Embed Size (px)
Citation preview

Antibiotic resistance is a worldwide problem associated with increased average length of stay, higher healthcare costs and increased mortality1-4. Enterococcus is among the top causes of bloodstream infection, infective endocarditis, intra-abdominal sepsis, and surgical site infections5-9. Vancomycin-resistanct Enterococci (VRE) first emerged in the 1980s and prevalence continues to increase5,10-12. VRE infection has long been associated with higher patient mortality, with at least part of the harms related to inadequate empiric antibiotic treatment3. A recent study found that a delay of greater than two days in effective therapy for Enterococcal infections was associated with a three-fold increase in 30-day mortality and that this delay was solely associated with vancomycin-resistance13. There is a need to predict vancomycin resistance in Enterococcus sterile isolates while susceptibility test results are pending. Screening swabs for AROs are attractive for this purpose because they are widely used in clinical practice and because they are frequently drawn on admission to hospital, with results available earlier than culture data. Screening swabs for MRSA have recently been demonstrated to have high specificity for predicting subsequent MRSA infections once Staphylococcus has been implicated as the causative organism, with high sensitivity demonstrated when drawn within 48 hour of cultures14. This study seeks to investigate the utility of screening VRE swabs for predicting vancomycin-resistance among subsequent Enterococcal sterile-site infections. We predicted that positive screening VRE swabs will reliably predict Enterococcal sterile culture vancomycin-resistance but that negative screening VRE swabs will be unreliable.
The Predictive Utility of Screening VRE Swabs in Selecting Empiric Antibiotics for Sterile-Site Infections Ian Brasg MD, Department of Medicine, University of Toronto, Marion Elligsen RPh, Department of Pharmacy, Sunnybrook Health Sciences Centre,
Derek MacFadden MD FRCPC, Division of Infectious Diseases, University of Toronto, and Nick Daneman MD MSc FRCPC, Division of Infectious Diseases & Clinical Epidemiology, University of Toronto, Toronto, ON, Canada
Methods
Abstract
Background
Results
Discussion
References
Background: Vancomycin-resistant Enterococcus (VRE) screening swabs are performed widely as a means of identifying VRE carriers and prevention transmission. We tested whether these results could have unintended benefits in predicting the vancomycin susceptibility of subsequent infections with Enterococcus experienced by these patients. Methods: A retrospective cohort study was conducted using an auto-populated antimicrobial stewardship database. Patients were included if 18 years of age or older, admitted to hospital between 2010 and 2015, and screened for VRE prior to developing an Enterococcus sterile-site infection. Test characteristics were derived using the screening swab result as test variable predicting the presence or absence of VRE in the sterile site Enterococcus species. Results: 619 patients had sterile cultures positive for Enterococcus during the study period. Of these, 488/619 (79%) had previously undergone VRE screening. A total of 19/488 screening swabs were positive for VRE (4%), and a total of 10/488 sterile culture Enterococcal isolates were vancomycin resistant (2%). All VRE sterile isolates were E. faecium. The overall specificity of VRE swabs was 97% (92%-99%) and the overall sensitivity was 70% (35%-92%). The positive predictive value was 37% (17%-61%) and the negative predictive value was 99% (98%-100%). The positive likelihood ratio was 28 (14-56) and the negative likelihood ratio was 0.31 (0.12-0.80). A positive VRE screening swab yielded a post-test probability of 0.36 for VRE sterile site infection. In the United States, where the prevalence of VRE among enterococcus sterile isolates is as high as 0.15, a positive VRE screening swab would yield a post-test probability of 0.83 of vancomycin resistance (based on the derived likelihood ratio). Conclusion: Prior VRE screening swab results are a useful tool for predicting vancomycin-resistance among sterile site Enterococcal infections. The results of this study suggest that those with a positive VRE screening swab, in whom enterococcus is being considered as a potential etiologic agent, should receive empiric treatment with linezolid or daptomycin until culture and sensitivity results are available; this may lead to earlier effective therapy, decreased average length of stay and reduced mortality.
