Embed Size (px)
Citation preview

316
TCM Vol. 13, No. 8, 2003
C3H and C57BL/6 mouse model: evidencefor involvement of endothelial cells but notblood cells or cholesterol metabolism. CircRes 86:1078–1084.
Shi W, Wang X, Tangchitpiyanond K, Wong J,et al.: 2002. Atherosclerosis in C3H/HeJmice reconstituted with apolipoproteinE-null bone marrow. Arterioscler ThrombVasc Biol 22:650–655.
Shih DM, Gu L, Xia Y-R, et al.: 1998. Micelacking serum paraoxonase are susceptibleto organophosphate toxicity and athero-sclerosis. Nature 394:284–287.
Sing CF, Stengard JH, Kardia SL: 2003.Genes, environment, and cardiovasculardisease. Arterioscler Thromb Vasc Biole-publication ahead of print.
Slack J, Evans KA: 1966. The increased riskof death from ischaemic heart disease infirst degree relatives of 121 men and 96women with ischaemic heart disease. JMed Genet 2:239–257.
Smith DJ, Lusis AJ: 2002. The allelic struc-ture of common disease. Hum Mol Genet11:2455–2461.
Sugiyama F, Churchill GA, Higgins DC, et al.:2001. Concordance of murine quantitativetrait loci for salt-induced hypertensionwith rat and human loci. Genomics 71:70–77.
Talmud PJ, Hawe E, Martin S, et al.: 2002.Relative contribution of variation withinthe APOC3/A4/A5 gene cluster in determin-ing plasma triglycerides. Hum Mol Genet11:3039–3046.
Thomas AE, Green FR, Lamlum H, HumphriesSE: 1995. The association of combinedalpha and beta fibrinogen genotype onplasma fibrinogen levels in smokers andnon-smokers. J Med Genet 32:585–589.
Todd JA: 1999. From genome to aetiology ina multifactorial disease, type 1 diabetes.Bioessays 21:164–174.
Tward A, Xia Y-R, Wang XP, et al.: 2002. De-creased atherosclerotic lesion formation inhuman serum paraoxonase transgenicmice. Circulation 106:484–490.
Ueda, H, Howson JM, Esposito, L, et al.:2003. Association of the T-cell regulatorygene CTLA4 with susceptibility to autoim-mune disease. Nature 423:506–511.
Vockley J, Rinaldo P, Bennett MJ, et al.: 2000.Synergistic heterozygosity: disease result-ing from multiple partial defects in one ormore metabolic pathways [review]. MolGenet Metab 71:10–18.
Wang X, Paigen B: 2002. Quantitative traitloci and candidate genes regulating HDLcholesterol: a murine chromosome map.Arterioscler Thromb Vasc Biol 22:1390–1401.
PII S1050-1738(03)00143-9 TCM
Electrical Remodeling in Cardiac Hypertrophy
Joseph A. Hill*
In recent years, electrical remodeling has emerged as an importantpathophysiologic mechanism in many types of cardiac pathology.Because clinical heart disease often involves both hypertrophic and fail-ure phenotypes, identification of disease-specific mechanisms is essen-tial. This review focuses on mechanisms of electrical remodeling incardiac hypertrophy, emphasizing transmembrane Ca
2
�
fluxes andCa
2
�
-responsive signaling pathways. Where information is available,the remodeling of hypertrophy is contrasted with what is known aboutheart failure.
(Trends Cardiovasc Med 2003;13:316–322)
© 2003, Elsevier Inc.
Joseph A. Hill is at the Departments of Inter-nal Medicine and Molecular Biology, Univer-sity of Texas Southwestern Medical CenterDallas, Texas, USA.
* Address correspondence to: Joseph A.Hill, MD, PhD, Cardiology Division, Depart-ment of Internal Medicine, UT SouthwesternMedical Center, 5323 Harry Hines Blvd.Dallas, TX 75390-8573, USA. Tel.: (
�
1) 214-648-1400; fax: (
�
1) 214-648-1450; e-mail:[email protected].
© 2003, Elsevier Inc. All rights reserved.1050-1738/03/$-see front matter
hypertension (Brown et al. 2000, Korenet al. 1991, Levy et al. 1990), and poses asignificant public health problem in theUnited States today.
Patients with echocardiographicallydocumented hypertrophy are at signifi-cantly increased risk of developing ma-lignant arrhythmias, which accounts fora substantial component of the mortal-ity associated with cardiac hypertrophy(Brown et al. 2000). Mechanisms under-lying these arrhythmias are multifacto-rial, but they stem, at least in part, fromdisordered electrical currents arisingfrom prolongation of ventricular actionpotentials. The resulting delay in therecovery of excitability, a consistent fea-ture of ventricular hypertrophy (Armoun-das et al. 2001, Hart 1994), predisposes toearly and late afterdepolarizations. Hyper-trophy is also associated with myocardialfibrosis, altered electrotonic coupling be-tween cells, slowed conduction, and dis-persion of refractoriness, all of whichpredispose to re-entrant mechanisms ofarrhythmia. Together, these “electrical re-modeling” responses underlie the propen-sity to arrhythmia, syncope, and suddendeath.
