Embed Size (px)
Citation preview


DisasterNursing andEmergencyPreparedness
for Chemical, Biological, and Radiological Terrorism
and Other Hazards
Second Edition
EDITOR Tener Goodwin Veenema, PhD, MPH, MS, CPNP

About the Editor
Tener Goodwin Veenema, PhD, MPH, MS, CPNP,is an Associate Professor of Clinical Nursing, AssistantProfessor of Emergency Medicine, and Program Directorfor Disaster Nursing and Strategic Initiatives at the Cen-ter for Disaster Medicine and Emergency Preparednessat the University of Rochester School of Nursing andSchool of Medicine and Dentistry. Dr. Veenema is alsoPresident and Chief Executive Officer of the TenER Con-sulting Group, LLC, which provides consultation andworkforce development for emergency preparedness tofederal, state agencies, and corporate organizations. Shehas received numerous awards and research grants forher work, and in June 2004, Dr. Veenema was electedinto the National Academies of Practice and was se-lected as a 2004 Robert Wood Johnson Executive NurseFellow. In 2006, Dr. Veenema was the recipient of theKlainer Entrepreneurial Award in health care.
Dr. Veenema received her Bachelor of Science de-gree in Nursing from Columbia University in 1980 andwent on to obtain a Master of Science in Nursing Admin-istration (1992) and a Master in Public Health (1999)from the University of Rochester School of Medicineand Dentistry. In 2001, she earned a PhD in Health Ser-vices Research and Policy from the same institution.Dr. Veenema is a nationally certified Pediatric NursePractitioner, and worked for many years in the Pedi-atric Emergency Department at Strong Memorial Hospi-tal (Rochester, New York).
A highly successful author and editor, Dr. Veen-ema has published books and multiple articles onemergency nursing and disaster preparedness. The firstedition of this textbook, published in August 2003, re-ceived an American Journal of Nursing Book-of-the-YearAward.
Dr. Tener Goodwin Veenema, in her role as Chief Ex-ecutive Officer of the TenER Consulting Group, LLC, isthe author and developer of “ReadyRN: A Comprehen-sive Curriculum for Disaster Nursing and Emergency
Preparedness” and collaborated with the American RedCross to customize the ReadyRN curriculum for useby the American Red Cross in educating and trainingAmerican Red Cross health care professionals in pro-viding health-related disaster and emergency responseservices.
Dr.Veenema’s ReadyRN Comprehensive Curriculumfor Disaster Nursing and Emergency Preparedness wasalso published in 2007 as an innovative e-learning onlinecourse by Elsevier, and the companion ReadyRN Hand-book for Disaster Nursing and Emergency Preparednesswill be published in fall 2007.
While at the University of Rochester, Dr. Veenemadeveloped the curriculum for a 30-credit Masters pro-gram entitled “Leadership in Health Care Systems: Dis-aster Response and Emergency Management,” the firstprogram of its kind in the country to be offered at aschool of nursing. The program offers course contenton the Fundamentals of Disaster Management, Chemi-cal, Biological and Radiological Terrorism, Global PublicHealth and Complex Human Emergencies, Leadershipand Strategic Decision Making, and Communication inDisaster Response and Emergency Preparedness.
Dr. Veenema has served as a reviewer to the In-stitute of Medicine Committee on the Review Panel forthe Smallpox Vaccination Implementation, Jane’s Chem-Bio Handbook, 2nd Edition, and serves on the edito-rial board for the journal Disaster Management andResponse, sponsored by the Emergency Nurses Associa-tion. Dr. Veenema is an Associate Editor for the Journalof Disaster Medicine and Public Health Preparedness,sponsored by the American Medical Association.
Dr. Veenema frequently serves as a subject-matterexpert for the National American Red Cross, multiplestate health departments and nurses associations, aswell as the Registered Nurses Association of Ontario,Canada. She is a member of the World Association ofDisaster Medicine (WADEM).
ii

Copyright C© 2007 Springer Publishing Company, LLC
All rights reserved.
No part of this publication may be reproduced, stored in a retrieval system, ortransmitted in any form or by any means, electronic, mechanical, photocopying,recording, or otherwise, without the prior permission of Springer PublishingCompany, LLC.
Springer Publishing Company, LLC11 West 42nd StreetNew York, NY 10036–8002www.springerpub.com
Acquisitions Editor: Sally J. BarhydtProduction Editor: Matthew ByrdCover Design: Mimi FlowComposition: Aptara
07 08 09 10/ 5 4 3 2 1
Library of Congress Cataloging-in-Publication Data
Disaster nursing and emergency preparedness for chemical, biological, and radiologicalterrorism and other hazards / Tener Goodwin Veenema. – 2nd ed.
p. ; cm.Includes bibliographical references and index.ISBN-13: 978-0-8261-2144-8ISBN-10: 0-8261-2144-61. Disaster nursing. 2. Emergency nursing. I. Veenema, Tener Goodwin.
[DNLM: 1. Disasters. 2. Emergency Nursing. 3. Terrorism. WY 154 D6109 2007]
RT108.D56 2007616.02′5–dc22
2007012380
Printed in the United States of America by Bang Printing

Preface
It is quite probable that at some time in the future, nursesmay be called upon to respond to a mass casualty eventor disaster outside of the hospital. Advance preparationof our national nursing workforce for such an event ispredicted on the belief that mastery of the knowledge andskills needed to respond appropriately to such an eventcan improve patient outcomes.
I wrote these words in the spring of 2002 as I fin-ished the summary section of chapter 9 (p. 199) in thefirst edition of this book—3 1/2 years before HurricaneKatrina would wreak its devastation on the communi-ties of the Gulf Coast. When the first edition of thebook was released, our country was still reeling from the9/11 attacks and fearful of another outbreak of anthrax.These two events had resulted in an immediate aware-ness of our lack of national emergency preparedness andheightened vulnerability to disaster events. Health careproviders were barraged by an onslaught of informationfrom numerous sources (of varying quality) regardingtopics such as disaster planning and response, biologi-cal agents, hazardous materials accidents, the dangersof radiation, therapeutics, and so forth. Resources onthe Internet alone had increased exponentially. My ownresearch on these topics had revealed that the existingdisaster textbooks were written by and for physiciansand public health officials. There was a major gap in theliterature for nurses. Given the approximately 2.7 mil-lion nurses in this country, I found this to be not onlyunacceptable but a major threat to population healthoutcomes. Therefore, the genesis of the book was the de-sire to fill this gap in the literature and to provide nurseswith a comprehensive resource that was evidence basedwhenever possible, and broad in scope and deep in de-tail. We were very successful and the first edition was ex-tremely well received, garnering an AJN Book of the Yearaward along with multiple additional accolades, and forthat I am eternally grateful. The book is currently beingused nationwide by universities and schools of nursing,hospitals, public health departments, and multiple othersites where nurses work.
The second edition of this textbook has an equallyambitious goal—to once again provide nurses and nursepractitioners with the most current, valid, and reliableinformation available for them to acquire the knowledge
and skill set they will need to keep themselves, their pa-tients, and families safe during any disaster event. Onceagain, we have held ourselves to the highest standardspossible. Every chapter in the book has been researched,reviewed by experts, and matched to the highest stan-dards for preparing health professions’ students for ter-rorism, disaster events, and public health emergencies.
The framework of the book is consistent with theUnited States National Response Plan, the National In-cident Management System, and is based on the Cen-ters for Disease Control and Prevention’s (CDC) Com-petencies for public health preparedness and the CDCGuidelines for response to chemical, biological, and ra-diological events. This textbook will provide nurses witha heightened awareness for disasters and mass casualtyincidents, a solid foundation of knowledge (educationalcompetencies) and a tool box of skills (occupationalcompetencies) to respond in a timely and appropriatemanner.
Since September 11, 2001, our national concerns forthe health and safety of our citizens has expanded toinclude additional hazards such as emerging infectiousdiseases (SARS, West Nile virus, avian influenza), thedetonation of major explosive devices, and the use ofnuclear weapons by countries unfriendly to the UnitedStates. We possess a heightened awareness of the forcesof Mother Nature and the health impact on communi-ties affected by natural disasters. We continue to face agrowing national shortage of nurses and nurse educa-tors, a health care system that is severely stressed finan-cially, and emergency departments that are functioningin disaster mode on a daily basis. We have reason to be-lieve that these challenges for the profession will onlyintensify in the coming years. Nurses are challenged tobe prepared for all hazards—to plan for pandemic in-fluenza, chemical, biological, radiological/nuclear, andexplosive (CBRNE) events, mass casualty incidents in-volving major burns, and surge capacity to accommo-date a sudden influx of hundreds, possibly thousands, ofpatients. In response to these concerns and the requestsof nurses across the country, I have added several newchapters in the second edition that serve to strengthenthe health systems focus of the book and to add a strongclinical presence.
v

vi Preface
Since 2003, the Department of Homeland Security,the Federal Emergency Management Administration(FEMA), the CDC, and other federal and nonfederalagencies have devoted significant resources to increas-ing our level of national emergency preparedness. Wehad made significant progress on certain fronts, but withregard to our level of workforce preparedness in thehealth professions, we have a long way to go. In theyears since the first edition of this textbook was pub-lished, other nursing texts and educational resourceshave been developed and published, and this author ap-plauds these initiatives. There is much work to be done,and it is personally rewarding to witness increased in-terest in disaster nursing as more nurses get involved.
As an emergency nurse and pediatric nurse practi-tioner, I have worked in the field of disaster nursing andemergency preparedness for many years, with a focus onpromoting the health of the community and the healthof the consumer by structuring, developing, and foster-ing an environment that is prepared for any disaster ormajor public health emergency. I have lobbied for theadvancement of the profession of nursing in the disas-ter policy and education arena, and I remain personallycommitted to my work in preparing a national nurs-ing workforce that is adequately prepared to respond toany disaster or public health emergency. This includesworking to establish sustainable community partner-ships that foster collaboration and mutual planning forthe health of our community. It includes looking at inno-vative applications of technology to enhance sustainablelearning and disaster nursing response. It means givingreflective consideration of the realities of the clinical de-mands placed on nurses during catastrophic events andthe need for consideration of altered standards for clini-cal care during disasters and public health emergencies.
This textbook continues to be a reflection of mylove for writing and research, as well as a deep desire tohelp nurses protect themselves, their families, and theircommunities. Disaster nursing is a patient safety issue.Nurses can only protect their patients if they them-selves are safe first. The second edition represents asubstantive attempt to collect, expand, update, and in-clude the most valid and reliable information currentlyavailable about various disasters, public health emer-gencies, and acts of terrorism. The target audience forthe book is every nurse in America—making every nursea prepared nurse—staff nurses, nurse practitioners, ed-ucators, and administrators. The scope of the book isbroad and the depth of detail intricate. My goal is to pro-duce a second edition that represents a well-researchedand well-organized scholarly work that will serve as amajor reference for all our nation’s nurses on the top-ics of disaster nursing and emergency preparedness. It ismy hope that nurse educators will be pleased to discoverthe expanded organization of the book and the inclusionof new chapters, case studies, and study questions. Theinsertion of Internet-based activities is designed to stim-ulate critical thinking in students and to provide themwith the skill set to stay updated regarding these topics.
Ideally, this book represents the foundation for bestpractice in disaster nursing and emergency preparedness,and is a stepping stone for the discipline of disaster nurs-ing research. Chapters in this book were based on em-pirical evidence whenever it was available. However,the amount of research in existence addressing disasternursing and health outcomes is limited, and much workremains to be done. The editor welcomes constructivecomments regarding the content of this text.
Tener Goodwin Veenema

Acknowledgments
As with the first edition of this book, I continue to pro-fess that researching, revising, designing, and deliver-ing this book was a true labor of love—I enjoyed everyminute of it! And like any effective disaster response,this textbook was a coordinated team effort. The secondedition is significantly larger than the first—several newchapters have been added, all of the content updated,and the clinical focus expanded. Additionally, the en-tire book has been mapped to the Centers for DiseaseControl and Prevention’s competencies for public healthemergency preparedness—this represents nothing lessthan a Herculean effort. There are so many exceptionalindividuals, all over the country, who helped to makethis book a reality.
My special thanks must first go to each of the won-derful chapter authors who researched, reviewed, andrevised their manuscripts, assuring that the informationcontained within was valid, accurate, and reliable, andreflected the most current state of the science. This wasa tremendous challenge given the highly transitional na-ture of many of the topic areas. The science was rapidlyevolving (and continues to evolve) and as with the firstedition, the structure of many disaster and emergencyresponse systems was rapidly changing (and continuesto change) during the year it was written.
I would like to first thank my fabulous colleagueswho were chapter authors and/or contributors for thefirst edition and stayed committed to this project for thesecond edition. My very sincere thanks go to KathleenCoyne Plum, PhD, RN, NPP (Monroe County Depart-ment of Human Services); Kristine Qureshi, RN, CEN,DNSc (University of Hawaii); Brigitte L. Nacos, PhD andKristine M. Gebbie, DrPH, RN, FAAN (Columbia Univer-sity); Lisa Marie Bernardo, RN, PhD, MPH (Universityof Pittsburgh); Erica Rihl Pryor, RN, PhD and Dave Pig-ott, MD, FACEP (University of Alabama); Linda Landes-man, DrPH, MSW, ACSW, LCSW, BCD (NYC Health &Hospitals Consortium); Kathryn McCabe Votava, PhD,RN and Cathy Peters, MS, RN, APRN-BC (University ofRochester); P. Andrew Karam, PhD, CHP (MJW Cor-poration); Joan Stanley, PhD, RN, CRNP (AmericanAssociation of Colleges of Nursing); Lt. Col. RichardRicciardi, RN, FNP and Patricia Hinton Walker, PhD,RN, FAAN (Uniformed Services University of the Health
Services); Janice B. Griffin Agazio, PhD, CRNP, RN(The Catholic University of America); Eric Croddy, MA(Monterey Institute for International Studies); and GaryAckerman, MA (Center for Terrorism and IntelligenceStudies). Thank you so much for your wonderful con-tributions and for your ongoing support of this book.
Very special acknowledgments and many thanksgo to my international colleagues at the University ofUlster—Pat Deeny, Kevin Davies, and Mark Gillespie,and welcome to Wendy Spencer. These wonderful in-dividuals were committed to providing a broad and il-lustrative international perspective for the book. Theirresultant chapter, Global Issues in Disaster Relief Nurs-ing, is evidence of their expert knowledge, extensiveexperience in the field, and dedication to internationalcollegiality. I will always remain grateful to each of themfor their contributions to the field.
My thanks go once again to Jonathan Tucker, myspecial contributor, for allowing me to reprint a portionof his work from his wonderful book Scourge: The Onceand Future Threat of Smallpox. It continues to be theperfect segue into the Chemical and Biological Terrorismsection of the book.
I wish to thank each of the case study authors andwelcome the following new authors to the second edi-tion of the book. Thanks go to Ziad N. Kazzi, MD,FAAEM, along with his colleagues Dave Pigott, MD,FACEP and Erica Pryor, RN, PhD at the University of Al-abama at Birmingham Center for Disaster Preparedness.The quality of their work is incredible, as is their gen-erosity in sharing it.
Another very special welcome and thanks go toRoberta Lavin (Health and Human Services) and LynnSlepski (Department of Homeland Security). Robertaand Lynn made sure that the descriptions of the Na-tional Response Plan and all components of the federaldisaster program were as accurate as possible up to thetime of publication. They are also two of the nicest andmost generous individuals one would ever want to meet.
Welcome and thanks go to Christopher Lentz, MD,FACS, FCCM; Dixie Reid, PA; Brooke Rea, MS, RN; andKerry Kehoe, MS (University of Rochester) for theirchapter addressing the recognition and management ofburns and guidelines for disaster planning for a surge of
vii

