Embed Size (px)
Citation preview
CASE REPORT
Ganesh Prasad Æ Asan Rafee Æ Aslam Chougle
Divergent dislocation of the elbow treated with a cast brace: case report
Received: 26 June 2005 / Accepted: 23 February 2006 / Published online: 12 April 2006� Springer-Verlag 2006
Abstract Divergent dislocation of the elbow is a severeinjury leading to a significant amount of soft tissuestripping. Achieving a good functional outcome fol-lowing this injury remains a challenge. We present a casereport which was managed conservatively in a cast braceand achieved satisfactory functional results. To ourknowledge, this method of treatment has not been de-scribed in the English literature.
Keywords Elbow Æ Divergent dislocation Æ Brace
Luxation divergente du coude traitee par attelle articulee
Resume La luxation divergente du coude constitue unelesion severe entraınant d’importants arrachements detissus mous. L’obtention d’un bon resultat apres ce typede lesion est un veritable defi. Nous presentons un casclinique qui fut traite de facon conservative par immo-bilisation platree et avec succes. A notre connaissance,ce type de traitement n’a pas encore ete decrit dans lalitterature anglaise.
Mots cles Coude Æ Luxation divergente Æ Platre
Introduction
Transverse divergent dislocation of the elbow is a rareinjury where the olecranon lies medial and the radial
head lateral the distal humerus [3]. The proximal end ofthe ulna is in fact displaced posteromedially with thecoronoid process wedged against the distal and medialedge of the trochlea. As a result of this displacement themedial condyle of the humerus is rotated anteriorly andthe lateral condyle posteriorly [7]. The head of the radiusis displaced lateral to the capitellum, anterior and distalto the lateral epicondyle of the humerus. The usualmechanism of injury is pronation of the elbow withhyperextension.
Clinical descriptions of the dislocation were given by[5] and [6]. There have been 11 radiologically verifiedcases in the English literature since then. The majority ofthese have been in children where the functional out-come has been good [2, 3]. To our knowledge there havebeen no reports of this injury being treated with a castbrace in an adult.
Case report
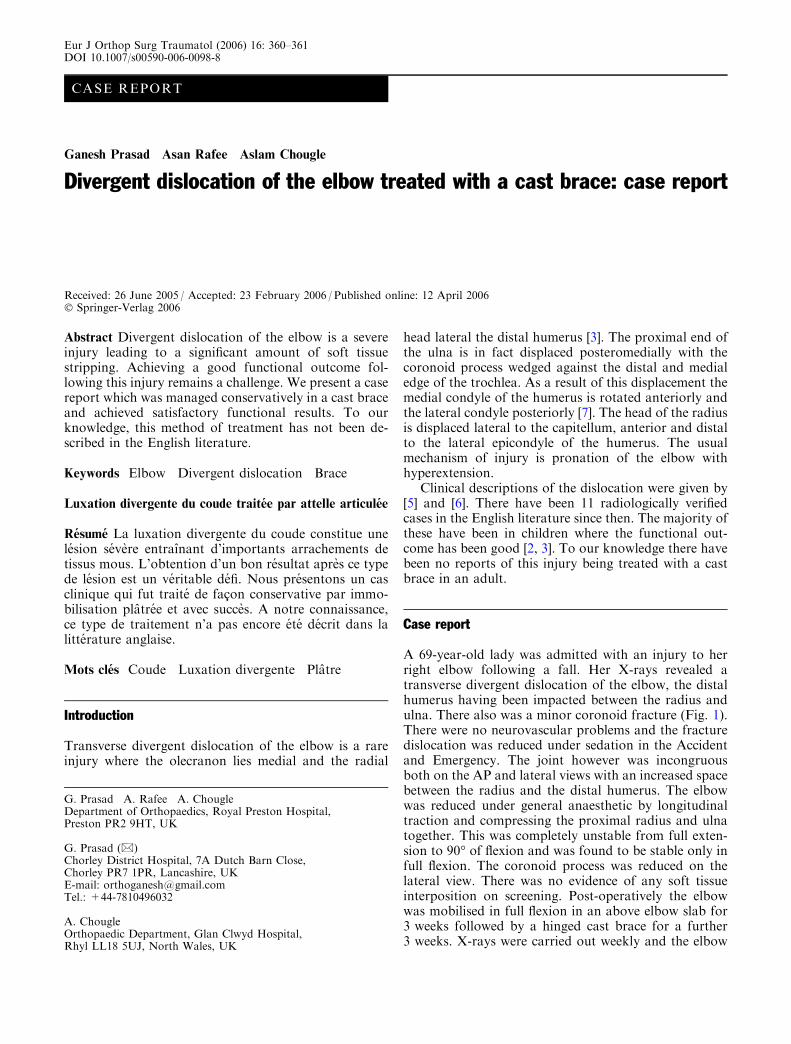
A 69-year-old lady was admitted with an injury to herright elbow following a fall. Her X-rays revealed atransverse divergent dislocation of the elbow, the distalhumerus having been impacted between the radius andulna. There also was a minor coronoid fracture (Fig. 1).There were no neurovascular problems and the fracturedislocation was reduced under sedation in the Accidentand Emergency. The joint however was incongruousboth on the AP and lateral views with an increased spacebetween the radius and the distal humerus. The elbowwas reduced under general anaesthetic by longitudinaltraction and compressing the proximal radius and ulnatogether. This was completely unstable from full exten-sion to 90� of flexion and was found to be stable only infull flexion. The coronoid process was reduced on thelateral view. There was no evidence of any soft tissueinterposition on screening. Post-operatively the elbowwas mobilised in full flexion in an above elbow slab for3 weeks followed by a hinged cast brace for a further3 weeks. X-rays were carried out weekly and the elbow
