Embed Size (px)
DESCRIPTION
paeds
Citation preview

Electrolyte and Acid-Base Disorders

• The fetus has very high TBW, which gradually decreases to approximately 75% of birthweight for a term infant.
• Premature infants have higher TBW than term infants.
• During the 1st yr of life, TBW decreases to approximately 60% of body weight and basically remains at this level until puberty

Fluid Compartments
• TBW is divided between 2 main compartments: intracellular fluid (ICF) and extracellular fluid (ECF).
• In the fetus and newborn, the ECF volume is larger than the ICF volume.
• By 1 yr of age, the ratio of the ICF volume to the ECF volume approaches adult levels. The ECF volume is approximately 20-25% of body weight, and the ICF volume is approximately 30-40% of body weight, close to twice the ECF volume

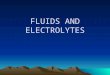
Compartments of total body water, expressed as percentages of body weight, in an older child or adult.

Web Figure 52-3 The concentrations of the major cations and anions in the intracellular space and the plasma, expressed in mEq/L.

The plasma osmolality is normally 285-295 mOsm/kg.
Glucose and urea normally contribute little to the plasma osmolality;. multiplication of the sodium value by 2 provides an approximation of the osmolality.

• Urea is not confined to the extracellular space because it readily crosses the cell membrane and its intracellular concentration approximately equals its extracellular concentration.
• Whereas an elevated sodium concentration causes a shift of water from the intracellular space, with uremia, there is no osmolar gradient between the 2 compartments and, consequently, no movement of water.

• The only exception is during hemodialysis, when the decrease in extracellular urea is so rapid that the intracellular urea does not have time to equilibrate. This may lead to the disequilibrium syndrome, in which water shifts into brain cells, potentially causing severe symptoms.
•

• Ethanol, because it freely crosses cell membranes, is another ineffective osmole. The effective osmolality can be calculated as follows:
effective osmolality = 2Na + Glucose/18
• The effective osmolality (also called the tonicity) determines the osmotic force that is mediating the shift of water between the ECF and the ICF.

• Hyperglycemia causes an increase in the plasma osmolality because it is not in equilibrium with the intracellular space.
• During hyperglycemia there is a shift of water from the intracellular space to the extracellular space.
• This is clinically important in children with hyperglycemia during diabetic ketoacidosis.
• The shift of water causes dilution of the sodium in the extracellular space, causing hyponatremia despite an elevated plasma osmolality.

• Corrected Sodium = Measured sodium + (((Serum glucose - 100)/100) x 1.6)
where [Na]measured = sodium concentration measured by the clinical laboratory and [Na]corrected = corrected sodium concentration (the sodium concentration if the glucose concentration were normal and its accompanying water moved back into the cells). The [Na]corrected is the more reliable indicator of the patient's true ratio of total body sodium to TBW, the normal determinant of the sodium concentration.

• Normally, the measured osmolality and the calculated osmolality are within 10 mOsm/kg.
• However, there are some clinical situations in which this does not occur.
• The presence of unmeasured osmoles causes the measured osmolality to be significantly elevated in comparison with the calculated osmolality. This difference is the osmolal gap, which is present when the measured osmolality exceeds the calculated osmolality by >10 mOsm/kg.

• Examples of unmeasured osmoles include ethanol, ethylene glycol, methanol, and mannitol. These substances increase the measured osmolality but are not part of the equation for calculating osmolality.
• The presence of an osmolal gap is a clinical clue to the presence of unmeasured osmoles and may be diagnostically useful when there is clinical suspicion of poisoning with methanol or ethylene glycol.

• Pseudohyponatremia is a second situation in which there is discordance between the measured osmolality and the calculated osmolality.
• It occurs in patients with large amounts of lipids and proteins in the body.
• In such situations, the plasma osmolality is normal despite the presence of pseudohyponatremia, because the method for measuring osmolality is not appreciably influenced by the percentage of serum that is composed of lipids and proteins.
• Pseudohyponatremia is diagnosed by the finding of a normal measured plasma osmolality despite hyponatremia.

• Whereas many children with high plasma osmolality are dehydrated—as seen with hypernatremic dehydration or diabetic ketoacidosis—high osmolality does not always equate with dehydration.
• A child with salt poisoning or uremia has an elevated plasma osmolality but may be volume overloaded.

Regulation of osmolality and volume
• Osmoreceptors in the hypothalamus sense the plasma osmolality.
• An elevated effective osmolality leads to secretion of antidiuretic hormone (ADH) by neurons in the supraoptic and paraventricular nuclei in the hypothalamus.

