Embed Size (px)
Citation preview
945
Preliminary Communications
CARBON-DIOXIDE LASER FOREXCISION OF BURN ESCHARS
STANLEY STELLAR*RALPH GER
NORMAN LEVINESTANLEY M. LEVENSON
Department of Neurosurgery, St. Barnabas Hospital,and Department of Surgery, Albert Einstein College of
Medicine, Bronx, New York, U.S.A.
Summary In experiments in pigs, a continuous-wave carbon-dioxide laser was used
to excise the eschar 24 hours after third-degreeburning. Blood-loss was notably reduced comparedwith that expected for ordinary scalpel excision, andthe fact that autografts " took " readily is an indica-tion of the absence of significant damage to under-lying tissue.
* Present address: Department of Neurosurgery, St. Barnabas MedicalCenter, Livingston, New Jersey, U.S.A.
EXTENSIVE third-degree burning is always veryserious and often lethal. Much of the resultant
morbidity and mortality is due to infection originatingin the irreparably damaged tissue. So long as de-vitalised tissue is present, infection is a threat.Although local antibiotic and chemotherapeutic agentshave helped reduce bacterial colonisation and infec-tion of the burned tissue, sepsis remains the principalcause of death in patients with extensive third-degreeburns. Recovery and return of function in these
patients is contingent on the earliest safe removal ofthe burn eschar and skin grafting. Because spon-taneous sloughing of the deeply burned skin generallyrequires 21-35 days, early surgical excision of theeschar and skin grafting have been advocated. Whenthe deep burn is extensive, this procedure involvesprolonged anaesthesia and massive blood-loss and
replacement (up to 40 units of whole blood for a singlepatient). We have investigated the use of lasers forthe excision of third-degree burns.We were able to reduce the blood-loss accompanying
the excision of deeply burned skin by excising theburn eschar with a continuous-wave carbon-dioxidelaser (10-6 IL wavelength), which coagulates promptlysmall blood-vessels in the plane of excision withoutsignificantly damaging the underlying tissue. Skin
grafting could be done immediately and successfully.Our experiments were done on 3-month-old
Hampshire-Landrace pigs and have ranged from theexcisions of small, circular, 5 cm. diameter, standard-ised third-degree contact burns to large (23 x 28 cm.)third-degree areas. Eschar was excised asepticallyunder pentobarbitone anxsthesia 24 hours after theburn injury. Experiments in which blood-loss wasmeasured have shown that the laser excisions resultin less than 5% of the blood-loss encountered whencomparable areas are excised with the ordinaryscalpel.Excision of burn slough, by whatever means, must
damage the underlying tissue as little as possible. Thecritical test of the condition of the tissue at the baseof the wound is its ability to accept an immediatelyapplied skin autograft. In pigs undergoing laser
excisions of large third-degree burns (from 18 x 23 cm.to 23 x 28 cm.), the " takes " of immediately appliedautografts (0-002 in. thick) have been from 90% to100%. The grafts have become vascularised promptlyand have persisted intact during the 2 months ofobservation post-operatively. So far we have seen no
gross evidence of systemic toxicity due to our use ofthe laser in removing burn eschars of up to 20% totalbody-surface area of the pigs.The laser thus seems to be a promising instrument
for the excision of third-degree burn eschars. It offersthe advantage of reducing blood-loss without causingsignificant injury to the underlying tissue or noticeablesystemic toxicity. Autografts applied to a freshlylased surface show excellent " takes " and persist in anormal fashion.
Supported by grant from the Army Medical Research andDevelopment Command DADA 17-70-C to the Albert EinsteinCollege of Medicine, Yeshiva University and N.I.H. researchcareer award 5-K6-GM-14,208 to S. M. L. The laser waskindly provided by the American Optical Corporation ResearchLaboratory (Dr. Thomas Polany, and Mr. Herbert C. Bredmeier),Framingham, Massachusetts, U.S.A.
Requests for reprints should be addressed to S. S.
DIPHOSPHONATES AND PAGET’SDISEASE OF BONE
ROGER SMITH R. G. G. RUSSELLMARGARET BISHOP
Metabolic Unit, Nuffield Department of Orthopœdic Surgery,University of Oxford
Summary The diphosphonate, CH3C(OH)(PO3HNa)2 (disodium etidronate), has been
given at a daily oral dose of 20 mg. per kg. body-weightto 4 patients with biochemically active Paget’s disease.The increased alkaline phosphatase in plasma and theincreased hydroxyproline in plasma and urine fellsteadily to about half their initial value after threemonths’ treatment. This suggests that the diphosphon-ate reduces the excessive bone turnover in this disease.
