Embed Size (px)
Citation preview

Epidermolysis bullosa Heddie 0. Sedano, DDS, Dr. O.,* and Robert J. Go&n, DDS, MS,** Minneapolis, Minn.
UNIVERSITY OF MINNESOTA SCHOOL OF DENTISTRY
During the last 10 years, there has been considerable progress in the knowledge of epidermolysis bullosa,
which has led to recognition of at least 18 different varieties. This review article attempts to classify these
varieties and to emphasize the orodental findings in patients with epidermolysis bullosa.
(ORAL SURC ORAL MED ORAL PATHOL 1989;67:555-63)
E pidermolysis bullosa (EB) includes several hered- itary and nonhereditary vesicular disorders that affect the skin and, frequently, oral and other muco- sal sites. Vesicles may develop at sites of trauma. Heat may precipitate blisters in some varieties of EB.
The term epidermolysis bullosa is actually incor- rect because cytolysis of the epidermis is observed in only 3 or 4 of the subtypes. Nevertheless, it is preserved because of its many years of common usage.
Present classifications of EB are based primarily on the anatomic level at which the splitting that forms the vesicle occurs. Moreover, clinical findings (e.g., scarring) and inheritance are considered.’
The basic classification is as follows (also see Table I): l Type I. Intraepidermal forms, characterized as
nonscarring varieties having autosomal dominant and X-linked inheritance.
l Type ZZ. Junctional forms, most being character- ized by skin atrophy; having autosomal recessive inheritance.
l Type ZZZ. Dermal forms, characterized by atro- phy and scarring, with autosomal dom- inant and recessive varieties.
l Type IV. Acquired (nonhereditary) variety, known as EB acquisita.
Here only those types with oral mucosal and/or dental manifestations will be described. Details on other types of EB can be found in the works of Bergenholtz and 01sson2 Haber and coworkers,3 Gedde-Dahl and Lamprecht,4 and Gedde-Dahl.S
*Professor. **Regents’ Professor and Chairman, Department of Oral Pathol-
ogy and Genetics.
EPIDERMOLYSIS BULLOSA SIMPLEX (Koebner
type)
Systemic features. The most frequently involved
areas are sites of friction or trauma. Altered nails are observed in about 20% of the cases. There is no scarring and/or pigmentation after healing. The disorder principally involves the feet, the hands, and the neck, and rarely the ankles, the knees, the trunk, and the elbows. It generally manifests neonatally or during infancy when the child begins to crawl. Heat seems to be an important precipitating factor in blister production.6 After the third year of life, generally only hands and feet are affected, but the nails become normal. The condition improves at puberty. This type of EB must be differentiated from the Weber-Cockayne type, in which only the feet are affected. This latter form of EB more commonly (70% versus 40%) appears before 1 year of age, and does not manifest oral lesions.
Oral features. Occasional intraoral blisters less severe than those in other types of EB are seen at any site. Teeth are not affected.5*7*8
Histologic and laboratory findings. Histologic study reveals splitting through the basal layer above the PAS-positive basement membrane. Adjacent to areas of cleavage, the basal cells are vacuolated, with nuclei displaced to the epidermal end of the cell. Ultrastructural studies have confirmed these find- ings9,‘0 (Fig. 1). No histochemical abnormality has been observed.”
EPIDERMOLYSIS BULLOSA ATROPHICANS GENERALISATA GRAVIS (Herlitr type)
Systemic features. This autosomal recessive type of EB was described by Herlitz as EB letalis. Since several infants with this form have survived into adulthood, the term letalis should be discarded. It
555

556 Sedan0 and Gorlin ORAL SLIKG ORAI. MED ORAL I~,mtot~
!k4ay 1989
Fig. 1. EB simplex (Koebner type). The bulla (B) is formed through basal keratinocytes (K). Note the presence of an intact basement membrane zone with normal hemidesmosomes (HD) and anchoring fibrils (AFJ. (Original magnification, X8,600.) (From Haber RM, Hanna W, Ramsay CA, Boxall LBH. J Am Acad Dermatol 1985;13:252-78.)
can also be assumed that several cases have been misdiagnosed.‘*
Within the first few hours of life, hemorrhagic vesicles are seen at the base of the fingernails. The nails become loose and are shed.13 Involvement of the trunk, the umbilicus, the face, the scalp, and the extremities follows. The palms and soles are never affected. There seems to be an absence of reaction to trauma. Some affected infants die within the first few months of life, generally from secondary sepsis. The patients who survive never have resultant syn- dactyly, and their hands and feet are affected to a minor degree.3 Anemia, growth retardation, and nail dystrophy are often present.3,4 Large excoriated areas result with age.
