Embed Size (px)
Citation preview

Economics of Early Childhood Development
Prashant Bharadwaj University of California, San Diego & NBER
(with various co-authors)
Introduction
Prashant Bharadwaj, UCSD
• Health and education are important for economic growth
• Health is an important input into the production of education • Recent literature emphasizes early childhood health

Introduction
Prashant Bharadwaj, UCSD

• What are some determinants of early childhood health? – Maternal education – Maternal behavior – Gender preferences – Air quality & environmental factors
• What are some consequences of early childhood health? – Mortality – Cognitive outcomes – Resilience to economic shocks
• Can policy help those born with poor health? – Medical interventions in early childhood
Research questions
Prashant Bharadwaj, UCSD

• Many ways to answer these questions
• Sometimes RCTs are not possible
• My approach: administrative and pre-existing survey data
• Allows us to study similar questions in broad variety of settings
• External validity & direct policy analysis
Overall approach to research
Prashant Bharadwaj, UCSD
• Maternal education – Zimbabwe, Mozambique & Namibia
• Maternal smoking & smoking bans - Norway
• Gender preferences – India, Bangladesh, China, Pakistan, Sri Lanka, Thailand, Ghana
• Environmental exposure - UK
• Birth weight and cognitive outcomes – Chile
• Birth weight and income - Sweden
• Medical interventions in early childhood – Chile and Norway
Countries visited in this talk
Prashant Bharadwaj, UCSD

Maternal education and child mortality in Zimbabwe
Prashant Bharadwaj, UCSD & NBER Karen Grepin, NYU Wagner

This paper
• Examine the role of maternal education on child survival in Zimbabwe
• Examine fertility related responses to increased education
• Role of intermediate factors in explaining this relationship – healthy behaviors, vaccinations, female empowerment etc
Education under colonial rule
• Racially segregated school system
• Only a few secondary schools available to blacks, almost all in urban areas
• Limited secondary school enrollment for black girls
• Relatively high quality by regional standards

Education in Zimbabwe 1980
• Education a bit political priority for Marxist oriented ZANU-PF
• First education reforms announced in 1979
• End of the war allowed children to re-enter schools
• School fees reduced/removed
• Rapid construction of secondary schools

Expansion of schools

Data
• 5 rounds of the DHS: 1988, 1994, 1999, 2005-06, 2010-11
• 2 measures of schooling: years of schooling completed, attended any secondary school
• Survival: whether child alive at the time of survey, whether child survived past age 1, survived past age 5
• Other fertility and health utilization outcomes also collected

Age at the time of reform and education - Mothers

Maternal vs Paternal education

Child mortality

Heterogeneity in child mortality

Child mortality by birth order

Fertility related outcomes

Child Health

Was it something about “independence”?

Was it something about “independence”?

Smoking bans, Maternal smoking and Birth outcomes
Prashant Bharadwaj, UCSD & NBER Julian V. Johnsen, University of Bergen
Katrine V. Loken, University of Bergen & IZA

Introduction An important externality of smoking is the harm it might
cause to non-smokers. • Adults and children: passive smoking • In utero: active and passive smoking A vast medical literature has examined the (mainly negative)
association between smoking and various health outcomes. Governments all over the world have adopted policies to
deter its citizens from smoking – public information, ad campaigns, taxes, age restrictions
and smoking bans in public areas.
Smoking Bans – Bharadwaj, Johnsen and Loken (2013)

Introduction Smoking bans in public areas • World wide policy (e.g. common in European countries, 50
% of Americans lives under bans prohibiting smoking in public areas)
We will study effects on infant birth outcomes, regardless of
mother's smoking status. • Hence, the change in the negative externality in this case
are a combination of – Active smoking: maternal behavior change (likely to occur
as a result of the law) – Passive smoking: reduction in smoke exposure due to
others not being allowed to smoke.
Smoking Bans – Bharadwaj, Johnsen and Loken (2013)

Introduction
Norway extends smoking ban to restaurants and bars in June 2004.
Research design • Differences in differences strategy comparing – mothers giving birth before reform (exposed to
smoking) and after reform (not exposed to smoking)
– mothers in treated occupation (restaurants and bars) and mothers in control occupations
Smoking Bans – Bharadwaj, Johnsen and Loken (2013)