Introduction
IN Paget’s disease of bone there is excess resorptionand disorderly formation of bone which often resultsin severe deformities. Biochemical changes include anincrease above normal in plasma-alkaline-phosphataseand in urinary total hydroxyproline (T.H.P.). Sub-stances recently used in the medical treatment of thiscondition include calcitonin, 1,2 which inhibits boneresorption, and mithramycin,3 which is a cytotoxicagent. Both appear to relieve bone pain and to reduceplasma-alkaline-phosphatase and urinary T.H.P. Both
agents have to be administered by injection. Mithra-mycin, in particular, has serious side-effects. The
diphosphonate compounds 4,6 offer an alternative
approach to the therapy of Paget’s disease. Thesecompounds bind to hydroxyapatite crystals and in-hibit their growth and dissolution in vitro. 4-8 Inanimals certain diphosphonates inhibit bone resorp-tion 4,7 and, at higher doses, inhibit bone mineralisa-tion.8 They are also effective by mouth. It thereforeseemed logical to study their effect in Paget’s disease,
946
and we present here our preliminary findings in 4 suchpatients.
Methods
4 male patients (table i) were admitted to a metabolicward for two to six weeks before and at the start of treat-ment. They were on a constant low-gelatin diet and were notconfined to bed. After baseline measurements had beenmade, the diphosphonate CH3C(OH)(POsHNa)s (disodiumetidronate, ’ EHDP ’) was started at a single daily dose of20 mg. per kg. body-weight, given in tablet form with fruitjuice before breakfast. The drug was continued after dis-charge (one to four weeks after the first dose) from hospitaland the patients were seen every two weeks for biochemicaltests. Before each test they were on a low-gelatin diet forforty-eight hours and urine was collected during the secondtwenty-four-hour period. Blood was taken before breakfast(fasting) when the patients were in hospital and during theday (non-fasting) when they were outpatients.Analytical Methods
