Embed Size (px)
Citation preview

This care process model (CPM) was created by the Sepsis Workgroup at Intermountain Healthcare to present current evidence-based care standards that will improve septic patient outcomes and reliability of care as well as reduce costs of sepsis care. It guides the assessment and treatment of adult inpatients presenting with severe sepsis or septic shock in the emergency department (ED), operating room (OR), intensive care unit (ICU), acute care facility, or post-discharge care facility.
Why Focus ON SEPSIS AND SEPTIC SHOCK?Sepsis, severe sepsis, and septic shock are major healthcare challenges that affect millions of people each year. Rapid diagnosis and treatment are key to preventing the progression of sepsis to organ failure, septic shock, and death.KUM, LEV1 Because many diverse diagnoses meet criteria for non-severe sepsis, this CPM focuses specifically on the management of severe sepsis and septic shock. These conditions warrant attention because they are:
• Common. Sepsis is the most common inpatient diagnosis for adults at Intermountain facilities, and it is the most commonly diagnosed condition in the hospital setting, affecting up to 40 % of hospitalized patients.
• Costly. The cost of hospital treatment for sepsis exceeds $24 billion annually, making it the most expensive condition to treat in the U.S. healthcare system.TOR Intermountain has spent more than $800 million to treat sepsis patients in the last three years.ALL
• Associated with high mortality. Severe sepsis has a 10 – 20 % mortality rate, and for septic shock, the mortality rate is up to 40 %. Septic shock is a leading cause of death in U.S. hospitals.LIU Further, those who do survive severe sepsis are more likely to suffer organ damage, cognitive impairment, and / or physical disabilities that may be long-term or permanent.
Compliance with a sepsis bundle of evidence-based care both improves patient outcomes and reduces cost.LEI Early identification and appropriate management in the initial hours of sepsis present a critical opportunity. Successful completion of the required elements of care requires clear communication among care team members to ensure that the continuum of care is timely and correct.
WHAT’S INSIDE?ALGORITHMSDiagnosis. . . . . . . . . . . . . . . . . . . . . . . . . . 3Treatment . . . . . . . . . . . . . . . . . . . . . . . . . 6
OVERVIEW . . . . . . . . . . . . . . . . . . . . . . 2
DIAGNOSIS . . . . . . . . . . . . . . . . . . . . . . 2
TREATMENT . . . . . . . . . . . . . . . . . . . . . 4
Standardized power plans . . . . . . . . . . . . 4Bundles . . . . . . . . . . . . . . . . . . . . . . . . . . . 4Care team transitions . . . . . . . . . . . . . . . . 5Tidal volume conversion tables . . . . . . . . 8
RESOURCES . . . . . . . . . . . . . . . . . . . . . 9
REFERENCES . . . . . . . . . . . . . . . . . . . .10
D E V E L O P M E N T A N D D E S I G N O F
Care Process Models
C a r e P r o c e s s M o d e l M O N T H 2 0 1 5
2 0 15 U p d a t e
R E C O G N I T I O N A N D M A N A G E M E N T O F
Severe Sepsis and Septic Shock
C a r e P r o c e s s M o d e l A U G U S T 2 0 2 0
GOALS & MEASURESIntermountain has the following system goals related to sepsis:
• Reduce mortality rate of sepsis, severe sepsis, and septic shock
• Increase compliance with the severe sepsis and septic shock bundles, including time points at:
– 3 h after presentation and
– 6 h after presentation
• Increase % of sepsis patients for whom the suspected infection source is documented
©2014 – 2020 INTERMOUNTAIN HEALTHCARE. ALL RIGHTS RESERVED. 1
12 12
3
4567
8
9
1011 12 1
2
3
4567
8
9
1011
Indicates an Intermountain measure

S E P S I S A N D S E P T I C S H O C K A U G U S T 2 0 2 0
© 2014 - 2020 INTERMOUNTAIN HEALTHCARE. ALL RIGHTS RESERVED. 2
OVERVIEWSevere sepsis and septic shock are major healthcare problems affecting millions of people each year and killing 10 – 40% of patients with the conditions. While sepsis patients meet the criteria for systemic inflammatory response syndrome (SIRS), which is a nonspecific inflammatory response, the inflammatory response occurring during sepsis is secondary to cytokine release. Severe sepsis and septic shock are distinct also in that they involve some degree of organ dysfunction (see page 3).