In recent years, electrical remodelinghas emerged as an important patho-physiologic mechanism in many typesof cardiac pathology. Although consider-able progress has been made recently in
Hypertrophic growth of the heart is anadaptive response that develops in re-sponse to pressure or volume stress, mu-tations of sarcomeric (or other) proteins,or loss of contractile mass from prior in-farction. Hypertrophy accompanies manyforms of heart disease including ische-mic disease, hypertension, heart failure,and valvular disease. Initially an adap-tive response that preserves cardiac out-put and minimizes wall tension, cardiachypertrophy predisposes to ischemia,arrhythmia, and heart failure, the latterbeing the leading cause of combinedmorbidity and mortality in the UnitedStates (afflicting an estimated 4.8 millionindividuals) (Consensus Committee 1999).Cardiac hypertrophy is itself an inde-pendent predictor of cardiovascular mor-bidity and mortality, above and beyond

TCM Vol. 13, No. 8, 2003
317
elucidating the molecular pathogenesisof cardiac hypertrophy (as reviewed re-cently in Frey and Olson 2003), under-standing of mechanisms underlying hy-pertrophic action potential prolongationis limited. As a result, means of treatinghypertrophy-associated arrhythmias re-main disappointingly ineffective. Of ad-ditional interest, there is evidence to sug-gest that alterations in transmembraneCa
2
�
fluxes—a central feature of electricalremodeling—contribute to the pathogene-sis of hypertrophy by abnormally activat-ing Ca
2
�
-responsive signaling pathways.This review focuses on mechanisms
of electrical remodeling in cardiac hyper-trophy, emphasizing transmembrane Ca
2
�
fluxes and Ca
2
�
-responsive signaling path-ways. Where information is available,the remodeling of hypertrophy is con-trasted with what is known about heartfailure. Electrical remodeling in theatrium (Allessie et al. 2002, Brundel etal. 2002) and in the failing ventricle (Ar-moundas et al. 2001, Marban 1999), bothof which are major sources of morbidityand mortality, have each been reviewedrecently.
• Electrical Anatomy of Cardiomyocyte Repolarization
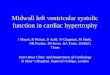
Recovery of excitability by repolariza-tion of the cell membrane is governed bya delicate balance between inward andoutward ionic currents; a relative shifttoward inward current favors action po-tential (AP) prolongation (Figure 1). In-ward currents active during repolari-zation include the L-type Ca
2
�
current(I
Ca,L
), which is active in phase 2 of theAP, and the inward current mediated bythe Na
�
/Ca
2
�
exchanger (I
NCX
), which isactive in phase 3. T-type Ca
2
�
currentsare normally absent from ventricularcardiomyocytes, but I
Ca,T
is upregulatedin some models of heart failure.
Outward currents that repolarize theventricular myocyte are numerous andcomplex (Figure 1), and there is sub-stantial interspecies variation in the pro-file of repolarizing currents. These K
�
currents include at least two isoforms oftransient outward current (I
to
), whichcontrol the rapid repolarization of phase1, thereby establishing the voltage levelof the phase 2 plateau. Starting with theterminal portions of phase 2, delayedrectifier (I
Kr
, I
Ks
, and in some instancesI
Kur
) K
�
currents activate. During the
terminal portion of repolarization, andthroughout diastole, inward rectifier (I
K1
)currents are important.
Electrophysiologic characteristics ofventricular tissue are heterogeneousacross the ventricular wall, and this het-erogeneity underlies a number of physio-logic (upright T wave on the surfaceelectrocardiogram) and pathologic (tor-sades de pointes, J wave of Osborne, Uwaves) processes (Antzelevitch et al.1995). In mammals ranging in size fromhumans and dogs to mice (Guo et al.1999, Kuo et al. 2001, Wang et al. 2001a),I
to
is expressed as a gradient across theventricular wall: I
to
is expressed at highlevels in subepicardial myocytes leadingto short APs; in the subendocardialzone, low-density expression of I
to
con-tributes to the relative lengthening ofAPs. Little is known about the molecularevents regulating transmural expressionof ion channel genes.
The basal heterogeneity of electricalrepolarization within the ventricle isoften accentuated in heart disease, lead-ing to abnormal degrees of dispersion ofrefractoriness. Longstanding evidencefrom clinical electrophysiologic studies,surface electrocardiography, and animalmodels points to disorders of ventricularrefractoriness as a major predisposingfactor in the development of reentrantventricular arrhythmias (Janse and Wit1989, Tomaselli et al. 1994).
• Myocardial Stress Responses
Stress induces changes in the structural,functional, and electrophysiologic prop-erties of the heart. These “remodeling”
adaptations involve cardiac myocytes,elements of the interstitial matrix, fibro-blasts, and the coronary vasculature.These adaptations are secondarily com-pounded by activation of neurohumoralreflex pathways, including adrenergicand cytokine pathways and the renin-angiotensin-aldosterone system. Many ofthese remodeling responses provide short-term benefit, but in the long term canprove maladaptive, leading to progres-sive myocardial decompensation.
Along these lines, hypertrophic trans-formation of the myocardium may be amilestone in the pathophysiologic pro-gression of heart failure (Figure 2). Atthe cellular level, cardiomyocyte hyper-trophy is characterized by an increase incell size, enhanced protein synthesis,and heightened organization of the sar-comere. These changes in cellular phe-notype are preceded and accompaniedby re-induction of the so-called “fetal geneprogram,” a pattern of gene expressionmimicking that seen during embryonicdevelopment. There are numerous par-allels in the altered gene expression ofcardiac hypertrophy and failure, and acti-vation of a number of signaling pathwaysis capable of inducing either phenotype.
