Embed Size (px)
Citation preview

Differentiation of poorly differentiated colorectaladenocarcinomas from well- or moderatelydifferentiated colorectal adenocarcinomas atcontrast-enhanced multidetector CT
Ji Eun Kim,1 Jeong Min Lee,2 Jee Hyun Baek,2 Sung Kyung Moon,3 Se Hyung Kim,2
Joon Koo Han,2 Byung Ihn Choi2
1Department of Radiology, Gyeongsang National University School of Medicine, Jinju, Korea2Department of Radiology and Institute of Radiation Medicine, Seoul National University College of Medicine, Seoul National
University Hospital, 28 Yongon-dong, Chongno-gu, Seoul 110-744, Korea3Department of Radiology, Kyung Hee University College of Medicine, Seoul, Korea
Abstract
Purpose: The purpose of the study is to describe the CTfindings of poorly differentiated (PD) colorectal adeno-carcinoma (CRAC) compared with those of well- (WD)or moderately differentiated (MD) CRAC.Materials and methods: One hundred and thirteenpatients with pathologically proven PD (n = 26), WD(n = 35), or MD (n = 52) CRACs and who hadundergone preoperative, contrast-enhanced multidetec-tor CT (MDCT) imaging were included. Analysis of theCT findings included the morphologic and enhancementfeatures of primary tumors and regional lymph nodes(LNs), and the presence of direct invasion, colonicobstruction, and distant metastasis. The significance ofthese findings was determined using the v2 test.Results: Significant features favoring the diagnosis of PDCRACs over WD or MD CRACs included their bulkyshape, heterogeneous enhancement, iso- or hypoattenu-ation compared with that of muscle, nodular pericolic fatinfiltration, regional LNs > 10 mm, and/or with iso- orhypoattenuation compared with that of muscle, and thepresence of distant metastasis (P < 0.05). When at leasttwo of these seven imaging features were used incombination, the sensitivity and specificity in the diag-nosis of PD CRACs were 88% and 70%, respectively.Conclusion: Using characteristic CT features, one candifferentiate PD CRAC from WD or MD CRAC with ahigh degree of accuracy on contrast-enhanced MDCT.
Key words: Poorly differentiated (PD)—Colorectaladenocarcinoma (CRAC)—Multidetector CT (MDCT)
Colorectal cancer (CRC) is the fourth most commonmalignancy and is the second leading cause of cancer-related mortality in the United States [1]. Accurate pre-operative staging is the most essential step for deter-mining the optimal treatment option and surgicalplanning for patients with CRC. Multidetector CT(MDCT) is currently the preoperative imaging modalityof choice for CRC staging, particularly in patients withT2 or higher stage cancers [2], whereas high-resolutionmagnetic resonance imaging plays a pivotal role in thepretreatment assessment of rectal cancer [3]. In additionto TNM staging, previous studies have shown thatcolorectal adenocarcinomas (CRACs) show differentprognoses according to the histologic grade based ontumor differentiation. Although the frequency of poorlydifferentiated (PD) CRAC is low, i.e. ranging from 3.3%
to 18% of all CRCs [4, 5], their prognosis is typicallyreported to be poor and more unfavorable than that ofwell-differentiated (WD) or moderately differentiated(MD) CRACs [6–9]. As colonoscopic biopsy is usuallyperformed for diagnosing CRCs before beginning treat-ment, pathologic evaluation of these biopsy samples mayprovide information regarding tumor differentiation.However, biopsy has some limitations for evaluatingtumor grades due to the following reasons: (1) ThereCorrespondence to: Jeong Min Lee; email: [email protected]
ª Springer Science+Business Media New York 2014
AbdominalImaging
Abdom Imaging (2014)
DOI: 10.1007/s00261-014-0176-z

could be a discrepancy between the biopsy and resectedspecimen due to sampling bias or tumor heterogeneity;and (2) Histologic grading may make it difficult to makeobjective judgments, especially when the grading is per-formed in biopsy-obtained material [10]. Therefore, dif-ferentiating PD CRACs from WD or MD CRACs onpreoperative imaging may define subsets of patients whohave a worse prognosis and are more likely to developtumor recurrence, which might lead to the more rationalapplication of adjuvant chemotherapy and possible fu-ture neoadjuvant chemotherapy. Previous study of CTcolonography in 29 patients with colorectal neoplasmsdemonstrated that the degree of enhancement did notcorrelate with degree of histologic differentiation [14];however, to date, no studies have been performed toassess the imaging features of CRACs such as tumormorphology, attenuation, and enhancement pattern onMDCT according to the tumor differentiation in largestudy population including sufficient number of PDCRACs. Therefore, the purpose of this study was todescribe the CT findings of PD CRACs and to identifythe features that differentiate it from WD or MDCRACs.