viii Acknowledgments
burn patients. Dr. Lentz, as the Director of the regionalBurn/Trauma Center at the University of Rochester Med-ical Center, along with his wife Dixie Reid, are burnexperts and tireless advocates for clinical excellence inthe care of the severely burned patient. Both Brooke Rea(Burn Program Manager) and Kerry Kehoe (former Ad-ministrator Division of Trauma & Burn) are graduates ofthe Leadership in Health Care Systems in Disaster Re-sponse and Emergency Health Care Systems, and so itis an even greater pleasure to be able to include them inthis edition of the book. Brooke’s talents and leadershipskills were clearly evident in her effort to produce thischapter, and I send her my special thanks.
A sincere welcome and thanks go out to two newauthors and former students of mine, Tara Sacco, MS,BS, RN and Jennifer Byrnes, MLS, MPH (Universityof Rochester). Tara is a graduate of the Leadership inHealth Care Systems program in Health Promotion andHealth Education; Jennifer is a graduate of the Mas-ter’s in Public Health program. Both are talented re-searchers and writers, and it is my guess that you willbe hearing more from them in the future. Their chapterson Traumatic Injuries Due to Explosions and Blast Ef-fects, and Emerging Infectious Diseases (respectively)broadly expanded the clinical focus of the book andprovided valuable new clinical resource information fornurses.
Welcome and thanks go to Amy T. Campbell, JD,MBE (University of Rochester, Division of Medical Hu-manities) for her detailed legal review and update of thechapter on Legal and Ethical Issues in Disaster Responseand to Joy Spellman (Burlington County College, NewJersey) for her contributions on preparing and promot-ing the role of the public health nurses during disasters.Both of these authors were so gracious and generouswith their expertise. Thank you.
A very special warm welcome and thanks go toElizabeth A. Davis, JD, Ed.M and her colleagues AlanClive, PhD, Jane A. Kushma, PhD, and Jennifer Mincin,MPA. Elizabeth is the Founder and President of Eliza-beth Ann Davis Associates (http://www.eadassociates.com/) and is a nationally recognized expert/advocatefor vulnerable populations. It was extremely importantto me to add a substantive piece on planning for andresponding to the needs of high-risk, high-vulnerabilitypopulations in this edition of the book, and Alan, Eliz-abeth, Jane, and Jennifer provided a superb chapter onthis topic (and in a relatively short time frame). My sin-cere thanks and admiration go out to each of you foryour work.
Welcome and gratitude go to Manish Shah, MD,MPH, FACEP; Jeremy Cushman, MD, MS; Charles Mad-dow, MD, FACEP; and Jonnathan Busko, MD, MPH,EMT-P (University of Rochester, Department of Emer-gency Medicine), and to my colleague John Benitez,MD, MPH at the Center for Disaster Medicine and
Emergency Preparedness (University of Rochester, De-partment of Emergency Medicine). Manish Shah, alongwith his colleagues Jeremy, Charles, and Jonnathan,contributed a comprehensive overview of EmergencyMedical Services as it currently exists in this country.This well-designed and well-organized chapter was awonderful new addition to the book. John Benitez isDirector of the Western New York Regional Poison Con-trol Center, who along with Sharon Benware, RN, con-tributed to the chapter addressing chemical agents ofconcern.
I want to express my continued appreciation andsincere gratitude to Lisa Bernardo, Erica Pryor, Kris-tine Qureshi, and Kathy Plum for their elegant contri-butions, for their ongoing support and encouragement,and for their willingness to make recommendations thatstrengthened the content of the book. I have the ultimaterespect for each of you, and I am sincerely grateful forour ongoing relationships!
Special thanks go out to my wonderful friends andcolleagues, Diane Yeater, Associate Director for DisasterHealth Services and to Nancy McKelvey, Chief Nurseat the American Red Cross, National Headquarters inWashington, DC. Thank you for your contributions andyour insight into national disaster preparedness and re-sponse initiatives.
I am so fortunate to call the University of RochesterSchool of Nursing my academic home. This phenom-enal school is a leader in excellence in nursing edu-cation and in entrepreneurship for nurses, and I havelearned something from every one of my talented col-leagues. I wish to once again thank Dean Patricia Chiver-ton for creating an environment that supports new andvisionary initiatives and for supporting and encourag-ing me to do the work that I want to do. I am eternallygrateful to Pat and to each of my fellow faculty mem-bers in the Leadership in Health Care Systems Master’sProgram.
As I finish the second edition of this book, I wouldalso like to acknowledge 19 wonderfully talented in-dividuals and very special, terrific friends—my col-leagues in the 2004 Robert Wood Johnson Execu-tive Nurse Fellowship: Carla Baumann, Suzanne Boyle,Kathleen Capitulo, June Chan, Theresa Daggi, KathrynFiandt, Margaret Frankhauser, Mary Hooshmand, PaulKuehnert, Mary Joan Ladden, Joan Marren, MarciaMaurer, Marcella McKay, Wanda Montalvo, KathleenMurphy, Cheri Rinehart, Mary Lou de Leon Siantz,Kristen Swanson, and Bonnie Westra. We have sharedan amazing experience in this wonderful program, andthey have provided me with insight and guidance formy work, of which this book represents a portion of theoverall project—ReadyRN: Making Every Nurse a Pre-pared Nurse. Their incredible work inspired me. Butmostly I am grateful for the fun, friendship, and sup-port they offered. They believed in my vision for disaster

Acknowledgments ix
nursing and for this book, and they are always there forme when I need them. Thank you.
Special thanks to Loretta Ford, former Dean and Pro-fessor Emeritus at the University of Rochester School ofNursing, and founder of the nurse practitioner role. Ihave had the amazing good fortune of having Lee as mymentor in the Robert Wood Johnson Executive NurseFellowship Program. There are no words to describethis feisty, energetic, phenomenally talented nurse andscholar. She is a role model to the entire profession ofnursing, and my life is richer for having known her.Her wisdom and guidance have played a pivotal role inmuch of my work the past few years. Her kindness andsupport have sustained me. Thank you so much Lee.
I wish to thank all of my reviewers and those whoprovided valued commentary and recommendations.Special thanks to Lori Barrette (University of Rochester),Janice Springer (American Red Cross), and Lou Romig,MD, FAAP, FACEP. Just as there is no perfect researchstudy, there is also not a perfect textbook or referencemanual. This fact, however, did not dissuade us fromseeking to make this book and every section in it thevery best it could be. Many thanks to all who sharedtheir wisdom and expertise during the preparation ofthe book.
I would like to acknowledge Sally Barhydt and hercolleagues at Springer Publishing Company in New YorkCity. I sincerely thank you, Sally, for all your hard workin assisting with the publication of the second edition,and for your ongoing commitment to me as an author.
I will be eternally grateful to my colleague and re-search assistant Adam B. Rains for his assistance withthe preparation of this very large manuscript. Adam’s in-telligence, humor and wit—and limitless talent—were agift to this project.
Many thanks go to three very special women whoare the best friends anyone could ask for—KatherineLostumbo, Barbara Wale, and Maryanne Townsend. Thewarmth of your friendship continues to sustain me.
Finally, the people to whom I owe the most are myfamily. To my mother, thank you for all you have donefor me and for thinking that I am much more capablethan I really am. You often told me, “to thine own selfbe true,” when making my life’s decisions—great advicethat I have often passed down to my children. Thanksto my dad—I love you lots.
To my four children, I sincerely thank you for thejoy you have brought to my life. You are my greatestaccomplishment. My sons Kyle, Blair, and Ryne—I loveyou so much. A huge and especially special thank yougoes to my wonderful daughter Kendall, who has beena terrific help to me for many, many years. Her wordsof encouragement (and the sound of her laughter) havealways kept me going! She is my very best friend andthe most incredible person I know.
And to my husband and partner in all life’s adven-tures, my deepest thanks. I could not have done any ofthis without you. You have helped me in too many waysto mention, and I am so appreciative of each and everymoment we have shared. Thank you.

Contributors
Gary Ackerman, MADirectorCenter for Terrorism and Intelligence StudiesA Division of the Akribis GroupSan Jose, California
Janice B. Griffin Agazio, PhD, CRNP, RNAssistant ProfessorThe Catholic University of AmericaSchool of NursingWashington, DC
Sherri-Lynne Almeida, DrPH, MSN, Med, RN, CENChief Operating Officer—Team Health SouthwestHouston, Texas
Knox Andress, RN, FAENDesignated Regional CoordinatorLouisiana Region 7 Hospital PreparednessDirector of Emergency PreparednessLouisiana Poison CenterShreveport, Louisiana
Randal D. Beaton, PhD, EMTResearch ProfessorDepartment of Psychosocial and CommunityHealthSchool of NursingAdjunct Research ProfessorDepartment of Health ServicesSchool of Public Health and Community MedicineUniversity of WashingtonSeattle, Washington
John G. Benitez, MD, MPHAssociate Professor of Emergency Medicine,Environmental Medicine and PediatricsUniversity of Rochester School of Medicine andDentistryDirector, Finger Lakes Regional Resource CenterManaging and Associate Medical DirectorRA Lawrence Poison and Drug Information CenterRochester, New York
Sharon Benware, RN, CSPIRA Lawrence Poison and Drug Information CenterRochester, New York
Lisa Marie Bernardo, RN, PhD, MPHAssociate ProfessorUniversity of Pittsburgh School of NursingPittsburgh, Pennsylvania
Jonnathan Busko, MD, MPH, EMT-PEmergency Physician / Medical Director,OperationsEastern Maine Medical CenterBangor, MaineRegional Medical Director, Maine EMSRegion 4Medical Director, Maine Medical Strike TeamNew England MMRSMedical Director, Northeastern Maine RegionalResource Center andCenter for Emergency PreparednessEastern Maine Healthcare System
Jennifer A. Byrnes, MLS, MPHUniversity of Rochester School of Medicineand DentistryRochester, New York
Amy T. Campbell, JD, MBEDivision of Medical HumanitiesUniversity of Rochester Medical CenterRochester, New York
Alan Clive, PhDEmergency Management ConsultantSilver Spring, Maryland
Eric Croddy, MASenior Research AssociateMonterey Institute of International StudiesCenter for Nonproliferation StudiesMonterey, California
xi

xii Contributors
Jeremy T. Cushman, MD, MSDivision of EMS and Office of PrehospitalCareDepartment of Emergency MedicineUniversity of Rochester School of Medicine andDentistryRochester, New York
Kevin Davies, RRC, RN, MA, RNT, PGCESenior Lecturer in NursingSchool of Care SciencesUniversity of GlamorganPontypridd, South Wales, United Kingdom
Elizabeth A. Davis, JD, Ed.MDirectorEAD & Associates, LLCEmergency Management & Special Needs ConsultantsNew York, New York
Pat Deeny, RN, RNT, BSc (Hons) NursingAd Dip Ed.Senior Lecturer in NursingUniversity of Ulster, Magee CampusDerry-Londonderry, Northern Ireland
Mary Kate Dilts Skaggs, RN, MSNDirector of Nursing Emergency ServicesSouthern Ohio Medical CenterPortsmouth, Ohio
Kristine M. Gebbie, DrPH, RN, FAANElizabeth Standish Gill Associate ProfessorColumbia University School of NursingCenter for Health PolicyNew York, New York
Mark Gillespie, RN, MScAdvanced Nursing, Critical Nurse SpecialistLecturer Trauma NursingUniversity of Ulster, MageeDerry-Londonberry, Northern Ireland
Kevin D. Hart, JD, PhDAssistant ProfessorDepartment of Community and PreventativeMedicineUniversity of Rochester School of Medicineand DentistryRochester, New York
Angela J. Hodge, RN, BSN, CENClinical Coordinator for Emergency ServicesSouthern Ohio Medical CenterPortsmouth, Ohio
P. Andrew Karam, PhD, CHPSenior Health PhysicistMJW CorporationRochester, New York
Ziad N. Kazzi, MD, FAAEMAssistant ProfessorMedical ToxicologistDepartment of Emergency MedicineUniversity of AlabamaBirmingham, Alabama
Kerry Kehoe, MSAdministrator, Division of Trauma, Burn &Emergency SurgeryUniversity of Rochester Medical CenterRochester, New York
Paul Kuehnert, MS, RNDeputy DirectorKane County Department of HealthAurora, Illinois
Jane A. Kushma, PhDAssociate ProfessorInstitute for Emergency PreparednessJacksonville State UniversityJacksonville, Alabama
Linda Young Landesman, DrPH, MSW, ACSW,LCSW, BCDNYC Health and Hospitals CorporationNew York, New York
Roberta Proffitt Lavin, MSN, APRN, BCCAPT, United States Public Health ServiceDirector, Office of Human Services EmergencyPreparedness and ResponseAdministration for Children and FamiliesDepartment of Health and Human ServicesWashington, DC
Christopher W. Lentz, MD, FACS, FCCMMedical Director, Strong Regional Burn CenterAssociate Professor of Surgery andPediatricsUniversity of Rochester School of Medicine andDentistryRochester, New York
Charles L. Maddow, MD, FACEPDepartment of Emergency MedicineUniversity of Rochester School of Medicine andDentistryRochester, New York

Contributors xiii
Nancy McKelvey, MSN, RNChief Nurse/Healthcare Partnerships LeadAmerican Red CrossWashington, DC
Jennifer Mincin, MPASenior Project ManagerEAD & Associates, LLCEmergency Management & Special Needs ConsultantsNew York, New York
Brigitte L. Nacos, PhDDepartment of Political ScienceColumbia UniversityNew York, New York
Karen NasonExecutive DirectorAssociation of Rehabilitation NursesRehabilitation Nursing Certification Board
Sally A. Norton, PhD, RNAssistant Professor of NursingUniversity of Rochester School of NursingRochester, New York
Cathy Peters, MS, RN, APRN-BCAssistant Clinical ProfessorUniversity of Rochester School of NursingAssistant Clinical Professor, Adjunct FacultyDivision of Medical HumanitiesUniversity of Rochester School ofMedicineRochester, New York
David C. Pigott, MD, FACEPResidency Program DirectorAssociate Professor and Vice Chair for EducationDepartment of Emergency MedicineUniversity of Alabama at BirminghamBirmingham, Alabama
Kathleen Coyne Plum, PhD, RN, NPPDirector, Office of Mental Health,Monroe County Department of Human ServicesRochester, New YorkAdjunct Associate Professor, University of RochesterSchool of NursingRochester, New York
Erica Rihl Pryor, RN, MSN, PhDDoctoral Program Coordinator and Assistant ProfessorUniversity of Alabama School of NursingUniversity of Alabama at BirminghamBirmingham, Alabama
Kristine Qureshi, RN, CEN, DNScAssociate ProfessorSchool of Nursing and Dental HygieneUniversity of Hawaii at ManoaHonolulu, Hawaii
Irwin Redlener, MDAssociate Dean & DirectorThe National Center for Disaster PreparednessColumbia University Mailman School of Public HealthNew York, New York
Dixie Reid, PAPhysician AssistantTrauma/Burn/Emergency SurgeryUniversity of Rochester School of Medicine andDentistryRochester, New York
Brooke Rera, MS, RNBurn Program ManagerUniversity of Rochester/Strong Memorial HospitalRochester, New York
Lt. Col. Richard Ricciardi, RN, FNPUniformed Services University of the Health SciencesGraduate School of NursingBethesda, Maryland
Lou E. Romig, MD, FAAP, FACEPPediatric Emergency MedicineMiami Children’s HospitalPediatric Medical Advisor, Miami-Dade Fire RescueDepartmentSouth Florida Regional Disaster Medical AssistanceTeam (FL-5 DMAT)Miami, Florida
Tara Sacco, MS, BS, RNBurn Trauma UnitUniversity of Rochester Medical CenterRochester, New York
Manish N. Shah, MD, MPH, FACEPDirector, EMS ResearchAssistant ProfessorDepartment of Emergency MedicineDepartment of Community and Preventive MedicineUniversity of Rochester School of Medicine andDentistryRochester, New York
Capt. Lynn A. Slepski, RN, MSN, PhD-C, CCNSSenior Public Health AdvisorDepartment of Homeland SecurityWashington, DC

xiv Contributors
Joy Spellman, MS, RNDirector, Center for Public Health PreparednessBurlington County CollegeMt. Laurel, New Jersey
Wendy SpencerUniversity of Ulster
Janice Springer, RN, PHN, MADisaster Health ServicesAmerican Red CrossWashington, DC
Joan M. Stanley, PhD, RN, CRNPDirector of Education PolicyAmerican Association of Colleges ofNursingWashington, DC
Jennifer TimonyPresidentNational Student Nurses’ Association, Inc.
Kathryn McCabe Votava, PhD, RNPresidentGoodCare.comWashington, DC
Patricia Hinton Walker, PhD, RN, FAANVice President for Nursing Policy and ProfessorUniformed Services University of theHealth SciencesBethesda, Maryland
Dianne YeaterDirector for Disaster Health ServicesAmerican Red CrossWashington, DC