Smoking Bans – Bharadwaj, Johnsen and Loken (2013)

Empirical strategy
• Differences-in-differences strategy Yijt=α1+α2 Treatj+α3 Postt+α4(Treatj*Postt)+α5 Xijt+εijt α4 is the reduced form effect of the reform on
outcomes Y • Close to 100 % compliance: Almost all mothers in
sample likely to be treated.
Smoking Bans – Bharadwaj, Johnsen and Loken (2013)
Data
Different administrative data sets linking children to mothers and fathers through unique identifiers.
Medical birth register 1967-2010: • information on birth weight, gestational age, APGAR
scores, smoking behavior of pregnant women Linked to other administrative data: • information on type of occupation (NACE codes),
annual income, sickness absence, educational outcomes
Smoking Bans – Bharadwaj, Johnsen and Loken (2013)

Smoking Bans – Bharadwaj, Johnsen and Loken (2013)

Smoking Bans – Bharadwaj, Johnsen and Loken (2013)

Smoking Bans – Bharadwaj, Johnsen and Loken (2013)
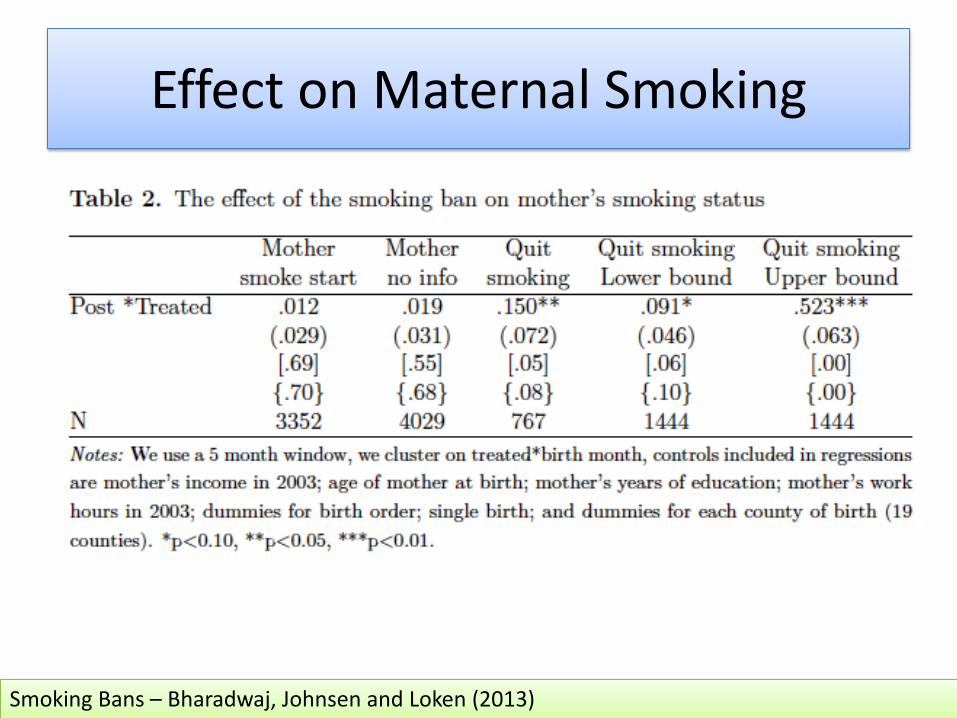
Effect on Maternal Smoking
Smoking Bans – Bharadwaj, Johnsen and Loken (2013)

Effects by smoking status

Sibling fixed effects estimates
Smoking Bans – Bharadwaj, Johnsen and Loken (2013)

Synthetic control group

Placebo tests

Conclusion We find a positive effect of smoking ban on lower tail of the
birth weight distribution • 1.9 pp fewer children born with Very Low Birth Weight
(<1500 gram) • 2.5 pp fewer children born with Low Birth Weight (<2000
gram) • 2.6 pp fewer children born pre-term (before gestational
week 37) Make some progress on understanding mechanisms: • active smoking: mothers in restaurant/bars more likely to
quit smoking as a result of the reform • passive smoking: no effects for children of mothers who
do not smoke
Smoking Bans – Bharadwaj, Johnsen and Loken (2013)

