Embed Size (px)
Citation preview

Aus der Universitäts-Hautklinik
der Albert-Ludwigs-Universität Freiburg i.Br.
The Molecular Basis of Dystrophic EpidermolysisBullosa: Mutation Detection and Study of Clinical,Biochemical and Molecular Findings in 29 Patients
INAUGURAL-DISSERTATION
zur
Erlangung des Medizinischen Doktorgrades
der Medizinischen Fakultät
der Albert-Ludwigs-Universität
Freiburg i.Br.
Vorgelegt 2005von Johannes S. Kerngeboren in Würzburg

Dekan Prof. Dr. med. Christoph Peters 1. Gutachter Prof. Dr. med. Leena Bruckner-Tuderman 2. Gutachter PD Dr. med. Jürgen Kohlhase Jahr der Promotion 2006

Part of this work has been published in:
1. C. Has, J.S. Kern and L. Bruckner-Tuderman. 2004. Hereditäre blasenbildende Hauterkrankun-gen. Hautarzt. 55(10):920-933
2. M. Stefanova, K. Zemke, B. Dimitrov, C. Has, J.S. Kern, L. Bruckner-Tuderman and K.Kutsche. Disruption of ERBB21P is not associated with dystrophic epidermolysis bullosa inboth father and son carrying a balanced 5;13 translocation. J Invest Dermatol. in press
3. J.S. Kern, J. Kohlhase, L. Bruckner-Tuderman, C. Has. Expanding the COL7A1 mutationdatabase: novel and recurrent mutations and unusual genotype-phenotype constellations in 41patients with dystrophic epidermolysis bullosa. J Invest Dermatol. in press

Contents
Abbreviations 3
1 Abstract - Zusammenfassung 4
2 Introduction 6
3 Materials and methods 13
3.1 Materials . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 133.1.1 Technical equipment . . . . . . . . . . . . . . . . . . . . . . . . . . . . 133.1.2 Reagents . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 143.1.3 Buffers and solutions . . . . . . . . . . . . . . . . . . . . . . . . . . . 153.1.4 Enzymes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 163.1.5 Primary antibodies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 163.1.6 Secondary antibodies . . . . . . . . . . . . . . . . . . . . . . . . . . . . 173.1.7 Ready to use kits . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 173.1.8 Primers for COL7A1 PCR from gDNA . . . . . . . . . . . . . . . . . . 17
3.2 Patients . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 223.3 Mutation detection . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 22
3.3.1 Isolation of gDNA . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 223.3.2 Amplification of gDNA fragments by PCR . . . . . . . . . . . . . . . . 223.3.3 Agarose gel electrophoresis . . . . . . . . . . . . . . . . . . . . . . . . 253.3.4 DNA sequencing . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 253.3.5 Restriction enzyme digestion . . . . . . . . . . . . . . . . . . . . . . . . 263.3.6 RNA isolation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 263.3.7 RT-PCR . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 27
3.4 In situ and in vitro characterization of procollagen VII/collagen VII . . . . . . . 28
1

Contents
3.4.1 Indirect immunofluorescence of skin cryosections . . . . . . . . . . . . . 283.4.2 Cell culture . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 283.4.3 Indirect immunofluorescence of cultured keratinocytes . . . . . . . . . . 29
3.5 Protein biochemistry . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 293.5.1 Protein extraction from keratinocytes . . . . . . . . . . . . . . . . . . . 293.5.2 Determination of protein concentration . . . . . . . . . . . . . . . . . . 293.5.3 SDS polyacrylamide gel electrophoresis and immunoblotting . . . . . . . 303.5.4 Limited pepsin-trypsin digestion . . . . . . . . . . . . . . . . . . . . . . 31
3.6 Bioinformatics . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 31
4 Results 33
4.1 COL7A1 mutations and their consequences . . . . . . . . . . . . . . . . . . . . 334.1.1 Clinical features . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 334.1.2 Indirect immunofluorescence . . . . . . . . . . . . . . . . . . . . . . . . 334.1.3 Mutation survey . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 334.1.4 Novel and recurrent COL7A1 mutations . . . . . . . . . . . . . . . . . . 34
4.2 Interesting constellations and genotype-phenotype correlations . . . . . . . . . . 394.2.1 Patient 20: Three mutations or a polymorphism? . . . . . . . . . . . . . 394.2.2 Patient 21: First case of de novo mutation in RDEB . . . . . . . . . . . . 454.2.3 Patients 1 and 7: Novel glutamic acid to glycine substitution . . . . . . . 504.2.4 Patient 2: Glycine substitution with predominantly mucosal involvement 544.2.5 Patient 19: RDEB in child and Klinefelter’s syndrome in father . . . . . 58
5 Discussion 59
Bibliography 65
Curriculum Vitae 70
Acknowledgements 71
2

Abbreviations
AE-buffer = TE-buffer
APS ammonium peroxodisulfat
BPE bovine pituitary extract
BSA bovine serum albumin
BSB blue sample buffer
cDNA copy DNA
COL7A1 gene encoding for collagen VII α1 chain
COL17A1 gene encoding for collagen XVII α1 chain
CSGE conformation sensitive gel electrophoresis
DDEB dominant DEB
DEB dystrophic EB
DEJZ dermal epidermal junction zone
dHPLC denaturating high performance liquid chromatography
DMEM dulbecco’s modified eagles medium
EB Epidermolysis bullosa
EBS EB simplex
EDTA ethylenediaminetetraacetic
EGF epidermal growth factor
EM electron microscopy
ET mix Dyenamic ET dye terminator kit (Amersham)
FCS foetal calf serum
FITC fluorescein isothioscyanate
fl-CMM fluorescent chemical cleavage of mismatch
gDNA genomic DNA
Hepes N2 hydroxyethylpiperazine N’2ethansulfonic acid
HS-RDEB Hallopeau-Siemens RDEB
IIF indirect immunofluorescence
IVF in vitro fertilization
JEB junctional EB
KGM keratinocyte growth medium
LAMB3 gene encoding for laminin β3 chain
NBT-solution Nitro blue tetrazolium chloride solution
NC non collagenous domain
NHK normal human keratinocytes
nonHS-RDEB non Hallopeau-Siemens RDEB
PBS phosphate buffered saline
PCR polymerase chain reaction
PTC premature termination codon
PTT protein truncation test
RDEB recessive DEB
RE restriction enzyme
RT-PCR reverse transcriptase PCR
RT room temperature
SDS-PAGE sodium dodecyl sulfate polyacrylamide gel electrophoresis
TBE tris borate EDTA
TBS tris buffered saline
TD PCR touch down PCR
TE-buffer tris EDTA buffer
TEMED N,N,N’,N’ tetramethylethylenediamine
WT wild type
3

1 Abstract - Zusammenfassung
Abstract
Dystrophic epidermolysis bullosa (DEB) is a hereditary skin disorder characterized by trauma-induced blistering. It is caused by mutations in the collagen VII gene, COL7A1, which consistsof 118 small exons. Molecular diagnostics in DEB remain complex due to the gene structure,large variety of mutations, high rate of novel mutations, and the heterogeneity of phenotypes.Using a highly sensitive and efficient strategy for COL7A1 mutation analysis with direct auto-mated DNA sequencing and the implementation of software tools we disclosed mutations in 29DEB patients, including 18 novel mutations and the first de novo mutation in recessive DEB.Genotype-phenotype correlations were assessed with RT-PCR, immunochemical collagen VIIprotein analysis, and collagen triple helix stability assays using limited proteinase digestion andtemperature gradients. In a very rare DEB form with solely mucosal involvement and no skinblistering, the glycine substitution G2689R led to decreased thermal stability of collagen VII.The mutation E2059G did not influence thermal stability but resulted in reduction of collagenVII levels, and mild clinical affection. Elucidation of the clinical, genetic and biological back-ground of 29 DEB patients contributes to the EB mutation database, the understanding of themechanisms underlying DEB and lays a basis for novel therapeutic approaches.
4

1 Abstract - Zusammenfassung
Zusammenfassung
Epidermolysis bullosa dystrophica (EBD) ist eine erbliche Hautkrankheit, die durch trauma-induzierte Blasenbildung charakterisiert ist. Sie wird durch Mutationen im Kollagen VII Gen,COL7A1, welches aus 118 kleinen Exonen besteht, verursacht. Die molekulare Diagnostik beiEBD bleibt aufgrund der Genstruktur, der großen Vielfalt der Mutationen, der hohen Rate un-bekannter Mutationen und der Heterogenität der Phänotypen komplex. Jedoch ist ein besse-res Verständnis von Mutations-Konstellationen und Genotyp-Phänotyp Korrelationen essenti-ell um molekulare Therapien für diese verheerende Krankheit zu entwickeln. In dieser Arbeithaben wir eine effiziente Strategie für die COL7A1 Mutationsanalyse durch direkte Sequen-zierung etabliert und die Mutationen von 29 EBD Patienten aufgedeckt. Diese Strategie hatteeine sehr hohe Sensitivität von 92,7% und die Implementierung ausgereifter Software verbes-serte die Effizienz signifikant. Wir haben 18 bisher unbekannte COL7A1 Mutationen identi-fiziert, 3 Insertion/Deletionen, 2 Nonsense-, 10 Missense- und 3 Splice-Site-Mutationen. DieRate gefundener unpublizierter Mutationen war 47%. Wir deckten auch den ersten Fall einerde novo Mutation in rezessiver EBD auf. Die zwei Mutationen 425A>G und R1933X warenrekurrent. Genotyp-Phänotyp Korrelationen wurden mittels RT-PCR, immunochemischer Kol-lagen VII Proteinanalyse und Kollagen Triple-Helix Stabilitätsprüfungen mit limitierten Prote-inase Verdauungen und Temperaturgradienten aufgedeckt. In einer sehr seltenen EBD Form mitausschließlicher Schleimhautbeteiligung und ohne epidermale Blasenbildung führte die Glyzin-Substitution G2689R zur Reduktion der thermalen Stabilität von Kollagen VII. Die MutationE2059G beeinflusste die thermale Stabilität nicht, aber führte zu verringertem Kollagen VII undmilder klinischer Beteiligung. Die Aufhellung klinischer, genetischer und biologischer Hinter-gründe von 29 EBD Patienten trägt zur EB Mutationsdatenbank und dem Verständnis der EBDzugrunde liegenden Krankheitsmechanismen bei und bildet eine Basis für neue therapeutischeAnsätze.
5

2 Introduction
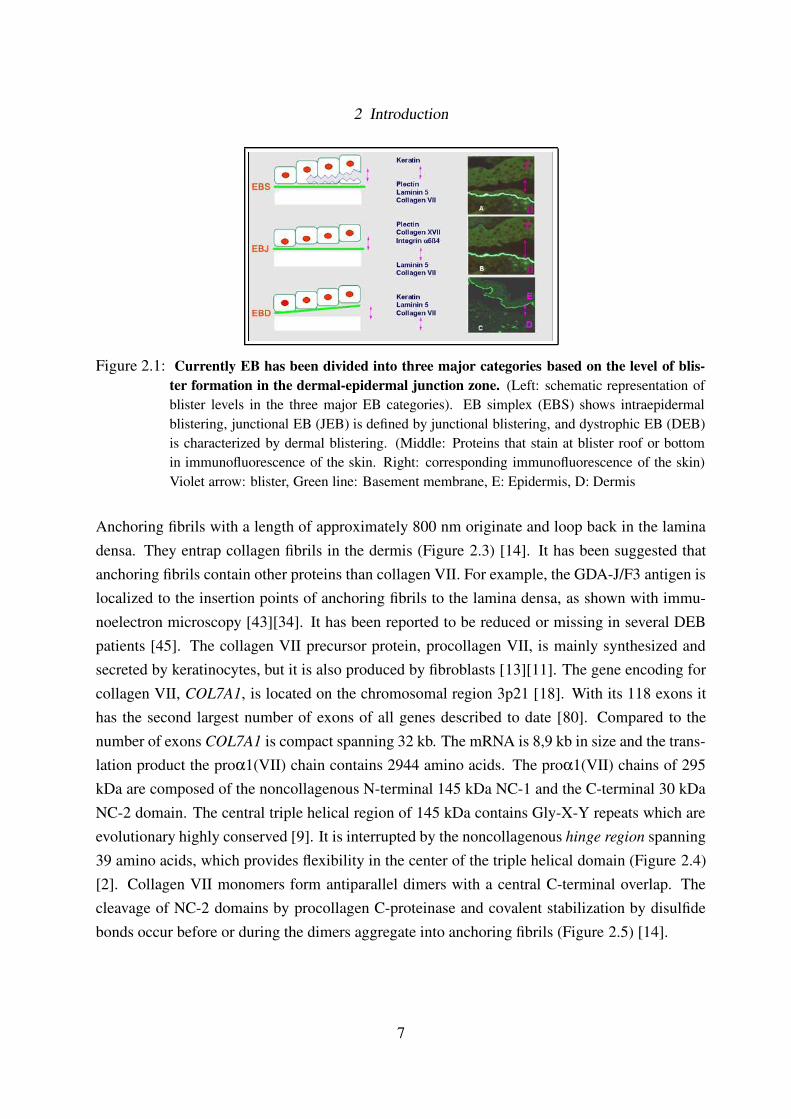
Epidermolysis bullosa (EB) is a clinically and genetically heterogeneous group of heritable skindisorders. It is characterized by blistering of the skin and mucous membranes, following minortrauma, with a broad range of clinical severity [30][7]. Currently EB has been divided into threemajor categories based on the level of blister formation in the dermal-epidermal junction zone(DEJZ) (Figures 2.1 and 2.2) [31]. EB simplex (EBS) shows intraepidermal blistering and iscaused by defects in the genes for keratin 5, keratin 14 and plectin. Junctional EB (JEB) is aheterogeneous group with extreme clinical variation. It is defined by junctional blistering andcaused by mutations in the genes for laminin 5, α6β4 integrin and collagen XVII.
Dermal blistering and scarring are the hallmarks of dystrophic EB (DEB). It can be inheritedby autosomal dominant or autosomal recessive transmission [31][7]. Immunofluorescence of theskin has shown that collagen VII, the major component of the anchoring fibrils, is reduced or neg-ative in DEB [12][10]. Transmission electron microscopy revealed alterations or absence of an-choring fibrils in the skin of DEB patients [81][10]. It has now been demonstrated that all formsof DEB are caused by mutations in COL7A1, the gene coding for collagen VII [38][83][42].
Anchoring fibrils and DEJZ
Collagen VII is the major component of the anchoring fibrils. These fibrils connect the epidermalbasement membrane to the underlying dermis [9]. Together with other protein complexes suchas hemidesmosomes [56] and anchoring filaments [1] they form the so called DEJZ (Figure2.2). The DEJZ, or epidermal basement membrane separates and at the same time attaches theepidermis and the dermis. It provides stability and resistance against external mechanical stress.The study of pathomechanisms underlying acquired and inherited blistering skin disorders, suchas EB, has significantly contributed to understanding of the structure and function of the DEJZ.Basement membranes similar to the DEJZ can be found in other organs like mucous and placentalmembranes. This explains why some forms of EB are not limited to the skin.
6
2 Introduction
Figure 2.1: Currently EB has been divided into three major categories based on the level of blis-ter formation in the dermal-epidermal junction zone. (Left: schematic representation ofblister levels in the three major EB categories). EB simplex (EBS) shows intraepidermalblistering, junctional EB (JEB) is defined by junctional blistering, and dystrophic EB (DEB)is characterized by dermal blistering. (Middle: Proteins that stain at blister roof or bottomin immunofluorescence of the skin. Right: corresponding immunofluorescence of the skin)Violet arrow: blister, Green line: Basement membrane, E: Epidermis, D: Dermis
Anchoring fibrils with a length of approximately 800 nm originate and loop back in the laminadensa. They entrap collagen fibrils in the dermis (Figure 2.3) [14]. It has been suggested thatanchoring fibrils contain other proteins than collagen VII. For example, the GDA-J/F3 antigen islocalized to the insertion points of anchoring fibrils to the lamina densa, as shown with immu-noelectron microscopy [43][34]. It has been reported to be reduced or missing in several DEBpatients [45]. The collagen VII precursor protein, procollagen VII, is mainly synthesized andsecreted by keratinocytes, but it is also produced by fibroblasts [13][11]. The gene encoding forcollagen VII, COL7A1, is located on the chromosomal region 3p21 [18]. With its 118 exons ithas the second largest number of exons of all genes described to date [80]. Compared to thenumber of exons COL7A1 is compact spanning 32 kb. The mRNA is 8,9 kb in size and the trans-lation product the proα1(VII) chain contains 2944 amino acids. The proα1(VII) chains of 295kDa are composed of the noncollagenous N-terminal 145 kDa NC-1 and the C-terminal 30 kDaNC-2 domain. The central triple helical region of 145 kDa contains Gly-X-Y repeats which areevolutionary highly conserved [9]. It is interrupted by the noncollagenous hinge region spanning39 amino acids, which provides flexibility in the center of the triple helical domain (Figure 2.4)[2]. Collagen VII monomers form antiparallel dimers with a central C-terminal overlap. Thecleavage of NC-2 domains by procollagen C-proteinase and covalent stabilization by disulfidebonds occur before or during the dimers aggregate into anchoring fibrils (Figure 2.5) [14].
7