1. Klein E, Smith D, Laxminarayan R. Hospitalizations and Deaths Caused by Methicillin-Resistant Staphylococcus aureus, United States, 1999–2005. Emerging Infectious Diseases 2007;13:1840-6. 2. De Kraker M, Davey P, Grundmann H, group Bs. Mortality and Hospital Stay Associated with Resistant Staphylococcus aureus and Escherichia coli Bacteremia: Estimating the Burden of Antibiotic Resistance in Europe. PLoS Medicine 2011;8:1-8. 3. DiazGranados CA, Zimmer S, Klein M, Jernigan J. Comparison of Mortality Associated with Vancomycin-Resistant and Vancomycin- Susceptible Enterococcal Bloodstream Infections: A Meta-analysis. Clinical Infectious Diseases 2005;41:327-33. 4. Lloyd-Smith P, Younger J, Lloyd-Smith E, Green H, Leung V, Romney MG. Economic analysis of vancomycin-resistant enterococci at a Canadian hospital: assessing attributable cost and length of stay. J Hosp Infect 2013;85:54-9. 5. Munita JM, Murray BE, Arias CA. Daptomycin for the treatment of bacteraemia due to vancomycin-resistant enterococci. Int J Antimicrob Agents 2014;44:387-95. 6. Murdoch Dea. Clinical Presentation, Etiology, and Outcome of Infective Endocarditis in the 21st Century: The International Collaboration on Endocarditis–Prospective Cohort Study. ARCH INTERN MED 2009;169:463-73. 7. The Clinical Significance of Positive Blood Cultures in the 1990s: A Prospective Comprehensive Evaluation of the Microbiology, Epidemiology, and Outcome of Bacteremia and Fungemia in Adults. Clinical Infectious Diseases 1997;24:584-602. 8. Brook I, Frazier E. Aerobic and anaerobic microbiology in intra-abdominal infections associated with diverticulitis. J Med Microbio 2000;49:827-30. 9. Hidron AI, Edwards JR, Patel J, et al. NHSN annual update: antimicrobial-resistant pathogens associated with healthcare-associated infections: annual summary of data reported to the National Healthcare Safety Network at the Centers for Disease Control and Prevention, 2006-2007. Infect Control Hosp Epidemiol 2008;29:996-1011.
10. Barber KE, King ST, Stover KR, Pogue JM. Therapeutic options for vancomycin-resistant enterococcal bacteremia. Expert Rev Anti Infect Ther 2015;13:363-77. 11. Arias CA, Murray BE. The rise of the Enterococcus: beyond vancomycin resistance. Nat Rev Microbiol 2012;10:266-78. 12. Biedenbach DJ, Moet GJ, Jones RN. Occurrence and antimicrobial resistance pattern comparisons among bloodstream infection isolates from the SENTRY Antimicrobial Surveillance Program (1997-2002). Diagn Microbiol Infect Dis 2004;50:59-69. 13. Zasowski EJ, Claeys KC, Lagnf AM, Davis SL, Rybak MJ. Time Is of the Essence: The Impact of Delayed Antibiotic Therapy on Patient Outcomes in Hospital-Onset Enterococcal Bloodstream Infections. Clin Infect Dis 2016;62:1242-50. 14. MacFadden D, Elligsen M, Robicsek A, Ricciuto D, Daneman N. Utility of prior screening for methicillin-resistant Staphylococcus aureus in predicting resistance of S. aureus infections. CMAJ 2013;185:E725-E30. 15. Salgado CD. The risk of developing a vancomycin-resistant Enterococcus bloodstream infection for colonized patients. Am J Infect Control 2008;36:S175 e5-8. 16. Karki S, Land G, Aitchison S, et al. Long-term carriage of vancomycin-resistant enterococci in patients discharged from hospitals: a 12-year retrospective cohort study. J Clin Microbiol 2013;51:3374-9. 17. Sohn KM, Peck KR, Joo EJ, et al. Duration of colonization and risk factors for prolonged carriage of vancomycin-resistant enterococci after discharge from the hospital. Int J Infect Dis 2013;17:e240-6. 18. Yoon YK, Lee SE, Lee J, et al. Risk factors for prolonged carriage of vancomycin-resistant Enterococcus faecium among patients in intensive care units: a case-control study. J Antimicrob Chemother 2011;66:1831-8. 19. Vazquez-Guillamet C, Kollef MH. Treatment of Gram-positive infections in critically ill patients. BMC Infect Dis 2014;14:92.