Standard laboratory methods were used for calcium(atomic absorption spectroscopy, Perkin Elmer 290B),phosphorus 9 and alkaline phosphatase.10 Total urinaryhydroxyproline was measured after hydrolysis by a modifi-cation of the method of Prockop and U denfriend. 11 Plasma-hydroxyproline was measured after ethanol precipitationof the plasma-proteins 12; the values given therefore includethe free and most of the peptide-bound hydroxyproline.The normal upper limit of urinary T.H.P. is taken as
50 mg. per twenty-four hours, 13 and that of plasma-hydroxyproline as 2-5 mg. per litre (personal data). Twenty-four hour urine collections were judged to be complete onthe basis of repeated measurements of urinary creatinine.
Results
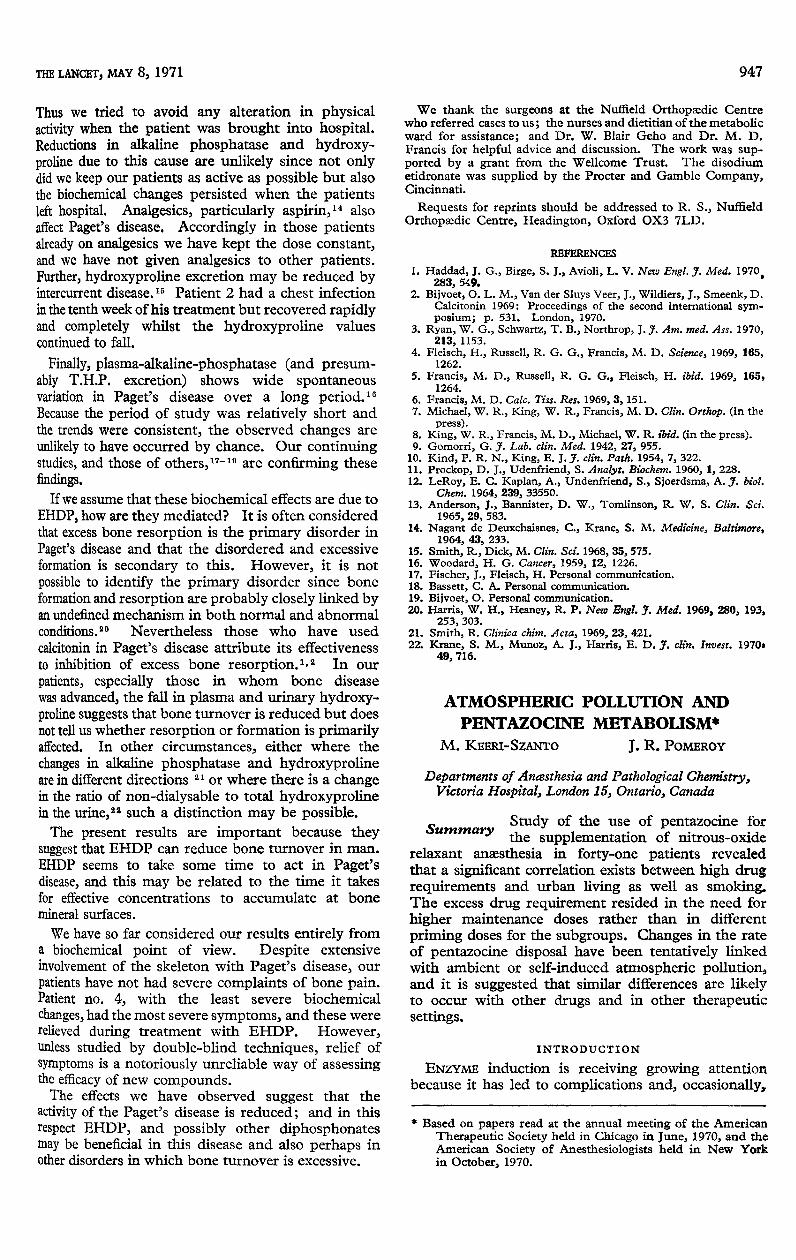
In table i the cases are arranged in order of study.The initial biochemical results are the mean of threemeasurements on separate days before treatment.
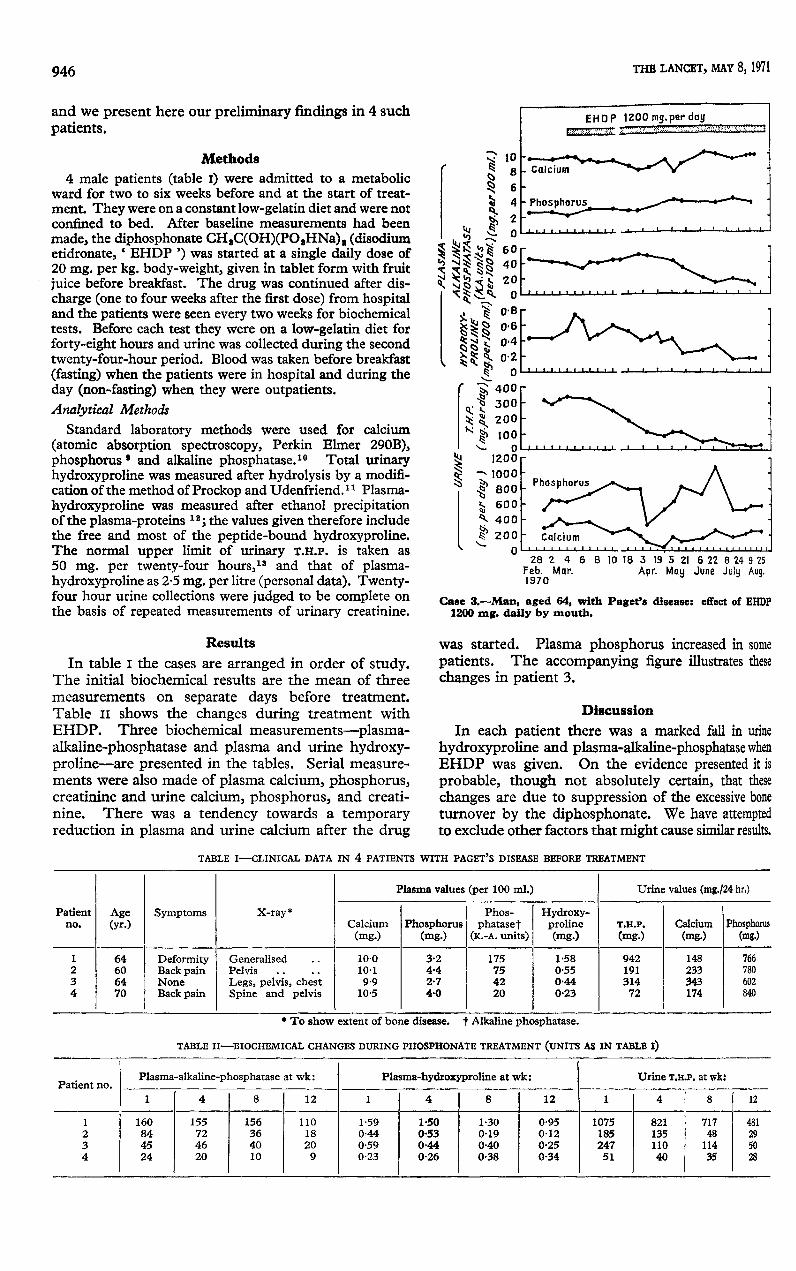
Table II shows the changes during treatment withEHDP. Three biochemical measurements-plasma-alkaline-phosphatase and plasma and urine hydroxy-proline-are presented in the tables. Serial measure-ments were also made of plasma calcium, phosphorus,creatinine and urine calcium, phosphorus, and creati-nine. There was a tendency towards a temporaryreduction in plasma and urine calcium after the drug
Case 3.-Man, aged 64, with Paget’s disease : effect of EHDP1200 mg. daily by mouth.
was started. Plasma phosphorus increased in somepatients. The accompanying figure illustrates thesechanges in patient 3.
Discussion
In each patient there was a marked fall in urinehydroxyproline and plasma-alkaline-phosphatase whenEHDP was given. On the evidence presented it is
probable, though not absolutely certain, that these
changes are due to suppression of the excessive boneturnover by the diphosphonate. We have attemptedto exclude other factors that might cause similar results.
TABLE I-CLINICAL DATA IN 4 PATIENTS WITH PAGET’S DISEASE BEFORE TREATMENT
. To show extent of bone disease. t Alkaline phosphatase.
TABLE II-BIOCHEMICAL CHANGES DURING PHOSPHONATE TREATMENT (UNITS AS IN TABLE I)
947