In contrast to sepsis, septicemia refers to the presence of infectious agents in the bloodstream. The infectious agents responsible for this condition may arise from various sources, including the skin, lungs, abdomen, or urinary tract. Septicemia can rapidly become life-threatening, and patients with this condition are often treated in a hospital’s ICU. Similar to polytrauma, acute myocardial infarction, or stroke, early identification and appropriate management in the initial hours of sepsis and / or septicemia result in improved outcomes.
DIAGNOSISThe following are common clinical characteristics of both SIRS and sepsis:
• Fever or hypothermia
• Tachycardia
• Tachypnea• Elevated or suppressed white blood cells (WBCs) or a shift to immature white
cell forms
Patients presenting with these signs who have a suspected infection should be evaluated for potential sepsis (see page 3).
TREATMENTTimely and precise treatment is key to reducing mortality and other adverse outcomes in septic patients. Intermountain has developed tools within the normal physician workflow to remind physicians when to implement critical elements of care, assist them with decision support, and improve efficiency when managing septic patients.
BundlesSevere sepsis and septic shock bundles encompass key elements of care that should be received by all patients with one of these conditions.RHO Because the Centers for Medicare & Medicaid Services (CMS) monitors Intermountain’s compliance with bundle elements and assigns a non-compliant designation to the entire bundle if any one element is unmet, it is critical for physicians to implement bundles and complete all steps on time. This CPM includes elements for the Severe Sepsis 3-hour, Septic Shock 6-hour, and Maintenance 24-hour bundles (see algorithm 2 on page 6). Compliance with CMS sepsis bundles improves patient outcomes.LEV2
Note: “Time zero” or “time of presentation” for bundle initiation is defined as the time of triage in the ED. If the patient presents from another care venue, it is the time of earliest chart annotation consistent with all elements of sepsis (formerly severe sepsis) or septic shock.LEV1
DEFINITIONS
Terms referenced in this CPM:
Bacteremia: Bacteria are cultured from the blood (with or without a systemic response).
Bundle: Key elements of care that all patients with that condition should receive. If any one bundle element is deficient, a non-compliant designation is assigned to the entire bundle.
CVP: Central venous pressure.
HR: Heart rate.
Infection: Localized inflammation of body tissues caused by a microorganism (bacterium, virus, protozoan, or fungus). Examples: pneumonia, UTI, skin or soft tissue, bone or joint, endocardium, meninges, or body cavity (e.g., pleura or peritoneum).
INR: International normalized ratio.
IVC: Inferior vena cava.
MAP: Mean arterial pressure.
PBW: Predicted body weight.
PTT: Partial thromboplastin time.
SaO2: Arterial oxygen percent saturation.
SBP: Systolic blood pressure.
ScvO2: Central venous oxygen saturation.
Sepsis: A systemic response to infection secondary to the release of cytokines.
Septic shock: Poor global perfusion of the major organs manifested by either hypotension unresponsive to fluid administration or a serum lactate > 4.0 mmol / L.
Septicemia: Infectious agents in the blood that result in a host’s systemic response.
Severe sepsis: When sepsis results in one or more organ's dysfunction.
SIRS: Systemic inflammatory response syndrome.
SVI: Stroke volume index.
US: Ultrasound.

S E P S I S A N D S E P T I C S H O C K A U G U S T 2 0 2 0
© 2014 - 2020 INTERMOUNTAIN HEALTHCARE. ALL RIGHTS RESERVED. 3
Patient presents with suspected infection
ALGORITHM 1: DIAGNOSIS OF SEVERE SEPSIS OR SEPTIC SHOCK
no
DOCUMENT suspected source of infection
EVALUATE for systemic inflammatory responseDetermine if AT LEAST TWO of the following criteria are met for sepsis:
� Temperature > 38.3°C or < 36°C
� Heart rate > 90 beats per minute
� Respiratory rate > 20 breaths per minute
� White blood cell (WBC) count > 12,000 / mm3, < 4,000 / mm3, or > 10 % immature (band) forms
TREAT severe sepsis or septic shock per algorithm on page 6
Sepsis criteria NOT met; TREAT infectious condition
EVALUATE for ANY of the following signs of acute organ dysfunction:
• SBP < 90 mm Hg • SBP decrease > 40 mm Hg from patient's known baseline
• MAP < 65 mm Hg • Creatinine > 2 mg / dL • Acute respiratory failure requiring new or increased need for invasive or non-invasive mechanical ventilation
• Urine output < 0.5 mL / kg / hr for > 2 hours
• Total bilirubin > 2 mg / dL • Platelets < 100,000 / mm3
• INR > 1.5 or PTT > 60 seconds • Lactate > 2 mmol / L
Sepsis possible; TREAT infectious
condition as necessary
≥ 2 criteria met?
