Embed Size (px)
Citation preview

Visit This Book’s Web Page / Buy Now / Request an Exam/ReviewThis is sample from Quick Reference for Otolaryngology
© Springer Publishing Company
QuickRefeRence OtOlaRyngOlOgy
Guide for APRNs, PAs, and Other Health Care Practitioners
Kim ScottConsultants
Richard F. Debo
Alan S. Keyes
David W. Leonard
for
9 780826 196064
ISBN 978-0-8261-9606-4
11 W. 42nd StreetNew York, NY 10036-8002 www.springerpub.com
the only text of its kind for practicing clinicians, Quick Reference for Otolaryngology is a comprehensive, quick-access reference written specifically for nurses, physician’s assistants, and medical students. not only is it useful as a reference guide for clinicians, it is a learning system designed to foster retention and comprehension, and an in-depth review for written boards and ent certification. the book is authored by a nurse practitioner with three prac-ticing otolaryngologists—among the most highly respected professionals in their fields—as consultants.
the guide is consistently organized by anatomical region and contains, for each topic, normal and abnormal findings; easy-to-follow tables, charts, diagrams, photographs, radi-ology images, and algorithms to guide in the workup; differential diagnosis; diagnostic methods; medical therapy; and treatment alternatives. the text includes step-by-step diag-nostic and treatment procedure protocols used in clinical settings and current staging criteria for common cancer diagnoses. another important feature is the guide’s overview of surgical management for specific conditions. topics are covered on a “need to-know” basis for written boards and certification review. this reference will be a valuable companion for clinicians in general practice and those entering the ent field, and for use as a diagnosis guide for referral.
Key Features:
• Provides key differential diagnosis guidelines• includes 15 “how-to” procedure protocols used in clinical settings, and current staging
criteria for eight of the more common cancer diagnoses • Presents overviews of surgical management for specific conditions• Serves as a concise reference guide and review for written boards and ent certification• Seven videos illustrating actual procedures, including nasal endoscopy, flexible laryn-
goscopy, and others, accompany the book
Quick RefeRence for OtOlaRyngOlOgyGuide for APRNs, PAs, and Other Health Care Practitioners
Kim Scott, fnP, MSn, ae-c, cORlnWith text consultants, Richard f. Debo, MD, facS, alan S. keyes, MD, facS, and David W. leonard, MD, facS Q
uic
k R
efeRen
ce
for OtO
laRy
ng
OlO
gy
Scott
Quick Reference for OTOLARYNGOLOGY
Guide for APRNs, PAs, andOther Health Care Practitioners
Scott_96064_PTR_00_i-x_03-11-14.indd iScott_96064_PTR_00_i-x_03-11-14.indd i 3/24/2014 9:06:13 PM3/24/2014 9:06:13 PMHetzelCampbell_19360_PTR_00_pi-xxviii.indd viHetzelCampbell_19360_PTR_00_pi-xxviii.indd vi 10/4/2017 5:52:12 PM10/4/2017 5:52:12 PM
This is a sample from QUICK REFERENCE FOR OTOLARYNGOLOGY: GUIDE FOR APRNS, PAS, AND
VISIT THIS BOOK’S WEB PAGE BUY NOW REQUEST AN EXAM OR REVIEW COPY
© Springer Publishing Company
OTHER HEALTH CARE PRACTITIONERS

ABOUT THE CONSULTANTS
Richard F. Debo, MD, FACS, earned his medical degree from the Uniformed Services University of the Health Sciences, Bethesda, Maryland, in 1984. He completed his intern-ship and residency in Otolaryngology/Head and Neck Surgery at Walter Reed Army Medical Center in 1989. He has also received subspecialty training in Head and Neck Surgical Oncology at the University of Virginia in 1993. His military career included ser-vice as the Chief of Otolaryngology at Ft. Campbell, Kentucky, during which time he was deployed for the fi rst Persian Gulf War as the chief of Otolaryngology/Head and Neck Surgery with the 86th Evacuation Hospital. He completed his military career as an attend-ing in Otolaryngology and Head and Neck Oncology at Madigan Army Medical Center, teaching residents and providing care for patients with head and neck cancer and thyroid problems. Dr. Debo’s academic appointments have included clinical instructor of surgery at the Uniformed Services University of the Health Sciences, clinical assistant professor at the University of Washington Department of Otolaryngology/Head and Neck Sur-gery, and as assistant professor of Clinical Otolaryngology-Head and Neck Surgery at the Eastern Virginia Medical School Department of Otolaryngology. He is also adjunct clinical faculty at Old Dominion University in Norfolk, Virginia. Dr. Debo is also a board-certifi ed fellow of the American Academy of Otolaryngology/Head and Neck Surgery and he is a fellow of the American College of Surgeons. He is a fellow of the American Academy of Otolaryngic Allergy. His interests also include allergic rhinitis, and general and pediatric otolaryngology.
Alan S. Keyes, MD, FACS, is board certifi ed in otolaryngology and an associate of the American Academy of Otolaryngic Allergy. Dr. Keyes received his undergraduate educa-tion at the University of Washington and his medical degree at the Medical College of Virginia. He served in the Navy for 10 years as an otolaryngologist including the role of Department Head at the Naval Hospital in Charleston, South Carolina. Dr. Keyes is cur-rently an assistant professor of otolaryngology at the Eastern Virginia Medical School.
David W. Leonard, MD, FACS, earned his medical degree from the Uniformed Services University of the Health Sciences (USUHS) in Bethesda, Maryland, after receiving his bachelor’s degree in chemistry from the New College of Sarasota, Florida. He continued his training as a surgical intern and completed his residency in Otolaryngology Head and Neck Surgery at the National Naval Medical Center (NNMC), Bethesda, Maryland, in 1996. He remained as an attending physician, teaching residents in otolaryngology from 1996 to 2002 and treating many high-ranking members of the executive and legislative branches of government. During his tour at NNMC, he held numerous positions, includ-ing Assistant Residency Director, and Assistant Professor of Surgery (USUHS). Intimately involved with research, he authored 10 journal articles. He was concurrently assigned to the USNS Comfort hospital ship as the sole Otolaryngologist from April 1998 to Febru-ary 2002 and also completed the Navy War College’s Command and Staff Program. Dr. Leonard also served at the Naval Hospital Jacksonville, Florida, as the Otolaryngology Department Head, chairman of the Credentials Subcommittee, vice-chairman Executive Committee of the Medical Staff, and director Surgical Services. He retired as a U.S. Navy Captain with over 26 years of service, and joined Eastern Virginia Ear, Nose, and Throat Specialists in 2010. Dr. Leonard is board certifi ed by the American Board of Otolaryngol-ogy, is a Fellow of the American Academy of Otolaryngology/Head and Neck Surgery, Fellow of the American College of Surgeons, and is a member of the American Academy of Otolaryngic Allergy.
Scott_96064_PTR_00_i-x_03-11-14.indd iiScott_96064_PTR_00_i-x_03-11-14.indd ii 3/24/2014 9:06:13 PM3/24/2014 9:06:13 PMHetzelCampbell_19360_PTR_00_pi-xxviii.indd viHetzelCampbell_19360_PTR_00_pi-xxviii.indd vi 10/4/2017 5:52:12 PM10/4/2017 5:52:12 PM
This is a sample from QUICK REFERENCE FOR OTOLARYNGOLOGY: GUIDE FOR APRNS, PAS, AND
VISIT THIS BOOK’S WEB PAGE BUY NOW REQUEST AN EXAM OR REVIEW COPY
© Springer Publishing Company
OTHER HEALTH CARE PRACTITIONERS

ABOUT THE AUTHOR
Kim Scott, FNP, AE-C, CORLN, is a family nurse practitioner, board certifi ed as an asthma educator and an otorhinolaryngology nurse. Kim has experience working as a registered nurse in the Cardiovascular Intensive Care Unit and General Intensive Care Unit at Norfolk General Hospital in Beaufort, South Carolina, before becoming a nurse practitioner. She received her Bachelor’s of Nursing degree at Virginia Com-monwealth University, Medical College of Virginia, 2001. She received her master’s degree as a family nurse practitioner at the Medical University of South Carolina, in 2004. Kim specialized in allergy, asthma, and sinus disease, working for Baz Allergy, Asthma & Sinus Center in Fresno, California, before joining Eastern Virginia Ear, Nose & Throat Specialists in October 2008. She is a member of the American Acad-emy of Otolaryngology, the American Academy of Otolaryngic Allergy, and the American Academy of Allergy, Asthma & Immunology. She is also adjunct clinical faculty at Old Dominion University in Norfolk, Virginia.
Scott_96064_PTR_00_i-x_03-11-14.indd iiiScott_96064_PTR_00_i-x_03-11-14.indd iii 3/24/2014 9:06:13 PM3/24/2014 9:06:13 PMHetzelCampbell_19360_PTR_00_pi-xxviii.indd viHetzelCampbell_19360_PTR_00_pi-xxviii.indd vi 10/4/2017 5:52:12 PM10/4/2017 5:52:12 PM
This is a sample from QUICK REFERENCE FOR OTOLARYNGOLOGY: GUIDE FOR APRNS, PAS, AND
VISIT THIS BOOK’S WEB PAGE BUY NOW REQUEST AN EXAM OR REVIEW COPY
© Springer Publishing Company
OTHER HEALTH CARE PRACTITIONERS

Scott_96064_PTR_00_i-x_03-11-14.indd ivScott_96064_PTR_00_i-x_03-11-14.indd iv 3/24/2014 9:06:13 PM3/24/2014 9:06:13 PMHetzelCampbell_19360_PTR_00_pi-xxviii.indd viHetzelCampbell_19360_PTR_00_pi-xxviii.indd vi 10/4/2017 5:52:12 PM10/4/2017 5:52:12 PM
This is a sample from QUICK REFERENCE FOR OTOLARYNGOLOGY: GUIDE FOR APRNS, PAS, AND
VISIT THIS BOOK’S WEB PAGE BUY NOW REQUEST AN EXAM OR REVIEW COPY
© Springer Publishing Company
OTHER HEALTH CARE PRACTITIONERS

Quick Reference for OTOLARYNGOLOGY
Kim Scott, FNP, MSN, AE-C, CORLN
CONSULTANTS
Richard F. Debo, MD, FACS
Alan S. Keyes, MD, FACS
David W. Leonard, MD, FACS
Guide for APRNs, PAs, andOther Health Care Practitioners
Scott_96064_PTR_00_i-x_03-11-14.indd vScott_96064_PTR_00_i-x_03-11-14.indd v 3/24/2014 9:06:13 PM3/24/2014 9:06:13 PMHetzelCampbell_19360_PTR_00_pi-xxviii.indd viHetzelCampbell_19360_PTR_00_pi-xxviii.indd vi 10/4/2017 5:52:12 PM10/4/2017 5:52:12 PM
This is a sample from QUICK REFERENCE FOR OTOLARYNGOLOGY: GUIDE FOR APRNS, PAS, AND
VISIT THIS BOOK’S WEB PAGE BUY NOW REQUEST AN EXAM OR REVIEW COPY
© Springer Publishing Company
OTHER HEALTH CARE PRACTITIONERS