Among the genes differentially ex-pressed in cardiac hypertrophy and fail-ure are those encoding sarcolemmal ionchannels and electrogenic transporters.By altering the excitability and recoveryresponses of the heart—primarily by in-ducing AP prolongation—these expres-sion changes contribute importantly tothe arrhythmias that are a prominentfeature of this disease. By altering Ca2�
homeostasis, these expression changes
Figure 1. Schematic diagram illustrating the major inward and outward currents active dur-ing the mammalian ventricular action potential. The diagram, adapted from the Sicilian Gam-bit initiative, is not intended to be comprehensive.

318 TCM Vol. 13, No. 8, 2003
may contribute to cardiac growth andultimately to myocardial dysfunction(Figure 3).
A central role for intracellular Ca2�
signaling in hypertrophy has been pro-posed (Frey et al. 2000, Wickenden et al.1998). In heart failure, disturbances ofCa2� metabolism lead to disordered reg-ulation of contractile performance andgene transcription. Cardiac contractionis initiated by systolic increases in intra-cellular Ca2�, which in heart failure areblunted, leading to depressed contrac-tile function. In addition, diastolic levelsof intracellular Ca2� are increased in fail-ing myocardium, contributing to ventric-ular stiffness (diastolic dysfunction). Un-
derlying mechanisms include (a) defectiveregulation of the sarcoplasmic reticulum(SR) Ca2�-release channel ryanodine re-ceptor 2 (RyR2), coupled with (b) defec-tive sequestration of Ca2� secondary todecreased expression of the SR Ca2�
pump [SERCA2, sarco(endo)plasmicreticulum CA2� adenotriphosphatase] andalterations in the expression and phos-phorylation of phospholamban, the majorregulator of SERCA2a activity (Hasen-fuss and Pieske 2002).
In hypertrophy, there is evidence tosuggest that Ca2� signaling may be dif-ferent from heart failure, with increasedCa2� transients (Wickenden et al. 1998)and increased inward Ca2� current (ICa,L)
(Armoundas et al. 2001, Mukherjee andSpinale 1998, Wang et al. 2001a). Ineither case, altered Ca2� handling con-tributes to the activation of several ki-nase and phosphatase cascades, includ-ing those involving mitogen-activatedprotein kinases, protein kinase C, andcalcineurin (recently reviewed in Vlahoset al. 2003). Together, such abnormalprofiles of signal transduction lead todisturbances of gene regulation, con-tributing directly to disease progression.
• AP Prolongation
Lengthening of the ventricular AP iscommonly observed in both cardiac hy-pertrophy and failure, a finding thatcontrasts with the AP shortening observedin the stressed (fibrillating) atrium. Incertain types of heart disease, includingheart failure in particular, there is evi-dence of diminished outward currentleading to AP prolongation; in other typesof myocardial disease, increased inwardcurrent underlies AP prolongation. Amajor goal of investigation in the field isto identify disease-specific mechanisticpathways leading to AP prolongation inhopes of developing new antiarrhythmictherapies.
In many models of heart failure, di-minished outward, repolarizing currentsecondary to downregulated K� channelexpression (particularly Ito) is observed(Armoundas et al. 2001, Nabauer andKaab 1998). Indeed, among the severalK� currents active in the heart, reduceddensity of Ito is the most consistent elec-trophysiologic change observed in heartfailure. Little is known about mechanismsunderlying downregulated K� current inheart failure, although diminished den-sity of Ito generally correlates with de-creased channel transcript levels.
In contrast with heart failure, AP pro-longation in hypertrophy often stemsfrom upregulated inward Ca2� current,particularly in models of modest hyper-trophy. Indeed, some evidence suggeststhat the density of L-type Ca2� current(ICa,L) is inversely correlated with the se-verity of hypertrophy or ventricular dys-function; in models of mild-to-moderatehypertrophy, ICa,L is often increased,whereas in severe hypertrophy and fail-ure, ICa,L is similar to control levels orsometimes decreased (for a discussion,see Armoundas et al. 2001). Ca2� channelsubunit transcript levels and ICa,L are
Figure 2. Hypothetic natural history of stress-induced heart disease illustrated with four-chamber sections of normal murine heart and hearts from surgically induced pressure-overloadhypertrophy and failure.
Figure 3. Hypothesis: Activation of stress-responsive signaling pathways alters the expressionand activity of Ca2� handling proteins, which lead to further activation of Ca2�-activatedsignaling pathways, action potential prolongation (and arrhythmias), and disease progression(transition to failure).

TCM Vol. 13, No. 8, 2003 319
decreased in myocytes isolated fromfibrillating atria (Allessie et al. 2001).Whereas the molecular basis for theseobservations is unknown, recent find-ings implicate Ca2�-responsive signalingpathways (see below). These findingsalso suggest the logical hypothesis (Fig-ure 3) that increased Ca2� channel ac-tivity contributes to the pathogenesis ofthe disease—and the progression fromhypertrophy to failure—a hypothesis weare currently testing.
