Embed Size (px)
Citation preview

Q1
Q10 Q2
Q4
Q3
Q9
12345678910111213141516171819202122232425262728293031323334353637383940414243444546474849505152535455
Research ajog.org
56
OBSTETRICS 5758596061626364656667Detection of triploid, molar, and vanishing-twin pregnancies by a single-nucleotidepolymorphism-based noninvasive prenataltestKirsten J. Curnow, PhD; Louise Wilkins-Haug, PhD, MD; Allison Ryan, PhD;Eser Kırkızlar, PhD; Melissa Stosic, MS; Megan P. Hall, PhD; Styrmir Sigurjonsson, PhD;Zachary Demko, PhD; Matthew Rabinowitz, PhD; Susan J. Gross, MD
686970
OBJECTIVE: We sought to determine the ability of single-nucleotide were vanishing twin, 48.7% were viable twin, 5.3% were diandric 71727374757677787980818283848586polymorphismebased noninvasive prenatal testing (NIPT) to identifytriploid, unrecognized twin, and vanishing twin pregnancies.
STUDY DESIGN: The study included 30,795 consecutive reportedclinical cases received for NIPT for fetal whole-chromosome an-euploidies; known multiple gestations were excluded. Cell-freeDNA was isolated from maternal blood samples, amplified via19,488-plex polymerase chain reaction, and sequenced.Sequencing results were analyzed to determine fetal chromosomecopy number and to identify the presence of additional fetalhaplotypes.
RESULTS: Additional fetal haplotypes, indicative of fetal triploidy,vanishing twin, or undetected twin pregnancy, were identified in 130(0.42%) cases. Clinical confirmation (karyotype for singleton preg-nancies, ultrasound for multifetal pregnancies) was available for58.5% (76/130) of cases. Of the 76 cases with confirmation, 42.1%
From Natera Inc, San Carlos, CA (Drs Curnow, Ryan, Kırkızlar, Hall, SigurjonRabinowitz, and Gross and Ms Stosic) and Division of Maternal-Fetal MediciObstetrics and Gynecology, Brigham and Women’s Hospital, and Harvard MMA (Dr Wilkins-Haug).
Received June 9, 2014; revised Aug. 11, 2014; accepted Oct. 7, 2014.
This study was supported by Natera.
K.J.C., A.R., E.K., M.S., M.P.H., S.S., Z.D., M.R., and S.J.G. are employeesstock or options to hold stock in the company. L.W-H. participated in multicsponsored by Ariosa and Sequenom and received partial grant support, butreceive any funding.
Presented at the International Conference on Prenatal Diagnosis and TherapJuly 20-23, 2014, and at the EuropeanHumanGeneticsConference 2014 of tHuman Genetics, Milan, Italy, May 31eJune 3, 2014.
Corresponding author: Susan J. Gross, MD. [email protected]
0002-9378/$36.00 � ª 2014 Elsevier Inc. All rights reserved. � http://dx.doi.org/10.1
FLA 5.2.0 DTD � YMOB10068_proof
triploids, and 3.9% were nontriploid pregnancies that lacked evidenceof co-twin demise. One pregnancy had other indications suggestingtriploidy but lacked karyotype confirmation. Of the 5 vanishing twincases with a known date of demise, 100% of losses occurred in thefirst trimester; up to 8 weeks elapsed between loss and detection byNIPT.
CONCLUSION: This single-nucleotide polymorphismebased NIPTsuccessfully identified vanished twin, previously unrecognized twin,and triploid pregnancies. As vanishing twins are more likely to beaneuploid, and undetected residual cell-free DNA could bias NIPTresults, the ability of this method to identify additional fetal haplotypesis expected to result in fewer false-positive calls and prevent incorrectfetal sex calls.
Key words: noninvasive prenatal testing, single-nucleotide poly-morphism, triploidy, vanishing twin
878889
Cite this article as: Curnow KJ, Wilkins-Haug L, Ryan A, et al. Detection of triploid, molar, and vanishing-twin pregnancies by a single-nucleotide polymorphism-basednoninvasive prenatal test. Am J Obstet Gynecol 2014;211:x.ex-x.ex.