Copyright © 2014 Springer Publishing Company, LLC
All rights reserved.
No part of this publication may be reproduced, stored in a retrieval system, or transmitted in any form or by any means, electronic, mechanical, photocopying, recording, or otherwise, without the prior permission of Springer Pub-lishing Company, LLC, or authorization through payment of the appropriate fees to the Copyright Clearance Center, Inc., 222 Rosewood Drive, Danvers, MA 01923, 978-750-8400, fax 978-646-8600, [email protected] or on the Web at www.copyright.com.
Springer Publishing Company, LLC11 West 42nd StreetNew York, NY10036www.springerpub.com
Acquisitions Editor: Margaret ZuccariniComposition: Newgen Imaging
ISBN: 978-0-8261-9606-4e-book ISBN: 978-0-8261-9607-1
Videos can be found at www.springerpub.com/scott-otolaryngology-videosAn Image Bank can be found at www.springerpub.com/scott-otolaryngology-image-bank
14 15 16 17/ 5 4 3 2 1
The author and the publisher of this Work have made every effort to use sources believed to be reliable to provide information that is accurate and compatible with the standards generally accepted at the time of publication. Because medical science is continually advancing, our knowledge base continues to expand. Therefore, as new information becomes available, changes in procedures become necessary. We recommend that the reader always consult current research and specifi c institutional policies before performing any clinical procedure. The author and publisher shall not be liable for any special, consequential, or exemplary damages resulting, in whole or in part, from the readers’ use of, or reliance on, the information contained in this book. The publisher has no responsibility for the persistence or accuracy of URLs for external or third-party Internet websites referred to in this publication and does not guarantee that any content on such websites is, or will remain, accurate or appropriate.
CIP data is available from the Library of Congress.
Special discounts on bulk quantities of our books are available to corporations, professional associations, pharma-ceutical companies, health care organizations, and other qualifying groups. If you are interested in a custom book, including chapters from more than one of our titles, we can provide that service as well.
For details, please contact:Special Sales Department, Springer Publishing Company, LLC11 West 42nd Street, 15thFloor, New York, NY 10036–8002Phone: 877-687-7476 or 212-431-4370; Fax: 212-941-7842E-mail: [email protected]
Printed in the United States of America by Bradford & Bigelow.
Scott_96064_PTR_00_i-x_03-11-14.indd viScott_96064_PTR_00_i-x_03-11-14.indd vi 3/24/2014 9:06:13 PM3/24/2014 9:06:13 PMHetzelCampbell_19360_PTR_00_pi-xxviii.indd viHetzelCampbell_19360_PTR_00_pi-xxviii.indd vi 10/4/2017 5:52:12 PM10/4/2017 5:52:12 PM
This is a sample from QUICK REFERENCE FOR OTOLARYNGOLOGY: GUIDE FOR APRNS, PAS, AND
VISIT THIS BOOK’S WEB PAGE BUY NOW REQUEST AN EXAM OR REVIEW COPY
© Springer Publishing Company
OTHER HEALTH CARE PRACTITIONERS

Preface ix
1. Physical Examination Documentation of Normal and Abnormal Findings From the Ear, Nose, and Throat Examination 1
Procedure Protocol: Pneumatic Otoscopy 5 Procedure Protocol: Rinne and Weber Tuning Fork Tests 7 Procedure Protocol: Nasal Endoscopy 11 Procedure Protocol: Evaluating the Nasopharynx With Indirect
Mirror Examination 12
Video 1.1: Nasal endoscopy
Video 1.2: Flexible fi beroptic laryngoscopy
Procedure Protocol: Flexible Fiberoptic Laryngoscopy 22 Procedure Protocol: Evaluating the Larynx With Indirect
Mirror Examination 23
2. Ear, Nose, and Throat Anatomy and Physiology Normal Findings 33
3. Physical Examination of the Cranial Nerves for the Head and Neck 61
4. Evaluation and Management of Facial Nerve Conditions 89
5. Evaluation and Management of Hearing and Tinnitus 101
6. Evaluation and Management of External Ear Conditions 129 Procedure Protocol: Ear Cleaning 134 Procedure Protocol: Otowick Insertion 134
7. Evaluation and Management of Middle Ear Conditions 149 Procedure Protocol: Myringotomy With and Without Tympanostomy
or Pressure Equalizer Tube Insertion 160 Procedure Protocol: Paper Patch Myringoplasty 166
8. Evaluation and Management of Inner Ear Conditions 179 Procedure Protocol: Epley Maneuver 190
9. Evaluation and Management of Olfactory Disorders 201
10. Evaluation and Management of the Nose—External Conditions 209
Contents
Scott_96064_PTR_00_i-x_03-11-14.indd viiScott_96064_PTR_00_i-x_03-11-14.indd vii 3/24/2014 9:06:13 PM3/24/2014 9:06:13 PMHetzelCampbell_19360_PTR_00_pi-xxviii.indd viHetzelCampbell_19360_PTR_00_pi-xxviii.indd vi 10/4/2017 5:52:12 PM10/4/2017 5:52:12 PM
This is a sample from QUICK REFERENCE FOR OTOLARYNGOLOGY: GUIDE FOR APRNS, PAS, AND
VISIT THIS BOOK’S WEB PAGE BUY NOW REQUEST AN EXAM OR REVIEW COPY
© Springer Publishing Company
OTHER HEALTH CARE PRACTITIONERS
Share Quick Reference for Otolaryngology

11. Evaluation and Management of the Nasal Cavity and Paranasal Sinuses 215 Procedure Protocol: Silver Nitrate Cauterization for Epistaxis 229 Procedure Protocol: Nasal Packing for Epistaxis 230 Staging Criteria: How to Read and/or Determine Cancer Staging 242 Staging Criteria: TNM Staging System for the Nasal Cavity and
Paranasal Sinuses 243
12. Evaluation and Management of Nasopharynx Conditions 249 Staging Criteria: TNM Staging System for the Nasopharynx 253
13. Evaluation and Management of Oropharynx Disorders 255 Procedure Protocol: Needle Drainage and Incision and Drainage
of a Peritonsillar Abscess 272 Procedure Protocol: Lingual Frenulectomy 280 Staging Criteria: TNM Staging Criteria: Lip and Oral Cavity Cancer 284 Staging Criteria: TNM Staging Criteria: Oropharyngeal
and Hypopharyngeal Cancer 285
14. Evaluation and Management of Sleep Apnea 291
15. Evaluation and Management of Salivary Gland Conditions 301 Staging Criteria: TNM Staging Criteria for Salivary Gland
Cancerous Tumors 315
16. Evaluation and Management of Benign Neck Conditions 323
17. Overview of Malignant Neck Conditions 345
18. Evaluation and Management of Thyroid Disorders 355 Staging Criteria: TNM Staging Criteria for Thyroid Cancer 368
19. Evaluation and Management of Parathyroid Disorders 373
20. Evaluation and Management of Trachea Disorders and Conditions 383
21. Evaluation and Management of Esophageal Disorders 401
22. Evaluation and Management of Larynx and Hypopharynx Disorders 413
Video 22.1: Stroboscopy: False vocal cord use
Video 22.2: Left vocal cord paralysis patient 1
Video 22.3: Left vocal cord paralysis patient 2
Video 22.4: Stroboscopy: Normal vocal cord function
Video 22.5: Stroboscopy: Bilateral ball-valving vocal cord polyps
Staging Criteria: TNM Staging Criteria for Larynx 433
23. Overview of Lesions of the Skin: Head and Neck 437 Procedure Protocol: Biopsy of Skin Lesion 439 Staging Criteria: TNM Staging Criteria for Mucosal Melanoma of the
Head and Neck 442
24. Evaluation and Management of Allergic and Nonallergic Disorders 445
25. Overview of Commonly Ordered Tests in ENT 473
Index 479
Scott_96064_PTR_00_i-x_03-11-14.indd viiiScott_96064_PTR_00_i-x_03-11-14.indd viii 3/24/2014 9:06:14 PM3/24/2014 9:06:14 PMHetzelCampbell_19360_PTR_00_pi-xxviii.indd viHetzelCampbell_19360_PTR_00_pi-xxviii.indd vi 10/4/2017 5:52:12 PM10/4/2017 5:52:12 PM
This is a sample from QUICK REFERENCE FOR OTOLARYNGOLOGY: GUIDE FOR APRNS, PAS, AND
VISIT THIS BOOK’S WEB PAGE BUY NOW REQUEST AN EXAM OR REVIEW COPY
© Springer Publishing Company
OTHER HEALTH CARE PRACTITIONERS

Health care providers encounter patients with ear, nose, and throat disorders on a daily basis. These are some of the main reasons why patients seek medical attention. Quick Refer-ence for Otolaryngology: Guide for APRNs, PAs, and Other Health Care Practitioners is a compre-hensive, easy-to-read guide formatted for quick reference on any ENT topic. It showcases the pertinent need-to-know information for how to treat and manage most ENTdisorders. This guide is written from an advanced practice perspective, supported by the collabora-tion of three practicing otolaryngology physicians. Together, we have simplifi ed each ENT topic, presenting what is necessary for the practicing health care professional to know.
While there are many textbooks written on ENT disorders, many are rather lengthy or too basic to meet the needs of the primary care provider. Quick Reference for Otolaryngol-ogy eliminates the confusion and simplifi es each ENT topic by incorporating easy-to-follow tables, charts, diagrams, artwork, diagnostic explanations, therapy/treatments, and pro-cedure protocols. The quick review format enables easy access to needed information and provides a useful aid for written boards and certifi cation review.
Specifi c need-to-know information for each topic is bolded so that it stands out and can’t be missed. Each topic addresses the latest guidelines and incorporates suggested medications and treatment protocols. Additionally, the book provides important guidance for differential diagnosis, when the primary care provider should refer for specialty care, and an invaluable overview of surgical management for specifi c conditions. Commonly ordered tests in ENT are included as the last chapter in the book.
Some additional unique offerings include:
Procedure Protocols used in clinical settings ■
Staging Criteria for the more common cancer diagnoses ■
Videos that capture: ■
Nasal endoscopy ■
Flexible fi beroptic laryngoscopy ■
Left vocal cord paralysis (two patient examples) ■
Stroboscopy: Normal vocal cord function ■
Stroboscopy: Bilateral ball-valving vocal cord polyps ■
As a family nurse practitioner myself, I felt the need for a quick guide on ENT disorders and believed there was certain pertinent information that an advanced practice provider needed to know to be successful in treating patients on a daily basis. This book will be use-ful on many levels by a wide variety of health care professionals. Its depth and scope of clinical content and guidelines provides that much-needed clinical reference for successful primary care practice.
Kim Scott
Preface
Videos can be found at www.springerpub.com/scott-otolaryngology-videosAn Image Bank can be found at www.springerpub.com/scott-otolaryngology-image-bank
Scott_96064_PTR_00_i-x_03-11-14.indd ixScott_96064_PTR_00_i-x_03-11-14.indd ix 3/24/2014 9:06:14 PM3/24/2014 9:06:14 PMHetzelCampbell_19360_PTR_00_pi-xxviii.indd viHetzelCampbell_19360_PTR_00_pi-xxviii.indd vi 10/4/2017 5:52:12 PM10/4/2017 5:52:12 PM
This is a sample from QUICK REFERENCE FOR OTOLARYNGOLOGY: GUIDE FOR APRNS, PAS, AND
VISIT THIS BOOK’S WEB PAGE BUY NOW REQUEST AN EXAM OR REVIEW COPY
© Springer Publishing Company
OTHER HEALTH CARE PRACTITIONERS

Scott_96064_PTR_00_i-x_03-11-14.indd xScott_96064_PTR_00_i-x_03-11-14.indd x 3/24/2014 9:06:15 PM3/24/2014 9:06:15 PMHetzelCampbell_19360_PTR_00_pi-xxviii.indd viHetzelCampbell_19360_PTR_00_pi-xxviii.indd vi 10/4/2017 5:52:12 PM10/4/2017 5:52:12 PM
This is a sample from QUICK REFERENCE FOR OTOLARYNGOLOGY: GUIDE FOR APRNS, PAS, AND
VISIT THIS BOOK’S WEB PAGE BUY NOW REQUEST AN EXAM OR REVIEW COPY
© Springer Publishing Company
OTHER HEALTH CARE PRACTITIONERS