Discrimination begins in the womb: Evidence of sex selective prenatal investments
Prashant Bharadwaj, UCSD & NBER Leah K. Lakdawala, Michigan State University

Introduction Sex discrimination
Bharadwaj & Lakdawala
• Sex-based discrimination is a major concern in various parts of South and Southeast Asia
• Two important questions:
1. What is the extent of sex discrimination?
2. Why does sex discrimination occur?
• Documentation of discrimination is quite difficult

Introduction Discrimination in prenatal care
Bharadwaj & Lakdawala
• Relatively under-explored channel of sex discrimination
• Why examine prenatal care?
• Large literature on the impact of in utero events
• Early life health is important for later life success
• Example: Neonatal tetanus
• Even if sex-selective abortion can be prevented, this channel of discrimination might persist and have long term impacts

Introduction Preview of results
Bharadwaj & Lakdawala
• Mothers in India are 1.1 percentage points more likely to visit antenatal clinics when pregnant with a boy
• Gender gap in tetanus immunization accounts for 4-10% of excess female neonatal mortality
• In Northern India:
• 4.6% more likely to visit antenatal clinics
• 3% more likely to receive tetanus shots
• 16% more likely to deliver in non-home facility
• Similar results found in data from China, Pakistan and Bangladesh

Bharadwaj & Lakdawala
Methodology and problems Basic specification
Carei = β Malei + α Fi + ui
We start with the most basic specification
Care: Prenatal care (number of visits, tetanus shots etc) Male: dummy variable for whether the child was male or not F: observed covariates (mother’s characteristics, birth order, gender composition etc)
Under equal treatment we do not expect β to have any predictive power

• Reverse causality: what if prenatal check ups cause male births?
• Prenatal check ups sex determination females aborted higher correlation between males and prenatal care
• Examine decision to attend prenatal care conditional on having made at least one prenatal visit
• Also exploit timing of prenatal visit
Bharadwaj & Lakdawala
Methodology and problems Problem – Sex selective abortions
Bharadwaj & Lakdawala
Methodology and problems Problem – Sex-selective abortions
• Other omitted variables: what if mothers who choose sex-selective abortion have different preferences/characteristics that also drive the decisions to use prenatal care?
• Wealth, education, and gender composition of previous children are highly predictive of who uses abortion
• Use mother fixed effects to get rid of time invariant characteristics

Bharadwaj & Lakdawala
Methodology and problems Problem – Selective recall
What if mothers selectively remember prenatal care when they have a boy?
• Mothers should then always selectively remember, even for periods when ultrasound technology was not widespread
• Exploit knowledge of timing of 1st prenatal check up
• Ultrasound receipt should not matter for results under this hypothesis

Bharadwaj & Lakdawala
Methodology and problems Problem – Medical complications
What if male fetuses require more attention from a medical perspective?
• While male fetuses are more fragile, recommendations regarding basic prenatal checks do not vary by sex of the fetus
• Have direct data on medical complications during pregnancy
Data
Bharadwaj & Lakdawala
• India: 1992, 1998 and 2004 NFHS
• women between the ages of 15-49
• prenatal care information on the youngest child born within 5 years of survey date
• ultrasound information in 1998 (sub sample) and 2004
• Other countries: various DHS samples
• China: Health and Nutrition Survey (various years)

Bharadwaj & Lakdawala
Results Using ultrasound data
Full Sample Northern Region At least 2 Antenatal
Visits Tetanus Shot At least 2 Antenatal Visits Tetanus Shot
1998 and 2004 samples restricted to mothers who have been to antenatal clinic at least once
Ultra No Ultra Ultra No Ultra Ultra No Ultra Ultra No Ultra
(1) (2) (3) (4) (5) (6) (7) (8) Male 0.530** 0.117* 0.170 0.041 0.692** 0.080 0.938** 0.110
(0.223) (0.061) (0.233) (0.080) (0.299) (0.118) (0.396) (0.153) Constant 3.184*** 2.388*** 5.517*** 2.292*** 2.226 0.362 5.690*** 1.809**
(1.086) (0.300) (1.137) (0.307) (1.441) (0.575) (1.852) (0.822) P-value of the test that the coefficient on Male is the same in the with and without ultrasound samples
0.074 0.600 0.057 0.051

