Embed Size (px)
Citation preview

Behov. Res. & Therapy, Vol. 18. pp. 449 to 455
0 Pergamon Press Ltd 1980. Printed in Great Brnain
EFFECTS OF IMAGINAL EXPOSURE TO FEARED DISASTERS IN OBSESSIVE-COMPULSIVE
CHECKERS*
EDNA B. FoAt, GAIL STEKETEE, RALPH M. TURNER and STEVEN C. FISCHER Temple University School of Medicine
Summary-The combined effects of imaginal exposure to feared catastrophes and in uivo ex- posure to external stimuli were compared with the effects of in uiw exposure alone in 15 obsessive-compulsives with checking rituals. The first group received 90 min of uninterrupted exposure in imagination, which concentrated mainly on disastrous consequences, followed by 30 min of exposure in uiw to stimuli-situations which triggered rituals. The second group was given 2 hr of exposure in viw only. Both groups were prevented from performing rituals. Treatment consisted of 10 daily sessions within a 2 week period.
Assessments were conducted before and after treatment and at follow-up ranging from 3 months to 2.5 yr with a mean of 11 months. At post-treatment both groups improved consider- ably and did not differ. But at follow-up those who received imaginal and in vioo exposure maintained their gains, whereas the group who were treated by exposure in eir?o alone evidenced partial relapse on four of the six dependent measures. The results tend to indicate that a closer match between a patient’s internal fear model and the content of exposure enhances long term treatment efficacy.
The differential effects of exposure in imagination and exposure in uivu have been the subject of several investigations. Studying agoraphobics, Matthews et al. (1976) compared the effects of eight sessions of exposure in imagination followed by eight sessions in uiuo with 16 sessions of combined imaginal and in uiuo exposure and with 16 sessions of exposure in uiuo only. No differences between these two exposure modalities were detected, nor did the addition of imaginal exposure enhance the effect of exposure in practice.
Other studies have found actual confrontation with the feared situation superior to exposure in fantasy. Emmelkamp and Wessels (1975) compared four sessions each of prolonged exposure in uiuo, imaginal exposure and a combination of the two. After an intermediate evaluation, all patients received eight sessions of self-observation which is a variant of exposure in viva They’ found actual exposure superior to imaginal. Moreover self-observation added little to the effect obtained by exposure in uiuo or to that found by combining imaginal and in uiuo procedures, but did enhance the gains resulting from imaginal flooding alone.
When concurrent imaginal and in vim exposures were contrasted with successive approximation (again, a variant of exposure in uiuo), both methods of treatment resulted in significant improvement and differed only on the phobic anxiety measure, those who received imaginal exposure showing greater improvement (Everaerd, Rijken and Emmel- kamp, 1973). In yet another study (Emmelkamp, 1974) no differences were found between combined imaginal and in uiuo treatment. vs self-observation. But the group who received all three procedures evidenced the greatest improvement, perhaps because it resulted in more actual confrontations with the feared stimuli. The seeming superiority of in vim exposure to imaginal exposure was also found with obsessive-compulsive patients. Raba- vilas, Boulougouris and Stefanis (1976) reported prolonged exposure in uiuo superior to short exposure in uiuo and to long and short exposure in fantasy.
Although most studies have examined the relative efficacy of different modalities of exposure, of equal importance is the content of exposure and its relevance to the patient’s symptomatology. Lang (1977) has suggested that the degree of match between the
* This research was supported by Grant lROl-MH-31634-01Al from the Clinical Research Branch of the National Institute of Mental Health awarded to the senior author.
t Requests for reprints should be addressed to Edna B. Foa Ph.D., Department of Psychiatry, Temple University. c/o E.P.P.I., 3300 Henry Avenue, Philadelphia, PA 19129, U.S.A.