Materials and methods
Patients
Our institutional review board approved this retrospec-tive study and waived the requirement for informedconsent. We performed a computerized search of ourhospital’s pathology database from April 2006 to April2009 using the search terms, colorectal carcinoma andcolectomy or resection. This search identified 1105 pa-tients with histopathologically proven colorectal carci-nomas, who had undergone curative or palliative surgeryat our hospital. We then used the following inclusioncriteria: (a) patients had to have undergone preoperativecontrast-enhanced MDCT examination, including portalvenous (PV) phase scanning, within 2 months prior totheir surgery at our hospital; (b) patients had to havereceived a diagnosis of PD, WD, or MD CRAC onhistopathologic examination of their surgical specimen;and (c) patients had to have not received preoperativechemotherapy or radiation therapy. Three hundred andeighty-six patients of the total 1105 patients wereexcluded from our study because they did not havepreoperative PV phase CT scan data (n = 66), thepreoperative CT scan had been checked more than2 months prior to surgery (n = 44) or they had receiveda histopathologic diagnosis other than that of colorectaladenocarcinoma (n = 276, mucinous carcinomas[n = 218], signet-ring cell carcinomas [n = 34], andother rare carcinomas such as medullary, adenosqua-mous, spindle-cell, or undifferentiated carcinomas[n = 24]). Then, among 719 patients with CRAC (WD[n = 279], MD [n = 414] or PD [n = 26] CRACs), 35
patients with WD CRACs and 52 patients with MDCRACs were selected in our study, after matching theirage and sex distribution with those of patients who hadreceived a diagnosis of PD CRAC. Finally, 113 patientswith an overall mean age of 62 years ± 12 (standarddeviation) (overall age range, 26–83 years; 44 males;mean male age, 61 years ± 14; age range of males,26–82 years; 69 females; mean female age, 62 years ± 11;age range of females 33–83 years) were included in ourretrospective study.
All of these patients had undergone curative or pal-liative surgery for their CRAC (right hemicolectomy[n = 55], left hemicolectomy [n = 4], anterior resection[n = 49]), total colectomy [n = 4], and segmentalresection [n = 1]) and had received a histopathologicdiagnosis of adenocarcinoma of the colorectum withassigned tumor grades based on the tumor differentiationin the TNM classification [12], i.e., grade 1 is defined asWD, grade 2 as MD, grade 3 as PD, and grade 4 asundifferentiated. Tumor grade was assessed based on theleast differentiated component according to the WorldHealth Organization classification [13]. Forty-fourpatients had lesions located in the right colon includingthe cecum, ascending colon, and hepatic flexure colon, 14had lesions located in the transverse colon, four hadlesions located in the descending colon, 46 had lesionslocated in the sigmoid colon, four had lesions located inthe rectosigmoid junction, and one had a lesion locatedin the upper rectum. According to the classificationsystem of the American Joint Committee on Cancer,seventh edition [14], the tumor stage was T1 for six (5%)cancers, T2 for eight (7%) cancers, T3 for 71 (63%)cancers, and T4 for 28 (25%) cancers. The node stage wasN0 for 32 (28%) cancers, N1 for 25 (22%) cancers, andN2 for 56 (50%) cancers. The metastasis stage was M0for 81 (72%) cancers and M1 for 32 (28%) cancers. Theclinicopathologic data are shown in Table 1.
Acquisition of CT images
Thirty-nine patients underwent single-phase CT duringthe PV phase, and 74 patients underwent dual-phase CTduring the late arterial and PV phases. CT was per-formed at our medical institution using the following CTscanners: MX 8000 four-channel scanner (MarconiMedical Systems, Cleveland, OH, USA) for 10 patients,LightSpeed Ultra eight-channel scanner (GE Healthcare,Milwaukee, WI, USA) for 13 patients, Sensation 1616-channel scanner (Siemens Medical Solutions, Erlangen,Germany) for 47 patients, and Brilliance 64 64-channelscanner (Philips Healthcare, Cleveland, OH, USA) for 43patients. For 4-, 8-, 16-, and 64-detector CT examina-tions, detector collimations of 2.5, 1.25, 0.75, and0.625 mm, respectively, were used. A section thickness of3.0–3.2 mm with a 3-mm reconstruction interval, a fieldof view of 300–370 mm, a gantry rotation time of 0.5 s,
J. E. Kim et al.: Differentiation of poorly differentiated colorectal adenocarcinomas

an effective amperage setting of 150–200 mAs, and apeak voltage of 120 kVp were used for all CT scanners.
For dynamic phase imaging, a fixed dose of 1.5 ml ofnonionic contrast material (iopromide [370 mg of iodineper milliliter], Ultravist 370; Schering, Berlin, Germany)per kilogram of body weight (555 mgI/kg) was injectedinto an antecubital vein at a rate of 2.0–4.0 mL/sec usinga power injector (Multilevel CT; Medrad, Indianola, PA,USA). The scanning delay for the late arterial phase was17 s for the 4–16 channel CT scanner and 19 s for the 64-channel CT scanner after achieving enhancement of thedescending aorta of up to 100 HU, as measured by anautomatic bolus-tracking technique provided by themanufacturer of each CT scanner. The PV phase scanswere obtained 70 s after the contrast material adminis-tration.
Imaging analysis
A consensus review of all images was performed on apicture archiving and communication system worksta-tion monitor (m-view; Marotech, Seoul, Korea) by two,attending, body radiologists (J.H.B. and S.K.M., with sixand 5 years, respectively, of clinical experience) whointerpreted abdominal CT images of the gastrointestinalsystem as part of their daily clinical and research prac-tice. They were blinded to the histopathologic diagnosisof the colorectal lesions regarding cellular differentiationand TNM staging, although they were aware that all
patients had a presumptive diagnosis of CRACs. Theimages were presented to the readers in random orderand were thus reviewed. All of the reconstructed multi-planar reformation images, including coronal and/orsagittal image sets, as well as axial image sets, werereviewed. To reduce the learning bias, a set of sampleimages representing CT findings to be analyzed, butwhich were not included in the study population, werefirst shown to the readers. Discrepancies were resolvedduring a third analysis session during which a decisionwas reached by consensus of the two radiologists.