ANY sign of acute organ dysfunction*?
yes
no yes
*Note: Organ dysfunction associated with preexisting chronic conditions should not be considered as meeting acute organ dysfunction criteria (e.g. Creatinine > 2 mg / dL in patients with end stage renal disease).

S E P S I S A N D S E P T I C S H O C K A U G U S T 2 0 2 0
©2014 - 2018 INTERMOUNTAIN HEALTHCARE. ALL RIGHTS RESERVED. 4
Standardized power plans (order sets)Power plans for septic patients include the important elements of care as pre-checked, default items. Although power plans need to be modified for specific patient needs to achieve safe and effective care, they correlate with improved outcomes when used appropriately. For this reason, the use of the sepsis power plans is strongly encouraged, and their use is monitored closely.
Early antibiotic administrationEarly antibiotic administration in sepsis is associated with increased survival. Antibiotics should be ordered < 2 hours from ED arrival for patients with severe sepsis (a systemic response to infection resulting in dysfunction of one or more organ systems). Recommended empiric antibiotics should be selected from the relevant ED power plans for the suspected source of infection. Antibiotics should be ordered < 1 hour from ED arrival for patients with septic shock (poor global perfusion of the major organs manifested by either hypotension, unresponsiveness to fluid administration, or a serum lactate ≥ 4.0 mmol / L). Use the relevant ED power plan as reference for antibiotic selection. If the source of infections is unknown, use broad-spectrum antibiotics.
Care team transitionsThe resuscitation and care of patients with severe sepsis and septic shock requires multiple experts and use of many locations within a facility — ED, OR, ICU, acute care, post-discharge care facility — plus home care. During the critical phase of resuscitation, the patient will likely transition across different locations, care teams, and shift changes.
Many of the elements of sepsis care are time-sensitive. Excellent communication among care team members is imperative for smooth and uninterrupted resuscitation. Both the transferring team and receiving team must understand exactly where the patient is within the resuscitation process, what has already been accomplished, and what remains to be done and when.
KEY RECOMMENDATIONSUse the following Intermountain sepsis treatment plan tools to facilitate physician workflow:
• Power plans (pre-defined order sets) are applied as appropriate by patient's primary disease and location:
– ICU admissions – Non-ICU admissions
• Bundles (sets of actions) must be completed to meet compliance standards, sometimes within a specific time frame as follows (see page 6):
– Severe Sepsis 3-hour bundle
– Septic Shock 6-hour bundle
– Maintenance 24-hour bundle
Use a combination of tools, including electronic resources and bedside handoffs (see below) to ensure smooth care, especially during team transitions. These tools help keep all caregivers on track:
• Checklists
• Electronic alerts
• Smart time clocks
• Computer displays
• Handoff tool (see page 5 for Adult Sepsis Bundle Worksheet)

© 2014 - 2020 INTERMOUNTAIN HEALTHCARE. ALL RIGHTS RESERVED. 5
©2020 INTERMOUNTAIN HEALTHCARE. ALL RIGHTS RESERVED.
S E P S I S A N D S E P T I C S H O C K A U G U S T 2 0 2 0
ADULT SEPSIS BUNDLE WORKSHEET PLACE PATIENT STICKER HERE
Discuss worksheet progress in RN handoff upon admission. This is not part of the patient record. All nursing activities and interventions must be documented in iCentra.
Severe Sepsis Recognition1. Known or Suspected Source
of Infection: _________________
2. Signs of Possible Sepsis (at least 2): • Temperature > 38.3 °C OR < 36 °C • Tachycardia > 90 bpm • Tachypnea > 20 bpm • WBC > 12,000 / mm3 or < 4,000 / mm3
or immature forms > 10 %
3. Acute Organ Dysfunction Criteria* (at least 1): • SBP < 90 (or 40 points lower than patient’s normal) or MAP < 65
• Respiratory failure (evidenced by a new need for invasive or non-invasive mechanical ventilation)
• Creatinine > 2.0 mg / dL • Urine output < 0.5 mL / kg / hr for > 2 hr • INR > 1.5 or PTT > 60 secs • Platelet count < 100,000 / mcL • Lactate > 2 mmol / L • Total bilirubin > 2 mg / dL
*Organ dysfunction associated with pre-existing chronic conditions should not be considered as meeting acute organ dysfunction criteria (e.g. Creatinine > 2.0 mg / dL in end-stage renal disease).