• Hypertrophic Regulation of the Cardiac Ca2� Channel
Entry of a small amount of Ca2� via L-type channels triggers the release of muchlarger amounts of Ca2� from intracel-lular stores. As a result, modest changesin ICa,L-mediated Ca2� flux are amplifiedwithin the cell. In many species, mem-brane impedance is relatively high duringphase 2 of the AP; thus, changes in ICa,L
have important effects on AP morphol-ogy and duration.
The L-type channel in heart is com-prised of a large pore-forming subunit�11.2 plus auxiliary subunits �2-� and �.In failing human ventricular myocytes,Ca2� channel activity may exceed thatpredicted from constant levels of �11.2transcript and protein, suggesting post-translational regulation of the channelcomplex, possibly via phosphorylation(Schröder et al. 1998). Several kinaseshave been shown to phosphorylate thechannel, including protein kinases Aand C, and Ca2�–calmodulin-dependentkinase (Kamp and Hell 2000). These re-actions have been shown to regulate nu-merous aspects of channel function, in-cluding expression, voltage-dependentactivation and inactivation, and recov-ery from inactivation. These alterationsin channel function, in turn, are impor-tant in controlling heart rate, inotropy,and lusitropy.
As noted above, the cellular and mo-lecular phenotype of hypertrophy is mod-ulated by the degree of hypertrophy andthe primary lesion that induces hyper-trophy. Working with a model of in vivopressure overload hypertrophy in mice,our laboratory has found that outwardK� currents (Ito, IK1) do not change,whereas ICa,L increases, inducing greateraction potential prolongation in subendo-cardial myocytes given their relative lackof repolarizing Ito (Wang et al. 2001a).
Other models of moderate hypertrophyalso manifest increased ICa,L.
In pressure-overload hypertrophy, thebiophysical properties of ICa,L are un-changed except for recovery from inacti-vation, which is accelerated in hyper-trophied myocytes (Wang et al. 2001a).Whereas Ca2�, acting via calmodulin(Erickson et al. 2003), and protein ki-nase A-mediated phosphorylation (Kampand Hell, 2000) regulate L-type Ca2�
channel inactivation, the kinetics of chan-nel inactivation are unchanged, suggest-ing little involvement of these pathways.Similarly, steady-state activation andinactivation are unchanged. In contrast,recovery from inactivation is significantlyaccelerated in hypertrophied myocytes(Wang et al. 2001a).
Calcineurin is a protein phosphatasethat dephosphorylates transcription fac-tors of the nuclear factor of activated Tcells (NFAT) family, leading to theirtranslocation to the nucleus to activatetarget genes. It is well established thatactivation of the calcineurin/NFAT path-way is sufficient for the development ofcardiac hypertrophy and failure (Mol-kentin et al. 1998), and recent evidencedemonstrates that calcineurin is neces-sary in many models (reviewed in Freyand Olson 2003). In pressure-overloadhypertrophy, hypertrophic increases inICa,L are blocked by cyclosprine A (CsA),a specific inhibitor of calcineurin (Wanget al. 2001a), suggesting an importantregulatory role for this pathway. In addi-tion, calcineurin blockade prevented theaccelerated recovery from ICa,L inactiva-tion seen with hypertrophy. Because cal-cineurin suppression blocks hypertro-phy in numerous models—including ourown (Antos et al. 2002, Hill et al. 2000and 2002, Wang et al. 2001a)—it will beimportant to determine whether CsA-mediated changes in ICa,L are secondaryto the abrogated structural changes ofhypertrophy or vice versa, or are sepa-rate phenomena. Because AP prolonga-tion did not normalize completely withCsA, electrogenic transport processes inaddition to ICa,L must be involved.
A precedent exists in other systems inwhich calcineurin, which is activated byintracellular Ca2�, feeds back to regulateCa2� homeostasis. In yeast, calcineurinis involved in the regulation of Ca2�
pumps and exchangers responsible forCa2� homeostasis (Rusnak and Mertz2000). In mammalian tissues, calcineurin
directly regulates the function of severalproteins involved in Ca2� homeostasisincluding the inositol triphosphate andryanodine receptors in heart and theneuronal Na�-Ca2� exchanger (reviewedin Carafoli et al. 1999). Work from ourlaboratory (Wang et al. 2001b) (see be-low) has demonstrated that calcineurinregulates expression and function of thecardiac Na�-Ca2� exchanger.
Calcineurin regulates voltage-operatedCa2� channels (VOCCs) in a variety ofsystems, although there is disagreementregarding the nature and extent of itsregulatory function. Early studies inmolluscan and mammalian neurons im-plicated calcineurin as an inhibitor ofVOCCs; more recently, studies in rodentneuroblastoma/glioma hybrid cell lines(NG108-15) (Lukyanetz et al. 1998) andvascular smooth muscle (Schuhmannet al. 1997) demonstrated calcineurin-mediated negative feedback, possibly in-volving dephosphorylation of the chan-nel complex itself. Conversely, otherstudies using electrophysiologic and bio-chemical assays in rat pituitary tumor(GH3) cells (Victor et al. 1997, Zeilhoferet al. 2000) present evidence againstcalcineurin-mediated dephosphorylationand inactivation of L-type Ca2� channels.Recent work performed in cultured hip-pocampal neurons (Norris et al. 2002)provides the first evidence that cal-cineurin selectively enhances L-type Ca2�
channel activity in cultured neurons.Calcineurin overexpression in transgenicmice induces increased density of ICa,L
(Yatani et al. 2001) in the context of se-vere hypertrophy that decompensatesrapidly to failure and sudden death(Molkentin et al. 1998).