909192
he recent introduction of cell-free9394
T DNA (cfDNA)-based noninvasiveprenatal testing (NIPT) has offered
pregnant women a more accuratemethod for detecting fetal aneuploidiesthan traditional serum screening
sson, Demko,ne, Department ofedical School, Boston,
of Natera Inc and holdenter clinical trialsdid not personally
y, Brisbane, Australia,he EuropeanSociety of
016/j.ajog.2014.10.012
MONTH 2014 Am
9596979899100101102103104105106107108109110
� 21 October 2014 � 8:
methods.1-12 NIPT noninvasively de-termines fetal chromosome copy num-ber by interrogating cfDNA isolatedfrom maternal plasma, with the fetuscontributing anywhere from <2% to>30% of the total cfDNA.3,7,13 OtherNIPT approaches use quantitative“counting” methods where fetal chro-mosome copy number is determined bycomparing the absolute number ofsequence reads from the chromosome(s)of interest (eg, chromosome 21) toreference chromosome(s), inferring fetaltrisomy when this is above a pre-determined threshold. This approachcannot determine the source of DNA(fetal or maternal) and is therefore un-able to detect additional fetal haplotypesassociated with triploidy or vanishingtwins. Vanishing twins were reported to
erican Journal of Obstetrics & Gynecology 1.e154 pm � ce

F1�
Research Obstetrics ajog.org
111112113114115116117118119120121122123124125126127128129130131132133134135136137138139140141142143144145146147148149150151152153154155156157158159160161162163164165166
167168169170171172173174175176177178179180181182183184185186187188189190191192193194195196197198199200201202203204205206207208209210211212213214215216217218219220221222
account for 15% of false positives in arecent counting-based NIPT study.14
This likely results in unnecessary inva-sive prenatal testing. A more recentapproach using a single-nucleotidepolymorphism (SNP)-based methodalong with sophisticated informatics canresolve this potential source of false-positive results. This approach iden-tifies the presence of additional fetalhaplotypes, indicative of a triploid ordizygotic multifetal pregnancy, and de-termines parental origin.10,12
Using the SNP-based approach, theprevalence of cases found to have addi-tional fetal haplotypes within 30,795consecutive cases undergoing routineclinical NIPT was determined, and isreported here. Clinical follow-up ofthese cases is also described.
MATERIALS AND METHODS
PatientsThe current study included all samplesfrom participating centers received forcommercial testing from March 1,through Nov. 30, 2013, that received anNIPT result. This study received a noti-fication of exempt determination froman institutional review board (Ethicaland Independent Review Services, no.14064-01). All samples were analyzed atNatera’s CLIA- and CAP-certified labo-ratory in San Carlos, CA. Analysis wasperformed for all samples on chromo-somes 13, 18, 21, X, and Y, and includeddetection of trisomy 21 , trisomy 18,trisomy 13, monosomy X, sex chromo-some abnormalities (47,XXX/XXY/XYY), fetal sex, and additional fetalhaplotypes.
Sample collection and NIPTMaternal blood samples (>13 mL) werecollected in Streck (Omaha, NE) BCTsand processed at Natera (San Carlos,CA) within 6 days of collection. Allsamples were accompanied by a requi-sition form from the ordering clinician,and included the following patient in-formation: gestational age, maternal dateof birth, maternal weight, whether it wasa multigestation pregnancy, and whethera paternal buccal swab was included.Ordering clinicians determined in-dication(s) for testing. Cases accepted
1.e2 American Journal of Obstetrics & Gynecology
FLA 5.2.0 DTD
for analysis were indicated as singletonpregnancies by ordering clinicians. Re-sults were reported directly to theordering clinician or distributionpartners.Samples were considered outside of
the specifications for testing and werenot analyzed if there was insufficientblood volume or the wrong tube wasused, the sample was damaged, thesample was received at the laboratory>6days after collection, the gestational agewas <9 weeks, the patient used an eggdonor, or the patient had a confirmedmultiple gestation.15 Testing was per-formed on all samples with sufficientblood volume (>13 mL) as describedpreviously using validated laboratorymethodologies (cfDNA isolation, poly-merase chain reaction amplificationtargeting 19,488 SNPs, high-throughputsequencing, and analysis using the Next-generation Aneuploidy Test Using SNPs[NATUS] algorithm).9-12,15 Sampleswere subject to a stringent set of quality-control metrics9-13,15 before reports weresent to ordering clinicians.The NATUS algorithm incorporates