Bharadwaj & Lakdawala
Results Mother fixed effects
Prenatal Care
Number of Prenatal visits Tetanus Shot
Number of Tetanus Shots
Iron Pills Non-Home Delivery
(1) (2) (3) (4) (5) (6) Male 0.022 0.112* 0.031** 0.082** 0.029* 0.004
(0.015) (0.064) (0.015) (0.034) (0.016) (0.013) Birth Order 0.017 0.209 0.018 0.016 0.032 -0.019
(0.041) (0.181) (0.040) (0.095) (0.043) (0.036) Existing Sex Ratio of Children 0.020 0.093 -0.017 -0.021 0.006 -0.016
(0.018) (0.084) (0.018) (0.044) (0.021) (0.017) Mean of Dependent Variable 0.626 2.297 0.715 1.460 0.544 0.267
Number of Mothers 3968 3962 3956 3956 3982 3969

Bharadwaj & Lakdawala
Results Basic specification – previous children female

Bharadwaj & Lakdawala
Results Other countries
Coefficient on Male in various countries
Prenatal Care (1=Yes, 0=No)
Number of Prenatal visits
Tetanus Shot (1=Yes, 0=No)
Number of Tetanus Shots
Non-Home Delivery
(1=Yes, 0=No)
(1) (2) (3) (4) (5) China 0.046* 0.346* na na
(0.027) (0.205) Bangladesh 0.003 0.076** 0.028*** 0.039* 0.001
(0.009) (0.037) (0.009) (0.021) (0.003) Pakistan 0.018 0.184* 0.020 0.016 0.006
(0.015) (0.100) (0.016) (0.039) (0.014) Pakistan (Punjab Region) 0.019 0.268* 0.015 0.014 0.026
(0.021) (0.152) (0.023) (0.056) (0.020) Sri Lanka 0.002 na 0.010 na 0.014
(0.008) (0.016) (0.014) Thailand 0.005 na 0.020 na 0.014
(0.017) (0.022) (0.018) Ghana -0.013** 0.010 0.004 0.003 0.003 (0.006) (0.078) (0.009) (0.024) (0.010)

Bharadwaj & Lakdawala
Conclusions
• Discrimination in prenatal care is a potential problem
• Mothers in India (particularly in the North) appear to take better care of male fetuses compared to female fetuses
• Discrimination in tetanus shots can explain between 4-10% of excess female neonatal mortality
• Anti-abortion laws might not get around this problem

Long Term Impacts of Exposure to the Great London Smog
Prashant Bharadwaj, UCSD & NBER Josh Graff Zivin, UCSD
Jamie Mullins, Umass Amherst Matthew Neidell, Columbia

Bharadwaj & Lakdawala
The Great Smog of 1952
• Severe weather event in London in December 1952
• 5 day (Dec. 5th-9th) event of extreme ambient air pollution attributed to: – a temperature inversion – cold ground temperatures – windless conditions
• Approximately 12,000 “extra” deaths during event and in subsequent 2 months
• Led to the Clean Air Act of 1956

Bharadwaj & Lakdawala
The Great Smog of 1952

Bharadwaj & Lakdawala
Effects during childhood

Bharadwaj & Lakdawala
Long run effects

Consequences of early childhood health: the case of birth weight
Prashant Bharadwaj, UCSD
• Birth weight considered the most important measure of infant health and development
• Policy in both developed and developing countries focuses on improving birth weight and decreasing incidence of low birth weight
• We use birth weight as an input in the production of cognitive achievement


Prashant Bharadwaj, UCSD
Birth weight and test scores Questions we hope to answer
• Does birth weight affect intermediate outcomes like educational achievement?
• A potential mechanism via which birth weight affects later life outcomes
• Does the effect of birth weight on academic achievement persist?
• If birth weight is an “intervention” what happens to its effect over time?
• Do parents invest differentially based on birth weight?

