Embed Size (px)
Citation preview

Does the intravenous infusion of ritodrine or magnesium sulfate alter the hemodynamic response to hemorrhage in gravid ewes?
David H. Chestnut, MD, Christine S. Thompson, Geri L. McLaughlin, and Carl P. Weiner, MD
Iowa City, Iowa
The purpose of this study was to determine whether the intravenous infusion of ritodrine or magnesium sulfate alters the hemodynamic response to maternal hemorrhage in gravid ewes. Twenty-seven experiments were performed in 12 chronically instrumented animals at 0.8 of timed gestation. Each animal was subjected to hemorrhage (20 ml/kg over 60 minutes) during infusion of ritodrine (0.004 mg/kg/min), magnesium sulfate (4 gm/hour), or saline solution control. Infusion of magnesium sulfate increased the mean (:t:SEM) maternal serum magnesium concentration to 4.8 :t 0.2 mg/di before hemorrhage and 5.3 :!: 0.3 mg/di after hemorrhage. At the end of hemorrhage maternal mean arterial pressures were 63% :!: 4%, 82% :!: 2%, and 79% :!: 6% of baseline in the magnesium sulfate, ritodrine, and control groups, respectively. The maternal mean arterial pressure response in the magnesium sulfate group differed significantly from the maternal mean arterial pressure responses in the ritodrine and control groups (p < 0.01 ). Fetal pH was decreased significantly only in the magnesium sulfate group (p = 0.0001 ). Fetal Po2 was decreased significantly in the magnesium sulfate and ritodrine groups (p < 0.001) but not in the control group. We conclude that magnesium sulfate but not ritodrine, worsened the maternal hypotensive response to hemorrhage in gravid ewes. (AM J OssrET GYNECOL 1988;159:1467-73.)
Key words: Hemorrhage, pregnancy, preterm labor, tocolytic agent, magnesium sulfate, ritodrine
Obstetricians often avoid 13-sympathomimetic toco
lytic agents (ritodrine, terbutaline) in patients at risk
for hemorrhage for fear that severe hypotension will occur. 1 In comparison with ritodrine, magnesium sul
fate results in less severe cardiovascular side effects in
unstressed patients.' In many centers magnesium sul
fate is the tocolytic agent of choice in patients at risk
for hemorrhage." However, magnesium relaxes vascular smooth muscle' and may not be innocuous in
patients at risk for hemorrhage. To our knowledge,
there are no published data regarding the hemodynamic response to hemorrhage during infusion of rito
drine or magnesium sulfate in pregnant patients or animals. The purpose of the present study was to ad
dress the following question: Does the intravenous in
fusion of ritodrine or magnesium sulfate alter the hemodynamic response to maternal hemorrhage in
gravid ewes?
From the Departmeni1 of Anesthesia and Obstetrics and Gynecology. Universit_v of Iowa College of Medicine.
Supported in part by a grant from the American Societ_v of Ane.1thesiologists.
Presented in part at the Thirty-fifth Annual Meeting of the Society for Gynecologic Investigation, Baltimore, Maryland, March 17-20, 1988. .
Reprints not available.