parental genotypic information, usesnumerous quality control metrics, anddetermines a sample-specific accuracyfor each interrogated chromo-some.9-12,15 Briefly, the algorithm con-siders parental genotypic information,crossover frequency data, and possiblefetal chromosome copy numbers(monosomy/disomy/trisomy) at 19,488evaluated polymorphic loci. Bycomparing the observed fetal allele dis-tributions from the sequencing data tothe predicted distributions, the algo-rithm determines the fetal ploidy statewith the maximum likelihood for eachinterrogated chromosome; thismaximum likelihood probability isincorporated into a risk score forreporting purposes.15 The NATUS al-gorithm is currently only validated forsingleton gestations. However, the algo-rithm is able to determine when cfDNAsequencing results do not match themodeled fetal copy numbers with a highlikelihood, and can identify the presenceof additional fetal haplotypes that indi-cate either fetal triploidy or the presenceof an undetected dizygotic multiple
MONTH 2014
� YMOB10068_proof � 21 October 2014 � 8:
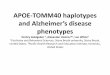
gestation. The presence of an additionalfetal haplotype was identified when alltested chromosomes failed to match thedisomy hypothesis, and when the addi-tional haplotype was apparent fromallele distributions. At this time, the al-gorithm cannot distinguish dizygotictwin gestations from triploidy pregnan-cies due to similar allele distributions(Figure 1 ½); therefore these are reportedas 1 call. Specifically, in a euploidsingleton pregnancy, where the maternalalleles are AA (with dimorphic allelesarbitrarily labeled as A and B), the 2expected fetal genotypes include AA andAB. By contrast, in dizygotic twin andtriploid pregnancies where the maternalalleles are AA, there are 3 expected fetalgenotypes for both triploid (AAA, AAB,ABB) (Figure 1, A) and dizygotic twin(AA/AA, AA/AB, AB/AB) (Figure 1, B)pregnancies. This results in equivalent Ballele distributions (0, 1, or 2 B alleles),and very similar A allele distributions intriploid (1, 2, or 3) and dizygotic twin (2,3, or 4) pregnancies.
For cases with an identified additionalfetal haplotype, a report was sent to theordering clinician or laboratory indi-cating that the results were consistentwith a possible triploid or vanishing twinpregnancy, and recommending follow-up counseling and testing; after reportdelivery, a Natera genetic counselorcontacted the ordering clinician/pro-vider to answer questions related to theNIPT findings.
Clinical outcomesFollow-up information on cases iden-tified with an additional fetal haplotypewas requested by telephone at regularintervals from ordering clinicians andpartner laboratories. All informationdetailing ultrasound findings andpregnancy outcomes were recorded inthe laboratory follow-up database.Follow-up information directly re-ported to Natera by providers was alsorecorded. Multifetal pregnancies wereconfirmed by ultrasound, which isconsistent with how they are clinicallydiagnosed in practice. Cases were cate-gorized as follows: (1) “confirmedvanishing twin pregnancy” if ultra-sound detected a second empty sac or
54 pm � ce

F2�
web4C=FPO
FIGURE 1TITLE Q6
13 18 21 X 1
0
Frac
tion
of A
alle
le re
ads
AA
BB
AB
AAA/AA (X)
ABB
Fetal Maternal
AAB/AB (X)
AAA
ABB AAB
BBB
AAB
BBB/BB(X) ABB/AB(X)
Y
AA(X) AB(X) BB(X)
13 18 21 X 1
0
Frac
tion
of A
alle
le re
ads
AA
BB
AB
AA/AA
AB/AB
Fetus 1/2 Maternal
AA/AB
AA/AA
AB/AB AA/AB
BB/AB BB/BB
AB/AB
BB/BB AB/BB
Y
Graphical representation of sequencing data obtained from A, 1 paternal triploidy sample and B, 1 vanishing twin sample. It is important to note that thisis not how algorithm makes copy number calls, but is 1 method for visualizing data. All interrogated single-nucleotide polymorphisms (SNPs) are
assumed to be dimorphic and are designated as A and B for simplicity. Briefly, for each graph, number of A allele reads as fraction of total reads is plotted
(y-axis) against position of each of several thousand interrogated SNPs on chromosomes of interest (x-axis). X-axis represents linear position of each SNP
along chromosome, and each spot corresponds to single SNP. As plasma cell-free DNA (cfDNA) is mixture of fetal and maternal cfDNA, vertical position of
each spot represents sum of contribution of both fetal and maternal allele reads, and is function of fetal fraction. To more readily visualize maternal and
fetal contributions, spots are colored according to maternal genotype: SNPs for which mother is homozygous for A allele (AA) are red, SNPs for which
mother is homozygous for B allele (BB) are blue, and SNPs for which mother is heterozygous (AB) are green. Since majority of plasma cfDNA is maternal in