Prashant Bharadwaj, UCSD Prashant Bharadwaj, UCSD
Birth weight and test scores Preview of results
• Birth weight matters for academic success: a 10% increase in birth weight improves scores in math by 0.05 SD
• Low birth weight children realize scores that are up to 0.13 SD less
• Large scale education interventions in developing countries realize gains of 0.15-0.4 SD
• This effect appears to persist in some cases
• Suggested reason for this pattern: parental investments might “make up” for lower birth weight

Prashant Bharadwaj, UCSD
Birth weight and test scores Problems with estimation
• Birth weight could be correlated with other attributes that could affect school performance
• For example:
• Richer mothers have better performing children and children of higher birth weight
• Parents might devote more time to children with lower birth weight and parental time affects school performance
• Need to overcome omitted variables bias
Birth weight and test scores Identification strategy – Twins fixed effects
Prashant Bharadwaj, UCSD
• We examine birth weight and test score patterns by examining twins
• A pretty old idea in the labor/development literature
• Observed and unobserved family characteristics are identical for twin pairs
• Added assumption: parents do not practice differential investments between twins, based on birth weight
• Data allows us to partially test this assumption

Twins

Birth Weight Differentials among Twins
Prashant Bharadwaj, UCSD
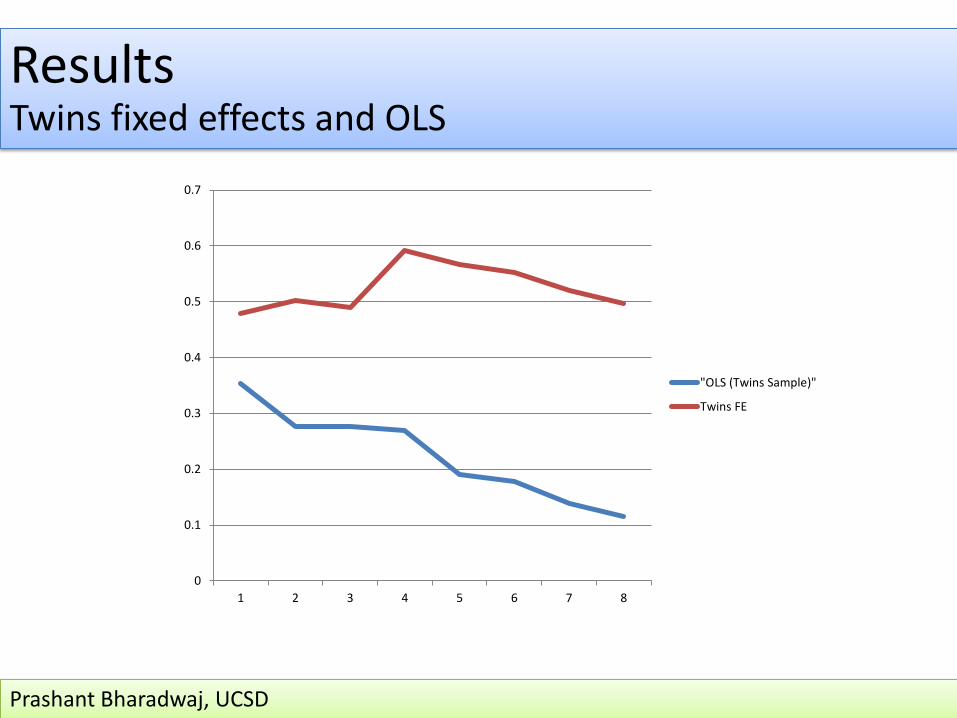
Results Twins fixed effects and OLS
Prashant Bharadwaj, UCSD
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
1 2 3 4 5 6 7 8
"OLS (Twins Sample)"
Twins FE