HetzelCampbell_19360_PTR_00_pi-xxviii.indd viHetzelCampbell_19360_PTR_00_pi-xxviii.indd vi 10/4/2017 5:52:12 PM10/4/2017 5:52:12 PM
ShareQuick Reference for Otolaryngology
HetzelCampbell_19360_PTR_00_pi-xxviii.indd viHetzelCampbell_19360_PTR_00_pi-xxviii.indd vi 10/4/2017 5:52:12 PM10/4/2017 5:52:12 PM
This is a sample from QUICK REFERENCE FOR OTOLARYNGOLOGY: GUIDE FOR APRNS, PAS, AND
VISIT THIS BOOK’S WEB PAGE BUY NOW REQUEST AN EXAM OR REVIEW COPY
© Springer Publishing Company
OTHER HEALTH CARE PRACTITIONERS
INSTRUMENTS NEEDED TO CONDUCT A THOROUGH EAR, NOSE, AND THROAT (ENT) EXAMINATION
Head mirror or headlight ■
Nasal speculum ■
Tongue depressor ■
Endoscope (rigid and fl exible to be used for nasal endoscopy and direct laryngoscopy) ■
Indirect nasopharyngeal/laryngeal mirror ■
ENT microscope ■
Otoscope with bulb pneumatic attachment ■
Tuning fork 512 Hz ■
Stethoscope ■
THE EAR
Proper technique of the otoscopic examination: Retract the auricle up and back while inserting the speculum. This straightens the external auditory canal (EAC) and pro-vides best visualization of the tympanic membrane (TM).
Normal Ear Exam
Document:
The auricle and external auditory canal (EAC) are nontender and without evidence ■
of discharge, scaling, erythema, foreign body, cerumen, or lesions. The TM is gray and translucent with normal light refl ex. NOTE: Lack of a light refl ex is not a diag-nostic fi nding. A light refl ex can be present in a severely diseased ear, while it may be absent or abnormal in a normal ear.
Figure 1.1: Normal tympanic membrane.
1Physical ExaminationDocumentation of Normal and Abnormal Findings From the Ear, Nose, and Throat Examination
Scott_96064_PTR_01_1-32_03-11-14.indd 1Scott_96064_PTR_01_1-32_03-11-14.indd 1 3/24/2014 9:08:36 PM3/24/2014 9:08:36 PMHetzelCampbell_19360_PTR_00_pi-xxviii.indd viHetzelCampbell_19360_PTR_00_pi-xxviii.indd vi 10/4/2017 5:52:12 PM10/4/2017 5:52:12 PM
This is a sample from QUICK REFERENCE FOR OTOLARYNGOLOGY: GUIDE FOR APRNS, PAS, AND
VISIT THIS BOOK’S WEB PAGE BUY NOW REQUEST AN EXAM OR REVIEW COPY
© Springer Publishing Company
OTHER HEALTH CARE PRACTITIONERS

Pinna
The function of the pinna is to collect sound by acting as a funnel and amplifying the sound directly to the auditory canal.
Figure 1.2: Pinna.
FIGURE 1.1 Normal tympanic membrane.
FIGURE 1.2 Pinna.
HelixScaphoid
fossaCrura ofantihelix
Triangularfossa
Crus of helix
Tragus
Externalauditory meatus
Intertragicnotch
Antitragus
Lobule
Auriculartubercle
Cymba ofconcha
Concha ofauricle
Cavum ofconcha
Antihelix
Helix
Scott_96064_PTR_01_1-32_03-11-14.indd 2Scott_96064_PTR_01_1-32_03-11-14.indd 2 3/24/2014 9:08:37 PM3/24/2014 9:08:37 PMHetzelCampbell_19360_PTR_00_pi-xxviii.indd viHetzelCampbell_19360_PTR_00_pi-xxviii.indd vi 10/4/2017 5:52:12 PM10/4/2017 5:52:12 PM
This is a sample from QUICK REFERENCE FOR OTOLARYNGOLOGY: GUIDE FOR APRNS, PAS, AND
VISIT THIS BOOK’S WEB PAGE BUY NOW REQUEST AN EXAM OR REVIEW COPY
© Springer Publishing Company
OTHER HEALTH CARE PRACTITIONERS

Possible Abnormal FindingsDocument the presence of any of the following abnormal fi ndings:
Edema ■
Erythema of auricle ■
Erythema of lobule ■
Swelling overlying mastoid region ■
Herpetic eruption ■
Lesion(s) ■
Hematoma ■
Tenderness—localized ■
Congenital malformations: ■ Darwin’s tubercle; lop ear deformity; dysplastic; elfi n ear (pointed); low-set ears; ear cleft; preauricular pit; macrotia; microtia; anotia; acces-sory auricles
Conchal Bowl
The conchal bowl, or concha, describes the cartilage that is situated near the ear canal and looks like a bowl. Just like the pinna, it helps to funnel sounds into the canal.
Possible Abnormal FindingsDocument the presence of any of the following abnormal fi ndings:
Crusting ■
Scaling ■
Weeping ■
Erythema ■
Scabbing ■
External Auditory Canal
The EAC (also called external acoustic or auditory meatus) allows effi cient sound transmission to occur from the environment to the TM. The EAC also allows for ade-quate protection from direct injury to the TM related to the depth of the canal and its shape.
Possible Abnormal FindingsDocument the presence of any of the following abnormal fi ndings:
Bloody discharge ■ Cerumen impaction ■
EAC obstructed ■
Otorrhea ■
Cerebrospinal fl uid (CSF) otorrhea ■
Debris ■
Edema ■
Erythema ■
Exostoses ■
Fissure ■
Foreign body ■
Hairy ■
Infl ammed ■
Figure 1.3: External, middle, and inner ear.
Scott_96064_PTR_01_1-32_03-11-14.indd 3Scott_96064_PTR_01_1-32_03-11-14.indd 3 3/24/2014 9:08:38 PM3/24/2014 9:08:38 PMHetzelCampbell_19360_PTR_00_pi-xxviii.indd viHetzelCampbell_19360_PTR_00_pi-xxviii.indd vi 10/4/2017 5:52:12 PM10/4/2017 5:52:12 PM
This is a sample from QUICK REFERENCE FOR OTOLARYNGOLOGY: GUIDE FOR APRNS, PAS, AND
VISIT THIS BOOK’S WEB PAGE BUY NOW REQUEST AN EXAM OR REVIEW COPY
© Springer Publishing Company
OTHER HEALTH CARE PRACTITIONERS

Macerated ■
Mass/lesion ■
Mastoid bowl clean ■
Mastoid bowl debris ■
Mastoid bowl granulation tissue ■
Meatoplasty open ■
Osteoma ■
Packing in place ■
Purulent discharge ■
Scabbed ■
Scaling ■
Stenotic ■
Swollen ■
Tenderness ■
Well healed/healing ■
Congenital malformations: ■ Atresia; septation; duplication
Middle Ear
The middle ear contains three ossicles, which transfer sound vibrations of the TM into waves in the fl uid and membranes within the cochlea of the inner ear. The space behind the TM is called the tympanic cavity and directly off this cavity is the eustachian tube, which connects to the nasopharynx. The eustachian tube is responsible for equalizing pressure in the tympanic cavity.
Figure 1.4: Tympanic membrane.
FIGURE 1.3 External, middle, and inner ear.
Auricle(pinna)
External ear Middle ear Inner ear
(not to scale)
Malleus Incus
Auditory ossicles
Stapes
Temporalbone
Externalauditorymeatus
Tympanicmembrane
Semicircularcanals
Oval window
Facial nerve
Acousticnerve (VIII)
Vestibularnerve
Cochlearnerve
Vestibule
Round window
Eustachian tube
Scott_96064_PTR_01_1-32_03-11-14.indd 4Scott_96064_PTR_01_1-32_03-11-14.indd 4 3/24/2014 9:08:38 PM3/24/2014 9:08:38 PMHetzelCampbell_19360_PTR_00_pi-xxviii.indd viHetzelCampbell_19360_PTR_00_pi-xxviii.indd vi 10/4/2017 5:52:12 PM10/4/2017 5:52:12 PM
This is a sample from QUICK REFERENCE FOR OTOLARYNGOLOGY: GUIDE FOR APRNS, PAS, AND
VISIT THIS BOOK’S WEB PAGE BUY NOW REQUEST AN EXAM OR REVIEW COPY
© Springer Publishing Company
OTHER HEALTH CARE PRACTITIONERS

Possible Abnormal FindingsDocument the presence of any of the following abnormal fi ndings:
Drainage noted from behind the TM ■
Effusion noted ■
Fluid fi lling middle ear space ■
Glomus tumor present ■
Ossicles partially visible ■
Purulent effusion ■
Congenital malformations ■
Ossicular deformity■
FIGURE 1.4 Tympanic membrane.
Pars flaccida
Incus
Pars tensa
Umbo
Cone of light
Handle of malleus
Short process
of malleus
PROCEDURE PROTOCOL: PNEUMATIC OTOSCOPY
Purpose: To evaluate the mobility of the tympanic membrane (TM).
Proper technique: Using a bulb pneumatic attachment to the otoscope, the specu-lum of the otoscope must form a tight seal in the ear canal. Gently “puff” the bulb, which causes both negative and positive pressure to the TM.
Positive Pressure Negative Pressure
Causes the TM to retract inward. ■
If the middle ear is under positive ■
pressure (e.g., from ear infection) the TM will move when positive pressure is applied but not when negative pressure is applied.
Causes the TM to bulge outward. ■
If the middle ear is under negative ■
pressure, the TM will not move when positive pressure is applied; when negative pressure is applied, the TM will bulge outward.
Scott_96064_PTR_01_1-32_03-11-14.indd 5Scott_96064_PTR_01_1-32_03-11-14.indd 5 3/24/2014 9:08:39 PM3/24/2014 9:08:39 PMHetzelCampbell_19360_PTR_00_pi-xxviii.indd viHetzelCampbell_19360_PTR_00_pi-xxviii.indd vi 10/4/2017 5:52:12 PM10/4/2017 5:52:12 PM
This is a sample from QUICK REFERENCE FOR OTOLARYNGOLOGY: GUIDE FOR APRNS, PAS, AND
VISIT THIS BOOK’S WEB PAGE BUY NOW REQUEST AN EXAM OR REVIEW COPY
© Springer Publishing Company
OTHER HEALTH CARE PRACTITIONERS

Tympanic Membrane
The TM separates the external ear canal from the middle ear. Its function is to transmit sound from the air to the ossicles inside the middle ear. The two areas of the TM are the pars fl accida and pars tensa. The pars fl accida is most commonly where cholesteatomas can be found. The pars tensa forms most of the TM and this is the area in which perfora-tions most commonly occur. The pars tensa consists of three layers: skin, fi brous tissue, and mucosa.
Possible Abnormal FindingsDocument the presence of any of the following abnormal fi ndings:
Atelectatic ■
Bulging ■
Crusting ■
Decreased movement ■
Dull ■
Fluid behind eardrum—bloody ■
Fluid behind eardrum—clear yellow ■
Fluid behind eardrum—clear, watery ■
Fluid behind eardrum—cloudy yellow ■
Fluid behind eardrum—mucoid ■
Cholesteatoma ■
Infl amed ■
Incudostapedial (IS) joint pexy ■
Mobile with pneumotoscopy ■
Mobile with Valsalva ■
Pressure equalization (PE) tube in place and patent ■
PE tube in place but obstructed ■
PE tube has extruded ■
Perforation—centrally ■
Perforation—marginally ■
Polyp ■
Retracted ■
Retraction pocket ■
Scarring ■
Thickening ■
Figure 1.5: Central tympanic membrane perforation.
FIGURE 1.5 Central tympanic membrane perforation.
Scott_96064_PTR_01_1-32_03-11-14.indd 6Scott_96064_PTR_01_1-32_03-11-14.indd 6 3/24/2014 9:08:39 PM3/24/2014 9:08:39 PMHetzelCampbell_19360_PTR_00_pi-xxviii.indd viHetzelCampbell_19360_PTR_00_pi-xxviii.indd vi 10/4/2017 5:52:12 PM10/4/2017 5:52:12 PM
This is a sample from QUICK REFERENCE FOR OTOLARYNGOLOGY: GUIDE FOR APRNS, PAS, AND
VISIT THIS BOOK’S WEB PAGE BUY NOW REQUEST AN EXAM OR REVIEW COPY
© Springer Publishing Company
OTHER HEALTH CARE PRACTITIONERS

