Embed Size (px)
Citation preview

Kliniske undersøgelsers hierarki
Dirac kursus 4 b30-3-2005
Henrik E. Poulsen
Professor, Overlæge dr.med.Klinisk Farmakologisk Afdeling Q7642
RigshospitaletTel 3545 7671 [email protected]



sheSeptember 1999
http://www.themedweb.co.uk/didyouknow/
Zoneterapi
Vaginal zoneterapiSkrevet af Camilla Kjems
God sex er healende og en af forudsætningerne for et velfungerende forhold, mener Irina Andersen, der ved hjælp af vaginal akupressur kan afhjælpe problemer med underlivet og sexlivet.
Mange kvinder har problemer med underlivet og sexlivet. De døjer med krampe og svie og har måske svært ved at få orgasme. Irina Andersen er kvinden, der tager over, hvor mange læger giver op. Hun kan som den eneste i Danmark behandle med den gamle tantriske behandlingsform vaginal akupressur.
Vaginal accupressurLigesom zoneterapi forløser vaginal akupressur fysiske og psykiske problemer ved hjælp af tryk med fingrene. Men hvor zoneterapienstager udgangspunkt i fødderne, arbejder den vaginale akupressur med tryk indeni og udenpå skeden, på hofterne lænden og ryggen. – Hvor huden under fødderne er meget grov, er vaginaen noget af det fineste, hvilket betyder, at denne behandling er meget effektiv,fortæller Irina.
Vaginal akupressur kan afhjælpe:- Krampe, svie og kløe i skeden- Ubehag ved elskov- Skedekrampe- Problemer med at få orgasme- Problemer i forbindelse med fødsel og graviditet- Tilbagevendende svamp og blærebetændelse- Incest- og overgrebsproblematikker
Stort erotisk potentialeSelvom det er en meget intim behandlingsform, oplever kvinderne, der kommer hos Irina, det sjældent som noget ubehageligt.
Eksempel på en forkert bøjet tommelfinger:
Eksempel på en rigtig bøjet tommelfinger:

Vi er da meget mere objektive I vores aktuelle moderne behandling ?
Diabetes today (Type II, NIDDM)
Treatment:
Dietary counseling and a strict diet, insulin sensitizers/secretion stimulants
Diabetes units are manned with doctors and dieticians
There are no physiotherapist and no training centres
Diabetes is a muscle disease !
Diabetes and impaired glucose tolerance: main reason is lack of exercise
Exercise in the untrained can double or triple insulin sensitivity

Hvorledes rankeres (videnskabelig) evidence ?
Adams H, Brott T, Furland A, Gomez C, Grotta J, Helgason C et al.
Guidelines for the managment of patients with acute ischemic stroke. Astatementfor healthcare professionals from a special writing group of the stroke counsil, American Heart Association
Stroke 1994; 25:1901-14
Kaste M, Olsen TS, Orgogozo J-M, Bogousslavsky J, Hacke W for the EUSI Excecutive Committee
Organization of stroke care, Education, Stroke Units and Rehabilitation
Cerebrosvasc Dis 2000;10(suppl 3): 1-11

The hierarchy of clinical evidence:
Level I: Highest level of evidenceprimary endpoints from randomized, double-blinded study with adequate sample sizeproperly performed meta-analysis of quality outstanding randomizedtrials
Level II: Intermediate level of evidencerandomized, non-blinded trialssmall randomized trialspre-defined secondary end-points of large randomized trials
Level III: Lower level of evidenceprospective case series with concurrent or historical control epidemiologypost hoc analyses of randomized trialsgovernmental or other public clearing reports
Level IV: undetermined level of evidencecase reportssmall case series without controlgeneral agreement despite lack of scientific evidence from controlled trials

TABLE 1. GRADES OF EVIDENCE FOR THE PURPORTED QUALITYOF STUDY DESIGN *
I Evidence obtained from at least one properly randomized, controlled trial.
II-1 Evidence obtained from well-designed controlled trialswithout randomization.
II-2 Evidence obtained from well-designed cohort or case–controlanalyticstudies, preferably from more than one center orresearch group.
II-3 Evidence obtained from multiple time series with or withoutthe intervention. Dramatic results in uncontrolledexperiments (such as the results of the introduction ofpenicillin treatment in the 1940s) could also be regarded as this type of evidence.
III Opinions of respected authorities, based on clinicalexperience; descriptivestudies and case reports; or reportsof expert committees.
*The grades are those of the U.S. Preventive Services Task Force.2nd ed. Baltimore: Williams & Wilkins, 1996
Concato J, NEJM 2000;342:1887-92