Discussion Data on parental investments
Prashant Bharadwaj, UCSD
• Survey to parents part of SIMCE • Extensive questions on parental involvement with children
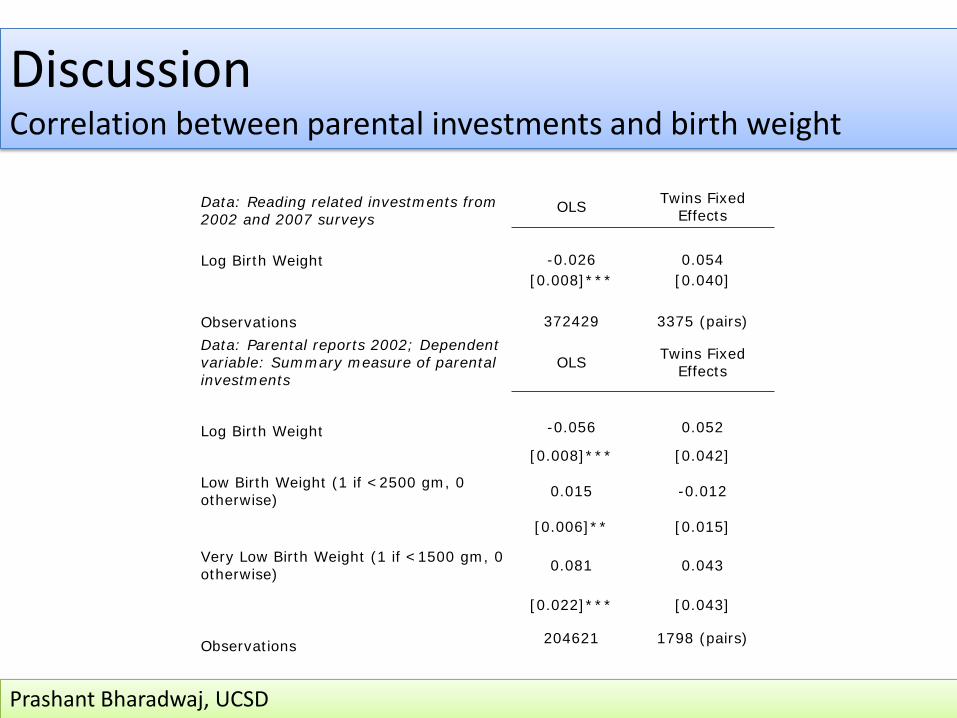
Discussion Correlation between parental investments and birth weight
Prashant Bharadwaj, UCSD
Data: Reading related investments from 2002 and 2007 surveys
OLS Twins Fixed Effects
Log Birth Weight -0.026 0.054 [0.008]*** [0.040]
Observations 372429 3375 (pairs) Data: Parental reports 2002; Dependent variable: Summary measure of parental investments
OLS Twins Fixed Effects
Log Birth Weight -0.056 0.052
[0.008]*** [0.042]
Low Birth Weight (1 if <2500 gm, 0 otherwise) 0.015 -0.012
[0.006]** [0.015]
Very Low Birth Weight (1 if <1500 gm, 0 otherwise) 0.081 0.043
[0.022]*** [0.043]
Observations 204621 1798 (pairs)

Discussion Correlation between parental investments and birth weight
Prashant Bharadwaj, UCSD
Individual investment variables from 2002 OLS Twins Fixed
Effects Investment detail:
Give books to child 0.001 -0.021 [0.016] [0.070]
Review homework with child -0.081 0.052 [0.012]*** [0.079]
Do homework with child -0.111 -0.054 [0.014]*** [0.085]
Study with child -0.123 -0.045
[0.014]*** [0.089] Read stories to child -0.108 0.058
[0.015]*** [0.081] Pose math problems to child -0.046 0.071
[0.013]*** [0.061] Talk to child -0.002 0.027
[0.009] [0.046] Make child do errands 0.038 0.063
[0.014]*** [0.065] Make child write short texts -0.14 0.191
[0.016]*** [0.094]** Play games with child 0.002 0.06
[0.015] [0.102] Write the child messages -0.026 0.103
[0.017] [0.090] Incetivize child to read -0.048 0.066
[0.014]*** [0.081]