Oral features. Extremely fragile and hemorrhagic bullae are found in almost all patients, especially at the junction of the hard and soft palates.14 Oral ulcerations, as well as blistering, can be seen at birth or shortly thereafter.ls Hypoplastic and pitted enam- el leading to extensive caries principally affects the molar teeth.16 Perioral and perinasal crusted and granular hemorrhagic lesions tend to develop between the sixth and twelfth month of life.3,4’17 These lesions are believed to be pathognomonic for the Herlitz type of EB in older patients.’
Histologic and laboratory jindings. Histologic examination of the skin shows epidermal-dermal splitting following the rete ridge contour. Inflamma- tion is not present in the early stages.‘8v19 The stratum germinativum of intact skin also may have
vesicles at the dermoepidermal junction.2*” Similar findings are observed in the oral mucosa. The cells of the basal layer are palisaded as a result of extracel- lular vacuolization. Electron microscopic observation demonstrates separation between the plasma mem- brane of the basal cell and the basement membrane.9 The basic defect is hypoplasia of hemidesmosomes and lack of the sub-basal dense plate1s*20 (Fig. 2).
The ultrastructural studies of Arwill and cowork- ers14 in skin and oral mucosa from patients with the Herlitz form demonstrated fewer hemidesmosomes and tonofilaments than in normal infants. Early changes were edema of the subepithelial connective tissue; degeneration of mitochondria; an electron- opaque perinuclear zone that, upon dissolution, frees remnants of tonofibrils and mitochondria; and wid- ened intercellular spaces between epithelial basal cells. Minute vesicles were found between the base- ment membrane and the basal cell membrane in the intermediate zone, but desmosomes remained intact. The lamellated pattern of the hemidesmosomes dis- appeared and was replaced by a granular sub- stance.
Microscopic and microradiographic studies showed the lamellar enamel varying in thickness from 50 to 400 pm, the outer and inner zones being more mineralized than the intermediate zone. Free globular structures with variable degrees of mineral- ization were seen at the surface and within the enamel. The cervical enamel was more mineralized than the incisal edge. The dentinoenamel junction
Volume 67 Number 5
Epidermolysis bullosa 557
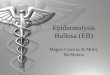
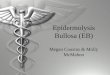
Fig. 2. Junctional EB. The bulla (B) is formed through the lamina lucida between the plasma membrane of basal keratinocytes (K) and the basement membrane (urrowsj. D, dermis. (Original magnification, ~13,000.) (From Haber RM, Hanna W, Ramsay CA, Boxall LBH. J Am Acad Dermatol 1985;13:252- 78.)
had foldings in the permanent teeth but was normal in the deciduous teeth. The enamel stroma was hyalinized, lamellar, and, at times, globular.
Intense proliferation of the dental lamina and the inner and outer enamel epithelium was observed in decalcified sections. The latter also manifested meta- plasia to stratified squamous epithelium. Vascular proliferation was marked about the tooth germs, and hemorrhage was noted in the dental sac and stellate reticulum.2’~ 22
Similar findings have been reported in the decidu- ous dentition of an infant with the Herlitz form of EB.23
DOMINANT DYSTROPHIC (HYPERTROPHIC) FORM (Cockayne-Touraine type)
Systemic features. This form of EB is character- ized by flat, pink, scar-producing bullae of the ankles, the knees, the hands, the elbows, and the feet, in decreasing order of frequency.6 Milia are common but less numerous than in the recessive dysplastic type. In 80% of the cases, the nails are thick and dystrophic. Hyperhidrosis of palms and soles may also occur. The conjunctiva and cornea are not affected. These changes become evident before 1 year of age in about 20% of patients. Improvement occurs with age.
Oral features. Teeth are not affected by 20% of patients manifest oral bullae6sz4 and milia.25 These milia are epidermoid cysts developing in areas of previous bulla formation.