This study explores the utility of VRE screening swab results in predicting the resistance profile of subsequent Enterococcal sterile site infections. The study demonstrates that a positive VRE screening swab suggests that VRE is highly probable in Enterococcal sterile culture isolates and necessitates empiric coverage while awaiting definitive susceptibility testing. A negative VRE swab, however, cannot be relied on to predict vancomycin-sensitivity in Enterococcal sterile culture isolates. This work is the first to demonstrate the value of VRE screening swabs in predicting resistance among Enterococcal sterile isolates. Previous studies generally involved specialized clinical settings and immunocompromised patient and did not look at VRE as a proportion of all Enterococcal sterile site infections15. This study ensured blinding of the reference sterile culture to screening swab results and independence of the decisions to obtain screening swabs and sterile cultures. Restriction of the study to sterile cultures provides confidence that positive reference results reflect true infection. The diagnostic test employed is already available and employed for other purposes at many centers; the conclusions of the study can therefore be immediately implemented at little to no additional cost, increasing the quality of care provided. The findings of the study are mechanistically consistent with the relatively long duration of rectal carriage of VRE once colonized and with the potential for un-colonized patients to acquire VRE with repeated healthcare exposure16. The median duration of VRE colonization has been estimated to be 4-9 weeks in some studies16-18. The study is also consistent with rectal colonization with VRE being an intermediate step in the acquisition of a VRE sterile site infection. Our analysis of the regional variation in the post-test probability of VRE sterile site infection based on published prevalence data demonstrates the exquisite sensitivity to slight increases in the prevalence of VRE in Enterococcal sterile culture isolates. The relatively high possibility of VRE sterile culture isolate in a patient with a positive VRE screening swab in most regions necessitates effective empiric coverage with linezolid and daptomycin5,10,19. This is the most important implication of the study. Potential limitations of the study relate to its retrospective cohort construction and include the assumption that accurate cultures were obtained in all sterile site infections. It is expected that future work performed at multiple centers and in an area of higher VRE prevalence will confirm the broad trends described herein. Our study demonstrates that positive VRE screening reliably increases the probability of VRE in Enterococcal sterile site cultures beyond the threshold of empiric coverage. Our results suggest VRE should be covered in a patient with positive VRE screening swab and sterile site speciation demonstrating Enterococcus while awaiting antibiotic sensitivities. Patients at high epidemiologic risk for VRE infection should receive even earlier empiric coverage. Supportive work demonstrates that this is not just a theoretical construct; patient survival may directly relate to appropriate empiric coverage of VRE13.
Variable No. (%) of patients
Age, yr, mean ± SD 65 ± 17
Sex Male 296 (61) Female 192 (39)
Screening Result for VRE Positive 19 (4) Negative 469 (96)
Vancomycin Resistance of Enterococcus Sterile Isolates
Positive 10 (2) Negative 478 (98)
Enterococcus Sterile Isolates Species E. faecalis 347 (71) E. faecium 141 (29)
Admission Type Medical 214 (45) Surgical 255 (54) Obstetrical 3 (1) Admitted to intensive care unit 208 (43) Swab and isolate collection performed on same admission 374 (77)
Sterile Cultures by Site
Blood 353 (72) Bone 21 (4) CSF 7 (1) Dialysate 3 (1) Fluid 106 (22)
Time Between Swab and Isolate Collection
Immediate (< 48 h) 76 (16) Recent (48 h to 14 d) 190 (39) Remote (> 14 d) 222 (45) Time from swab to isolate collection, d, median (IQR) 12 (4 - 31)
Table 1. Baseline characteristics of 488 patients with sterile isolates that tested positive for Enterococcus spp. and had prior screening for vancomycin-resistant Enterococcus.