Analysis of the CT findings included evaluation of the(a) location and shape of the tumor; (b) enhancementpattern and degree of the tumor; (c) pericolic fat infil-tration; (d) size and enhancement degree of the regionallymph nodes (LNs); and (e) the presence of direct inva-sion, colonic obstruction, and distant metastasis. Thetumor locations were classified as involving the rightcolon including the cecum, ascending and hepatic flexurecolon, transverse colon, left colon including the splenicflexure colon and descending colon, sigmoid colon, andrectosigmoid junction or rectum. Tumor shapes wereclassified as intraluminal polypoid mass, ulcerofungat-ing/ulceroinfiltrative, or bulky. If the tumor was asmooth marginated, protruding mass into the coloniclumen with a sharp line dividing it from the adjacentnormal colorectal wall, and the wall of the tumor-bearingsegment was seen as the same as that of the adjacent,normal colorectal wall, then it was considered to be an
Table 1. Clinicopathologic findings of 113 CRACs
Finding PD CRAC (n = 26) WD CRAC (n = 35) MD CRAC (n = 52)
Mean age (years) 63 61 62Male:Female patient ratio 11:15 15:20 18:34Tumor location
Right colon (Cecum, AC, and HF) 12 (46) 12 (34) 20 (38)Transverse colon 5 (19) 3 (9) 6 (12)Left colon (SF and DC) 2 (8) 0 2 (4)Sigmoid colon 7 (27) 16 (46) 23 (44)Rectosigmoid junction 0 3 (9) 1 (2)Upper rectum 0 1 (3) 0
Surgical procedureRight hemicolectomy 16 (62) 14 (40) 25 (48)Left hemicolectomy 1 (4) 0 3 (6)Anterior resection 6 (23) 20 (57) 23 (44)Total colectomy 3 (11) 0 1 (2)Segmental resection 0 1 (3) 0
Tumor stageT1 0 6 (17) 0T2 1 (4) 7 (20) 0T3 12 (46) 22 (63) 37 (71)T4 13 (50) 0 15 (29)
Node stageN0 3 (12) 25 (71) 4 (8)N1 5 (19) 9 (26) 11 (21)N2 18 (69) 1 (3) 37 (71)
Distant metastasisM0 14 (54) 32 (91) 35 (67)M1 12 (46) 3 (9) 17 (33)
Data are numbers of patients, with percentages in parenthesesAC, ascending colon; HF, hepatic flexure colon; SF, splenic flexure colon; DC, descending colon
J. E. Kim et al.: Differentiation of poorly differentiated colorectal adenocarcinomas

intraluminal polypoid mass [15]. If the tumor was a wall-thickening mass with a height-to-width ratio of <1, thenit was considered to be a ulcerofungating or ulceroinfil-trative mass [2, 10, 16]. When the outer diameter of thetumor-bearing segment was larger than the outer diam-eter of the expected, adjacent, normal well- or partiallydistended colorectal segment (not exceeding 9 cm indiameter in the cecum, 6 cm in other segments of thecolorectum) and the tumor showed an exophytic com-ponent which was defined as disproportionately expan-sile growth (>1 cm) outer to the imaginary line of theouter wall of most of the tumor, it was considered to be abulky mass (Fig. 1).
The tumor enhancement pattern was first evaluatedregarding its homogeneity, i.e., homogeneous vs. heter-ogeneous. Then, the relative degree of enhancement, i.e.,higher attenuation to the liver, attenuation between thatof the liver and muscle, or the same or lower attenuationto the muscle, of the lesion compared with theenhancement of the hepatic parenchyma and muscle, wasevaluated in the PV phase scan. When the tumor wascomposed of an inner layer with higher attenuation tothe liver and an outer layer with attenuation betweenthat of the liver and muscle, it was considered to have alayering pattern. Pericolic fat infiltration was assessed interms of whether it had no, hazy, linear, or nodular
infiltration in the mesentery adjacent to the tumor-bearing colorectal segment. If the peritumoral mesenteryshowed the same appearance as the adjacent, normal,homogeneous, intra-abdominal fat, then it was consid-ered not to be pericolic fat infiltration (Fig. 2A). If therewas ill-defined, slightly increased density in the peritu-moral mesentery, then it was considered to be hazy(Fig. 2B). If there was well-defined, increased density ofa linear configuration in the peritumoral mesentery, thenit was considered to be linear (Fig. 2C). When the well-defined, increased density in the peritumoral mesenterythat is continuous with the primary tumor showed anodular configuration, it was considered to be nodular(Fig. 2D). If different types of fat infiltration were ob-served around the CRAC, we chose the type of fatinfiltration showing a thicker and denser component andthereby being considered to represent more severe localtumor extension, i.e., hazy < linear < nodular.