2 Introduction
Figure 2.2: The DEJZ, or epidermal basement membrane attaches the epidermis to the dermis. Itprovides stability and resistance against external mechanical stress. It is build of a com-plex network of highly specialized proteins. Plectin, Collagen XVII and α6β4 integrin formhemidesmosomes, that attach basal keratinocytes to the basement membrane. Collagen VII isthe major component of the anchoring fibrils. Anchoring fibrils connect the epidermal base-ment membrane to the underlying dermis. EB simplex (EBS) shows intraepidermal blisteringwithout scarring and is caused by defects in the genes for keratin 5, keratin 14 and plectin.Junctional EB (JEB) is defined by junctional blistering and caused by mutations in the genesfor laminin 5, α6β4 integrin and collagen XVII. Dystrophic EB (DEB) is characterized bydermal blistering. All subtypes of DEB are caused by mutations in the gene for Collagen VII.With modifications from [8].
Figure 2.3: Immunoelectron microscopy of collagen VII at the basement membrane of human fore-skin. Collagen VII is the major component of the anchoring fibrils (AF). Bar, 250 nm. Withmodifications from [46].
8

2 Introduction
Figure 2.4: The procollagen VII proα1(VII) chain contains 2944 amino acids. The proα1(VII)chains of 295 kDa are composed of the globular noncollagenous N-terminal NC-1 and theC-terminal noncollagenous NC-2 domain. The central triple helical region contains Gly-X-Y repeats. It is interrupted by the noncollagenous hinge region spanning 39 amino acids,which provides flexibility in the center of the triple helical domain. The diagram indicatesthe relative positions of the nine consecutive fibronectin type III domains (FNIII) and vonWillebrand Factor homologies (vWFA) within NC-1, as well as the relative position of theKunitz module (KU) within the NC-2 domain.
Figure 2.5: Schematic representation of anchoring fibril polymerization. Collagen VII monomersform antiparallel dimers with a central C-terminal overlap. The cleavage of NC-2 domainsby procollagen C-proteinase and covalent stabilization by disulfide bonds occur before orduring the dimers aggregate into anchoring fibrils. With modifications from [9].
9

2 Introduction
COL7A1 mutations and dystrophic EB
So far, more than 200 distinct COL7A1 mutations have been identified in DEB [59][48][85][54][33]. They are distributed over the entire gene and are molecularly heterogenous: missensemutations, especially glycine substitutions within the gene region corresponding to the triplehelix, splice site mutations leading to in-frame or out-of-frame exon skipping or intron insertion,nonsense mutations or small insertion-deletions leading to PTCs. In addition, many recessiveDEB patients are compound heterozygous, this means that two different types of mutation canbe combined. This is one reason for the large variety of clinical phenotypes in DEB. Still, somecorrelations between DEB subtypes and mutation categories have been demonstrated [42].
Dominant DEB (DDEB) has a rather mild clinical phenotype mostly limited to the skin. Blis-tering usually occurs at birth or shortly thereafter. There is a predilection for the extremities.Patients often have nail dystrophy and loss of nails. Immunofluorescence of the skin shows pos-itive or reduced collagen VII staining at the blister roof [36]. Glycine substitution mutations inthe triple helical region are characteristic for DDEB. They cause the disease through dominantnegative interference. Yet, in contrast to other collagens where glycine substitutions are commonand cause severe phenotypes [78], in COL7A1 they are less frequent and can cause very mildphenotypes [9]. Furthermore, glycine substitutions can be inherited in an autosomal recessivemanner, sometimes causing difficulty to distinguish dominant from recessive transmission [51].
Recessive non Hallopeau-Siemens DEB (nonHS-RDEB) is characterized by generalized blister-ing at birth, mucosal involvement, dystrophy of teeth and loss of nails. There are no mutilationsor syndactylies. Immunofluorescence of the skin shows reduced collagen VII staining at theblister roof [36]. The genetic background is heterogeneous including missense mutations, splicesite mutations resulting in in-frame exon skipping, or mutations at the end of the collagen VIImolecule at least in one of both alleles. Frequently, non-HS RDEB patients are compound het-erozygous, and the second mutation often causes a PTC [42].
Hallopeau-Siemens recessive DEB (HS-RDEB) is one of the most severe subtypes of EB. Gener-alized blistering is already present at birth and increases progressively. Poorly healing ulcerationsand scarring are typical. The synechia and mutilations of hand and feet, which are HS-RDEBcharacteristic, can already develop early in life. Oral and gastrointestinal involvement leads tomalnutrition. Malnutrition and protein loss through ulcerations result in growth retardation andanemia. Immunofluorescence of the skin shows absence or strong reduction of collagen VII[36]. In the majority of HS-RDEB cases the genetic defects cause PTCs. These lead to nonsensemediated mRNA decay or truncated collagen VII polypeptides degraded within the cell [17][42].
10

2 Introduction
In many cases distinguishing different DEB subtypes is challenging. Recently patients with com-binations of dominantly and recessively transmitted mutations have been described [22][86][35].Considering the structure of COL7A1, the heterogeneity of mutations, the possibility of combina-tions and different pathomechanisms, it becomes clear that genotype-phenotype correlations areonly beginning to emerge. For the same reasons giving a medical prognosis upon the underlyinggenetic defects remains delicate.
HS-RDEB as well as nonHS-RDEB patients have a high risk of developing squamous cell carci-noma at a young age [31], with molecular insight in this issue only beginning to emerge [52][72].As there is no causal treatment for EB up to now, efforts are made to develop somatic gene ther-apy. Different approaches for ex vivo gene therapy have been made. Collagen VII deficienthuman keratinocytes or fibroblasts have been genetically treated by COL7A1 cDNA integrationthrough a bacteriophage [74][73] or injection of a lentivirus expressing full-length type VII col-lagen [16]. These cells have been used to regenerate skin on immuno deficient mice. Baldeschiet al have used a retroviral system to gene correct human collagen VII deficient keratinocytes[3]. Other techniques are to apply recombinantly produced collagen VII directly to regenerateskin on immuno deficient mice [87], or to apply a lentiviral vector directly (in vivo somatic genetherapy) [88]. These attempts are promising, but they still have to be tested in animal modelsbefore first trials in humans can be undertaken.
Mutation detection in COL7A1
Mutation detection in DEB is essential for final diagnosis, to allow genetic counseling and reli-able prenatal diagnosis for the family and, with restrictions, to give a prognosis for the patient.COL7A1 is large (32kb) and has an unusual structure of 118 small exons and very small introns.More than 200 different mutations have been reported. They are distributed over the entire gene.Many RDEB patients are compound heterozygous. The rate of novel mutations found remainedhigh in recent studies [85][33]. Therefore mutation detection in COL7A1 remains technicallytedious, time consuming and expensive. Different mutation detection strategies include con-formation sensitive gel electrophoresis (CSGE) [19], protein truncation test (PTT), fluorescentchemical cleavage of mismatch (fl-CMM) [85] and denaturating high performance liquid chro-matography (dHPLC) [77].
11

2 Introduction
Aims of this study
Aims of this study were to establish efficient mutation detection in COL7A1 by direct sequenc-ing. This strategy was chosen due to its high sensitivity and specificity, and due to recentlydecreasing costs. Another objective was digital analysis and management of the high amountof sequencing data that would be produced. Using the above technical advances, the COL7A1
mutations of 29 DEB patients subject to this study should be disclosed, allowing new insightinto the mutations underlying DEB. Together with clinical assessment and functional studies ofcollagen VII - such as in situ and in vitro characterization of collagen VII, immunoblotting andlimited protein digestion assays - this should enhance our understanding of genotype-phenotypecorrelations and improve the knowledge of the biology of DEB.
12

3 Materials and methods
3.1 Materials
All items not listed here were standard laboratory products bought from BD Labware, Heidel-berg; Eppendorf, Hamburg; Merck, Darmstadt; Neolab, Heidelberg; Nunc, Wiesbaden; Roche,Mannheim; Roth, Karlsruhe; Sigma-Aldrich, Munich.
3.1.1 Technical equipment
Agarose gel chambers mini, midi, large Roth, Karlsruhe
Automated sequencer ABI Prism 3100 ABI, Darmstadt
Automated sequencer Megabace 500 Amersham, Freiburg
Blot chamber WWU, Muenster
Cooling centrifuge 5417R Eppendorf, Hamburg
Cooling centrifuge Biofuge fresco Heraeus, Hanau
Centrifuge Labofuge 400 Heraeus, Hanau
Confocal laser scanning microscope LSM 510 Carl Zeiss, Oberkochen
Cryomicrotome CM1900 Leica, Wetzlar
Elisa reader Multiskan EX Thermo Electron, Bremen
Gel documentation system Intas GDS, Goettingen
Immunofluorescence microscope Axiophot & digital Axio Cam MRc Carl Zeiss, Oberkochen
Laminar flow Ehret, Emmendingen
Laminar flow Heraeus, Hanau
PH-meter Sartorius, Goettingen
Power supply Power pac 300 Biorad, Muenchen
Power supply P25, P30 Biometra, Goettingen
SDS-gel mini chamber Biometra, Goettingen
Spectrophotometer Bio Photometer Eppendorf, Hamburg
Thermal cycler PTC-100, minicycler Biozym, Hess. Oldendorf
Thermal cycler Mastercycler gradient Eppendorf, Hamburg
Thermal mixer Thermomixer comfort Eppendorf, Hamburg
13

3 Materials and methods
3.1.2 Reagents
AE-buffer (TE) Qiagen, Hilden
Agarose Sigma-Aldrich, Munich
Big dye terminator kit 1.1 ABI, Darmstadt
Biogel P100 Biorad, Munich
Chemiluminescence film Hyperfilm ECL Amersham, Freiburg
Dual Color Precision Plus Protein Standard (marker for SDS-PAGE) Biorad, Munich
DNA molecular weight marker X (0,07-12,2 kbp) Roche, Mannheim
Developer for x-ray films Adefo-Chemie, Nuernberg
Dyenamic ET dye terminator kit (ET mix) Amersham, Freiburg
Eukitt Kindler, Freiburg
Fixation for x-ray films Sterling, Bad Homburg
Lumi light western blotting substrate Roche, Mannheim
Millipore multiscreen 96 well plate Millipore, Schwalbach
Mowiol Calbiochem, Bad Soden
Nucleotides dNTP Eppendorf, Hamburg
Pefabloc SC (4-(2-Aminoethyl)-benzolsulfonyl-fluoride-hydrochloride) Roche, Mannheim
Protran BA85 Cellulosenitrat Schleicher&Schuell, Dassel
Primer synthesis Biomers.net, Ulm
Ready load 100bp DNA ladder Invitrogen, Karlsruhe
Sephadex G50 fine Amersham, Freiburg
Media solvents and adjuvants for cell culture
Antibiotic-Antimycotic (10000 U/ml penicilin G, 10000mg/ml streptomycin, 25µg/ml ampho-
tericin B)
Invitrogen, Karlsruhe
DMEM +20mM Hepes ICN Biomedicals, Meckenheim
Dulbecco’s modified eagle medium (DMEM) Invitrogen, Karlsruhe
Foetal calf serum (FCS) Seromed, Berlin
Keratinocyte-sfm + supplements (EGF+BPE) (KGM) Invitrogen, Karlsruhe
PBS w/o Ca++, Mg++ Invitrogen, Karlsruhe
Trypsin-EDTA Invitrogen, Karlsruhe
14

3 Materials and methods
3.1.3 Buffers and solutions
Blue sample buffer for SDS-PAGE (BSB) 8M Urea1M Tris/HCl, pH 6,80,01% (w/v) bromphenolblue20% (w/v) SDS5% (v/v) Glycerin
0,1M DTT
Buffer 3 (detection buffer for alkaline phosphatase) 100mM Tris/HCl, pH 9,5
100mM NaCl
DNA-sample buffer for agarose gel electrophoresis 50% GlycerolTBE 1x
1% Bromphenolblau
Electro transfer buffer 25mM Tris0,2M Glycine, pH 8,3-8,420% (v/v) Methanol
0,1% (w/v) SDS
Mowiol 20g Mowiol 4-8880ml PBS
40ml Glycerin
NBT-solution
75mg/ml Nitro blue tetrazolium chloride in 70% (v/v) Dimethylformamide
PBS 137mM NaCl2,7mM KCl9,6mM Na2HPO4
1,8mM KH2PO4
Protein extraction buffer (storable) 1% Nonidet P4020mM Tris/HCl, pH 7,5
100mM NaCl
Protein extraction buffer complete (prepare day of extraction) 1 ml Protein extraction buffer (stock)4mM EDTA (20µl 200mM)
1mM Pefabloc (10µl 100mM)
SDS-PAGE Electrophoresis buffer 25mM Tris0,2M Glycine, pH 8,3-8,4
0,1% (w/v) SDS
Separation gel buffer 1,5M Tris/HCl, pH 8,8
0,4% (w/v) SDS
Stacking gel buffer 0,5M Tris/HCl, pH 6,8
0,4% (w/v) SDS
15

3 Materials and methods
TBE 1M Tris1M Boric acid
20mM EDTA-Na22H2O
TBS 0,15M NaCl
0,05M Tris/HCl, pH 7,4
X-Phosphate Solution
50mg/ml 5-Brome-4-chlor-3-indolylphosphate toloidinsalt in dimethylformamide
3.1.4 Enzymes
Hot Master Hot Start Taq polymerase (5U/µl) Eppendorf, Hamburg
Hot Start Taq polymerase with antibody (5U/µl) Genaxxon, Stafflangen
Pepsin (47U/g) Sigma-Aldrich, Munich
Trypsin (3,6U/mg) Serva, Heidelberg
Soybean trypsin inhibitor (from Glycine max, type I-S, Lypophilized powder) Sigma-Aldrich, Munich
Restriction enzymes New England Biolabs, Frankfurt; Roche, Mannheim; Invitrogen, Karlsruhe
3.1.5 Primary antibodies
Primary antibodies Epitope (working dilution) Type Origin Source
LH7,2 Collagen VII NC-1 domain (IF 1:100) monoclonal mouse I. Leigh, London, UK [49]
NC1-F3 Collagen VII NC-1 domain (Blot 1:5000) polyclonal rabbit S. Mecklenbeck, Muenster [53]
a-VII-aff Collagen VII triple helical domain (IF 1:1, Blot 1:20) polyclonal rabbit L. Bruckner-Tuderman, Freiburg [13]
NC2-10 Collagen VII NC-2 domain (Blot 1:250 - 1:1000) polyclonal rabbit L. Bruckner-Tuderman, Freiburg [11]
GDA-J/F3 GDA-J/F3 antigen (IF 1:100) monoclonal mouse L. Bruckner-Tuderman, Freiburg [34]
CIV-22 Collagen IV (IF 1:2) monoclonal mouse B. Odermatt, Zuerich [71]
16

3 Materials and methods
3.1.6 Secondary antibodies
Secondary antibodies (working dilution)
Immunofluorescence:
Anti rabbit-IgG FITC labeled (1:30) Dako, Hamburg
Anti mouse-IgG FITC labeled (1:30) Dako, Hamburg
Immunoblotting
Anti rabbit-IgG POD labeled (1:5000) Kirkegaard & Perry, Gaithersburg, MD, USA
Anti rabbit- IgG AP labeled (1:30000) Sigma-Aldrich, Munich
3.1.7 Ready to use kits
Advantage RT-for-PCR Kit BD Biosciences, Heidelberg
DyEx 2.0 Spin Kit Qiagen, Hilden
Dc-Proteinassay Biorad, Munich
Perfect RNA Eukaryotic Mini Eppendorf, Hamburg
QIAquick Gel extraction kit Qiagen, Hilden
Qiaquick PCR Purification kit Qiagen, Hilden
QiAmp DNA mini kit Qiagen, Hilden
QiAmp RNA blood mini kit Qiagen, Hilden
3.1.8 Primers for COL7A1 PCR from gDNA
Exons gDNA-Primers Product size (bp)
1 5-CAGGCAAGACCAGGACTCGG-3
5-GTCGTGGAGTTGGCTGGGTT-3
307
2 5-ACCATCCCAAGTCCCAGTGA-3
5-TGTTTCTGCAAAGACCTGGC-3
375
3, 4 5- GGCCAGAAGAGATCCTGAGT-3
5-CTGACCTGTCACTCCTGCTC-3
422
17