Characteristic Overall Immediate Recent Remote E. faecium E. faecalis True positive, no. 7 2 2 3 7 0 True negative, no. 466 73 182 211 127 339 False positive, no. 12 1 5 6 4 8 False negative, no. 3 0 1 2 3 0
Sensitivity, % (95% CI) 70 (35-92) 100 (20-100) 67 (13-98) 60 (17-93) 70 (35-92) N/A
Specificity, % (95% CI) 97 (92-99) 99 (92-100) 97 (94-99) 97 (94-99) 97 (92-99) 98 (95-99)
Positive predictive value, % (95% CI) 37 (17-61) 67 (13-98) 29 (5-70) 33 (9-69) 64 (32-88) 0 (0-40)
Negative predictive value, % (95% CI)
99 (98-100)
100 (94-100)
99 (97-100)
99 (96-100) 98 (93-99) 100
(60-100)
Positive likelihood ratio (95% CI) 28 (14-56) 74 (11- 520) 25 (7.7-81) 22 (7.5-63) 23 (8.1-66) N/A
Negative likelihood ratio (95% CI) 0.31 (0.12-0.80) 0 (0-N/A) 0.34
(0.069-1.7) 0.41
(0.14-1.2) 0.31
(0.12-0.80) N/A
Table 2. Test characteristics of the prediction of vancomycin resistance among sterile clinical isolates of Enterococcus spp. using prior screening swabs. Overall results included, along with stratification by time between screening swab
and isolate collection.
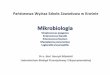
Figure 1. Each scatter plot point represents published
data on the regional prevalence of VRE among
sterile isolates of Enterococcus and the calculated post-test
probability using the positive likelihood ratio derived in the
study. The scatterplot demonstrates that small
increases in prevalence are associated with large increases in post-test
prevalence of VRE. VRE = Vancomycin-Resistant
Enterococci.
Antibiotic resistance is a worsening problem worldwide that has been associated with increased average length of stay, higher healthcare costs and increased mortality1-4
. Enterococcus is among the top causes of bloodstream infection, infective endocarditis, intra-abdominal sepsis, and surgical site infections
5-9
. Vancomycin resistance first emerged in the 1980s after the dissemination of ampicillin-resistant
E. faecium due to increasing use of the drug in humans and of a related glycopeptide in domesticated animals5,10,11
. Vancomycin-Resistant Enterococcus (VRE) prevalence continues to increase, particularly in
E. faecium, where as much as 80% of isolates are resistant in some settings12
.
Among patients with enterococcal sterile site infections, VRE has long been associated with higher patient mortality, and although this may include a contribution of increased virulence or patient comorbidities, at least part of the harms are related to inadequate empiric antibiotic treatment3
. Very few antibiotic agents are effective against VRE, and those that are tend not be used as part of initial empiric treatment regimens
3,13
. A recent study found that a delay of greater than two days in effective therapy for Enterococcal infections was associated with a three-fold increase in 30-day mortality and that this delay was solely associated with vancomycin-resistance
14
.
Ways are needed to predict the likelihood of vancomycin resistance in Enterococcus isolates while susceptibility test results are pending. Screening swabs for AROs are attractive for this purpose because they are widely used in clinical practice and because they are frequently drawn on admission to hospital, with results available earlier than culture data. A number of previous studies have investigated the prevalence of VRE infection among patients known to be colonized with VRE15
. Unfortunately, these studies investigated the prevalence of VRE among all causes of bacterial infection, rather than the prevalence of vancomycin resistance among Enterococcal infections.
Screening swabs for MRSA have recently been demonstrated to have high specificity for predicting subsequent MRSA infections once Staphylococcus has been implicated as the causative organism16
. When drawn within 48 hours of cultures, they were also found to be helpful for predicting the absence of methicillin-resistance in the clinical isolate. This study seeks to investigate the utility of screening VRE swabs for predicting vancomycin-resistance among subsequent Enterococcal sterile-site infections. We predicted that positive screening VRE swabs will reliably predict Enterococcal sterile culture vancomycin-resistance but that negative screening VRE swabs will be unreliable.