G. Prasad Æ A. Rafee Æ A. ChougleDepartment of Orthopaedics, Royal Preston Hospital,Preston PR2 9HT, UK
G. Prasad (&)Chorley District Hospital, 7A Dutch Barn Close,Chorley PR7 1PR, Lancashire, UKE-mail: [email protected].: +44-7810496032
A. ChougleOrthopaedic Department, Glan Clwyd Hospital,Rhyl LL18 5UJ, North Wales, UK
Eur J Orthop Surg Traumatol (2006) 16: 360–361DOI 10.1007/s00590-006-0098-8
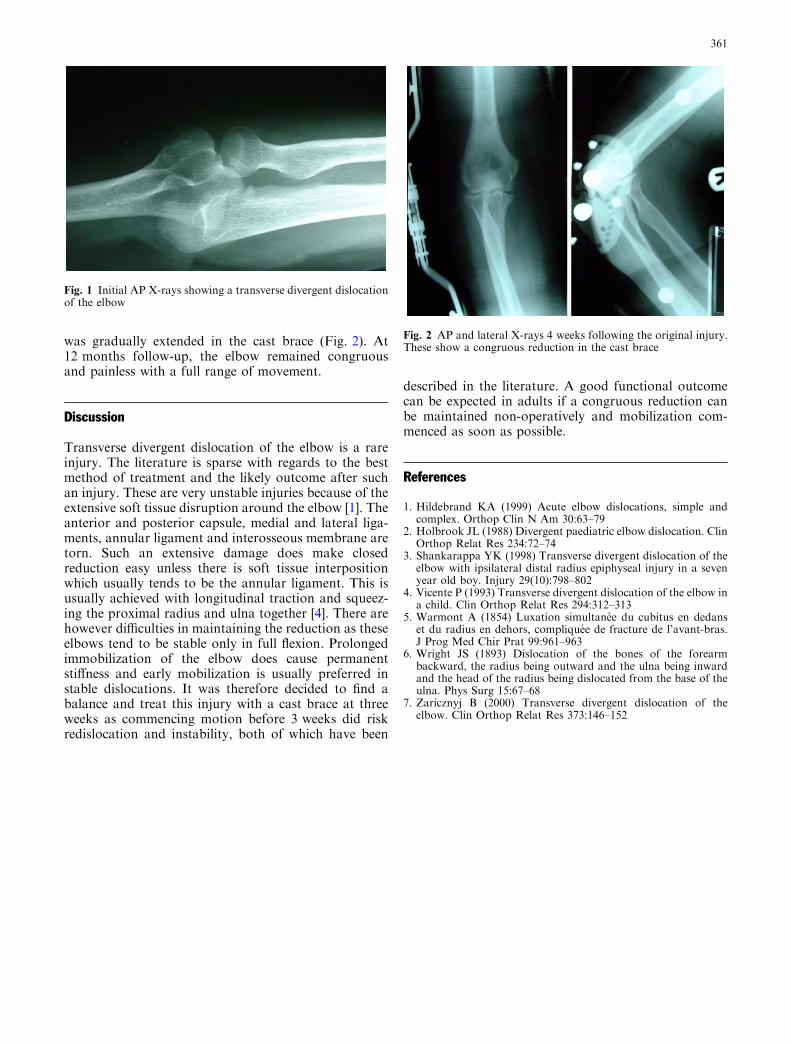
was gradually extended in the cast brace (Fig. 2). At12 months follow-up, the elbow remained congruousand painless with a full range of movement.
Discussion
Transverse divergent dislocation of the elbow is a rareinjury. The literature is sparse with regards to the bestmethod of treatment and the likely outcome after suchan injury. These are very unstable injuries because of theextensive soft tissue disruption around the elbow [1]. Theanterior and posterior capsule, medial and lateral liga-ments, annular ligament and interosseous membrane aretorn. Such an extensive damage does make closedreduction easy unless there is soft tissue interpositionwhich usually tends to be the annular ligament. This isusually achieved with longitudinal traction and squeez-ing the proximal radius and ulna together [4]. There arehowever difficulties in maintaining the reduction as theseelbows tend to be stable only in full flexion. Prolongedimmobilization of the elbow does cause permanentstiffness and early mobilization is usually preferred instable dislocations. It was therefore decided to find abalance and treat this injury with a cast brace at threeweeks as commencing motion before 3 weeks did riskredislocation and instability, both of which have been
described in the literature. A good functional outcomecan be expected in adults if a congruous reduction canbe maintained non-operatively and mobilization com-menced as soon as possible.
References
1. Hildebrand KA (1999) Acute elbow dislocations, simple andcomplex. Orthop Clin N Am 30:63–79
2. Holbrook JL (1988) Divergent paediatric elbow dislocation. ClinOrthop Relat Res 234:72–74
3. Shankarappa YK (1998) Transverse divergent dislocation of theelbow with ipsilateral distal radius epiphyseal injury in a sevenyear old boy. Injury 29(10):798–802
4. Vicente P (1993) Transverse divergent dislocation of the elbow ina child. Clin Orthop Relat Res 294:312–313
5. Warmont A (1854) Luxation simultanee du cubitus en dedanset du radius en dehors, compliquee de fracture de l’avant-bras.J Prog Med Chir Prat 99:961–963
6. Wright JS (1893) Dislocation of the bones of the forearmbackward, the radius being outward and the ulna being inwardand the head of the radius being dislocated from the base of theulna. Phys Surg 15:67–68
7. Zaricznyj B (2000) Transverse divergent dislocation of theelbow. Clin Orthop Relat Res 373:146–152
Fig. 1 Initial AP X-rays showing a transverse divergent dislocationof the elbow
Fig. 2 AP and lateral X-rays 4 weeks following the original injury.These show a congruous reduction in the cast brace
361