-
8/13/2019 endocrinesystem-121228084635-phpapp01
1/79
Under the guidance of:Dr. Sandeep
Tandon
Professor and Head of Dept. of Pedodontics
Dr. Ambika SinghRathore
Dr. Rinku Mathur
Dr .Shantanu Jain
Dr. Tripti Sharma Ra
1
-
8/13/2019 endocrinesystem-121228084635-phpapp01
2/79
CONTENT:
Introduction
Evolution of Endocrine system
Chemical characteristics of Hormones
Regulation of Hormone Release
Hypothalamus & its Hormone
Various glands and their importance
Disorders of Endocrine system common inChildren
References2
-
8/13/2019 endocrinesystem-121228084635-phpapp01
3/79
INTRODUCTION:
Constant internal environment
(i.e., homeostasis) should be maintained.
Two systems help ensure communication:
Rapid transmission Long-lasting regulatoryaction
Both systems interact: Stimuli from the nervoussystem can
influence the release of certain hormonesand vice versa.
NERVOUSSYSTEM
HORMONAL
Neuroendocrine
3
-
8/13/2019 endocrinesystem-121228084635-phpapp01
4/79
EVOLUTIONOFENDOCRINESYSTEM The nervous systemcoordinates rapid
and precise responses to
stimuli using action potentials.
The endocrine system maintains homeostasis and long-termcontrol
using chemical signals.
The most primitive endocrine systems seem to be those of
theneurosecretorytype, in which the nervous system either
secretesneurohormones directly into the circulation or stores them
inneurohemal organs (neurons whose endings directly contactblood
vessels, allowing neurohormones to be secreted into the
circulation), from which they are released in large amounts
asneeded.
True endocrine glands probably evolved later in the
evolutionaryhistory of the animal kingdom as separate,
hormone-secretingstructures.
4
http://www.emc.maricopa.edu/faculty/farabee/biobk/BioBookglossN.htmlhttp://www.emc.maricopa.edu/faculty/farabee/biobk/BioBookglossA.htmlhttp://www.emc.maricopa.edu/faculty/farabee/biobk/BioBookglossE.htmlhttp://www.emc.maricopa.edu/faculty/farabee/biobk/BioBookglossH.htmlhttp://www.britannica.com/EBchecked/topic/410737/neurosecretory-cellhttp://www.britannica.com/EBchecked/topic/410635/neurohormonehttp://www.britannica.com/EBchecked/topic/410631/neurohemal-organhttp://www.britannica.com/EBchecked/topic/69887/blood-vesselhttp://www.britannica.com/EBchecked/topic/69887/blood-vesselhttp://www.britannica.com/EBchecked/topic/69887/blood-vesselhttp://www.britannica.com/EBchecked/topic/69887/blood-vesselhttp://www.britannica.com/EBchecked/topic/410631/neurohemal-organhttp://www.britannica.com/EBchecked/topic/410631/neurohemal-organhttp://www.britannica.com/EBchecked/topic/410631/neurohemal-organhttp://www.britannica.com/EBchecked/topic/410635/neurohormonehttp://www.britannica.com/EBchecked/topic/410737/neurosecretory-cellhttp://www.emc.maricopa.edu/faculty/farabee/biobk/BioBookglossH.htmlhttp://www.emc.maricopa.edu/faculty/farabee/biobk/BioBookglossE.htmlhttp://www.emc.maricopa.edu/faculty/farabee/biobk/BioBookglossE.htmlhttp://www.emc.maricopa.edu/faculty/farabee/biobk/BioBookglossE.htmlhttp://www.emc.maricopa.edu/faculty/farabee/biobk/BioBookglossA.htmlhttp://www.emc.maricopa.edu/faculty/farabee/biobk/BioBookglossA.htmlhttp://www.emc.maricopa.edu/faculty/farabee/biobk/BioBookglossA.htmlhttp://www.emc.maricopa.edu/faculty/farabee/biobk/BioBookglossN.htmlhttp://www.emc.maricopa.edu/faculty/farabee/biobk/BioBookglossN.htmlhttp://www.emc.maricopa.edu/faculty/farabee/biobk/BioBookglossN.html
-
8/13/2019 endocrinesystem-121228084635-phpapp01
5/79
CONVERGENT EVOLUTION:
Similarities among the endocrine systems ofcrustaceans,
arthropods, and vertebrates.
The vertebrate endocrine system consists
of glands (pituitary, thyroid, adrenal), and
diffuse cell groups scattered in epithelial tissues.
Endocrine glands arise during development for all
threeembryologic tissue layers (endoderm, mesoderm,ectoderm).
The type of endocrine product is determined by whichtissue layer
a gland originated in.