• Sodium-Calcium Exchanger
The Na�-Ca2� exchanger (NCX) is animportant mechanism of Ca2� elimina-tion during diastole. NCX catalyzes thebidirectional exchange of three Na� ionsfor a single Ca2� ion; one net chargemoves per reaction cycle, generating atransmembrane current that approachesone-half the magnitude of the L-typeCa2� current. NCX expression is maxi-mal near the time of birth and declinespostnatally (Boerth et al. 1994), and isrequired for normal cardiac develop-ment (Wakimoto et al. 2000). In severalmodels of heart failure, NCX activity andprotein levels are increased (Philipson

320 TCM Vol. 13, No. 8, 2003
and Nicoll 2000), which has been pro-posed to be an adaptive mechanism thatpreserves Ca2� metabolism and hencemyocardial function and lusitropy. Onthe other hand, increased NCX maycontribute to depletion of intracellularCa2� stores (Pieske et al. 1999) and com-promised systolic function (Schillingeret al. 2000), anoxia-induced cytosolicCa2� overload (Ladilov et al. 1999), andarrhythmogenesis (Pogwizd et al. 1999,Sipido et al. 2000, Zygmunt et al. 2000).
In a model of compensated hypertro-phy without systolic dysfunction or clin-ical heart failure, NCX1 transcript andprotein levels are increased to an extentsimilar to that reported in heart failure(Wang et al. 2001b). Interestingly, NCXfunction, assayed as INCX, is decreased.Similar downregulation of INCX was re-ported in a genetic model of modest hy-pertrophy (Mitarai et al. 2000), and dis-sociation of NCX protein and activitylevels in hypertrophy has been described(Boateng et al. 2001). These findingscontrast with heart failure, in whichseveral (Flesch et al. 1996, Hobai andO’Rourke 2000, Kent et al. 1993, Studeret al. 1994), although not all (Hasenfusset al. 1999, Yao et al. 1998), studies havedocumented increased exchanger activ-ity and often decreased expression of SRCa2�-adenosine triphosphatase (ATPase),reflecting a “fetal” pattern of calcium-cycling protein expression.
NCX activity is controlled by cytoso-lic concentrations of Ca2�, Na�, and ATP,intracellular pH, and phosphorylationof a large central cytoplasmic domain ofthe exchanger, and this regulation mayby altered in heart failure (Armoundaset al. 2003). In rodents, NCX contributesless to diastolic relaxation comparedwith rabbits and larger mammals becauseof relatively greater SR Ca2�-ATPase activ-ity. In heart failure, because NCX is oftenincreased and SR Ca-pump activity isoften diminished, there is a relative shifttoward Ca2� elimination from failingmyocytes, which may account for ablunted force-frequency relation. NCXhas been proposed to underlie delayedafterdepolarizations in human heart fail-ure (reviewed in Bers et al. 2002).
In contrast with heart failure, de-creased INCX in hypertrophy may favorCa2� sequestration in SR stores, therebyaugmenting the systolic performance ofthe hypertrophic heart. This Ca2� over-load, however, may be important in the
ultimate progression to heart failure. Itis tempting to speculate that NCX activ-ity is regulated differently in hypertro-phy and failure and may contribute tothe pathophysiologic transition fromhypertrophy to failure (Figure 3).
• Therapeutic Implications
Antiarrhythmic pharmacotherapy is basedprimarily on ion channel blockers thattarget channels selective for Na�, Ca2�,and K�. Following clinical trials such asCAST and SWORD, this mode of ther-apy has fallen into disfavor. It is likely,however, that elucidation of mechanismsunderlying AP prolongation in hyper-trophy and heart failure may have sig-nificant implications in devising drug-based therapeutic approaches to treatingarrhythmias in these diseases.
In recent years, the importance ofdevice-based therapy to treat arrhyth-mias has risen dramatically. These ther-apies are designed to induce favorableremodeling of the myocardium to benefitpatients with heart disease. For example,recognition that atrioventricular nodeablation after periods of rapid atrial fi-brillation is associated with bradycar-dia-dependent ventricular arrhythmias(Ozcan et al. 2001) has led to revisedrecommendations regarding postabla-tion pacing strategies. Recent data indi-cate that biventricular and left ventricu-lar resynchronization pacing therapiesfavorably remodel ventricular myocar-dium to reduce cardiovascular mortalityand provide significant clinical improve-ment (Abraham et al. 2002). It is likelythat advances in the molecular under-standing of electrical remodeling willimpact future developments in device-based therapies for arrhythmias (Chenet al. 2002).
• Summary
Cardiac hypertrophy has been viewed asa pathologic milestone in a disease pro-gression leading to heart failure, a syn-drome in which compensatory responsessuch as vasoconstriction, neurohumoralrecruitment, and cytokine activation aremaladaptive in the long term. To thislist, we might add “electrical remodel-ing,” a sweeping term that encompassesalterations in the electrogenic transportprocesses of the cardiac myocyte (Na-
bauer and Kaab 1998, Wickenden et al.1998). Although increased influx andintracellular sequestration of Ca2� mayprove beneficial by maximizing inotro-pic potential in the short run, the resultingchanges in AP morphology predispose tomalignant arrhythmia, and attendant al-terations in signal transduction maycontribute directly to disease progres-sion (Figure 3).