Methods
The protocol was approved by The University of Iowa Animal Care Committee. Mixed breed ewes were
obtained from a commercial breeder at 118 days of timed gestation (term = 145 days). Each animal fasted
for 36 hours before operation. At 120 days' gestation each animal was given a general orotracheal anesthetic
(thiopental sodium 600 to 750 mg, halothane 1 %, ni
trous oxide 50%, oxygen 50%). With sterile technique, laparotomy and hysterotomy were performed, and the
fetus was exteriorized. Catheters (PE-90) were placed
in the fetal descending aorta via each femoral artery and in the amniotic cavity. The fetus was replaced in the uterus. Additional catheters (PE-240) were placed
in the maternal descending aorta via the left mammary and femoral arteries and in the maternal inferior
vena cava via the left mammary and femoral veins. All
catheters were tunneled subcutaneously and exterior
ized via a small incision in the left Hank. After operation each animal was kept in an ap
proved cage in a restricted area, fed a balanced diet,
and allowed a recovery of at least 72 hours before
experimentation. Procaine penicillin G 500,000 U and dihydrostreptomycin 625 mg (Combiotic, Pfizer, New York) were given to the mother before operation
and daily for 3 days after operation. Gentamicin 80 mg
1467

1468 Chestnut et al. December 1988 Am J Obstet Gynecol
Table I. Baseline maternal and fetal hemodynamic, acid-base, and blood gas measurements
Magnesium Ritodrine sulfate Control (n = IO) (n = 9) (n = 8)
Maternal Hematocrit (%) 26 ± 1 28 ± 1 26 ± 1 Systolic arterial pressure (mm Hg) ll4 ± 5 110 ± 5 112 ± 4 Diastolic arterial pressure (mm Hg) 71 ± 4 69 ± 3 72 ± 2 Mean arterial pressure (mm Hg) 88 ± 4 85 ± 3 88 ± 3 Heart rate 99 ± 6 98 ± 6 98 ± 5 Arterial pH 7.46 ± 0.01 7.45 ± 0.02 7.45 ± 0.01 Arterial Po2 (mm Hg) 106 ± 3 109 ± 3 JOI ± 3 Arterial Pco, (mm Hg) 36 ± 1 35 ± I 34 ± 4
Fetal Hematocrit (%) 39 ± 2 41 ± 2 41 ± 2 Systolic arterial pressure (mm Hg) 59 ± 2 60 ± 2 61 ± 2 Diastolic arterial pressure (mm Hg) 34 ± I 33 ± I 36 ± 2 Mean arterial pressure 44 ± I 43 ± I 47 ± 3 Heart rate 168 ± 4 159 ± 5 170 ± 8 Arterial pH 7.34 ± 0.01 7.33 ± 0.01 7.33 ± 0.01 Arterial Po, (mm Hg) 21 ± I 21 ± I 19 ± I Arterial Pco, (mm Hg) 51 ± 2 50 ± 2 51 ± 2
Fetal arterial pressures were corrected for variations in intrauterine pressure by subtracting the simultaneously measured amniotic fluid pressure. Maternal and fetal arterial blood samples were obtained from the maternal and the fetal descending aorta, respectively. Blood gas and acid-base values were corrected for temperature. All values are expressed as mean ± SEM.
was given to the mother on each experiment day, and gentamicin 40 mg was given via the amniotic catheter during operation and on each experiment day.
Each experiment was done with the animal standing unrestrained within an approved transfer cart. The experimental sequence was:
l. Acute hydration with 250 ml of normal saline solution intravenously over 15 minutes
2. l hour for baseline measurements 3. 50 ml intravenous bolus over 5 minutes
Magnesium sulfate group-4 gm magnesium sulfate in 5% dextrose in water Ritodrine group-5% detrose in water only Control group-5% dextrose in water only
4. Intravenous infusion of tocolytic agent (tocolytic agent was diluted in normal saline solution, and total volume of normal saline solution was 100 ml/hr in each group) Magnesium sulfate group-magnesium sulfate, 4 gm/hr Ritodrine group-ritodrine, 0.002 mg/kg/min for 45 minutes, then 0.004 mg/kg/min Control group-normal saline solution only
5. Maternal hemorrhage (20 ml/kg), begun 90 minutes later and performed over 60 minutes, with a constant-rate withdrawal pump (each animal received 15,000 U heparin 10 minutes before start of hemorrhage)
6. 5-minute wait 7. Reinfusion of blood over 60 minutes (intravenous
infusion of magnesium sulfate, ritodrine, or normal saline solution control was continued until all blood had been reinfused)
Maternal and fetal arterial serum magnesium concentrations were determined at baseline, just before hemorrhage, and just after hemorrhage. Serum magnesium concentrations were determined according to a bichromatic colorimetric method. (Arterial blood samples for magnesium concentrations were obtained during each experiment, but magnesium concentrations were actually determined only on the days that magnesium sulfate was given.)