449

450 EDNA B. FOA, GAIL STEKETES RALPH M. TURNER and STEVEN C. FISCHER
patient’s internal fear model and the imaginal scene will influence the effectiveness of treatment. When exposure in fantasy includes only tangible cues, thus simply shadowing exposure in uivo situations, it is not surprising that the latter will prove more effective. However, for many neurotic patients anxiety is generated by borh environmental tangible cues and thoughts of possible disasters following exposure to these stimuli. Exposure to tangible cues may be done either in uiuo or in imagination, whereas feared disasters can be presented only in fantasy. If the matching hypothesis is tenable, patients who fear disastrous consequences which cannot be produced in reality should improve more when imaginal exposure to these stimuli is added to in uivo exposure. R’achman (1976) has suggested that the internal fear model of patients with checking rituals centers around responsibility for potential catastrophes. We therefore hypothesized that these patients would benefit more from a combination of imaginal exposure to disasters and in uiuo exposure to tangible cues than from the latter alone.
Patients METHOD
Patients were 15 obsessive-compulsives who manifested checking rituals and reported fears of disastrous consequences upon failure to carry out rituals. The sample was com- prised of eight males and seven females with a mean age of 37 yr and mean symptom duration of 15 yr, Criteria for inclusion in the study were as follows: age range of IS-60 yr; checking rituals presented as the main complaint and severe enough to cause considerable interference in everyday functioning; absence of overt psychosis.
Design
Subjects were divided into two groups in successive order of applying for treatment. Group 1 received imaginal exposure, in uivo exposure and response prevention. Group 2 was treated with exposure in uivo only combined with response prevention.
Assessments were conducted on the following occasions: before treatment, after treat- ment and at follow-up which ranged from 3 months to 2.5 yr with a mean of 11 months.
Treatment procedure
Each patient was first interviewed by a senior psychologist who determined her or his suitability for treatment according to the criteria described above. Following acceptance into the study patients were contacted by their therapists, all of whom were trained in behavior therapy.
The program consisted of three stages: (1) ~n~~~tio~ gathering period (2 weeks}. Patients were seen by their therapists for
four sessions, each lasting approximately 90 min. History and the nature of the complaint were discussed and general information about the patient was gathered. The material thus collected served to prepare a list of obsessions and compulsions and to design the treatment program. This included setting up the place of treatment (home or hospital), listing the behaviors to be under response prevention, designating supervisors for re- sponse prevention, constructing scenes for exposure in fantasy and preparing situations and/or objects for exposure in oioo. Patients were hospitalized when they lived out of town or when cooperative supervisors were unavailable at home.
(2) Treatment (2 weeks). Patients in group 1 received 10 daily sessions (excluding weekends) of exposure in imagination (1.5 hr) followed by exposure in vivo (0.5 hr). In group 2, 10 daily sessions (excluding weekends) of exposure in uiuo (2 hr) were adminis- tered. For both groups, response prevention was in force from the first session and treatment was conducted partly in the patient’s natural environment and partly in the therapist’s office.
The three ‘treatment components are described below:
(a) Exposure in ima~nation-On the basis of the initial interviews, three or four scenes were constructed for each patient. The scenes varied with respect to their potential

Exposure to feared disasters 451
for eliciting anxiety. The first scene to be introduced was one expected by the patient to elicit about 60 SUDS (subjective units of discomfort ranging from 0 to 100). When some decrease in anxiety was reported, scenes that evoke about 70 or 80 SUDS were intro- duced. Finally, a scene evoking 100 SUDS was presented by the fifth session. All patients lay on a recliner with their eyes closed during the entire flooding session and were instructed to imagine the scenes described by the therapist as vividly as possible. Details of the procedure and a brief example of an imaginal scene have been described elsewhere (Foa and Chambless, 1977).
(b) Exposure in Gvu-Gradual exposure in uiuo to situations which evoke discomfort and the urge to ritualize was conducted daily. Each day a new discomfort-arousing situation was added to the previous ones; the most disturbing situation was presented by the fifth day. During the second week of treatment patients were confronted with all stimuli combined. They were instructed to further expose themselves to the same stimu- lus situations for at least 2 hr between sessions; this homework was continued on the weekends.