3 Materials and methods
5 5-AGCAGGAGTGACAGGTCAGC-3
5-GGGTCAGGAGCACATAGGAT-3
337
6 5-GTGTACCCTGACCTAGACCC-3
5-GAGGTCACTTTATCTTGCCC-3
369
7 5-TCAGGAGTATAGGTGGTGGC-3
5-CAGGGATTCATGGAGCTAGA-3
281
8 5-CAATTCTGCCAGCCTCTGAC-3
5-GGCTTGCAGACTCAGGACTC-3
285
9 5-GTGAGAGATGTGGCTGAGGG-3
5-GCACATGGGATGTCAGTGGC-3
320
10 5-GTGAGAAGGCTGGGCACTTT-3
5-ACAGGGTCAGACCAGCAGAG-3
258
11 5-GAAGGGATGGACAGGCAAGG-3
5-AGCACAGCATAGAGGCAGCC-3
284
12 5-CAGTGAGTGGGGGAGGTGTC-3
5-GAAGGAGAGCGCTGGAGGTA-3
274
13 5-CCTTCTCACTCTGCGTCCCT-3
5-AACCAGGACCAGAGTGAGGC-3
295
14 5-TGAGTACTGCAGGAGGCTTG-3
5-TGAGGTCAGAGGGAAATGCT-3
315
15 5-AATGAGGGTATGGGTGCCAG-3
5-GGAGGAGGGAGTGGGATTCT-3
337
16 5-CCCACTCCTTCCTGCCTGTT-3
5-AACAGGGATGGAGGCAGCTC-3
295
17 5-ACAGAGTTTGCTAGCCCTGG-3
5-CTGGGCAATCAGGAACACAC-3
263
18 5-GCTGCCTAAAGTGACCTGTC-3
5-GCATACAGCAATGGTTAGGG-3
316
19 5-CCCTAACCATTGCTGTATGC-3
5-CCAAAGGCTCACTACCAATC-3
288
20 5-CAGGGTCTGAGAGGAGGGAG-3
5-CCATCAGTGTCTCGCCTACC-3
323
21 5-AACCCAGTTAACAGAGCCAG-3
5-GGAGGAGTCACTCAGAGTCG-3
325
22 5-ACCCAGGATCTCAGATCTCT-3
5-TGCAGGAGACAGAACTTGAT-3
294
23 5-AGTTGGGGCTCTGTGGAGAC-3
5-CAAGTTACTGAAGCGGGCAG-3
263
24 5-ATAGTGGGCATAGTGGGAAG-3
5-TGTGAGAGAGCTGGGAGAAT - 3
333
18

3 Materials and methods
25 5-CACCCTGATGTGTTTCTCCA-3
5-GGAAGGACATGTCAGAACCC-3
290
26 5-GCATGGACTCCTGGGGCTAT-3
5-TAAGGTGGGGTCCAGTGGCT-3
299
27 5-GTAAGGAGTAGGCTGATGGG-3
5-AGGGTCTCTTTGAGGTTGAA-3
346
28, 29, 30, 31 5-GGGACTGGGTGGTAGAATAT-3
5-GAGACAGCTTTGAGGAGTGC-3
548
32, 33 5 - TCTGCCTCACTGTTCCACCC - 3
5 - GCTCAGGCGAATGTCAACGT - 3
450
34, 35 5-TGCTCTCTAAGTGTCTTCCC-3
5-CCCACTACACATCACTTGCC-3
444
36 5-GGTATGTGGAGGCAAGTGAT-3
5-CAAGGACTTTGGGAGAACTG-3
321
37, 38 5-CCTCATGAGTGCCATGTGAT-3
5-AGAGACCCACACCCCTGAG-3
443
39, 40 5-CCCTTGTGACCCTTTGATT-3
5-CAAGAACTATGAAGCCCAGC–3
440
41, 42 5 - TTTCTCCTTCAGGGTGACTC - 3
5 - CACGTTCGCCCTGATGGAAA - 3
589
43 5-CTGGAGAGAAGGTAAGTGCA-3
5-GAAGTCAGAACCAGAAAGGC-3
188
44, 45, 46 5 - TCTAGCCCTGTCTGTCCATA - 3
5- TATAGGAGGGTCACTGCTCA -3
461
47, 48 5-GACTTCCAATTCCATGTGAC-3
5-CTGTGGATGGAAGGATAAGA-3
399
49, 50 5-GGGCAGTTGGTGAAGGTTGT-3
5-AAGAGGGAGGTGATGCAGGA-3
312
51, 52, 53 5 - CCTTGAGAACTGCTTGCTTC - 3
5 - TTTCCTATCACCTTCATGCC - 3
579
54 5-TGATGGGAACCTCTGATGTG-3
5-GAAGATTGGGAGGGTTTAGC-3
299
55, 56 5-ACACACGCATCTGAAGGCTA-3
5-AGGTTTCAGAGGGACAGTGG-3
543
57, 58, 59, 60 5-CCTCACAGACCCTGTATCCC - 3
5-GGATCTGATAACCCAGGCTC - 3
575
61, 62 5-ATGAGCCTGGGTTATCAGAT - 3
5-TCTCTCGGATGCTGTGACTA - 3
506
63, 64 5- GCCCAAGGGATATCTCAGAG - 3
5-TCTTGGCTGTGTAGGTGTGC - 3
312
19

3 Materials and methods
65, 66 5 - GTAGTGTCTTGCAGCCAGA - 3
5 - CATCAGCACCCTGAGACCTC- 3
372
67, 68 5-AGAGAAAGGAGATTCAGGCG-3
5-TTTGGATCCAGTCTCCCCA-3
509
69, 70 5-TGAGTGCGGATGTTGGGTAG-3
5-GCCCAAGTTCCCTTGAGTGT-3
433
71 5-GCAGGAGCTTCTCTGTCATG-3
5-ACAGCAAGAGGTCAGAGGAG-3
196
72 5 - TCAAGGTGGGTTGTTTAGGG - 3
5 - GGAAGAGAGAATGCTGGTGG - 3
321
73 5 - GGGTGTAGCTGTACAGCCAC - 3
5 - CCCTCTTCCCTCACTCTCCT - 3
286
73-75 5-CCACCAGCATTCTCTCTTCCA-3
5-TGGCTTCCTGGTCACTAGTCA-3
556
74-75 internal primers for sequencing 5-AGCCTGGAAAGCCTGGTATT-3
5-ACAGGACTAAGGCAGGGATG-3
382
76 5-AAGCCACCCTTAGCTTGGT-3
5-TGGGGATGAGATGTCAAGTCA-3
295
77, 78 5 -GCTAAGGTCAGTGTGTGGAA - 3
5 - CCCTAGACAGAGTCAGACCC - 3
431
79 5-GTAAGTCCTTGCCCAACACC-3
5-CGAGAGGCACACAGACACAG-3
341
80, 81, 82 5-CAAGTGAGGCCCAGATTGAG-3
5-GGCATGGACACAGCTTGAAG-3
481
83, 84, 85 5 - TAGTGTGCGCCAACCTCCTG - 3
5 - CTGCCTGTCGACCCTTGACC - 3
485
86, 87 5 - GTCAAGGGTTGGGCTCCAGG - 3
5 - TGGAAACAGGCTTGTGGGTG - 3
404
88, 89 5 - CACAAGCCTGTTTCCAAATG - 3
5 - GGGTGGGTAAACTATGGGTC - 3
331
90, 91 5-CGCATATTTAAGCTCTGGCC-3
5-CTTATGCCCGCCATCACACT-3
319
92, 93 5 - AGCCCGTGTCTGAACTCTGT - 3
5 - ACTCCCTCTTCCTCCTGTGG - 3
311
94, 95 5 - TGATGAGAGTCCTGGGAGGG - 3
5 - CCCATCCTAAGTCCTCACGA - 3
457
96, 97 5 - TCGTGAGGACTTAGGATGGG - 3
5 - GAGGTTGGAAATCAGAGGCA - 3
383
98, 99 5 - CTCTTGCCTCTGATTTCCAA - 3
5 - CCCGCACCTGAATTCTAATA - 3
429
20

3 Materials and methods
100, 101, 102 5-GAAGGTCCTGGCATGAGTGG-3
5-TGCCCTCACAGTAGCTGTGG-3
565
103, 104 5 - CGGGCTCGTTGTATTCTAAG - 3
5 - CAAAAGCTACCACACTGGTG - 3
513
105, 106 5-GGCGATTCTCTTTGGTCCCT-3
5-GCAGTGGGGTGAGCCTTAGG-3
457
107, 108 5-GTACAGAGGGGATGGGGGCT-3
5-AGCCTTCCTTGTCCCTACAC-3
358
109, 110 5 - GAGTTCAGGGAGGTTCCAGA - 3
5 - TGGTTATGAGGTTGGAAGGG - 3
419
111, 112 5-AACCTCTGAAGCTGTGGCCC-3
5-GGGTCAGGGTGCTGGGTGAG-3
399
113 5-TCCATGCAGTCTCACCATAG-3
5-CTTGACTGCTTGCCCTGTAA-3
236
114, 115 5 - CCCTCTGCCTGTGTGTCTCT - 3
5 - CTGCATTCATGGACACCCAT - 3
418
116 5 - ACAGTGGAAATCAGTGCTGC - 3
5 - AGGGTTTGTGGGAATCAGAG - 3
275
117 5 - TCAACCCTCTCTGATTCCCA - 3
5 - AAGGACTCCTCCCCCAGAAC - 3
324
118 5 - TCTCCGGGGAAGGTCAGATG - 3
5 - CATCACAGGCTTGGGTCAAG - 3
355
21

3 Materials and methods
3.2 Patients
In this study 29 patients with clinically defined dystrophic epidermolysis bullosa were investi-gated. Based on family history, 26 were considered recessive and three dominant. The patientswere referred to the Epidermolysis bullosa Zentrum of the University of Freiburg, or materialand clinical information were sent by cooperating centers. Following informed consent, EDTA-blood samples were obtained from all patients and near relatives. In most cases, skin biopsieswere taken for immunofluorescence staining and cell culture. The study was approved by theethical committee of the University of Freiburg.
3.3 Mutation detection
3.3.1 Isolation of gDNA
Genomic DNA (gDNA) was extracted from white blood cells in EDTA-blood samples and, in onecase, from buccal swabs using QiAmp DNA mini kit (Qiagen) according to the manufacturer’sprotocol. Concentration and purity were measured by spectrophotometry. gDNA quality wasverified by 0,8% agarose gel electrophoresis using 3 µl of each sample and 3 µl of loading buffer.gDNA was diluted to 10 ng/µl in AE-buffer.
3.3.2 Amplification of gDNA fragments by PCR
For amplification of all 118 COL7A1 exons and exon/intron boundaries, 73 pairs of primers weredesigned according to Christiano et al. [19] with modifications (cf. 3.1.8 ). New primers weredesigned with Web Primer [69] or Primer3 [63]. To improve mutation detection, we set up aworking strategy based on priority regions. We classified COL7A1 exons in three categoriesaccording to the number and frequency of reported mutations and arranged primer pairs on 96-well plates according to their annealing temperatures. The first plate contained 22 primer pairscorresponding to the most frequently affected gene regions; plate 2 contained 31 primer pairscorresponding to intermediately affected gene regions and plate 3 contained 20 primer pairsof regions very rarely reported to contain mutations (cf. Table 3.9). For PCR hot start Taq
polymerases (Eppendorf, Genaxxon) were used. For reaction mix and PCR conditions see Table3.10 and Table 3.11.
22

3 Materials and methods
Table 3.9: ”Priority strategy for COL7A1”
High Priority Exons and Annealing Temperature
Annealing
Temperature56◦ 58◦ 59◦ 60◦ 61◦ 62◦ 63◦ 65◦
Exons 37-38 44-45-46 34-35 73 3-4 105-106 76 111-112
51-52-53 72 79 74-75 5 107-108 83-85
103-104 80-82 13 94-95
109-110 69-70
114-115
Medium Priority Exons and Annealing Temperature
Annealing
Temperature56◦ 58◦ 59◦ 60◦ 61◦ 62◦ 63◦ 65◦
Exons 61-62 19 36 2 17 117 92-93 67-68
90-91 6 21 118
113 7 22 11
20 14 27 9
41-42 63-64 10
116 54 23
12 55-56
Low Priority Exons and Annealing Temperature
Annealing
Temperature56◦ 58◦ 59◦ 60◦ 61◦ 62◦ 63◦ 65◦
Exons 28-31 88-89 18 47-48 8 16 1
98-99 25 43 100-102 39-40 65-66
15 57-60
24
96-97
32-33
71
23

3 Materials and methods
Table 3.10: Reaction mixture for PCR
Substance Vol (µl)
H2O 28,3
Buffer (x10) 5
dNTP (2,5mM) 4
Primer up (20µM) 1,25
Primer do (20µM) 1,25
HS Taq (5U/µl) 0,2
DNA (10ng/µl) 10
Final volume 50
Table 3.11: PCR and sequencing conditions
Name 2PCR(TD)a 5PCR(TD)a Seqb Seqc PCRd
1. Initial denaturation 2min 94◦C 5min 94◦C 95◦C 1min - -
2. Denaturation 94◦C 30s 94◦C 45s 95◦C 20s 96◦C 10s 94◦C 45s
3. Annealing (AT) 30s (AT) 45s (AT) 15s (AT) 5s (AT) 45s
4. Elongation 70◦C 30s 70◦C 45s 60◦C 1min 60◦C 3min 72◦C 45s
Number of cycles (2. - 4.) 35 40 25 25 40
5. Final elongation 70◦C 10min 70◦C 10min - - 72◦C 10min
AT: annealing temperaturea 2PCR, 2PCRTD, 5PCR and 5PCRTD for PCR from gDNA, (TD: touch down conditions, first five cycles AT+5◦C)The programme 2PCR was used for all exons except for exons: 11, 41-42, 47-48, 57-60, 79, 86-87, 111-112, 114-115, 117 (programme 2PCRTDused); 1, 13, 100-102 (programme 5PCR used); 12, 43, 67-68, 74-75, 75-76 (programme 5PCRTD used).b Sequencing reaction for Megabace 500 (Amersham) sequencerc Sequencing reaction for ABI prism 3100 (ABI) sequencer, rapid thermal ramp is 1◦C/sd PCR from cDNA touch down conditions (first five cycles AT+5◦C)
24

3 Materials and methods
3.3.3 Agarose gel electrophoresis
2% agarose TBE-buffer gels, stained with 0,5% ethidiumbromide, were used to evaluate PCRproducts. 0,5 cm slots were loaded with 5 µl PCR product and 3 µl DNA sample buffer or 2,5 µlReady load 100 bp DNA ladder (Invitrogen), respectively. Gels were run at 100 V for 45 min,visualized and documented using a digital documentation system (Intas GDS).
3.3.4 DNA sequencing
Before sequencing, PCR products were purified either with the QIAquick PCR purification kit(Qiagen) according to the manufacturer’s protocol, or using the polymeric gel Biogel P100 (Bio-rad) in Millipore multiscreen 96 well filter plates, to eliminate undesired side products and un-used dNTPs. To prepare the Millipore filter plates, each well was loaded with 400 µl of BiogelP100 (Biorad) and fixed on a 96 well plate. The plates were then centrifuged at 1100 rpm for3 min. The flow through was discarded. The Millipore multiscreen filter plates, containing theBiogel P100, were then fixed on new sterile 96 well plates. They were now ready for loading ofthe PCR products. After loading the PCR products to the wells, the plates were centrifuged at1100 rpm for 4 min. The purified PCR products were obtained in the sterile 96 well plates, theMillipore filter plates were discarded. The DNA concentration of PCR products was measuredby spectrophotometry.
For the sequencing reaction either upstream primers, for forward sequencing, or downstreamprimers, for reverse sequencing, were used. The primers used were the same as for PCR (exceptexons 73-75, cf. 3.1.8). For the composition of the reaction mix see Table 3.12. The sequencingreactions were carried out in the same thermal cyclers as the PCR, the reaction conditions weredifferent for the two different sequencers used (Megabace 500 or ABI prism 3100) and are listedin Table 3.11.
The products of the sequencing reactions were purified either with the DyEx 2.0 spin kit (Qiagen)according to the manufacturer’s protocol or using the polymeric gel Sephadex G50 (Amersham)in Millipore multiscreen 96 well filter plates. In this case the procedure was the same as forpurifying PCR products, using Sephadex G50 (Amersham) instead of Biogel P100 (Biorad).The centrifugation steps were carried out at 1500 rpm instead of 1100 rpm.
The obtained samples were then submitted to automated sequencing in a Megabace 500 or ABIprism 3100 sequencer. The sequencers delivered raw-data, that were stored digitally. Throughbase calling of the raw-data, DNA electropherogram sequences were obtained.
25

3 Materials and methods
Table 3.12: Reaction mix for sequencing of PCR products
Megabace 500 Vol (µl) ABI prism 3100 Vol (µl)
PCR product x (30-50ng) PCR product x (30-50ng)
Primer up/do (5µM) 1 Primer up/do (5µM) 1
DMSO (50%) - DMSO (50%) 1
ET mix 3 Big dye 1.1 1
H2O ad 15 H2O ad 10
Final volume 15 Final volume 10
In the beginning of this study, DNA electropherogram sequences were compared to the referencesequence from the NCBI Entrez Nucleotide database [61] manually, either on printout or usingstandard sequence alignment software. To improve the efficiency of the protocol, automatedmutation detection software was tested and later used routinely (cf. 3.6).
3.3.5 Restriction enzyme digestion
To confirm sequence variants by a second method, restriction enzyme (RE) digestion was per-formed wherever possible. The database Webcutter [70] was used to find out whether the variantwould lead to new or eliminate existing cutting sites. RE digestion was performed in a finalvolume of 20 µl with up to 500 ng of DNA according to the manufacturer’s protocols. DigestedPCR products were analyzed by agarose gel electrophoresis.
In case of novel mutations, 124 normal control chromosomes were analyzed [23].
3.3.6 RNA isolation
Total RNA was extracted from a confluent 75 cm2 keratinocyte culture with Perfect RNA Eu-karyotic Mini kit (Eppendorf) or QiAmp RNA blood mini kit (Qiagen) according to the manu-facturers’ protocols. RNA concentrations and OD260/280 ratios were determined spectrophoto-metrically.
26