Maternal and fetal arterial blood gas and acid-base values were determined at baseline, just before hemorrhage, and at 15-minute intervals thereafter. These values were determined with an Instrumentation Laboratory (Leighton, Mass.) 1302 blood gas analyzer. All values were corrected for temperature.
Fetal blood was replaced immediately by an equal volume of normal saline solution. At the end of an experiment, the fetus was transfused with a volume of maternal blood equal to that removed from the fetus during the experiment.
Only one experiment was performed per day, and each animal rested at least 48 hours between experiments. Experiments were performed in random order. No animal underwent the same experiment twice. We intended to perform all three experiments in each animal; however, preterm delivery, fetal death, or an occluded intravascular catheter precluded the performance of all three experiments in each animal.
Maternal and fetal systemic arterial pressures and amniotic fluid pressure were recorded continuously with a Beckman (Sensormedics, Anaheim, Calif.) R61 l recorder. Fetal arterial pressures were corrected for variations in intrauterine pressure by subtracting the

Volume 159 Number 6
Percent of
Baseline
200
180
160
140
120
100
80 D Ritodrine
• MgS04
0 \ 0 Control [1 I
A 0 30 60
Hemorrhage during infusion of ritodrine or magnesium 1469
90
• Hemorrhage begun
Transfusion started
+ 11
120 150 • Hemorrhage completed
185 215
• Transfusion completed
Minutes after Start of Infusion
110
100
90
Percent
of 80 Baseline
70
60
B 0 30 60 90
• Hemorrhage begun
Transfusion started
+ 11
120 150 • Hemorrhage completed
185 215
• Transfusion completed
Minutes after Start of Infusion
Fig. I. A, Maternal heart rate responses over time. B, Maternal mean arterial pressure responses over time. All values are expressed as mean ( ± SEM) percent of baseline.
simultaneously measured amniotic fluid pressure. Maternal and fetal mean arterial pressures were calculated arithmetically. Maternal and fetal heart rates were calculated from maternal and fetal arterial waveforms. All hemodynamic data were interfaced to an AST (Irvine, Calif.) 286 Premium computer with a customized physiologic data acquisition system. Hemodynamic measurements over time were compared with baseline measurements and are expressed as mean ( ± SEM) percent of baseline. Statistical analysis was by repeated measures analysis of variance, followed by t tests for individual measurements. Bonferroni adjustment was performed when appropriate; p < 0.05 was significant.
Results
Twenty-seven experiments were performed in 12 animals. Ten animals had singleton fetuses, and two had
twin fetuses. The mean ( ± SEM) maternal weight was 64 ±: l kg. The three treatment groups were similar with regard to baseline hemodynamic, acid-base, and blood gas measurements (Table I).
Ritodrine (n = 10) increased maternal heart rate 84% ± 12% at 90 minutes (p = 0.0001) (Fig. 1, A). Magnesium sulfate (n = 9) increased maternal heart rate 16% ± 6% at 90 minutes, a difference of borderline significance (p = 0.08). Normal saline solution control (n = 8) did not significantly alter maternal heart rate.
Ritodrine decreased maternal mean arterial pressure 6% ± l % at 90 minutes (p = 0.0003) (Fig. 1, B). Neither magnesium sulfate nor normal saline solution control significantly altered maternal mean arterial pressure.