• Acknowledgments
The author gratefully acknowledges thethoughtful advice and careful reading ofthe manuscript provided by Dr. YangganWang. This work was supported by agrant from the Donald W. Reynolds Car-diovascular Clinical Research Center atUniversity of Texas Southwestern.
References
Abraham WT, Fisher WG, Smith AL, et al.:2002. Cardiac resynchronization in chronicheart failure. New Engl J Med 346:1845–1853.
Allessie M, Boyden P, Camm AJ, et al.: 2001.Pathophysiology and prevention of atrialfibrillation. Circulation 103:769–777.
Allessie M, Ausma J, Schotten U: 2002. Elec-trical, contractile and structural remodel-ing during atrial fibrillation. CardiovascRes 54:230–246.
Antos CL, McKinsey TA, Frey N, et al.: 2002.Activated glycogen synthase-3� suppressescardiac hypertrophy in vivo. Proc NatlAcad Sci USA 99:907–909.
Antzelevitch C, Sicouri S, Lukas A, et al.:1995. Regional differences in the electro-physiology of ventricular cells: physiologi-cal implications. In Zipes DP, Jalife J, eds.Cardiac Electrophysiology: From Cell toBedside. Philadelphia, WB Saunders, 228–245.
Armoundas AA, Wu R, Juang G, et al.: 2001.Electrical and structural remodeling of thefailing ventricle. Pharmacol Ther 92:213–230.
Armoundas AA, Hobai IA, Tomaselli GF, et al.:2003. Role of sodium-calcium exchanger inmodulating the action potential of ventric-ular myocytes from normal and failinghearts. Circ Res 93:46–53.
Bers DM, Pogwizd SM, Schlotthauer K: 2002.Upregulated Na/Ca exchange is involved inboth contractile dysfunction and arrhythmo-genesis in heart failure. Basic Res Cardiol97:I36–I42.

TCM Vol. 13, No. 8, 2003 321
Boateng SY, Naqvi RU, Koban MU, et al.:2001. Low-dose ramipril treatment improvesrelaxation and calcium cycling after estab-lished cardiac hypertrophy. Am J Physiol280:H1029–H1038
Boerth SR, Zimmer DB, Artman M: 1994.Steady-state mRNA levels of the sarcolem-mal Na�-Ca2� exchanger peak near birth indeveloping rabbit and rat hearts. Circ Res74:354–359.
Brown DW, Giles WR, Croft JB: 2000. Leftventricular hypertrophy as a predictor ofcoronary heart disease mortality and theeffect of hypertension. Am Heart J 140:848–856.
Brundel BJJM, Henning RH, et al.: 2002. Mo-lecular mechanisms of remodeling in humanatrial fibrillation. Cardiovasc Res 54:315–324.
Carafoli E, Genazzani A, Guerini D: 1999.Calcium controls the transcription of itsown transporters and channels in develop-ing neurons. Biochem Biophys Res Com-mun 266:624–632.
Chen X, Piacentino V III, Furukawa S, et al.:2002. L-type Ca2� channel density and reg-ulation are altered in failing human ven-tricular myocytes and recover after supportwith mechanical assist devices. Circ Res91:517–524.
Consensus Committee: 1999. Consensus rec-ommendations for the management ofchronic heart failure. Am J Cardiol 83:1A–38A.
Erickson MG, Liang H, Mori MX, et al.: 2003.FRET two-hybrid mapping reveals func-tion and location of L-type Ca2� channelpreassociation. Neuron 39:97–107.
Flesch M, Schwinger RHG, Schiffer F, et al.:1996. Evidence for functional relevance ofan enhanced expression of the Na�-Ca2�
exchanger in failing human myocardium.Circulation 94:992–1002.
Frey N, Olson EN: 2003. Cardiac hypertro-phy: the good, the bad and the ugly. AnnuRev Physiol 65:45–79.
Frey N, McKinsey TA, Olson EN: 2000. De-coding calcium signals involved in cardiacgrowth and function. Nat Med 6:1221–1227.
Guo W, Xu H, London B, et al.: 1999. Molecu-lar basis of transient outward K� currentdiversity in mouse ventricular myocytes. JPhysiol (Lond) 521:587–599.
Hart G: 1994. Cellular electrophysiology incardiac hypertrophy and failure. Cardio-vasc Res 28:933–946.
Hasenfuss G, Pieske B: 2002. Calcium cyclingin congestive heart failure. J Mol Cell Car-diol 34:951–969.
Hasenfuss G, Schillinger W, Lehnart SE, etal.: 1999. Relationship between Na�-Ca2�-exchanger protein levels and diastolicfunction of failing human myocardium.Circulation 99:641–648.
Hill JA, Karimi M, Kutschke W, et al.: 2000.Cardiac hypertrophy is not a requiredcompensatory response to short-term pres-sure overload. Circulation101:2863–2869.
Hill JA, Rothermel BA, Yoo K-D, et al.: 2002.Targeted inhibition of calcineurin in pres-sure-overload hypertrophy: Preservation ofsystolic function. J Biol Chem 277:10,251–10,255.