Antibiotic resistance is a worsening problem worldwide that has been associated with increased average length of stay, higher healthcare costs and increased mortality1-4
. Enterococcus is among the top causes of bloodstream infection, infective endocarditis, intra-abdominal sepsis, and surgical site infections
5-9
. Vancomycin resistance first emerged in the 1980s after the dissemination of ampicillin-resistant
E. faecium due to increasing use of the drug in humans and of a related glycopeptide in domesticated animals5,10,11
. Vancomycin-Resistant Enterococcus (VRE) prevalence continues to increase, particularly in
E. faecium, where as much as 80% of isolates are resistant in some settings12
.
Among patients with enterococcal sterile site infections, VRE has long been associated with higher patient mortality, and although this may include a contribution of increased virulence or patient comorbidities, at least part of the harms are related to inadequate empiric antibiotic treatment3
. Very few antibiotic agents are effective against VRE, and those that are tend not be used as part of initial empiric treatment regimens
3,13
. A recent study found that a delay of greater than two days in effective therapy for Enterococcal infections was associated with a three-fold increase in 30-day mortality and that this delay was solely associated with vancomycin-resistance
14
.
Ways are needed to predict the likelihood of vancomycin resistance in Enterococcus isolates while susceptibility test results are pending. Screening swabs for AROs are attractive for this purpose because they are widely used in clinical practice and because they are frequently drawn on admission to hospital, with results available earlier than culture data. A number of previous studies have investigated the prevalence of VRE infection among patients known to be colonized with VRE15
. Unfortunately, these studies investigated the prevalence of VRE among all causes of bacterial infection, rather than the prevalence of vancomycin resistance among Enterococcal infections.
Screening swabs for MRSA have recently been demonstrated to have high specificity for predicting subsequent MRSA infections once Staphylococcus has been implicated as the causative organism16
. When drawn within 48 hours of cultures, they were also found to be helpful for predicting the absence of methicillin-resistance in the clinical isolate. This study seeks to investigate the utility of screening VRE swabs for predicting vancomycin-resistance among subsequent Enterococcal sterile-site infections. We predicted that positive screening VRE swabs will reliably predict Enterococcal sterile culture vancomycin-resistance but that negative screening VRE swabs will be unreliable.
Antibiotic resistance is a worsening problem worldwide that has been associated with increased average length of stay, higher healthcare costs and increased mortality1-4
. Enterococcus is among the top causes of bloodstream infection, infective endocarditis, intra-abdominal sepsis, and surgical site infections
5-9
. Vancomycin resistance first emerged in the 1980s after the dissemination of ampicillin-resistant
E. faecium due to increasing use of the drug in humans and of a related glycopeptide in domesticated animals5,10,11
. Vancomycin-Resistant Enterococcus (VRE) prevalence continues to increase, particularly in
E. faecium, where as much as 80% of isolates are resistant in some settings12
.
Among patients with enterococcal sterile site infections, VRE has long been associated with higher patient mortality, and although this may include a contribution of increased virulence or patient comorbidities, at least part of the harms are related to inadequate empiric antibiotic treatment3
. Very few antibiotic agents are effective against VRE, and those that are tend not be used as part of initial empiric treatment regimens
3,13
. A recent study found that a delay of greater than two days in effective therapy for Enterococcal infections was associated with a three-fold increase in 30-day mortality and that this delay was solely associated with vancomycin-resistance
14
.
Ways are needed to predict the likelihood of vancomycin resistance in Enterococcus isolates while susceptibility test results are pending. Screening swabs for AROs are attractive for this purpose because they are widely used in clinical practice and because they are frequently drawn on admission to hospital, with results available earlier than culture data. A number of previous studies have investigated the prevalence of VRE infection among patients known to be colonized with VRE15
. Unfortunately, these studies investigated the prevalence of VRE among all causes of bacterial infection, rather than the prevalence of vancomycin resistance among Enterococcal infections.
