Patient with Post-Transplant EBV Lymphoproliferative Disease
Lane 1: EBV- B cell
Lane 2: EBV+ B cell
Lane 3: EBV- LPD
Lane 4: EBV+ LPD

EBV in B CellInfectious mononucleosisX-Linked Lymphoproliferative DiseaseChronic active EBVHodgkin Disease Burkitt LymphomaLymphoproliferative disease
EBV in Other Cells
Nasopharyngeal carcinomaGastric carcinomaNasal T/NK cell lymphomasPeripheral T cell lymphomasOral hairy leukoplakiaSmooth muscle tumors in transplant patients
Diseases Associated with EBV

Diseases Driven by Epstein-Barr Virus
Infectious mononucleosis
Chronic Active EBV
X-linked lymphoproliferative disease
Lymphoproliferative disease
Oral hairy leukoplakia
Hodgkin disease EBV EBV-Driven
Nasopharyngeal carcinoma Gene Cell
T cell lymphoma Expression Proliferation
Burkitt lymphoma
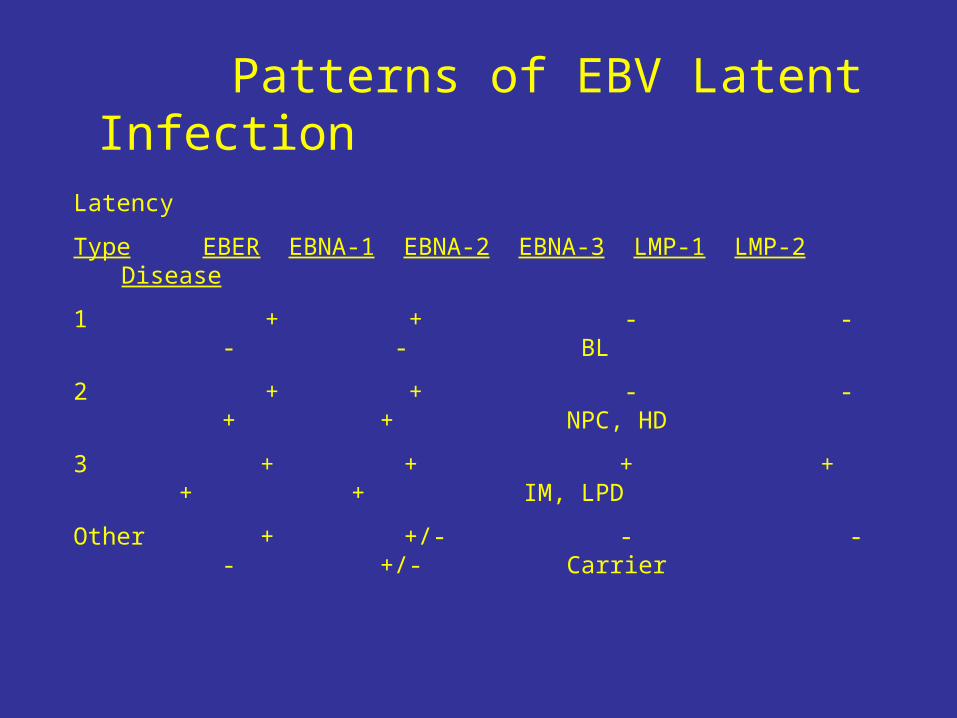
Latency
Type EBER EBNA-1 EBNA-2 EBNA-3 LMP-1 LMP-2 Disease
1 + + - - - - BL
2 + + - - + + NPC, HD
3 + + + + + + IM, LPD
Other + +/- - - - +/- Carrier
Patterns of EBV Latent Infection