SCARRING EPIDERMOLYSIS BULLOSA WITH DERMOLYTIC BLISTERS (Hallopeau-Siemens type)
Systemic manifestations. This type of EB is divid- ed into four autosomal recessively inherited sub- types, which are difficult to differentiate (Table I). Bullae are usually manifested at or shortly after birth, arising at sites of pressure or trauma or appearing spontaneously. In infants, the most com- monly affected areas are the occiput, the scapulas, the elbows, the fingers, the buttocks, and the feet. In older children, the hands, the feet, the knees, and the elbows are most often involved. Bullae leave painful ulcers upon rupture. Healing is often followed by keloidal scars, causing contraction and various degrees of pigmentation or depigmentation. Milium- like cysts can develop in scar areas. Loss of underly- ing bone and interference with growth, resulting in dwarfism, are also sequelae to scars. Formation of clawhand and enclosure of the hand in a glovelike epidermal sac have been noted frequently26 (Fig. 3). Nikolsky’s sign is often present. The nails may be extremely involved; they are often dystrophic or absent.5 Hyperhidrosis of palms and soles is an inconsistent finding but may be marked. Hair may be deficient.
Ocular changes such as essential shrinkage of the conjunctiva, nonspecific blepharitis, symblepharon, conjunctivitis, and keratitis with cornea1 opacity and vesicle formation have been noted.5
Hoarseness, aphonia, and dysphagia may occur as

555 Sedan0 and Gorlin OKAL Suno ORAL MED ORAL PATHOL May 1989
Table I --
Onset Feet Hand
Type 1: Intraepidermal blister formation Nonscarring EB with autosomal
dominant inheritance EB simplex generalized Koebner
type (D-EBS-K) EB simplex localized
Weber-Cockayne type (D-EBS-WC)
EB simplex with mottled pigmentation (D-EBS-M)
EB simplex Ogna (D-EBS-0) EB herpetiformis Dowling-Meara
(D-EBH-DM) EB Bart Congen; localized absence
of skin (D-EB-B) Nonscarring EB with X-linked
inheritance Dystrophica bullosa hereditaria,
macular type, Mendes Da Costa (X-DBM-MC)
Type II: Junctional blister formation with hemidesmosome defect. atrophicans group Nonscarring EB with autosomal
recessive inheritance EB atrophicans generalisata Gravis
Herlitz (R-EBA-GH) EB atrophicans generalisata mitis
(R-EBA-Mitis) EB atrophicans localisata
(R-EBA-L) EB atrophicans inversa (R-EBA-I) EB progressiva (R-EBP) juvenile
onset deposit type Type III: Dermolytic blister formation,
dystrophic group Scarring EB with autosomal dominant
inheritance EB dystrophica Cockayne-Touraine
type (D-EBD-CT) EB dystrophica Albopapuloidea
Pasini (D-EBD-P) EB pretibial (D-EBD-KP)
(Kuske-Portugal disease) Scarring EB with autosomal recessive
inheritance EB dystrophica Hallopeau-Siemens
(R-EBD-HS) Local Generalized Mutilans EB dystrophica inversa
(R-EBD-I) Type IV: Acquired phenocopies of
dystrophic epidermolysis bullosa EB acquisita (A-EB)
Birth to l/2 year
First to third decade
? First month
At birth
First to third year
First days
At birth
At birth
First days 5 to 8 yr
Birth to five year
First weeks
11 to 24 yr
First weeks First weeks First weeks Neonatal
Adult
Yes
Yes
Yes
Yes
+- Yes No
No No No
Some
No
Yes Yes
Yes
Yes Yes
Yes
Yes Yes
No Yes
No
Rarely No Yes Some
Yes No
No No
No
No No No
Yes at infancy
Yes
Yes
No Yes
Yest at infancy
Yes
No
No Yes
Yes
No
No
No No
Yes
Yes
Yes
Yes Yes
Rarely
No
No
Yes No
Yes
Yes
No
Rarely Yes
Yes
Yes
No
Yes
Yes
No
No
Yes
No
Yes
Yes
Yes
No
No
No
Rarely
Yes
No
Yes Yes Yes + No
Yes Yes Yes t No
Yes Yes Yes No
Yes No Yes + No Yes t+ Rarely Yes No
Yes Yes + Yes t+ Yes
Yes Yes No Yes No Slight

Volume 67 Number 5
Epidermolysis bullosa 5%
Teeth Nails Seasonal variation
No
No
No
No
Warm weather
Summer
No Some
No
No Yes
Yes
Yes
Yes
No
No
No
No
Slight
Yes + Yes ++ No
No
Yes Yes
Yes
No Yes
Yes
Yes
Yes
No
Yes
Summer No
No
‘3
No
Summer
No
No
No
No
Yes
Yes
Slight
No
No
No
Yes Yes ++ No
No No No
Yes No
Fig. 3. Marked atrophy of skin with loss of nails and clawhand deformity as sequelae to marked blistering. (From R&k1 H. Hautarzt 1963;65:477-83.)