The size of the regional LNs according to the short-axis diameter was classified as no visible LNs, <5, 5 to10 mm or more than 10 mm. The degree of enhancementof regional LNs during the PV phase was assessed inorder to determine whether the same or lower attenua-tion compared with that of the muscle was seen withinthe regional LNs. Regional LNs were defined as nodeslocated along the course of the major vessels supplyingthe tumor-bearing colorectum, along the vasculararcades of the marginal artery, and along the mesocolicborder of the colon [14]. The presence or absence ofdirect invasion to other organs or structures as well ascolonic obstruction and distant metastasis were alsoevaluated on the CT images. In order to objectivelyassess the bulky component of a tumor, a third radiologistwith five years of clinical experience reading gastroin-testinal CT imaging (J.E.K.) measured the maximumwall thickness of the tumor on the PV phase imageshowing the largest cross-sectional tumor profile withoutclinical or pathology information. Intraluminal polypoidmasses were excluded from the measurement of maxi-mum wall thickness as they had been designated as notinvolving the colorectal wall during the qualitative imageanalysis.
Statistical analysis
The results of the image review were compared for PDCRACs and WD or MD CRACs. Categorical variableswere expressed as counts and proportions. The v2 testwas used to compare the categorical variables of interestin PD CRACs and WD or MD CRACs. The quantita-tive variable was expressed as the mean ± standarddeviation. The t test was used to compare the maximumwall thickness in the three types of CRACs. A P value<0.05 was considered to indicate a significant difference,and a 95% confidence interval (CI) was reported for each
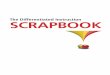
Fig. 1. Illustration showing the ‘‘bulky shape’’ of the tumor.When the outer diameter (red arrow) of the tumor-bearingsegment (T) was larger than the outer diameter (gray arrow)of the expected, adjacent, normal well- or partially distendedcolorectal segment (not exceeding 9 cm in diameter in thececum and 6 cm in other segments of the colorectum) (N),and the tumor showed an exophytic component which wasdefined as disproportionately expansile growth (>1 cm) outerto the imaginary line (dotted line) of the outer wall of most ofthe tumor, it was considered to have a bulky shape.
J. E. Kim et al.: Differentiation of poorly differentiated colorectal adenocarcinomas

significant variable. The odds ratios (with 95% CIs) forthe differentiation of PD CRACs from WD or MDCRACs were calculated for each CT criterion. The sen-sitivity and specificity of each significant CT criterionand a combination of significant CT criteria were alsocalculated. Statistical analysis was performed usingMedCalc software (MedCalc for Windows, version12.7.0; Ostend, Belgium).
Results
Imaging analysis
The results of the CT findings are summarized inTable 2. With regard to lesion shape, 11 (42%) of the 26PD CRACs were bulky lesions, whereas 20 (57%) of the35 WD CRACs and 51 (98%) of 52 MD CRACs wereulcerofungating or ulceroinfiltrative lesions (Figs. 3, 4, 5,
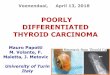
Fig. 2. Analyzed types of pericolic fat infiltration. A No per-icolic fat infiltration was defined as when peritumoral mesen-tery has the same appearance as the adjacent, normal,homogeneous, intra-abdominal fat (arrows). B Hazy pericolicfat infiltration was defined as when there is ill-defined, slightlyincreased density in the peritumoral mesentery (arrows). C
Linear pericolic fat infiltration was defined as when there iswell-defined, increased density of a linear configuration in theperitumoral mesentery (arrows). D Nodular pericolic fat infil-tration was defined as when the well-defined, increaseddensity that is continuous with the primary tumor shows anodular configuration (arrows).
J. E. Kim et al.: Differentiation of poorly differentiated colorectal adenocarcinomas

and 6) (P < 0.0001). Most WD (n = 30, 86%) and MD(n = 41, 79%) CRACs showed homogenous enhance-ment, while 17 (65%) of the 26 PD CRACs showedheterogeneous enhancement (Figs. 3 and 5)(P < 0.0001). Sixteen of the 26 PD CRACs (62%) hadattenuation similar to or lower than that of muscleduring the PV phase; however, 30 (86%) of the 35 WDCRACs and 34 (65%) of the 52 MD CRACs hadattenuation between that of the liver and muscle (Figs. 4and 6) (P < 0.0001). PD CRACs showed a greatermaximal wall thickness than WD or MD CRACs(21.0 ± 9.4 vs. 17.9 ± 5.8 vs. 13.6 ± 3.6, P < 0.001). Interms of the pericolic fat infiltration, 17 (65%) of the 26PD CRACs were nodular; however, only six (17%) of the35 WD CRACs and 16 (31%) of the 52 MD CRACs werenodular (P = 0.0019). Most of the PD CRACs (n = 19,73%) showed regional LNs more than 10 mm in theirshort-axis diameter (Figs. 3 and 4), whereas this was onlyevident in four (11%) of the 35 WD CRACs and in 12
(23%) of the 52 MD CRACs (P < 0.0001). With regardto the degree of enhancement of the regional LNs duringthe PV phase, 18 of the 26 PD CRACs (69%) hadregional LNs with the same or lower attenuation comparedwith that of the muscle (Figs. 3 and 4); however, three(9%) of the 35 WD CRACs and 17 (33%) of the 52 MDCRACs had such LNs (P = 0.0002). Finally, 12 (46%)of the 26 PD CRACs showed distant metastasis, whilethis was only evident in three (9%) WD CRACs and in 17(33%) MD CRACs (P = 0.0401). The presence of directinvasion and colonic obstruction did not differ signifi-cantly between the PD CRACs and WD or the MDCRACs (P > 0.05).