EBV+: 90% of cases in developing countries – jaw tumors
20% cases in US – children with abdominal tumors
AIDS patients – tumors in lymph nodes
EBV may be one “hit” but all tumors have c-myc translocations
Dysregulation of c-myc oncogene
Only EBV EBNA-1 expressed
Therapy: Chemotherapy
Burkitt Lymphoma
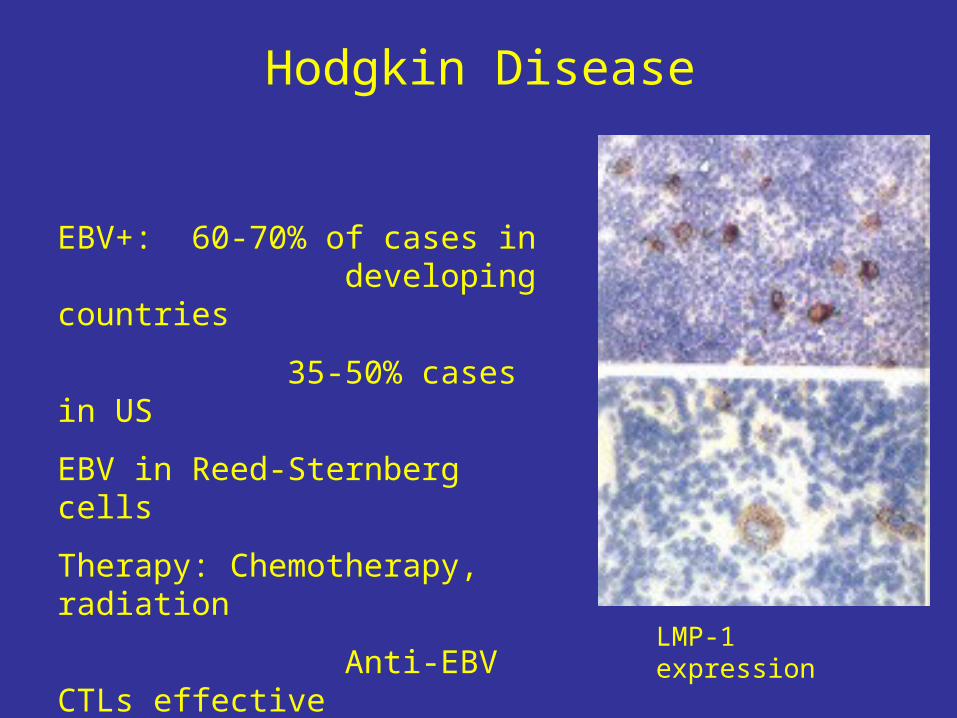
EBV+: 60-70% of cases in developing countries
35-50% cases in US
EBV in Reed-Sternberg cells
Therapy: Chemotherapy, radiation
Anti-EBV CTLs effective in some cases
Hodgkin Disease
LMP-1 expression

EBV-Associated Smooth Muscle Tumors
Occur in transplant recipients, AIDS patients, congenitial immunodeficiency
Pathology: leiomyosarcomas and leiomyomas in various organs (especially transplant) and lymph nodes
Some tumors regress with reduced immunosuppression

EBV Lymphoproliferative Disease
Occurs with immunodeficiency (AIDS, congenital) or after
transplantation, RA and MTX
Symptoms: Infectious Mononucleosis
Mass lesions in organs (less often lymph nodes)
Risk Factors: Primary infection GVHD with increased immune suppression T cell depleted bone marrow
CMV
Cohen NEJM 2000

Risk for EBV PTLD
• Primary infection- higher viral loads, no memory T cells to EBV
• CMV infection• Polymorphisms corresponding to low
production of IFN-, TNF-; high levels of IL-10
• Level of intensity of T cell immunosuppression

EBV Viral Load is Increased in Patients
with Lymphoproliferative Disease
Riddler, Blood 1994
Viral Load Used to Monitor Transplant Patients:Increased EBV load at onset of LPD
Used to initiate preemptive therapy

Treatment of EBV Lymphoproliferative Disease
• Reduce immunosuppression- Early, polymorphic lesions often responsive Later monomorphic lesions can have chromosomal changes
• Excise localized lesions• Radiation therapy (for CNS lesions) or chemotherapy• Anti-CD20 monoclonal antibody (rituximab)• Interferon-• For stem cell transplant recipients: donor lymphocyte
infusions or donor EBV-specific cytotoxic T cell infusions• For solid organ transplant recipients: autologous or HLA-
matched, EBV-specific, cytotoxic T cell infusions
Cutaneous Lymphomas Associated with EBV-infected T cells
Non-immunosuppressed Patients More often in Asians
• Hydroa vacciniforme: vesciulopapular lesions on face and hands, fever, can progress to T cell lymphoma
• Angiocentric NK/T cell lymphomas:ulcers, vesicles, nodules, papules on nose, checks, lips, extremities, trunk
• EBV subcutaneous T cell lymphoma: plaques, fever, hepatosplenomegaly, pancytopenia, panniculitis, hemophagocytosis
Cutaneous Lymphomas Associated with EBV-infected B cells
Immunosuppressed Patients
• Cutaneous ulcerated nodules- B cell lymphomas after transplant or in patients with AIDS
• Cutaneous B cell lymphomas in patients with rheumatoid arthritis or polymyositis receiving methotrexate- resolution in some after drug stopped