Dedication
Our world is not safe. Fraught with peril, it continuesto be a dangerous place in which to live. And yet weknow that our children need safe homes, safe schools,and safe communities to live in if they are to grow tobe healthy, happy, and secure adults. They are countingon us to be there for them—no matter what the cir-cumstances. They are counting on us to provide love,protection, and a safe harbor in the storm. They arecounting on us to be prepared. They are counting on usto rescue them when they need rescuing. This textbookis dedicated to our nation’s children—four in particular.To Kyle, Kendall, Blair, and Ryne—you are everything tome. Always know how much I love you and that homeis a safe harbor. And know that I tried to make the worlda safer place.
xv

Foreword
Most doctors, nurses, and other health workers look for-ward to a life pursuing their chosen career in relativeorder, peace, and tranquility. However, the unexpected,by its very nature, can strike anywhere, at any time, andinvolve anybody or everybody, including those who areunprepared. A disaster can happen in any communityat any time. It is an inescapable fact brought into focusby the calamitous events we have seen befall our fellowcitizens in just the past 5 years. From the four hurri-canes that hit our coastal regions in just one 6-weekperiod in 2004 to the twin shocks of the South Asiatsunami and Hurricane Katrina; earthquakes in Indone-sia; floods; terrorist bombings in the London subwayand Iraq (an everyday phenomenon in Baghdad); anda humanitarian crisis of unimaginable horror in Sudan,it is clear that no community is immune. Nurses havea primary role in preparing for and managing medicalcare during these episodic, but catastrophic, events. Ona global scale, nurses are active participants in caringfor victims of a wide variety of disasters that take placeon an almost daily basis.
The second edition of Disaster Nursing and Emer-gency Preparedness for Chemical, Biological, and Radio-logical Terrorism and Other Hazards has been designedto provide emergency caregivers with a concise refer-ence for managing specific disaster-preparedness andresponse issues while providing the prerequisite back-ground necessary to begin an in-depth study of thehealth consequences of the most common types of dis-asters. The experience of the editor and many of thechapter authors is unique. The organizations for whichthey work cover the range of disasters that strike thisworld. We owe an enormous debt of gratitude to themall for their unstinting efforts to update this classic work.
Postdisaster evaluations conducted by nurses of themanagement of disasters by health professionals haveprovided critical data for mitigating the human impactof these events and enhancing future responses to disas-ters. This has been especially true regarding HurricaneKatrina. As a result, disaster management is well rec-ognized as far more than just triage and mass casu-alty management. Since the first edition of this bookwas published, we have seen significant changes inthe health management of disasters, whether natural
or man-made. It is increasingly appreciated that thephenomenon goes far beyond the punctual provisionof relief to the population affected and extends fromadvanced preparedness to the problems of long-termrehabilitation. While always emphasizing the use ofproven management methods and practices, Dr. Veen-ema challenges nursing health professionals with ques-tions that must still be answered in order for them torespond effectively in emergency situations. I know thatdecision makers at the highest echelons of governmenthave increasingly relied on the nursing profession toaddress the myriad problems facing a disaster-affectedcommunity.
In the relatively short period of time that has elapsedsince September 11, 2001, it is remarkable that a consid-erable body of new knowledge and experience relatedto the adverse health effects of disasters has already ac-cumulated. In fact, disaster research has accelerated tosuch an extent that we probably need to update the re-sults of this research at a minimum of every year so thatwe can apply the lessons learned during one disaster tothe management of the next. Conveying so much infor-mation in so few pages, with the right mix of scientificdata and human concern, in a practical and clear for-mat, is no mean task. As the most comprehensive text-book on disaster nursing ever published (except for thegroundbreaking first edition published in 2003), Disas-ter Nursing and Emergency Preparedness for Chemical,Biological, and Radiological Terrorism and Other Haz-ards does exactly that and more. With years of experi-ence, Dr. Veenema and co-authors give the reader ampletechnical descriptions of each kind of disaster (partic-ularly chemical, biological, radiological terrorism, andother hazards), an examination of the kinds of issuesand problems that arise in planning hospital and emer-gency department disaster response, and an up-to-datereview of the more common medical and managementissues that might face a nurse involved in a local disas-ter. Unique chapters include those addressing the legaland ethical issues in disaster response, the role of themedia, effective communication with the public (a ma-jor deficiency during Hurricane Katrina and the SouthAsia tsunami), the special needs of children during dis-asters and public health emergencies, and the evolving
xvii

xviii Foreword
priorities of the Departments of Health and Human Ser-vices and Homeland Security.
Like the first edition, the second edition includeswell-designed case studies that provide realistic, hands-on experiences that challenge the reader to apply infor-mation provided in the chapters. Dr. Veenema’s inclu-sion of “Key Messages” and “Learning Objectives” thatintroduce each major section of the book, plus uniquecase studies addressing natural, industrial, and terror-ism disasters, has resulted in the creation of a major re-source that will serve as a timely, comprehensive, andstructured text for the education of hospital, community,state, and national health and medical emergency man-agers, as well as nursing students who will assume ma-jor mass emergency preparedness responsibilities im-mediately after graduation.
It is incumbent that all health care workers, andnurses in particular, react professionally, efficiently, ra-tionally, and effectively when disaster strikes. To do so,they need some fundamental principles and knowledge
on which to base their activities. This highly topicalbook will serve as the most up-to-date course textbookand desk reference available not only for nursing pro-fessionals responsible for preparing their hospitals forresponding to disasters and other public health emer-gencies but also for emergency managers and other de-cision makers charged with ensuring that disasters arewell managed.
Eric K. Noji, MD, MPH, FACEPProgram Director
Pandemic Avian Influenza PreparednessProgram
Global Epidemic Intelligence NetworkCenter for Disaster Medicine & Humanitarian
AssistanceDepartment of Military & Emergency Medicine
Uniformed Services University of theHealth Sciences
Bethesda, Maryland

Foreword
In the years since the first edition of this book was pub-lished, the complexity of terrorism has continued to in-crease. We now are very aware that terrorists exist, notonly outside our country trying to get in, but also insideour country in small towns and large cities where someof our own citizens are plotting our downfall.
I have always said that nurses are the glue that holdsour health care delivery system (as fragmented as it is)together. Once a nurse, always a nurse! Nurses in ourcommunities are also expected to be able to respond tothe natural and man-made disasters that we will surelyencounter in the next few years. Our response must beevidence based, as is so well exemplified by these chap-ters. This text gathers together the best thoughts aboutevidence-based response wherever possible and identi-fies where the evidence is spotty and slim.
As the founder of the International Nursing Coali-tion for Mass Casualty Education in March 2001(now the Nursing Emergency Preparedness EducationCoalition), which now represents over 80 nursing orga-nizations, friends of nursing, and subject matter experts,I was not privy to any special vision. I knew that ourpublic health infrastructure was rickety—at best—andthat, in the event of any kind of mass casualty event,nurses would be expected to be in the forefront. I also
knew that disaster nursing had virtually disappearedfrom our curricula, although we still incorporated basicpopulation-based public health principles. If one goodthing comes out of the tragedy of 9/11, it will be thatmonies granted from Congress to address terrorism willserve a dual role and also help strengthen our publichealth infrastructure.
The book you are about to read offers a comprehen-sive analysis of a broad range of disasters possible in to-day’s world—both those wreaked by humans as well asby nature. This text is the next generation of informationneeded by nurses to be informed about and responsiveto the needs of our citizens in a disaster. Katrina was awake-up event. The roles that nurses and nurse assis-tants played in that disaster were selfless and inspiring.Katrina only served to undergird our awareness that wemust be vigilant and prepared!
Colleen Conway-Welch, PhD, RN, CNM, FAAN,FACNM
Nancy & Hilliard Travis Professor of NursingDean
Vanderbilt University School of Nursing
xix

Special Foreword
As a Robert Wood Johnson Executive Nurse Fellow, Dr.Veenema, a disaster nursing expert, chose to pursuea lofty fellowship goal of “creating a national nursingworkforce adequately prepared to respond to a disasteror any major public health emergency.” This monumen-tal undertaking sounds and is formidable. Still, this sec-ond edition of her highly successful earlier publication,Disaster Nursing, convinces me she is well on the waytoward that goal.
This expanded and updated edition is all encom-passing and forms the basis for all her other effortsin developing printware and software and educationalforums, coordinating and collaborating with volunteerand governmental agencies, and encouraging educa-tional and professional organizations to help preparenurses and other health professionals for natural andman-made disasters. The breadth and depth of this pub-lication are phenomenally comprehensive and practi-cal as well as theoretically and scientifically sound. Its
expanded scope ranges from preparedness and man-agement to specific types of disasters, ending withchapters on nursing education, research, and globalconnections.
I would find this edition particularly useful for itsteaching/learning framework that focuses the learneron goals and expected outcomes. Case studies expeditediscourse and critical thinking as do references and In-ternet sources.
In its expanded form and extensive content, this sec-ond edition is indeed required reading as a textbook, areference, a compendium of comprehensive topics, andfoundational to “making every nurse a prepared nurse.”
Loretta C. Ford, RN, PNP, EdDDean Emeritus
University of Rochester School of NursingFounder of the Nurse Practioner Program
xx

Contents
About the Editor . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . ii
Preface . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . v
Acknowledgments . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . vii
Contributors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . xi
Dedication . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . xv
Foreword (Eric K. Noji ) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . xvii
Foreword (Colleen Conway-Welch ) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . xix
Special Foreword (Loretta C. Ford ) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . xx
P A R T I
DISASTER PREPAREDNESS
Chapter 1 Essentials of Disaster Planning . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3Tener Goodwin Veenema
Chapter 2 Leadership and Coordination in Disaster Health Care Systems:The Federal Disaster Response Network . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25Roberta Lavin, Lynn Slepski, and Tener Goodwin Veenema
Chapter 3 Emergency Health Services . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 51Jeremy T. Cushman, Manish N. Shah, Charles L. Maddow, and Jonnathan Busko
Chapter 4 American Red Cross Disaster Health Services and Disaster Nursing . . . . . . . . . . . . . . . 67Dianne Yeater and Nancy McKelvey
Chapter 5 Understanding the Psychosocial Impact of Disasters . . . . . . . . . . . . . . . . . . . . . . . . . . 81Kathleen Coyne Plum
Chapter 6 Legal and Ethical Issues in Disaster Response . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 101Amy T. Campbell, Kevin D. Hart, and Sally A. Norton
Chapter 7 Crisis Communication: The Role of the Media . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 119Brigitte L. Nacos
xxi

xxii Contents
P A R T I I
DISASTER MANAGEMENT
Chapter 8 Disaster Management . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 137Kristine Qureshi and Kristine M. Gebbie
Chapter 9 Disaster Triage . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 161Kristine Qureshi and Tener Goodwin Veenema
Chapter 10 Restoring Public Health Under Disaster Conditions: Basic Sanitation, Waterand Food Supply, and Shelter . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 179Tener Goodwin Veenema
Chapter 11 Managing Emergencies Outside of the Hospital: Special Events, Mass Gatherings,and Mass Casualty Incidents . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 205Tener Goodwin Veenema
Chapter 12 Management of Burn Mass Casualty Incidents . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 221Christopher Lentz, Dixie Reid, Brooke Rera, and Kerry Kehoe
Chapter 13 Traumatic Injury Due to Explosives and Blast Effects . . . . . . . . . . . . . . . . . . . . . . . . . 239Tara Sacco
Chapter 14 Management of Psychosocial Effects . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 255Kathleen Coyne Plum and Tener Goodwin Veenema
Chapter 15 Unique Needs of Children During Disasters and Other Public Health Emergencies . . . . 273Lisa Marie Bernardo
Chapter 16 Identifying and Accommodating High-Risk and High-Vulnerability Populations . . . . . . . 309Alan Clive, Elizabeth A. Davis, Jane A. Kushma, and Jennifer Mincin
P A R T I I I
NATURAL AND ENVIRONMENTAL DISASTERS
Chapter 17 Natural Disasters . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 327Linda Young Landesman and Tener Goodwin Veenema
Chapter 18 Environmental Disasters and Emergencies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 351Tener Goodwin Veenema

Contents xxiii
P A R T I V
DISASTERS CAUSED BY CHEMICAL, BIOLOGICAL, AND RADIOLOGICAL AGENTS
Chapter 19 Biological and Chemical Terrorism: A Unique Threat . . . . . . . . . . . . . . . . . . . . . . . . . . 365Eric Croddy and Gary Ackerman
Chapter 20 Surveillance Systems for Detection of Biological Events . . . . . . . . . . . . . . . . . . . . . . . 389Erica Rihl Pryor
Chapter 21 Biological Agents of Concern . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 403David C. Pigott and Ziad N. Kazzi
Chapter 22 Early Recognition and Detection of Biological Events . . . . . . . . . . . . . . . . . . . . . . . . . 423Erica Rihl Pryor
Chapter 23 Emerging Infectious Disease . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 437Jennifer A. Byrnes
Chapter 24 Design and Implementation of Mass Immunization and ProphylacticTreatment Clinics . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 459Kathryn McCabe Votava
Chapter 25 Chemical Agents of Concern . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 483Tener Goodwin Veenema, John Benitez, and Sharon Benware
Chapter 26 Mass Casualty Decontamination . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 505Tener Goodwin Veenema
Chapter 27 Radiological Incidents and Emergencies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 521Andrew Karam
P A R T V
SPECIAL TOPICS
Chapter 28 Directions for Nursing Education . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 545Joan M. Stanley and Tener Goodwin Veenema
Chapter 29 Directions for Nursing Research and Development . . . . . . . . . . . . . . . . . . . . . . . . . . . 559Richard Ricciardi, Janice B. Griffin Agazio, Roberta P. Lavin, andPatricia Hinton Walker

xxiv Contents
Chapter 30 Global Issues in Disaster Relief Nursing . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 571Pat Deeny, Kevin Davies, Mark Gillespie, and Wendy Spencer
Chapter 31 The Role and Preparation of the Public Health Nurse for Disaster Response . . . . . . . . . 589Joy Spellman
Epilogue Disaster Recovery: Creating Sustainable Disaster-Resistant Communities . . . . . . . . . . 601Tener Goodwin Veenema
Appendices I Internet Resources on Disaster Preparedness, Emergency Care, andBioterrorism . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 603
II Glossary of Terms Commonly Used in Disaster Preparedness andResponse . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 607
III Bioterrorism and Emergency Readiness: Competencies for All PublicHealth Workers . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 615
IV Federal Emergency Management Agency: Emergency Response ActionSteps . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 617
V Anthrax Summary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 620
VI Botulism Summary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 621
VII Plague Summary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 622
VIII Smallpox Summary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 623
IX Tularemia Summary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 624
X Viral Hemorrhagic Fevers Summary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 625
XI Biological Weapon (BW) Agent Lab Identification . . . . . . . . . . . . . . . . . . . . . . 626
XII Patient Isolation Precautions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 630
XIII Creating a Personal Disaster Plan . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 632
INDEX . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 637