Sensitivity and specificity for the CT diagnosis
Table 3 summarizes the sensitivity and specificity of eachsignificant CT criterion in the differentiation of PDCRACs from WD or MD CRACs. The highest odds
Table 2. CT Findings in PD CRACs and WD or MD CRACs
Finding PD CRAC (n = 26) WD CRAC (n = 35) MD CRAC (n = 52) P value*
Tumor shape <0.0001Intraluminal polypoid mass 0 11(31) 0Ulcerofungating/ulceroinfiltrative mass 15 (58) 20 (57) 51 (98)Bulky 11 (42) 4 (11) 1 (2)
Enhancement pattern of the tumor <0.0001Homogeneous 9 (35) 30 (86) 41 (79)Heterogeneous 17 (65) 5 (14) 11 (21)
Enhancement degree of the tumor during the PVP <0.0001Higher attenuation compared with that of the liver 0 0 1 (2)Attenuation between that of the liver and muscle 5 (19) 30 (86) 34 (65)The same or lower attenuation compared with that of the muscle 16 (62) 5 (14) 13 (25)Layering pattern 5 (19) 0 4 (8)
Maximal wall thickness (mm)� 21.0 ± 9.4 17.9 ± 5.8 13.6 ± 3.6 <0.001§
Pericolic fat infiltration 0.0019No 2 (8) 10 (29) 2 (4)Hazy 5 (19) 12 (34) 15 (29)Linear 2 (8) 7 (20) 19 (37)Nodular 17 (65) 6 (17) 16 (31)
Size of regional LNs <.0001No visible LNs 1 (4) 11 (31) 3 (6)<5 mm 0 5 (14) 7 (13)5–10 mm 6 (23) 16 (46) 30 (58)More than 10 mm 19 (73) 4 (11) 12 (23)
Enhancement degree of the regional LNs during the PVP 0.0002The same or lower attenuation compared with that of the musclePresent 18 (69) 3 (9) 17 (33)Absent 7 (27) 21 (60) 32 (62)No visible LNs 1 (4) 11 (31) 3 (6)
Direct invasion 0.0615Present 8 (31) 3 (9) 8 (15)Absent 18 (69) 32 (91) 44 (85)
Colonic obstruction 0.5285Present 1 (4) 2 (6) 7 (13)Absent 25 (96) 33 (94) 45 (87)
Distant metastasis .0401Present 12 (46) 3 (9) 17 (33)Absent 14 (54) 32 (91) 35 (67)
Data are numbers of patients, with percentages in parentheses* Between PD CRACs and WD or MD CRACs; calculated with the v2 test�Mean maximal wall thickness ± standard deviation§Among the three types of CRACs; calculated with the t testPVP, portal venous phase; LN, lymph nodes
J. E. Kim et al.: Differentiation of poorly differentiated colorectal adenocarcinomas

ratio was achieved with the same or lower attenuationcompared with that of muscle within the tumor (12.409,95% CI 4.178–36.855) followed by the regional LNsmore than 10 mm in their short-axis diameter (12.045,95% CI 4.333–33.481), bulky shape (12.027, 95% CI
Fig. 4. Poorly differentiated (PD) colon adenocarcinoma in a68-year-old male. On axial contrast-enhanced MDCT image ob-tained during the portal venous phase, a bulky mass involving theproximalascendingcolondemonstratesattenuationsimilar to thatof the muscle. The maximum wall thickness (inner to outer wall) ofthe tumor was 45 mm (yellow, dotted arrow). The mass isaccompanied by hazy pericolic fat infiltration and abuts the adja-cent small bowel (white arrow). In the adjacent mesocolon, lymphnodes more than 10 mm in short-axis diameter are seen and theyshow the same attenuation as the tumor (red arrow). The histo-pathologic tumor and node stage were T3 and N2a, respectively.
Fig. 5. Moderately differentiated (MD) colon adenocarci-noma in a 61-year-old male. On axial portal venous phaseMDCT image, a homogenous ulceroinfiltrative mass withattenuation between that of the liver and muscle involves thesigmoid colon. A pericolic lymph node with a short-axisdiameter of 5–10 mm and the same attenuation as the tumoris seen (arrow). The histopathologic tumor and node stagewere T3 and N2a, respectively.
Fig. 3. Poorly differentiated (PD) colon adenocarcinoma in a59-year-old male. Axial contrast-enhanced MDCT imageobtained during the portal venous phase shows a heteroge-nous bulky mass in the hepatic flexure colon. The maximumwall thickness of the tumor was measured from the inner wallto the outer wall, not including the central necrotic portion(yellow, dotted arrow). The tumor invades the adjacent jeju-num (white arrow). Conglomerated lymph nodes with thesame or lower attenuation compared with that of the muscleare seen in the adjacent mesocolon and small bowel mes-entery (red arrows). Liver metastasis was also present at thattime of diagnosis. The histopathologic tumor and node stagewere T4b and N2b, respectively.
Fig. 6. Well-differentiated (WD) colon adenocarcinoma in a60-year-old male. On axial portal venous phase MDCT image,an ulcerofungating mass between attenuation of the liver andmuscle involves the proximal ascending colon. The mass isaccompanied by linear pericolic fat infiltration. Several peri-colic lymph nodes of various sizes and with the same atten-uation as the tumor are seen (red arrows). Thehistopathologic tumor and node stage were T3 and N0,respectively.