Glands of ectodermal and endodermal origin: peptideand amine
hormones;
Mesodermal origin glands:hormones based on lipids. 5
http://www.emc.maricopa.edu/faculty/farabee/biobk/BioBookglossE.htmlhttp://www.emc.maricopa.edu/faculty/farabee/biobk/BioBookglossE.htmlhttp://www.emc.maricopa.edu/faculty/farabee/biobk/BioBookglossM.htmlhttp://www.emc.maricopa.edu/faculty/farabee/biobk/BioBookglossE.htmlhttp://www.emc.maricopa.edu/faculty/farabee/biobk/BioBookglossE.htmlhttp://www.emc.maricopa.edu/faculty/farabee/biobk/BioBookglossM.htmlhttp://www.emc.maricopa.edu/faculty/farabee/biobk/BioBookglossE.htmlhttp://www.emc.maricopa.edu/faculty/farabee/biobk/BioBookglossE.htmlhttp://www.emc.maricopa.edu/faculty/farabee/biobk/BioBookglossM.htmlhttp://www.emc.maricopa.edu/faculty/farabee/biobk/BioBookglossE.htmlhttp://www.emc.maricopa.edu/faculty/farabee/biobk/BioBookglossE.html
-
8/13/2019 endocrinesystem-121228084635-phpapp01
6/79
WHAT ARE HORMONES?????
( TOSPURON)
Hormones are molecules thatare produced by endocrine
glands:i. The hypothalamus,
ii. Pituitary gland,
iii. Adrenal glands,
iv. Gonads, (i.e., testes andovaries),
v. Thyroid gland,
vi. Parathyroid glands, and
vii. Pancreas6
-
8/13/2019 endocrinesystem-121228084635-phpapp01
7/79
The term endocrine implies that in response to
specific stimuli, the products of those glands are
released into the bloodstream.
The hormones then are carried via the
blood to their target cells.
The target cells for each hormone are characterized by
the presence of docking molecules(i.e., receptors) for
the hormone that are located either on the cell surface
or inside the cell. The interaction between the hormone and its
receptor
triggers a cascade of biochemical reactions in the target
cell that eventually modify the cells function or activity.7
-
8/13/2019 endocrinesystem-121228084635-phpapp01
8/79
CHEMICALCHARACTERISTICSOFHORMONES
Amines (from tyrosine)I. hydroxylation - catecholaminesII.
iodination - thyroid hormones
Peptides/proteins Steroids (from cholesterol)
I. adrenocorticoidsII. sex hormones
III. active metabolites of vitamin D
Their mechanisms of action (e.g., whether they canenter their
target cells and how they modulate theactivity of those cells) also
differ.
8
-
8/13/2019 endocrinesystem-121228084635-phpapp01
9/79
MECHANISMOFACTION:
STEROIDS: produced by gonads; structure similar to
cholesterol.
Enter their target cells and interact with the
cytoplasm or in the cell nucleus
Hormone-receptor complexes bind to certain regions
of the cells genetic material (i.e., the DNA)
Regulating the activity of specific hormone-responsive genes
9
-
8/13/2019 endocrinesystem-121228084635-phpapp01
10/79
MECHANISMOFACTION:
10
-
8/13/2019 endocrinesystem-121228084635-phpapp01
11/79
Amino acid derivatives:
are modified versions of building blocks of proteins.
thyroid gland & adrenal glands (i.e., the adrenal
medulla)
Enter the cell, where they interact with receptor proteins
that
are already associated with specific DNA regions. The
interaction modifies the activity of the affected genes.
Polypeptide and protein hormones:
found primarily in the hypothalamus, pituitary gland, and
pancreas
Because of their chemical structure, the polypeptide and
protein hormones cannot enter cells. Instead, they interactwith
receptors on the cell surface.
11
-
8/13/2019 endocrinesystem-121228084635-phpapp01
12/79
REGULATIONOFHORMONERELEASE
Constant feedback from the target glands to the
hypothalamus and pituitary gland ensures that the
activity of the hormone system involved remains
within appropriate boundaries.