An example of in viva exposure treatment for a patient who checked lights, windows. doors and the basement gate, as well as checking the toilet before flushing and retracing his route after driving is as follows: In the first session he was required to turn lights and appliances on and off once. After each action he was instructed to leave the room immediately and focus his attention on his failure to check. This procedure was repeated for 2 hr using different switches. The second session consisted of exposure to situations from the first session with the addition of opening and closing doors and windows. Repeated flushing of the toilet without looking into the toilet bowl was added in the third session and the basement gate in the fourth session. By session five the patient was asked to drive alone on the highway without retracing his route. He reported to the therapist every 20 min.
(c) Response prevention-Patients were not permitted to engage in any ritualistic behavior from the first session. Normal checking was allowed (e.g., one check of the door before leaving home). Response prevention was conducted at home or in the hospital under the supervision of relatives, friends or hospital staff. The supervisor was instructed to stay with the patient at his or her request whenever an urge to check was difficult to resist. Force was not used, but any violations of response prevention were reported to the therapist.
(3) Follow-up. All patients received a set of instructions to be followed for several weeks. These included a list of items which the patient was permitted to check once a day. Concomitantly, deliberate exposure to situations which previously evoked urges to check was requested. Three patients from group 1 and five patients from group 2 received additional treatment on a once-a-week basis for other problems, e.g., social skills training and marital therapy. The mean number of additional sessions for group 1 was 14 and for group 2, 18.
Measures
Independent assessor. On the basis of .a 45-60 min interview an independent assessor rated each patient on the following six scales: severity of compulsions, obsessions and urges to ritualize, main fear, avoidance, and severity of obsessive-compulsive symptoms. All scales ranged from 0 (no symptoms) to 8 (severe symptomatology). In addition, severity of depression was rated on a 0 to 8 scale. The assessor was instructed to collect information about the patients’ behavior, life style, daily activities, etc. These data pro- vided the basis for his ratings. He was specifically instructed to avoid requesting patients to evaluate themselves.
RESULTS
To ensure that the two groups were initially similar, a Fisher’s exact test was per- formed on the following variables: age, sex, work status, hospitalization during treat- ment, the degree of therapist’s experience and additional sessions after the experimental

EDNA B. FOA, GAIL STEKETEE, RALPH M. TURNER and STEVEN C. FISCHER 452
6
I I I I I I I I I
PRE POST FOLLOW UP PRE POST FOLLOW UP PAE POST FOLLOW UP
COMWLSIONS OBSE!BIONS URGES
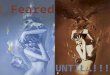
Fig. 1. Mean severity of compulsions, obsessions and urges for the two experimental groups at pre- and post-treatment and at follow-up (mean 11 months).
0
7
6
5
s
;4
3
2
I
*
X \
\
\ \ \
\
\
\..
\ \
\ X-.
X
I I I I 1 I I I 1
PM POST FOLLOW UP PRE POST FOLLOW UP PRE POST FOLLOW UP
MAIN FEAR AVOIVANCE O-C SYIlPTOw3
Fig. 2. Mean severity of main fear, avoidance and overall obsessive-compulsive symptoms for the two experimental groups at pre- and post-treatment and at follow-up (mean 11 months).

Exposure to feared disasters 453
Table 1. Probabilities associated with the Z scores calculated for the Mann- Whitney fI test
Variable Pre-test Occasion Post-test Follow-up
Obsessions 0.39 0.42 0.06 Compulsions 0.41 0.40 0.04 Urges to ritualize 0.16 0.36 0.05 Main fear 0.21 0.42 0.21 Avoidance 0.32 0.36 0.21 O-C symptoms 0.01 0.33 0.03
program. Groups did not differ significantly on any of these variables. In addition, no significant differences between groups were detected when a one way analysis of variance was conducted on severity of depression (F = 0.397, p = 0.54), duration of symptoms (F = 1.747, p = 0.21) and years of education (F = 0.377, p = 0.92).
The mean severity of symptoms as rated on the six scales (obsessions, compulsions, urges to ritualize, main fear, avoidance and obsessive-compulsive symptoms) was calcu- lated separately for each group on the following three occasions: before treatment, after treatment and at follow-up. These are depicted in Figs. 1 and 2. Inspection of these figures suggests the absence of differences between the groups at pre- and post-treatment. At follow-up group 1 (imaginal and in uioo exposure) retained improvement more than did group 2 (exposure in uiuo alone).