• The axons of these neurons terminate in the posterior pituitary.
• Circulating ADH binds to its V2 receptors in the collecting duct cells of the kidney, and, via the generation of cyclic adenosine monophosphate, causes insertion of water channels (aquaporin-2) into the renal collecting ducts.

• This produces increased permeability to water, permitting resorption of water into the hypertonic renal medulla.
• The end result is that the urine concentration increases and water excretion decreases.

• The regulation of ADH secretion is tightly linked to plasma osmolality, responses being detectable with a 1% change in the osmolality.
• ADH secretion virtually disappears when the plasma osmolality is low, allowing excretion of maximally dilute urine.
• The consequent loss of free water (water without sodium) corrects the plasma osmolality. ADH secretion is not an all-or-nothing response; there is a graded adjustment as the osmolality changes.

• Production of concentrated urine under the control of ADH requires a hypertonic renal medulla. The countercurrent multiplier, produced by the loop of Henle and the vasa recta, generates this hypertonicity.
• ADH stimulates sodium transport in the loop of Henle, helping to maintain this gradient when water retention is necessary.
• Water intake is regulated by hypothalamic osmoreceptors, although these are different from the osmoreceptors that determine ADH secretion.
• These hypothalamic osmoreceptors, by linking to the cerebral cortex, stimulate thirst when the serum osmolality increases. Thirst occurs with a small increase in the serum osmolality.

• When volume depletion is present, both ADH secretion and thirst are stimulated, regardless of the plasma osmolality.
• angiotensin II, which is increased during volume depletion, is known to stimulate thirst.
• In the syndrome of inappropriate antidiuretic hormone (SIADH), ADH continues to be produced despite a low plasma osmolality. In the presence of ADH, urinary dilution does not occur, and sufficient water is not excreted

• The minimum urine osmolality is approximately 30-50 mOsm/kg.
• This places an upper limit on the kidney's ability to excrete water; sufficient solute must be present to permit water loss.
• Volume depletion is an extremely important cause of decreased water loss by the kidney despite a low plasma osmolality. This “appropriate” secretion of ADH occurs because volume depletion takes precedence over the osmolality in the regulation of ADH.

• The normal response to increased plasma osmolality is conservation of water by the kidney.
• In central diabetes insipidus, this does not occur because of an absence of ADH secretion.
• Patients with nephrogenic diabetes insipidus have an inability to respond to ADH and produce dilute urine despite an increase in plasma osmolality

• The maximum urine osmolality is about 1,200 mOsm/kg. The obligatory solute losses dictate the minimum volume of urine that must be produced, even when maximally concentrated.
• Obligatory water losses increase in patients with high salt intake or high urea losses, as may occur after relief of a urinary obstruction or during recovery from acute tubular necrosis.
• An increase in urinary solute and, consequently, water losses occurs with an osmotic diuresis, which occurs classically from glycosuria in diabetes mellitus as well as iatrogenically after mannitol administration. There are developmental changes in the kidney's ability to concentrate the urine.

• The maximum urine osmolality in a newborn, especially a premature newborn, is less than that in an older infant or child. This limits the ability to conserve water and makes such a patient more vulnerable to hypernatremic dehydration.
• Very high fluid intake, as seen with psychogenic polydipsia, can dilute the high osmolality in the renal medulla, which is necessary for maximal urinary concentration. I

• If fluid intake is restricted in patients with this condition, there may be some impairment in the kidney's ability to concentrate the urine, although this defect corrects after a few days without polydipsia.
• This may also occur during the initial treatment of central diabetes insipidus with desmopressin acetate; the renal medulla takes time to achieve its normal maximum osmolality. Loop diuretics, such as furosemide, by inhibiting sodium resorption in the ascending limb of the loop of Henle, decrease medullary hypertonicity, preventing excretion of maximally concentrated urine.

Regulation of Volume • Because sodium is the principal extracellular cation and it is restricted to
the ECF, adequate body sodium is necessary for maintenance of intravascular volume.
• The principal extracellular anion, chloride, is also necessary, but for simplicity, sodium balance is considered the main regulator of volume status because body content of sodium and that of chloride usually change proportionally, given the need for equal numbers of cations and anions.
• In some situations, chloride depletion is considered the dominant derangement causing volume depletion (metabolic alkalosis with volume depletion). In other situations, such as volume depletion with metabolic acidosis, sodium depletion may exceed chloride depletion.

• The kidney determines sodium balance because there is little homeostatic control of sodium intake, even though salt craving does occasionally occur, typically in children with chronic renal salt loss.
• The kidney regulates sodium balance by altering the percentage of filtered sodium that is resorbed along the nephron.
• Normally, the kidney excretes <1% of the sodium filtered at the glomerulus. In the absence of disease, extrarenal losses and urinary output match intake, with the kidney having the capacity to adapt to large variations in sodium intake.
• When necessary, urinary sodium excretion can be reduced to virtually undetectable levels or increased dramatically.