3 Materials and methods
Table 3.13: Primers for PCR from cDNA
Exons cDNA-Primers Product size (bp)
2-4 5-TGACCTGCACGCGCCTTTACG-3
5-CCACAGCAAATAGCTTGACCCC-3
400
25-27 5-GCCACTCAAGACAATGCTCA-3
5-TCTGGCCCTTTGGACAATAC-3
586
67-71 5-AGCTCCTGGTATCCTTGGACC-3
5-TTCTCCTTTCTCTCCCCGTT-3
571
94-101 5-TTGGGTTCCCGGGTCAGACAGG-3
5-CATGTCCCCCTTGGCACCCCGT-3
400
Table 3.14: Reaction mixture for PCR from cDNA
Substance Vol (µl)
H2O ad 50
Buffer x10 5
dNTP (2,5mM) 4
Primer up (20µM) 1,25
Primer do (20µM) 1,25
DMSO (100%) 2
Genaxxon HS Taq (5U/µl) 0,2
cDNA 2,5-10
Final volume 50
3.3.7 RT-PCR
Reverse transcription was performed with the Advantage RT-for-PCR Kit (BD Biosciences) with0,5µg of total RNA, using oligo dT primers, according to the manufacturer’s protocol. Primersfor the regions of interest were designed with Web primer [69] or Primer3 [63] (Table 3.13). Forreaction mix and PCR conditions see Table 3.14 and Table 3.11.
RT-PCR products were analyzed by agarose gel electrophoresis (cf. 3.3.3). In case of multiplebands, e.g. from aberrant splicing products, distinct bands were cut from the agarose gel. Then,cDNA was extracted with the QiAQuick Gel extraction kit (Qiagen), according to the manufac-turer’s protocol, and submitted to direct sequencing (cf. 3.3.4).
27

3 Materials and methods
3.4 In situ and in vitro characterization of procollagen
VII/collagen VII
3.4.1 Indirect immunofluorescence of skin cryosections
Skin biopsies were frozen in liquid nitrogen. 2-4 µm cryosections were incubated at RT with50 µl of the chosen first antibody (dilution cf. 3.1.5) over night in a wet chamber. Then they werewashed 5x4min with TBS. The incubation time with 50 µl of the respective second antibody was30 min - 2 h at RT. Afterwards the cryosections were again washed 5x4 min with TBS and driedcarefully. For supplementary nuclear staining with propidium iodide (dilution 1:50-1:100), thecryosections were incubated with the reagent for 1 min in a wet chamber, then washed 4x5 minwith TBS and dried carefully. As a final step, the slides were mounted in Mowiol and dried at4◦C for 30 min, then stored at -20◦C.
Cryosections were visualized with confocal laser scanning microscopy (Zeiss LSM510, 30 mWargon laser at 488 nm) or digital immunofluorescence microscopy (Zeiss Axiophot) and storeddigitally.
3.4.2 Cell culture
Skin biopsies were transported in DMEM containing 20 mM Hepes (ICN Biomedicals) and1% Antibiotic-Antimycotic (Invitrogen). Subcutaneous tissue and the dermis were removed.The sample was rinsed 3-4 times with PBS (Invitrogen) containing 8% Antibiotic-Antimycotic.Thereafter it was incubated at 37◦C in 30 ml Trypsin-EDTA (Invitrogen) 0,05/0,02% (w/v) inPBS until the epidermis had loosened from dermis remnants (15-30 min). Enzymatic digestionwas stopped with 10 ml PBS containing 10% FCS (Seromed). The released cells were cen-trifuged in a 50 ml Falcon tube for 10 min at 1000 rpm. The pellet was suspended in 7 mlKGM (Invitrogen). 1-2 million cells were plated in one 25 cm2 flask and incubated at 37◦C and5% CO2. The medium was changed the next day and thereafter every 2-3 days.
Subconfluent cultures were passaged. The medium was discarded and the cells were washedtwice with PBS. 1-2 ml Trypsin-EDTA 0,05/0,02% (w/v) in PBS were added per 25 cm2 flask.After the detachment of cells, trypsinization was stopped with PBS containing 10% FCS. 10 mlcell suspension were centrifuged 10 min at 1000 rpm. The pellet was resuspended in KGM,0,5 - 1mio cells were plated in one 25 cm2 flask.
Before freezing, cells were trypsinized and centrifuged as for passaging. The cell pellet obtained
28

3 Materials and methods
from a 25 cm2 flask was suspended in 400 µl DMEM, containing 20 mM Hepes, 1% Antibiotic-Antimycotic, 10% FCS and 10% DMSO, and stored in liquid nitrogen. Cells frozen in liquidnitrogen were thawed and directly cultivated in fresh KGM in 25 cm2 flasks or 6 well plates asdescribed above.
3.4.3 Indirect immunofluorescence of cultured keratinocytes
Keratinocytes were cultivated on cover slips in six well plates using 2 ml of medium per well.50 µM ascorbic acid was added to stimulate collagen synthesis and, 48 h later the medium wasdiscarded. Cells were washed twice with PBS, then fixed 15 min in methanol at -20◦C. After dry-ing 5-10 min at room temperature the cover slips were fixed to object holders with Eukitt. Theywere finally dried 30 min at -20◦C. Immunofluorescence staining was performed as described in3.4.1 with 60 µl of first and 100 µl of second antibody solution.
3.5 Protein biochemistry
3.5.1 Protein extraction from keratinocytes
To a 25 cm2 keratinocytes culture 50 µM ascorbic acid was added 48 h before harvesting for hy-droxylation of the collagenous domain. After discarding the medium, the cell layer was washedon ice three times with 10 ml cold PBS. 330 µl of complete protein extraction buffer (cf. 3.1.3)where added and the flask gently rocked for 30 min at 4◦C. The flask cover was mechanicallyremoved and the cell layer immediately collected with a scraper and pipetted in 1,5 ml tubes.After 30 min of centrifugation at 14000rpm at 4◦C the supernatant was aliquoted and stored at-80◦C.
3.5.2 Determination of protein concentration
The protein concentration in cell extracts was determined with the Dc-Proteinassay (Biorad)according to the manufacturer’s protocol. Optical density at 620nm was measured on an ELISA-reader (Ascent Multiskan software) against a double BSA standard calibration curve.
29

3 Materials and methods
Table 3.15: SDS-polyacrylamide gel compositions
Separation gels 4,5% µl 7,5% µl 15% µl
H2O 2100 3815 875
Separation buffer 875 1875 875
Acrylamide 525 1810 1750
TEMED 1,8 7,5 1,8
APS (10%) 8,8 75 8,8
Stacking gel 4,5% µl
H2O 1800
Stacking buffer 750
Acrylamide 450
TEMED 9
APS (10%) 20
3.5.3 SDS polyacrylamide gel electrophoresis and immunoblotting
Proteins were precipitated with ethanol as follows: 1:2:3 volumes of cell extract , TBS and100% EtOH over night at -20◦C. The samples were then centrifuged for 20 min at 13000 rpm at4◦C and afterwards washed with 70% ethanol. The supernatant was discarded and the obtainedpellets dissolved in 40 µl BSB. The samples were heated 3 min to 95◦C prior to loading 5 µl perslot on the SDS polyacrylamide gel. As a marker, 3 µl Dual Color Precision Plus Protein Standard(Biorad) were loaded on the gel. The following mini SDS polyacrylamide gel concentrationswere used: 4,5%-15% gradient or 7,5% separation gels and 4,5% stacking gels (Table 3.15).Gels were run 30 min at 10 mA, then 2 h at 25 mA.
The electrotransfer of proteins from gel to a nitrocellulose membrane was performed for 2 hat 300 mA. For immunoblotting, the nitrocellulose membrane was blocked with 2% milk-TBSfor 30 min. The membrane was incubated over night with the chosen first antibody diluted inmilk-TBS (cf. 3.1.5). After washing 5x4 min with milk-TBS the second antibody (also dilutedin milk-TBS) incubation time was 2 h. For detection by alkaline phosphatase, the membranewas washed 3x4 min with TBS and 2x4 min with buffer 3 (cf. 3.1.3). Then it was incubated1-20 min with NBT/X-phosphate solution in the dark (66 µl NBT and 33 µl X-phosphate dilutedin 10 ml buffer 3). The reaction was stopped by washing with TBS and drying. For detectionby chemiluminescence substrate, the membrane was washed 5x4min with TBS. The lumi lightwestern blotting substrate (Roche) was used according to the manufacturer’s protocol.
30

3 Materials and methods
Table 3.16: Online tools and databases
Tool Application Accession Web link
(cf. Bibliog-
raphy)
Online Mendelian Inheritance in Man database
(OMIM)
Epidermolysis bullosa phenotype *120120 [61]
NCBI Entrez Nucleotide COL7A1 cDNA NM_000094 [61]
COL7A1 gDNA L23982 [61]
NCBI Entrez Gene COL7A1 gene, links COL7A1 [61]
Human Gene Mutation Database Cardiff COL7A1 mutations COL7A1 [59]
Swiss-Prot/TrEMBL Collagen VII protein CA17 HUMAN [68]
Webcutter Restriction enzyme database - [70]
Webprimer Primer design - [69]
Primer3 Primer design - [63]
Pole Bioinformatique Lyonnais (Network Protein
Sequence Analysis)
Protein secondary structure predic-
tion
- [62]
PSIPRED Protein secondary structure predic-
tion
- [64]
3.5.4 Limited pepsin-trypsin digestion
Pepsin digests the N- and C-terminal domains of procollagen VII, therefore the triple helicaldomain can be obtained. 200 µl of protein extract were calibrated to pH 2.5 with 2 µl glacialacetic acid. They were then treated with 2 µl of 1 mg/ml pepsin (Sigma, in 0,1 M acetic acid)for 2 h at 4◦C. To stop the reaction the pH was recalibrated to 8 by adding 80 µl of 1 M Tris(unbuffered).
To determine the helix-to-coil transition temperature, the samples were then heated to 30◦-45◦C(2◦C steps) for 2 min in a thermal gradient cycler. Afterwards they were treated with 0,57 U/mltrypsin (Serva) for 2 min at room temperature. This reaction was stopped by adding 15 µg/mlsoybean trypsin inhibitor (Sigma) [6][29]. Samples were then analyzed by immunoblotting.
3.6 Bioinformatics
The online tools and databases used are listed in Table 3.16. Due to the large amount of dataproduced by sequencing 118 exons - 36 kb of COL7A1 it was necessary to find more efficient
31

3 Materials and methods
ways to analyze and store sequence data. To evaluate how existing IT technologies could beintegrated in COL7A1 mutation detection three commercial programs Mutation Surveyor [65],SecScape 2.1.1 [57], SequencePilot [60] and one Open Source project Staden Package [67] weretested in detail. Criteria applied were sensitivity (mutations found/all mutations in analyzeddata), specificity, accuracy (type of mutation, position, exons vs. introns, splitting of heterozy-gous in/del mutations), possibility to export data, creation of customized reports, total cost ofownership and ease of use.
This document was created with LATEX/LYX typesetting and BibTEX/Pybliographic referencemanager under SuSE Linux 9.11.
32

4 Results
4.1 COL7A1 mutations and their consequences
4.1.1 Clinical features
All 29 patients in this study (Table 4.1) presented with mechanobullous lesions of the skin andscarring since birth. Based on the pedigree, 26 patients had recessive dystrophic EB (RDEB) withthe parents clinically unaffected. Twelve patients had Hallopeau-Siemens RDEB (HS-RDEB)based on clinical assessment or negative immunofluorescence for collagen VII. In six patients,Hallopeau-Siemens RDEB could not be excluded due to their young age. They were thereforeclassified as RDEB-not specified. Three patients exhibited dominant dystrophic EB (DDEB).
4.1.2 Indirect immunofluorescence
IIF was performed in 22 out of 29 patients. In four cases no biopsy or data from cooperating cen-ters were available. In three cases we decided not to take another skin biopsy because electronmicroscopy had shown anchoring fibrils to be reduced. IIF was the most important diagnostictool to distinguish DEB from other EB forms. It also allowed a fast first prognosis for the patient:DDEB correlated well with positive or reduced collagen VII stainings, non HS-RDEB with re-duced collagen VII levels. In all HS-RDEB cases collagen VII staining was absent. NeverthelessIIF is not always perfectly specific or free of artefacts. The quality of the skin cryosections playsan important role. Furthermore IIF diagnosis needs professional experience, even though muchless than the assessment of electron microscopy of the skin.
4.1.3 Mutation survey
By direct sequencing we identified both disease causing mutations in 22 RDEB patients and onemutation in 4 RDEB patients. In all three DDEB patients, one mutation was found (Table 4.1).
33

4 Results
31 different mutations were identified: six insertion/deletions, eight nonsense mutations, 12 mis-sense mutations and five splice site mutations (Table 4.2). A list of COL7A1 polymorphisms isprovided in Table 4.3, twelve of them were identified in this study. One exonic polymorphismfound in this study, 3605G>A, R1202H in exon 27 was present among normal controls, one6696C>A, P2232P was silent. The other ten polymorphisms found in this study were intronic.
Our mutation detection strategy had a very high sensitivity of 92,7% (Table 4.4). The most laborintensive part of our protocol was analysis of the sequences. We were able to reduce the workloadsignificantly with the software Mutation Surveyor [65]. This program was chosen because it hadthe best sensitivity of all tested programs as compared to manual printout sequence analysis. Itwas also the most convenient to use. The improvement of efficiency by this software justifiedits relatively high price. With our present strategy, the entire COL7A1 gene could be screenedwithin less than one week.
4.1.4 Novel and recurrent COL7A1 mutations
We found three novel insertion/deletions, 62dupT, 1474del11 and 5944_5945delGGinsTA lead-ing to frameshift and PTC and two novel nonsense mutations, Q2170X and R2261X. Fur-thermore, 10 novel missense mutations were disclosed (G1492R, G1522R, G1525R, G1616R,G2034E, E2059G, G2413E, G2689R, G2737R). All except E2059G were glycine substitutionsand situated within the triple helical region. They lead to reduced levels of collagen VII in theskin, as shown with IF staining. Three novel splice site mutations were disclosed. The mutation426+1g>a in intron 3 lead to out-of-frame exon skipping or insertion of an intron. The muta-tion 3550+2t>g in intron 26 lead to activation of a cryptic splice site and in-frame deletion of13 amino acids. This was shown with RT-PCR of keratinocyte mRNA and direct sequencingof transcripts. Mutation 4899+1g>a in intron 51 replaces the consensus +1g of the donor splicesite, potentially leading to exon skipping or activation of cryptic splice sites. Verification was notpossible because keratinocytes were not available.
The non population specific, frequent splice site mutation 425A>G was disclosed in 11% ofalleles of unrelated individuals, the nonsense mutation R1933X in 7% of alleles. In patients withorigins in the Middle East the nonsense mutation R578X was recurrent (Table 4.2).
34

4 Results
Table 4.1: Phenotypes and genotypes of families analyzed
Collagen VII
Patient no. Diagnosisa Proteinb Exon(s) Mutation 1 Mutation 2 Consequences
1 non HS-RDEB +/- 73 E2059G E2059G Missense/missense
2 nonHS-RDEB +/- 80/109 6527insC G2689R PTC/missense
3 nonHS-RDEB +/- In26 3550+2t>g 3550+2t>g in frame deletion
4 nonHS-RDEB +/- 4/42 497dupA G1492R PTC/missense
5 nonHS-RDEB +/- 51 G1616R G1616R Missense/missense
6 nonHS-RDEB +/- 103/95 G2575R 7344G>A Missense/PTC
7 nonHS-RDEB +/- 51/73 R1632X E2059G PTC/missense
8 nonHS-RDEB AF+/- 45 G1522R ND Missense
9 RDEB NA 3/61 425A>G G1782V PTC/missense
10 RDEB +/- 1 62dupT ND PTC/ND
11 RDEB +/- 110 G2737R ND PTC/ND
12 RDEB +/- 70 R1933X ND PTC/ND
13 RDEB NA 3/94 425A>G G2413E PTC/missense
14c RDEB AF+/- 72 5944_5945delGGinsTA 5944_5945delGGinsTA PTC/PTC
15c HS-RDEB AF+/- 80 Q2170X Q2170X PTC/PTC
16 HS-RDEB - 13 R578X R578X PTC/PTC
17 HS-RDEB - 70 R1933X R1933X PTC/PTC
18 HS-RDEB - 3/34 425A>G R1343X PTC/PTC
19 HS-RDEB - 3 425A>G 425A>G PTC/PTC
20 HS-RDEB - In3/11 426+1g>a 1474del11 PTC/PTC
21 HS-RDEB - 38/70 4249delG R1933X (de novo) PTC/PTC
22 HS-RDEB - 3/86 425A>G R2261X PTC/PTC
23 HS-RDEB - 105 R2610X R2610X PTC/PTC
24c HS-RDEB - 5 R185X R185X PTC/PTC
25c HS-RDEB - 13 R578X R578X PTC/PTC
26 HS-RDEB NA 4/In51 497dupA 4899+1g>a PTC/PTC
27 DDEB NA 73 G2034E (de novo) Missense
28 DDEB + 75 G2076D Missense
29 DDEB +/- 45 G1525R Missense
NA: not available; ND: not determinedaHS-RDEB: Hallopeau-Siemens recessive DEB; nonHS-RDEB non Hallopeau-Siemens recessive DEB RDEB recessive dystrophic EB notspecified; DDEB dominant DEBbIndirect immunofluorescence: + present, +/- reduced, - absent; Electron microscopy: AF+/- anchoring fibrils reducedcDNA-based prenatal diagnosis in patients family performed
35