a result of bullae of the larynx or pharynx. Scarring of the larynx may lead to stenosis. Frequently the upper part of the esophagus may become stenotic in childhood, with consequent dysphagia.27*28 Complete obstruction is also a complication.27+29 Typical find- ings in the hand are overconstricted, slender meta- carpals with pointed and clawlike, distal phalan- ges.26
Oral features. The teeth have hypoplastic enamel rapidly affected by dental caries, delayed eruption, and frequent retention30’33 (Figs. 4 and 5). There is no correlation between the degree of cutaneous involve- ment and the degree of dental involvement.34
Oral bullae have been reported in at least 16% of cases,8 but we estimate this figure to be higher. Oral mucosal vesicles form soon after birth from the negative pressure produced by the sucking reflex. The lingual mucosa appears thick, gray, and smooth and may become bound down. Repeated blistering with scar formation may lead to diminished oral opening, ankyloglossia, tongue atrophy, elimination of buccal and vestibular sulci, and perioral stric- ture.‘2,35 Even routine dental management or the slightest abrasion from normal toothbrushing may cause the eruption of bullae on the lips and the oral mucosa.35 Other oral changes include severe peri- odontal disease with alveolar bone resorption,30 atro- phy of the maxilla with resultant relative mandibular prognathism, increased mandibular angle,26,36 and oral carcinoma (Fig. 6).37-39
Histology and laboratory findings. Histologic study shows the bullae to occur below the PAS- positive basement membrane.” Hemidesmosomes and tonofibrils are absent or decreased in numbers

560 Sedan0 and Gorlin
Fig. 4. Pitted hypoplastic enamel in patient with Hallo- peau-Siemens type of EB. (From Rodermund OE. Derma- to1 Wochenschr 1967;153:350-7.)
Fig. 5. Radiographs from another patient showing marked enamel hypoplasia and periodontal disease.
(Fig. 7). Another finding has been an increase in elastic and preelastic fibers in the corium.” Histolog- ic studies of unerupted teeth have shown hypoplasia of enamel with absence of prismatic structure21s40 and defective cementum.4’ Accentuation of enamel tuft formation and irregular dentinal foldings and indentations of the dentinoenamel junction have been reported in extracted teeth.12
ORAL SLRC ORAL MED ORAL PATHOL May 1989
Fig. 6. Extensive squamous cell carcinoma initially developing in lower lip mucosa. (From Riichl H. Hautarzt 1956;7:463-4).
ORAL MANIFESTATIONS OF OTHER FORMS OF EB.
Epidermolysis bullosa acquisita. This nonheredi- tary form of EB manifests in adulthood with blisters developing in areas of trauma. It can be associated with amyloidosis, multiple myeloma, diabetes, melli- tus, and inflammatory bowel disease. The last asso- ciation may represent a gastrointestinal cutaneous syndrome with an immune pathogenesis.42 Oral lesions are rare but have been observed.43 Scarring or cicatricial junctional type of EB has autosomal recessive inheritance. 2-5 Patients are affected from birth with skin blisters and absence of nails. Upon healing, the blisters leave deep scars that produce marked disfigurement and atrophy of hands and feet and around the nares. Diminished oral opening can occur. Intraoral blisters can be found at any site but are not as profuse and severe as those in other forms of EB. Extensive dental caries, leading to complete loss of teeth, has been noted in every patient with this condition.