FIGURE 1.6 Tympanosclerosis.
(continued)
Tympanosclerosis ■
Visible air bubbles ■
Visible meniscus ■
Figure 1.6: Tympano-sclerosis.
PROCEDURE PROTOCOL: RINNE AND WEBER TUNING FORK TESTS
Introduction
The tuning fork tests the cochleovestibular nerve (CN VIII). The Rinne and Weber tuning fork tests help to distinguish between conductive hearing loss (CHL) and sensorineural hearing loss (SNHL) by measuring air and bone conduction. Both tests use the 512 Hz fork.
Air conduction (AC) is measured by hearing sound via the ear canal and middle ear. By evaluating AC, you are evaluating whether or not CHL exists.
Bone conduction (BC) is measured by hearing sound transmission to the inner ear via the mastoid process. By evaluating BC, you are evaluating whether or not SNHL exists. NOTE: Do the Weber test fi rst then confi rm your fi ndings with the Rinne test.
Weber Test Rinne Test
Purpose: Detects existence of a difference in function between the two ears.
TEST:1. Strike the tuning fork against
your patella or elbow.2. Place the tuning fork on the
patient’s forehead, in the midline.
3. Ask: “Where is the sound heard best? Right ear, left ear, or both ears?”
Purpose: Confi rms CHL if suspected when Weber test was done.
TEST:1. Strike the tuning fork against your
patella or elbow.2. Place the tuning fork on the
mastoid process. Once the patient hears the sound, move the fork in front of the patient’s ear canal.
3. Ask the patient, “Which sound was louder? On the bone or next to your ear?”
Scott_96064_PTR_01_1-32_03-11-14.indd 7Scott_96064_PTR_01_1-32_03-11-14.indd 7 3/24/2014 9:08:41 PM3/24/2014 9:08:41 PMHetzelCampbell_19360_PTR_00_pi-xxviii.indd viHetzelCampbell_19360_PTR_00_pi-xxviii.indd vi 10/4/2017 5:52:12 PM10/4/2017 5:52:12 PM
This is a sample from QUICK REFERENCE FOR OTOLARYNGOLOGY: GUIDE FOR APRNS, PAS, AND
VISIT THIS BOOK’S WEB PAGE BUY NOW REQUEST AN EXAM OR REVIEW COPY
© Springer Publishing Company
OTHER HEALTH CARE PRACTITIONERS

THE NOSE
FIGURE 1.7 External nose.
Frontal bone
Nasal bones
Upper lateralnasal cartilages
Septal cartilage anddorsum of the nose
Tip
Lower lateralnasal cartilages
Greater alar cartilage
Medial crus
Septal cartilage
Columalla
Alla
Alargroove
Lateral crus
PROCEDURE PROTOCOL: RINNE AND WEBER TUNING FORK TESTS (continued)
Weber Test Rinne Test
INTERPRETATION:Normal test:
Sound is equal in both the ears.Document: Weber is intact without
lateralization.
If the sound is louder in one ear:This could mean CHL in that ear or SNHL in the opposite ear.
If the sound is quieter in one ear:This could mean SNHL in that ear or CHL in the opposite ear.
Document if abnormal:Weber lateralized to (right/left) ear.
INTERPRETATION:Normal test (or a positive Rinne test):
Sound is heard louder when the tuning fork is in front of the ear canal.
This doesn’t rule out the possibility that SNHL could exist in that ear.
Document: AC > BC.
CHL is confi rmed if:The sound is heard louder when the tuning fork was on the bone.
Document if abnormal:BC > AC or AC > BC.
Scott_96064_PTR_01_1-32_03-11-14.indd 8Scott_96064_PTR_01_1-32_03-11-14.indd 8 3/24/2014 9:08:42 PM3/24/2014 9:08:42 PMHetzelCampbell_19360_PTR_00_pi-xxviii.indd viHetzelCampbell_19360_PTR_00_pi-xxviii.indd vi 10/4/2017 5:52:12 PM10/4/2017 5:52:12 PM
This is a sample from QUICK REFERENCE FOR OTOLARYNGOLOGY: GUIDE FOR APRNS, PAS, AND
VISIT THIS BOOK’S WEB PAGE BUY NOW REQUEST AN EXAM OR REVIEW COPY
© Springer Publishing Company
OTHER HEALTH CARE PRACTITIONERS

Proper technique when examining the nose: Using a headlight, inspect the nose for evidence of previous trauma such as scars or deformities. Examine the skin for lesions. Look at the nares and columella for symmetry. Insert a nasal speculum into the nasal cavity. Lift the ala and gently open the speculum vertically. NOTE: Try to avoid touching the patient’s nasal septum with the speculum as this may cause some pain or discomfort. Also, remove the speculum from the nose while it is in an open position; if it is closed when you remove it, you may pull out nasal hair.
Examine the septum for deviation, spur projection, or perforation. Inspect the infe-rior and middle turbinates mucosa for color, discharge, swelling, or lesions. Note any pol-yps present within the vestibule or adjacent to the middle turbinate (middle meatus).
Normal Nose Examination
Document:
■ No discharge. Septum is midline. Inferior and middle turbinates are normal. NOTE: 80% or more of patients will have a deviated septum. This does not necessarily indicate an abnormal fi nding.
Nose External: Possible Abnormal Findings
Document the presence of any of the following abnormal fi ndings:
Asymmetry ■
Asymmetric columella ■
Asymmetric cartilage ■
Bulbous ■
Deformed ■
Deviation of bone structure ■
Dorsal hump ■
Lesion ■
Narrow ■
Saddle deformity ■
Scarring of skin ■
Swelling ■
Wide ■
Congenital malformations that can be seen on physical examination: ■
Arhinia (absent external nasal structures and nasal passages) ■
Nasal cleft ■
Congenital malformations that cannot be seen on physical examination: ■
Choanal atresia (the back of the nasal passage [choana] is blocked by either bone ■
or soft tissue formed during fetal development)Nasal encephalocele ■
Glioma ■
Nasal dermoid ■
Teratoma ■
Nose Internal
Document evidence of any nasal obstruction by percentage (i.e., 20%, 50%, 80%, etc.).
Nares: Possible Abnormal FindingsDocument the presence of any of the following abnormal fi ndings:
Asymmetry ■
Foreign body or material ■
Figure 1.7: External nose.
Scott_96064_PTR_01_1-32_03-11-14.indd 9Scott_96064_PTR_01_1-32_03-11-14.indd 9 3/24/2014 9:08:43 PM3/24/2014 9:08:43 PMHetzelCampbell_19360_PTR_00_pi-xxviii.indd viHetzelCampbell_19360_PTR_00_pi-xxviii.indd vi 10/4/2017 5:52:12 PM10/4/2017 5:52:12 PM
This is a sample from QUICK REFERENCE FOR OTOLARYNGOLOGY: GUIDE FOR APRNS, PAS, AND
VISIT THIS BOOK’S WEB PAGE BUY NOW REQUEST AN EXAM OR REVIEW COPY
© Springer Publishing Company
OTHER HEALTH CARE PRACTITIONERS

Protrusion of septal cartilage into nares ■
Crusting ■
Discharge—watery ■
Discharge—bloody ■
Discharge—purulent ■
Deviation of caudal portion of septum ■
Tobacco-stained vibrasseae ■
Nasal Mucosa: Possible Abnormal FindingsDocument the presence of any of the following abnormal fi ndings:
Bleeding ■
Boggy ■
Congested ■
Crusting ■
Discharge—watery ■
Discharge—bloody ■
Discharge—purulent ■
Dry ■
Erythema ■
Polyps ■
Telangiectasia ■
Ulcerated ■
Bony and/or Cartilaginous Septum: Possible Abnormal FindingsDocument the presence of any of the following abnormal fi ndings:
Bleeding ■
Crusting ■
Deviation to the right or left ■
Dry ■
Impinging on inferior turbinate ■
Impinging on middle turbinate ■
Midline ■
Perforation noted ■
Scarring present ■
Spur present ■
Tortuous ■
Ulcerated ■
Turbinates—Inferior and/or Middle: Possible Abnormal FindingsDocument the presence of any of the following abnormal fi ndings:
Atrophied ■
Bluish ■
Boggy ■
Congested ■
Edema ■
Enlarged ■
Erythema ■
Hypertrophy ■
Infl amed ■
Lesion present ■
Scott_96064_PTR_01_1-32_03-11-14.indd 10Scott_96064_PTR_01_1-32_03-11-14.indd 10 3/24/2014 9:08:43 PM3/24/2014 9:08:43 PMHetzelCampbell_19360_PTR_00_pi-xxviii.indd viHetzelCampbell_19360_PTR_00_pi-xxviii.indd vi 10/4/2017 5:52:12 PM10/4/2017 5:52:12 PM
This is a sample from QUICK REFERENCE FOR OTOLARYNGOLOGY: GUIDE FOR APRNS, PAS, AND
VISIT THIS BOOK’S WEB PAGE BUY NOW REQUEST AN EXAM OR REVIEW COPY
© Springer Publishing Company
OTHER HEALTH CARE PRACTITIONERS

Pale pink ■
Cyanotic ■
Surgically reduced ■
PROCEDURE PROTOCOL: NASAL ENDOSCOPY
Introduction
Nasal endoscopy involves evaluating the nasal and sinus passages (if previous history of sinus surgery) with direction visualization using a fl exible fi beroptic endoscope or a rigid endoscope.
Indications
Mucopurulent drainage ■
Nasal congestion ■
Hyposmia ■
Anosmia ■
Sinusitis ■
To obtain culture of nasal secretions ■
Septal deformity ■
Nasal obstruction or foreign body ■
To evaluate for nasal masses or polyps ■
To evaluate the nasopharynx ■
Eustachian tube dysfunction ■
Facial pain or pressure ■
Epistaxis ■
Epiphora ■
Postoperative evaluation and debridement and removal of crusting after func- ■
tional endoscopic sinus surgery
Contraindications
No absolute contraindications exist. However, the examination should be per-formed carefully so as to not provoke bleeding, especially in patients on antico-agulants or with a bleeding disorder.
Equipment Needed
Endoscope ■
Spray containing topical anesthetic and vasoconstrictor; for example, Afrin ■
and lidocaine
Procedure Protocol
Seat the patient comfortably in an examination chair. Instruct the patient to ■
move the hips to the back of the chair, straighten the back, lean forward, and tilt the chin up as if “sniffi ng fl owers.”Position yourself in front or to the side of the patient. ■
Video 1.1: Nasal endoscopy.
(continued)
Scott_96064_PTR_01_1-32_03-11-14.indd 11Scott_96064_PTR_01_1-32_03-11-14.indd 11 3/24/2014 9:08:43 PM3/24/2014 9:08:43 PMHetzelCampbell_19360_PTR_00_pi-xxviii.indd viHetzelCampbell_19360_PTR_00_pi-xxviii.indd vi 10/4/2017 5:52:12 PM10/4/2017 5:52:12 PM
This is a sample from QUICK REFERENCE FOR OTOLARYNGOLOGY: GUIDE FOR APRNS, PAS, AND
VISIT THIS BOOK’S WEB PAGE BUY NOW REQUEST AN EXAM OR REVIEW COPY
© Springer Publishing Company
OTHER HEALTH CARE PRACTITIONERS