Magnesium sulfate increased the mean ( ±: SEM) ma-
1470 Chestnut et al.
Percent of
Baseline
120
110
100
90
80
70
01-
A 0
D Ritodrine
• MgS04
0 Control
30 60 90 +
Hemorrhage begun·
Transfusion started
+ 11
120 150 +
Hemorrhage completed
185 215 +
Transfusion completed
December 1988 Am J Obst ct Gynecol
Minutes after Start of Infusion
110
100
Percent 90
of Baseline
80
70
o 1- I
0
B
D Ritodrine
• MgS04
O Control
30 60 90 +
Hemorrhage begun
Transfusion started
+ II
120 150 + Hemorrhage
completed
185 215 + Transfusion
completed
Minutes after Start of Infusion
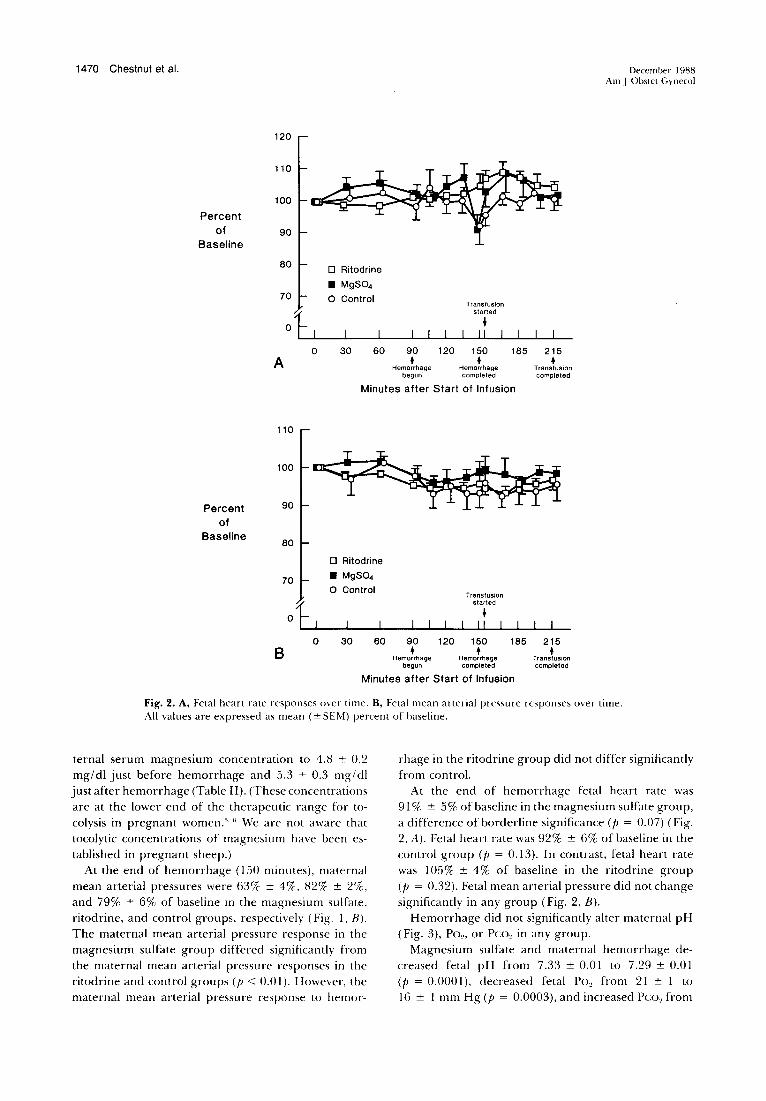
Fig. 2. A, Fetal heart rate responses over time. B, Fetal mean arterial pressure responses over time. All values are expressed as mean ( ± SEM) percent of baseline.
ternal serum magnesium concentration to 4.8 ± 0.2 mg/di just before hemorrhage and 5.3 ± 0.3 mg/di just after hemorrhage (Table II). (These concentrations are at the lower end of the therapeutic range for tocolysis in pregnant women.' " We are not aware that tocolytic concentrations of magnesium have been established in pregnant sheep.)