P A R T I
Disaster
Preparedness

Key Messages■ The frequency of natural disasters, the individuals affected by them, and the eco-
nomic costs associated with loss have been steadily increasing over recent years.■ While disasters are often unexpected, sound disaster planning can anticipate
common problems and mitigate the consequences of the event.■ Different types of disasters are associated with distinct patterns of illness and
injury, and early assessment of risks and vulnerability can reduce morbidity andmortality later on.
■ Effective disaster plans are based on knowledge of how people behave. Key com-ponents and common tasks must be included in any disaster preparedness plan.
■ The actual process of planning is more important than the resultant written planbecause those who participate in planning are more likely to accept preparednessplans in general.
■ Disaster planning must overcome apathy and complacency.■ Disasters are different from daily emergencies; most cannot be managed simply
by mobilizing additional personnel and supplies. Certain commonly occurringproblems can be anticipated and addressed during planning.
■ A professional mandate exists that calls for nurses to participate in the develop-ment of and serve as an integral part of a community’s disaster preparednessplan.
■ Nurses must participate as full partners with both the medical community andemergency management community in all aspects of disaster response andrecovery.
Learning ObjectivesWhen this chapter is completed, readers will be able to
1. Classify the major types of disasters based on their unique characteristics anddescribe their consequences.
2. Identify societal factors that have contributed to increased losses (human andproperty) as the result of disasters.
3. Describe two principles of disaster planning, including the agent-specific and theall-hazards approach, and the basic components of a disaster plan.
4. Discuss the five areas of focus in emergency and disaster planning: prepared-ness, mitigation, response, recovery, and evaluation.
5. Describe risk assessment, hazard identification, and vulnerability analysis.6. Assess constraints on a community’s or organization’s ability to respond.7. Describe the core preparedness actions.8. Recognize situations suggestive of an increased need for additional comprehen-
sive planning.

1Essentials of DisasterPlanningTener Goodwin Veenema
The principles of disaster planning, the common tasksconsistent across all disaster responses, and the keycomponents of a disaster preparedness plan areintroduced in this chapter. Definitions of the different typesof disasters are provided, along with a classificationsystem for disasters based on their common and uniquefeatures; onset, duration, and effect (immediateaftermath); and reactive period. The concept of thedisaster time line as an organizational framework forstrategic planning is introduced. The five areas of focus in
emergency and disaster preparedness—preparedness,mitigation, response, recovery, and evaluation—areaddressed. Risk assessment, hazard identification andmapping, and vulnerability analysis are presented asmethods for decision making and planning. The conceptsof disaster epidemiology and measurement of themagnitude of a disaster’s impact on population health areexplored. Situations suggestive of an increased need forplanning, such as bioterrorism and hazmat (hazardousmaterial) events, are addressed.
C H A P T E R O V E R V I E W
INTRODUCTION
Disasters have been integral parts of the human expe-rience since the beginning of time, causing prematuredeath, impaired quality of life, and altered health sta-tus. The risk of a disaster is ubiquitous. On average, onedisaster per week that requires international assistanceoccurs somewhere in the world. The recent dramatic in-crease in natural disasters, their intensity, the numberof people affected by them, and the human and eco-
nomic losses associated with these events have placedan imperative on disaster planning for emergency pre-paredness. Global warming, shifts in climates, sea-levelrise, and societal factors may coalesce to create futurecalamities. Finally, war, acts of aggression, and the inci-dence of terrorist attacks are reminder of the potentiallydeadly consequences of man’s inhumanity toward man.
A review of recent disasters since 2000—politicalstrife and conflicts in Angola, Afghanistan, Ethiopia,D.R. Congo, Sudan, Iraq, and Sierra Leone—indicatesthat few disasters are the result of a single cause and

4 Part I Disaster Preparedness
effect. The disasters unfolding in this century are fre-quently complex human emergencies associated withglobal instability, economic decay, political upheavaland collapse of government structures, violence andcivil conflicts, famine, and mass population displace-ments. The Sumatra tsunami and Hurricane Katrina,as well as the 2004 and 2006 hurricane seasons, pointto more natural disasters and their growing complex-ity, which create considerable challenges to disasterplanners.
In the United States, nurses constitute the largestsector of the health care workforce and will certainly beon the front lines of any emergency response. As part ofthe country’s overall plan for disaster preparedness, allnurses must have a basic understanding of disaster sci-ence and the key components of disaster preparedness,including the following:
(1) The definition and classification system for disastersand major incidents based on common and uniquefeatures of disasters (onset, duration, effect, and re-active period).
(2) Disaster epidemiology and measurement of thehealth consequences of a disaster.
(3) The five areas of focus in emergency and disasterpreparedness: preparedness, mitigation, response,recovery, and evaluation.
(4) Methods such as risk assessment, hazard identifica-tion and mapping, and vulnerability analysis.
(5) Awareness of the role of the nurse in a much largerresponse system.
This chapter introduces the reader to the princi-ples of disaster planning, the common tasks consistentacross all disaster responses, and the key componentsof a disaster preparedness plan.
DEFINITION AND CLASSIFICATIONOF DISASTERS
Disasters have many definitions. Disaster may be de-fined as any destructive event that disrupts the nor-mal functioning of a community. Disasters have beendefined as ecologic disruptions, or emergencies, of aseverity and magnitude that result in deaths, injuries,illness, and property damage that cannot be effectivelymanaged using routine procedures or resources and thatrequire outside assistance (Landesman et al., 2001).Health care providers characterize disasters by whatthey do to people—the consequences on health andhealth services. A medical disaster is a catastrophicevent that results in causalities that overwhelm thehealth care resources in that community (Al-Madhari& Zeller, 1997). Noji (1997) describes disasters quitesimply, as “events that require extraordinary efforts be-yond those needed to respond to everyday emergencies”
(p. 1). Disasters may be classified into two broad cate-gories: natural (those caused by natural or environmen-tal forces) or man-made (human generated). The WorldHealth Organization defines natural disaster as the “re-sult of an ecological disruption or threat that exceedsthe adjustment capacity of the affected community”(Lechat, 1979). Natural disasters include earthquakes,floods, tornadoes, hurricanes, volcanic eruptions, icestorms, tsunamis, and other geologic or meteorologi-cal phenomena. Man-made disasters are those in whichthe principal direct causes are identifiable human ac-tions, deliberate or otherwise (Noji, 1996). Man-madedisasters include biological and biochemical terrorism,chemical spills, radiological (nuclear) events, fire, ex-plosions, transportation accidents, armed conflicts, andacts of war.
Human-generated disasters can be further dividedinto three broad categories: (a) complex emergencies,(b) technologic disasters, and (c) disasters that are notcaused by natural hazards but occur in human settle-ments. Complex emergencies involve situations wherepopulations suffer significant casualties as a result ofwar, civil strife, or other political conflict. Some disastersare the result of a combination of forces such as drought,famine, disease, and political unrest that displace mil-lions of people from their homes. These humanitariandisasters can be epic in proportion, such as civilians flee-ing the Iraq war or refugees displaced by the conflict inDarfur. With technologic disasters, large numbers of peo-ple, property, community infrastructure, and economicwelfare are directly and adversely affected by major in-dustrial accidents; unplanned release of nuclear energy;and fires or explosions from hazardous substances suchas fuel, chemicals, or nuclear materials (Noji, 1996).The distinction between natural and human-generateddisasters may be blurred; a natural disaster, or phe-nomenon, may trigger a secondary disaster, the resultof weaknesses in the human environment. An exampleof this is a chemical plant explosion following an earth-quake. Such combinations, or synergistic disasters, arecommonly referred to as NA-TECHs (Natural and Tech-nological Disasters) (Noji, 1996). A NA-TECH disasteroccurred in the former Soviet Union, when windstormsspread radioactive materials across the country, increas-ing by almost 50% the land area contaminated in an ear-lier nuclear disaster. Disasters can and do occur simul-taneously (e.g., a chemical attack along with a nuclearassault), potentiating the death and devastation createdby each.
Disasters are frequently categorized based on theironset, impact, and duration. For example, earthquakesand tornadoes are rapid-onset events—short durationsbut with a sudden impact on communities. Hurricanesand volcanic eruptions have a sudden impact on acommunity; however, frequently advance warnings areissued enabling planners to implement evacuation andearly response plans. A bioterrorism attack may be

Chapter 1 Essentials of Disaster Planning 5
sudden and unanticipated and have a sudden and pro-longed impact on a community.
In contrast, droughts and famines have a more grad-ual onset or chronic genesis (the so-called creeping dis-asters) and generally have a prolonged impact. Factorsthat influence the impact of a disaster on a commu-nity include the nature of the event, time of day or year,health and age characteristics of the population affected,and the availability of resources (Gans, 2001). Furtherclassification of terms in the field of disaster sciencedistinguishes between hazards and disasters. Hazardspresent the possibility of the occurrence of a disastercaused by natural phenomena (e.g., hurricane, earth-quake), failure of man-made sources of energy (e.g.,nuclear power plant), or by human activity (e.g., war).
Defining an event as a disaster also depends on thelocation in which it occurs, particularly the populationdensity of that location. For example, an earthquake oc-curring in a sparsely populated area would not be con-sidered a disaster if no people were injured or affectedby loss of housing or essential services. However, theoccurrence of even a small earthquake could produceextensive loss of life and property in a densely pop-ulated region (such as Los Angeles) or a region withinadequate construction or limited medical resources.Similarly, numbers and types of casualties that mightbe handled routinely by a large university hospital ormetropolitan medical center could overwhelm a smallcommunity hospital.
Hospitals and other health care facilities may fur-ther classify disasters as either “internal” or “external.”External disasters are those that do not affect the hos-pital infrastructure but do tax hospital resources due tonumbers of patients or types of injuries (Gans, 2001).For example, a tornado that produced numerous in-juries and deaths in a community would be consideredan external disaster. Internal disasters cause disruptionof normal hospital function due to injuries or deathsof hospital personnel or damage to the physical plant,as with a hospital fire, power failure, or chemical spill(Aghababian, Lewis, Gans, & Curley, 1994). Unfortu-nately, one type of hospital disaster does not necessarilypreclude the other, and features of both internal and ex-ternal disasters may be present if a natural phenomenonaffects both the community and the hospital. This wasthe case with Hurricane Andrew (1992), which causedsignificant destruction in hospitals, in clinics, and in thesurrounding community when it struck south Florida(Sabatino, 1992), and Hurricane Katrina (2005) whenit impacted the Gulf Coast, rupturing the levee in NewOrleans (Berggren, 2005).
DECLARATION OF A DISASTER
In the United States, the Robert T. Stafford Disaster Re-lief and Emergency Assistance Act, passed by Congress
in 1988 and amended in 2000, provides for federal gov-ernment assistance to state and local governments tohelp them manage major disasters and emergencies.Under the Stafford Act, the president may provide fed-eral resources, medicine, food and other consumables,work assistance, and financial relief (Stafford Act). Onaverage, 38 presidential disaster declarations are madeper year; most are made immediately following im-pact, and review of recent years’ data suggests that thenumber of disasters is increasing (see Table 1.1; Fed-eral Emergency Management Agency [FEMA], 2007).If the consequences of a disaster are clear and im-minent and warrant redeployment actions to lessen
1.1 Federally Declared Disasters1976–2007
YEAR TOTAL DISASTER DECLARATIONS
1976 301977 221978 251979 421980 231981 151982 241983 211984 341985 271986 281987 231988 111989 311990 381991 431992 451993 321994 361995 321996 751997 441998 651999 502000 452001 452002 492003 562004 682005 482006 522007 14 (as of March, 2007)
Total 1,193
Average 38
Source: Federal Emergency Management Agency (2007). Retrieved3/07/07 from http://www.fema.gov/news/disaster totals annual.fema

6 Part I Disaster Preparedness
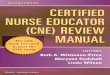
Figure 1.1 Billion dollar U.S. weather disasters, 1980–2004—National Oceanic and Atmo-spheric Administration.Source: Retrieved from the World Wide Web 5/10/06 at http://www.1.nedc.noaa.gov/pub/data/special/billion2004.pdf
or avert the intensity of the threat, a state’s gover-nor may request assistance even before the disasterhas occurred. A library of all past and current feder-ally declared disasters in the United States can be lo-cated at the FEMA Web site (http://www.fema.gov/library/dizandemer.shtm). A current list of internationaldeclared disasters and emergencies and links to diseaseoutbreaks can be located on the World Health Organi-zation’s Web site (http://www.who.int/health topics/disasters/en/).
HEALTH EFFECTS OF DISASTERS
Disasters affect communities and their populations indifferent ways. Damaged and collapsed buildings are ev-idence of physical destruction. Roads, bridges, tunnels,rail lines, telephone and cable lines, and other trans-portation and communication links are often destroyed.Public utilities (e.g., water, gas, electricity, and sewagedisposal) may be disrupted. A substantial percentage of
the population may be rendered homeless and forced torelocate temporarily or permanently. Disasters damageand destroy businesses and industry, agriculture, andthe economic foundation of the community. The im-pact of weather disasters alone has generated costs ofover a billion dollars (see Figure 1.1). The federal gov-ernment committed $85 billion to recovery efforts forHurricane Katrina alone. The health effects of disastersmay be extensive and broad in their distribution acrosspopulations (see chapter 8 for further discussion). Inaddition to causing illness and injury, disasters disruptaccess to primary care and preventive services. Depend-ing on the nature and location of the disaster, its effectson the short- and long-term health of a population maybe difficult to measure.
Epidemiology, as classically defined, is the quan-titative study of the distributions and determinants ofhealth-related events in human populations (Gordis,2004; see chapter 15 for further discussion). Disasterepidemiology is the measurement of the adverse healtheffects of natural and human-generated disasters and