• Urinary sodium excretion is regulated by both intrarenal and extrarenal mechanisms.
• The most important determinant of renal sodium excretion is the volume status of the child; it is the effective intravascular volume that influences urinary sodium excretion.
• The effective intravascular volume is the volume status that is sensed by the body's regulatory mechanisms.
• Heart failure is a state of volume overload, but the effective intravascular volume is low because poor cardiac function prevents adequate perfusion of the kidneys and other organs.
• This fact explains the avid renal sodium retention that is often present in patients with heart failure.

• Sodium resorption occurs throughout the nephron.
• Whereas the majority of filtered sodium is resorbed in the proximal tubule and the loop of Henle, the distal tubule and the collecting duct are the main sites for precise regulation of sodium balance.
• Approximately 65% of the filtered sodium is reclaimed in the proximal tubule, which is the major site for resorption of bicarbonate, glucose, phosphate, amino acids, and other substances that are filtered by the glomerulus.
• The transport of all these substances is linked to sodium resorption by cotransporters, or a sodium-hydrogen exchanger in the case of bicarbonate.

• This link is clinically important for bicarbonate and phosphate because their resorption parallels sodium resorption.
• In patients with metabolic alkalosis and volume depletion, correction of the metabolic alkalosis requires urinary loss of bicarbonate, but the volume depletion stimulates sodium and bicarbonate retention, preventing correction of the alkalosis.

• Volume expansion causes increased urinary losses of phosphate, even when there is phosphate depletion.
• Resorption of uric acid and urea occurs in the proximal tubule and increases when sodium retention increases.
• This arrangement accounts for the elevated uric acid and BUN measurements that often accompany dehydration, which is a stimulus for sodium retention in the proximal tubule. The cells of the proximal tubule are permeable to water; thus, water resorption in this segment parallels sodium resorption.

• The loop of Henle is, in terms of absolute amount, the 2nd most important site of sodium resorption along the nephron.
• The Na+,K+,2Cl− cotransporter on the luminal side of the membrane reclaims filtered sodium and chloride, whereas most of the potassium is recycled back into the lumen.
• This is the transporter that is inhibited by furosemide and other loop diuretics, which are highly effective at increasing sodium excretion.

• The ascending limb of the loop of Henle is not permeable to water, permitting sodium retention without water.
• ADH stimulates sodium retention in this segment; this arrangement helps create a more hypertonic medulla, which maximizes water conservation when ADH acts in the medullary collecting duct.
• Because loop diuretics inhibit sodium retention in this segment, their use causes a less hypertonic medulla, preventing excretion of maximally concentrated urine in the presence of ADH.

• Sodium retention in the distal tubule is mediated by the thiazide-sensitive Na+,Cl− cotransporter.
• This segment of the nephron is relatively impermeable to water, and along with sodium and chloride retention, the distal tubule is important for delivery of fluid with a low sodium concentration to the collecting duct.
• This allows for excretion of water without sodium in patients who stop secreting ADH because of low plasma osmolality.
• Thiazide diuretics, by inhibiting sodium and chloride retention in this segment, prevent the excretion of water without electrolytes—partially explaining the severe hyponatremia that occasionally develops in patients receiving chronic thiazide diuretics.

• The collecting duct, the final segment of the nephron, is important for the regulation of excretion of water, potassium, acid, and sodium.
• Even though the amount of sodium resorbed in this segment is less than in any other segment, this is the critical site for the regulation of sodium balance.
• Sodium resorption occurs via a sodium channel that is regulated by aldosterone.
• When these channels are open under the influence of aldosterone, almost all of the sodium can be resorbed. The uptake of sodium creates a negative charge in the lumen of the collecting duct, which facilitates the secretion of potassium and hydrogen ions.

• The potassium-sparing diuretics amiloride and triamterene block these sodium channels, and the inhibition of sodium uptake decreases potassium excretion.
• The potassium-sparing diuretic spironolactone blocks the binding of aldosterone to its receptor; thus, it indirectly decreases the activity of the sodium channels.
• The collecting duct is important for the regulation of water balance because it responds to ADH by inserting water channels that increase the permeability to water, and the hypertonicity of the renal medulla allows for maximal concentration of the urine.

• A number of systems are involved in the regulation of renal sodium excretion. The amount of sodium filtered at the glomerulus is directly proportional to the GFR.
• If sodium resorption in the nephron were constant, complete resorption of sodium with a small decrease in the GFR and significant renal sodium wasting with a small increase would result.
• This does not occur, however, because sodium resorption in the nephron is proportional to sodium delivery, a principle called glomerular tubular balance.