At the end of hemorrhage (150 minutes), maternal mean arterial pressures were 63% ± 4%. 82% ± 2%, and 79% ± 6% of baseline in the magnesium sulfate, ritodrine, and control groups, respectively (Fig. I, B). The maternal mean arterial pressure response in the magnesium sulfate group differed significantly from the maternal mean arterial pressure responses in the ritodrine and control groups (p < 0.0 I). However, the maternal mean arterial pressure response to hemor-
rhage in the ritodrine group did not differ significantly from control.
At the end of hemorrhage fetal heart rate was 91 % ± 5% of baseline in the magnesium sulfate group, a difference of borderline significance (p = 0.07) (Fig. 2, A). Fetal heart rate was 92% ± 6% of baseline in the control group (p = 0.13). In contrast, fetal heart rate was I 05% ± 4% of baseline in the ritodrine group (p = 0.32). Fetal mean arterial pressure did not change significantly in any group (Fig. 2, B).
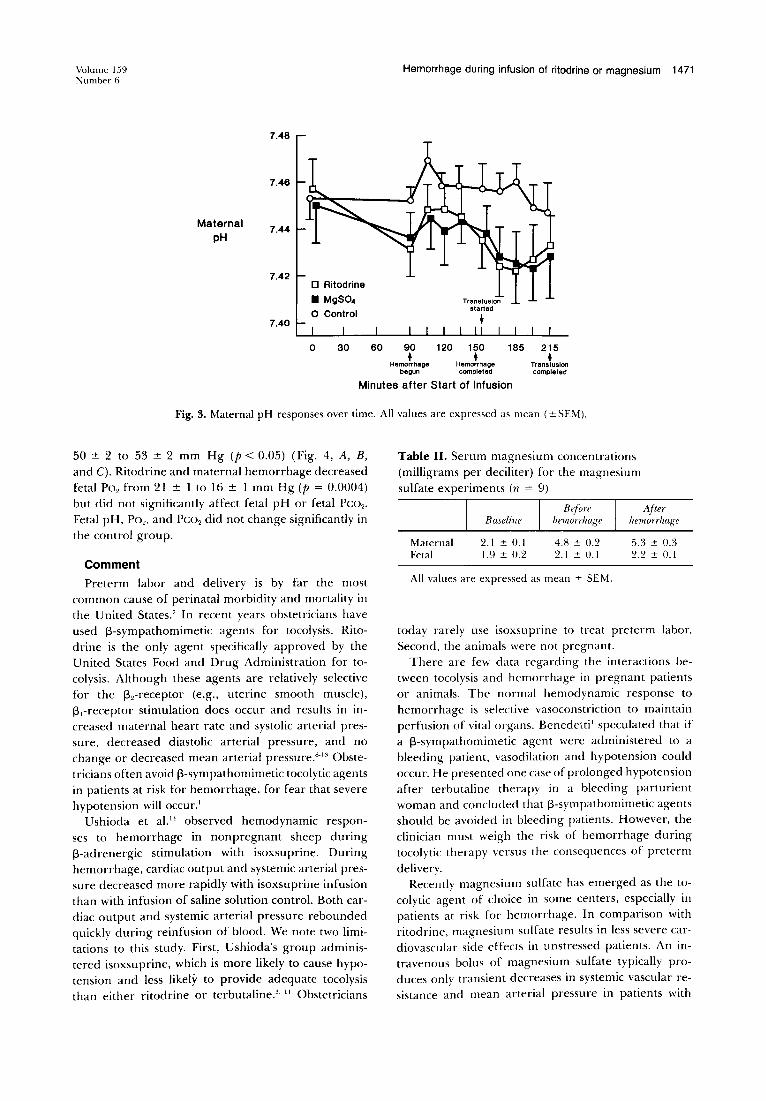
Hemorrhage did not significantly alter maternal pH (Fig. 3), Po,, or Pco" in any group.