To maintain the bodys homeostasis
Negative feedback mechanism
Short-loop feedback Positive-feedback mechanisms
12
-
8/13/2019 endocrinesystem-121228084635-phpapp01
13/79
Negative Feedback Loop
13
-
8/13/2019 endocrinesystem-121228084635-phpapp01
14/79
Positive Feedback Loop
14
-
8/13/2019 endocrinesystem-121228084635-phpapp01
15/79
THEHYPOTHALAMUSANDITSHORMONES
Why is the Hypothalamus so Important?Eating and drinking,
Sexual functions and behaviors,
Blood pressure and heart rate,Body temperature maintenance,
The sleep-wake cycle, and
Emotional states (e.g., fear, pain, anger, andpleasure)
15
-
8/13/2019 endocrinesystem-121228084635-phpapp01
16/79
Neurosecretory cells
16
-
8/13/2019 endocrinesystem-121228084635-phpapp01
17/79
THEHYPOTHALAMIC-HYPOPHYSEAL
PORTALSYSTEM
17
-
8/13/2019 endocrinesystem-121228084635-phpapp01
18/79
hypothalamic nuclei
superiorhypophysealartery superficial
capillary plexus
trabecular artery deepcapillary plexus
inferiorhypophysealartery
long portal veins
superficialcapillary plexus
18
-
8/13/2019 endocrinesystem-121228084635-phpapp01
19/79
hypothalamic nuclei
superiorhypophysealartery superficial
capillary plexus
trabecular artery deepcapillary plexuslong portal veins
short portal veins
inferiorhypophysealartery
19
-
8/13/2019 endocrinesystem-121228084635-phpapp01
20/79
hypothalamic nuclei
superiorhypophysealartery superficial
capillary plexus
trabecular artery deepcapillary plexuslong portal veins
short portal veinssecondary
capillaryplexus
adeno-
hypophysealcapillaryplexus inferior
hypophysealartery
20
-
8/13/2019 endocrinesystem-121228084635-phpapp01
21/79
superiorhypophysealartery superficial
capillary plexus
deepcapillary plexuslong portal veins
short portal veins
hypothalamic nuclei
trabecular artery
adeno-
hypophysealcapillaryplexus
hypophyseal vein
inferiorhypophysealartery
21
-
8/13/2019 endocrinesystem-121228084635-phpapp01
22/79
Corticotrophin (CRH) Somatostanin
ACTH
Gonadotropin (GnRH) Dopamine
LH & FSH
Thyrotropin (TRH) TSH
Growth-Hormone (GHRH)
GH
HYPOTHALAMIC
HORMONES
RELEASING INHIBITING
22
-
8/13/2019 endocrinesystem-121228084635-phpapp01
23/79
23
-
8/13/2019 endocrinesystem-121228084635-phpapp01
24/79
THEPITUITARYANDITSMAJORHORMONES
24
-
8/13/2019 endocrinesystem-121228084635-phpapp01
25/79
There is also an intermediate lobeinmany animals,but is
rudimentary in humans.
For instance, in fish, it is believed to controlphysiological
color change.
In adult humans, it is just a thin layer of cells
between the anterior and posterior pituitary.The intermediate
lobe produces melanocyte-stimulating hormone(MSH), although
thisfunction is often (imprecisely) attributed to theanterior
pituitary.
INTERMEDIATE LOBE
25
http://en.wikipedia.org/wiki/Pars_intermediahttp://en.wikipedia.org/wiki/Melanocyte-stimulating_hormonehttp://en.wikipedia.org/wiki/Melanocyte-stimulating_hormonehttp://en.wikipedia.org/wiki/Melanocyte-stimulating_hormonehttp://en.wikipedia.org/wiki/Melanocyte-stimulating_hormonehttp://en.wikipedia.org/wiki/Melanocyte-stimulating_hormonehttp://en.wikipedia.org/wiki/Melanocyte-stimulating_hormonehttp://en.wikipedia.org/wiki/Melanocyte-stimulating_hormonehttp://en.wikipedia.org/wiki/Pars_intermedia
-
8/13/2019 endocrinesystem-121228084635-phpapp01
26/79
GROWTH HORMONE Most abundant of the pituitary hormones
Pivotal role in controlling the bodys growth
and development.
1. Stimulates the linear growth of the bones;
2. Promotes the growth of internal organs, fat (i.e.,adipose)
tissue, connective tissue, endocrine glands,and muscle; and
3. Controls the development of the reproductive organs.
4. GH affects carbohydrate, protein, and fat (i.e.,
lipid)metabolism.
GH levels in the blood are highest during earlychildhood and
puberty and decline thereafter. 26
-
8/13/2019 endocrinesystem-121228084635-phpapp01
27/79
27
-
8/13/2019 endocrinesystem-121228084635-phpapp01
28/79
INDIRECTACTIONOFGROWTHHORMONE
28
-
8/13/2019 endocrinesystem-121228084635-phpapp01
29/79
Two hypothalamic hormones control GH release:
(1) GHRH:stimulates GH release,
(2) Somatostatin:inhibits GH release.
Shor t -loop feedback com ponent :
GH acts on the hypothalamus to stimulate somatostatin
release.
In addition, GH release is enhanced by
Stress, such as low blood sugar levels (i.e.,
hypoglycemia) or severe exercise, and by the onset of
deep sleep.
Acute and chronic alcohol consumption have been
shown to reducethe levels of GH and IGF-1 in the
blood. 29
-
8/13/2019 endocrinesystem-121228084635-phpapp01
30/79
PROLACTIN. Central role in the development of the female
breast and in the initiation and maintenance oflactation after
childbirth.