Since the present data do not meet the assumptions underlying the t test, the Mann- Whitney U Test was selected to test differences between groups. After calculating the V values, a correction for ties was performed. The probabilities associated with the values of the resulting 2 scores are presented in Table 1. At pre- and post-test no significant differences between the two groups were detected, with the exception of obsessive- compulsive symptoms on which the groups differed at pre-test only (p = 0.01). At fol- low-up groups 1 and 2 were significantly different on four of the six dependent variables: obsessions (p = 0.06) compulsions (p = 0.04), urges to ritualize (p = 0.05) and obsessive- compulsive symptoms @ = 0.04). On main fear and avoidance, no significant differences were found.
DISCUSSION
The data obtained in the present study partially support the hypothesis that obsessive- compulsives with checking rituals who received both imaginal exposure to feared disas- ters and in yivo exposure to tangible cues will show more improvement than those exposed in viuo only. While at the end of treatment no differences between the two groups were detected on any of the six measures, at follow-up patients that did not receive imaginal exposure evidenced more relapse on four of the six dependent measures. The remaining two measures showed the same trend. Thus the treatment that included imaginal exposure seemed to effect more stable gains than did exposure in uivo alone. While the lack of control groups limits this conclusion, it should be noted that all patients had received more than 10 sessions of psychotherapy prior to the present study with no reported reduction in symptomatology. Moreover, no changes were evident during 3 weeks of no treatment prior to behavior therapy (Foa and Goldstein, 1978).
Additional treatment given during the follow-up period cannot account for the observed differences between the groups, since patients in both groups received approxi- mately the same number of follow-up sessions (14 for group 1 and 18 for group 2). Furthermore, of those who received more therapy, six showed various degrees of relapse and three remained stable or improved further. In contrast, of the six patients who had no further treatment, five maintained or improved upon their gains and only one relapsed. The greater number of relapses observed among those who received further treatment can be attributed to the presence of additional problems in those patients. However, a nearly equal number’ of patients from each group (4 and 5) required more

454 EDNA B. FOA. GAIL STEKETEE, RALPH M. TURNER and STEVEN C. FISCHER
treatment; therefore, this factor again cannot account for the differences between the two groups.
The results of the present study are not congruent with those reported in the literature. As noted previously, with agoraphobics the addition of flooding in imagination was not found to enhance improvement achieved by in uiuo exposure only (Emmelkamp, 1974; Emmelkamp and Wessels, 1975; Everaerd, Rijken and Emmelkamp, 1973), despite the fact that imaginal exposure by itself has been demonstrated effective (e.g., Boulougouris, Marks and Marset, 1971).
Generally, variants of exposure in uiuo have been found equally effective. The addition of modeling to exposure in uiuo did not improve outcome (Boersma et al., 1976; Emmel- kamp, 1976; Emmelkamp and Emmelkamp-Benner, 1975; Marks, Hodgson and Rach- man, 1975). Likewise, exposure with a therapist did not differ from self-exposure (Emmel- kamp and Kraanen, 1977). Only on variables affecting the ‘quantity’ of exposure, that is direct vs vicarious exposure in uiuo (Roper, Rachman and Marks, 1975) and long vs short duration of exposure (Rabavilas, Boulougouris and Stefanis, 1976; Stern and Marks, 1973) were differences among groups observed. Perhaps, then, in uiuo exposure is such a powerful manipulation that a ceiling effect for improvement results, thus obscuring the impact of procedural variations. Our results at post-test are congruent with such a supposition, as is the picture which emerged when we analyzed the results of a short term follow-up of only 3-6 months. At that point patients who received in uiuo exposure bnly manifested more relapse, but no significant differences between the two groups were detected (Foa, Steketee and Turner, 1978); yet, after a longer follow-up period this trend continued and resulted in the marked group differences reported here. Can it be that the effects of procedural variations are not immediate but rather assisr in maintenance of gains over time? The failure to detect differences between exposure modalities in the experi- ments discussed above might then be due to the fact that follow-up did not exceed 6 months and in most studies was only 1-3 months.