Magnesium sulfate and maternal hemorrhage decreased fetal pH from 7.33 ± 0.01 to 7.29 ± 0.01 (p = 0.0001 ), decreased fetal Po, from 21 ± 1 to 16 ± 1 mm Hg (p = 0.0003), and increased Pc:o, from
Volume 159 Number 6
Maternal pH
7.48
7.46
7.44
7.42
7.40
D Ritodrine
• MgS04 0 Control
0 30
Hemorrhage during infusion of ritodrine or magnesium 1471
60 90 +
Hemorrhage begun
Transfusion started
+
120 150 +
Hemorrhage completed
185 215 +
Transfusion completed
Minutes after Start of Infusion
Fig. 3. Maternal pH responses over time. All values are expressed as mean ( ± SEM).
50 ± 2 to 53 ± 2 mm Hg (p < 0.05) (Fig. 4, A, B, and C). Ritodrine and maternal hemorrhage decreased fetal Po2 from 21±Ito16 ±I mm Hg (p = 0.0004) but did not significantly affect fetal pH or fetal Pco2 •
Fetal pH, Po2, and Pco2 did not change significantly in the control group.
Comment
Preterm labor and delivery is by far the most common cause of perinatal morbidity and mortality in the United States.' In recent years obstetricians have used Jj-sympathomimetic agents for tocolysis. Ritodrine is the only agent specifically approved by the United States Food and Drug Administration for tocolysis. Although these agents are relatively selective for the Jjrreceptor (e.g., uterine smooth muscle), Jj,-receptor stimulation does occur and results in increased maternal heart rate and systolic arterial pressure, decreased diastolic arterial pressure, and no change or decreased mean arterial pressure."·"' Obstetricians often avoid Jj-sympathomimetic tocolytic agents in patients at risk for hemorrhage, for fear that severe hypotension will occur.'
Ushioda et al. 11 observed hemodynamic responses to hemorrhage in nonpregnant sheep during Jj-adrenergic stimulation with isoxsuprine. During hemorrhage, cardiac output and systemic arterial pressure decreased more rapidly with isoxsuprine infusion than with infusion of saline solution control. Both cardiac output and systemic arterial pressure rebounded quickly during reinfusion of blood. We note two limitations to this study. First, Ushioda's group administered isoxsuprine, which is more likely to cause hypotension and less likely to provide adequate tocolysis than either ritodrine or terbutaline.'· " Obstetricians
Table II. Serum magnesium concentrations (milligrams per deciliter) for the magnesium sulfate experiments (n = 9)
Before After Baseline hemorrhage hemorrhage
Maternal 2.1 ± 0.1 4.8 ± 0.2 5.3 ± 0.3 Fetal 1.9 ± 0.2 2.1 ± 0.1 2.2 ± 0.1
All values are expressed as mean ± SEM.
today rarely use isoxsuprine to treat preterm labor. Second, the animals were not pregnant.
There are few data regarding the interactions between tocolysis and hemorrhage in pregnant patients or animals. The normal hemodynamic response to hemorrhage is selective vasoconstriction to maintain perfusion of vital organs. Benedetti' speculated that if a Jj-sympathomimetic agent were administered to a bleeding patient, vasodilation and hypotension could occur. He presented one case of prolonged hypotension after terbutaline therapy in a bleeding parturient woman and concluded that Jj-sympathomimetic agents should be avoided in bleeding patients. However, the clinician must weigh the risk of hemorrhage during tocolytic therapy versus the consequences of preterm
delivery. Recently magnesium sulfate has emerged as the to
colytic agent of choice in some centers, especially in patients at risk for hemorrhage. In comparison with ritodrine, magnesium sulfate results in less severe cardiovascular side effects in unstressed patients. An intravenous bolus of magnesium sulfate typically produces only transient decreases in systemic vascular resistance and mean arterial pressure in patients with