Severe Sepsis and Septic Shock Resuscitation 3-Hour BundleTo be completed within a maximum of 3 hours from sepsis presentation time
PRESENTATION TIME: Enter ER triage time
3-HOUR GOAL TIME:
Enter time 3 hours from ER triage
Draw serum lactate Initials Time Lactate result: _______ mmol / L
Draw blood cultures (prior to antibiotics) Initials Time
Give antibiotics intravenously Initials Time
Isotonic crystalloid (30 mL / kg) administered over < 90 min for those with: • SBP < 90 mm Hg OR
• MAP < 65 mm Hg OR
• Decrease in SBP by > 40 mm Hg OR
• Initial lactate > 4 mmol / L
Initials Time
Actual body weight: ______ kg X 30 mL / kg of isotonic crystalloid = _______ mL administered over less than 90 minutes (if BMI > 30 may use 30 mL / kg predicted body weight (PBW)
Check BP every 15 minutes while in ED Initials Time
Severe Sepsis and Septic Shock Treatment 6-Hour BundleTo be completed within a maximum of 6 hours from presentation time for persistent hypertension
(MAP < 65 mm Hg within an hour after 30 mL / kg isotonic crystalloid bolus completion) OR initial lactate ≥ 4 mmol / L
PRESENTATION TIME: Enter ER triage time
6-HOUR GOAL TIME:
Enter time 3 hours from ER triage
Sepsis Alert – iCentra monitors vital signs and lab results in real time; if those values meet the rules for severe sepsis or septic shock, it will activate the Sepsis Alert. When this occurs, minimize the alert window and go immediately to assess the patient.Consult with the treating provider if you believe the alert is reasonably valid. At that time the sepsis orders or power plans can be launched to guide delivery of the bundle and SEP-1 compliance.
Use this sheet to track progress and as a reminder of times by which actions must be completed. It may also be helpful for continuity of care when transferring care to another unit or clinician.
Antibiotics should be ordered according to the recommendations represented in the power plans.
• For severe sepsis, antibiotics should be ordered < 2 hours from ED arrival.
• For septic shock, antibiotics should be ordered < 1 hour from ED arrival.
• Use source targeted antibiotics within the timeline if possible; if source unknown, use broad spectrum antibiotics.
Consider viral PCR testing when appropriate due to seasonality or local factors.
Repeat lactate (if initial lactate > 2 mmol / L) Initials Time Lactate result: ______ mmol / L
Vasopressors if SBP or MAP remain low after fluids (preferentially start norepinephrine at 0.02 mcg / kg / min)
Initials Time
Perform ONE of the following 3 options if SBP or MAP remain low after fluids OR Lactate ≥ 4 mmol / L:
Document a focused clinical exam including 5 of 8 exam elements. (List on right.)
OR
State that a sepsis-focused clinical exam has been performed.
OR
Perform any ONE of the list below:1. CVP measurement2. ScvO2 measurement3. Bedside cardiac and IVC US with
documentation4. Passive leg raise OR fluid challenge with
SVI % change
Initials Time
Document focused clinical exam of 5 of the following 8:• SaO2 %• Capillary refill• Cardiopulmonary assessment• Peripheral pulses• Skin color or condition• Urine output•Vital signs•Shock index = (HR in BPM) / (SBP)
Initials Time
• CVP result: ________• ScvO2 result: ________ %• Cardiac and IVC US done:____ • Passive leg raise done,