Why Control ? Why Randomization
One statistician to another:How’s your wife?Compared to what !
Nosocomialborder
Diseaseactivity
Timespring autumn
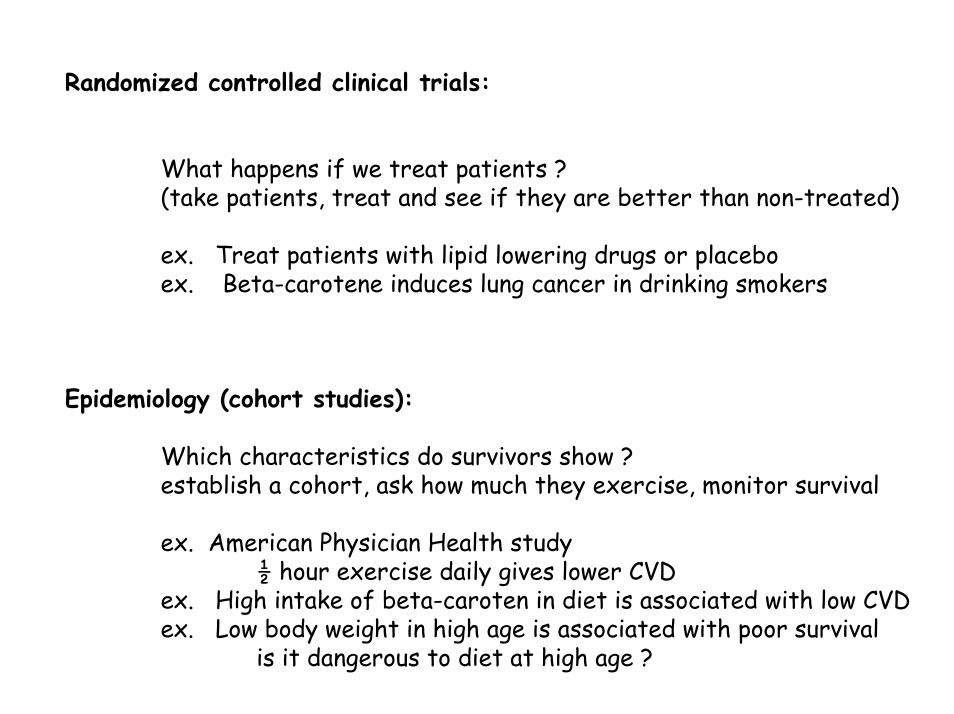
Randomized controlled clinical trials:
What happens if we treat patients ?(take patients, treat and see if they are better than non-treated)
ex. Treat patients with lipid lowering drugs or placeboex. Beta-carotene induces lung cancer in drinking smokers
Epidemiology (cohort studies):
Which characteristics do survivors show ?establish a cohort, ask how much they exercise, monitor survival
ex. American Physician Health study½ hour exercise daily gives lower CVD
ex. High intake of beta-caroten in diet is associated with low CVDex. Low body weight in high age is associated with poor survival
is it dangerous to diet at high age ?

BMJ 1996;312:71-72 (13 January) Editorials Evidence based medicine: what it is and what it isn't “It's about integrating individual clinical expertise and the best external evidence”
“Evidence based medicine, whose philosophical origins extend back to mid-19th century Paris and earlier, remains a hot topic for clinicians, public health practitioners, purchasers, planners, and the public.”
“the Cochrane Collaboration and Britain's Centre for Review and Dissemination in York are providing systematic reviews of the effects of health care; new evidence based practice journals arebeing launched; and it has become a common topic in the lay media”
“Evidence based medicine is the conscientious, explicit, and judicious use of current best evidence in making decisions about the care of individual patients”
“Evidence based medicine is neither old hat nor impossible to practice”

”Errors” in clinical trials:
The classical errors:
Type I and Type II errors difference due to chance, overse a true difference
Other errors
Type III erors: Wrong statistical methodWrong patient groupWrong diagnosisWrong primary variableWrong design……Wrong strategy (commercially inspired)Wrong comparison (placebo ? best available treatment?……no ”intention to treat analysis”
Type IV errors: Doing the study for the ”wrong reasons”

Publication bias:
Bekelman JE JAMA. 2003;289:454-465. Data Synthesis Aggregating the results of thesearticles showed a statistically significant association between industry sponsorship and pro-industryconclusions (pooled Mantel-Haenszel odds ratio, 3.60; 95% confidence interval, 2.63-4.91). Industrysponsorship was also associated with restrictions onpublication and data sharing. The approach to managing financial conflicts varied substantiallyacross academic institutions and peer-reviewedjournals. Conclusions Financial relationships among industry, scientific investigators, and academic institutions arewidespread. Conflicts of interest arising from theseties can influence biomedical research in importantways.