Screening swabs for MRSA have recently been demonstrated to have high specificity for predicting subsequent MRSA infections once Staphylococcus has been implicated as the causative organism16
. When drawn within 48 hours of cultures, they were also found to be helpful for predicting the absence of methicillin-resistance in the clinical isolate. This study seeks to investigate the utility of screening VRE swabs for predicting vancomycin-resistance among subsequent Enterococcal sterile-site infections. We predicted that positive screening VRE swabs will reliably predict Enterococcal sterile culture vancomycin-resistance but that negative screening VRE swabs will be unreliable.
Study Design and Patient Selection: Retrospective cohort study. All patients at single centre in Toronto (Sunnybrook HSC) between April 1, 2010 and December 31, 2015 with positive sterile isolates for Enterococcus spp. and prior screening for VRE. Sterile sites: Blood, cerebrospinal fluid, pleural fluid, peritoneal fluid, synovial fluid and tissue biopsies. Inclusion criteria: Older than one-year old. Patients were only included once (most recent isolate/screening results). Data Sources: Data derived from pre-existing database. Auto-populated with pharmacy, microbiology and patient characteristics. VRE screening protocols and methods: Rectal screening for VRE on admission day 1 for the following circumstances: (1) known previous ARO colonization, infection or contact, (2) previous receipt of healthcare in a high-risk area outside of Canada, (3) admission to healthcare facility within the preceding year, (4) receipt of home healthcare services or hemodialysis, (5) residence in a shelter or other high-risk communal setting, or (6) inability to answer screening questions. Surveillance swabs were also obtained to facilitate transfer to a critical-care unit or in the context of an identified outbreak. [Swab collection and transport media information and citation]. VRE screening rectal swabs were cultured on chromogenic media to screen for VRE and Enterococcus species (Brilliance VRE Agar, Oxoid). Incubation at 37ºC for 22-24 hours in the dark. Vancomycin resistance was confirmed by instilling sample in Triton X-100 lysis buffer and performing PCR for vanA and vanB [PCR source, ?homegrown primers]. An intermediate saline dilution method was used for presumed vancomycin-resistant E. faecalis colonies. Screening deemed positive if there was a positive culture and PCR result and deemed negative if no VRE by either technique. Enterococcus spp. Sterile isolate protocols: Isolates collected from sterile sites and cultured according to routine practices for the site of origin. Possible Enterococcus identified by presence of colonies of gram positive cocci in pairs and chains in appropriate culture media. Speciation confirmed using the Vitek MS system (bioMérieux). Susceptibilities performed using PCR for vanA and vanB [PCR source]. Covariates: We extracted the following covariates: patient demographics (age, sex), clinical characteristics (admission category, intensive care unit exposure), microbiologic characteristics (sterile specimen site, species of Enterococcus), and the time lapse between the screening swab and sterile site culture.
Statistical Analysis: The test characteristics of VRE swab results were examined for their value in predicting vancomycin resistance in Enterococcus spp. sterile isolates. Test characteristics of interest include sensitivity, specificity, negative predictive value, positive predictive value, positive likelihood ratio, and negative likelihood ratio. Test variable: VRE screening result. Response variable: Vancomycin-sensitivity of sterile isolates were deemed the test and response variables respectively. True positive: positive VRE screening, VRE sterile isolate. False positive: positive VRE screening, vancomycin-sensitive sterile isolate.True negative: negative VRE screening, vancomycin-sensitive sterile isolate. False negative: negative VRE screening, VRE sterile isolate. Confidence intervals were calculated using the efficient-score method corrected for continuity.Further analyzed by time between screening swab and sterile isolate. ‘Immediate’ – 0 to 48 hours. ‘Recent’ – 48 hours to 14 days.‘Remote’ – greater than 14 days. Regional VRE Prevalence and Calculated Post-Test Probability: The post-test probabilities of VRE among Enterococcal sterile site infections, given prior positive VRE screening results, were calculated using published VRE prevalence data for representative regions and the derived positive likelihood ratio. A scatter plot was made illustrating the logistical relationship of the data using Stata (Stata 14.1, Statacorp, College Station, Tx).