Factors control Prolactin release:
1. Response to the rise in estrogen levels in theblood that
occurs during pregnancy.
2. In nursing women, Prolactin is released inresponse to
suckling by the infant.
3. Dopamine, which has an inhibitory effect.
4. Alcohol consumption by nursing women caninfluence lactation
both through its effects on therelease of prolactin and oxytocin.
30
-
8/13/2019 endocrinesystem-121228084635-phpapp01
31/79
POSTERIOR PITUITARY:
31
VASOPRESSIN
-
8/13/2019 endocrinesystem-121228084635-phpapp01
32/79
VASOPRESSIN Vasopressin (arginine vasopressin, AVP; anti-
diuretic hormone, ADH)is a peptide hormone
formed in the hypothalamus, then transported viaaxons to, and
released from, the posterior pituitary.
Two principles site of action:
KIDNEY & BLOOD VESSEL
32
http://www.cvphysiology.com/Blood%20Pressure/BP008.htmhttp://www.cvphysiology.com/Blood%20Pressure/BP008.htm
-
8/13/2019 endocrinesystem-121228084635-phpapp01
33/79
MECHANISMSREGULATINGTHERELEASEOFAVP
Hypovolemia:decreased central venouspressure, the decreased
firing of atrial stretchreceptors leads to an increase in AVP
release.
Hypotension,whichdecreases arterial
baroreceptor firingand leads to enhancedsympathetic activity,
increases AVP release.
Angiotensin II receptors located in a region ofthe hypothalamus
regulate AVP release anincrease in angiotensin II simulates AVP
release.
Increased sympathetic activation stimulatesAVP release
33
http://www.cvphysiology.com/Blood%20Pressure/BP012.htmhttp://www.cvphysiology.com/Blood%20Pressure/BP012.htmhttp://www.cvphysiology.com/Blood%20Pressure/BP012.htmhttp://www.cvphysiology.com/Blood%20Pressure/BP012.htmhttp://www.cvphysiology.com/Blood%20Pressure/BP012.htmhttp://www.cvphysiology.com/Blood%20Pressure/BP012.htmhttp://www.cvphysiology.com/Blood%20Pressure/BP012.htm
-
8/13/2019 endocrinesystem-121228084635-phpapp01
34/79
OXYTOCIN HORMONE
I. Stimulates the contractions of the
uterus during childbirth.
I. In nursing women, the hormone activates milkejection in
response to suckling by the infant
(i.e., the so-called let-down reflex).
34
-
8/13/2019 endocrinesystem-121228084635-phpapp01
35/79
THEADRENALGLANDSANDTHEIRHORMONES
35
-
8/13/2019 endocrinesystem-121228084635-phpapp01
36/79
Action of Cortisol:
1. Cortisol increases glucose levels in the blood bystimulating
gluconeogenesis in the liver andpromotes the formation of glycogen
in the liver.
2. Reduces glucose uptake into muscle and adipose
tissue,3. Promotes protein and lipid breakdown into products
(i.e., amino acids and glycerol, respectively) that canbe used
for gluconeogenesis.
4. Protect the body against the deleterious effects ofvarious
stress factors.
5. Suppress tissue inflammation in response to injuriesand to
reduce the immune response to foreignmolecules. 36
-
8/13/2019 endocrinesystem-121228084635-phpapp01
37/79
ACTION OF ALDOSTERONE:
Regulate the bodys water and electrolyte balance.
Conserve sodium and to excrete potassium from thebody.
Reducing water excretion and increasing blood
volume.
Decreases the ratio of sodium to potassiumconcentrations in
sweat and saliva, therebypreventing sodium loss via those
routes.
Controlled primarily by another hormone system,
thereninangiotensin system, which also controls kidneyfunction.
37
-
8/13/2019 endocrinesystem-121228084635-phpapp01
38/79
THETHYROIDANDITSHORMONES
38
-
8/13/2019 endocrinesystem-121228084635-phpapp01
39/79
THYROID HORMONE PRODUCTION
39
-
8/13/2019 endocrinesystem-121228084635-phpapp01
40/79
THYROID HORMONE PRODUCTION
40
-
8/13/2019 endocrinesystem-121228084635-phpapp01
41/79
ACTIONOFTHYROIDHORMONE
Stimulates the production of certain proteins
involved in heat generation in the body, afunction that is
essential for maintaining bodytemperature in cold climates.
Promotes other metabolic processes involvingcarbohydrates,
proteins, and lipids that helpgenerate the energy required for the
bodysfunctions.