origin, spots mainly distribute according to maternal genotype. Contribution of fetal allele reads results in segregation into distinct clusters. Because loci
targeted on Y chromosome are homologous to loci on X chromosome, but differ by 1 nucleotide, probes hybridize to both chromosomes. However,
targeted alleles have chromosomally distinct, nondimorphic identities, so are not color-coded; all alleles from X chromosome are assigned as A alleles,
and all alleles from Y chromosome are assigned as B alleles. A, Confirmed paternal triploidy, 22.6% fetal cfDNA fraction. Position of peripheral red and
blue clusters indicates additional haplotypes, as indicated to right of plot. Alleles for X chromosome are indicated (X). Presence of B alleles from Y
chromosome shifts cluster downward, indicating presence of single Y chromosome (based on distribution of reads). Together, this suggests fetal
chromosomal complement of 69,XXY. B, Confirmed vanishing twin, 19.6% fetal cfDNA fraction. Position of peripheral red and blue clusters indicates
additional haplotypes, as indicated to right of plot. Presence of B alleles from Y chromosome shifts cluster downward, indicating presence of single Y
chromosome (based on distribution of reads). Together, this suggests presence of vanishing twins, as indicated to right of plot; “Fetus 1/2” indicates
genotypes of fetus 1/fetus 2. Center green clusters only segregate and are readily visible at higher fetal fractions.
Curnow. SNP-based NIPT detects vanishing twin pregnancies. Am J Obstet Gynecol 2014.
ajog.org Obstetrics Research
223224225226227228229230231232233234235236237238239240241242243244245246247248249250251252253254255256257258259260261262263264265266267268269270271272273274275276277278
279280281282283284285286287288289290291292293294295296297298299300301302303304305306307308309310311312313314315316317318319320321322323324325326327328329330331332333334
second sac containing a deceased fetus;(2) “confirmed ongoing twin preg-nancy” if ultrasound showed an on-going and viable twin pregnancy; (3)“confirmed fetal triploidy” if triploidywas confirmed by invasive testing ortesting of products of conception(POC); (4) “unconfirmed fetal trip-loidy” included cases without invasivediagnostic testing but with ultrasoundfindings consistent with triploidy; (5)“confirmed nontriploid pregnancy”included cases where invasive diag-nostic testing ruled out fetal triploidyand there was no evidence of co-twindemise; (6) “pregnancy loss” for caseswhere patients experienced sponta-neous abortion and did not obtain
FLA 5.2.0 DTD
karyotype confirmation; or (7) “nofollow-up” where follow-up informa-tion was requested but was notreceived by the time of manuscriptsubmission.
Statistical analysisDifferences in the maternal age andgestational age between confirmedtwin and confirmed vanishing twin co-horts were determined using a Mann-Whitney rank sum test. A t test wasused to compare the fetal fraction inconfirmed twin and vanishing twincases. SigmaPlot 12.5 (Systat Software,San Jose, CA) was used for all statisti-cal analyses. A P value of < .05 wasconsidered statistically significant.
MONTH 2014 Am
� YMOB10068_proof � 21 October 2014 � 8:
Unless otherwise indicated, data arepresented as the mean � SD.
RESULTS
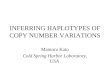
Study participants and samplesIn the present cohort of 30,795 caseswith an NIPT result, 130 (0.42%)received a report indicating the presenceof additional fetal haplotypes. For thewhole cohort, the mean maternal agewas 33.6 � 6.1 (range, 13.0e63.0) years(Figure 2 ½, A), and the mean gestationalage was 14.5 � 4.7 (range, 9.0e40.9)weeks (Figure 2, B); maternal age wasconfirmed for the single case with amaternal age >52 years. For the 130cases where an additional fetal haplotypewas identified by NATUS, the mean
erican Journal of Obstetrics & Gynecology 1.e355 pm � ce

½F3� ½T1�
web4C=FPO
FIGURE 2Maternal age and gestational age histograms
Maternal age (years)
15 20 25 30 35 40 45 50 55 60
Cou
nt
0
500
1000
1500
2000
2500
3000
3500
Gestational age (weeks)
10 15 20 25 30 35 40
Cou
nt
0
1000
2000
3000
4000
5000
6000
Maternal age (years)
15 20 25 30 35 40 45 50 55 60
Cou
nt
0
5
10
15
20
25
30
Gestational age (weeks)
10 15 20 25 30 35 40
Cou
nt
0
5
10
15
20
25
30
A, Maternal and B, gestational age histograms for whole cohort. C, Maternal and D, gestational age histograms for cases with identified additional fetal
haplotypes. Although not apparent because of scale of Y-axis, within whole cohort there were 8 cases with maternal ages of 49-63 years; maternal age
was confirmed for single case with maternal age of >52 years.