1472 Chestnut et al.
7.36
7.34
Fetal pH
7.32
7.30 a Ritodrine
• MgS04 0 Control
7.28
A 0 30 60 90
+ Hemorrhage
begun
Tranafuaion started
+
120 150 +
Hemorrhage completed
185 215 +
Transfusion completed
December 1988 Am J Obstet Gynecol
Minutes after Start of Infusion
Fetal Po2
(mmHg)
24
22
20
18
16
B 0 30 60 90
+ Hemorrhage
begun
Transfusion started
t I II
120 150 +
Hemorrhage completed
185
Minutes after Start of Infusion
215 +
Transfusion completed
Fetal Pco2
(mmHg)
47
45
c 0
D Ritodrine
• MgS04 0 Control
30 60 90 +
Hemorrhage begun
Transfusion started
t I II
120 150 +
Hemorrhage completed
185
Minutes after Start of Infusion
215 +
Transfusion completed
Fig. 4. A, Fetal pH responses over time. B, Fetal Po2 responses over time. C, Fetal Pco2 responses over time. All values are expressed as mean ( ± SEM).
pregnancy-induced hypertension. '5·
16 Benedetti" stated: "In most instances of suspected clinical abruption and documented placenta previa, magnesium sulfate is an effective and safe alternative to betamimetic therapy. This agent has no significant vasodilatory properties and will not work against the body's own compensatory mechanisms in handling volume Joss."
In the present study of gravid ewes, magnesium sulfate but not ritodrine worsened the maternal hypotensive response to hemorrhage. Magnesium retards acetylcholine release and interferes with the transmission of nerve impulses at both neuromuscular junction and sympathetic ganglia. 17 Others reported earlier that magnesium attenuated vasoconstrictor responses of (anesthetized, nonpregnant) canine mesenteric, renal, and forelimb vessels to both adrenergic and nonadrenergic agonists.' 8
·20 Lee et al. 21 recently observed that
magnesium sulfate blunted the increase in mean arterial pressure after angiotensin II and norepinephrine in chronically instrumented pregnant (0.80 to 0.93 gestation) and nonpregnant rabbits. Magnesium sulfate may have few cardiovascular effects in unstressed pa-
tients or animals, but it worsened the hypotensive response to hemorrhage in gravid ewes in the present study. We speculate that magnesium attenuated the compensatory cardiovascular response to hemorrhage in the present study. We also speculate that ritodrine's inotropic and chronotropic activity helped maintain maternal cardiac output and mean arterial pressure during hemorrhage.
In the present study hemorrhage significantly decreased fetal pH only in the magnesium sulfate group. Fetal Po2 was decreased in the magnesium sulfate and ritodrine groups but not in the control group. It is interesting that there were divergent Po2 responses in the ritodrine and control groups despite similar decreases in maternal mean arterial pressure in those two groups. We did not measure uteroplacental blood flow in the present study. However, we speculate that ritodrine-induced vasodilation may have caused a "steal" of perfusion away from the uteroplacental circulation.22
We conclude that magnesium sulfate, but not ritodrine, worsened the maternal hypotensive response to

Volume 159 Number 6
hemorrhage in gravid ewes. We acknowledge that the steady withdrawal of blood from pregnant sheep is not identical to the bleeding that occurs in women with placental abnormality. Nevertheless, the present study suggests that the use of magnesium sulfate for tocolysis in patients at risk for hemorrhage should be reevaluated.
REFERENCES
I. Benedetti TJ. Maternal complications of parenteral 13-sympathomimetic therapy for premature labor. AM J 0BSTET GYNECOL 1983;145:1-6.
2. Beall MH, Edgar BW, Paul RH, Smith-Wallace T. A comparison of ritodrine, terbutaline, and magnesium sulfate for the suppression of preterm labor. AM J 0BSTET GvNECOL 1985;153:854-9.
3. Benedetti TJ. Life-threatening complications of betamimetic therapy for preterm labor inhibition. Clin Perinatal 1986; 13:843-52.