Plays an essential role in the development of thecentral nervous
system during late fetal and
early postnatal developmental stages. Required for the normal
development of teeth,
skin, and hair follicles as well as for thefunctioning of the
nervous, cardiovascular, andgastrointestinal systems
41
-
8/13/2019 endocrinesystem-121228084635-phpapp01
42/79
Parafollicular C cells) in the thyroid gland produce
calcitonin,a hormone that helps maintain normal
calcium levels in the blood.
Specifically, calcitoninlowers calcium levels in the
blood by reducing the release of calcium from the
bones; inhibiting the constant erosion of bones
(i.e., bone resorption), which also releasescalcium; and
inhibiting the reabsorption of calcium
in the kidneys.
42
-
8/13/2019 endocrinesystem-121228084635-phpapp01
43/79
THEPARATHYROIDGLANDS
ANDTHEIRHORMONES
43
-
8/13/2019 endocrinesystem-121228084635-phpapp01
44/79
ROLEOFPARATHYROIDHORMONE
Increases calcium levels in the blood, helping to
maintain bone quality and an adequate supply ofcalcium.
Causes re-absorption of calcium from and excretion
of phosphate in the urine.
Promotes the release of stored calcium from thebones as well as
bone resorption.
PTH stimulates the absorption of calcium from the
food in the gastrointestinal tract.
Functions facilitated by a substance
called1,25-dihydroxycholecalciferol, a derivative ofvitamin D.
44
-
8/13/2019 endocrinesystem-121228084635-phpapp01
45/79
CALCIUMHOMEOSTASIS
45
-
8/13/2019 endocrinesystem-121228084635-phpapp01
46/79
THEPANCREASANDITSHORMONES
46
-
8/13/2019 endocrinesystem-121228084635-phpapp01
47/79
TWODISTINCTLYDIFFERENTFUNCTIONS
EXOCRINE ENDOCRINE
Digestive Enzymes
Islets of
Langerhans
PANCREAS
INSULIN GLUCAGON
47
-
8/13/2019 endocrinesystem-121228084635-phpapp01
48/79
INSULIN & GLUCAGON
Beta cells of Islet Alpha cells of Islet
Blood sugar-lowering Increases blood glucose levels
hormone Actions opposite to insulin
Effect of Insulin:
1. Inhibits gluco-neogenesis
2. Insulin promotes the formation of storage formsof energy
(e.g., glycogen, proteins, and lipids)and suppresses the breakdown
of those storednutrients. 48
-
8/13/2019 endocrinesystem-121228084635-phpapp01
49/79
REGULATION OF BLOOD GLUCOSE
LEVELS
49
-
8/13/2019 endocrinesystem-121228084635-phpapp01
50/79
THEGONADSANDTHEIRHORMONES
OVARIES AND TESTES
They produce the germ cells.Synthesize steroid sex hormones that
are
necessary for the development and function ofboth female and
male reproductive organs and
secondary sex characteristics.Affect the metabolism of
carbohydrates and
lipids, the cardiovascular system, and bonegrowth and
development.
50
-
8/13/2019 endocrinesystem-121228084635-phpapp01
51/79
51
-
8/13/2019 endocrinesystem-121228084635-phpapp01
52/79
DIABETES
''Type 1 diabetes is growing by 5% per year amongpre-school
children in India.
It is estimated that 70,000 children, who are under15 years,
developjuvenile type 1 diabeteseach year(almost 200 children a
day!).
Symptoms of Diabetes in Children:
Stomach pains,
Headaches
Behaviour problems Weight loss, thirst, tiredness and frequent
urination.
Detected through the presence of ketoacidosis52
http://www.fatfreekitchen.com/diabetes/diabetes.htmlhttp://www.fatfreekitchen.com/diabetes/diabetes.htmlhttp://www.fatfreekitchen.com/diabetes/diabetes.htmlhttp://www.fatfreekitchen.com/diabetes/diabetes.htmlhttp://www.fatfreekitchen.com/diabetes/diabetes.htmlhttp://www.fatfreekitchen.com/diabetes/diabetes.htmlhttp://www.fatfreekitchen.com/diabetes/diabetes.htmlhttp://www.fatfreekitchen.com/diabetes/diabetes.html
-
8/13/2019 endocrinesystem-121228084635-phpapp01
53/79
CAUSES:
Type I (Juvenile Diabetes): bodys inabilityto produce
insulin
Genetic factors; environmental factors
Increased Type 2 Diabetes: linkedoverwhelmingly to lifestyle
changes that havecontributed to increased weight problems andlack
of activity in children. 53
-
8/13/2019 endocrinesystem-121228084635-phpapp01
54/79
TREATMENT:
INSULIN: The advent of insulin pumps for
administration has allowed many children addedflexibility in
their daily lives.
Monitoring blood sugar levels
Crucial factor
Diet:reduced consumption of fats and sugars,
intake fibers, vegetables and fruits.