Chapter 1 Essentials of Disaster Planning 7
the factors that contribute to those effects, with theoverall objective of assessing the needs of disaster-affected populations, matching available resources toneeds, preventing further adverse health effects, eval-uating program effectiveness, and planning for con-tingencies (Lechat, 1990; Noji, 1996). Disasters affectthe health status of a community in the followingways:
■ Disasters may cause premature deaths, illnesses, andinjuries in the affected community, generally exceed-ing the capacity of the local health care system.
■ Disasters may destroy the local health care infrastruc-ture, which will therefore be unable to respond to theemergency. Disruption of routine health care servicesand prevention initiatives may lead to long-term con-sequences in health outcomes in terms of increasedmorbidity and mortality.
■ Disasters may create environmental imbalances, in-creasing the risk of communicable diseases and envi-ronmental hazards.
■ Disasters may affect the psychological, emotional,and social well-being of the population in the affectedcommunity. Depending on the specific nature of thedisaster, responses may range from fear, anxiety, anddepression to widespread panic and terror.
■ Disasters may cause shortages of food and cause se-vere nutritional deficiencies.
■ Disasters may cause large population movements(refugees) creating a burden on other health care sys-tems and communities. Displaced populations andtheir host communities are at increased risk for com-municable diseases and the health consequences ofcrowded living conditions. (Noji, 1996)
THE DISASTER CONTINUUM
The life cycle of a disaster is generally referred to as thedisaster continuum, or emergency management cycle.This life cycle is characterized by three major phases,preimpact (before), impact (during), and postimpact (af-ter), and provide the foundation for the disaster timeline (Figure 1.2). Specific actions taken during thesethree phases, along with the nature and scope of theplanning, will affect the extent of the illness, injury, anddeath that occurs.
The five basic phases of a disaster management pro-gram include preparedness, mitigation, response, recov-ery, and evaluation (Kim & Proctor, 2002; Landesman,2001). There is a degree of overlap across phases, buteach phase has distinct activities associated with it.
Preparedness refers to the proactive planning effortsdesigned to structure the disaster response prior to itsoccurrence. Disaster planning encompasses evaluatingpotential vulnerabilities (assessment of risk) and the
propensity for a disaster to occur. Warning (also knownas forecasting) refers to monitoring events to look forindicators that predict the location, timing, and magni-tude of future disasters.
Mitigation includes measures taken to reduce theharmful effects of a disaster by attempting to limit itsimpact on human health, community function, and eco-nomic infrastructure. These are all steps that are takento lessen the impact of a disaster should one occur andcan be considered as prevention measures. Preventionrefers to a broad range of activities, such as attemptsto prevent a disaster from occurring, and any actionstaken to prevent further disease, disability, or loss oflife. Mitigation usually requires a significant amount offorethought, planning, and implementation of measuresbefore the incident occurs.
The response phase is the actual implementation ofthe disaster plan. Disaster response, or emergency man-agement, is the organization of activities used to ad-dress the event. Traditionally, the emergency manage-ment field has organized its activities in sectors, such asfire, police, hazardous materials management (hazmat),and emergency medical services. The response phasefocuses primarily on emergency relief: saving lives, pro-viding first aid, minimizing and restoring damaged sys-tems such as communications and transportation, andproviding care and basic life requirements to victims(food, water, and shelter). Disaster response plans aremost successful if they are clear and specific, simple tounderstand, use an incident command system, are rou-tinely practiced, and updated as needed. Response ac-tivities need to be continually evaluated and adjusted tothe changing situation.
Recovery actions focus on stabilizing and return-ing the community (or an organization) to normal (itspreimpact status). This can range from rebuilding dam-aged buildings and repairing infrastructure, to relocatingpopulations and instituting mental health interventions.Rehabilitation and reconstruction involve numerousactivities to counter the long-term effects of the disasteron the community and future development.
Evaluation is the phase of disaster planning and re-sponse that often receives the least attention. After adisaster, it is essential that evaluations be conducted todetermine what worked, what did not work, and whatspecific problems, issues, and challenges were identi-fied. Future disaster planning needs to be based on em-pirical evidence derived from previous disasters.
DISASTER PLANNING
Effective disaster planning addresses the problemsposed by various potential events, ranging in scale frommass casualty incidents, such as motor vehicle collisionswith multiple victims, to extensive flooding or earth-quake damage, to armed conflicts and acts of terrorism

8 Part I Disaster Preparedness
Figure 1.2 Disaster nursing timeline.Copyright Tener Goodwin Veenema, PhD, MPH, MS, CPNP
(Gans, 2001). The disaster-planning continuum is broadin scope and must address collaboration across agen-cies and organizations, advance preparations, as wellas needs assessments, event management, and recoveryefforts. Although public attention frequently focuses onmedical casualties, it is imperative to consider numer-ous other factors when disaster plans and responses arebeing designed and developed. Participation by nursesin all phases of disaster planning is critical to ensurethat nurses are aware of and prepared to deal with what-ever these numerous other factors may turn out to be.Individuals and organizations responsible for disasterplans should consider all possible eventualities—from
the sanitation needs of crowds at mass gatherings, to thepsychosocial needs of vulnerable populations, to evac-uation procedures for buildings and geographic areas—when designing a detailed response (Leonard, 1991; Par-illo, 1995). Completion of the disaster planning processshould result in the production of a comprehensive dis-aster or “emergency operations plan.”
TYPES OF DISASTER PLANNING
The two major types of disaster plans are those thattake the agent-specific approach and those that use the

Chapter 1 Essentials of Disaster Planning 9
all-hazards approach. Communities that embrace theagent-specific approach focus their preparedness activ-ities on the most likely threats to occur based on theirgeographic location (e.g., hurricanes in Florida). Theall-hazards approach is a conceptual model for disas-ter preparedness that incorporates disaster managementcomponents that are consistent across all major typesof disaster events to maximize resources, expenditures,and planning efforts. It has been observed that despitetheir differences many disasters share similarities be-cause certain challenges and similar tasks occur re-peatedly and predictably. The Department of HomelandSecurity’s National Response Plan encourages all com-munities to prepare for disasters using the all-hazardsapproach instead of stand-alone plans, and the agencypublished its guidelines for all-hazards preparedness ti-tled Guide for All-Hazards Emergency Operations Plan-ning (1996). These guidelines are helpful in developingcommunity emergency operations plans.
Problems, issues, and challenges are commonly en-countered across several types of disasters (Auf derHeide, 1996, 2002; Landesman, 2001). Frequently, theseissues and challenges can be effectively addressed incore preparedness activities and include the following:
1. Communication problems.2. Triage, transportation, and evacuation problems.3. Leadership issues.4. The management, security of, and distribution of
resources at the disaster site.5. Advance warning systems and the effectiveness of
warning messages.6. Coordination of search and rescue efforts.7. Media issues.8. Effective triage of patients (prioritization for care
and transport of patients).9. Distribution of patients to hospitals in an equitable
fashion.10. Patient identification and tracking.11. Damage or destruction of the health care infrastruc-
ture.12. Management of volunteers, donations, and other
large numbers of resources.13. Organized improvisational response to the disrup-
tion of major systems.14. Finally, encountering overall resistance (apathy) to
planning efforts. Auf der Heide states, “Interest indisaster preparedness is proportional to the recencyand magnitude of the last disaster” (1989).
CHALLENGES TO DISASTER PLANNING
Adequate planning can address many of these issuesin advance and even eliminate some as problems in the
Figure 1.3 New York, NY, October 5, 2001—The clean-upoperation continues all through the week and weekend, withthousands of tons having been removed already.Photo by Andrea Booher/FEMA News Photo. Source: FEMA, 2001
event of future disaster situations. Challenges to addressproactively are discussed next.
Communication, sharing information among orga-nizations and across many people, is a major priorityin any disaster planning initiative. Failure of the com-munication system may occur in the event of a disas-ter, as a result of damage to the infrastructure causedby the disaster, as well as lack of operator familiarity,excessive demands, inadequate supplies, and lack ofintegration with other communications providers andtechnologies. Backup communications systems, such aswireless, hardwire, and cellular telephones, may reducethe impact of disrupted standard communications, but,frequently, even advanced technology has been ineffec-tual during disasters (Garshnek & Burkle, 1999). Alter-native ways for the public, as well as health providers,to get accurate information is critically important. The9/11 World Trade Center disaster demonstrated the needfor reliable communication systems such as two-way ra-dios and assured backup systems (see Figure 1.3).
A detailed process for the efficient and effective dis-tribution of all types of resources, including supplemen-tal personnel, equipment, and supplies among multi-ple organizations and the establishment of a securityperimeter around a disaster site should also be in-cluded in the plan. Leadership responsibilities and co-ordination of all rescue efforts (across territories andjurisdictions) should be worked out in advance of anyevent.
Advance warning systems and the use of evacua-tion from areas of danger save lives and should be in-cluded in community disaster response plans wheneverappropriate. Warnings can now be made months in ad-vance, in the case of El Nino, to seconds in advanceof the arrival of earthquake waves at some distancefrom the earthquake. Computers are being programmedto respond to warnings automatically, shutting down

10 Part I Disaster Preparedness
Figure 1.4 New Orleans, LA, September 9, 2005—Neighborhoods throughout the area re-main flooded as a result of Hurricane Katrina. Crews work on areas where there have beenbreaks in the levee in order to avoid additional flooding.Photo by Jocelyn Augustino. Source: FEMA, 2005
or appropriately modifying transportation systems, life-lines, and manufacturing processes. Warnings are be-coming much more useful to society as lead time andreliability are improved and as society devises ways torespond effectively. Effective dissemination of warningsprovides a way to reduce disaster losses that have beenincreasing in the United States as people move into at-risk areas (FEMA, 2000).
A plan for the use of the mass media for the purposeof disseminating public health messages in the postim-pact phase in order to avoid health problems (e.g., watersafety, food contamination) should be developed in ad-vance. Nurses and other disaster responders may needtraining in how to interact effectively with the media.(See chapter 5 for further discussion.)
A comprehensive disaster plan will account for theeffective triage of patients (prioritization for care andtransport of patients) and distribution of patients to hos-pitals (a coordinated, even distribution of patients toseveral hospitals as opposed to delivering most of thepatients to the closest hospital). Review of previous dis-aster response efforts reveals that patients are frequently
transferred without adequate triage and that patientdistribution to existing health care facilities is oftengrossly unequal and uncoordinated (Auf der Heide,1996, 2002).
Disaster planning must include a community mu-tual aid plan in the event that the hospital(s), nursinghome(s), or other residential health care facility needs tobe evacuated. Plans for evacuation of health care facili-ties must be realistic and achievable, and contain suffi-cient specific detail as to where patients will be relocatedto and who will be there to care for them. Patient evacu-ation was a major challenge to disaster response effortsfollowing Hurricane Katrina, and was hampered by thedestruction of all major transportation routes in and outof the city. Pre-planning for the possibility of the needto evacuate entire health care facilities must address al-ternative modes of transportation and include adequatesecurity measures (see Figure 1.4).
For large-scale disasters involving a broad geo-graphic region, disaster-medical aid-centers may needto be established and evenly spaced throughout a com-munity. These disaster-medical aid-centers are provided

Chapter 1 Essentials of Disaster Planning 11
Figure 1.5 New Orleans, LA, August 31, 2005—People walkthrough the New Orleans floodwaters to get to higher ground.New Orleans was under a mandatory evacuation order as aresult of flooding caused by Hurricane Katrina.Photo by Marty Bahamonde. Source: FEMA, 2005
in addition to existing emergency medical services andshould be set up no more than an hour’s walk from anylocation involved in the disaster to ensure maximum ac-cessibility (Schultz, Koenig, & Noji, 1996). Casualty col-lection points for both patients and health care providersmay also need to be established in large-scale events(see Figure 1.5). Potential collection points may includegolf courses and shopping malls, or any large expanse ofopen land capable of accommodating both ground andair transport to serve as a staging area (Schultz et al.,1996).
Information systems need to be identified or devel-oped that will track patients across multiple (and per-haps temporary) settings. Patient tracking during disas-ters is a major challenge because of lack of registrationat shelters, and hospital communication systems thatdo not interface with other hospitals or county healthdepartments. Family reunification was a major issuefollowing hurricanes Katrina and Rita, and has per-sisted as a major challenge to meaningful recovery initi-atives.
HAZARD IDENTIFICATION,VULNERABILITY ANALYSIS,AND RISK ASSESSMENT
Hazard identification and mapping, vulnerability analy-sis, and risk assessment are the three cornerstone meth-ods of data collection for disaster planning (see Table1.2). The first step in effective disaster planning requiresadvance identification of potential problems for the in-stitution or community involved (Gans, 2001). Differenttypes of disasters are associated with distinct patternsof illness and injuries, and limited predictions of thesehealth outcomes can sometimes be made in advance,with appropriate and adequate data. Hazards are situ-ations or items that create danger and the potential forthe disaster to occur. Hazard identification and analysisis the method by which planners identify which eventsare most likely to affect a community and serves as thefoundation for decision making for prevention, mitiga-tion, and response. Hazards may include items suchas chemicals used by local industry; transportation ele-ments such as subways, airports, and railroad stations;or collections of large groups of people in areas withlimited access, such as skyscrapers, nursing homes, orsports stadiums (see Table 1.3). Environmental and me-teorological hazards must also be considered, such asthe presence of fault lines and seismic zones and theseasonal risks posed by blizzards, ice storms, tornadoes,hurricanes, wildfires, and heat waves. The National FireProtection Association’s Technical Committee on Disas-ter Management issued international codes and stan-dards that require a community’s hazard identificationto include all natural, technological, and human haz-ards (NFPA, 2004).
Vulnerability is the “state of being vulnerable—open to attack, hurt, or injury” (Merriam Webster’s Col-legiate Dictionary, 2002). The disaster planning teammust identify vulnerable groups of people—those at par-ticular risk of injury, death, or loss of property from eachhazard. Vulnerability analysis can provide predictionsof what individuals or groups of individuals are mostlikely to be affected, what property is most likely to sus-tain damage or be destroyed, and what resources will beavailable to mitigate the effects of the disaster. Vulnera-bility analysis should be conducted for each hazard thatis identified and must be regularly updated to accommo-date population shifts and changes in the environment(Landesman, 2001).
Risk assessment is an essential feature of disasterplanning and is in essence a calculation or model ofrisk, in which a comprehensive inventory is createdincluding all existing and potential dangers, the pop-ulation most likely to be affected by each danger, anda prediction of the health consequences. Risk analysisuses the elements of hazard analysis and vulnerability

12 Part I Disaster Preparedness
1.2 Methods for Data Collection forDisaster Planning
HAZARD IDENTIFICATION AND MAPPINGHazard identification is used to determine which events are mostlikely to affect a community and to make decisions about who orwhat to protect as the basis of establishing measures forprevention, mitigation, and response. Historical data and datafrom other sources are collected to identify previous andpotential hazards. Data are then mapped using aerialphotography, satellite imagery, remote sensing, and geographicinformation systems.
VULNERABILITY ANALYSISVulnerability analysis is used to determine who is most likely tobe affected, the property most likely to be damaged or destroyed,and the capacity of the community to deal with the effects of thedisaster. Data are collected regarding the susceptibility ofindividuals, property, and the environment to potential hazards inorder to develop prevention strategies. A separate vulnerabilityanalysis should be conducted for each identified hazard.
RISK ASSESSMENTRisk assessment uses the results of the hazard identification andvulnerability analysis to determine the probability of a specifiedoutcome from a given hazard that affects a community withknown vulnerabilities and coping mechanisms (risk equalshazard times vulnerability). The probability may be presented asa numerical range (i.e., 30% to 40% probability) or in relativeterms (i.e., low, moderate, or high risk). Major objectives of riskassessment include
■ Determining a community’s risk of adverse health effects dueto a specified disaster (i.e., traumatic deaths and injuries fol-lowing an earthquake)
■ Identifying the major hazards facing the community and theirsources (i.e., earthquakes, floods, industrial accidents)
■ Identifying those sections of the community most likely to beaffected by a particular hazard (i.e., individuals living in or nearflood plains)
■ Determining existing measures and resources that reduce theimpact of a given hazard (i.e., building codes and regulationsfor earthquake mitigation)
■ Determining areas that require strengthening to prevent ormitigate the effects of the hazard
Source: Information obtained from Landesman, L. (2001). Chapter 5: Haz-ard assessment, vulnerability analysis, risk assessment and rapid healthassessment. In Public health management of disasters: The practice guide.Washington, DC: American Public Health Association. The author grate-fully acknowledges Dr. Linda Landesman and the American Public HealthAssociation for permission to reproduce this work.
1.3 Hazard Analysis
Natural EventsDroughtWildfire (e.g., forest, range)AvalancheWinter storms/blizzard: Snow, ice, hailTsunamiWindstorm/typhoon/cycloneHurricane/typhoon/cycloneBiological eventHeat waveExtreme coldFlood or wind-driven waterEarthquakeVolcanic eruptionTornadoLandslide or mudslideDust or sand stormLightning stormTechnological eventsHazardous material releaseExplosion or fireTransportation accident (rail, subway, bridge, airplane)Building or structure collapsePower or utility failureExtreme air pollutionRadiological accident (industry, medical, nuclear power plant)Dam or levee failureFuel or resource shortageIndustrial collapseCommunication disruptionHuman eventsEconomic failuresGeneral strikesTerrorism (e.g., ecological, cyber, nuclear, biological, chemical)Sabotage, bombsHostage situationCivil unrestEnemy attackArsonMass hysteria/panicSpecial events (mass gatherings, concerts, sporting events,
political gatherings)