4. Altura BM, Altura BT. Magnesium ions and contraction of vascular smooth muscles: relationship to some vascular diseases. Fed Proc 1981 ;40;2672-9.
5. Elliott JP. Magnesium sulfate as a tocolytic agent. AM J 0BSTET GYNECOL !983;147:277-84.
6. Hollander DI, Nagey DA, Pupkin MJ. Magnesium sulfate and ritodrine hydrochloride: a randomized comparison. AMj 0BSTET GYNECOL 1987;156:631-7.
7. Gonik B, Creasy RK. Preterm labor: its diagnosis and management. AM J 0BSTET GY:-.iECOL 1986; 154:3-8.
8. Barden TP. Effect of ritodrine on human uterine motility and cardiovascular responses in term labor and the early postpartum state. AM J 0BSTET GYNECOL 1972; 112:645-52.
9. Bieniarz J, I vankovich A, Scommegna A. Cardiac output during ritodrine treatment in premature labor. A:11 J OBSTET GYNECOL 1974;118:910-20.
10. Ehrenkranz RA, Walker AM, Oakes GK, McLaughlin MK, Chez RA. Effect of ritodrine infusion on uterine and umbilical blood flow in pregnant sheep. AM J 0BSTET Gvr\ECOL 1976; 126:343-9.
11. Nuwayhid BS, Cabalum MT, Lieb SM, et al. Hemody-
Hemorrhage during infusion of ritodrine or magnesium 1473
namic effects of isoxsuprine and terbutaline in pregnant and nonpregnant sheep. AM J OBSTET GYNECOL 1980; 137:25-9.
12. Chestnut DH, WeinerCP, WangJP, HerrigJE, MartinJG. The effect of ephedrine upon uterine artery blood flow velocity in the gravid guinea pig subjected to terbutaline infusion and acute hemorrhage. Anesthesiology 1987;66: 508-12.
13. Chestnut DH, Ostman LG, Weiner CP, Hdez MJ, Wang JP. The effect of vasopressor agents upon uterine artery blood flow velocity in the gravid guinea pig subjected to ritodrine infusion. Anesthesiology l 988;68:363-6.
14. Ushioda F, Nuwayhid B, Kleinman G, Tabsh K, Brinkman CR, Assali NS. The contribution of the 13-adrenergic system to the cardiovascular response to hypovolemia. AM .J 0BSTET GYNECOL 1983;147:423-9.
15. Young BK, Weinstein HM. Effects of magnesium sulfate on toxemic patients in labor. Obstet Gynecol 1977;49: 681-5.
16. Cotton DB, Gonik B, Dorman KF. Cardiovascular alterations in severe pregnancy-induced hypertension: acute effects of intravenous magnesium sulfate. AM J OllSTE'I GYNECOL 1984; 148: 162-5.
17. Barker ES: Physiologic and clinical aspects of magnesium metabolism. J Chronic Dis 1967; 11 :278-91.
18. Frohlich ED, Scott .JB, Haddy FJ. Effect of cations on resistance and responsiveness of renal and forelimb vascular beds. Amj Physiol 1962;203:583-7.
19. Texter EC, Laureta HC, Frohlich ED, Chou CC. Effects of major cations on gastric and mesenteric vascular resistances. Amj Physiol 1967;212:569-73.
20. Levowitz BS, Goldson H, Rashkin A, et al. Magnesium ion blockade of regional vasoconstriction. Ann Surg 1970; 172:33-40.
21. Lee MI, Todd HM, Bowe A. The effects of magnesium sulfate infusion on blood pressure and vascular responsiveness during pregnancy. AM .J Ossrn Gn;u:o1. 1984; 149:705-8.
22. Van de Walle AFGM, Martin CB. Effect of ritodrine on uteroplacental blood flow and cardiac output distribution in unanesthetized pregnant guinea pigs. A~I .J OllSTr-I GY:\ECOL 1986; 154: 189-94.