Hobai IA, O’Rourke B: 2000. Enhanced Ca2�-activated Na�-Ca2� exchange activity in ca-nine pacing-induced heart failure. Circ Res87:690–698.
Janse MJ, Wit AL: 1989. Electrophysiologicalmechanisms of ventricular arrhythmias re-sulting from myocardial ischemia and in-farction. Physiol Rev 69:1049–1169.
Kamp TJ, Hell JW: 2000. Regulation of car-diac L-type calcium channels by protein ki-nase A and protein kinase C. Circ Res87:1095–1102
Kent RL, Rozich JD, McCollam PL, et al.:1993. Rapid expression of the Na�-Ca2� ex-changer in response to cardiac pressureoverload. Am J Physiol 265:H1024–H1029.
Koren MJ, Devereux RB, Casale PN, et al.:1991. Relation of left ventricular mass andgeometry to morbidity and mortality in un-complicated essential hypertension. AnnInt Med 114:345–352.
Kuo H-C, Cheng C-F, Clark RB, et al.: 2001. Adefect in the Kv channel-interacting pro-tein 2 (KChIP2) gene leads to a completeloss of Ito and confers susceptibility to ven-tricular tachycardia. Cell 801–813.
Ladilov Y, Haffner S, Balser-Schäfer C, et al.:1999. Cardioprotective effects of KB-R7943:a novel inhibitor of the reverse mode ofNa�/Ca2� exchanger. Am J Physiol 276:H1868–H1876.
Levy D, Garrison RJ, Savage DD, et al.: 1990.Prognostic implications of echocardio-graphically determined left ventricular massin the Framingham Heart Study. New EnglJ Med 322:1561–1566.
Lukyanetz EA, Piper TP, Sihra TS: 1998. Cal-cineurin involvement in the regulation ofhigh-threshold Ca2� channels in NG108-15(rodent neuroblastoma glioma hybrid)cells. J Physiol 510:371–385.
Marban E: 1999. Heart failure: the electro-physiologic connection. J Cardiovasc Elec-trophysiol 10:1425–1428.
Mitarai S, Reed TD, Yatani A: 2000. Changesin ionic currents and �-adrenergic receptor
signaling in hypertrophied myocytes over-expressing G�q. Am J Physiol 279:H139–H148.
Molkentin JD, Lu J-R, Antos CL, et al.: 1998.A calcineurin-dependent transcriptionalpathway for cardiac hypertrophy. Cell 93:215–228.
Mukherjee R, Spinale FG: 1998. L-type cal-cium channel abundance and functionwith cardiac hypertrophy and failure: a re-view. J Mol Cell Cardiol 30:1899–1916.
Nabauer M, Kaab S: 1998. Potassium chan-nel down-regulation in heart failure. Cardio-vasc Res 37:324–334.
Norris CM, Blalock EM, Chen K-C, et al.:2002. Calcineurin enhances L-type Ca2�
channel activity in hippocampal neurons:increased effect with age in culture. Neuro-science 110:213–225.
Ozcan C, Jahangir A, Friedman PA, et al.:2001. Long-term survival after ablation ofthe atrioventricular node and implantationof a permanent pacemaker in patients withatrial fibrillation. New Engl J Med 344:1043–1051.
Pieske B, Maier LS, Bers DM, et al.: 1999.Ca2� handling and sarcoplasmic reticulumCa2� content in isolated failing and non-failing human myocardium. Circ Res 85:38–46.
Philipson KD, Nicoll DA: 2000. Sodium-calcium exchange: a molecular perspective.Annu Rev Physiol 62:111–133.
Pogwizd SM, Qi M, Yuan W, et al.: 1999. Up-regulation of Na�/Ca2� exchanger expres-sion and function in an arrhythmogenicrabbit model of heart failure. Circ Res85:1009–1019.
Rusnak F, Mertz P: 2000. Calcineurin: formand function. Physiol Rev 80:1483–1521.
Schillinger W, Janssen PML, Emami S, et al.:2000. Impaired contractile performance ofcultured rabbit ventricular myocytes afteradenoviral gene transfer of Na�-Ca2� ex-changer. Circ Res 87:581–587.
Schröder F, Handrock R, Beuckelmann DJ,et al.: 1998. Increased availability andopen probability of single L-type calciumchannels from failing compared with non-failing human ventricle. Circulation 98:969–976.
Schuhmann K, Romanin C, Baumgartner W,et al.: 1997. Intracellular Ca2� inhibitssmooth muscle L-type Ca2� channels byactivation of protein phosphatase type 2Band by direct interaction with the channel.J Gen Physiol 110:503–513.
Sipido KR, Volders PGA, Marieke de GrootSH, et al.: 2000. Enhanced Ca2� release andNa/Ca exchange activity in hypertrophied

322 TCM Vol. 13, No. 8, 2003
canine ventricular myocytes: potential linkbetween contractile adaptation and arrhyth-mogenesis. Circulation 102: 2137–2144.
Studer R, Reinecke H, Bilger J, et al.: 1994.Gene expression of the cardiac Na�-Ca2�
exchanger in end-stage human heart fail-ure. Circ Res 75:443–453.
Tomaselli GF, Beuckelmann DJ, Calkins HG,et al.: 1994. Sudden cardiac death in heartfailure. The role of abnormal repolariza-tion. Circulation 90:2534–2539.