Discussion Correlation between parental investments and birth weight
Prashant Bharadwaj, UCSD
Child reports of parental investments
1 2
Data: Student self reports 2009 OLS Twins Fixed Effects
Summary measure of investment -0.018 0.072 [0.004]*** [0.058] Observations 179740 1827 (pairs)
Investment detail: OLS Twins Fixed Effects
Explains matter I do not understand -0.042 0.291 [0.007]*** [0.125]**
Helps me study -0.032 0.088
[0.009]*** [0.134]
Goes over material with me before a test -0.028 0.149
[0.008]*** [0.134]
Helps me do chores -0.025 -0.057
[0.009]*** [0.156]
Checks my homework -0.017 0.193 [0.009]* [0.171] [0.007]*** [0.133]

Discussion Twins fixed effects vs Siblings fixed effects
-0.3
-0.2
-0.1
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
1 2 3 4 5 6 7 8
Twins FE
Siblings 1 year apart
Siblings 5 years apart
Prashant Bharadwaj, UCSD

Health Endowments and Unemployment during Macroeconomic Crises
Prashant Bharadwaj, UCSD & NBER Petter Lundborg, Lund University
Dan-Olof Rooth, Linneaus University

Introduction
• Economic fluctuations can have heterogeneous impacts
– Who is affected during economic downturns?
• Inequality can increase during recessions
• Presence of a social safety net can mitigate some of these effects
Bharadwaj, Lundborg & Rooth

Context & Questions
• Economic crisis in Sweden in the early 1990’s
• Unemployment went from 2% to 12% in a year
• Were low birth weight adults more likely to lose their jobs?
– Is this all due to occupational sorting pre-crisis?
• Does the presence of a strong social safety net help?
Bharadwaj, Lundborg & Rooth

Unemployment rate 1980-2010. Swedish LFS
24
68
1012
1980 1985 1990 1995 2000 2005 2010Year
Unemployment

Twins FE – UI Take Up
Bharadwaj, Lundborg & Rooth

Twins FE – UI Take Up Private Sector
Bharadwaj, Lundborg & Rooth

Conclusions
Bharadwaj, Lundborg & Rooth
• Economic downturns affect those born with poor health
• Potentially important source of heterogeneity when examining impacts of recessions
• Presence of a social safety net appears incredibly important
• Policy conclusions

Medical interventions and school achievement
• Do medical interventions at birth matter for later life achievement?
• We examine whether medical attention given to very low birth weight newborns has long term impacts on academic achievement
• Two main challenges in answering question of interest:
– Health interventions not randomly assigned
– Parental behaviors might respond to health intervention
Prashant Bharadwaj, UCSD

VLBW Classification • Very Low Birth Weight (VLBW) classification is for children born below 1500 grams
at birth
• Extensive medical literature focusing on what to do with VLBW infants
• “There also are standardized protocols for the treatment of newborns who weigh <1500 g and for cases of respiratory distress syndrome.” (Gonzalez et al, Pediatrics, 2000)
• Cutoffs however, are somewhat arbitrary:
• “Birth weight is a continuous variable and the limit at 2,500 grams does not represent a biologic category, but simply a point on a continuous curve. The infant born at 2,499 grams does not differ significantly from one born at 2,501 grams on the basis of birth weight alone...As with the 2,500 gram limit, designation of very low birth weight infants as those weighing 1,500 grams or less reflected convention rather than biologic criteria.” (ADKW 2010, IOM 1985)
Prashant Bharadwaj, UCSD

What happens to VLBW infants in Chile?
Technical Guidance – Monitoring of infants below 1500 grams or less than 32 weeks gestation (1999 publication)

• All infants of BW less than 1500 g should be treated in the Neonatal Service at tertiary level, since most likely require Intensive Care Unit (NICU). Should be treated in the best possible conditions, making it important presence in the immediate attention of a Neonatologist and specialized Matron. The clinical characteristics of each patient determine the need for additional laboratory tests, imaging and procedures.
• Thermoregulation: Transfer of RN transport incubator to the NICU. Radiant heat
cradle if you need multiple procedures. (Must be transferred as soon as possible to an intensive care incubator, ideally within 3 hours). Incubator should be preferred initially intensive care if it does not require multiple procedures. Cover with plastic cover for newborn to prevent insensible water loss.
What happens to VLBW infants in Chile?
from: www.prematuros.cl (Commission of Neonatalogy, Chile)
Prashant Bharadwaj, UCSD