Curnow. SNP-based NIPT detects vanishing twin pregnancies. Am J Obstet Gynecol 2014.
Research Obstetrics ajog.org
335336337338339340341342343344345346347348349350351352353354355356357358359360361362363364365366367368369370371372373374375376377378379380381382383384385386387388389390
391392393394395396397398399400401402403404405406407408409410411412413414415416417418419420421422423424425426427428429430431432433434435436437438439440441442443444445446
maternal age was 34.3 � 5.7 (range,19.0e52.0) years (Figure 2, C), and themean gestational age was 13.3 � 4.1(range, 9.0e38.0) weeks (Figure 2, D).While the majority of NIPT sampleswere from women at early gestationalages, samples were received up to 40weeks’ gestation (Figure 3); 2% (658/30,795) of samples were from women intheir third trimester.
Clinical outcomesKaryotype or ultrasound confirmation(karyotype for singleton pregnancies,ultrasound for multifetal pregnancies)
1.e4 American Journal of Obstetrics & Gynecology
FLA 5.2.0 DTD
was available for 76 (58.5%) of the 130cases identified with additional parentalhaplotypes. This included 32 (42.1%)vanishing twin, 37 (48.7%) viable twin, 4(5.3%) triploid pregnancies, and 3(3.9%) nontriploid pregnancies thatlacked evidence of co-twin demise(Table 1). For the 3 nontriploid preg-nancies, 2 had euploid karyotypes, and 1was shown to be a trisomy 18 fetus(Appendix; Supplementary Table).
Multifetal pregnanciesVanishing twin cases had a significantlyhigher median maternal age than twin
MONTH 2014
� YMOB10068_proof � 21 October 2014 � 8:
cases, 37.5 and 33.0 years, respectively(P < .001). The median gestational agewas slightly lower in vanishing twin casesthan in twin cases, 12.1 and 13.0 weeks,respectively (P ¼ .018). There was nosignificant difference (P¼ .686) betweenthe average fetal fraction of vanishedtwin (11.0 � 3.8%) and twin (11.4 �4.3%) pregnancies. Of the 32 vanishingtwin cases, 25 (78.1%) were in the firsttrimester and 7 (21.9%) were in thesecond trimester at the time of NIPTsampling. Five cases reported an esti-mated date of fetal demise: demiseoccurred in the first trimester in all 5
55 pm � ce

½T2�
½T3�
web4C=FPO
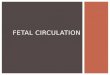
FIGURE 3Graphical representation of timeelapsed between estimated fetaldemise and detection by NIPT for5 confirmed vanishing twincases
Gestational Age (weeks)
4 6 8 10 12 14 16 18
NIPTFetal Demise
NIPT
Fetal Demise NIPT
Fetal Demise NIPT
Fetal Demise NIPT
Fetal Demise
Each line indicates individual confirmed van-
ishing twin case with known estimated date of
fetal demise. Longest period between fetal
demise and NIPT was 8 weeks.
NIPT, noninvasive prenatal testing.
Curnow. SNP-based NIPT detects vanishing twin pregnan-cies. Am J Obstet Gynecol 2014.
TABLE 1Follow-up information on twins/triploidy callsAll cases (n [ 130a) Value
Multifetal pregnancies
Ongoing twinb 37
Vanishing twinb 32
Singleton pregnancies
Confirmed triploidc 4
Unconfirmed triploid 1d
Confirmed nontriploid 3e
Unknown fetal no.
Pregnancy lossf 3
No follow-upg 50
a Total no. of cases with “additional fetal haplotypes”(twins/triploidy) result at �9 wk of gestation; b Con-firmed by ultrasound detection of multifetal preg-nancy; c Confirmed by karyotype; d Patient hadultrasound findings that were consistent with triploidfetus, amniocentesis was not possible because ofoligohydramnios; e Invasive testing revealed singleeuploid fetus in 2 pregnancies and single trisomy 18fetus in 1 pregnancy; f Patient experienced sponta-neous abortion and did not obtain karyotype confir-mation, ultrasound was suggestive of singletonpregnancy; g Follow-up information was not available.