Exercise: helps in lowering blood glucose levels
of the body54
-
8/13/2019 endocrinesystem-121228084635-phpapp01
55/79
COMPLICATIONS
Sudden hypoglycemia & hyperglycemia
Immediately giving the child a glucose tablet orglucose
beverage
LONG-TERM COMPLICATIONS
Problems of the kidney, heart, lungs, eyes, feetand nerves.
High blood sugar or high cholesterol levels55
-
8/13/2019 endocrinesystem-121228084635-phpapp01
56/79
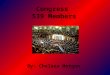
GIGANTISM Gigantism refers to abnormally
high linear growth due toexcessive action of insulin-like
growth factor-I (IGF-I) while the
epiphyseal growth plates are
open during childhood.
Acromegaly is the same disorderof IGF-I excess when it
occurs
after the growth plate cartilage
fuses in adulthood.
Robert Wadlow, called the Alton
giant,who stood 8 feet 11 inches
tall at the time of his death in his
mid-20s 56
-
8/13/2019 endocrinesystem-121228084635-phpapp01
57/79
CAUSES
Causes of excess IGF-I action may bedivided into 3
categories:
Those originating from primary GH excessreleased from the
pituitary;
Those caused by increased GH-releasinghormone (GHRH) secretion
or hypothalamicdysregulation; and
Hypothetically, those related to the excessiveproduction of
IGF-binding protein, whichprolongs the half-life of circulating
IGF-I. 57
-
8/13/2019 endocrinesystem-121228084635-phpapp01
58/79
-
8/13/2019 endocrinesystem-121228084635-phpapp01
59/79
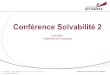
PITUITARYDWARFISM The achondroplastic
dwarf has anorthopedic reason forhaving short limbs anda short
spinal
colum. The pituitarydwarflacks growthhormone (an
endocrinereason).
SYMPTOMS: GH Deficiency
Low blood sugar59
-
8/13/2019 endocrinesystem-121228084635-phpapp01
60/79
RISKFACTORS:
Disease of the hypothalamus of the brain
Disease of the front of the pituitary gland in the brain
Newborns who had some type of serious medical event (such
as a lack of oxygen) happen in the perinatal period, are at
risk
for the type of growth hormone deficiency caused by damageto the
hypothalamus.
TREATMENT:
Treatment with human growth hormone
theoretically corrects the deficiency, but ismost successful
when the child is young. It mustbe given by injection.
60
-
8/13/2019 endocrinesystem-121228084635-phpapp01
61/79
PRECOCIOUSPUBERTY Precocious puberty
describes pubertyoccurring at an unusuallyearly age.
CAUSES:
Central:
damage to the inhibitorysystem of the brain
hypothalamic hamartomaproduces pulsatile
gonadotropin-releasinghormone(GnRH)
Langerhans cellhistiocytosis 61
http://en.wikipedia.org/wiki/Pubertyhttp://en.wikipedia.org/wiki/Hypothalamic_hamartomahttp://en.wikipedia.org/wiki/Gonadotropin-releasing_hormonehttp://en.wikipedia.org/wiki/Gonadotropin-releasing_hormonehttp://en.wikipedia.org/wiki/Langerhans_cell_histiocytosishttp://en.wikipedia.org/wiki/Langerhans_cell_histiocytosishttp://en.wikipedia.org/wiki/Langerhans_cell_histiocytosishttp://en.wikipedia.org/wiki/Langerhans_cell_histiocytosishttp://en.wikipedia.org/wiki/Langerhans_cell_histiocytosishttp://en.wikipedia.org/wiki/Langerhans_cell_histiocytosishttp://en.wikipedia.org/wiki/Gonadotropin-releasing_hormonehttp://en.wikipedia.org/wiki/Gonadotropin-releasing_hormonehttp://en.wikipedia.org/wiki/Gonadotropin-releasing_hormonehttp://en.wikipedia.org/wiki/Gonadotropin-releasing_hormonehttp://en.wikipedia.org/wiki/Hypothalamic_hamartomahttp://en.wikipedia.org/wiki/Hypothalamic_hamartomahttp://en.wikipedia.org/wiki/Puberty
-
8/13/2019 endocrinesystem-121228084635-phpapp01
62/79
PERIPHERALCAUSES
Secondary sexual development induced by sex
steroidsfrom other abnormal sources isreferred to asperipheral
precocious puberty.