Chapter 1 Essentials of Disaster Planning 13
analysis to identify groups of people at particular riskof injury or death from each individual hazard. The cal-culation of estimated risk (probability estimate) may beconstant over time, or it may vary by time of day, sea-son, or location relative to the community (Gans, 2001).Risk assessment necessitates the cooperation of corpo-rate, governmental, and community groups to produce acomprehensive listing of all potential hazards (Leonard,1991; Waeckerle, 1991).
The following disaster prevention measures can beimplemented following the analysis of hazards, vulner-ability, and risk:
■ Prevention or removal of hazard (e.g., closing downan aging industrial facility that cannot implementsafety regulations).
■ Removal of at-risk populations from the hazard (e.g.,evacuating populations prior to the impact of a hurri-cane; resettling communities away from flood-proneareas).
■ Provision of public information and education (e.g.,providing information concerning measures that thepublic can take to protect themselves during a tor-nado).
■ Establishment of early warning systems (e.g., usingsatellite data about an approaching hurricane for pub-lic service announcements).
■ Mitigation of vulnerabilities (e.g., sensors for venti-lation systems capable of detecting deviations fromnormal conditions; sensors to check food, water, cur-rency, and mail for contamination).
■ Reduction of risk posed by some hazards (e.g., relo-cating a chemical depot farther away from a schoolto reduce the risk that children would be exposed tohazardous materials; enforcing strict building regula-tions in an earthquake-prone zone).
■ Enhancement of a local community’s capacity to re-spond (e.g., health care coordination across the en-tire health community, including health departments,hospitals, clinics, and home care agencies).
Regardless of the type of approach used by planners(agent-specific or all-hazard), all hazards and potentialdangers should be identified before an effective disasterresponse can be planned.
CAPACITY TO RESPOND
Resource identification is an essential feature of disas-ter planning. A community’s capacity to withstand adisaster is directly related to the type and scope of re-sources available, the presence of adequate communi-cation systems, the structural integrity of its buildingsand utilities (e.g., water, electricity), and the size andsophistication of its health care system (Cuny, 1998;
Gans, 2001). Resources include both human and phys-ical elements, such as organizations with specializedpersonnel and equipment. Disaster preparedness shouldinclude assembling lists of health care facilities; med-ical, nursing, and emergency responder groups; pub-lic works and other civic departments; and volunteeragencies, along with phone numbers and key contactpersonnel for each. Hospitals, clinics, physician offices,mental health facilities, nursing homes, and home careagencies must all have the capacity to ensure continuityof patient care despite damage to utilities, communica-tion systems, or their physical plant. Communicationsystems must be put in place so that hospitals, healthdepartments, and other agencies both locally and re-gionally, can effectively communicate with each otherand share information about patients in the event ofa disaster. Within hospitals, departments should havereadily available a complete record of all personnel,including home addresses and home, pager, and cel-lular phone numbers to ensure access 24 hours a day.Resource availability will vary with factors such as timeof day, season, and reductions in the workforce. Creativ-ity may be needed in identifying and mobilizing humanresources to ensure an adequate workforce (see CaseStudy 1.1). Disaster plans must also include alternativetreatment sites in the event of damage to existing healthcare facilities or in order to expand the surge capacityof the present health care system.
Coordination between agencies is also necessary toavoid chaos if multiple volunteers respond to the disas-ter and are not directed and adequately supervised. Aswith the 9/11 disaster, many national health care work-ers and emergency medical services responders whocame to New York to help returned because the numbersof volunteer responders overwhelmed the local responseeffort.
CORE PREPAREDNESS ACTIVITIES
1) Theoretical foundation for disaster planning. Dis-aster plans are “constructed” in much the same way asone builds a house. Conceptually, they must have a firmfoundation grounded in an understanding of human be-havior. Effective disaster plans are based on empiricalknowledge of how people normally behave in disasters(Landesman, 2001). Any disaster plan must focus firston the local response and best estimates of what peopleare likely to do as opposed to what planners “want peo-ple to do.” Realistic predictions of population behaviorsaccompanied by disaster plans that are flexible in de-sign, and easy to change, will be of greater value to allpersonnel involved in a disaster response.
2) Disaster planning is only as effective as the as-sumptions upon which it is based. The effectiveness ofplanning is enhanced when it is based on information

14 Part I Disaster Preparedness
that has been empirically verified by systematic fielddisaster research studies (Auf der Heide, 2002). Sounddisaster preparedness includes a comprehensive reviewof the existing disaster literature.
3) Core preparedness activities must go beyond theroutine. Most disasters cannot be managed merely bymobilizing more equipment, personnel, and supplies.Disasters differ from routine daily emergencies, and theypose significant problems that have no counterpart inroutine emergency responses. Many disaster-related is-sues and challenges have been identified in the disasterliterature, and they can be anticipated and planned for(Auf der Heide, 2002).
4) Community needs assessment. A communityneeds assessment must be conducted to identify thepreexisting prevalence of disease and to identify thosehigh-risk, high-need patients that may need to be trans-ported in the event of an evacuation or whose needsmay necessitate the provision of care in nontraditionalsites. This needs assessment provides a foundation forplanning along with baseline data for establishing theextent of the impact of the disaster.
5) Identify leadership and command post. The pro-cess of planning is often more important than the finalwritten plan because those individuals who participatein the planning process will be more likely to acceptand abide by the final product. The issue of “who’s incharge” is critical to all components of the disaster re-sponse and must be determined before the event occurs.The process of disaster planning is important to estab-lishing relationships, identifying leaders, and laying thegroundwork for smooth responses. Identification of thecommand post must also be decided in advance andcommunicated to all members of the organization orcommunity (see chapter 6 for further discussion).
6) The first 24–48 hours: design of the local re-sponse. A plan for the mobilization of local authorities,personnel, facilities, equipment, and supplies for the ini-tial postimpact 48-hour period is composed of the nextlevel of the foundation of the disaster response. Mostdisaster casualties will arrive at the hospital within 1hour of impact, and very few trapped casualties are res-cued alive after the first day (Noji, 1996b). Thus, theeffectiveness of the local response is a key determinantin preventing death and disability (Auf der Heide, 2002).Communities must be prepared to handle the immedi-ate postimpact phase in the event that they are alsoisolated from outside resources or supplies (as hap-pened in the immediate aftermath of 9/11 when allplanes were grounded for the first time in U.S. avia-tion history). This stage of the disaster planning willinvolve many organizations and disciplines, from lo-cal institutions to municipal, state, and federal govern-ments, including private, volunteer, and internationalagencies. First, local organizational leaders and execu-tives from each agency must come together and work
as a planning group to conduct the initial assessments(risk, hazard, and vulnerability), establish a coordinatedprocess for response, design effective and complemen-tary communication systems, and create standard cri-teria for the assessment of the scope of damage to thecommunity.
7) Identification and accommodation of vulnerablepopulations. A community disaster plan must accom-modate the needs of all people, including patients re-siding in hospitals and long-term care facilities such asnursing homes, assisted living, psychiatric care facili-ties, and rehabilitation centers. Children in residentialliving centers, individuals detained in the criminal jus-tice system, and prison populations must all be accom-modated within the plan. Poison control and suicidehotlines need to be maintained, and the continuity ofhome health care services must be safeguarded as well(see Case Study 1.2). School districts, day care centers,and employers must be kept aware and up to date re-garding the community’s disaster plan.
8) State and federal assistance. Finally, state andfederal assistance programs are added to the plan, andconsideration of the need for mutual aid agreements (be-tween communities or regions) is begun. Groups andorganizations are most helpful when they understandtheir own capabilities and limitations, as well as thoseof the organizations with which interactions are antic-ipated or intended. Disaster plans should be designedto be both structured and flexible, with provisions madefor plan activation and decision making by first-line em-ergency responders or field-level personnel, if necessary.
9) Identification of training and educational needs,resources, and personal protective equipment (PPE).The disaster plan provides direction for identifying train-ing needs, including mock drills, and acquiring addi-tional resources and PPE. A comprehensive discussionof PPE is found in chapter 26.
10) Plan for the early conduct of damage assess-ment. In emergency medical care, response time iscritical (Schultz et al., 1996). A critical component toany disaster response is the early conduct of a properdamage assessment to identify urgent needs and to de-termine relief priorities for an affected population (Lil-libridge, Noji, & Burkle, 1992). Disaster assessment pro-vides managers with objective information about theeffects of the disaster on a community and can beused to match available resources to the population’sneeds. The early completion of this task and the sub-sequent mobilization of resources to areas of greatestneed can significantly reduce the adverse effects of adisaster. Identification of who will be responsible forthis rapid assessment and what variables the assess-ment will contain needs to be identified in advance aspart of the disaster planning process. Guha-Sapir (1991)developed a template, or tool, from disaster epidemi-ology that includes useful indicators for a rapid needs

Chapter 1 Essentials of Disaster Planning 15
assessment after earthquakes and which can be used toestimate the following factors:
■ Overall magnitude of the effect of the disaster (ge-ographical extent, number of individuals affected,estimated duration).
■ Effect on measurable health outcomes (deaths, ill-nesses, injuries).
■ Integrity of the health care delivery system.■ Specific health care needs of survivors.■ Disruption of services vital to the public’s health
(water, power, sanitation).■ Extent of response to the disaster by local author-
ities.
EVALUATION OF A DISASTER PLAN
An essential step in disaster planning and preparednessis the evaluation of the disaster response plan for its ef-fectiveness and completeness by key personnel involvedin the response. The comprehension of people expectedto execute the plan and their ability to perform dutiesmust be assessed. The availability and functioning ofany equipment called for by the disaster plan need tobe evaluated and reviewed on a systematic basis. Sev-eral methods may be used to exercise the disaster plan,the most comprehensive of which would be its full im-plementation in an actual disaster. Disaster drills mayalso provide an excellent means of testing plans for theircompleteness and effectiveness. Drills can be staged aslarge, full-scale exercises, using moulaged victims andrequiring vast resources of supplies and personnel, orthey may be limited to a small segment of the disas-ter response, such as drills that assess the effectivenessof communications protocols or notification procedures.The disaster plan also may be assessed by using “table-top” academic exercises, mock patients, computer sim-ulations, or seminar sessions focusing on key personnelor limited aspects of the disaster response.
Improved performance during the drill, with en-hanced understanding of disaster planning and re-sponse, is more likely when personnel are notified inadvance that a drill is scheduled. The specific goal ofany drill should be clearly communicated. If drills areto be used as training sessions as well as evaluationsof preparations and response plans, personnel are morelikely to make the correct or most appropriate responsechoices during the drill if they are prepared. Frequentdrills will assure that knowledge and skills are current.Consequently, they will be more likely to take appro-priate actions when faced with an unexpected disastersituation in the future. The more realistic the exercise,the more likely it is that useful information about thestrengths and weaknesses of both the disaster plan andthe responders will be acquired. A shortage of available
resources is a common factor in many disasters; withoutexperiencing at least some of the stress that accompa-nies that situation, it is unlikely that the disaster planand response will be taxed at a level that realisticallysimulates the circumstances of an actual disaster.
Essential features of all effective disaster drills arethe inclusion of all individuals and agencies likely tobe involved in the disaster response and a critique,with debriefing, of all participants following the exer-cise. This should include representation from all sectorsof the emergency management field, all health care dis-ciplines, government officials, school officials, and themedia. The news media has a vital role in disasters, andfailure to include the media in planning activities canlead to a dysfunctional response (Auf der Heide, 2002).Regardless of the format used, the critique should con-sider comments from everyone involved in the drill. Dis-aster planners should review all observations and com-ments and respond with modifications of the disasterplan, if necessary. Any modifications made to disasterplans or response procedures must be communicatedto all groups involved or affected. Periodic evaluationsof disaster plans are essential to ensure that person-nel are adequately familiar with their roles in disastersituations, as well as to accommodate changes in popu-lation demographics, regional emergency response op-erations, hospital renovations and closings, and othervariables. At a minimum, disaster drills should takeplace once every 12 months in the community, and morefrequently in hospitals and other long-term care facili-ties.
SITUATIONS SUGGESTIVE OF ANINCREASED NEED FOR PLANNING
Disasters Within Hospitals
Most hospital plans concern themselves with “exter-nal” events, dealing specifically with the managementof large volumes of patients arriving from an emergencythat has occurred somewhere other than in the hospital(Aghababian et al., 1994). “Internal” disasters refer toincidents that disrupt the everyday, routine services ofthe medical facility and may or may not occur simulta-neously with an external event. Although these concur-rent events are rare, experiences such as the Northridgeearthquake, Hurricane Andrew, and Hurricanes Katrinaand Rita are evidence that they can happen (Aghababianet al., 1994; Quarantelli, 1983; Wolfson & Walker, 1993)with devastating consequences. Before Hurricane Kat-rina’s impact, there were 22 hospitals in New Orleans.Following the rupture of the levy, all 22 hospitals had tobe evacuated. Health care facilities need to define whatconstitutes an internal disaster. In general, an internal