SVI % change: ________%• Fluid challenge, volume _____mL
and SVI % change: _______%
Severe Sepsis and Septic Shock 24-hr Maintenance Bundle (Not part of SEP-1 reporting)
1. Glucose management
2. Stress-dose steroids if on high-dose vasopressors
3. Lung-protective ventilation
Complete in the ICU
1. Target 90 – 180 mg2. Hydrocortisone (50 mg IV Q6)3. Target Vt 6 mL / kg (4 – 8 mL / kg)
maintain Pplat < 30 cm H2O

BEGIN Severe Sepsis and Septic Shock Resuscitation 3-Hour Bundle (completed within 3 hours of time zero)
�DRAW serum lactate �DRAW blood cultures prior to giving antibiotics �GIVE antibiotics intravenously according to recommendations represented in the power plans
– For severe sepsis, antibiotics should be given < 2 hours after arrival at ED – For septic shock, antibiotics should be given < 1 hour after arrival at ED – Use source-targeted antibiotics within the time line if possible; if source is unknown, use broad-spectrum antibiotics
S E P S I S A N D S E P T I C S H O C K A U G U S T 2 0 2 0
© 2014 - 2020 INTERMOUNTAIN HEALTHCARE. ALL RIGHTS RESERVED. 6
ALGORITHM 2: SEVERE SEPSIS / SEPTIC SHOCK TREATMENT
Patient meets severe sepsis or septic shock criteria
Is patient hypotensive* and / or lactate ≥ 4 mmol / L?no yes
BEGIN Severe Sepsis and Septic Shock Treatment 6-Hour Bundle (completed within 6 hours of time zero)
� If initial lactate was > 2, REPEAT serum lactate � If SBP or MAP remain low after fluids, START vasopressors to maintain MAP ≥ 65 mm Hg. Norepinephrine is the preferred vasopressor for initial therapy starting at 0.02 mcg / kg / min unless contraindicated (b).RHO
� If hypotension* or need for vasopressors continues, REPEAT volume status and tissue perfusion assessment choosing ANY ONE of the following three options:• Document that a severe sepsis or septic shock-focused exam was performed• Document FIVE of the EIGHT following elements of the focused exam:
– Vital signs – Cardiopulmonary exam
• Document ANY ONE of the following: – CVP measurement (c) – ScvO2 measurement (d)
BEGIN Severe Sepsis and Septic Shock 24-hour Maintenance Bundle • If on high-dose vasopressors, GIVE hydrocortisone (50 mg IV every 6 hours).DEL DISCONTINUE steroids when patient is weaned off vasopressors. • ACHIEVE and MAINTAIN an average glucose between 90 – 180 mg / dL using bedside measurements performed at least every 4 hours for at least the first 24 hr.HAL
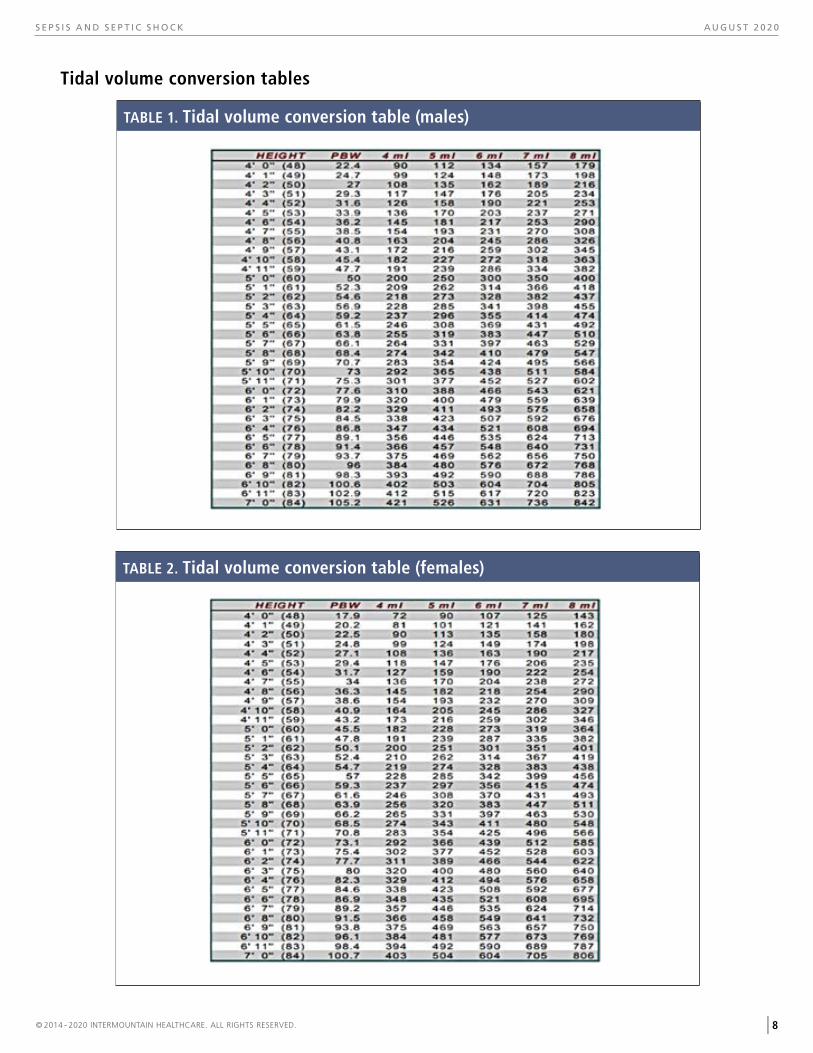
• If mechanically ventilated, target tidal volume (VT) at 6 mL / kg PBW (range: 4 – 8 mL / kg PBW) AND maintain Pplat < 30 cm H2O (see Tidal volume tables on page 8).ACU
� DOCUMENT and COMMUNICATE presentation time (this is time zero)
no
– Peripheral pulse – Capillary refill evaluation
– Skin examination – SaO2 %
– Urinary output – Shock index (HR in BPM / SBP)
– Cardiovascular and IVC ultrasound – Passive leg raise or fluid challenge using a non-invasive cardiac output monitor
yes
*Hypotension: • MAP < 65 mm Hg or • SBP < 90 mm Hg or • SBP > 40 mm below baseline
GIVE 30 mL / kg isotonic crystalloid over 30 – 90 minutes, and REASSESS blood pressure
If BMI > 30, may give initial fluid bolus as 30 mL / kg PBW (a)
Is patient still hypotensive* and / or lactate elevated?