4 Results
Table 4.2: Mutations found in this study
cDNA Protein Ex/In Diagnosis Frequency References
Insertion/deletion
62dupT PTC Ex 1 RDEB 1 this study
497dupA PTC Ex 4 RDEB 2 [21]
1474del11 PTC Ex 11 RDEB 1 this study
4249delG PTC Ex 38 RDEB 1 [20]
5944_5945delGGinsTA PTC Ex 72 RDEB 2 this study
6527insC PTC Ex 80 RDEB 1 [40]
Nonsense mutations
553C>T R185X Ex 5 RDEB 2 [40]
1732C>T R578X Ex 13 RDEB 4 [28]
4027C>T R1343X Ex 34 RDEB 1 [39]
4894C>T R1632X Ex 51 RDEB 1 [85]
5797C>T R1933X Ex 70 RDEB 4 [85]
6508C>T Q2170X Ex 80 RDEB 2 this study
6781C>T R2261X Ex 86 RDEB 1 this study
7828C>T R2610X Ex 105 RDEB 2 [40]
Missense mutations
4474G>A G1492R Ex 42 RDEB 1 this study
4564G>C G1522R Ex 45 DDEB 1 this study
4573G>A G1525R Ex 45 DDEB 1 this study
4846G>A G1616R Ex 51 RDEB 2 this study
5345G>T G1782V Ex 61 RDEB 1 this study
6101G>A G2034E Ex 73 DDEB 1 this study
6176A>G E2059G Ex 73 RDEB 3 this study
6227G>A G2076D Ex 75 DDEB 1 [47]
7238G>A G2413E Ex94 RDEB 1 this study
7723G>A G2575R Ex 103 RDEB 1 [79]
8065G>A G2689R Ex 109 RDEB 1 this study
8209G>C G2737R Ex 110 RDEB 1 this study
Splice site mutations
425A>G PTC Ex 3 RDEB 6 [32]
426+1g>a PTC In 3 RDEB 1 this study
3550+2t>g in frame deletion In 26 RDEB 2 this study
4899+1g>a PTC In51 RDEB 1 this study
7344G>A PTC Ex 95 RDEB 1 [32]
36

4 Results
Table 4.3: Polymorphisms in COL7A1
cDNA Protein Ex/In
1 54G>C A18A Ex 1
2 1639 G>T V547L Ex 13
3 1639C>T P595L Ex 14
4 2314+15g>a In 17
5 2678C>A A893E Ex 20
6 2710+34t>g In 20
7 2817G>A P939P Ex 21
8 2992-12c>t In 22
9 3139+12a>g In 23
10 3148C>T R1050C Ex 24
11 3359G>A R1120K Ex 25
12* 3605G>A R1202H Ex 27
13 3723+9g>a In 27
14 3830C>T P1277L Ex 30
15 3975+39cc/c In 32
16* 4047+38a>c In 34
17* 4199-60c>t In 36
18* 4199-99a>g In 36
19* 4224+29g>t In 37
20* 4518+14t>a In 43
21 4613G>A R1538H Ex 46
22 4818+18a>t In 50
23 4899+27t>c In 51
cDNA Protein Ex/In
24 5086C>T R1696C Ex 55
25 5097+117a>g In 55
26* 5388+138c>t In 61
27* 5459C>G P1820R Ex 63
28 5518G>C Ex 64
29* 5590G>A A1864T Ex 66
30 5923G>A E1975K Ex 72
31 6188G>A R2063Q Ex 74
32 6279+25c>t In 75
33 6618+21a>g In 82
34 6653C>G G2218G Ex 84
35* 6696C>A P2232P Ex 84
36* 6937-17c>a In 88
37 7286C>T P2429L Ex 95
38 7382-15c>a In 96
39 7381+29t>c In 96
40 7759-98c>a In 103
41 7984-7ins/del In 107
42 8045+30c>t In 108
43 8304+34c>t In 111
44 8305-20g>c In 111
45* 8620+26g>a In 116
46 8997C>T Ex 118
*identified in this study
37

4 Results
Table 4.4: Summary of the 28 families analyzed in this study
MutationsMutation type Number of published mutations Novel mutations in this studyInsertion/deletion 72 3
Nonsense 36 2
Missense 89 10
Splice site 37 3
Regulatory 1
Total 235 18AllelesTotal analyzed Mutation found in Novel mutation found in55* 51 24
*52 alleles from 26 RDEB patients and 3 alleles from 3 DDEB patients
Sensitivity 92,7%Rate novel mutations (Alleles) 47%
38

4 Results
4.2 Interesting constellations and genotype-phenotype
correlations
Several patients in this study had interesting novel mutations and/or unusual genotype-phenotypeconstellations. Therefore, we also performed further functional studies on RNA and proteinlevel. In the following, their clinical presentation, in vivo and in situ findings, genetic findingsand studies on RNA and protein level will be presented, to allow further understanding of theirconstellations and enhance the understanding of genotype-phenotype correlations.
4.2.1 Patient 20: Three mutations or a polymorphism?
Patient 20 was a 22 year old male, first child of non-consanguineous unaffected parents of Ger-man origin. His cousin was also affected by RDEB. The patient’s sister was unaffected (Figure4.1). Onset of the disease was at birth. Clinical diagnosis was HS-RDEB, based on synechia andcontractures of both hands, generalized blistering and extensive scarring. He also suffered fromoral and esophageal blistering (Figure 4.2). IIF of the skin showed blister formation with colla-gen IV and other DEJZ markers staining at the blister roof. Collagen VII staining was negative(Figure 4.3).
The first mutation disclosed in the patient was a novel splice site mutation 426+1g>a. RT-PCRof patient’s keratinocyte mRNA and direct sequencing of the distinct bands showed that themutation led to two aberrant transcripts: one skipping exon three and one including intron 3.Both aberrant transcripts led to downstream PTCs (Figure 4.4). The second sequence variantfound in the patient was 4373C>T, P1458L in exon 40. It was absent among 144 chromosomesof the control population. It created a new restriction enzyme site for Sty I. The mother washeterozygous carrier of the sequence variant. On protein level, secondary structure predictionindicated significant change of the protein’s secondary structure from coil to sheet (Figure 4.5),arguing against a polymorphism. Unexpectedly, a third sequence aberration, 1474del11 in exon11, was found by sequencing of the entire gene. It was the second disease-causing mutation inthis patient, because it leads to a frameshift and PTC upstream of the sequence variant 4373C>T,P1458L. It abolished a restriction enzyme site for Bal I (Figure 4.6). Again, the mother washeterozygous carrier of the mutation. In accordance with the mutations leading to PTCs in earlyexons (Figure 4.7) and antigen mapping, immunoblotting showed that the patient’s keratinocytesdid not produce procollagen VII (Figure 4.8).
39

4 Results
Figure 4.1: Pedigree of Patient 20. Patient 20 (arrow) was the first child of non-consanguineous unaf-fected parents of German origin. His cousin was also affected by RDEB. The patient’s sisterwas unaffected
A B C
Figure 4.2: Patient 20 presented clinically with HS-RDEB. A: Synechia and contractures of the lefthand; B: Generalized blistering and extensive scarring, e.g. on the shoulder with ulcerations;C: The patient presented with carious teeth and microstomia and also suffered from oral andesophageal blistering.
A B C D
Figure 4.3: Absence of collagen VII staining in IIF of the skin of patient 20. A, C: IIF of normalskin shows linear staining of collagen IV (A) and VII (C) at the dermal-epidermal junction;B: IIF of the skin of patient 20 showed blister formation with collagen IV (CIV-22 antibody)staining at the blister roof; D: Collagen VII staining (a-VII-aff antibody) was absent. *:Blister cavity, D: Dermis, E: Epidermis.
40

4 Results
A B
C
Figure 4.4: Novel splice site mutation 426+1g>a in Patient 20. A: Patient 20 was heterozygous (blackarrow) for the novel splice site mutation 426+1g>a in intron 3. B: RT-PCR of patient’skeratinocyte mRNA lead to three distinct bands (red arrows) in agarose gel electrophoresis.C: Direct sequencing of the three distinct bands from RT-PCR showed that the mutation ledto two aberrant transcripts: one skipping exon three and one including intron 3. Both aberranttranscripts led to downstream PTCs. One normal transcript resulted from the normal allele.NC: Normal control
41

4 Results
A B
C
Figure 4.5: Sequence variant 4373C>T, P1458L, disease causing in patient 20? A: The second se-quence variant found in patient 20 (black arrow) was 4373C>T, P1458L in exon 40; B: Itcreated a new restriction enzyme site for Sty I. The normal control PCR product of 377bp(NC) was not cleaved. StyI digestion of the patient’s PCR product (*) produced 2 additionalfragments of 171 and 206 bp. The mother was heterozygous carrier of the sequence variant,which was absent among 144 control chromosomes a (data not shown). C: On protein level,secondary structure prediction indicated significant change from coil to sheet (red arrow),also arguing against a polymorphism [62].
42

4 Results
A B
Figure 4.6: The deletion 1474del11 was the second disease causing mutation in patient 20. A: Thethird sequence aberration (arrow) in patient 20 was the deletion 1474del11 in exon 11. It wasthe second disease-causing mutation in this patient, because it leads to a frameshift and PTCupstream of the sequence variant 4373C>T, P1458L (Figure 4.5). B: The deletion 1474del11abolished a restriction enzyme site for BalI. BalI RE digestion cleaved the normal controlPCR product (NC) into 2 fragments of 186 and 98bp. In patient 20 (*) and his mother anadditional non cleaved 273bp band from the mutated allele was visible. Therefore the variantP1458L and the upstream deletion 1474del11 had been inherited in cis from the mother.
Figure 4.7: Positions of mutations in patient 20. Mutations are indicated in a schematic procollagenVII α1 chain: the patient was heterozygous for the paternal splice site mutation 426+1g>a inintron 3 (blue), for the maternal mutation 1474 del11 in exon11 and for the maternal sequencevariant P1458L in exon 40 (red). Numbers: Amino acid postitions
43

4 Results
Figure 4.8: Patient 20’s keratinocytes were devoid of procollagen VII. In agreement with the hypoth-esis that PTC causing mutations in early exons lead to the absence of the gene product, noprocollagen VII (PCVII) was found by immunoblotting of patient 20’s keratinocyte extracts(*, left lane), in contrast to NHK extracts (right lane). A 4,5%-15% SDS polyacrylamidegel under denaturating conditions was used to separate proteins. NC2-10 was used as firstantibody. The total protein concentration in both samples was equal.
44

4 Results
4.2.2 Patient 21: First case of de novo mutation in RDEB
Patient 21 was a 17 year old girl, second child of non-consanguineous unaffected parents ofGerman origin with no family history of EB. The older brother was not affected. The mother’sthird pregnancy was terminated by induced abortion, the forth pregnancy resulted in spontaneousabortion of twins. The fifth pregnancy resulted in an unaffected girl (Figure 4.9). In the indexpatient, onset of the disease was at birth. Clinical diagnosis was HS-RDEB with mild synechiaand contracture of both hands, generalized blistering and extensive scarring (Figure 4.10). Thepatient also had occasional oral and esophageal blistering. Altogether the clinical manifestationwas less severe than in patient 20. IIF of the skin showed dermal-epidermal separation withcollagen IV and other DEJZ markers staining at the blister roof. Collagen VII staining wasnegative (Figure 4.11).
The first mutation found was 4249delG in exon 38, a previously known mutation. It created a newrestriction enzyme site for HypC4V (Figure 4.12). Mother and sister were heterozygous carriersof the mutation. The second mutation was R1933X, which is recurrent. The father was not carrierof the mutation. Haplotype analysis had been performed by A.M. Christiano (DebRA MolecularDiagnostics Laboratory, Department of Dermatology and Cutaneous Biology, Jefferson MedicalCollege, Thomas Jefferson University, Philadelphia) in 1994 in the context of prenatal diagnosisof the fifth pregnancy, since mutations had not been detected in the index patient at the time. Theunborn inherited the same haplotypes as the index patient; therefore it was assumed that it wouldbe affected by RDEB. In the meantime, EM studies of a fetal skin biopsy showed the unborn tobe unaffected. The family decided to carry out the pregnancy and an unaffected child was born.These data show that R1933X was a de novo mutation, resulting from three eventualities: eithera singular de novo event or germline mosaicism in the father, or somatic mosaicism in the indexpatient. By direct sequencing we demonstrated that the mutation was present in the patient’sleukocyte and buccal swab gDNA and keratinocyte mRNA. These results argue against somaticmosaicism in the patient and for a singular de novo event or germline mosaicism in the father. Asthe family did not wish any further children, we were not able to perform analysis of the father’ssperm (Figures 4.13 and 4.14).
Both mutations resulted in PTCs in gene regions corresponding to the protein’s triple helicalregion (Figure 4.15). In concert with antigen mapping and electron microscopy, no procollagenVII was found by immunoblotting of the patient’s keratinocyte extracts (Figure 4.16).
45

4 Results
Figure 4.9: Pedigree of Patient 21. The patient (arrow) was the second child of non-consanguineousunaffected parents of German origin with no family history of EB. The older brother wasnot affected. The mother’s third pregnancy was terminated by induced abortion, the forthpregnancy resulted in spontaneous abortion of twins. The fifth pregnancy resulted in anunaffected girl.
A B C D
Figure 4.10: Clinical diagnosis of patient 21 was HS-RDEB. A: She presented with mild synechiaand contracture of both hands; B: Generalized blistering and erosions, here on the back; C:Extensive scarring, here on the left elbow; D: Toe nail loss. She also showed occasionaloral and esophageal blistering. Altogether, the clinical manifestation was less severe than inpatient 20.
A B C D
Figure 4.11: IIF of the skin of patient 21 showed dermal-epidermal separation. A, C: IIF of normalskin shows linear staining of collagen IV (A) and VII (C) at the dermal-epidermal junction;B: In IIF of the skin of patient 21 collagen IV (CIV-22 antibody) and other DEJZ markersstained at the blister roof; C: Collagen VII staining (a-VII-aff antibody) was absent. Thenuclei were stained red with propidium iodide for better contrast. *: Blister cavity, D:Dermis, E: Epidermis
46

4 Results
A B
Figure 4.12: Deletion 4249delG in Patient 21. A: Patient 21 was heterozygous for 4249delG (arrow)in exon 38. B: The mutation created a new restriction enzyme site for HypC4V (B). In thenormal control (NC), father and older brother the PCR product size was 422 bp. The PCRproduct of patient 21 (*), her mother and her younger sister was additionally cleaved in twofragments of 341 and 81bp (not visible on the gel). Thus, they were heterozygous carriersof the mutation (+).
A B
Figure 4.13: The mutation 5797C>T, R1933X in patient 21. A: Patient 21 was heterozygous for therecurrent nonsense mutation 5797C>T, R1933X (arrow) in exon 70. It was present neither inthe father nor any other family member. B: PCR or RT-PCR from gDNA or mRNA, derivedfrom cells with origins in different embryonic layers, showed that the mutation 5797C>T(arrows) was present in patient’s leukocyte gDNA, keratinocyte mRNA and mucosal gDNA(buccal swab) arguing against somatic mosaicism.
47

4 Results
Figure 4.14: First case of de novo mutation in RDEB: 5797C>T, R1933X in patient 21. Haplotypeanalysis of the patient (arrow) and family members had been performed in the context ofprenatal diagnosis of the mother’s fifth pregnancy, since mutations had not been detectedin the index patient at the time. The unborn inherited the same haplotypes as the indexpatient (red and white: maternal alleles, gray and blue: paternal alleles, +: mutation ormarker present, -: mutation or marker absent); therefore it was assumed that it would beaffected by RDEB. In the meantime, EM studies of a fetal skin biopsy showed the unbornto be unaffected. The family decided to carry out the pregnancy and an unaffected childwas born. These data show that R1933X (highlighted in the father’s allele) was a de novomutation. Mutations 4249delG and R1933X were added to the original analysis.
Figure 4.15: Positions of mutations in patient 21. Mutations are indicated in a schematic procollagenVII α1 chain: the patient was heterozygous for the maternal deletion 4249delG in exon 38(red) and for the de novo nonsense mutation R1933X in exon 70 (blue). Numbers: Aminoacid positions
48

4 Results
Figure 4.16: Patient 21’s keratinocytes were lacking procollagen VII. No procollagen VII (PCVII)was found by immunoblotting of patient 21’s keratinocyte extracts (*, left lane) in contrastto NHK extracts (right lane). A 4,5%-15% SDS polyacrylamide gel under denaturatingconditions was used to separate proteins. NC2-10 was used as first antibody. The totalprotein concentration in both samples was equal.
49