Thus we tried to avoid any alteration in physicalactivity when the patient was brought into hospital.Reductions in alkaline phosphatase and hydroxy-proline due to this cause are unlikely since not onlydid we keep our patients as active as possible but alsothe biochemical changes persisted when the patientsleft hospital. Analgesics, particularly aspirin,14 alsoaffect Paget’s disease. Accordingly in those patientsalready on analgesics we have kept the dose constant,and we have not given analgesics to other patients.Further, hydroxyproline excretion may be reduced byintercurrent disease. 16 Patient 2 had a chest infectionin the tenth week of his treatment but recovered rapidlyand completely whilst the hydroxyproline valuescontinued to fall.
Finally, plasma-alkaline-phosphatase (and presum-ably T.H.P. excretion) shows wide spontaneousvariation in Paget’s disease over a long period. 16 eBecause the period of study was relatively short andthe trends were consistent, the observed changes areunlikely to have occurred by chance. Our continuingstudies, and those of others, 11-19 are confirming thesefindings.
If we assume that these biochemical effects are due to
EHDP, how are they mediated? It is often consideredthat excess bone resorption is the primary disorder inPaget’s disease and that the disordered and excessiveformation is secondary to this. However, it is notpossible to identify the primary disorder since boneformation and resorption are probably closely linked byan undefined mechanism in both normal and abnormalconditions."" Nevertheless those who have usedcalcitonin in Paget’s disease attribute its effectivenessto inhibition of excess bone resorption. 1, 2 In our
patients, especially those in whom bone diseasewas advanced, the fall in plasma and urinary hydroxy-proline suggests that bone turnover is reduced but doesnot tell us whether resorption or formation is primarilyaffected. In other circumstances, either where the
changes in alkaline phosphatase and hydroxyprolineare in different directions 21 or where there is a changein the ratio of non-dialysable to total hydroxyprolinein the urine,22 such a distinction may be possible.The present results are important because they
suggest that EHDP can reduce bone turnover in man.EHDP seems to take some time to act in Paget’sdisease, and this may be related to the time it takesfor effective concentrations to accumulate at bonemineral surfaces.