Curnow. SNP-based NIPT detects vanishing twinpregnancies. Am J Obstet Gynecol 2014.
ajog.org Obstetrics Research
447448449450451452453454455456457458459460461462463464465466467468469470471472473474475476477478479480481482483484485486487488489490491492493494495496497498499500501502
503504505506507508509510511512513514515516517518519520521522523524525526527528529530531532533534535536537538539540541542543544545546547548549550551552553554555556557558
cases (Figure 3). The time betweendemise and NIPT sampling ranged from2-8 weeks (Table 2).
Triploid pregnanciesAll triploidy cases in this cohort weredetermined to be diandric (Table 3),indicating that in each case the addi-tional fetal haplotype was paternal inorigin. Fetal sex was determined for alltriploidy cases by analysis of fetal sexchromosome copy numbers; the fetalkaryotype matched the fetal sex deter-mined by NIPT for all 3 triploidy caseswhere karyotype specifics were commu-nicated during follow-up (Table 3).For triploidy cases 1, 2, and 4 detailed inTable 3, the pregnancies spontaneouslyaborted and karyotype confirmationwas obtained from the POC; duringclinical follow-up, 2 of these cases werereported as partial mole pregnancies. Fortriploidy cases 3 and 5 (Table 3), clinicalevaluation identified large placentasand oligohydramnios in both cases.
COMMENT
This SNP-based NIPT approach identi-fied previously undetected twin andtriploid pregnancies in women under-going routine prenatal screening. Thismethod was previously validated for
FLA 5.2.0 DTD
detecting fetal trisomy 21, trisomy 18,trisomy 13, monosomy X, and sexchromosome trisomies in singletonpregnancies, as well as additional fetalhaplotypes indicating twin or triploidpregnancies.9-12 This is the first reportdetailing the clinical outcomes followingNIPT identification of additional fetalhaplotypes in a large general screeningpopulation.Because this SNP-based method ana-
lyzes polymorphic loci, incorporatesgenotypic information, and does notrequire a reference chromosome, it isuniquely able to detect the presence ofadditional fetal haplotypes associatedwith dizygotic twins and triploidy.However, this method is currently un-able to distinguish between these possi-bilities. Ultrasound examination shouldreadily distinguish between an ongoingtwin and a singleton pregnancy, andmayreveal the presence of a vanished twin. Aconfirmed ongoing twin pregnancy maywarrant close monitoring of the preg-nancy, as twin pregnancies involve aunique set of complications16,17; theadditional haplotype merely suggestsdizygotic twins. In the case of aconfirmed singleton pregnancy withNIPT-identified additional haplotypes,options include repeat NIPT, taking await-and-see approach, or follow-updiagnostic testing to rule out triploidy;invasive testing should be carefullyconsidered in light of other indicationsgiven the inherent risks to mother andbaby.18 Where ultrasound indicates asingleton pregnancy and where triploidyindications are lacking, or where invasivetesting ruled out triploidy, the possibilityof early and undetected co-twin demisecannot be ruled out. Most vanishingsoccur in the first trimester,19 so clinicaldetection is largely dependent onwhether a patient receives an early ul-trasound and the time of fetal demise.Thus, for patients electing NIPT, an ul-trasound may provide helpful informa-tion to assess fetal number and detect thepresence of a vanishing twin or fetaltriploidy.The ability to detect vanished twins is
clinically important. Specifically, theincreased rate of abnormalities invanished twins is likely to generate
MONTH 2014 Am
� YMOB10068_proof � 21 October 2014 � 8:
false-positive results when usingmethods that can only asses total DNAand are unable to detect additionalhaplotypes. Indeed, 2 recent studies us-ing counting-based methods attributed asignificant proportion of false positivesto vanishing twins: in 1 study 15% ofNIPT false-positive results were shownto involve vanished twins,14 and in asecond study 33% (1/3) of trisomy 21false positives were attributed to van-ishing twins.20 Additionally, a vanishedtwin with discordant fetal sex may leadto the incorrect NIPT-based identifica-tion of fetal sex when compared to ul-trasound (eg, a female fetus where thereis a male vanished twin may be identifiedas male via NIPT). Both circumstanceslead to parental anxiety and may escalateto unnecessary invasive testing, whichcarries with it a small but real risk ofharm to mother and fetus.18
Similarly, identification of triploidpregnancies is beneficial because of thesubstantial clinical implications for
erican Journal of Obstetrics & Gynecology 1.e555 pm � ce

TABLE 2Case details for confirmed vanishing twin cases
CaseGA atdemise, wk
GA atNIPT, wk
Time from demiseto NIPT, wk Fetal fraction
1 8.0 10.3 2.3 11.7%
2 7.1 10.4 3.3 4.6%
3 8.6 12.6 4.0 12.8%
4 8.0 14.7 6.7 11.8%
5 7.0 15.0 8.0 8.1%
GA at estimated date of co-twin demise and at time of sample collection for NIPT, elapsed time between estimated demise andNIPT sampling, and fetal fraction for confirmed vanishing twin cases where clinical follow-up provided estimated date of fetaldemise.