Comparing risks
Relative risk Odds ratio
prospective study retrospective study
a/(a+c)RR= OR = ad/bc
b/(b+d)
Prospective classification
b+da+cc+ddcNoa+bbaYes
Gr 1Gr 1
Retrospective classification

To what degree is evidence based medicine practiced in Denmark ?
No certains estimates:
Qualified guess: maybe about 10-25 %
Hierachy of specialities:(prob heavy biassed) Cardiology (medical)
Oncology (medical)Psychiatry
anestesiology emergency medicine
toxicology
surgery

Why power calculation (1 of 3) ?
Simplified estimate of number of observations
N1 = N2 = 2(t2α,df + tβ,df )2 x (CV2 / MERIDIF2)
• t-values can be obtained from a statistical t-table, • SD is the standard variation of the measurement• MERIDIF is the Minimum RElevant DIfference.• If N1 = N2 is large t-values are about 2 and 1.7.
N1 = N2 = 2(2+1.7)2 x ( SD2 / MERIDIF2) = 27.4 x (SD2 / MERIDIF2)
30 x (CV2 / MERIDIF2) or 30 (CV /MERIDIF)2
[1] http://www.ebook.stat.ucla.edu/calculators/powercalc/[2] http://www.davidmlane.com/hyperstat/power.html/

Statistica 6.0
N1=n2= 30x (0,2/0,2)2 = 30 (stat: 23)
N1=n2= 30x (0,2/0,1)2 = 120 (stat: 86)

Independent Sample t-Test: Sample Size CalculationTwo Means, t-Test, Ind. Samples (H0: Mu1 = Mu2)
N vs. Power (Alpha = 0,05, Es = -0,5)
0,6 0,7 0,8 0,9 1,0
Power Goal
40
50
60
70
80
90
100
110
Req
uire
d S
ampl
e S
ize
(N)

Why Number needed to treat (NNT)?
1NNT =
p1 – p2
NNT = number needed to treat to avoid one case
p1 = observed incidence without treatmentp2 = observed incidence with treatment
Ex. Pneumococ vaccinationp1= 20/100.000, 70% treatment effect, mortality 20%
NNT = 7143 (sepsis); NT = 35.714 (death)

Relation between sample size (SS) and NNT
SS calculation for obtaining significant results
NNT treatment ”efficacy” in public health terms, dependent on incidence and efficacy.
If SS is very great one should consider if the trialshould be done, and whether it is an efficienttreatment

NEJM 2000; 342:1887-92

Epidemiology versus controlled intervention studies
RCT observational
Concato NEJM 342;25:1887-92

Antioxidant trials
Epidemiology consistantly indicate cancer and CVD protection
RCT gives conflicting indicationno effectpositive effectnegative effect

The ALLHAT study (JAMA 288:2981-2997 and 2998-3007)
Controlled trial diuretic chlorthalidone (Hygroton Novartis)Ca-blokker amlodipine (Norvasc, Pfizer)ACE-hæmmer lisinopril (Vivatec MSD, Zestril Zenica)
chlorthalidone 12,5 – 25 mg (0.25 – 0.50 kr [1999])amlodipine 2.5 – 10 mg (0.75 – 3,00 kr)lisinopril 10 -40 mg (1.15 – 4,60 kr)
Initieret af NIH
Pris US$ 125 mio
Rekruitment Feb 1994 – March 31 2002
N 33.357 med hypertension + 1 CHD risiko faktor
Outcome 1: fatal CHD, non-fatal AMI, intention to treat.2: all-cause mortality, stroke, +++

Recent test results are startling. In the largest hypertension clinical trial everconducted, an eight-year study involving more than 42,000 patients, a diureticactually proved more effective than the newer drugs in lowering bloodpressure and preventing cardiovascular complications.
Dec 9, 2002
BMJ 2004, 326:170 Spind doctors soft pedal on antihypertensives:
ALLHAT study JAMA 2002;288:2981-97
Ugeskrift for Læger · 14. april 2003, nr. 16Har det offentlige en selvstændig forskningsmæssig rolle i lægemiddeludviklingen?
STATUSARTIKELHenrik Enghusen Poulsen & Thor Buch Grønlykke




