EB nonscarring atrophicans generalisata mitis. This has autosomal dominant inheritance. Oral mucosa can be the site of bullae, mostly in trauma-

Volume 67 Number 5
Epidermolysis bullosa 56 1
Fig. 7. Hallopeau-Siemens type. The bulla (II) is formed below the basement membrane (arrowhead) and is associated with normal keratinocytes (K) and hemidesmosomes (HD). Note the total absence of anchoring fibrils and their replacement with a fuzzy electron-lucent material (F). (Original magnification, X44,000.) (From Haber RM, Hanna W, Ramsay CA, Boxall LBH. J Am Acad Dermatol 1985;13:252-78.)
related areas. Nodular excrescences on the palate and gingiva have been described.44 Teeth may have pitted enamel, resulting in unusually extensive caries.45
A possible new variety of EB has been reported by Nielsen and SjBlundM in two sisters, children of nonconsanguineous parents. The patients had hem- orrhagic blisters limited to the hands and feed and associated with partial alopecia, onychogryphosis, anodontia, and a condition that resembled amelogen- esis imperfecta. Light microscopic observation showed intraepithelial bullae formation. No EM studies were reported. Further reports are needed to add this condition to the EB classification.
DIFFERENTIAL DIAGNOSIS
In infants and children, EB may be confused with bullous impetigo (so-called pemphigus neonatorum), Ritter’s disease, porphyria congenita, congenital syphilis, or juvenile bullous dermatitis herpetiformis. In adults, the differential diagnosis includes pemphi- gus, drug eruptions, dermatitis herpetiformis, and butlous erythema multiforme.
Kindler syndrome, characterized by congenital bullae formation on pressure areas, which on healing leave atrophic scars, and severe photosensitivity and poikiloderma, should be included in the differential diagnosis. In Kindler syndrome, the oral mucosa is atrophic and shows multiple white macules.47 In patients with EB, cellophane adhesive tape stripping
will cause removal of the top layers of the epidermis. This phenomenon is not seen in Ritter’s disease or in generalized impetigo. The lesions of porphyria are generally confined to areas chronically exposed in the sun. Only the exposed skin is fragile; EB shows no localization of skin fragility.
LABORATORY AIDS
Because many of the clinical manifestations in the various subtypes of EB can be similar if not identical, it is imperative that proper typing of patients with EB be accomplished with electron microscopic, immunofluorescent, and immunohistochemical studies.3,4 Microscopically, the bullae are intraepi- dermal in the nonscarring forms, at the level of the epithelial-dermal junction in the trophic forms, and subepithelial or intradermal in the scarring forms. Unfortunately, light microscopy is not useful in differentiating among the severe types of EB. Peri- odic acid-Schiff stain has been used to subdivide the various types of EB according to the location of the basement membrane, but it is unreliable because, during the process of blister formation, there will be retractions in the actual position of the basal mem- brane. The basal membrane remains attached to the dermis in the EB simplex and junctional types, whereas it remains attached to the epidermis in the dystrophic types of EB.
Ultrastructural examinations are essential for an accurate diagnosis of EB types; neither regular light

562 Sedan0 and Gorlin ORAL SURG ORAL MED ORAL PATHOI May IY89
microscopy nor clinical features are sufficient or adequate for a proper diagnosis.
Tonofilaments, which are the intercellular bind- ings of the basal cells, have been shown to be defective in the intraepidermal types of EB. The junctional types of EB are characterized by defects in anchoring filaments of hemidesmosomes, whereas primary or secondary destruction of the anchoring fibrils, which extend from the basal lamina into the dermis, is observed in the dermal types of EB.*O
Other pathogenetic mechanisms for certain types of EB include degradation of collagen through colla- genases.48 Excessive secretion of collagenase by dys- trophic fibroblasts from patients with the simplex and the dystrophic forms of EB has been re- ported.49
Immunofluorescent mapping studies are used to differentiate among various types of EB by detecting the presence of four structural components within skin basement membrane: bullous pemphigoid anti- gen, laminin, type IV collagen, and lamina densa antigen- 1 (LDA- 1). The diagnosis is made by identi- fying the location of these antigens and their relation to the level of cleavage in a freshly induced blister.50 Prenatal diagnosis of the various types of EB is possible through fetoscopy with fetal skin sampling and electron microscopic studies.5’
REFERENCES
1. Kero M, Niemi KM. Epidermolysis bullosa. Int J Dermatol I986;25:75-82.
2. Bergenholtz A, Olsson 0. Epidermolysis bullosa hereditaria. I. Epidermolysis bullosa hereditaria letalis. A survey of the literature and report of 11 cases. Acta Derm Venereol (Stockh) 1968;48:220-41.
3. Haber RM, Hanna W, Ramsay CA, Boxall LBH. Hereditary epidermolysis bullosa. J Am Acad Dermatol 1985;13:252- 78.
4. Gedde-Dahl Jr T, Anton-Lamprecht 1. Epidermolysis bullosa. In: Emery AEH, Rimoin DL, eds. Principles and practice in medical genetics. London: Churchill Livingstone, 1983:672- 87.