GA, gestational age; NIPT, noninvasive prenatal testing.
Curnow. SNP-based NIPT detects vanishing twin pregnancies. Am J Obstet Gynecol 2014.
Q7
Research Obstetrics ajog.org
559560561562563564565566567568569570571572573574575576577578579580581582583584585586587588589590591592593594595596597598599600601602603604605606607608609610611612613614
615616617618619620621622623624625626627628629630631632633634635636637638639640641642643644645646647648649650
patients. Triploidy results in severe fetalabnormalities and elevated risks forspontaneous abortion, preeclampsia,excessive postdelivery bleeding, andgestational trophoblastic neoplasia.21,22
As such, timely detection of triploidcases may alter clinical management.The incorporation of parental genotypicinformation allowed for determinationof parental origin; all cases in this studywere diandric triploidy. Clinically, thesecases would likely present as partialmolar pregnancies, which would be atrisk for gestational trophoblasticneoplasia and choriocarcinoma, a ma-lignant trophoblastic cancer.23-25
Digynic triploidies should also bedetectable with this SNP-based method.
TABLE 3Case details for triploidy cases
Case
NIPT findings
Fetal fractionParent oforigina
Predicsex
1 5.1% Diandric XXX
2 11.4% Diandric XXY
3 22.6% Diandric XXY
4 12.2% Diandric XXY
5 6.4% Diandric XXX
a Parent of origin of extra fetal haplotype, as determined by NIPT;clinical follow-up; c Amniocentesis was not possible becausewith triploid fetus.
NIPT, noninvasive prenatal testing.
Curnow. SNP-based NIPT detects vanishing twin pregnanc
1.e6 American Journal of Obstetrics & Gynecology
FLA 5.2.0 DTD
However, these pregnancies present withvery small, nonmolar placentas,26 whichis correlated with decreased fetal cfDNAfractions and complicates detection us-ing NIPT.10 However, previous studiesshowed that an “extremely low fetalfraction” per se increased the risk of fetalchromosomal aneuploidy, includingdigynic triploidy.10,12
The prevalence of twin pregnancies isapproximately 1 in 30 births,27,28 withvanishing twins occurring in approxi-mately 30% of early diagnosed twinpregnancies.29-33 This is substantiallyhigher than for triploid pregnancies,which occur in approximately 1 in 2000pregnancies at 12 weeks of gestation,when many women undergo NIPT.34,35
Clinical outcomes
tedResult Karyotype
Triploidy 69,XXX
Triploidy 69,XXY
Triploidy N/Ab
Triploidy 69,XXY
Unconfirmedtriploidyc
b Detailed karyotype findings were not communicated duringof oligohydramnios, but ultrasound findings were consistent
ies. Am J Obstet Gynecol 2014.
MONTH 2014
651652653654655656657658659660661662663664665666667668669670
� YMOB10068_proof � 21 October 2014 � 8:
Thus, the substantially greater possibil-ity of a vanishing twin pregnancy (orunrecognized multiple gestation) shouldnot be overlooked upon a screen-positive result.
The increased incidence of twinningin developed countries, a reflection ofthe progressive rise in the averagematernal age at the time of concep-tion36,37 and increasing utilization ofassisted reproductive technology(ART),27 has important clinical impli-cations for prenatal screening. Specif-ically, twinning rates are higher inwomen using ART, so the proportion ofvanishing twin pregnancies is also likelyhigher. Indeed, 9% of conceptions usingintracytoplasmic sperm injection resul-ted in vanishing twin pregnancies.38
However, it is unclear how manywomen in this cohort used ART; thenumber of cases found to involve avanishing twin was 0.18% (additionalfetal haplotypes were identified in 0.42%of the 30,795 cases, and of those caseswith clinical follow-up, 42.7% werevanishing twin pregnancies, for 0.42%�42.7%). It may be reasonable to assumethat the rate of aneuploidy among van-ished twins is similar to that found inanalysis of POC samples, which was re-ported to be about 60%.39,40 This im-plies that approximately 0.11% of NIPTcases involve a chromosomally abnormalvanishing twin. As this is the same orderof magnitude as NIPT false-positiverates, it is not surprising that vanishingtwins have been found to be responsiblefor a significant proportion of falsepositives in some studies14,20 using NIPTmethods that cannot detect vanishedtwins. Determining a more precise cor-relation between vanishing twins andaneuploidy as well as fetal fraction is animportant area for ongoing research, butis beyond the scope of this present study.