yes
no
12 12
3
4567
8
9
1011 12 1
2
3
4567
8
9
1011
3-hour bundle
6-hour bundle
12 12
3
4567
8
9
1011 12 1
2
3
4567
8
9
1011
PERFORM further fluid resuscitation using non-invasive hemodynamic monitoring until ANY of the following occur:
• Patient becomes stable off vasopressors and lactate decreases significantly • Adequate cardiac volume and filling is shown using cardiac ultrasound • Patient is no longer fluid responsive (< 10 % increase in stroke volume index following passive leg raise or 500 mL isotonic crystalloid fluid bolus). If patient continues to need support at this time, use vasopressors only.
TREAT based on patient's initial lactate (mmol / L)≤ 2 2.1 – 3.9 ≥ 4.0
CONTINUE care for severe sepsis
REPEAT lactate within 3 hours of initial lactate, and CONTINUE care for severe sepsis
COMPLETE all elements of the severe sepsis and septic shock treatment 6-hour bundle
Is patient hypotensive* within an hour following fluid bolus?

S E P S I S A N D S E P T I C S H O C K A U G U S T 2 0 2 0
© 2014 - 2020 INTERMOUNTAIN HEALTHCARE. ALL RIGHTS RESERVED. 7
ALGORITHM NOTES
(a) Fluid bolus for hypotensive patients
Deliver 30 mL / kg (actual weight) isotonic crystalloid over 30 – 90 minutes. If BMI > 30, a fluid bolus of 30 mL / kg predicted body weight (PBW) may be used. The Tidal volume conversion tables on page 8 give PBW as determined by sex and height.
(c) Central venous pressure (CVP)w
Measurement of CVP is one of the Sepsis CMS Core (SEP-1) performance measures and is included as one option to document the assessment of tissue perfusion in the 3- to 6-hour bundle. CVP has been shown in multiple studies to be poorly predictive of fluid responsiveness.MAR, RHO CVP > 8 mm Hg was a resuscitation target in early goal-directed therapy for septic shock, but was not shown to be an essential component for sepsis resuscitation in the ProCESS, ProMISe, and ARISE trials. RIV, PRO, MOU, ARI
(d) ScvO2 %
Measurement of ScvO2 % is one of the CMS SEP-1 performance measures included as an option to document the assessment of tissue perfusion in the 3- to 6-hour bundle. ScvO2 % has been shown to be a marker of the adequacy of cardiac output for organ perfusion in patients with septic shock.WAL ScvO2 % > 70 % correlates with an ScvO2 % of > 65 %. ScvO2 > 70 % was a resuscitation target in early goal-directed therapy for septic shock; dobutamine and blood transfusions were used to increase ScvO2 % to > 70 % after a CVP > 8 mm Hg was achieved and MAP was maintained > 65 mm Hg with norepinephrine.RIV In the ProCESS, ProMISe, and ARISE trials, ScvO2 % was shown to not be essential as a target for resuscitation.PRO, MOU, ARI If measured, ScvO2 % should be interpreted in the clinical context to assess the adequacy of cardiac output for organ perfusion, and an ScvO2 % < 70 % may be acceptable if lactate is normal and other signs of organ perfusion are adequate. ScvO2 % that is low (i.e. < 60 %), may be due to cardiac insufficiency and should prompt consideration of echocardiography to characterize left and right ventricular function.