J. E. Kim et al.: Differentiation of poorly differentiated colorectal adenocarcinomas

3.652–39.606), heterogeneous enhancement (8.382, 95%
CI 3.167–22.181), regional LNs with the same or lowerattenuation compared with that of muscle (6.814, 95% CI2.474–18.771), nodular pericolic fat infiltration (5.581,95% CI 2.177–14.309), and the presence of distantmetastasis (2.871, 95% CI 1.146–7.196).
When we used at least two of the seven significantcriteria in combination, we were able to identify PDCRACs in most patients (n = 23, 88%), but only 26(30%) of the 87 patients with WD or MD CRACs. Whenwe used any five of these criteria in combination, we wereable to exclude almost all of the patients with WD orMD CRACs (n = 83, 95%) (Table 4).
Discussion
Our study results show that seven CT findings, i.e.,bulky shape, heterogeneous enhancement, the same orlower attenuation compared with that of muscle withinthe tumor, nodular pericolic fat infiltration, regionalLNs more than 10 mm in their short-axis diameter,regional LNs with the same or lower attenuation com-pared with that of muscle, and the presence of distantmetastasis, are significant predictors in the differentia-tion of PD CRACs from WD or MD CRACs. Inaddition, when we used two or more of these MDCTfindings in combination as the diagnostic criteria for PD
CRACs, we were able to differentiate PD CRACs fromWD or MD CRACs with high diagnostic accuracy.Given that PD CRACs and WD or MD CRACs havedifferent biologic behavior and prognosis [6–9, 17, 18],characterization of the histologic grades of CRAC dur-ing the preoperative imaging workup may be clinicallyimportant for predicting a patient’s prognosis and mightbe useful for determining the optimal therapeutic strat-egy. Poor differentiation is associated with a high risk ofrelapse after surgical resection of stage II colon cancer,i.e., T3 or T4 N0M0 [18, 19]. Although the use ofadjuvant chemotherapy for patients with low-risk stageII colon cancer remains controversial, high-risk stage IIpatients—defined by the presence of either a T4, bowelobstruction, perforation, PD histology, or inadequateLN sampling—are routinely treated with adjuvant che-motherapy [19]. Furthermore, recent study has shownencouraging pathological responses after neoadjuvantchemotherapy in locally advanced colon cancer, whichwas defined by T3 with ‡5 mm invasion beyond themuscularis propria or T4 [20]. Another recent study hassuggested TN stages, extramural tumor and/or venousinvasion, and the distance from tumor to nearest ret-roperitoneal fascia as CT findings for selection of coloncancer patients for neoadjuvant chemotherapy [21].Considering that previous studies have reported that PDCRAC has a higher tendency to penetrate through thebowel wall, invade veins, and metastasize to LNs anddistant sites [4, 6, 22], PD histology might be additionalpotential criteria for determination of neoadjuvantchemotherapy of locally advanced colon cancer in thefuture. Although the histologic grades of CRAC can bedetermined by pathologic evaluation of preoperativebiopsy samples through endoscopic examination, biopsycan have an intrinsic limitation of sampling bias, espe-cially in large, ulcerated CRACs, and malignant tumorsmay have large heterogeneity in terms of tumor differ-entiation [23]. Furthermore, histologic grading has beencriticized due to its difficulty making objective assess-ment, especially when performed using biopsy material[10]. Therefore, if CT scanning, which is the standard ofcare for the imaging workup for CRC staging, canprovide useful information regarding tumor differentia-tion, then it will be useful for predicting a patient’s
Table 3. Sensitivity and specificity of CT findings in the differentiation of PD CRACs from WD or MD CRACs
CT Finding Sensitivity (%) Specificity (%) Odds ratio*
The same or lower attenuation compared with that of muscle within the tumor 81 (21/26) 75 (65/87) 12.409 (4.178, 36.855)Regional LNs more than 10 mm in short-axis diameter 73 (19/26) 82 (71/87) 12.045 (4.333, 33.481)Bulky shape 42 (11/26) 94 (82/87) 12.027 (3.652, 39.606)Heterogeneous enhancement 65 (17/26) 82 (71/87) 8.382 (3.167, 22.181)Regional LNs with the same or lower attenuation compared with that of muscle 72 (18/25) 73 (53/73) 6.814 (2.474, 18.771)Nodular pericolic fat infiltration 65 (17/26) 75 (65/87) 5.581 (2.177, 14.309)Presence of distant metastasis 46 (12/26) 77 (67/87) 2.871 (1.146, 7.196)
Unless otherwise specified, data in parentheses are numbers of patients* Data in parentheses represent 95% confidence intervals
Table 4. Combined CT findings in the differentiation of PD CRACsfrom WD or MD CRACs
No. ofCT findings
PDCRAC(n = 26)
WD or MDCRAC(n = 87)
1 25 (96) 51 (59)2 23 (88) 26 (30)3 21 (81) 18 (21)4 15 (58) 9 (10)5 10 (38) 4 (5)6 5 (19) 1 (1)7 1 (4) 0
Data are numbers of patients with one or more of the following findingson CT images: lesion had the same or lower attenuation compared withthat of muscle, regional LNs more than 10 mm in short-axis diameter,bulky shape, heterogeneous enhancement, regional LNs with the sameor lower attenuation compared with that of muscle, nodular pericolicfat infiltration, and presence of distant metastasis. Numbers in paren-theses are percentages
J. E. Kim et al.: Differentiation of poorly differentiated colorectal adenocarcinomas

prognosis and might be useful for determining theappropriate therapeutic strategy.