5. Gedde-Dahl Jr T. Epidermolysis bullosa: a clinical, genetic, and epidemiologic study. Baltimore: Johns Hopkins, 197 I. 176 pp.
6. Davidson BCC. Epidermolysis bullosa. J Med Genet 1965; 21233-42.
7. Haber RM, Ramsay CA, Boxall LBH. Epidermolysis bullosa simplex with keratoderma of the palms and soles. J Am Acad Dermatol 1985;12:1040-4.
8. Schuermann H. Krankheiten der Mundschleimhaut und der Lippen. 2d ed. Berlin: Urban und Schwarzenberg, 1958.
9. Pearson RW. Epidermolysis bullosa hereditaria letalis. Arch Dermatol 1974;109:349-55.
10. Ritzenfeld P. Zur Histogenese und Differentialdiagnose hereditarer Epidermolysen. Arch Klin Exp Dermatd 1966; 224: 128-37.
11. Lowe LB. Hereditary epidermoljisis bullosa. Arch Dermatol 1967;95:587-95.
12. Crawford EG, Jefferson Burkes Jr E, Briggaman RA. Hered- itary epidermolysis bullosa: oral manifestations and dental therauv. ORAL SURG ORAL MED ORAL PATHOL 1976;42:490-
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
Haber RM, Hanna W, Ramsay CA, Boxall LBH. Cicatricial junctional epidermolysis bullosa. J Am Acad Dermatol 1985;12:836-44. Arwill T, Bergenholtz A, Thilander H. Epidermolysis bullosa hereditaria. V. The ultrastructure of oral mucosa and skin in four cases of the letalis form. Acta Pathol Microbial Stand 1968;74:31 l-24. Hashimoto 1, Anton-Lamprecht I, Meyburg P. Epidermolysis bullosa hereditaria letalis: report of a case and probable ultrastructural defects. Helv Paediatr Acta 1975;30:543-52. Carroll DL, Stephan MJ, Hays GL. Epidermolysis bullosa--- review and report of a case. J Am Dent Assoc 1983:107:749- 51. Wright JT. Epidermolysis bullosa: dental and anesthetic management of two cases. ORAL SURF ORAL MED ORAL PATHOL 1984;57:155-7. Maddison TG, Barter RA. Epidermolysis bullosa hereditaria letalis. Arch Dis Child 196 1;36:337-9. Roberts MH, Howell DRS, Bramhall JL, Reubner B. Epider- molysis bullosa letalis: report of three cases with particular reference to the histopathology of the skin. Pediatrics 1960;25:283-90. Hashimoto I, Gedde-Dahl Jr T, Schnyder UW, Anton- Lamprecht I. Ultrastructural studies in epidermolysis bullosa hereditaria. IV. Recessive dystrophic type with junctional blistering. Arch Dermatol Res 1976;257:17-32. Arwill T, Bergenholtz A, Olsson 0. Epidermolysis bullosa hereditaria. 111. Histologic study of changes in teeth in the polydysplastic, dystrophic, and lethal forms. ORAL SURC ORAL MED ORAL PATHOL 1965;19:723-44. Arwill T, Bergenholtz A, Oisson 0. Epidermolysis builosa hereditaria. IV. Histologic changes of the oral mucosa in the polydysplastic, dystrophica. and the letalis forms. Odontol Rev 1965;16:101-11. Brain EB, Wigglesworth JS. Developing teeth in epidermoly- sis bullosa hereditaria letalis: a histologic study. Br Dent J 1968;124:255-60. Touraine MA. Classification des Cpidermolyses bulleuses. Ann Dermatol Syphiligr 1942;2:309-12. Andreasen JO, Hjorting-Hansen E, Ulmansky M, Pindborg JJ. Milia formation in oral lesions in epidermolysis bullosa. Acta Path01 Microbial Stand 1965;63:37-41. Brinn LB, Khilnam MT. Epidermolysis bullosa with charac- teristic hand deformities. Radiology 1967;89:272-4. Becker MH, Swinyard CA: Epidermolysis bullosa dystrophi- ca in children; radiologic manifestations. Radiology 1968; 90: 124-8. Wey W, Schnyder UW. Uber Gsophagusstenosen bei Epider- molysis bullosa hereditaria und ihre Behandlung. Dermato- logica 1964;128:173-83. Hillemeier C. Touloukian R, McCallum R, Gryboski J. Esophageal web: a previously unrecognized complication of epidermolysis bullosa. Pediatrics 198 I ;67:678-82.