EBV LPD More Common at Sites with Chronic Inflammation
• Disease more frequent in transplanted organ Higher frequency of EBV+ cells
Antigenic stimulation with B cell proliferation Cytokine activation in organ
• Reports of EBV+ pyothorax-associated pleural lymphomas at site of pleural inflammation after tuberculosis (Arch Pathol Lab Med. 1996)
• Report of 3 cases of EBV+ large B cell lymphomas in patients with chronic inflammation (osteomyelitis- tumor at site of bone, chronic venous ulcers- tumor at site of ulcer) (J Pathol. 1997 )
Immunosuppressive Agents Associated with EBV LPD
• Steroids and Azathioprine• Methotrexate: Patients with RA, Polymyositits• Antibodies: ATG:
anti-thymocyte globulin ALG: anti-lymphocyte globulin OKT3: anti-CD3
• Calcineurin inhibitors: cyclosporine, tacrolimus• Sirolimus

Methotrexate, but not other Immunosuppressants, Induces EBV Lytic Replication
BMRF1
CY
(10
0 g
/ml)
Pre
dn
ison
e (1
0 m
)
_
AZ
A (
1 g
/ml)
CsA
(1
g/m
l)
CY
(10
g/
ml)
MP
A (
10
g/m
l)
Pre
dn
ison
e (1
m
)
MT
X (
5 g
/ml)
AZ
A (
10
g/m
l)
CsA
(10
g/
ml)
MP
A (
100
g/m
l)
MT
X (
50
g/m
l)
DRUG:
-actin
Feng et al JNCI 2004
Calcineurin Inhibitors and PTLD: Cyclosporine, Tacrolimus
• Inhibit generation of cytotoxic activity• Induce expression of IL-6 and TGF- that supports B
cell activation and proliferation• Enhance survival of EBV-transformed cells in vitro by
protecting from Fas-mediated apoptosis• Lower doses of cyclosporine allow T cell responses
to EBV in vitro and are associated with lower rates of lymphoma than higher doses
• In children tacrolimus is associated with a higher risk of LPD than cyclosporine in some, but not all studies.

Risk of PTLD in Pediatric Liver Transplant Recipients for Primary Tacrolimus Therapy
Cacciarelli et at Pediatric Transplantation 2001

Kaposi’s Sarcoma at the Site of Topical Tacrolimus
Cho et al. J. Am Acad Dermatol. 50:149-50, 2004
28 yo AIDS patient on HAART (CD 143) with psoriasis and seborrheic dermatitis treated with topical tacrolimus 0.1% ointment to axilla, groin, head for 1 month
Developed KS at these sites and in lungs while on tacrolimus

Lymphoma at Site of ATG or ALG Injections
Age Transplant AT/LG Sites of Lymphoma Ref
32 kidney horse buttock, nodes 1
33 kidney horse buttock, nodes, liver 2
32 heart rabbit thigh, brain, lung, nodes 3
18 heart rabbit thigh, chest wall, 3
abdominal nodes1. Deodhar et al N Engl J Med 280:1104-6, 19692. Cotton et al. Transplantation 16:154-7, 1973;
follow-up Herrera et al. Mil Med. 146:652-4, 1981 3. Weintraub and Warnke Transplantation 33:347, 1982

Lymphoma at Site of ALG(Cotton et al 1973; Herrera et al 1981)
47 y.o. renal transplant recipient thoracic duct canulation before and 3 wks after transplant
to deplete lymphocytes; prednisone, azothioprine Horse ALG i.m. in buttocks post transplant on x 14 d,
3 x/wk x 1 yr6 months after last ALG nodule at site >reticulum cell
sarcoma (no EBV studies), immunosuppression reduced, radiation to site;
One year later draining lymph nodes had histiocytic lymphoma, radiation (no EBV studies)
2 years later died of bacteremia-lymphoma in liver
Lymphoma at Site of ALG(Deodhar et al 1969)
32 y.o. renal transplant recipient on azathioprine and prednisone
Rejection 7 months after transplant: treated with actinomycin C and graft irradiation
Horse ALG i.m. in buttocks: 6 weeks later nodule at site, enlarge over 10 months; excised-reticulum cell sarcoma with lymph node involvement (no EBV studies); died of OI

Lymphoma at Site of ALG(Weintraub and Warnke 1982)
7 patients with NHL/182 heart transplants, 2 developed lymphoma at site of ATG
• 32 yo cardiac transplant recipient underwent two allogeneic heart transplantsDeveloped high grade immunoblastic lymphoma in thigh at site of rabbit ATG, later in brain and lung
• 18 yo cardiac transplant recipient underwent two allogeneic heart transplantsDeveloped large noncleaved cell lymphoma in thigh at site of rabbit ATG, later chest wall and abdomen
Summary: EBV LPD in Persons Receiving Immunosuppressants
• Most early, polymorphic lesions are EBV driven, and may respond to reduction in immunosuppression
• Later monomorphic lesions may have chromosomal changes and often require chemotherapy
• More common with primary EBV infection• May have genetic component (cytokine polymorphisms)• More common at site of chronic inflammation• Some occur at sites of local immunosuppression:
ATG or ALG injection sites – all patients on other immunosuppression