Causes can include: Endogenous sources
gonadaltumors (such as arrhenoblastoma)
adrenaltumors
germ cell tumor
congenital adrenal hyperplasia
McCuneAlbright syndrome Exogenous hormones
Environmental
As treatment for another condition62
http://en.wikipedia.org/wiki/Sex_steroidhttp://en.wikipedia.org/wiki/Sex_steroidhttp://en.wikipedia.org/wiki/Gonadhttp://en.wikipedia.org/wiki/Arrhenoblastomahttp://en.wikipedia.org/wiki/Adrenalhttp://en.wikipedia.org/wiki/Germ_cell_tumorhttp://en.wikipedia.org/wiki/Congenital_adrenal_hyperplasiahttp://en.wikipedia.org/wiki/McCune%E2%80%93Albright_syndromehttp://en.wikipedia.org/wiki/McCune%E2%80%93Albright_syndromehttp://en.wikipedia.org/wiki/McCune%E2%80%93Albright_syndromehttp://en.wikipedia.org/wiki/McCune%E2%80%93Albright_syndromehttp://en.wikipedia.org/wiki/McCune%E2%80%93Albright_syndromehttp://en.wikipedia.org/wiki/McCune%E2%80%93Albright_syndromehttp://en.wikipedia.org/wiki/Congenital_adrenal_hyperplasiahttp://en.wikipedia.org/wiki/Germ_cell_tumorhttp://en.wikipedia.org/wiki/Adrenalhttp://en.wikipedia.org/wiki/Arrhenoblastomahttp://en.wikipedia.org/wiki/Gonadhttp://en.wikipedia.org/wiki/Sex_steroidhttp://en.wikipedia.org/wiki/Sex_steroid
-
8/13/2019 endocrinesystem-121228084635-phpapp01
63/79
TREATMENT
GnRH agonists stimulate the pituitary to releaseFollicle
Stimulating Hormone(FSH) andLuteinizing Hormone(LH).
One possible treatment is with anastrozole.Histrelinacetate.
63
PEDIATRIC CUSHINGS SYNDROME
http://en.wikipedia.org/wiki/Follicle_Stimulating_Hormonehttp://en.wikipedia.org/wiki/Luteinizing_Hormonehttp://en.wikipedia.org/wiki/Anastrozolehttp://en.wikipedia.org/wiki/Histrelinhttp://en.wikipedia.org/wiki/Histrelinhttp://en.wikipedia.org/wiki/Anastrozolehttp://en.wikipedia.org/wiki/Luteinizing_Hormonehttp://en.wikipedia.org/wiki/Follicle_Stimulating_Hormone
-
8/13/2019 endocrinesystem-121228084635-phpapp01
64/79
PEDIATRIC CUSHINGS SYNDROME
(CS)
Rare in childhood and adolescence. Caused by prolonged exposure
to excessive
glucocorticoids which can be secreted endogenouslyor
administered exogenously.
Supra-physiological doses of exogenous gluco-corticoids in the
form of topical, inhaled or oralcorticosteroids.
Eczema and asthma are common conditions in
childhood often requiring treatment withcorticosteroids.
64
-
8/13/2019 endocrinesystem-121228084635-phpapp01
65/79
65
-
8/13/2019 endocrinesystem-121228084635-phpapp01
66/79
66
-
8/13/2019 endocrinesystem-121228084635-phpapp01
67/79
TREATMENT
Primary adrenal lesions
Surgical excision is the first-line therapy for
acortical-secreting ACT.
Mitotane therapy appears to be the treatmentof choice
Cushings disease
Medical therapies such as MetyraponeandKetoconazoleto lower
serum cortisol levels canbe used as a short-term measure, but
cannot berecommended as long-term therapy. 67
-
8/13/2019 endocrinesystem-121228084635-phpapp01
68/79
THYROID DISORDERS
Thyroid disease occurs lessfrequently in children than in
adults, the signsand symptoms can be similar.
Congenital hypothyroidism
Affects infants at birth, and occurs in about 1 in4000 live-born
babies.
Loss of thyroid function, due to the thyroidgland failing to
develop normally.
Enzyme defect leading to deficient hormoneproduction, iodine
deficiency and a brainpituitary gland abnormality.
68
-
8/13/2019 endocrinesystem-121228084635-phpapp01
69/79
Within the first week of life, a heelprick blood sampleistaken
to assess an infant's thyroid hormone level.
Infant is immediately given thyroid hormone replacement
therapy (T4 thyroxine). Normal growth and developmentshould then
continue, with no adverse effects on the child'smental
capacity.
Subtle symptoms: Severe:
1. Poor feeding Poor growth and development2. Constipation Dry
skin & hair3. Low body temperature Slow tendon reflex4. Slow
pulse Enlarged tongue5.
Prolonged jaundice, Umbilical hernia6. Increased sleepiness
Puffiness & swelling7. Decreased crying.
69
H
-
8/13/2019 endocrinesystem-121228084635-phpapp01
70/79
HYPERTHYROIDISMINNEWBORNS
Overactive thyroid gland: referred to as
NEONATAL HYPERTHYROIDISM.