PROCEDURE PROTOCOL: NASAL ENDOSCOPY (continued)
Using the mixture that contains a topical anesthetic and vasoconstrictor, direct ■
the spray posteriorly—parallel to the fl oor of the nose and not toward the ceiling. Wait several minutes after spraying to permit decongestant and anes-thetic to take effect. NOTE: Tell the patient that the solution may taste bitter and may produce a numbing sensation in the nose, mouth, and throat. The patient may feel like he or she cannot swallow or talk, but remind the patient that these functions are not affected with this medication.Introduce the scope gently into one nostril (usually the nostril that appears ■
more open than the other) and pass it along the fl oor of the nose. Try to avoid the nasal septum. If you are unable to advance along the fl oor of the nose because of a septal deviation or large inferior turbinate, try advancing the scope above the inferior turbinate or attempt entrance into the nasal cavity on the opposite side of the nose.During the examination, evaluate the nasal septum, inferior turbinate, inferior ■
meatus, nasopharynx, and eustachian tubes.Advance the scope along the middle meatus to examine the middle turbinate. ■
If possible, gently roll medial to the middle turbinate to examine the spheno-ethmoidal recess.If the patient previously had sinus surgery, evaluate the sinus cavities. ■
At the conclusion of the procedure, gently wash the endoscope with run- ■
ning water and place it in an enzymatic cleanser. Then rinse the scope of any cleanser and hang it up to dry before use on the next patient.
Potential Complications
Pain, bleeding, fainting (vasovagal response), and adverse drug reaction.
PROCEDURE PROTOCOL: EVALUATING THE NASOPHARYNX WITH INDIRECT MIRROR EXAMINATION
Introduction
Indirect mirror examination allows for more complete inspection of the nasophar-ynx without using a fi beroptic or rigid endoscopy. Various anatomical structures can be viewed with indirect mirror examination including the posterior soft pal-ate, posterior palatine tonsils, eustachian tube orifi ces, torus tubarius, fossa of Rosenmuller, and adenoids.
Indications
A patient who cannot tolerate the fl exible or rigid nasal endoscopy examination ■
A patient who is allergic to topical anesthetics or decongestants used for the ■
fl exible or rigid nasal endoscopy examinationTo evaluate for nasopharyngeal abnormalities including adenoid hypertro- ■
phy
(continued)
Scott_96064_PTR_01_1-32_03-11-14.indd 12Scott_96064_PTR_01_1-32_03-11-14.indd 12 3/24/2014 9:08:43 PM3/24/2014 9:08:43 PMHetzelCampbell_19360_PTR_00_pi-xxviii.indd viHetzelCampbell_19360_PTR_00_pi-xxviii.indd vi 10/4/2017 5:52:12 PM10/4/2017 5:52:12 PM
This is a sample from QUICK REFERENCE FOR OTOLARYNGOLOGY: GUIDE FOR APRNS, PAS, AND
VISIT THIS BOOK’S WEB PAGE BUY NOW REQUEST AN EXAM OR REVIEW COPY
© Springer Publishing Company
OTHER HEALTH CARE PRACTITIONERS

EXAM FINDINGS OF THE NOSE WITH ENDOSCOPIC OR MIRROR NASOPHARYNGEAL EXAMINATION
Normal Exam Findings of the Nose With Endoscopic or Mirror Nasopharyngeal Examination
Document:
Examination of the nasopharynx reveals normal mucosa, adenoids, posterior choa- ■
nae, and eustachian tubes.
Adenoid: Possible Abnormal FindingsDocument the presence of any of the following abnormal fi ndings:
Asymmetric ■
Enlarged ■
Nasopharyngeal lesion ■
Obstructing ■
Purulent ■
Surgically absent ■
Contraindications
No absolute contraindications exist.
Equipment Needed
Tongue blade ■
Indirect nasopharyngeal/laryngeal mirror ■
Headlamp ■
4 × 4 gauze ■
Procedure Protocol
Seat the patient comfortably in an examination chair. ■
Instruct the patient to move the hips to the back of the chair, straighten the ■
back, and lean forward with mouth open and tongue extended.Position yourself in front or to the side of the patient. Have your headlight on ■
throughout this procedure.If gagging is expected with the patient, a topical anesthetic can be applied ■
(e.g., Hurricaine spray).Using one hand, depress the tongue with a tongue blade. Or you can hold ■
the patient’s tongue or ask the patient to hold the tongue with a 4 × 4 gauze. Ask the patient to relax and breathe through the nose and mouth. This relaxes the soft palate. With your other hand, insert a small mirror into the mouth, along the surface of the tongue blade. Come to rest between the soft palate and the pharyngeal wall. Try to avoid touching the tongue, phar-ynx, or palate with the mirror as this may stimulate a gag refl ex. Rotate the mirror from side to side to view the posterior soft palate, tonsils, and nasopharynx.
Scott_96064_PTR_01_1-32_03-11-14.indd 13Scott_96064_PTR_01_1-32_03-11-14.indd 13 3/24/2014 9:08:44 PM3/24/2014 9:08:44 PMHetzelCampbell_19360_PTR_00_pi-xxviii.indd viHetzelCampbell_19360_PTR_00_pi-xxviii.indd vi 10/4/2017 5:52:12 PM10/4/2017 5:52:12 PM
This is a sample from QUICK REFERENCE FOR OTOLARYNGOLOGY: GUIDE FOR APRNS, PAS, AND
VISIT THIS BOOK’S WEB PAGE BUY NOW REQUEST AN EXAM OR REVIEW COPY
© Springer Publishing Company
OTHER HEALTH CARE PRACTITIONERS

Choana: Possible Abnormal FindingsDocument the presence of any of the following abnormal fi ndings:
Atretic ■
Lesion or mass present ■
Stenotic ■
Eustachian Tubes: Possible Abnormal FindingsDocument the presence of any of the following abnormal fi ndings:
Edema ■
Lesion or mass ■
Obstructed ■
Mucosa: Possible Abnormal FindingsDocument the presence of any of the following abnormal fi ndings:
Atrophic ■
Bleeding ■
Crusting ■
Edema ■
Erythema ■
Foreign body ■
Lesion or mass ■
Purulent ■
Ulcerated ■
Mueller Maneuver (Flexible Fiberoptic Laryngoscopy Examination Only)
Introduction: The Mueller maneuver is a technique on examination to evaluate for velopharyngeal and/or hypopharyngeal narrowing in a patient with suspected obstruc-tive sleep apnea. This is when the soft palate and the lateral or posterior pharyngeal walls fail to separate the oral cavity from the nasal cavity during the Mueller maneuver.
Proper technique: Place the fl exible fi beroptic scope in the hypopharynx where you can see the entire hypopharynx and larynx. Pinch the patient’s nostrils closed and ask the patient to close the lips and attempt to inhale. The test is positive if the hypophar-ynx collapses during the maneuver. Estimate percentage of collapse and document.
Normal FindingsDocument:
No retropalatine collapse ■
Abnormal FindingsDocument:
Retropalatine collapse (___%) ■
The Paranasal Sinuses
Normal Exam Findings of the Paranasal SinusesDocument:
Normal surgical appearance ■
No drainage, crusting, lesions, or polyps ■
Ostia are open ■
Figure 1.8: Paranasal sinuses.
Scott_96064_PTR_01_1-32_03-11-14.indd 14Scott_96064_PTR_01_1-32_03-11-14.indd 14 3/24/2014 9:08:44 PM3/24/2014 9:08:44 PMHetzelCampbell_19360_PTR_00_pi-xxviii.indd viHetzelCampbell_19360_PTR_00_pi-xxviii.indd vi 10/4/2017 5:52:12 PM10/4/2017 5:52:12 PM
This is a sample from QUICK REFERENCE FOR OTOLARYNGOLOGY: GUIDE FOR APRNS, PAS, AND
VISIT THIS BOOK’S WEB PAGE BUY NOW REQUEST AN EXAM OR REVIEW COPY
© Springer Publishing Company
OTHER HEALTH CARE PRACTITIONERS
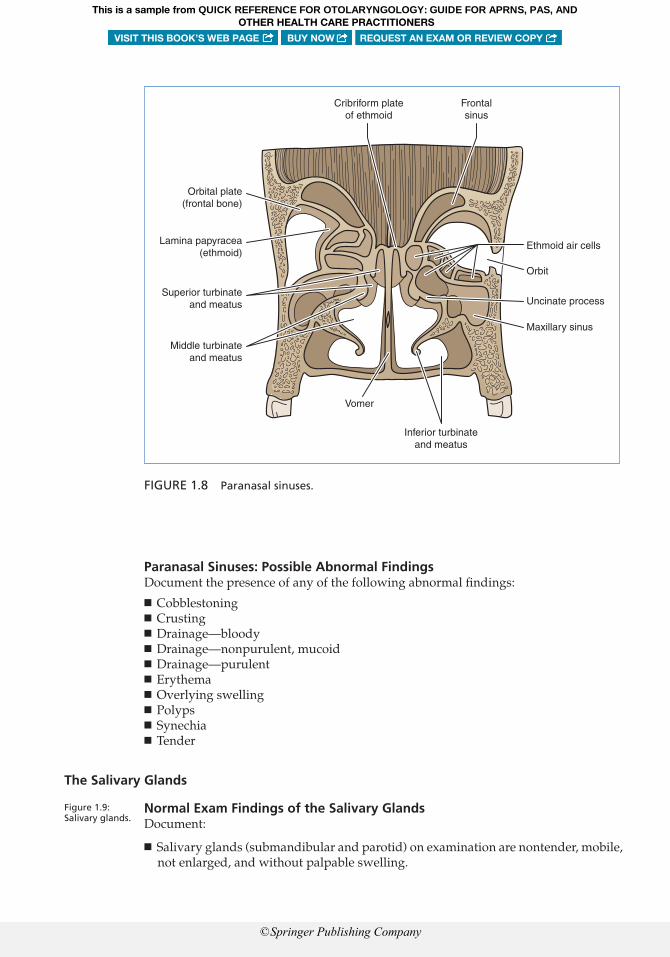
Paranasal Sinuses: Possible Abnormal FindingsDocument the presence of any of the following abnormal fi ndings:
Cobblestoning ■
Crusting ■
Drainage—bloody ■
Drainage—nonpurulent, mucoid ■
Drainage—purulent ■
Erythema ■
Overlying swelling ■
Polyps ■
Synechia ■
Tender ■
The Salivary Glands
Normal Exam Findings of the Salivary GlandsDocument:
Salivary glands (submandibular and parotid) on examination are nontender, mobile, ■
not enlarged, and without palpable swelling.
Figure 1.9: Salivary glands.
FIGURE 1.8 Paranasal sinuses.
Cribriform plateof ethmoid
Frontalsinus
Ethmoid air cells
Orbit
Uncinate process
Maxillary sinus
Inferior turbinateand meatus
Vomer
Middle turbinateand meatus
Superior turbinateand meatus
Lamina papyracea(ethmoid)
Orbital plate(frontal bone)
Scott_96064_PTR_01_1-32_03-11-14.indd 15Scott_96064_PTR_01_1-32_03-11-14.indd 15 3/24/2014 9:08:44 PM3/24/2014 9:08:44 PMHetzelCampbell_19360_PTR_00_pi-xxviii.indd viHetzelCampbell_19360_PTR_00_pi-xxviii.indd vi 10/4/2017 5:52:12 PM10/4/2017 5:52:12 PM
This is a sample from QUICK REFERENCE FOR OTOLARYNGOLOGY: GUIDE FOR APRNS, PAS, AND
VISIT THIS BOOK’S WEB PAGE BUY NOW REQUEST AN EXAM OR REVIEW COPY
© Springer Publishing Company
OTHER HEALTH CARE PRACTITIONERS