(b) Norepinephrine
Norepinephrine is the recommended vasopressor for septic shock.RHO In refractory septic shock with escalating dose of norepinephrine, may add vasopressin (up to 0.03 U / min) or epinephrine with the intent of raising MAP to target, or add vasopressin (up to 0.03 U / min) to decrease norepinephrine dosage, acknowledging that vasopressin added to norepinephrine was not shown to improve survival in septic shock.RHO, RUS Recommend against using dopamine in septic shock except in situations of bradyarrhythmia.RHO
S E P S I S A N D S E P T I C S H O C K A U G U S T 2 0 2 0
© 2014 - 2020 INTERMOUNTAIN HEALTHCARE. ALL RIGHTS RESERVED. 8
Tidal volume conversion tables
TABLE 1. Tidal volume conversion table (males)
TABLE 2. Tidal volume conversion table (females)

S E P S I S A N D S E P T I C S H O C K A U G U S T 2 0 2 0
© 2014 - 2020 INTERMOUNTAIN HEALTHCARE. ALL RIGHTS RESERVED. 9
LOCATING PATIENT EDUCATION MATERIALSIntermountain education materials are designed to support your efforts to educate and engage patients and families. They complement and reinforce team interventions by providing a means for patients to reflect and learn in another mode and at their own pace. To access these materials:
• In the iCentra EMR system, search for Intermountain items in the patient education module.
• Go to https://intermountainhealthcare.org/health-information/health-library/patient-handouts/, and search for the patient education library using keywords.
• Use Print It! for one-stop access and ordering for all Intermountain-approved education, such as fact sheets, booklets, and trackers.
PATIENT EDUCATION RESOURCESThe Intermountain Sepsis Workgroup, affiliated educators, and Patient and Provider Publications team have developed patient education material to directly support treatment recommendations in this care process model. Education for patients and families increases patient compliance with a treatment plan.
Intermountain-approved patient education materialsThe Sepsis fact sheet is an Intermountain-approved patient education resource, which can be accessed online and have prints ordered at minimal cost.
See access and ordering information at left.
1
FA C T S H E E T F O R PAT I E N T S A N D FA M I L I E S
Sepsis
What is sepsis?Sepsis is a serious, whole-body response to an infection. It causes inflammation and may cause organ dysfunction in the brain, lungs, kidneys, and blood clotting system.
Sepsis can progress to septic shock. A person with septic shock will have low blood pressure, which requires treatment with special drugs to raise it. Both sepsis and septic shock are serious and require aggressive medical treatment in a hospital.
What causes sepsis?Sepsis is caused by germs (bacteria, fungi, or viruses) growing inside you at high levels. The infection might be only in one area of the body, like in a tooth or lungs, or can be widely spread throughout the body in the blood. A doctor will order tests to locate the infection, but even with this testing, the cause of sepsis often remains unknown.
Although anyone can develop sepsis, it’s more likely to affect the following:
• The very old or the very young (for example, premature babies)
• People whose immune systems are already weakened because of illness, injury, or medicines they are taking
• Patients who are undergoing certain medical treatments (such as chemotherapy for cancer)
• Patients who have tubes or lines in their body to deliver or drain fluids such as catheters or IV’s
What are the signs and symptoms?To diagnose sepsis, doctors check symptoms and laboratory test results. Common signs and symptoms include an infection with the following:
• Temperature higher or lower than normal
• Fast heartbeat
• Fast breathing
• Very high or very low number of white blood cells (white blood cells are the parts of your blood that find and fight infection in the body)
• Severe shivering, also known as “shaking chills”
• Change in mental status (for example, confusion, memory loss, problems with thinking)
If the condition gets worse, blood pressure drops and vital organs (such as the kidneys or liver) may begin to fail.
Septic shock usually requires medical treatment in a hospital intensive care unit (ICU).
Sepsis fact sheet in English and Spanish
Provider resourcesTo find this CPM, go to intermountainphysician.org, under the Tools and Resources tab, select Care Process Models.

S E P S I S A N D S E P T I C S H O C K A U G U S T 2 0 2 0
REFERENCESACU Acute Respiratory Distress Syndrome Network, Brower RG, Matthay MA, Morris A, et al. Ventilation with
lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N Engl J Med. 2000;342(18):1301-1308.