Our study also showed that PD CRACs and WD orMD CRACs have significantly different features withregard to their shape, enhancement, and maximum wallthickness, as seen on MDCT images. PD CRACs fre-quently appeared as heterogeneous bulky lesions withthe same or lower attenuation compared with that ofmuscle. Meanwhile, WD or MD CRACs frequentlyappear as homogenous ulcerofungating/ulceroinfil-trative lesions with attenuation between that of liverand muscle. PD CRACs showed a greater maximal wallthickness than WD or MD CRACs (21.0 ± 9.4 vs.17.9 ± 5.8 vs. 13.6 ± 3.6, P < 0.001). Our results aresimilar to those of a previous study in which the au-thors compared the CT density to the histology and sizeof CRACs [24]. In their study, all PD CRACs showedheterogeneous enhancement, while 85% of WD CRACsand 52% of MD CRACs showed homogenousenhancement. As the tumor size increased, the numberof CRACs showing heterogeneous enhancement alsoincreased. On the pathology review in their study, it wasfound that low-density areas in the tumor were com-posed of fibrous or mucinous stroma or necrosis andthat high-density areas consisted primarily of well-developed, tubular, branching glands of adenocarcino-mas. The enhancement degree of PD CRACs seen inour study agrees with that determined by Kim et al.[25]. They showed that the mean blood flow, whichreflects the flow rate through the vasculature and isrelated to tumor vascularity, was significantly lower inPD CRACs compared to WD or MD CRACs in theirCT perfusion study of CRACs involving the sigmoidand rectum. However, Sosna et al. [11] have reporteddifferent results to ours. In their study of 29 colorectalneoplasms using 45-s-delay CT colonographic images,the degree of enhancement did not correlate with degreeof histologic differentiation. This discrepancy may bedue to the following reasons: First, in our study, mostlesions (93/113) were 4 cm or more in diameter, whereasmost lesions (16/29) were 2 cm or less in their study.Second, in our study, there were 26 PD CRACs, while,in their study, many lesions were adenomas (15/29) andmost CRACs were MD CRACs (9/14), but there wereonly 3 cases of PD CRACs. Therefore, our study resultsreflect a more representative nature of advanced colo-rectal tumors according to the tumor differentiationthan their study. Finally, the delayed time after the startof contrast material injection for postcontrast CT scanswas different: 45-s-delay in their study vs. 70-s-delay inour study. Based on our study results, we believe thatthe shape and enhancing features of the CRAC types,according to tumor differentiation, may be helpful inpreoperatively determining the histologic grades ofCRAC and that determination of a combination of
shape and enhancement features may further improvethe accuracy for making the correct diagnosis.
In terms of regional LNs, PD CRACs frequentlyshowed LNs more than 10 mm in short-axis diameterand/or having the same or lower attenuation comparedwith that of muscle. PD CRACs also more frequentlydemonstrated nodular pericolic infiltration and distantmetastasis. Our results are similar to those of previousstudies in which PD CRAC has a higher tendency topenetrate through the bowel wall, invade veins, andmetastasize to LNs and distant sites [4, 6, 22]. However,in our study, there was no significant difference regard-ing direct invasion between PD CRAC and WD or MDCRAC (8 (31%) of 26 vs. 11 (13%) of 87, P = 0.0615).Considering that the purpose of performing CRACsurgery with a curative intent is to achieve R0 resectionof the primary lesion along with the regional LNs,radiologists should give more attention to extramuraltumor infiltration, regional LNs, and distant metastaticsites in patients with PD CRAC during the pre-operativeimaging workup.
There are limitations to our study. First, because ofits retrospective nature and matching of three types ofCRAC with regard to patient sex and age, a certain de-gree of selection bias could not be avoided. Therefore,there is the possibility of a good fit of the data for ourstudy patient series, although this may not necessarilyextend to the CRAC population at large. Further studyin larger study population with CRAC will be warrantedto determine extent of extrapolation of our study results.Second, we did not evaluate the diagnostic performanceof MDCT for the evaluation of resectability which is oneof the major roles of preoperative imaging in patientswith CRCs. Third, as the CT images were reviewed bytwo radiologists in consensus, we could not assessinterobserver agreement or reproducibility between theradiologists. Subjective assessment of the morphologicfeatures of primary tumors in our study could potentiallylead to somewhat low interobserver agreement in actualclinical practice. However, the discrepancy rate betweenthe two reviewers was not high enough to change thestudy results as a set of sample images representing theCT findings to be analyzed, which were not included inthe study population, were shown to the reviewers inadvance.
In conclusion, MDCT can be used to differentiate PDCRAC from WD or MD CRAC with a high degree ofaccuracy if one uses specific CT features; knowledge ofthese characteristic CT findings may be helpful forprognostication in patients with primary CRACs.
Acknowledgments. Contract grant sponsor: This study was supportedby grant no. 0420120500 from the SNUH Research Fund. Contractgrant number: A100048.
Conflict of interest. None declared.