Salivary Glands: Possible Abnormal FindingsDocument the presence of any of the following abnormal fi ndings:
Abnormal consistency ■
Asymmetric ■
Enlarged ■
Lesion or mass ■
Mobile ■
Swollen ■
Tender ■
The Oral Cavity and Oropharynx
Normal Exam Findings of the Oral Cavity and OropharynxDocument:
Lips are moist. ■
Teeth are present and in good condition. ■
The tongue has no lesions. ■
The gums and mucosa have no swelling, bleeding, or infection. ■
The pharynx and tonsillar fossa are normal. ■
The openings of Stensen’s and Wharton’s ducts are identifi ed and nonobstructed. ■
Figure 1.10: Oral cavity and oropharynx.
FIGURE 1.9 Salivary glands.
Parotidsalivary gland
Stensen’sduct
Masseter muscle
Sublingual ducts
Sublingualsalivary gland
Submandibular salivary gland
Wharton’s duct
Scott_96064_PTR_01_1-32_03-11-14.indd 16Scott_96064_PTR_01_1-32_03-11-14.indd 16 3/24/2014 9:08:44 PM3/24/2014 9:08:44 PMHetzelCampbell_19360_PTR_00_pi-xxviii.indd viHetzelCampbell_19360_PTR_00_pi-xxviii.indd vi 10/4/2017 5:52:12 PM10/4/2017 5:52:12 PM
This is a sample from QUICK REFERENCE FOR OTOLARYNGOLOGY: GUIDE FOR APRNS, PAS, AND
VISIT THIS BOOK’S WEB PAGE BUY NOW REQUEST AN EXAM OR REVIEW COPY
© Springer Publishing Company
OTHER HEALTH CARE PRACTITIONERS

Lips: Possible Abnormal FindingsDocument the presence of any of the following abnormal fi ndings:
Cracked ■
Cyanotic ■
Dry ■
Erythema ■
Excoriated creases at commissure ■
Fissured ■
Hemangioma ■
Lesion(s) ■
Pigmented ■
Vesicular eruption ■
Oral Cavity/Oropharynx: Possible Abnormal FindingsDocument the presence of any of the following abnormal fi ndings:
Teeth: ■
Caries ■
Dentures upper ■
Dentures lower ■
Discolored ■
FIGURE 1.10 Oral cavity and oropharynx.
Superior lip
Superior labialfrenulum
Palatoglossal arch
Palatopharyngeal arch
Posterior wallof oropharynx
Tongue
Lingual frenulum
Gingivae (gums)
Inferior labial frenulum
Vestibule
Duct ofsubmandibular gland
Palatine tonsil
Uvula
Soft palate
Hard palate
Gingivae (gums)
Inferior lip
Scott_96064_PTR_01_1-32_03-11-14.indd 17Scott_96064_PTR_01_1-32_03-11-14.indd 17 3/24/2014 9:08:45 PM3/24/2014 9:08:45 PMHetzelCampbell_19360_PTR_00_pi-xxviii.indd viHetzelCampbell_19360_PTR_00_pi-xxviii.indd vi 10/4/2017 5:52:12 PM10/4/2017 5:52:12 PM
This is a sample from QUICK REFERENCE FOR OTOLARYNGOLOGY: GUIDE FOR APRNS, PAS, AND
VISIT THIS BOOK’S WEB PAGE BUY NOW REQUEST AN EXAM OR REVIEW COPY
© Springer Publishing Company
OTHER HEALTH CARE PRACTITIONERS

Edentulous ■
Loose teeth ■
Orthodontic appliance ■
Pitted ■
Poorly developed ■
Teeth missing ■
Tender to percussion ■
Gingiva: ■
Bleeding ■
Excessive growth of soft tissue ■
Hypertrophic ■
Infl amed ■
Pyorrhea ■
Ulcerated ■
Hard palate: ■
Cleft ■
Erythematous ■
High arched ■
Lesion ■
Perforated ■
Petechiae ■
Submucous cleft ■
Torus palatinus ■
Ulcers—anteriorly ■
Ulcers—posteriorly ■
Soft palate: ■
Abnormal motion on phonation ■
Asymmetric ■
Bifed uvula ■
Cleft ■
Edematous uvula ■
Erythematous ■
Lesion noted ■
Petechiae ■
Ptotic ■
Ulcers ■
Well-healed UPPP (uvulopalatopharyngoplasty) ■
Tongue: ■
Ankyloglossia ■
Atrophic ■
Cracked ■
Deep red smooth surface at midline ■
Dry ■
Edematous ■
Fissured ■
Furrowed ■
Geographic ■
Leukoplakia ■
Lesion noted ■
Mass ■
Patchy areas devoid of papillae ■
Telangiectatic ■
Tender ■
Scott_96064_PTR_01_1-32_03-11-14.indd 18Scott_96064_PTR_01_1-32_03-11-14.indd 18 3/24/2014 9:08:45 PM3/24/2014 9:08:45 PMHetzelCampbell_19360_PTR_00_pi-xxviii.indd viHetzelCampbell_19360_PTR_00_pi-xxviii.indd vi 10/4/2017 5:52:12 PM10/4/2017 5:52:12 PM
This is a sample from QUICK REFERENCE FOR OTOLARYNGOLOGY: GUIDE FOR APRNS, PAS, AND
VISIT THIS BOOK’S WEB PAGE BUY NOW REQUEST AN EXAM OR REVIEW COPY
© Springer Publishing Company
OTHER HEALTH CARE PRACTITIONERS

Ulcerated ■
White patches ■
Oral mucosa: ■
Aphthous ulcers ■
Cyst ■
Dry ■
Erythroplasia ■
Koplik spots ■
Lesion noted ■
Leukoplakia ■
Oral warts present ■
Pigmented ■
Polyp ■
Ulcers—anteriorly ■
Ulcers—posteriorly ■
Vesicles ■
White patches ■
Pink ■
Moist ■
Oropharynx: ■
Bulging of pharyngeal wall (right/left) ■
Edema of uvula ■
Edema of posterior oropharyngeal wall ■
Erythema ■
Foreign body present ■
Hypersecretion ■
Lymphonodular tissue ■
Profuse lymphoid tissue (lateral bands) ■
Pterygoid tender ■
Purulence of posterior pharyngeal wall ■
Swelling of pharyngeal mucosa ■
Tender ■
Tonsils surgically absent ■
Uvular deviation ■
Well-healing palatal incision ■
Well-healing tonsil fossa ■
White exudate ■
■ Tonsils:Anteriorly displaced ■
Bleeding ■
Cryptic ■
Discharge present ( ■ describe)Erythematous ■
Fibropurulent pseudomembrane ■
Foreign body lodged in tonsillar tissue ■
Hypertrophic ■
Peritonsillar abscess ■
Tonsilliths ■
Ulcerated ■
Lingual tonsils: ■
■ The lingual tonsil is a small mound of lymph tissue located at the base of the tongue and can sometimes be diffi cult to assess without an endoscope.
Abnormal•
Figure 1.11: Tonsil size scoring.
Figure 1.12: Oropharynx, hypopharynx, trachea, and larynx.
Scott_96064_PTR_01_1-32_03-11-14.indd 19Scott_96064_PTR_01_1-32_03-11-14.indd 19 3/24/2014 9:08:45 PM3/24/2014 9:08:45 PMHetzelCampbell_19360_PTR_00_pi-xxviii.indd viHetzelCampbell_19360_PTR_00_pi-xxviii.indd vi 10/4/2017 5:52:12 PM10/4/2017 5:52:12 PM
This is a sample from QUICK REFERENCE FOR OTOLARYNGOLOGY: GUIDE FOR APRNS, PAS, AND
VISIT THIS BOOK’S WEB PAGE BUY NOW REQUEST AN EXAM OR REVIEW COPY
© Springer Publishing Company
OTHER HEALTH CARE PRACTITIONERS

Saliva: Possible Abnormal FindingsDocument the saliva description:
Bloody ■
Clear ■
Copious ■
Enlarged• Erythematous• Hypertrophied• Obstructing view of vallecula• Ulcerated•
Floor of mouth ( ■ FOM):Abnormal Warthin’s duct orifi ce ■
Discoloration ■
Cyst ■
Edematous ■
Erythroplasia ■
Lesion or mass ■
Leukoplakia ■
Torus mandibularis ■
Ulcerated ■
0Surgically removed tonsils
3Tonsils are beyond
the pillars
4Tonsils extend to midline
1Tonsils hidden within
tonsil pillars
2Tonsils extending to
the pillars
FIGURE 1.11 Tonsil size scoring.
Scott_96064_PTR_01_1-32_03-11-14.indd 20Scott_96064_PTR_01_1-32_03-11-14.indd 20 3/24/2014 9:08:45 PM3/24/2014 9:08:45 PMHetzelCampbell_19360_PTR_00_pi-xxviii.indd viHetzelCampbell_19360_PTR_00_pi-xxviii.indd vi 10/4/2017 5:52:12 PM10/4/2017 5:52:12 PM
This is a sample from QUICK REFERENCE FOR OTOLARYNGOLOGY: GUIDE FOR APRNS, PAS, AND
VISIT THIS BOOK’S WEB PAGE BUY NOW REQUEST AN EXAM OR REVIEW COPY
© Springer Publishing Company
OTHER HEALTH CARE PRACTITIONERS

Findings on Oral Bimanual Examination
Oral bimanual examination is a method of examination in which both the hands are used to examine the patient’s oral cavity from both the inside and outside at the same time.
Normal Findings on Oral Bimanual ExaminationDocument:
Palpation of the labial mucosa, buccal mucosa, hard and soft palate, oropharynx and ■
tonsillar region, retromolar trigone, tongue, fl oor of mouth, gingivae, and teeth are normal.
Purulent ■
Scant ■
Thick ■
Thin ■
Frontal sinus
Sella turcica
Adenoid
Pharyngeal opening ofauditory (eustachian) tube
Thyroid cartilage
Vocal fold (cord)
Transverse arytenoid muscle
Cricoid cartilage
Trachea
Esophagus
Sphenoid sinus
Soft palate
Hard palate
Incisive canal
Uvula
Oral cavity
Body of tongue
Palatine tonsil
Lingual tonsil
Base of tongue
Epiglottis
Hyoid bone
Thyrohyoid membrane
Nasopharynx
Oropharynx
Hypopharynx
FIGURE 1.12 Oropharynx, hypopharynx, trachea, and larynx.
Scott_96064_PTR_01_1-32_03-11-14.indd 21Scott_96064_PTR_01_1-32_03-11-14.indd 21 3/24/2014 9:08:46 PM3/24/2014 9:08:46 PMHetzelCampbell_19360_PTR_00_pi-xxviii.indd viHetzelCampbell_19360_PTR_00_pi-xxviii.indd vi 10/4/2017 5:52:12 PM10/4/2017 5:52:12 PM
This is a sample from QUICK REFERENCE FOR OTOLARYNGOLOGY: GUIDE FOR APRNS, PAS, AND
VISIT THIS BOOK’S WEB PAGE BUY NOW REQUEST AN EXAM OR REVIEW COPY
© Springer Publishing Company
OTHER HEALTH CARE PRACTITIONERS

PROCEDURE PROTOCOL: FLEXIBLE FIBEROPTIC LARYNGOSCOPY
Indications
Alteration of voice/swallowing/feeling of foreign substance in throat ■
History of head and/or neck cancer ■
Airway obstruction ■
Sleep apnea ■
Contraindications
Patients with signs of acute airway obstruction or possibility of epiglottitis should be immediately referred to the supervising physician or transported by ambulance to the emergency department.
Equipment Needed
Spray containing a topical anesthetic and a vasoconstrictor (e.g., Afrin and ■
lidocaine) ■ Endoscope
Procedure Protocol
Seat the patient comfortably in an examination chair. Instruct the patient to ■
move the hips to the back of the chair, straighten the back, lean forward, and tilt the chin up as if “sniffi ng fl owers.”Decongest with a spray mixture that contains a topical anesthetic and vaso- ■
constrictor (i.e., Afrin and lidocaine). Direct the spray posteriorly—parallel to the fl oor of the nose and not toward the ceiling. Wait several minutes after spraying to permit decongestant and anesthetic to take effect. NOTE: Tell your patient that the solution may taste bitter and may produce a numbing sensation in the nose, mouth, and throat. The patient may feel like he or she cannot swal-low or talk, but ensure the patient that these functions are not affected with this medication.Position yourself in front or to the side of the patient. Introduce the scope gen- ■
tly into one nostril (usually the nostril that appears more open than the other) and pass it along the fl oor of the nose. Try to avoid the nasal septum.
Figure 1.13: Larynx landmarks.
Oral Bimanual Examination: Possible Abnormal FindingsDocument the presence of any of the following abnormal fi ndings:
Asymmetry ■
Bleeding ■
Depression ■
Edema ■
Erythema ■
Induration ■
Lesion or mass ■
Tenderness ■
■ Ulceration
Video 1.2: Flexible fi beroptic laryngoscopy.
(continued)
Scott_96064_PTR_01_1-32_03-11-14.indd 22Scott_96064_PTR_01_1-32_03-11-14.indd 22 3/24/2014 9:08:46 PM3/24/2014 9:08:46 PMHetzelCampbell_19360_PTR_00_pi-xxviii.indd viHetzelCampbell_19360_PTR_00_pi-xxviii.indd vi 10/4/2017 5:52:12 PM10/4/2017 5:52:12 PM
This is a sample from QUICK REFERENCE FOR OTOLARYNGOLOGY: GUIDE FOR APRNS, PAS, AND
VISIT THIS BOOK’S WEB PAGE BUY NOW REQUEST AN EXAM OR REVIEW COPY
© Springer Publishing Company
OTHER HEALTH CARE PRACTITIONERS