ARI ARISE Investigators, ANZICS Clinical Trials Group, Peake SL, et al. Goal-directed resuscitation for patients with early septic shock. N Engl J Med. 2014;371(16):1496-1506.
ALL Allen TL, Jarman AF, Dong L, et al. Quality lowers cost: The cost effectiveness of a multicenter treatment bundle for severe sepsis and septic shock [SAEM abstract 129]. Society for Academic Emergency Medicine Annual Meeting Abstracts 2015; 22(S1):S64.
DEL Dellinger RP. Cardiovascular management of septic shock. Crit Care Med. 2003;31(3):946-955.
HAL Hall MJ, Williams SN, DeFrances CJ, Golosinskiy A. Inpatient care for septicemia or sepsis: A challenge for patients and hospitals. NCHS Data Brief. 2011;(62):1-8.
KUM Kumar A, Roberts D, Wood KE, et al. Duration of hypotension before initiation of effective antimicrobial therapy is the critical determinant of survival in human septic shock. Crit Care Med. 2006;34(6):1589-1596.
LEI Leisman DE, Doerfler ME, Ward MF, et al. Survival benefit and cost savings from compliance with a simplified 3-hour sepsis bundle in a series of prospective, multisite, observational cohorts. Crit Care Med. 2017;45(3):395-406.
LEV1 Levy MM, Evans LE, Rhodes A. The Surviving Sepsis campaign bundle: 2018 Update. Crit Care Med. 2018;46(6):997-1000.
LEV2 Levy MM, Gesten FC, Phillips GS, et al. Mortality changes associated with mandated public reporting for sepsis: The results of the New York State initiative. Am J Respir Crit Care Med. September 2018:rccm.201712-2545OC.
LIU Liu V, Escobar GJ, Greene JD, et al. Hospital deaths in patients with sepsis from 2 independent cohorts. JAMA. 2014;312(1):90.
MAR Marik PE, Baram M, Vahid B. Does central venous pressure predict fluid responsiveness?: A systematic review of the literature and the tale of seven mares. Chest. 2008;134(1):172-178.
MOU Mouncey PR, Osborn TM, Power GS, et al. Trial of early, goal-directed resuscitation for septic shock. N Engl J Med. 2015;372(14):1301-1311.
PRO ProCESS Investigators, Yealy DM, Kellum JA, et al. A randomized trial of protocol-based care for early septic shock. N Engl J Med. 2014;370(18):1683-1693.
RHO Rhodes A, Evans LE, Alhazzani W, et al. Surviving sepsis campaign. Crit Care Med. 2017;45(3):486-552.
RIV Rivers E, Nguyen B, Havstad S, et al. Early goal-directed therapy in the treatment of severe sepsis and septic shock. N Engl J Med. 2001;345(19):1368-1377.
RUS Russell JA, Walley KR, Singer J, et al. Vasopressin versus norepinephrine infusion in patients with septic shock. N Engl J Med. 2008;358(9):877-887.
TOR Torio C, Moore B. National Inpatient Hospital Costs: The Most Expensive Conditions by Payer, 2013. HCUP Statistical Brief #204. May 2016. Agency for Healthcare Research and Quality, Rockville, MD. http://www.hcup-us.ahrq.gov/reports/statbriefs/sb204-MostExpensive-Hospital-Conditions.pdf. Accessed March 19, 2018.
WAL Walley KR. Use of central venous oxygen saturation to guide therapy. Am J Respir Crit Care Med. 2011;184(5):514-520.
This CPM presents a model of best care based on the best available scientific evidence at the time of publication. It is not a prescription for every physician or every patient, nor does it replace clinical judgment. All statements, protocols, and recommendations herein are viewed as transitory and iterative. Although physicians are encouraged to follow the CPM to help focus on and measure quality, deviations are a means for discovering improvements in patient care and expanding the knowledge base. Send feedback to Colin Grissom, MD, Intermountain Healthcare ([email protected]).
©2014 - 2020 INTERMOUNTAIN HEALTHCARE. ALL RIGHTS RESERVED. Patient and Provider Publications CPM101 - 08/20 10







![Digiti Sonus: Advanced Interactive Fingerprint ... · fingerprint sonification, there is a deep body of work on biometric fingerprint pattern rec ognition [2]. It is both an active](https://img.dokumen.tips/doc/110x75/5f0d73037e708231d43a695f/digiti-sonus-advanced-interactive-fingerprint-fingerprint-sonification-there.jpg)





