If the mother has Graves' disease, the thyroid-
stimulating antibodies in her blood can cross theplacenta and
stimulate the unborn child's thyroidgland,thus producing too much
thyroid hormone.
Some newborns may hardly be affected if the levels
of antibodies are low. No treatment may be necessary as the
mother's
antibodies will soon clear from the baby'sbloodstream, usually
within 2 to 3 months.
70
NEWBORNS WITH ADVANCED HYPERTHYROIDISM
-
8/13/2019 endocrinesystem-121228084635-phpapp01
71/79
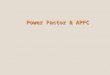
NEWBORNSWITHADVANCEDHYPERTHYROIDISM
TREATMENT
Anti-thyroid drugs is safe and effective, and will only beneeded
for a short period of time, until the stimulating
antibodies pass from the baby's bloodstream.If the mother is on
a high dose of anti-thyroid medication,
the diagnosis can be delayed by about a week until theinfant
clears the anti-thyroid medication.
EXTREMELY FASTPULSE
IRRITABILITY
FLUSHED MOIST SKIN
INFANT TENDS TO BE THIN &LONG
71
H '
-
8/13/2019 endocrinesystem-121228084635-phpapp01
72/79
HASHIMOTO'STHYROIDITIS
The most common cause of
hypothyroidismin childrenand adolescents isHashimoto's
thyroiditis, anautoimmune disease.
As the thyroid gland becomesincreasingly underactive,physical
and mental changeswill become more obvious.
Symptoms of hypothyroidismdevelop very slowly
72
-
8/13/2019 endocrinesystem-121228084635-phpapp01
73/79
SIGNSANDSYMPTOMS
The first sign is that the child's growth ratedecreases
unexpectedly and skeletaldevelopment is delayed.
GOITRE
DecreasedEnergy
Lethargy
Dry Itchy Skin&
Constipation
WEIGHTGAIN
PoorConcentration 73
-
8/13/2019 endocrinesystem-121228084635-phpapp01
74/79
TREATMENT
Thyroid hormone replacement istaken daily for life.
The dosage of thyroid hormone needs to be age-appropriate, as
the body's demands for thyroid
hormone vary with age.
SIDE-EFFECTS:In children who have had long-standing
hypothyroidism, ultimate height potential may bepartly lost.As
the child regains normal thyroid function,
behavioural problems may arise as their physicaland mental
processes speed up
74
GRAVES' DISEASE
-
8/13/2019 endocrinesystem-121228084635-phpapp01
75/79
GRAVES DISEASE
The most common causeof hyperthyroidism inchildren and
adolescentsis an autoimmunecondition called Graves'disease.
In Graves' disease thebody produces antibodiesthat stimulate the
thyroidgland uncontrollably, tomake too much thyroidhormone.
75
-
8/13/2019 endocrinesystem-121228084635-phpapp01
76/79
SIGNS AND SYMPTOMS
Increased Energy,
hyperactive, restless, Easilydistracted
Enlarged Thyroid Gland, fastpulse, nervousness, heat
intolerance, weight loss
Accelerated growth rate,Shaky hands
Muscle weakness, diarrhoea,and Sleep & behavioural
disturbances.76
TREATMENT
-
8/13/2019 endocrinesystem-121228084635-phpapp01
77/79
TREATMENT Propylthiouracil (PTU) or Carbimazole.
Period of 'block and replace therapy' (anti-thyroiddrugs as well
as thyroxine) is useful.
Throughout a child's treatment, thyroid hormone levels willneed
to be monitored regularly, along with their clinicalsymptoms.
SIDE EFFECTSAnti-thyroid drugs can, however, occasionally stop
the
production of white blood cells or platelets.
Sore throats, mouth ulcers, excessive bruising or skinrashes can
indicate this.
The only safe action is to stop the medication until afterthe
result of the blood test.
77
REFERENCES
-
8/13/2019 endocrinesystem-121228084635-phpapp01
78/79
REFERENCES: Susanne Hiller-Sturmhfel and Andrzej Bartke. The
Endocrine
Syste An Overview.Alcohol Health & Research World;
Vol.22(3):1998; 153-64
Ashley B. Grossman, Martin O. Savage.Pediatric CushingsSyndrome:
Clinical Features, Diagnosis, and Treatment.ArqBras Endocrinol
Metab 2007;51/8:1261-1271)
Kim E. Barrett, Susan M. Barman. GanongsReview of
MedicalPhysiology;Vol.23:451-568
Arthur C. Guyton. Textbook of Medical Physiology
10thedi;993-
1019
K. Sembulingham. Essentials Of Medical Physiology;3rdedi;667-714
78
-
8/13/2019 endocrinesystem-121228084635-phpapp01
79/79
Presented by:
Dr. Ruby Kharkwal1styear postgraduate studentDepartment of
Pedodontics
79