J. E. Kim et al.: Differentiation of poorly differentiated colorectal adenocarcinomas

References
1. Siegel R, Naishadham D, Jemal A (2013) Cancer statistics, 2013.CA Cancer J Clin 63:11–30
2. Horton KM, Abrams RA, Fishman EK (2000) Spiral CT of coloncancer: imaging features and role in management. Radiographics20:419–430
3. Kaur H, Choi H, You YN, et al. (2012) MR imaging for preop-erative evaluation of primary rectal cancer: practical consider-ations. Radiographics 32:389–409
4. Takeuchi K, Kuwano H, Tsuzuki Y, et al. (2004) Linicopatho-logical characteristics of poorly differentiated adenocarcinoma ofthe colon and rectum. Hepatogastroenterology 51:1698–1702
5. Kazama Y, Watanabe T, Kanazawa T, et al. (2008) Poorly dif-ferentiated colorectal adenocarcinomas show higher rates ofmicrosatellite instability and promoter methylation of p16 andhMLH1: a study matched for T classification and tumor location. JSurg Oncol 97:278–283
6. Chung CK, Zaino RJ, Stryker JA (1982) Colorectal carcinoma:evaluation of histologic grade and factors influencing prognosis. JSurg Oncol 21:143–148
7. Jass JR (1988) The pathological grading and staging of rectalcancer. Scand J Gastroenterol Suppl 149:21–38
8. Mehrkhani F, Nasiri S, Donboli K, Meysamie A, Hedayat A (2009)Prognostic factors in survival of colorectal cancer patients aftersurgery. Colorectal Dis 11:157–161
9. Cho YB, Chun HK, Yun HR, et al. (2009) Histological gradepredicts survival time associated with recurrence after resection forcolorectal cancer. Hepatogastroenterology 56:1335–1340
10. Rosai J, Ackerman LV (2011) Gastrointestinal tract—large bowel.In: Rosai J (ed) Rosai and Ackerman’s Surgical Pathology, 10th edn.Amsterdam: Elsevier, pp 762–768
11. Sosna J, Morrin MM, Kruskal JB, et al. (2003) Colorectal neo-plasms: role of intravenous contrast-enhanced CT colonography.Radiology 228:152–156
12. International Union Against Cancer (UICC) (2002) Histopathol-ogical grading. In: Sobin LH, Wittekind C (eds) TNM classificationof malignant tumor, 6th edn. New York: Wiley-Liss, p 13
13. Hamilton SR, Vogelstein B, Kudo S (2000) Carcinoma of the colonand rectum. In: Hamilton S, Aaltonen L (eds) World health orga-
nization classification of tumors-pathology and genetics of tumors ofthe digestive system. Lyon: IARC Press, pp 105–119
14. Edge SB, Byrd DR, Compton CC, et al. (2010) Colon and rectum.In: Edge SB (ed) AJCC cancer staging manual, 7th edn. New York:Springer, pp 143–156
15. George SM, Makinen MJ, Jernvall P, et al. (2000) Classification ofadvanced colorectal carcinomas by tumor edge morphology: evi-dence for different pathogenesis and significance of polypoid andnonpolypoid tumors. Cancer 89:1901–1909
16. Cooper HS, Slemmer JR (1991) Surgical pathology of carcinoma ofthe colon and rectum. Semin Oncol 18:367–380
17. Dukes CE, Bussey HJ (1958) The spread of rectal cancer and itseffect on prognosis. Br J Cancer 12:309–320
18. Biffi R, Botteri E, Bertani E, et al. (2013) Factors predicting worseprognosis in patients affected by pT3 N0 colon cancer: long-termresults of a monocentric series of 137 radically resected patients in a5-year period. Int J Colorectal Dis 28:207–215
19. Weiser MR, Posner MC, Saltz LB (2013) Adenocarcinoma of thecolon and rectum. In: Yeo CJ, Pemberton JH (eds) Shackelford’ssurgery of the alimentary tract, 7th edn. Philadelphia: ElsevierSaunders, p 2066
20. Foxtrot Collaborative Group (2012) Feasibility of preoperativechemotherapy for locally advanced, operable colon cancer: the pilotphase of a randomised controlled trial. Lancet Oncol 13:1152–1160
21. Nørgaard A, Dam C, Jakobsen A, et al. (2014) Selection of coloncancer patients for neoadjuvant chemotherapy by preoperative CTscan. Scand J Gastroenterol 49:202–208
22. Masuda H, Abe Y, Takayama T (2005) Microsatellite instability inpoorly differentiated colorectal adenocarcinoma, particularly inrelation to two subtypes. Hepatogastroenterology 52:82–85
23. De Sousa E, Melo F, Vermeulen L, Fessler E, Medema JP (2013)Cancer heterogeneity—a multifaceted view. EMBO Rep 14:686–695
24. Furukawa H, Hara T, Taniguchi T (1992) Colorectal carcinomaevaluated by incremental dynamic CT: comparison of CT density,histology, and tumor size. Gastroenterol Jpn 27:334–340
25. Kim JW, Jeong YY, Chang NK, et al. (2012) Perfusion CT incolorectal cancer: comparison of perfusion parameters with tumorgrade and microvessel density. Korean J Radiol 13(Suppl 1):S89
J. E. Kim et al.: Differentiation of poorly differentiated colorectal adenocarcinomas