We have so far considered our results entirely froma biochemical point of view. Despite extensiveinvolvement of the skeleton with Paget’s disease, ourpatients have not had severe complaints of bone pain.Patient no. 4, with the least severe biochemicalchanges, had the most severe symptoms, and these wererelieved during treatment with EHDP. However,unless studied by double-blind techniques, relief ofsymptoms is a notoriously unreliable way of assessingthe efficacy of new compounds.The effects we have observed suggest that the
activity of the Paget’s disease is reduced; and in thisrespect EHDP, and possibly other diphosphonatesmay be beneficial in this disease and also perhaps inother disorders in which bone turnover is excessive.
We thank the surgeons at the Nuffield Orthopardic Centrewho referred cases to us; the nurses and dietitian of the metabolicward for assistance; and Dr. W. Blair Geho and Dr. M. D.Francis for helpful advice and discussion. The work was sup-ported by a grant from the Wellcome Trust. The disodiumetidronate was supplied by the Procter and Gamble Company,Cincinnati.
Requests for reprints should be addressed to R. S., NuffieldOrthopaedic Centre, Headington, Oxford OX3 7LD.
REFERENCES
1. Haddad, J. G., Birge, S. J., Avioli, L. V. New Engl. J. Med. 1970283, 549.
2. Bijvoet, O. L. M., Van der Sluys Veer, J., Wildiers, J., Smeenk, D.Calcitonin 1969: Proceedings of the second international sym-posium; p. 531. London, 1970.
3. Ryan, W. G., Schwartz, T. B., Northrop, J. J. Am. med. Ass. 1970,213, 1153.
4. Fleisch, H., Russell, R. G. G., Francis, M. D. Science, 1969, 165,1262.
5. Francis, M. D., Russell, R. G. G., Fleisch, H. ibid. 1969, 165,1264.
6. Francis, M. D. Calc. Tiss. Res. 1969, 3, 151.7. Michael, W. R., King, W. R., Francis, M. D. Clin. Orthop. (in the
press).8. King, W. R., Francis, M. D., Michael, W. R. ibid. (in the press).9. Gomorri, G. J. Lab. clin. Med. 1942, 27, 955.
10. Kind, P. R. N., King, E. J. J. clin. Path. 1954, 7, 322.11. Prockop, D. J., Udenfriend, S. Analyt. Biochem. 1960, 1, 228.12. LeRoy, E. C. Kaplan, A., Undenfriend, S., Sjoerdsma, A. J. biol.
Chem. 1964, 239, 33550.13. Anderson, J., Bannister, D. W., Tomlinson, R. W. S. Clin. Sci.
1965, 29, 583.14. Nagant de Deuxchaisnes, C., Krane, S. M. Medicine, Baltimore,
1964, 43, 233.15. Smith, R., Dick, M. Clin. Sci. 1968, 35, 575.16. Woodard, H. G. Cancer, 1959, 12, 1226.17. Fischer, J., Fleisch, H. Personal communication.18. Bassett, C. A. Personal communication.19. Bijvoet, O. Personal communication.20. Harris, W. H., Heaney, R. P. New Engl. J. Med. 1969, 280, 193,
253, 303.21. Smith, R. Clinica chim. Acta, 1969, 23, 421.22. Krane, S. M., Munoz, A. J., Harris, E. D. J. clin. Invest. 1970,
49, 716.
ATMOSPHERIC POLLUTION AND
PENTAZOCINE METABOLISM*M. KEERI-SZANTO J. R. POMEROY
Departments of Anœsthesia and Pathological Chemistry,Victoria Hospital, London 15, Ontario, Canada
Summary Study of the use of pentazocine forthe supplementation of nitrous-oxide
relaxant anæsthesia in forty-one patients revealedthat a significant correlation exists between high drugrequirements and urban living as well as smoking.The excess drug requirement resided in the need forhigher maintenance doses rather than in different
priming doses for the subgroups. Changes in the rateof pentazocine disposal have been tentatively linkedwith ambient or self-induced atmospheric pollution,and it is suggested that similar differences are likelyto occur with other drugs and in other therapeuticsettings.
* Based on papers read at the annual meeting of the AmericanTherapeutic Society held in Chicago in June, 1970, and theAmerican Society of Anesthesiologists held in New Yorkin October, 1970.
INTRODUCTION
ENZYME induction is receiving growing attentionbecause it has led to complications and, occasionally,





