Why did exposure to contact cues alone effect the same reduction of subjective anxiety and urges to ritualize which was obtained by exposure to both contact cues and feaied disasters? We suggest that exposure in uiuo may produce short term habituation to feared disasters, whereas imaginal exposure specifically directed at such feared consequences may result in long term habituation, therefore consolidating treatment gains. Thus, a match between a patient’s fear model and the content of exposure might be necessary for the maintenance of improvement if not for the immediate gain. Because no direct behav- ioral observations were recorded and because our results deviate from the ‘no difference pattern’ found throughout the literature, a replication of this study is in order.
REFERENCES BOERSMA K., DEN HENGST S. D., DEKKER J. and EMMELKAMP P. M. G. (1976) Exposure and response prevention
in the natural environment: A comparison with obsessive-compulsive patients. Behau. Res. Ther. 14, 19-24. BOULOUG~URIS J. C.. MARKS I. M. and MARSET P. (1971) SuDerioritv of flooding (imolosion) to desensitization
for reducing pathological fear. Behau. Res. Th&. 9, i-18. _ _. .
EMMELKAMP P. M. G. (1974) Self observation versus flooding in the treatment of agoraphobia. Behau. Rex Ther. 12229-237.
EMMELKAMP P. M. G. and EMMELKAMP-BENNER A. (1975) Effects of historically portrayed modeling and group treatment of self-observation: A comparison with agoraphobics. Behau. Res. Ther. 13. 135-139.
EMMELKAMP P. M. G. and KRAANEN J. (1977) Therapist-controlled exposure in viuo: A comparison with obsessive-compulsive patients. Behau. Res. Ther. 15, 491-495.
EMMELKAMP P. M. G. and WE~~EL.S H. (1975) Flooding in imagination vs flooding in viuo: A comparison with agoraphobics. Behau. Res. Ther. 13, 7-15.
EVERMRD W. T. A. M., RUKEN H. M. and EMMELKAMP P. M. G. (1973) A comparison of ‘flooding’ and ‘successive approximation’ in the treatment of agoraphobia. Behau. Res. Ther. 11. 105-l 17.
FOA E. B. and CHAMBLESS D. L. (1977) Habituation of subjective anxiety during flooding in imagery. Behau. Res. Ther. 16, 391-399.
FOA E. B. and GOLDSTEIN A. (1978) Continuous exposure and complete response prevention in the treatment of obsessive-compulsive neurosis. Behau. Ther. 9. 821-829.
FOA E. B., SIZKETEE G. and TURNER R. M. (1978) Effects of exposure to disastrous ruminations in obsessive- compulsive checkers. Paper read at the Annual Conference of the British Association for Behaviour Psychotherapy, July 2. 1978, Stirling, Scotland.

Exposure to feared disasters 455
LANG P. J. (1977) Imagery in therapy: An information processing analysis of fear. Behau. Ther. 8, 862-886. MARKS I. M., HODGKIN R. and RACHMAN S. (1975) Treatment of chronic obsessive-compulsive neurosis by in
oiuc exposure: A two-year follow-up and issues in treatment. Br. J. Psychist. 127, 349-364. MATTHEWS A. M., JOHNSTON D. W., LANCASHIRE M., MUNBY M., SHAW P. M. and GELDEX M. G. (1976)
Imaginal flooding and exposure to real phobic treatment outcome with agoraphobic patients. Br. J. Psychiat. 129, 362-371.
RA~AVILAS A. D., BOULOUG~URIS J. G. and STEFANIS C. (1976) Duration of flooding sessions in the treatment of obsessive-compulsive patients. Behao. Res. Ther. 14, 349-355.
RACHMAN S. (1976) Obsessional-compulsive checking. Behav. Res. Ther. 14, 269-277. ROPER G., RACHMAN R. and MARKS I. M. (1975) Passive and participant modelling in exposure treatment of
obsessive-compulsive neurotics. Behao. Res. Ther. 13,271-279. STERN R. S. and MARKS I. M. (1973) Brief and prolonged flooding: A comparison in agoraphobic patients.
Archs gen. Psychiar. UI, 270-276.