If you are unable to advance along the fl oor of the nose because of a septal ■
deviation or large inferior turbinate, try advancing the scope above the infe-rior turbinate or attempt entrance into the nasal cavity on the opposite side of the nose.Once the scope is in the back of the nose, turn the scope downward to ■
examine the oropharynx, hypopharynx, and larynx. Observe the epiglot-tis and assess the tongue base. Ask the patient to extend the tongue to expose the vallecula. Assess both sides of the epiglottis. Ask the patient to blow the nose against closed nostrils or have the patient “blow the cheeks out” in order to infl ate the pyriform sinuses. Closely examine the true and false vocal cords and assess for mobility, color, swelling, nodules, or other mucosal lesions (see below for common abnormal fi ndings on fl exible fi beroptic laryngoscopy examination). NOTE: If you are using equipment with a screen or monitor, keep in mind that the right vocal cord will be on the left side of the screen and the left vocal cord will be on the right side of the screen. It is similar to looking at CT scans. The patient is anatomically facing you on the monitor.Instruct the patient to say “eee” to allow visualization of vocal cord mobility. ■
Note any incomplete abduction or adduction of the vocal cords. NOTE: If you have a hard time getting the vocal cords to completely abduct, ask the patient to “sniff” like sniffi ng a fl ower.Evaluate the subglottic trachea through the vocal cords for narrowing or ■
“subglottic stenosis.” After complete visualization of the larynx, with-draw the scope from the larynx and inspect the remainder of the hypo-pharynx.
Cleaning of the Equipment
At the conclusion of the procedure, gently wash the endoscope with running water and place it in an enzymatic cleanser. Then rinse the scope to remove any cleanser and hang up to dry before use on the next patient.
Potential Complications
Pain, bleeding, fainting, adverse drug reaction, laryngospasm, airway loss.
(continued)
PROCEDURE PROTOCOL: EVALUATING THE LARYNX WITH INDIRECT MIRROR EXAMINATION
Overview
Indirect mirror examination allows for more complete inspection of the larynx without doing a fl exible fi beroptic endoscopy. Various anatomical structures can be viewed with indirect mirror examination including the base of the tongue, vallecula, epiglottis, each arytenoid cartilage, aryepiglottic folds, pyriform fos-sae, and esophageal area.
Scott_96064_PTR_01_1-32_03-11-14.indd 23Scott_96064_PTR_01_1-32_03-11-14.indd 23 3/24/2014 9:08:47 PM3/24/2014 9:08:47 PMHetzelCampbell_19360_PTR_00_pi-xxviii.indd viHetzelCampbell_19360_PTR_00_pi-xxviii.indd vi 10/4/2017 5:52:12 PM10/4/2017 5:52:12 PM
This is a sample from QUICK REFERENCE FOR OTOLARYNGOLOGY: GUIDE FOR APRNS, PAS, AND
VISIT THIS BOOK’S WEB PAGE BUY NOW REQUEST AN EXAM OR REVIEW COPY
© Springer Publishing Company
OTHER HEALTH CARE PRACTITIONERS

PROCEDURE PROTOCOL: EVALUATING THE LARYNX WITH INDIRECT MIRROR EXAMINATION (continued)
Indications
Noncompliant patient with fl exible fi beroptic laryngoscopy ■
A patient who is allergic to topical anesthetics or decongestants used for the ■
fl exible fi beroptic laryngoscopy examinationTo evaluate for base of tongue and/or laryngeal abnormalities ■
Contraindications
No absolute contraindications exist.
Equipment Needed
Gauze squares ■
Tongue blade ■
Hurricaine spray ■
Headlamp ■
Indirect nasopharyngeal/laryngeal mirror ■
Procedure Protocol
Seat the patient comfortably in an examination chair. Instruct the patient to ■
move the hips to the back of the chair, straighten the back, and lean forward with mouth open and tongue extended.Position yourself in front or to the side of the patient. Wear your headlight ■
throughout this procedure.If gagging is expected with the patient, a topical anesthetic can be applied ■
(e.g., Hurricaine spray).Using one hand, wrap a gauze square around the patient’s tongue and hold ■
the tongue with your thumb and middle fi nger. Use your index fi nger to ele-vate the patient’s upper lip, as needed. Another option is to have the patient hold the tongue, while you use a tongue depressor.In the opposite hand, insert a small mirror. Use a mirror that has been pre- ■
viously “dipped” in a defog solution. Position the mirror so that it passes between the tonsils and elevates the soft palate. Encourage the patient to breathe deeply through the mouth and relax.The refl ected light in the small mirror from your headlight illuminates the ■
base of tongue and the laryngopharynx. A minor degree of rotation of the laryngeal mirror assists in illuminating and examining the various anatomical structures.Instruct the patient to say “eee” to allow visualization of vocal cord mobil- ■
ity. Note any incomplete abduction or adduction of the vocal cords. Evaluate the subglottic trachea through the vocal cords for narrowing or “subglottic stenosis.”
Scott_96064_PTR_01_1-32_03-11-14.indd 24Scott_96064_PTR_01_1-32_03-11-14.indd 24 3/24/2014 9:08:47 PM3/24/2014 9:08:47 PMHetzelCampbell_19360_PTR_00_pi-xxviii.indd viHetzelCampbell_19360_PTR_00_pi-xxviii.indd vi 10/4/2017 5:52:12 PM10/4/2017 5:52:12 PM
This is a sample from QUICK REFERENCE FOR OTOLARYNGOLOGY: GUIDE FOR APRNS, PAS, AND
VISIT THIS BOOK’S WEB PAGE BUY NOW REQUEST AN EXAM OR REVIEW COPY
© Springer Publishing Company
OTHER HEALTH CARE PRACTITIONERS

Epiglottis
Base of tongue(lingual tonsil)
Ventricular folds(false cords)
Vestibule
Aryepiglottic fold
Ventricle
ArytenoidEsophagus
Interarytenoidnotch
Piriform recess
Trachea
Glottic aperature
Vocal folds(true cords)
Vallecula
Median glosso-epiglottic fold
FIGURE 1.13 Larynx landmarks.
The Larynx With Flexible Fiberoptic Laryngoscopy and Indirect Mirror Examination
Larynx and Hypopharynx: Possible Abnormal FindingsDocument the presence of any of the following abnormal fi ndings:
Larynx: ■
Anterior web ■
Atresia ■
Diffuse edema ■
Dry mucosa ■
Erythema ■
Erythema—posterior commissure ■
Erythema—posterior one third of vocal cords ■
Exudate ■
Foreign body present ■
Granuloma formation ■
Indwelling prosthesis in place ■
Laryngeal contact ulcers ■
Laryngomalacia ■
Mucosal edema ■
Mucosal lesion ■
Status post laryngectomy ■
Submucosal edema ■
Voice prosthesis present ■
Hypopharynx: ■
Erythema ■
Scott_96064_PTR_01_1-32_03-11-14.indd 25Scott_96064_PTR_01_1-32_03-11-14.indd 25 3/24/2014 9:08:47 PM3/24/2014 9:08:47 PM
This is a sample from QUICK REFERENCE FOR OTOLARYNGOLOGY: GUIDE FOR APRNS, PAS, AND
VISIT THIS BOOK’S WEB PAGE BUY NOW REQUEST AN EXAM OR REVIEW COPYOTHER HEALTH CARE PRACTITIONERS
© Springer Publishing Company

Foreign body present ■
Lymphonodular tissue ■
Supraglottis: Possible Abnormal FindingsDocument the presence of any of the following abnormal fi ndings:
Epiglottis: ■
Angioedema ■
Asymmetry ■
Edema ■
Epiglottitis ■
Erythema ■
Exudate ■
Lesion ■
Mass ■
Omega-shaped ■
Vallecula: ■
Cyst ■
Edema ■
Erythema ■
Exudate ■
Lesion or mass ■
Pharyngeal walls: ■
Edema ■
Erythema ■
Exudate ■
Lesion or mass ■
Pyriform sinus: ■
Asymmetry ■
Exudate ■
Fullness ■
Lesion or mass ■
Mucus pooling ■
Glottis: ■
Anterior–posterior glottis compression ■
Glottic gap ■
Figure 1.14: Omega-shaped epiglottis and vallecula.
FIGURE 1.14 Omega-shaped epiglottis and vallecula.
OMEGA-SHAPED EPIGLOTTIS
VALLECULA
Scott_96064_PTR_01_1-32_03-11-14.indd 26Scott_96064_PTR_01_1-32_03-11-14.indd 26 3/24/2014 9:08:48 PM3/24/2014 9:08:48 PMHetzelCampbell_19360_PTR_00_pi-xxviii.indd viHetzelCampbell_19360_PTR_00_pi-xxviii.indd vi 10/4/2017 5:52:12 PM10/4/2017 5:52:12 PM
This is a sample from QUICK REFERENCE FOR OTOLARYNGOLOGY: GUIDE FOR APRNS, PAS, AND
VISIT THIS BOOK’S WEB PAGE BUY NOW REQUEST AN EXAM OR REVIEW COPY
© Springer Publishing Company
OTHER HEALTH CARE PRACTITIONERS

Interarytenoid area (posterior glottis): ■
Edema ■
Erythema ■
Lesion or mass ■
True vocal cords (TVC): ■
Atrophy ■
Bleb ■
Bowing ■
Edema ■
Erythema ■
Glottic cyst ■
Glottic obstruction present ■
Glottic web visualized ■
Granular appearance ■
Leukoplakia ■
Nodule ■
Paradoxic TVC mobility ■
Paralysis ■
Polyp ■
Poor mobility ■
Stenosis ■
Subglottic stenosis ■
Ulceration ■
Glottic gap ■
Prominent vocal process ■
False vocal cords: ■
Abnormal movements ■
Adduction ■
Dry mucosa ■
Edema ■
Edematous polyp ■
Fusiform polyp ■
Hemorrhagic polyp ■
Impairment of function ■
Leukoplakia ■
Pedunculated polyp ■
Poor mobility ■
Stenosis ■
Ulceration ■
White thickening ■
False cord compensation ■
Aryepiglottic folds: ■
Decreased mobility on inspiration ■
Decreased mobility on phonation ■
Arytenoid cartilage: ■
Arytenoid edema ■
Erythema of arytenoids ■
Lesion or mass ■
Subglottis: ■
Edema ■
Erythema ■
Exudate ■
Mass ■
Stenosis ■
Scott_96064_PTR_01_1-32_03-11-14.indd 27Scott_96064_PTR_01_1-32_03-11-14.indd 27 3/24/2014 9:08:52 PM3/24/2014 9:08:52 PMHetzelCampbell_19360_PTR_00_pi-xxviii.indd viHetzelCampbell_19360_PTR_00_pi-xxviii.indd vi 10/4/2017 5:52:12 PM10/4/2017 5:52:12 PM
This is a sample from QUICK REFERENCE FOR OTOLARYNGOLOGY: GUIDE FOR APRNS, PAS, AND
VISIT THIS BOOK’S WEB PAGE BUY NOW REQUEST AN EXAM OR REVIEW COPY
© Springer Publishing Company
OTHER HEALTH CARE PRACTITIONERS