4 Results
4.2.3 Patients 1 and 7: Novel glutamic acid to glycine substitution
The 52 year old patient 1 was a cousin of the mother of patient 7, who was 5 years old. Bothpatients were offspring of unaffected unrelated parents of German origin. No other cases of EBwere known in the family (Figure 4.17). Clinical diagnosis of patient 1 was non-HS RDEB.Onset of the disease was shortly after birth. He had episodic strong blistering. Hands showednail loss, minor synechia and mild flexion contracture. He had oral blistering, gum bleedingand carious teeth (Figure 4.18 A-C). Patient 7 also had non-HS RDEB. Onset of the disease wasat birth with continuous spontaneous blistering, oral and esophageal involvement (Figure 4.18D,E). In both patients IIF of the skin revealed reduced collagen VII staining (Figure 4.19). IIFof cultured keratinocytes from patient 7 showed reduced procollagen VII staining compared toNHKs (Figure 4.20).
Patient 1 was a homozygous carrier of the novel glutamic acid to glycine substitution E2059G inthe gene region corresponding to the the triple helical region of collagen VII (Figure 4.21). Themutation was not present in 150 normal alleles of a German control population. Patient 7 washeterozygous for the maternal mutation E2059G and for the paternal nonsense mutation R1632Xin exon 51 (data not shown). Therefore it is predicted that patient 7 is functionally homozygous
and all his procollagen VII contains the E2059G mutation.
Immunoblotting of keratinocyte extracts of patient 7 showed reduced levels of procollagen VIIas detected with antibodies against the NC-1 and NC-2 regions. The less sensitive antibodyagainst the triple helical region of collagen VII did not show any signal (Figure 4.22). Lim-ited pepsin-trypsin digestion of procollagen VII from keratinocyte extracts of patient 7 did notshow significant changes of the helix-to-coil transition temperature (data not shown). Secondarystructure predictions of mutated and normal procollagen VII showed no significant changes.
50

4 Results
Figure 4.17: Pedigree of patients 1 and 7. The 52 year old patient 1 (arrow) was a cousin of themother of patient 7 (arrow), who was 5 years old. Both patients were offspring of unaffectedunrelated parents of German origin. No other cases of RDEB were known in the family.
A B C
D E
Figure 4.18: The clinical diagnosis of patients 1 and 7 was non-HS RDEB. A: Patient 1 presentedwith episodic strong blistering, e.g. on the elbow. B, C: Hands showed nail loss, minorsynechia and mild flexion contracture. He also had oral blistering, gum bleeding and cariousteeth (not shown). D, E: Patient 7 presented with continuous spontaneous blistering, oraland esophageal involvement.
51

4 Results
A B C D
Figure 4.19: Reduced levels of collagen VII in the skin of patients 1 and 7. A, C: IIF of normalskin shows linear staining of collagen VII (LH 7.2 antibody). B: In patient 1 IIF of theskin revealed reduced collagen VII staining at the blister roof. D: In patient 7, the IIF alsorevealed reduced collagen VII staining, the skin cryosection showed no blister formation.Nuclei were stained red with propidium iodide for better contrast (C, D). *: Blister cavity,D: Dermis, E: Epidermis
A B C
D E F
Figure 4.20: Reduced levels of intracellular procollagen VII in keratinocytes from patient 7. IIFof cultured keratinocytes of a normal control (A-C) and patient 7 (D-F). The cells of patient7 exhibited a reduced intracellular IIF signal. Secreted collagen VII can not be visualized,since it diffuses into the culture medium. Different first antibodies were used; A, D: NC1-F3 antibody against the N-terminal part of procollagen VII; B, E: a-VII-aff antibody againstthe triple helical part of procollagen VII; C, F: NC2-10 antibody against the C-terminal partof procollagen VII (C, F).
52

4 Results
Figure 4.21: The novel glutamic acid to glycine substitution E2059G. Patient 1 was a homozygouscarrier of the novel glutamic acid to glycine substitution E2059G (arrow) in the gene re-gion corresponding to the the triple helical region of collagen VII. The mutation was absentamong 150 control alleles (not shown). Patient 7 was heterozygous for the maternal mu-tation E2059G and for the paternal nonsense mutation R1632X in exon 51 (not shown).Therefore it is predicted that patient 7 is functionally homozygous and all his procollagenVII contains the E2059G mutation.
A B C
Figure 4.22: Reduced levels of procollagen VII in keratinocyte extracts of patient 7. A: Im-munoblotting of keratinocyte extracts of patient 7 (*, right lane) showed reduced levelsof procollagen VII (PCVII), compared to NHK extracts (left lane) as detected with an an-tibody against the NC-1 domain. B: The less sensitive antibody against the triple helicalregion of collagen VII did not show any signal (*, right lane). C: Also with an antibodyagainst the NC-2 domain reduced levels of procollagen VII were detected in extracts of thepatient (*, right lane). A 4,5%-15% SDS polyacrylamide gel under denaturating conditionswas used to separate proteins. The total protein concentration in all samples was equal.
53

4 Results
4.2.4 Patient 2: Glycine substitution with predominantly mucosal
involvement
Patient 2 was a 52 year-old male, first child of non-consanguineous unaffected parents of Germanorigin. He had a younger brother who was also affected with EB. His two children were unaf-fected and there were no other cases of EB known in the family (Figure 4.23). Clinically he hada very mild nonHS-RDEB. Onset of the disease was at birth. He had localized oral, esophagealand anal blistering. Even after mechanical friction he did not develop blisters at hands and feet(Figure 4.24). His brother had similar clinical manifestations. Antigen mapping showed reducedcollagen VII staining at the blister roof (Figure 4.25). IIF of patient’s keratinocytes revealed nodifference of procollagen VII staining compared to NHKs (Figure 4.26).
Mutation detection disclosed a novel heterozygous glycine substitution G2689R in exon 109,corresponding to the very end of the triple helical region (Figure 4.27). The second mutation wasthe insertion 6527insC in exon 80, which is known to lead to a PTC. Therefore, it is predictedthat patient 2 is functionally homozygous and all produced procollagen VII carries the G2689Rmutation.
Immunoblotting of keratinocyte extract showed normal signals for procollagen VII with anti-bodies against NC-1, triple helical and NC-2 domains (Figure 4.28). Limited pepsin-trypsindigestion revealed that the helix-to-coil transition temperature of procollagen VII from patient 2was reduced to 33-35◦C. The helix-to-coil transition temperature of procollagen VII from NHKextracts was 39-41◦C (Figure 4.29).
Figure 4.23: Pedigree of Patient 2. The 52 year-old male (arrow), first child of non-consanguineousunaffected parents of German origin, presented with RDEB. His younger brother was alsoaffected with EB. His two children were unaffected and there were no other cases of EBknown in the family.
54

4 Results
A B
Figure 4.24: Patient 2 presented with a very mild nonHS-RDEB. A, B: Extramucosal manifestationwas limited to partial toe nail loss and nail dystrophy. He showed localized oral, esophagealand anal blistering. Even after mechanical friction he did not develop blisters at hands andfeet.
A B
Figure 4.25: Reduced levels of collagen VII in the skin of patient 2. A: IIF of normal human skinshowed no blister formation and linear staining of collagen VII (LH7.2 antibody). B: IIFof the skin of patient 2 revealed reduced collagen VII staining at the blister roof. *: Blistercavity, D: Dermis, E: Epidermis
55

4 Results
A B C
D E F
Figure 4.26: Normal levels of intracellular procollagen VII in patient 2’s keratinocytes. IIF ofcultured keratinocytes of a normal control (A-C) and patient 2 (D-F). The cells of patient2 exhibited a normal intracellular IF signal. Secreted collagen VII can not be visualized,since it diffuses into the culture medium. Different first antibodies were used; A, D: NC1-F3 antibody against the N-terminal part of procollagen VII; B,E: a-VII-aff antibody againstthe triple helical part of procollagen VII; C, F: NC2-10 antibody against the C-terminal partof procollagen VII.
Figure 4.27: The glycine substitution G2689R in patient 2. The patient was heterozygous for theglycine substitution G2689R in exon 109 (arrow), corresponding to the very end of the triplehelical region. G2689R was absent among 102 control chromosomes (data not shown). Thesecond mutation was the insertion 6527insC in exon 80, which is known to lead to a PTC(data not shown). Therefore, it is predicted that patient 2 is functionally homozygous and allproduced procollagen VII carries the G2689R mutation.
56

4 Results
A B C
Figure 4.28: Normal levels of procollagen VII in keratinocyte extracts of patient 2. Immunoblottingof patient 2 keratinocyte extracts (*, right lanes) showed normal signals for procollagen VII(PCVII), compared to NHK extracts (left lanes). Different first antibodies were used; A:antibody against the NC-1 domain; B: antibody against the triple helical domain; C: anti-body against the NC-2 domain. A 4,5%-15% SDS polyacrylamide gel under denaturatingconditions was used to separate proteins. The total protein concentration in all samples wasequal.
Figure 4.29: The glycine substitution G2689R leads to reduced stability of the triple helix of colla-gen VII. Limited pepsin-trypsin digestion revealed that the helix-to-coil transition tem-perature (Tm) of procollagen VII from patient 2 (*, lower lane) was reduced to 33-35◦C.The helix-to-coil transition temperature of procollagen VII from NHK extracts was 39-41◦C(upper lane). By limited pepsin digestion of the globular N- and C-terminal domains of pro-collagen VII, the triple helical region was obtained. To test their thermal stability sampleswere then heated to the indicated temperatures for 2 min 40s, followed by limited trypsin di-gestion. The helix-to-coil transition temperature is the temperature where 50% of the triplehelix were digested. A 7,5% SDS polyacrylamide gel under denaturating conditions wasused to separate proteins. LH7,2 was used as first antibody. NT: control not digested withtrypsin. Temperatures are rounded.
57

4 Results
4.2.5 Patient 19: RDEB in child and Klinefelter’s syndrome in father
Patient 19 was a one year old child of unrelated parents of Serbian origin. There were no othercases of EB known in the family. The father had Klinefelter’s syndrome. The pregnancy was in-duced by IVF through intracytoplasmatic sperm injection, after hormone treatment and testicularbiopsy of the father.
The patient had HS-RDEB with onset at birth, generalized blistering and extensive scarring.Synechia developed already at the age of one month. Antigen mapping was negative for collagenVII with all other DEJZ markers staining at the blister roof. Mutation detection revealed the childbeing homozygous for the recurrent splice site mutation 425A>G in exon 3.
58

5 Discussion
Mutation detection strategy
Detection of COL7A1 mutations by the ”priority strategy” and direct sequencing turned out tobe more efficient, reliable and, with over 90%, more sensitive than other approaches. Already inthe exons on the ”high priority” plate we identified most mutations (over 70% mutant alleles).In contrast, the recently tested PTT had a sensitivity of 58% in COL7A1 screening and fl-CCMof 81% [85]. Until now, routinely used techniques were CSGE [33][51] with a sensitivity ofabout 75% [19][85] and dHPLC [77]. Furthermore these protocols could not identify all types ofmutations [85] which is improved by our strategy. Direct sequencing even reveals most intronicpolymorphisms. In the initiating phases of this study, varying quality of electropherogram se-quences led to unsatisfactory results. Especially heterozygous mutations and insertion-deletionswere hard to disclose. This fact, and the possibility of undetected regulatory or splice site muta-tions, could explain why the sensitivity of our strategy in this cohort is not 100%. By changingthe automated sequencer we eliminated the problem of varying sequence quality, and the imple-mentation of sophisticated software tools allowed us to significantly improve the efficiency of theprotocol. The software dramatically reduced the workload of sequence-to-sequence comparison,so far the bottleneck of mutation detection by direct sequencing. Taken together, best sensitiv-ity, reliability, possibility of identifying all types of mutations, reduced workload and, recently,decreasing costs, our strategy turns out to be of high value for mutation screening in COL7A1.
Genetic conclusions
We performed molecular analysis of 29 DEB patients. 31 different mutations were identified,18 of which had not been reported before. We found the mutation in 51 of 55 alleles expected(sensitivity of 92,7%). In 24 of those alleles - a rate of 47% - the mutation was novel (Table4.4). Thus, even ten years after the DEB causing gene was identified, the detection rate of novel
59

5 Discussion
mutations remains constantly high. It has not changed significantly in mutation detection studiespublished in recent years [85][33]. These data contribute to the expanding Epidermolysis bullosamutation database [82][59] and imply that we still have to expect many novel mutations in thefuture, and that mutation detection in COL7A1 will have to be continued to get a more completepicture of the broad range of mutations underlying DEB.
Of the 51 mutated alleles identified, eight were insertion/deletions, 17 nonsense mutations, 15missense mutations and 11 splice site mutations. As in previous studies, mutations were dis-tributed over the entire COL7A1 gene (Table 4.2) [85][33]. In 10 RDEB patients both mutationswere identified, and we showed that these individuals were compound heterozygous. These ob-servations confirm the heterogeneity of mutations underlying DEB.
The splice site mutation 425A>G was the most frequent mutation found in this study (11% ofalleles). The mutation has been identified as a worldwide recurrent mutation [26][55]. Thissuggests that the donor splice site of exon 3 is a gene region with high mutational frequency.The finding of the novel splice site mutation 426+1g>a in this study supports this suggestion.The nonsense mutation R1933X in exon 70 was also recurrent and, interestingly, in one Germanpatient this mutation had arisen de novo (see below). As such an event occurs rarely in recessivediseases [80], this is an argument against a common founder mutation and and speaks for amutational hotspot, which is supported by the fact that the mutation is a transition at a CpGdinucleotide. One explanation why R1933X was not found more frequently in previous studiescould be that the commonly used CSGE is less sensitive for it. In this study we could not detectthe clustering of mutations in exon 73 described in previous reports [54][33]. This could, at leastin parts, be explained by the composition of our cohort of patients. Previous reports includedmore DDEB and mild RDEB patients. In those groups mutations in exon 73 seem more frequent.
Three novel splice site mutations 426+1g>a, 3550+2t>g and 4899+1g>a were disclosed in thisstudy. The mutation 426+1g>a leads to out-of-frame exon skipping or intron insertion causingdownstream PTCs. In combination with another PTC causing mutation the consequence is HS-RDEB (patient 20). In contrast, the mutation 3550+2t>g leads to activation of a cryptic splicesite and in-frame deletion of 13 amino acids. In homozygous state it correlates with a less severephenotype (patient 3). Effects of presumable splice site mutations can now be predicted fromgDNA sequences [58][66], also in COL7A1 [84]. Nevertheless, investigations on RNA levelshould be performed wherever possible to avoid inaccurate conclusions.
Patient 20 was affected by HS-RDEB. After identifying the splice site mutation 426+1g>a wefound a second sequence variant 4374C>T, P1458L. It was not found in 144 control chromo-somes of the same population and secondary structure prediction suggested alterations, arguing
60

5 Discussion
against a polymorphism. Proline substitutions have been rarely described in RDEB, but not inHS-RDEB. Therefore, we continued sequencing and found a third mutation, 1474del11 causinga PTC, that correlated well with the absence of protein and the severe phenotype. The variant4374C>T, P1458L and the deletion 1474del11 had been inherited in cis from the mother. Inthis allele the upstream PTC causing deletion 1474del11 might lead to silencing of the possibledominant negative effects of P1458L [80]. If the carrier, e.g. the mother of patient 20, is het-erozygous with a normal second allele, only normal collagen VII is produced. This case shows,that sequencing of the entire COL7A1 gene is necessary to rule out that sequence variants arepolymorphisms or mutations that are not disease causing. In mild DEB cases distinguishingpolymorphisms from mutations can remain difficult.
Recently Pfendner et al have reported their experience with prenatal diagnosis for EB [77]. Ofthe 144 cases described, only two remained unresolved. One of the two was the younger sister ofpatient 21. In her case prenatal diagnosis had been performed by haplotype analysis, since muta-tions of patient 21 had not been detected at the time. The unborn inherited the same haplotypesas the affected offspring; therefore it was assumed that it would be affected by RDEB. As EMstudies of a fetal skin biopsy showed the unborn to be unaffected, the family decided to carry outthe pregnancy, and an unaffected child was born. In this study we have disclosed both mutationsof patient 21, the maternal deletion 4249delG and the nonsense mutation R1933X. As R1933Xwas not present in the father and the younger sister, it is a de novo mutation (Figure 4.14). Thisexplains the at the time contradictory findings of haplotype analysis and EM studies of fetal skinbiopsy. To our knowledge this is the first case of a de novo mutation described in recessive DEB.In general de novo mutations are rarely disclosed in recessive diseases [80]. The patient had noclinical signs of somatic mosaicism. By direct sequencing we could show that the mutation waspresent in patient’s leukocyte and buccal swab gDNA and keratinocyte mRNA. These resultsargue against somatic mosaicism in the patient and for a germline mosaicism in the father or asingular de novo mutation event (Figure 4.13). Recently a case of maternal germ line mosaicismin dominant DEB has been described [25]. In junctional EB somatic mosaicism for a mutationin COL17A1 and parental germline mosaicism in LAMB3 have been described [44][24]. Thesefindings imply that prenatal diagnosis should be performed by determination of mutation carrierstatus from CVS. This technique is the most reliable and has the least side effects. Thereforemutation detection in DEB patients is indispensable in families who wish further children andconsider prenatal diagnosis. Concerning genetic counseling in EB families, unusual modes ofinheritance should be taken into consideration [90].
Notably, in several families subject to this study, distant relatives were affected by RDEB, driving
61