16 Part I Disaster Preparedness
event can be defined as any event that threatens thesmooth functioning of the hospital, medical center orhealth care facility, or that presents a potential danger topatients or hospital personnel (Aghababian et al., 1994).In the United States, the Joint Commission on Accredita-tion of Healthcare Organizations (JCAHO) requires thatall hospitals have comprehensive plans for both inter-nal and external disasters. A copy of the current JCAHOstandards for hospital disaster preparedness and a de-tailed discussion of these guidelines can be found in Ap-pendix XIV. Internal disasters or system support failurescan result in a myriad of responses, such as evacuationof patients and staff; decreased levels of service pro-vision; diversion of ambulances, helicopter transport,and other patients; and relocation of patient care areas.Sources of internal events include power failures, flood,water loss, chemical accidents and fumes, radiation ac-cidents, fire, explosion, violence, bomb threats, lossof telecommunications (inability to communicate withstaff), and elevator emergencies. The hospital setting isfull of flammable and toxic materials. The use of lasersnear flammable gases, multiple sources of radiation,storage of toxic chemicals, and potentially explosivematerials in hospitals and medical centers, magnifiesthe potential for a catastrophic event. Internal disasterplans are based on a “Hospital Incident ManagementSystem” and address the institution’s response to anypotential incident that would disrupt hospital function-ing. Similar to the disaster continuum, the phases of ahospital’s internal disaster response plan generally in-clude the identification of a command post and the fol-lowing three phases:
1) Alert phase, during which staff remain at their regu-lar positions, service provision is uninterrupted, andfaculty and staff await further instructions from theirsupervisors.
2) Response phase, during which designated staff reportto supervisors or the command post for instructions,the response plan is activated, and nonessential ser-vices are suspended.
3) Expanded response phase, when additional person-nel are required, off-duty staff are called in, and ex-isting staff may be reassigned based on patient needs(see chapter 6).
Internal disaster plans must address all potentialscenarios, including
■ loss of power, including auxiliary power;■ loss of medical gases;■ loss of water and/or water pressure;■ loss of compressed air and vacuum (suction);■ loss of telecommunications systems;■ loss of information technology systems;■ threats to the safety of patients and staff (violence,
terrorism, and bombs);
■ toxic exposures involving fumes, chemicals, or radi-ation;
■ immediate evacuation of all patients and personnel.
Internal disaster plans should be integrated with thehospital’s overall disaster preparedness protocol. Train-ing should be mandatory for all personnel. As with otherdisaster plans, drills should be designed and routinelyperformed to ensure that all staff are adequately pre-pared (see chapter 6 for a detailed discussion of themanagement of internal disasters).
Bioterrorism/Communicable Disease
Infectious disease outbreaks create unique challengesto planners. At what point does outbreak managementbecome disaster management? The investigation andmanagement of any communicable disease outbreak re-quires three steps: (a) recognition that a potential out-break is occurring; (b) investigation of the source, modeof transmission, and risk factors for infection; and (c)implementation of appropriate control measures. If out-break management exceeds or threatens to exceed thecapability and resources of the institution, then a disas-ter management model may be useful (Moralejo, Rus-sell, & Porat, 1997).
Institutional outbreaks of communicable diseaseare common. Most institutional outbreaks involve rel-atively few cases with minimum effect on the hospitaland external community. However, large outbreaks, out-breaks of rare diseases, smaller outbreaks in institutionslacking infection control departments, or outbreaks inthose with inadequate infection control personnel mayexceed an institution’s or a community’s coping capac-ities (Moralejo et al., 1997). The need for widespreadquarantine for the purposes of disease control (e.g.,smallpox epidemic) would rapidly overwhelm the ex-isting health care system and create significant staffingissues. Staff may refuse to come to work, fearing expo-sure to themselves and their families. Health care facil-ities play a vital role in the detection and response tobiological emergencies, including new emerging infec-tions, influenza outbreaks, and terrorist use of biologicalweapons. Assessment of the preparedness and capacityof each hospital to respond to and treat victims of aninfectious disease outbreak or biological incident mustbe conducted as part of disaster planning. The Agencyfor Healthcare Research and Quality (AHRQ, 2002) re-leased a survey tool that was widely used by hospitalsand health care facilities to assess their capacity to han-dle potential victims of bioterrorist attacks. In 2006, theAgency for Healthcare Research and Quality issued areport entitled “Altered Standards of Care in Mass Ca-sualty Events” with respect to bioterrorism and otherpublic health emergencies (AHRQ, 2005).

Chapter 1 Essentials of Disaster Planning 17
Hazardous Materials Disaster Planning
Every industrialized nation is heavily reliant on chem-icals. The United States is no exception; it produces,stores, and transports large quantities of toxic industrialagents. In fact, hazardous materials are present in everysector of American society and represent a unique andsignificant threat to civilians, the military, and healthcare workers both in the field and in the hospital emer-gency department. Situations involving hazardous ma-terials suggest a need for additional planning efforts(Levintin & Siegelson, 1996, 2002). The chemical in-dustry and the U.S. government have been making sub-stantial efforts since 9/11 to increase security prepared-ness. Industry is carrying out joint assessments withthe Federal Bureau of Investigation; the EnvironmentalProtection Agency; Coast Guard; FEMA; the Bureau ofAlcohol, Tobacco and Firearms; and the Office of Home-land Security (Institute of Medicine, 2002). In the UnitedStates, the Superfund Amendment and ReauthorizationAct requires that all hazardous materials manufactured,stored, or transported by local industry that could affectthe surrounding community be identified and reportedto health officials. Gasoline and liquid petroleum gasare the most common hazardous materials, but otherpotential hazards include chlorine, ammonia, and ex-plosives. Situations involving relocation of nuclearwaste materials also pose a considerable risk to thecommunities involved. Material safety data sheets stan-dardize the method of communicating relevant informa-tion about each material—including its toxicity, flamma-bility, and known acute and chronic health effects—and can be used as part of the hazard identificationprocess.
Clinically, the removal of solid or liquid chemi-cal agents from exposed individuals is the first stepin preventing serious injury or death. Civilian hazmatteams generally have basic decontamination plans inplace, though proficiency may vary widely (Institute ofMedicine, 1999). Few teams are staffed, trained, andequipped for mass decontamination. Hospitals need tobe prepared to decontaminate patients, despite plansthat call for field decontamination of patients prior totransport. Currently, few hospitals in the United Statesare prepared to manage this type of disaster. During ahazmat accident, the victims often ignore the rules ofthe disaster plan by seeking out the nearest hospital formedical care, regardless of that institution’s capabili-ties. If health care providers rush to the aid of contam-inated individuals without taking proper precautions(e.g., donning PPE), they may become contaminated—the newest victims (Levitin & Siegelson, 1996). Becausemismanagement of a hazmat incident can turn a con-tained accident into a disaster involving the entire com-munity, disaster planning initiatives must incorporate
victim decontamination and PPE into the planning pro-cess (Levitin & Siegelson, 1996, 2002). A detailed dis-cussion of hazmat and patient decontamination is foundin chapter 26.
PROFESSIONAL NURSING MANDATE
Caring for patients and the opportunity to save livesis what professional nursing is all about, and disasterevents provide nurses with an opportunity to do both.According to the American Nurses Association (ANA),“the aim of nursing actions is to assist patients, familiesand communities to improve, correct or adjust to physi-cal, emotional, psychosocial, spiritual, cultural, and en-vironmental conditions for which they seek help” anddefinitions of nursing have evolved to acknowledge sixessential features of professional nursing (ANA, 2003,pp. 1–5):
■ Provision of a caring relationship that facilitateshealth and healing.
■ Attention to the range of human experiences and re-sponses to health and illness within the physical andsocial environments.
■ Integration of objective data with knowledge gainedfrom an appreciation of the patient or group’s subjec-tive experience.
■ Application of scientific knowledge to the processesof diagnosis and treatment through the use of judg-ment and critical thinking.
■ Advancement of professional nursing knowledgethrough scholarly inquiry.
■ Influence on social and public policy to promote so-cial justice.
All nurses should have an awareness of the basiclife cycle of disasters, the health consequences associ-ated with the major events, and a framework to sup-port the necessary assessment and response efforts. Sev-eral nursing organizations have focused on the need forimproved disaster nursing preparation. The ANA, theEmergency Nurses Association (see Case Study 11.1),and the Association for Professionals in Infection Con-trol and Epidemiology have each issued position state-ments regarding the need for nurses to advance theirdisaster knowledge and preparedness skills. In addition,the National Student Nurses Association also recognizedthe need to prepare itself for practice in disaster settings(see Case Study 1.2). Although not all nurses will wantto become “disaster” nurses, it is imperative that eachnurse acquire a knowledge base and minimum set ofskills to enable them to plan for and respond to a disas-ter in a timely and appropriate manner.

18 Part I Disaster Preparedness
S U M M A R Y
Disasters are highly complex events that bring signif-icant destruction and devastation to the communitiesthey strike. A disaster’s immediate effects may be seenin injuries and deaths, disruption of the existing healthcare system and public health infrastructure, and so-cial chaos. Effective planning for disaster preparednessshould be based on the fundamentals of disaster knowl-edge and an understanding of how people behave dur-ing a disaster situation. Disasters often share a commonset of problems and challenges that can be addressedduring the planning process.
S T U D Y Q U E S T I O N S
1) Differentiate between “disaster,” “hazard,” and“complex emergency.” What are the criteria used toclassify the different types of disasters into cate-gories? Explain how these unique features providea structure for strategic planning.
2) What is the disaster continuum, and what are thefive foci of disaster management?
3) Compare and contrast risk assessment, hazard iden-tification, and vulnerability analysis.
4) The Southport County Health Department is holdinga planning meeting with key public health officialsand health care clinicians to address disaster pre-paredness. Southport is a town of 28,000 in north-west Montana and has experienced five blizzardsand one flood in the past 3 years. Using the five fo-cus areas of disaster planning, construct a disasterresponse plan for this community.
5) Why is the disaster planning process so important?6) What are some of the common problems, issues,
and challenges associated with disaster response?How can these problems and issues be addressedduring the preparedness phase?
7) What types of activities should a community pre-pare for during the first 24 hours following impactof a disaster?
8) Following Hurricane Andrew in south Florida, morethan 1,000 physicians’ offices were destroyed orsignificantly damaged. What impact did this haveon the burden of the health care system, andwhat kind of planning could have mitigated thiseffect?
9) Following Hurricane Katrina all of the hospitals lo-cated in New Orleans had to be evacuated. You area nurse working on Louisiana’s Gulf Coast and areconcerned that another hurricane may hit. What areyou doing to prepare? Where would you find re-
sources to help develop a plan for another majorevent?
10) Describe the impact nursing involvement can havein each of the five focus areas of disaster planningand response.
I N T E R N E T A C T I V I T I E S
1) Go to the National Traffic and Road Closure In-formation Web site at http://www.fhwa.dot.gov/trafficinfo/index.htm. In the event of a natural dis-aster involving severe weather conditions, locateupdated information on the status of roads in yourstate and locality. What other Web sites could you goto for current weather-related road conditions duringa disaster? What aspects of a disaster plan would thisinformation change?
2) Go to the FEMA Web site at http://www.fema.gov/pdf/library/fema strat plan fy03–08(no append).pdf. Review FEMA’s Strategic Plan for fiscal years2003–2008 entitled “A Nation Prepared.” Describethe agency’s goals and objectives. What is the all-hazard management system and who is involved?How would you integrate this federal plan into alocal or regional disaster plan?
3) FEMA is organized around four functional divisionsthat correspond to the phases of a disaster. Those areMitigation Division, Preparedness Division, RecoveryDivision, and Response Division. Why isn’t there anEvaluation Division? Do you think that FEMA shouldestablish an Evaluation Division? How quickly couldFEMA accomplish this?
4) Also located within the FEMA Web site is infor-mation regarding essentials of disaster planning forvulnerable populations. Find “Disaster preparednessfor people with disabilities” (http://www.fema.gov/library/disprepf.shtm. Describe the care of the vul-nerable following Hurricanes Katrina and Rita. Drafta proposal for disaster preparedness that includesidentification of high-risk, high-vulnerability individ-uals in your community, mapping of their location,and detailed plans for meeting their needs during adisaster.
5) Visit the U.S. Department of Health and Human Ser-vices, Office of Public Health Emergency Prepared-ness at http://www.hhs.gov/ophep/. What is thepurpose of this agency? Find the National DisasterMedical System (http://www.ndms.dhhs.gov/index.html). Why was this system developed, and what arethe responsibilities of the teams? How do you joina team? How are teams notified of current nationalconditions?

Chapter 1 Essentials of Disaster Planning 19
REFERENCESAgency for Healthcare Research and Quality (AHRQ).
(2002). Bioterrorism emergency planning and preparednessquestionnaire for healthcare facilities. Retrieved from http://www.ahrq.gov/about/cpcr/bioterr.pdf
Agency for Healthcare Research and Quality (AHRQ). (2005). Al-tered standards of care in mass casualty events. Rockville, MD.
Aghababian, R. V., Lewis, C. P., Gans, L., & Curley, F. J. (1994).Disasters within hospitals. Annals of Emergency Medicine, 23,771–777.
Al-Madhari, A. F., & Zeller, A. Z. (1997). Review of disaster defi-nitions. Prehospital Disaster Medicine, 12, 17.
American Nurses Association (ANA). (2003). Nursing’s social pol-icy statement (2nd ed.).
Auf der Heide, E. (1989). Disaster response: Principles of prepara-tion and coordination. St. Louis, MO: Mosby.
Auf der Heide, E. (1996). Disaster planning. Part II: Disaster prob-lems, issues, and challenges identified in the research liter-ature. Emergency Medicine Clinics of North America, 14(2),453–475.
Auf der Heide, E. (2002). Principles of hospital disaster planning.In D. E. Hogan & J. L. Burstein (Eds.), Disaster medicine.Philadelphia: Lippincott Williams & Wilkins.
Berggren, R. (2005). Hurricane Katrina: Unexpected necessities—Inside Charity Hospital. New England Journal of Medicine,353(15), 1550–1553.
Cuny, F. C. (1998). Principles of disaster management. Lesson 2:Program planning. Prehospital Disaster Medicine, 13, 63.
Federal Emergency Management Agency (FEMA). (1996). Guidefor all-hazards emergency operations planning. Retrieved fromhttp://www.fema.gov/pdf/rrr/slg101.pdf
Federal Emergency Management Agency (FEMA). (2000). Effec-tive disaster warnings. Available from http://www.fema.gov
Gans, L. (2001). Disaster planning and management. In A.Harwood-Nuss & A. Wefton (Eds.), The clinical practice ofemergency medicine (3rd ed., pp. 1702–1705). Philadelphia:Lippincott, Williams & Wilkins.
Garshnek, V., & Burkle, F. M. (1999). Telecommunication systemsin support of disaster medicine: Applications of basic informa-tion pathways. Annals of Emergency Medicine, 34, 213.
Gordis, L. (2004). Epidemiology (3rd ed.). Philadelphia: W. B.Saunders.
Guha-Sapir, D. (1991). Rapid needs assessment in mass emergen-cies: Review of current concepts and methods. World HealthStatistics Quarterly, 44, 171–181.
Institute of Medicine. (1999). Chemical and biological terrorism.Washington, DC: National Academy Press.
Institute of Medicine. (2002). Making the nation safer: The role ofscience and technology in countering terrorism. Washington,DC: National Academy Press.
Kim, D., & Proctor, P. (2002). Disaster management and the emer-gency department: A framework for planning. Nursing Clinicsof North America, 37(1), 171–188.
Landesman, L. Y. (2001). Public health management of disasters:The practice guide. Washington, DC: American Public HealthAssociation.
Landesman, L. Y., Malilay, J., Bissell, R. A., Becker, S. M., Roberts,L., & Ascher, M. S. (2001). Roles and responsibilities of publichealth in disaster preparedness and response. In L. F. Novick &J. S. Marr (Eds.), Public health issues in disaster preparedness:Focus on bioterrorism (pp. 1–56). Gaithersburg, MD: Aspen.
Lechat, M. F. (1979). Disasters and public health. Bulletin of theWorld Health Organization, 57(1), 11–17.
Lechat, M. F. (1990). Updates: The epidemiology of health effectsof disasters. Epidemiology Review, 12, 192–197.
Leonard, R. B. (1991). Emergency evacuations in disasters. Pre-hospital Disaster Medicine, 6, 463.
Levitin, H. W., & Siegelson, H. J. (1996). Hazardous materials:Disaster medical planning and response. Emergency MedicineClinics of North America, 14(2), 327–347.
Levitin, H. W., & Siegelson, H. J. (2002). Hazardous materials dis-asters. In D. E. Hagan & J. L. Burstein (Eds.), Disaster medicine(pp. 258–273). Philadelphia: Lippincott, Williams & Wilkins.
Lillibridge, S. A., Noji, E. K., & Burkle, F. M. (1992). Disasterassessment: The emergency health evaluation of a disaster site.Annals of Emergency Medicine, 22, 1715–1720.
Merriam Webster’s Collegiate Dictionary. (2002). Retrieved 3/7/07from http://www.merriamwebster.com/
Moralejo, D. G., Russell, M. L., & Porat, B. L. (1997). Outbreakscan be disasters: A guide to developing your plan. Journal ofNursing Administration, 27(7/8), 56–60.
National Fire Protection Administration (NFPA). (2004). 1600Standard on Disaster/Emergency Management and BusinessContinuity Programs. Quincy, MA.
Noji, E. K. (1996). Disaster epidemiology. Emergency MedicineClinics of North America, 14(2), 289–300.
Noji, E.K. (1997). The nature of disaster: General characteristicsand public health effects. In E. K. Noji (Ed.), The public healthconsequences of disasters. New York: Oxford University Press.
Parillo, S. J. (1995). Medical care at mass gatherings: Considera-tion for physician involvement. Prehospital Disaster Medicine,10, 273.
Quarantelli, E. (1983). Delivery of emergency medical care in dis-asters: Assumptions and realities. New York: Irvington Pub-lishers.
Robert T. Stafford Disaster Relief and Emergency Assistance Act,Pub. L. No. 93–288 (1988).
Sabatino, F. (1992). Hurricane Andrew: South Florida hospitalsshared resources and energy to cope with storm’s devastation.Hospitals, 66(24), 26–30.
Schultz, C. H., Koenig, K. L., & Noji, E. K. (1996). Current con-cepts: A medical disaster response to reduce immediate mor-tality after an earthquake. New England Journal of Medicine,334(7), 438–444.
Waeckerle, J. F. (1991). Disaster planning and response. New Eng-land Journal of Medicine, 324, 815.
Wolfson, J., & Walker, G. (1993). Hospital disaster preparedness:Lessons from Hurricane Andrew. Florida Public Health Infor-mation Center, College of Public Health, University of SouthFlorida, Tampa, FL.
ADDITIONAL READINGSEmergency Management Standards of the Joint Commission on
Accreditation of Health Care Organizations (JCAHO). (2001).Comprehensive accreditation manual for hospitals.
Emergency Management Standards of the Joint Commission onAccreditation of Health Care Organizations (JCAHO). (2002).Revisions to the Comprehensive accreditation manual for hos-pitals.
Joint Commission on Accreditation of Healthcare Organizations.(2005). Standing together: An emergency planning guide forAmerica’s communities. Retrieved 3/7/07 from http://www.jcaho.org/about+us/public+policy+initiatives/planningguide.pdf