The Neck
Normal Exam Findings of NeckDocument:
Nontender with full range of motion (ROM) on fl exion, extension, and lateral rotation. ■
Trachea is midline. ■
No lymphadenopathy or palpable mass/lesion present. ■
No bruit. ■
Thyroid is nonpalpable. ■
NOTE: If previous neck surgery, document “well healing” or “healed neck incision.” ■
Neck: Possible Abnormal FindingsDocument the presence of any of the following abnormal fi ndings:
Abnormal movements ■
Decreased ROM ■
Figure 1.15: Cartilages of larynx.
Epiglottis
Hyoid bone
Thyrohyoid membrane
Larynx location
Superior horn ofthyroid cartilage
Arytenoid cartilage(behind thyroid cartilage)
Thyroid cartilage
Cricothyroid ligament
Inferior horn ofthyroid cartilage
Cricoid cartilage
Trachea
Anterior View
FIGURE 1.15 Cartilages of larynx.
Scott_96064_PTR_01_1-32_03-11-14.indd 28Scott_96064_PTR_01_1-32_03-11-14.indd 28 3/24/2014 9:08:52 PM3/24/2014 9:08:52 PMHetzelCampbell_19360_PTR_00_pi-xxviii.indd viHetzelCampbell_19360_PTR_00_pi-xxviii.indd vi 10/4/2017 5:52:12 PM10/4/2017 5:52:12 PM
This is a sample from QUICK REFERENCE FOR OTOLARYNGOLOGY: GUIDE FOR APRNS, PAS, AND
VISIT THIS BOOK’S WEB PAGE BUY NOW REQUEST AN EXAM OR REVIEW COPY
© Springer Publishing Company
OTHER HEALTH CARE PRACTITIONERS
Tender—mild ■
Tender—exquisite ■
Lymphadenopathy ■
Mass—right ■
Mass—left ■
Midline nodule consistent with thyroglossal duct cyst ■
Subcutaneous emphysema ■
Sutures present ■
Carotid Arteries: Possible Abnormal FindingsDocument the presence of any of the following abnormal fi ndings:
Bruit ■
Tenderness to palpation ■
Visibly pulsatile ■
Trachea: Possible Abnormal FindingsDocument the presence of any of the following abnormal fi ndings:
Deviated to the right ■
Deviated to the left ■
Endotracheal tube in place ■
Tracheostomy present ■
Status post laryngectomy ■
Stenosis ■
The Neck: Lymphatic System
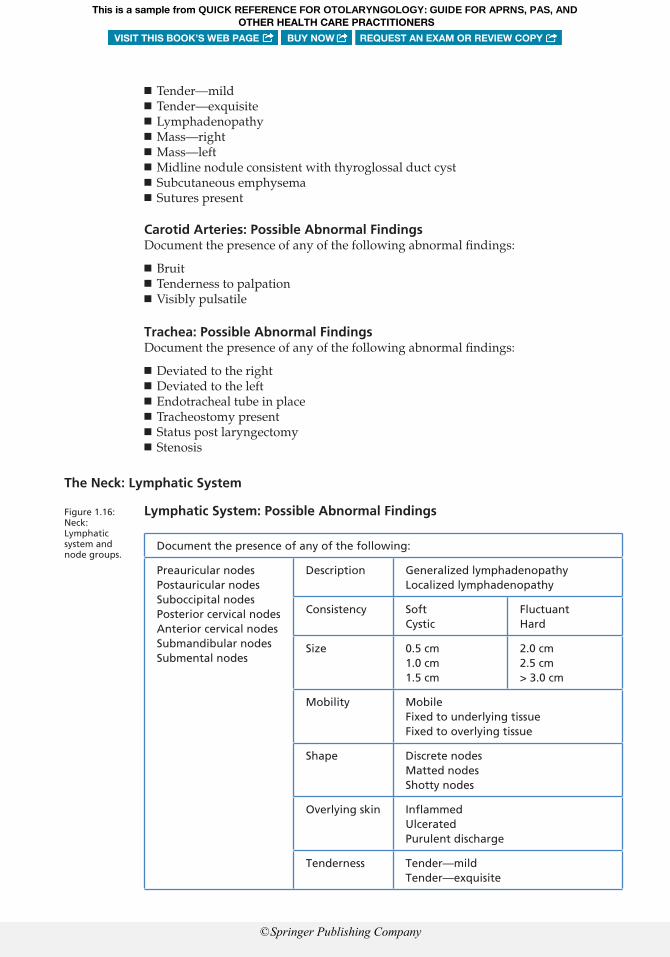
Lymphatic System: Possible Abnormal Findings
Document the presence of any of the following:
Preauricular nodesPostauricular nodesSuboccipital nodesPosterior cervical nodesAnterior cervical nodesSubmandibular nodesSubmental nodes
Description Generalized lymphadenopathyLocalized lymphadenopathy
Consistency SoftCystic
FluctuantHard
Size 0.5 cm1.0 cm1.5 cm
2.0 cm2.5 cm> 3.0 cm
Mobility MobileFixed to underlying tissueFixed to overlying tissue
Shape Discrete nodesMatted nodesShotty nodes
Overlying skin Infl ammedUlceratedPurulent discharge
Tenderness Tender—mildTender—exquisite
Figure 1.16: Neck: Lymphatic system and node groups.
Scott_96064_PTR_01_1-32_03-11-14.indd 29Scott_96064_PTR_01_1-32_03-11-14.indd 29 3/24/2014 9:08:52 PM3/24/2014 9:08:52 PMHetzelCampbell_19360_PTR_00_pi-xxviii.indd viHetzelCampbell_19360_PTR_00_pi-xxviii.indd vi 10/4/2017 5:52:12 PM10/4/2017 5:52:12 PM
This is a sample from QUICK REFERENCE FOR OTOLARYNGOLOGY: GUIDE FOR APRNS, PAS, AND
VISIT THIS BOOK’S WEB PAGE BUY NOW REQUEST AN EXAM OR REVIEW COPY
© Springer Publishing Company
OTHER HEALTH CARE PRACTITIONERS

FIGURE 1.16 Neck: Lymphatic system and node groups.
Superficial parotid nodes(deep parotid nodes deep
to parotid gland)
Occipital nodes
Mastoid nodes
Subparotid node (Level II)
Mandibular andsubmandibularnodes (Level I)
Submental nodes (Level I)
Suprahyoid node (Level I)
Internal jugular chain of nodes(deep lateral cervical nodes) (Levels II and III)
Anterior deep cervical (pretracheal andthyroid) nodes (deep to strap muscles) (Level VI)
Anterior superficial cervical nodes(anterior jugular nodes) (Level VI)
Supraclavicular nodes (Level IV)
Facial nodes(buccal nodes)
Jugulodigastric node (Level II)
Deep lateral nodes(spinal accessory nodes) (Level V)
Inferior deep cervical(scalene) node (Level IV)
Transverse cervicalchain of nodes (Level V)
Level I nodes Level II nodes Level III nodes
Level IV nodes Level V nodes Level VI nodes
Scott_96064_P
TR
_01_1-32_03-11-14.indd 30S
cott_96064_PT
R_01_1-32_03-11-14.indd 30
3/24/2014 9:08:52 PM
3/24/2014 9:08:52 PM
This is a sample from QUICK REFERENCE FOR OTOLARYNGOLOGY: GUIDE FOR APRNS, PAS, ANDOTHER HEALTH CARE PRACTITIONERS
VISIT THIS BOOK’S WEB PAGE BUY NOW REQUEST AN EXAM OR REVIEW COPY
© Springer Publishing Company

The Thyroid
Normally on examination, the thyroid is nonpalpable. However, if the thyroid is pal-pable, it can be felt on either side of the trachea just superior to the sternal notch.
Thyroid: Possible Abnormal FindingsDocument the presence of any of the following abnormal fi ndings:
Gland characteristics: ■
Asymmetric ■
Boggy ■
Enlarged ■
Hard ■
No palpable nodules ■
Smooth ■
Symmetric ■
Tender ■
Mass or nodule: ■
Size ■
Document in mm or cm• Location ■
Right upper lobe• Left upper lobe• Right mid-lobe• Left mid-lobe• Right lobe lower pole• Left lobe lower pole• Midline•
Texture ■
Soft• Firm• Cystic•
Mass or nodule: ■
Tenderness ■
Tender—mild• Tender—moderate• Tender—exquisite•
Other characteristics ■
Dominant nodule• Fixed nodule• Mobile• Moves laterally• Moves on swallowing• Multinodular• Solitary nodule•
BIBLIOGRAPHY
Bailey, B. J., & Johnson, J. T. (2006). Head and neck surgery—otolaryngology (p. 2686). Philadelphia, PA: Lippincott Williams & Wilkins.
Edwin, W. C., Jr. Indirect laryngoscopy and nasopharyngoscopy instructions. Welch Allen. Retrieved from http://www.welchallyn.com/documents/EENT/Illuminators/userinstructions_20070321_illu-minators_transilluminators_tongue_blade_holders.pdf. February 2, 2013.
Scott_96064_PTR_01_1-32_03-11-14.indd 31Scott_96064_PTR_01_1-32_03-11-14.indd 31 3/24/2014 9:08:54 PM3/24/2014 9:08:54 PMHetzelCampbell_19360_PTR_00_pi-xxviii.indd viHetzelCampbell_19360_PTR_00_pi-xxviii.indd vi 10/4/2017 5:52:12 PM10/4/2017 5:52:12 PM
This is a sample from QUICK REFERENCE FOR OTOLARYNGOLOGY: GUIDE FOR APRNS, PAS, AND
VISIT THIS BOOK’S WEB PAGE BUY NOW REQUEST AN EXAM OR REVIEW COPY
© Springer Publishing Company
OTHER HEALTH CARE PRACTITIONERS

Harris, L. L., & Huntoon, M. B. (2008). Core curriculum for otorhinolaryngology and head-neck nursing (2nd ed., p. 64). New Smyrna Beach, FL: Society of Otorhinolaryngology and Head-Neck Nurses,
Hawke, M., Keene, M., & Alberti, P. W. (1984). Clinical otoscopy: A text and colour atlas. Edinburgh: Churchill Livingstone.
Jafek, B. W., & Stark, A. K. (1996). ENT secrets. Philadelphia, PA: Hanley & Belfus.Lalwani, A. K. (2008). Current diagnosis and treatment otolaryngology head and neck surgery. New York: NY:
McGraw-Hill.Lee, K. J. (1999). Essential otolaryngology head and neck surgery (9th ed.). New York: McGraw-Hill.McCance, K. L., & Huether, S. E. (2002). Pathophysiology: The biologic basis for disease in adults and children
(4th ed., p. 427). St. Louis, MO: Mosby.Netter, F. H. (1989). Atlas of human anatomy (Plate 31). West Caldwell, NJ: Pharmaceuticals Division,
CIBA-GEIGY Corporation.Pansky, B. (1984). Review of gross anatomy (5th ed.). New York: Macmillian.
Scott_96064_PTR_01_1-32_03-11-14.indd 32Scott_96064_PTR_01_1-32_03-11-14.indd 32 3/24/2014 9:08:54 PM3/24/2014 9:08:54 PMHetzelCampbell_19360_PTR_00_pi-xxviii.indd viHetzelCampbell_19360_PTR_00_pi-xxviii.indd vi 10/4/2017 5:52:12 PM10/4/2017 5:52:12 PM
This is a sample from QUICK REFERENCE FOR OTOLARYNGOLOGY: GUIDE FOR APRNS, PAS, AND
VISIT THIS BOOK’S WEB PAGE BUY NOW REQUEST AN EXAM OR REVIEW COPY
© Springer Publishing Company
OTHER HEALTH CARE PRACTITIONERS