30. D’Angelo M. Le lesioni orali nell’epidermolisi bollosa. Miner- va Stomatol. 1981;30:169-74.
3 1. Kinast H, Schuh E. Die Epidermolysis bullosa und ihre orale Erscheinungsform. Oest 2 Stomatol 1973;70:166-75.
32. Matras H. Ein Beitrag zur Epidermolysis bullosa dystrophica mit Zahn- und Mundschleimhautverlinderungen. Oest Z Stomatol 1963;60:138-45.
33. Winstock D. Oral aspects of epidermolysis bullosa. Br J Dermatol 1962;74:43 l-8.
34. Rodermund OE. Zahnveranderungen bei Epidermolysis bul- loss. Dermatol Wochenschr 1967;153:350-7.
35. Block MS, Gross BD. Epidermolysis bullosa dystrophica recessiva. J Oral Maxillofac Surg 1982;40:753-8.
36. Alpert M. Roentgen manifestations of epidermolysis bullosa. Am J Roentgen01 1957;78:66-72.
37. Klausncr E. Zungenkrebs als Folgestand bei einem Falle von Epidermolysis bullosa (dygrophische Form). Arch Dermatol Syphilol (Berl) 1913;l 16171-8.
38. Rock1 H. Carcinom bei Eoidermolvsis bullosa dvstroohica. 500. . . Hautarzt 1956;7:463-4. ’ .

Volume 67 Number 5
Epidermolysis bullosa 563
39.
40.
41.
42.
43.
44.
45.
46.
47.
Schiller F. Zungencarcinom bei Epidermolysis bullosa dystro- phica. Arch Klin Exp Dermatol i960;209:643-51.
48. Sanchez G, Seltzer JL, Eisen AZ, Stapler P, Bauer EA. Generalized dominant epidermolysis bullosa simplex.
Delaire J. Ktrebel B. Billet J. Manifestation buccodentaires des epiddrmolyses bulleuses. Rev Stomatol (Paris) 1960;
Decrease activity of a gelatinolytic protease in cultured fibroblasts as a phenotypic marker. J Invest Dermatol
61:189-200. 1981;81:576-9. Hitchin AD. The defects of cementum in epidermolysis bullosa dvstronhica. Br Dent J 1973:135:437-41. Ray TL,- Levine JB, Weiss W, Ward PA. Epidermolysis bullosa acquisita and inflammatory bowel disease. J Am Acad Dermatol 1982;6:242-52. Nielsen R, Livden J, Thunold S. Oral lesions of epidermolysis bullosa acquisita. ORAL SURG ORAL MED ORAL PATHOL 1978; 45:749-54.- Giansanti JS. Oral nodular excrescences in epidermolysis bullosa. ORAL SURG ORAL MED ORAL PATHOL 1975:40:385- 90. Paller AS, Fine JD, Kaplan S, Pearson RW. The generalized atrophic benign form of junctional epidermolysis bullosa. Arch Dermatol 1986;122:704-10. Nielsen PG, Sjoulund E. Epidermolysis bullosa simplex localisata associated with anodontia, hair and nail disorders: a new syndrome. Acta Derm Venereol 1985;65:526-30. Shoshana Hachman Z, Garfunkel AA. Kindler syndrome in two related Kurdish families. Am J Med Genet 1985;20: 43-8.
49. Oakley CA, Priestley GC. Collagen synthesis and degrada- tion by epidermolysis bullosa fibroblasts. Acta Derm Venereol 1985;65:277-81.
50. Fine JD, Gay S. LDA-1 monoclonal antibody. Arch Dermatol 1986;122:48-51.
51. Anton-Lamprecht I, Jovanic V, Arnold ML, Rauskolb R, Kern B, Schenck W. Prenatal diagnosis of epidermolysis bullosa dystrophica Hallopeau-Siemens with electron micros- copy of fetal skin. Lancet 1981;2:1077-9.
Reprint requests to.
Dr. Heddie 0. Sedan0 University of Minnesota School of Dentistry Malcolm Moos Health Sciences Tower 515 Delaware St. S.E. Minneapolis, MN 55455