Victor RG, Rusnak F, Sikkink RA, et al.: 1997.Mechanism of Ca2�-dependent invativa-tion of L-type Ca2� channels in GH3 cells:direct evidence against dephosphorylationby calcineurin. J Membr Biol 156:53–61.
Vlahos CJ, McDowell SA, Clerk A: 2003. Ki-nases as therapeutic targets for heart fail-ure. Nat Rev Drug Discov 2:99–113.
Wakimoto K, Kobayashi K, Kuro-o M, et al.:2000. Targeted disruption of Na�/Ca2� ex-changer gene leads to cardiomyocyte apo-ptosis and defects in heartbeat. J BiolChem 275:36,991–36,998.
Wang Z, Kutschke W, Richardson KE, et al.:2001a. Electrical remodeling in pressure-overload cardiac hypertrophy: role of cal-cineurin. Circulation 104:1657–1663.
Wang Z, Nolan B, Kutschke W, et al.: 2001b.Na�/Ca2� exchanger remodeling in pres-sure-overload cardiac hypertrophy. J BiolChem 276:17,706–17,711.
Wickenden AD, Kaprielian R, Kassiri Z, et al.:1998. The role of action potential prolon-gation and altered intracellular calciumhandling in the pathogenesis of heart fail-ure. Cardiovasc Res 37:312–323.
Yao A, Su Z, Nonaka A, et al.: 1998. Abnormalmyocyte Ca2� homeostasis in rabbits withpacing-induced heart failure. Am J Physiol275:H1441–1448.
Yatani A, Honda R, Tymitz KM, et al.: 2001.Enhanced Ca2� channel currents in car-diac hypertrophy induced by activation ofcalcineurin-dependent pathway. J Mol CellCardiol 33:249–259.
Zeilhofer HU, Blank NM, Neuhuber WL, etal.: 2000. Calcium-dependent inactivationof neuronal calcium channel currents inindependent of calcineurin. Neuroscience95:235–241.
Zygmunt AC, Goodrow RJ, Antzelevitch C:2000. INaCa contributes to electrical hetero-geneity within the canine ventricle. Am JPhysiol 278:H1671–H1678.
PII S1050-1738(03)00144-0 TCM
Involvement of Progenitor Cellsin Vascular RepairBenjamin Hibbert, Steve Olsen, and Edward O’Brien*
Whereas the genesis of an arterial lesion is thought to be the result ofmigration and proliferation of vascular cells, recent insights into thebiology of progenitor cells now question this concept. Specifically, endo-thelial and smooth muscle cells appear to be derived from multiplesources such as circulating stem and progenitor cells, as well as tissue-resident progenitor cell populations. These cells may engraft at sites ofvascular injury and play an integral role in vascular repair. In thisreview, experimental data from in vitro studies, animal models, andscattered human observations are reviewed in the context of emerginghypotheses regarding the response to vascular injury. (Trends Cardio-vasc Med 2003;13:322–326) © 2003, Elsevier Inc.
arteries) are derived from cells of thedorsal mesocardium (Mikawa and Fisch-man 1992). In contrast, lineage-mappingstudies show that tunica media SMCs ofthe great vessels originate in the neuralcrest (deRuiter et al. 1990). However, asdiscussed below, more recent data suggestthat other sources of vascular cells suchas stem and progenitor cells, either cir-culating or resident in tissues, as well asvascular cell transdifferentiation, may beinvolved in the formation and repair ofblood vessels. Further elucidation of re-generative biology concepts is currentlyan active area of vascular research.
• Origin of Vascular Progenitor Cells
For the purposes of this discussion, astem cell is defined by its capacity toregenerate multiple (differentiated) celltypes and its ability to undergo self-renewal. In terms of commitment, pro-genitor cells appear to be beyond stemcells, and only differentiate toward par-ticular cell lineages. Moreover, progeni-tor cells have less capacity for self-renewal. In 1997, the first report of cir-culating CD34� vascular progenitor cellsfrom human peripheral blood demon-strated that these cells differentiate into
Although the kinetics of arterial repair iswell understood in various experimentalmodels, the origin of the cells that par-ticipate in these processes is less clear(Schwartz et al. 1995). In part, this con-fusion highlights the complexity of lesionformation, but also reflects an evolutionin the understanding of developmentaland regenerative biology. Earlier studies(Kirby and Waldo 1990, LeLievre and LeDouarin 1975) suggested that locally de-rived smooth muscle cells (SMCs) investa developing artery and arise from atleast two different lineages: one derivedfrom the neural crest (ectomesenchymalSMCs), the other originating in the me-soderm (mesenchymal SMCs). For ex-ample, it is held that epicardial vascularcapillaries (progenitors of the coronary
Benjamin Hibbert, Steve Olsen, and EdwardO’Brien are at the Vascular Biology Laboratory,Division of Cardiology, University of OttawaHeart Institute, Ottawa, Ontario, Canada.
* Address correspondence to: Dr. E.R.M.O’Brien, Vascular Biology Laboratory, Divi-sion of Cardiology, University of OttawaHeart Institute, Ottawa, Ontario K1Y 4W7,Canada. Tel.: (�1) 613-761-5030; fax: (�1)613-761-4237; e-mail: [email protected].
© 2003, Elsevier Inc. All rights reserved.1050-1738/03/$-see front matter