Prashant Bharadwaj, UCSD

Prashant Bharadwaj, UCSD

NICUs in Chile
• 28 NICUs, 1 in each region starting in 1991
• National standards set in 1991 for providing care at NICUs
• Drastic reductions in infant and neonatal mortality between 1991-2000
• Almost 99% of all births occur under skilled care
• 68% of births occur in a regional hospital with access to NICU
Prashant Bharadwaj, UCSD

Empirical Approach
• Regression discontinuity design
– Infants just below 1500 grams and or less than 32 weeks more likely to get treatment than infants just above 1500 grams
– Examine test scores many years later for children born above and below these cut offs
– Pre and post 1998 results likely indicative of the impact of the surfactant program
Prashant Bharadwaj, UCSD

Empirical Specification
- Bandwidth of 100 grams chosen. Results largely robust to various bandwidths - Polynomials do not alter results too much, depending on bandwidth
Prashant Bharadwaj, UCSD



Prashant Bharadwaj, UCSD

Math Scores and Birth Weight
Prashant Bharadwaj, UCSD
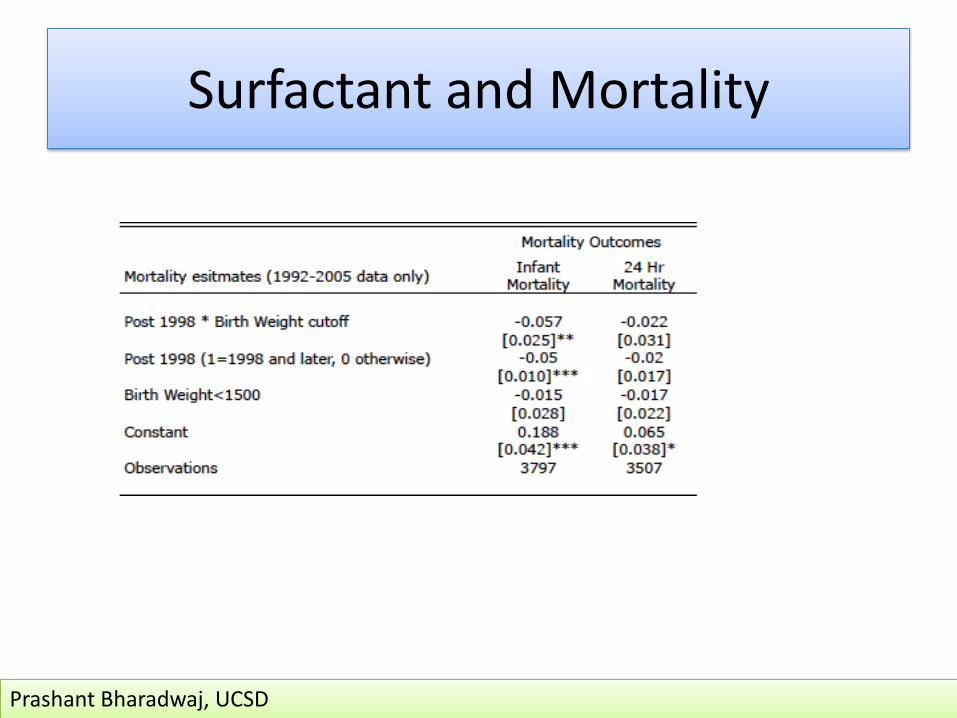
Surfactant and Mortality
Prashant Bharadwaj, UCSD

Prashant Bharadwaj, UCSD
Conclusions and Future work
• Birth weight is an important determinant of test scores
• Parental investments could matter for the long run effect
• Medical interventions in early childhood have a lasting impact on school achievement
• Future work: Better understanding parental investments
• Role of knowledge and income constraints in Nepal
• Role of parental disability on child outcomes





