• The renin-angiotensin system is an important regulator of renal sodium excretion.
• The juxtaglomerular apparatus produces renin in response to decreased effective intravascular volume. Specific stimuli for renin release are decreased perfusion pressure in the afferent arteriole of the glomerulus, decreased delivery of sodium to the distal nephron, and β1-adrenergic agonists, which increase in response to intravascular volume depletion.
• Renin, a proteolytic enzyme, cleaves angiotensinogen, producing angiotensin I. Angiotensin-converting enzyme (ACE) converts angiotensin I into angiotensin II.

• The actions of angiotensin II include direct stimulation of the proximal tubule to increase sodium resorption and stimulation of the adrenal gland to increase aldosterone secretion.
• Through its actions in the distal nephron—specifically, the late distal convoluted tubule and the collecting duct—aldosterone increases sodium resorption.
• Aldosterone also stimulates potassium excretion, increasing urinary losses.
• Along with decreasing urinary loss of sodium, angiotensin II acts as a vasoconstrictor, which helps maintain adequate blood pressure in the presence of volume depletion.

• Volume expansion stimulates the synthesis of atrial natriuretic peptide, which is produced by the atria in response to atrial wall distention.
• Along with increasing the GFR, atrial natriuretic peptide inhibits sodium resorption in the medullary portion of the collecting duct, facilitating an increase in urinary sodium excretion.

• Volume overload occurs when sodium intake exceeds output.
• In children with kidney failure, there is an impaired ability to excrete sodium.
• This impairment tends to be proportional to the decrease in the GFR, although in some kidney diseases, such as renal dysplasia and juvenile nephronophthisis, damaged tubules cause significant sodium loss until the GFR is quite low.
• In general, as the GFR decreases, restriction of sodium intake becomes increasingly necessary..

• The GFR is low at birth, limiting a newborn's ability to excrete a sodium load.
• In other situations, there is a loss of the appropriate regulation of renal sodium excretion.
• This loss occurs in patients with excessive aldosterone, as is seen in primary hyperaldosteronism or renal artery stenosis, wherein excess renin production leads to high aldosterone levels.
• In acute glomerulonephritis, even without significantly reduced GFR, the normal intrarenal mechanisms that regulate sodium excretion malfunction, causing excessive renal retention of sodium and volume overload.

• Renal retention of sodium occurs during volume depletion, but this appropriate response causes the severe excess in total body sodium that is present in heart failure, liver failure, nephrotic syndrome, and other causes of hypoalbuminemia.
• In these diseases, the effective intravascular volume is decreased, causing the kidney and the various regulatory systems to respond, leading to renal sodium retention and edema formation.

• Volume depletion usually occurs when sodium losses exceed intake.
• The most common etiology in children is gastroenteritis. Excessive losses of sodium may also occur from the skin in children with burns, in sweat from patients with cystic fibrosis, or after vigorous exercise.
• Inadequate intake of sodium is uncommon except in neglect, in famine, or with an inappropriate choice of liquid diet in a child who cannot take solids.

• Urinary sodium wasting may occur in a range of renal diseases, from renal dysplasia to tubular disorders, such as Bartter syndrome.
• The neonate, especially if premature, has a mild impairment in the ability to conserve sodium.
• Iatrogenic renal sodium wasting takes place during diuretic therapy. Renal sodium loss occurs as a result of derangement in the normal regulatory systems.
• An absence of aldosterone, seen most commonly in children with congenital adrenal hyperplasia due to 21-hydroxylase deficiency, causes sodium wasting.

• Isolated disorders of water balance can affect volume status and sodium balance.
• Because the cell membrane is permeable to water, changes in TBW influence both the extracellular volume and the intracellular volume.
• In isolated water loss, as occurs in diabetes insipidus, the impact is greater on the intracellular space because of its higher volume compared with the extracellular space.
• This is why, in comparison with other types of dehydration, hypernatremic dehydration has less impact on plasma volume; most of the fluid loss comes from the intracellular space.

• Yet, significant water loss eventually affects intravascular volume and will stimulate renal sodium retention, even if total body sodium content is normal.
• Similarly, with acute water intoxication or SIADH, there is an excess of TBW, but most is in the intracellular space.
• However, there is some effect on the intravascular volume, which causes renal excretion of sodium.
• Children with SIADH or water intoxication have high urine sodium concentrations, despite hyponatremia.
• This finding reinforces the concept that there are independent control systems for water and sodium, yet the 2 systems interact when pathophysiologic processes dictate, and control of effective intravascular volume always takes precedence over control of osmolality.