5 Discussion
attention to population carrier risks of EB. Recently the RDEB carrier frequency in the US hasbeen established to be 1/345 [76]. To allow accurate genetic counseling of RDEB families,carrier frequencies also have to be established in other populations.
DEB is a rare, but in many cases devastating disease. As medical treatment remains insufficient,families frequently ask for genetic counseling, prenatal diagnosis and the prognosis of their child.Furthermore the DEB causing mutations might be relevant for choosing suitable candidates forgene therapy in the near future. Therefore mutation detection remains an irreplaceable tool indiagnostics and prevention of DEB.
Genotype-phenotype correlations
The data reported in this study are in agreement with genotype-phenotype correlations reportedso far [42] (cf. introduction). In brief, all DDEB forms were caused by glycine substitutionsin the triple helical region. The nonHS-RDEB subtypes were caused by missense mutations,combination of missense mutation and PTC or, in one case, in frame deletion of 13 amino acids.All patients with assured HS-RDEB had two PTC causing mutations.
Whereas these general rules of genotype-phenotype correlations in DEB are now well estab-lished, exceptions to the rules exist, and mechanisms leading to the observed correlations stillhave to be fully elucidated. Comparing patients 20 and 21 (cf. sections 4.2.1 and 4.2.2), in thefirst, PTCs leading to protein truncation are situated much closer to the N-terminus. Yet bothpatients are collagen VII negative, as shown with IIF of the skin and immunoblotting. Thesefindings conform to a recently published report that the position of a PTC in COL7A1 alone doesnot correlate with the clinical severity of RDEB [41]. In our case the absence of protein mightwell be explained by nonsense-mediated mRNA decay [50][37], also found in DEB [17], or de-cay of truncated protein. Nevertheless, the difference of clinical manifestations in patient 20 and21 is noteworthy. Patient 20 suffers from severe HS-RDEB with mutilations of the hands, thatdeveloped early in life, generalized severe blistering and chronic ulcerations. Patient 21 has onlymild synechia and contractures of the hands, and large areas of the body are rarely affected byblistering. As both patients are collagen VII negative, the question arrises whether other factorsthan collagen VII might contribute to the DEB phenotype, e.g. environmental influences.
The unusual novel glutamic acid to glycine substitution E2059G in exon 73 was present in pa-tients 1 and 7 (cf. section 4.2.3). It correlated with a rather mild clinical phenotype. The amountof collagen VII in the skin was reduced as shown with IIF. Recently Chen et al. have shown ina study of recombinantly generated full-length type VII collagen, that the mutation R2008G in
62

5 Discussion
exon 73 caused intracellular accumulation of collagen VII [15]. Three other COL7A1 mutationsG2006D, G2034R, and G2015E within exon 73, close to the hinge region, have been shown tointerfere with protein folding and lead to accumulation of collagen VII in the cells [35]. Thismechanism can be excluded for E2059G since cultured keratinocytes showed no intracellular ac-cumulation but reduced levels of collagen VII staining by immunofluorescence. Immunoblottingof keratinocyte extracts also showed reduced levels of the protein. However, neither secondarystructure prediction for the altered protein nor limited pepsin-trypsin digestion showed differenceto the normal control. The mechanisms that lead to reduced production or increased decay ofproduced protein within the cell remain elusive.
Collagen VII is a remarkable exception among collagens regarding glycine substitutions. Gen-erally, in collagenous domains, glycine is present in every third position to allow triple helixformation [4]. In collagen VII glycine substitutions are not only less frequent than in othercollagens [9]. Also, the assumption that the replacement of a small glycine residue within thetriple helical region by another, bulkier amino acid would lead to dominant negative interference[78] does not always apply for collagen VII. In DEB glycine substitutions may be inherited ina recessive manner, with heterozygote carriers being unaffected [21]. There is also no obviouscorrelation between position of the glycine substitution within the triple helical region and clin-ical phenotype [9]. Very recently Persikov et al. found that any glycine substitution in COL7A1
causes DEB, whereas in COL1A1, COL1A2, COL3A1 and COL4A5 the distribution of residuesreplacing glycine was significantly different from that expected [75]. In those collagens residuescausing a higher destabilization of the triple helix were overrepresented. In this study we identi-fied nine novel glycine substitutions in COL7A1, a relatively high number compared to previousstudies. Yet there is no obvious correlation between mutation position or replacing residues andmode of inheritance or severity of phenotype. Concerning mutation detection, careful clinicalassessment is necessary to determine the mode of inheritance. In some dominantly inheritedforms, affected family members present with only subtle nail dystrophy [27]. To distinguishde novo dominant mutations from recessive forms, mutation detection in family members is es-sential [51]. As DEB cases with combinations of recessive and dominant mutations have beendescribed [21][86][35], screening of the entire COL7A1 gene is essential.
Some glycine substitutions have now been characterized in more detail. The glycine substi-tution G2749R has been shown to cause abnormal and incomplete folding of recombinantlyproduced collagen VII and to decrease resistance to pepsin and trypsin digestion [15]. Britting-ham et al. have used truncated recombinantly produced procollagen VII variants to investigatehow G2575R, found in a patient with RDEB, and G2623C correlated with DDEB, affect inter-
63

5 Discussion
molecular interactions [5]. In contrast to G2575R, the mutation G2623C was shown to preventformation of dimers and inhibit assembly of anchoring fibrils. The authors postulate that thismight be due to the proximity of G2623C to a critical binding site for the NC-2 domain duringdimer formation. These results show that genotype-phenotype correlations are complex and un-derlying mechanisms are only beginning to emerge. Future studies, also with skin equivalentsand animal models will help to improve our knowledge about these basic processes.
Patient 2 had very mild nonHS-RDEB. Even after mechanical stress he did not present with skinblistering. The only signs of EB were nail dystrophy and mucosal involvement with localizedoral, esophageal and anal blistering. He was functionally homozygous for the glycine substi-tution G2689R in exon 109. Staining of cultured keratinocytes and immunoblotting revealedthat he produced normal amounts of procollagen VII. Significant reduction of the helix-to-coiltransition temperature, as shown with limited pepsin-trypsin digestion, implies instability of theprotein and might cause reduced levels of collagen VII in the skin as shown with IIF. Reductionof helix-to-coil transition temperature of the collagen VII triple helix is typical for glycine sub-stitutions [53]. In fact, mucosal involvement in DEB is common [30] but the condition of DEBwithout skin blistering and mucosal involvement has only been described once before [89]. Thispatient was functionally homozygous for the glycine substitution G2775S in exon 112. Thesecases demonstrate that rarely DEB might be a differential diagnosis to gastrointestinal disor-ders like Crohn’s disease. In both probands the glycine substitution is located in the very distalcarboxy-terminus of the triple helical domain. Probably they do not cause the same degree ofdestabilization as more central glycine substitutions close to the hinge region. Higher tempera-ture and enhanced mechanical stress compared to the epidermis are possible explanations whyfirst manifestations of mild DEB forms can be mucosal. Nevertheless, molecular mechanismsleading to mucosal, but not cutaneous fragility in DEB remain elusive.
In summary, we have established an efficient protocol for mutation detection in COL7A1 bydirect sequencing. So far, our approach is the most sensitive and reliable, allowing final diagnosisin DEB, reliable prenatal diagnosis and genetic counseling for the families. Among other findingswe revealed the first case of a de novo mutation in recessive DEB. Elucidation of the clinical,genetical and biological background of 29 DEB patients contributes to the EB mutation database,the understanding of the mechanisms underlying DEB and the biology of anchoring fibrils as anessential component of the DEJZ.
64

Bibliography
[1] M. Aumailley and P. Rousselle. 1999. Laminins of the dermo-epidermal junction. Matrix Biol, 18(1):19–28.
[2] H.P. Bachinger, N.P. Morris, G.P. Lunstrum, D.R. Keene, L.M. Rosenbaum, L.A. Compton, and R.E. Burgeson. 1990. The relationship ofthe biophysical and biochemical characteristics of type VII collagen to the function of anchoring fibrils. J Biol Chem, 265(17):10095–101.
[3] C. Baldeschi, Y. Gache, A. Rattenholl, P. Bouille, O. Danos, J.P. Ortonne, L. Bruckner-Tuderman, and G. Meneguzzi. 2003. Geneticcorrection of canine dystrophic epidermolysis bullosa mediated by retroviral vectors. Hum Mol Genet, 12(15):1897–905.
[4] J. Bella, M. Eaton, B. Brodsky, and H.M. Berman. 1994. Crystal and molecular structure of a collagen-like peptide at 1.9 A resolution.Science, 266(5182):75–81.
[5] R. Brittingham, M. Colombo, H. Ito, A. Steplewski, D.E. Birk, J. Uitto, and A. Fertala. 2005. Single amino acid substitutions in procollagenVII affect early stages of assembly of anchoring fibrils. J Biol Chem, 280(1):191–8.
[6] P. Bruckner and D.J. Prockop. 1981. Proteolytic enzymes as probes for the triple-helical conformation of procollagen. Anal Biochem,110(2):360–8.
[7] L. Bruckner-Tuderman. 2002. Epidermolysis Bullosa. In: "Connective Tissue and its Heritable Disorders. Molecular, Genetic and MedicalAspects", pages 689–725. (P.M. Royce, B. Steinmann, editors) Wiley-Liss, New York, 2nd edition.
[8] L. Bruckner-Tuderman. 2003. Basement Membranes. In: "Fitzpatrick’s Dermatology in General Medicine", chapter 16. (I.M. Freedberg,A.Z. Eisen, K. Wolff, F.K. Austen, L.A. Goldsmith, S.I. Katz, editors) McGraw-Hill, New York, 6th edition.
[9] L. Bruckner-Tuderman, B. Hopfner, and N. Hammami-Hauasli. 1999. Biology of anchoring fibrils: lessons from dystrophic epidermolysisbullosa. Matrix Biol, 18(1):43–54.
[10] L. Bruckner-Tuderman, Y. Mitsuhashi, U.W. Schnyder, and P. Bruckner. 1989. Anchoring fibrils and type VII collagen are absent fromskin in severe recessive dystrophic epidermolysis bullosa. J Invest Dermatol, 93(1):3–9.
[11] L. Bruckner-Tuderman, O. Nilssen, D.R. Zimmermann, M.T. Dours-Zimmermann, D.U. Kalinke, T. Gedde-Dahl, Jr, and J.O. Winberg.1995. Immunohistochemical and mutation analyses demonstrate that procollagen VII is processed to collagen VII through removal of theNC-2 domain. J Cell Biol, 131(2):551–9.
[12] L. Bruckner-Tuderman, S. Ruegger, B. Odermatt, Y. Mitsuhashi, and U.W. Schnyder. 1988. Lack of type VII collagen in unaffected skinof patients with severe recessive dystrophic epidermolysis bullosa. Dermatologica, 176(2):57–64.
[13] L. Bruckner-Tuderman, U.W. Schnyder, K.H. Winterhalter, and P. Bruckner. 1987. Tissue form of type VII collagen from human skin anddermal fibroblasts in culture. Eur J Biochem, 165(3):607–11.
[14] R.E. Burgeson. 1993. Type VII collagen, anchoring fibrils, and epidermolysis bullosa. J Invest Dermatol, 101(3):252–5.
[15] M. Chen, F.K. Costa, C.R. Lindvay, Y.P. Han, and D.T. Woodley. 2002. The recombinant expression of full-length type VII collagen andcharacterization of molecular mechanisms underlying dystrophic epidermolysis bullosa. J Biol Chem, 277(3):2118–24.
[16] M. Chen, N. Kasahara, D.R. Keene, L. Chan, W.K. Hoeffler, D. Finlay, M. Barcova, P.M. Cannon, C. Mazurek, and D.T. Woodley. 2002.Restoration of type VII collagen expression and function in dystrophic epidermolysis bullosa. Nat Genet, 32(4):670–5.
[17] A.M. Christiano, S. Amano, L.F. Eichenfield, R.E. Burgeson, and J. Uitto. 1997. Premature termination codon mutations in the type VIIcollagen gene in recessive dystrophic epidermolysis bullosa result in nonsense-mediated mRNA decay and absence of functional protein.J Invest Dermatol, 109(3):390–4.
65

Bibliography
[18] A.M. Christiano, G.G. Hoffman, L.C. Chung-Honet, S. Lee, W. Cheng, J. Uitto, and D.S. Greenspan. 1994. Structural organization of thehuman type VII collagen gene (COL7A1), composed of more exons than any previously characterized gene. Genomics, 21(1):169–79.
[19] A.M. Christiano, G.G. Hoffman, X. Zhang, Y. Xu, Y. Tamai, D.S. Greenspan, and J. Uitto. 1997. Strategy for identification of sequencevariants in COL7A1 and a novel 2-bp deletion mutation in recessive dystrophic epidermolysis bullosa. Hum Mutat, 10(5):408–14.
[20] A.M. Christiano, S. LaForgia, A.S. Paller, J. McGuire, H. Shimizu, and J. Uitto. 1996. Prenatal diagnosis for recessive dystrophicepidermolysis bullosa in 10 families by mutation and haplotype analysis in the type VII collagen gene (COL7A1). Mol Med, 2(1):59–76.
[21] A.M. Christiano, J.A. McGrath, K.C. Tan, and J. Uitto. 1996. Glycine substitutions in the triple-helical region of type VII collagen resultin a spectrum of dystrophic epidermolysis bullosa phenotypes and patterns of inheritance. Am J Hum Genet, 58(4):671–81.
[22] A.M. Christiano, J.A. McGrath, and J. Uitto. 1996. Influence of the second COL7A1 mutation in determining the phenotypic severity ofrecessive dystrophic epidermolysis bullosa. J Invest Dermatol, 106(4):766–70.
[23] J.S. Collins and C.E. Schwartz. 2002. Detecting Polymorphisms and Mutations in Candidate Genes. Am. J. Hum. Genet., 71:1251–1252.
[24] P.B. Cserhalmi-Friedman, K. Anyane-Yeboa, and A.M. Christiano. 2002. Paternal germline mosaicism in Herlitz junctional epidermolysisbullosa. Exp Dermatol, 11(5):468–70.
[25] P.B. Cserhalmi-Friedman, M.C. Garzon, E. Guzman, A. Martinez-Mir, W.K. Chung, K. Anyane-Yeboa, and A.M. Christiano. 2001.Maternal germline mosaicism in dominant dystrophic epidermolysis bullosa. J Invest Dermatol, 117(5):1327–8.
[26] M. Csikos, H.I. Szocs, A. Laszik, S. Mecklenbeck, A. Horvath, S. Karpati, and L. Bruckner-Tuderman. 2005. High frequency of the425A–>G splice-site mutation and novel mutations of the COL7A1 gene in central Europe: significance for future mutation detectionstrategies in dystrophic epidermolysis bullosa. Br J Dermatol, 152(5):879–86.
[27] B. Dharma, C. Moss, J.A. McGrath, J.E. Mellerio, and A. Ilchyshyn. 2001. Dominant dystrophic epidermolysis bullosa presenting asfamilial nail dystrophy. Clin Exp Dermatol, 26(1):93–6.
[28] M.G. Dunnill, A.J. Richards, G. Milana, F. Mollica, R.A. Eady, and F.M. Pope. 1994. A novel homozygous point mutation in the collagenVII gene (COL7A1) in two cousins with recessive dystrophic epidermolysis bullosa. Hum Mol Genet, 3(9):1693–4.
[29] J. Engel and D.J. Prockop. 1991. The zipper-like folding of collagen triple helices and the effects of mutations that disrupt the zipper.Annu Rev Biophys Biophys Chem, 20:137–52.
[30] JD. Fine, EA. Bauer, J. McGuire, and A. Moshell, editors. 1999. Epidermolysis Bullosa: Clinical, Epidemiologic and LaboratoryAdvances, and the Findings of the National Epidermolysis Bullosa Registry. Johns Hopkins University Press, Baltimore.
[31] J.D. Fine, R.A. Eady, E.A. Bauer, R.A. Briggaman, L. Bruckner-Tuderman, A. Christiano, A. Heagerty, H. Hintner, M.F. Jonkman,J. McGrath, J. McGuire, A. Moshell, H. Shimizu, G. Tadini, and J. Uitto. 2000. Revised classification system for inherited epidermolysisbullosa: Report of the Second International Consensus Meeting on diagnosis and classification of epidermolysis bullosa. J Am AcadDermatol, 42(6):1051–66.
[32] R. Gardella, L. Belletti, N. Zoppi, D. Marini, S. Barlati, and M. Colombi. 1996. Identification of two splicing mutations in the collagentype VII gene (COL7A1) of a patient affected by the localisata variant of recessive dystrophic epidermolysis bullosa. Am J Hum Genet,59(2):292–300.
[33] R. Gardella, D. Castiglia, P. Posteraro, S. Bernardini, N. Zoppi, M. Paradisi, G. Tadini, S. Barlati, J.A. McGrath, G. Zambruno, andM. Colombi. 2002. Genotype-phenotype correlation in italian patients with dystrophic epidermolysis bullosa. J Invest Dermatol,119(6):1456–62.
[34] B. Gayraud, B. Hopfner, A. Jassim, M. Aumailley, and L. Bruckner-Tuderman. 1997. Characterization of a 50-kDa component of epithelialbasement membranes using GDA-J/F3 monoclonal antibody. J Biol Chem, 272(14):9531–8.
[35] N. Hammami-Hauasli, H. Schumann, M. Raghunath, O. Kilgus, U. Luthi, T. Luger, and L. Bruckner-Tuderman. 1998. Some, but not all,glycine substitution mutations in COL7A1 result in intracellular accumulation of collagen VII, loss of anchoring fibrils, and skin blistering.J Biol Chem, 273(30):19228–34.
[36] C. Has, J.S. Kern, and L. Bruckner-Tuderman. 2004. [Hereditary blistering disorders]. Hautarzt, 55(10):920, 922–30.
[37] J.A. Holbrook, G. Neu-Yilik, M.W. Hentze, and A.E. Kulozik. 2004. Nonsense-mediated decay approaches the clinic. Nat Genet,36(8):801–8.
66