20 Part I Disaster Preparedness
CASE STUDY
1.1 FEMA: The Disaster Process and Disaster AidPrograms
Response and Recovery
First response to a disaster is the job of local govern-ment’s emergency services with help from nearby mu-nicipalities, the state, and volunteer agencies. In a catas-trophic disaster, at the request of the governor, federalresources can be mobilized through the U.S. Depart-ment of Homeland Security’s Federal Emergency Man-agement Agency for search and rescue, electrical power,food, water, shelter, and other basic human needs. It isthe long-term recovery phase of disaster that places themost severe financial strain on a local or state govern-ment.
A major disaster could result from a hurricane,earthquake, flood, tornado, or major fire that the presi-dent determines warrants supplemental federal aid. Theevent must be clearly more than state or local gov-ernments can handle alone. If declared, funding comesfrom the president’s Disaster Relief Fund, which is man-aged by FEMA, and disaster aid programs of other par-ticipating federal agencies.
A presidential major disaster declaration puts intomotion long-term federal recovery programs, some ofwhich are matched by state programs, and designed tohelp disaster victims, businesses, and public entities.
An emergency declaration is more limited in scopeand without the long-term federal recovery programs ofa major disaster declaration. In general, federal assis-tance and funding are provided to meet a specific emer-gency need or to help prevent a major disaster fromoccurring.
The Major Disaster Process
A major disaster declaration usually follows these steps:
■ Local government responds, supplemented by neigh-boring communities and volunteer agencies. If over-whelmed, turn to the state for assistance.
■ The state responds with state resources, such as theNational Guard and state agencies.
■ Damage assessment by local, state, federal, and vol-unteer organizations determines losses and recoveryneeds.
■ A major disaster declaration is requested by the gov-ernor, based on the damage assessment, and an
agreement to commit state funds and resources tothe long-term recovery.
■ FEMA evaluates the request and recommends actionto the White House based on the disaster, the localcommunity, and the state’s ability to recover.
■ The president approves the request or FEMA informsthe governor it has been denied. This decision processcould take a few hours or several weeks, dependingon the nature of the disaster.
Disaster Aid Programs
There are three major categories of disaster aid:
Individual Assistance. Immediately after the declaration,disaster workers arrive and set up a central field officeto coordinate the recovery effort. A toll-free telephonenumber is published for use by affected residents andbusiness owners in registering for assistance. DisasterRecovery Centers also are opened where disaster victimscan meet with program representatives and obtain in-formation about available aid and the recovery process.
Disaster aid to individuals generally falls into thefollowing categories:
■ Disaster housing may be available for up to 18months, using local resources, for displaced per-sons whose residences were heavily damaged or des-troyed. Funding also can be provided for housingrepairs and replacement of damaged items to makehomes habitable.
■ Disaster grants are available to help meet other se-rious disaster-related needs and necessary expensesnot covered by insurance and other aid programs.These may include replacement of personal property,transportation, and medical, dental, and funeral ex-penses.
■ Low-interest disaster loans are available after a disas-ter for homeowners and renters from the U.S. SmallBusiness Administration (SBA) to cover uninsuredproperty losses. Loans may be for repair or replace-ment of homes, automobiles, clothing, or other dam-aged personal property. Loans are also available tobusinesses for property loss and economic injury.

Chapter 1 Essentials of Disaster Planning 21
■ Other disaster aid programs include crisis counseling,disaster-related unemployment assistance, legal aid,and assistance with income tax, Social Security, andVeteran’s benefits. Other state or local help may alsobe available.
■ After the application is taken, the damaged prop-erty is inspected to verify the loss. If approved, anapplicant will soon receive a check for rental assis-tance or a grant. Loan applications require more in-formation and approval may take several weeks afterapplication. The deadline for most individual assis-tance programs is 60 days following the president’smajor disaster declaration.
Audits are done later to ensure that aid went to onlythose who were eligible and that disaster aid funds wereused only for their intended purposes. These federalprogram funds cannot duplicate assistance provided byother sources such as insurance.
After a major disaster, FEMA tries to notify all dis-aster victims about the available aid programs and urgethem to apply. The news media are encouraged to visita Disaster Recovery Center, meet with disaster officials,and help publicize the disaster aid programs and thetoll-free teleregistration number.
Public Assistance. Public assistance is aid to state or lo-cal governments to pay part of the costs of rebuilding acommunity’s damaged infrastructure. In general, publicassistance programs pay for 75% of the approved projectcosts. Public assistance may include debris removal,emergency protective measures and public services, re-pair of damaged public property, loans needed by com-munities for essential government functions and grants
Source: FEMA. (2006). Available at: http://www.fema.gov/library/dproc.shtm
for public schools. Learn more about public assistanceat http://www.fema.gov/government/grant/pa/index.shtm.
Hazard Mitigation. Disaster victims and public entitiesare encouraged to avoid the life and property risks offuture disasters. Examples include the elevation or relo-cation of chronically flood-damaged homes away fromflood hazard areas, retrofitting buildings to make themresistant to earthquakes or strong winds, and adoptionand enforcement of adequate codes and standards bylocal, state, and federal government. FEMA helps funddamage mitigation measures when repairing disaster-damaged structures and through the hazard mitigation.
Contact Information for FEMA:
General Questions
[email protected]: 1 (800) 621-FEMA (332)TDD: TTY users can dial 1 (800) 462-7585 to use the
Federal Relay Service.Fax: 1 (800) 827-8112
Technical Assistance (Online Registration)
Telephone: 1 (800) 745-0243Fax: 1 (800) 827-8112Federal Emergency Management AgencyP.O. Box 10055Hyattsville, MD 20782-7055
CASE STUDY
1.2 National Student Nurses Association 2006Resolution for Student Nurses Disaster andEmergency Preparedness
Jennifer Timony
During the 2005–2006 academic year, I had the op-portunity to serve as the Resolutions Chairperson forthe National Student Nurses’ Association (NSNA). TheNSNA is an organization of over 45,000 nursing stu-dents from the United States and its commonwealths
and territories who are enrolled in associate, baccalau-reate, diploma, and generic graduate nursing programs.With its nationwide membership, the NSNA mentorsthe professional development of future nurses and facili-tates their entrance into the profession by providing edu-cational resources, leadership opportunities, and career

22 Part I Disaster Preparedness
guidance. As the chairperson of the Resolutions Com-mittee I guided the legislative process of writing andadopting resolutions that would guide the future actionsof the NSNA. At the midyear convention of the NSNAin Kentucky, I conducted a workshop on the processof writing a resolution and sought out fellow studentsto become the authors of quality materials for potentialresolutions. Students were encouraged to return to theirhome states and begin research on significant topics fornursing students at the national level.
Groups of students in Florida and Texas beganwriting about issues related to emergency and disas-ter preparedness as a response to the great devastationcaused by hurricanes and flooding in their areas. Theywanted to help after the hurricanes but were often metwith obstacles. The frustration created by these obsta-cles led them to want to do more to make changes.They authored resolutions aimed at addressing potentialsolutions for emergency and disaster preparedness fornursing students. The next step was to combine thesesresolutions into one comprehensive resolution to be pre-sented at the NSNA annual convention, which tookplace in Baltimore, Maryland, in April 2006. The Res-olutions Committee facilitated combining the materialso it could be presented before the House of Delegates,the voting body of the NSNA. The following is the res-olution as it was presented.
TOPIC: IN SUPPORT OF THE ESTABLISHMENTOF PROTOCOLS FOR DISASTER RELIEFGUIDING THE SCOPE OF PRACTICEFOR STUDENT NURSES AND THE COL-LECTION AND DISTRIBUTION OF DO-NATIONS
SUBMITTEDBY:
Texas Student Nurses Association andValencia Community College NursingStudent Association
AUTHORS: Blair Baker, Jessica Jones, MillicentJones, Jessica Macleary, Brieann Mellar,Starlit Monzingo, and Daniel Thurow
WHEREAS, student nurses have contributed to disas-ter relief from the time of The Jackson-ville yellow fever epidemic of 1888; and
WHEREAS, the American Red Cross recognizes thecontributions of student nurses in “de-livering critical community services formore than half a century”; and
WHEREAS, the United States has experienced manycrisis events, both natural and man-made, within the past four years; and
WHEREAS, no community is ever fully prepared tohandle a massive disaster with a largeinflux of patients; and
WHEREAS, professional nurses are often restrictedto acute care settings in times of disasterand crisis; and
WHEREAS, student nurses are an available and com-petent resource to assist in disaster reliefefforts; and
WHEREAS, no literature has identified the appropri-ate scope of practice to support studentnurse utilization in the area of disasterrelief; and
WHEREAS, the lack of a defined scope of practicefor student nurses during disaster reliefoperations is a repeated problem needingattention and is likely to reoccur; and
WHEREAS, the National Student Nurses’ Association(NSNA) has for the past 53 years beenthe connecting link and collective bodyof the state student nurses associationspromoting “civic responsibility”; there-fore be it
RESOLVED, that the National Student Nurses’ Asso-ciation (NSNA) support education andawareness of the need for the establish-ment of protocols guiding the scope ofpractice for student nurses in the area ofdisaster relief and the collection and dis-tribution of donations for disaster areas;and be it further
RESOLVED, that the NSNA encourage its constituentsto work collaboratively with their localand state disaster response and health-care agencies to develop a taskforce thatwill define the scope of practice of stu-dent nurses in disaster settings and de-velop a protocol for coordinating the col-lection and distribution of donations tobe sent to disaster areas; and be it fur-ther
RESOLVED, that the NSNA promote student involve-ment in community disaster responseplanning, implementation, and evalua-tion, and the collection and distributionof donations; and be it further
RESOLVED, that the NSNA send a copy of this resolu-tion to the President of the United States,the American Nurses Association, theAmerican Red Cross, the Federal Emer-gency Management Agency, the Ameri-can Association of Colleges of Nursing,the National League for Nursing, the Na-tional Organization for Associate DegreeNursing, state departments of health, theNational Council of State Boards of Nurs-ing, and all others deemed appropriateby the NSNA Board of Directors.

Chapter 1 Essentials of Disaster Planning 23
Discussion at the Resolutions Hearings at the an-nual meeting of the NSNA centered on inspiring fel-low students to be visionaries and agents of change.We were reminded to continue to advocate for our pa-tients by furthering our education, becoming involvedin our communities, and influencing future changes innursing. Fellow students encouraged the NSNA mem-bers to endorse programs that are already in place thatprovide disaster relief, training, education, and certifi-cation. Taking these steps in times of calm will allowus to meet needs when there are emergencies or disas-ters. Leadership by nurses in various community groupswill positively influence the changing image of nursing.Liability concerns were raised regarding nurses and stu-dents who are serving with the best of intentions. Na-tional consistency for scope of practice and licensure
was discussed. This resolution was one of 15 adoptedout of a total of 19 presented before the House of Dele-gates.
The task set before the newly elected board mem-bers of the NSNA is to begin to creatively implementthe 2006 resolutions. The constituent chapters will beguided in constructing programs to implement the re-solved statements and to empower the membership totake personal action as well. We are all part of support-ive communities, and we need to find creative ways togive back.
Source: National Student Nurses Association 2006 Resolutions.Retrieved June 2, 2006, from http://www.nsna.org/pubs/pdf/Resolution%202006.pdf

Key Messages■ The National Disaster Response Framework includes emergency management
authorities, policies, procedures, and resources of local, state, and federal gov-ernments, as well as voluntary disaster relief agencies, the private sector, andinternational resources to provide assistance following a disaster.
■ The Department of Homeland Security coordinates the National Response Plan(NRP) to provide supplemental assistance when the consequences of a disasteroverwhelm local and state capabilities.
■ The NRP coordinates with other federal emergency plans as necessary to meetthe needs of unique situations.
■ The NRP works hand-in-hand with the National Incident Management System andincorporates the tenets of the Incident Command System.
■ Nurses need to be aware of Emergency Support Function (ESF 8), Health andMedical Services, and its core provisions.
■ Nursing leadership during a disaster or mass casualty event demands a broadknowledge base and a unique skill set.
■ Changes in government structure in disaster response and in the public healthsystem may create opportunities for nurses to act in new, yet-to-be defined roles.
■ Nurses must actively seek out positions of leadership in health policy and disastermanagement.
■ Nurses must remain vigilant as this information is constantly changing as healthpolicy and federal restructuring continues.
Learning ObjectivesWhen this chapter is completed, readers will be able to
1. Describe the medical services system.2. Describe the National Response Plan and the National Incident Management Sys-
tem.3. List the 15 emergency support functions included in the plan, particularly the
emergency support function (ESF) 8.4. Discuss the purpose and scope of ESF 8.5. List the federal definitions of a disaster condition.6. Describe federal resources where nurses might volunteer, including the National
Disaster Medical System, Medical Reserve Corps, and U.S. Public Health Serviceand its Federal Medical Shelters.
7. Identify challenges to health systems leadership and coordination.8. Communicate the issues surrounding disaster nursing leadership.