Bibliography
[38] A. Hovnanian, P. Duquesnoy, C. Blanchet-Bardon, R.G. Knowlton, S. Amselem, M. Lathrop, L. Dubertret, J. Uitto, and M. Goossens.1992. Genetic linkage of recessive dystrophic epidermolysis bullosa to the type VII collagen gene. J Clin Invest, 90(3):1032–6.
[39] A. Hovnanian, L. Hilal, C. Blanchet-Bardon, Y. de Prost, A.M. Christiano, J. Uitto, and M. Goossens. 1994. Recurrent nonsense mutationswithin the type VII collagen gene in patients with severe recessive dystrophic epidermolysis bullosa. Am J Hum Genet, 55(2):289–96.
[40] A. Hovnanian, A. Rochat, C. Bodemer, E. Petit, C.A. Rivers, C. Prost, S. Fraitag, A.M. Christiano, J. Uitto, M. Lathrop, Y. Barrandon, andY. de Prost. 1997. Characterization of 18 new mutations in COL7A1 in recessive dystrophic epidermolysis bullosa provides evidence fordistinct molecular mechanisms underlying defective anchoring fibril formation. Am J Hum Genet, 61(3):599–610.
[41] A. Ishiko, T. Masunaga, T. Ota, and T. Nishikawa. 2004. Does the position of the premature termination codon in COL7A1 correlate withthe clinical severity in recessive dystrophic epidermolysis bullosa? Exp Dermatol, 13(4):229–33.
[42] A. Jarvikallio, L. Pulkkinen, and J. Uitto. 1997. Molecular basis of dystrophic epidermolysis bullosa: mutations in the type VII collagengene (COL7A1). Hum Mutat, 10(5):338–47.
[43] A. Jassim, O. Schofield, P. Whitehead, P. Purkis, A.H. Heagerty, J.A. Sachs, R.A. Eady, and I.M. Leigh. 1991. Detection of a novelbasement membrane antigen by GDA-J/F3 anti-human sperm fibrous sheath monoclonal antibody. Br J Dermatol, 125(2):101–7.
[44] M.F. Jonkman, H. Scheffer, R. Stulp, H.H. Pas, M. Nijenhuis, K. Heeres, K. Owaribe, L. Pulkkinen, and J. Uitto. 1997. Revertantmosaicism in epidermolysis bullosa caused by mitotic gene conversion. Cell, 88(4):543–51.
[45] P. Kahofer, L. Bruckner-Tuderman, D. Metze, H. Lemmink, H. Scheffer, and J. Smolle. 2003. Dystrophic epidermolysis bullosa inversawith COL7A1 mutations and absence of GDA-J/F3 protein. Pediatr Dermatol, 20(3):243–8.
[46] D.R. Keene, L.Y. Sakai, G.P. Lunstrum, N.P. Morris, and R.E. Burgeson. 1987. Type VII collagen forms an extended network of anchoringfibrils. J Cell Biol, 104(3):611–21.
[47] A. Kon, K. Nomura, L. Pulkkinen, D. Sawamura, I. Hashimoto, and J. Uitto. 1997. Novel glycine substitution mutations in COL7A1 revealthat the Pasini and Cockayne-Touraine variants of dominant dystrophic epidermolysis bullosa are allelic. J Invest Dermatol, 109(5):684–7.
[48] A. Kon, L. Pulkkinen, A. Ishida-Yamamoto, I. Hashimoto, and J. Uitto. 1998. Novel COL7A1 mutations in dystrophic forms of epider-molysis bullosa. J Invest Dermatol, 111(3):534–7.
[49] I.M. Leigh, P.E. Purkis, and L. Bruckner-Tuderman. 1987. LH-7.2 monoclonal antibody detects type VII collagen in the sub-lamina densazone of ectodermaly derived epithelia including skin. Epithelia, 1:17–29.
[50] J. Lykke-Andersen. 2004. Making structural sense of nonsense-mediated decay. Nat Struct Mol Biol, 11(4):305–6.
[51] R. Mallipeddi, O. Bleck, J.E. Mellerio, G.H. Ashton, R.A. Eady, and J.A. McGrath. 2003. Dilemmas in distinguishing between dominantand recessive forms of dystrophic epidermolysis bullosa. Br J Dermatol, 149(4):810–8.
[52] R. Mallipeddi, V. Wessagowit, A.P. South, A.M. Robson, G.E. Orchard, R.A. Eady, and J.A. McGrath. 2004. Reduced expressionof insulin-like growth factor-binding protein-3 (IGFBP-3) in Squamous cell carcinoma complicating recessive dystrophic epidermolysisbullosa. J Invest Dermatol, 122(5):1302–9.
[53] S. Mecklenbeck, S.H. Compton, J.E. Mejia, R. Cervini, A. Hovnanian, L. Bruckner-Tuderman, and Y. Barrandon. 2002. A microinjectedCOL7A1-PAC vector restores synthesis of intact procollagen VII in a dystrophic epidermolysis bullosa keratinocyte cell line. Hum GeneTher, 13(13):1655–62.
[54] S. Mecklenbeck, N. Hammami-Hauasli, B. Hopfner, H. Schumann, A. Kramer, W. Kuster, and L. Bruckner-Tuderman. 1999. Clustering ofCOL7A1 mutations in exon 73: implications for mutation analysis in dystrophic epidermolysis bullosa. J Invest Dermatol, 112(3):398–400.
[55] T. Murata, T. Masunaga, A. Ishiko, H. Shimizu, and T. Nishikawa. 2004. Differences in recurrent COL7A1 mutations in dystrophicepidermolysis bullosa: ethnic-specific and worldwide recurrent mutations. Arch Dermatol Res, 295(10):442–7.
[56] M.G. Nievers, R.Q. Schaapveld, and A. Sonnenberg. 1999. Biology and function of hemidesmosomes. Matrix Biol, 18(1):5–17.
[57] n.n. 2005. ABI PRISM SeqScape Software (Mutation detection software). www.appliedbiosystems.com.
[58] n.n. 2005. Automated splice site analysis. https://splice.cmh.edu.
[59] n.n. 2005. HGMD (Human Gene Mutation Database Cardiff). http://archive.uwcm.ac.uk/uwcm/mg/hgmd0.html.
67

Bibliography
[60] n.n. 2005. Jsi-medisys SequencePilot (Mutation analysis software). www.jsi-medisys.de.
[61] n.n. 2005. NCBI homepage. www.hcbi.nlm.nih.gov.
[62] n.n. 2005. Pole Bioinformatique Lyonnais (Network Protein Sequence Analysis). http://npsa-pbil.ibcp.fr.
[63] n.n. 2005. Primer3 (Primer design). http://frodo.wi.mit.edu/cgi-bin/primer3/primer3_www.cgi.
[64] n.n. 2005. PSIPRED (Protein structure prediction server). http://bioinf.cs.ucl.ac.uk/psipred/.
[65] n.n. 2005. Softgenetics Mutation Surveyor (DNA variant analysis software). www.softgenetics.com/ms/index.htm.
[66] n.n. 2005. Splice Site Presiction by Neural Network. www.fruitfly.org/seq_tools/splice.html.
[67] n.n. 2005. Staden Package (OpenSource) (Mutation analysis software). http://staden.sourceforge.net.
[68] n.n. 2005. Swiss-Prot/TrEMBL. http://us.expasy.org/sprot.
[69] n.n. 2005. Web Primer (Web based tool for primer design). http://seq.yeastgenome.org/cgi-bin/web-primer.
[70] n.n. 2005. Webcutter (Restriction enzyme database). http://rna.lundberg.gu.se/cutter2/.
[71] B.F. Odermatt, A.B. Lang, J.R. Ruttner, K.H. Winterhalter, and B. Trueb. 1984. Monclonal antibodies to human type IV collagen: usefulreagents to demonstrate the heterotrimeric nature of the molecule. Proc Natl Acad Sci USA, 81(23):7343–7.
[72] S. Ortiz-Urda, J. Garcia, C.L. Green, L. Chen, Q. Lin, D.P. Veitch, L.Y. Sakai, H. Lee, M.P. Marinkovich, and P.A. Khavari. 2005. TypeVII collagen is required for Ras-driven human epidermal tumorigenesis. Science, 307(5716):1773–6.
[73] S. Ortiz-Urda, Q. Lin, C.L. Green, D.R. Keene, M.P. Marinkovich, and P.A. Khavari. 2003. Injection of genetically engineered fibroblastscorrects regenerated human epidermolysis bullosa skin tissue. J Clin Invest, 111(2):251–5.
[74] S. Ortiz-Urda, B. Thyagarajan, D.R. Keene, Q. Lin, M. Fang, M.P. Calos, and P.A. Khavari. 2002. Stable nonviral genetic correction ofinherited human skin disease. Nat Med, 8(10):1166–70.
[75] A.V. Persikov, R.J. Pillitteri, P. Amin, U. Schwarze, P.H. Byers, and B. Brodsky. 2004. Stability related bias in residues replacing glycineswithin the collagen triple helix (Gly-Xaa-Yaa) in inherited connective tissue disorders. Hum Mutat, 24(4):330–7.
[76] E. Pfendner, J. Uitto, and J.D. Fine. 2001. Epidermolysis bullosa carrier frequencies in the US population. J Invest Dermatol, 116(3):483–4.
[77] E.G. Pfendner, A. Nakano, L. Pulkkinen, A.M. Christiano, and J. Uitto. 2003. Prenatal diagnosis for epidermolysis bullosa: a study of 144consecutive pregnancies at risk. Prenat Diagn, 23(6):447–56.
[78] D.J. Prockop and K.I. Kivirikko. 1995. Collagens: molecular biology, diseases, and potentials for therapy. Annu Rev Biochem, 64:403–34.
[79] H. Shimizu, J.A. McGrath, A.M. Christiano, T. Nishikawa, and J. Uitto. 1996. Molecular basis of recessive dystrophic epidermolysisbullosa: genotype/phenotype correlation in a case of moderate clinical severity. J Invest Dermatol, 106(1):119–24.
[80] T. Strachan and A.P. Read, editors. 2004. Human molecular genetics. Garland Science, New York, 3rd edition.
[81] M.J. Tidman and R.A. Eady. 1985. Evaluation of anchoring fibrils and other components of the dermal-epidermal junction in dystrophicepidermolysis bullosa by a quantitative ultrastructural technique. J Invest Dermatol, 84(5):374–7.
[82] J. Uitto. 2004. Epidermolysis bullosa: the expanding mutation database. J Invest Dermatol, 123(4):xii–xiii.
[83] J. Uitto, M. Ryynanen, A. M. Christiano, A. Hovnanian, R. Frantz, E. A. Bauer, and R. G. Knowlton. 1992. Genetic linkage of the typeVII collagen gene (COL7A1) to dominant dystrophic epidermolysis bullosa (DDEB) in families with abnormal anchoring fibrils. Clin.Res., 40(188A).
[84] V. Wessagowit, S.C. Kim, S. Woong Oh, and J.A. McGrath. 2005. Genotype-phenotype correlation in recessive dystrophic epidermolysisbullosa: when missense doesn’t make sense. J Invest Dermatol, 124(4):863–6.
[85] N.V. Whittock, G.H. Ashton, R. Mohammedi, J.E. Mellerio, C.G. Mathew, S.J. Abbs, R.A. Eady, and J.A. McGrath. 1999. Comparativemutation detection screening of the type VII collagen gene (COL7A1) using the protein truncation test, fluorescent chemical cleavage ofmismatch, and conformation sensitive gel electrophoresis. J Invest Dermatol, 113(4):673–86.
68

Bibliography
[86] J.O. Winberg, N. Hammami-Hauasli, O. Nilssen, I. Anton-Lamprecht, S.L. Naylor, K. Kerbacher, M. Zimmermann, P. Krajci, T. Gedde-Dahl, Jr, and L. Bruckner-Tuderman. 1997. Modulation of disease severity of dystrophic epidermolysis bullosa by a splice site mutationin combination with a missense mutation in the COL7A1 gene. Hum Mol Genet, 6(7):1125–35.
[87] D.T. Woodley, D.R. Keene, T. Atha, Y. Huang, K. Lipman, W. Li, and M. Chen. 2004. Injection of recombinant human type VII collagenrestores collagen function in dystrophic epidermolysis bullosa. Nat Med, 10(7):693–5.
[88] D.T. Woodley, D.R. Keene, T. Atha, Y. Huang, R. Ram, N. Kasahara, and M. Chen. 2004. Intradermal injection of lentiviral vectorscorrects regenerated human dystrophic epidermolysis bullosa skin tissue in vivo. Mol Ther, 10(2):318–26.
[89] K.P. Zimmer, H. Schumann, S. Mecklenbeck, and L. Bruckner-Tuderman. 2002. Esophageal stenosis in childhood: dystrophic epidermol-ysis bullosa without skin blistering due to collagen VII mutations. Gastroenterology, 122(1):220–5.
[90] J. Zlotogora. 2004. Parents of children with autosomal recessive diseases are not always carriers of the respective mutant alleles. HumGenet, 114(6):521–6.
69

Curriculum Vitae
Johannes S. Kern
Talstr. 5179102 [email protected]
PERSONAL DATA
Born 23rd September 1979In WürzburgNationality German
EDUCATION
Since 1999 Medical School, Freiburg, Germany9/2002 - 4/2003 Medical School, Grenoble, France8/2002 1. Teil der ärztlichen Prüfung8/2001 Ärztliche Vorprüfung1990 - 1999 Röntgen Gymnasium Würzburg1986 - 1990 Walther von der Vogelweide Grundschule Würzburg
DOCTORAL THESIS
8/2003 - 6/2005 In the Laboratory of Prof. Bruckner-Tuderman, Departmentof Dermatology, University of Freiburg
INTERNATIONAL EXPERIENCE
1/2005 Elective in the Department of Infectious Diseases, Univer-sity Hospital, Point-A-Pitre, Guadeloupe
9/2002 - 4/2003 Medical School, Grenoble, France3/2002 Elective in the Department of Internal Medicine, Spital Wil,
Switzerland
SCHOLARSHIP
since 6/2001 e-fellows.net scholarship (Deutsche Telekom, McKin-sey&Company, Verlagsgruppe Georg von Holtzbrinck)
70

Acknowledgements
I would like to express my deepest gratitude to Prof. L. Bruckner-Tuderman, for offering me thegreat opportunity to work in her laboratory; for a perfect introduction in the world of science; forcontinuous support; and for encouraging me to give my best throughout the work. Her toweringexample of an enthusiastic and energetic attitude towards science have been the best source ofmotivation.
I wish to express my warm thanks to Cristina Has, simply for being the best imaginable tutor;for teaching me the very basics of laboratory and scientific work; for being patient with me; forbeing there literally anytime; for answering innumerable questions and letting me participate inher concise and profound understanding of science; for never ending support; for pushing mewhen necessary and being a great motivator; for being critical; and for a splendid time.
I am greatly indebted to Gabi Grüninger for major assistance with mutation detection; MargitSchubert for cell work and introduction into the secrets of collagen VII western blotting; Bern-hard Kremer for helping me take the many confocal pictures; Käthe Thoma for help with thecryosections and Vera Morand, for sequencing work.
I wish to express my sincere thanks to Doris Höping, Hauke Schumann and Andreas Volz formedical attendance of the patients, for letting me participate in their work and helping me whennecessary.
I especially want to thank Claus Franzke for helpful discussion and valuable assistance withprotein biochemistry, as well as bioinformatics and protein secondary structure prediction.
I am deeply grateful to Marcel Müller for working with me on questions of computer assistedmutation detection, making the effort to become involved in our project, and for having a goodtime.
I owe my sincere thanks to the staff of the Molecular Dermatology lab: to Silke Hofmann, ElenaZimina, Vivien Schacht, Anja Fritsch, Corinna Baer and Ursula Voith, for fruitful discussions,for help in many ways in various little problems and for the good time we spent together.
I am greatly indebted to the patients and family members, who gave us the opportunity to carryout this study
I am deeply grateful to my precious friends, for supporting me, and for tolerating that I did nothave enough time for months.
Last but certainly not least I want to thank my family in the deepest way, my wonderful sisterLena, and my parents for making it all possible and giving me every imaginable support fromthe very beginning.
71