In this cohort, the average maternalage was significantly higher in confirmedvanishing twin than in confirmedongoing twin pregnancies, which isconsistent with the increased risk forfetal aneuploidies associated withincreasing maternal age. This suggeststhat increased rates of fetal aneuploidymay underlie the losses in the vanishingtwin cohort. Vanishing twin and
55 pm � ce

5
ajog.org Obstetrics Research
671672673674675676677678679680681682683684685686687688689690691692693694695696697698699700701702703704705706707708709710711712713714715716717718719720721722723724725726
727728729730731732733734735736737738739740741742743744745746747748749750751752753754755756757758759760761762763764765766767768769770771772773774775776777778779780781782
ongoing twin pregnancies could not bedistinguished by fetal fractions. Of note,algorithm estimates of fetal fraction arebased on a methodology validated insingleton pregnancies, and have not beenindependently validated in twin preg-nancies. Ongoing clinical studies arefocused on validating aneuploidy riskdetermination in multifetal pregnanciesusing this SNP-based technology.
It is unclear how long after demise theplacenta from a vanished twin maycontribute fetal cfDNA to maternal cir-culation. This is likely governed by therate of placental tissue autolysis and thegestational age of the fetus at the time ofdemise. Studies in singleton pregnancieshave shown that fetal cfDNA levels were5-fold higher in women at the time ofclinical recognition of spontaneousabortion than in women of the samegestational age with an ongoing preg-nancy,41 and remained elevated for atleast 7 days after spontaneous abortiondiagnosis.42 Further, this effect was morepronounced in chromosomallyabnormal spontaneous abortions than inspontaneous abortions with a normalkaryotype.42 As such, it is quite possiblethat in a multifetal pregnancy there maybe a similarly increased cfDNA contri-bution from a vanished twin immedi-ately following the loss, thuscompromising cfDNA screening resultsfor the viable twin. In the results re-ported here, fetal cfDNA from a van-ished twin was detectable for up to 8weeks following co-twin demise. Thus,there is the potential for vanished twinsto influence NIPT results long after co-twin demise.
A limitation of this study was incom-plete follow-up, reflecting the reality thatmany patients do not receive a first-trimester ultrasound or may transfercare. Nevertheless, where data were re-ported, the presence of additional fetalhaplotypes determined by NIPT wasconfirmed in the vast majority of casesby ultrasound detection of a multifetalpregnancy or karyotype confirmation offetal triploidy.
This SNP-based NIPT identified van-ishing twin, unrecognized ongoing twin,and triploid pregnancies. Identificationof partial (triploidy) and complete molar
FLA 5.2.0 DTD
pregnancies is important because of thesubstantial clinical implications for pa-tients, including the risk for gestationaltrophoblastic neoplasia and choriocar-cinoma. As vestigial placental tissue froma lost twin can contribute fetal cfDNA tomaternal circulation for weeks post-demise, identification of vanishing twinpregnancies is critical to avoid incorrectNIPT results and subsequent unnec-essary invasive procedures when non-SNP-based NIPTmethods are used.
ConclusionThe principal finding of this study wasthat SNP-based NIPT can uniquelydetect triploidy and unrecognized mul-tifetal pregnancies, including vanishingtwins, within a general screening popu-lation. Clinical outcomes revealed thatthe majority of these cases were unrec-ognized multifetal pregnancies, ongoingor vanishing twins, with a small numberof triploid pregnancies also detected.The ability to detect vanishing twinpregnancies is clinically important as itwill reduce the number of false-positiveresults and thereby reduce unnecessaryinvasive diagnostic procedures. Futurelongitudinal studies, designed to eval-uate the typical time period for whichresidual fetal cfDNA from vanishingtwins remains detectable, may providegreater insight into appropriate clinicalcare in these patients. -
REFERENCES
1. Bianchi DW, Platt LD, Goldberg JD,Abuhamad AZ, Sehnert AJ, Rava RP. Genome-wide fetal aneuploidy detection by maternalplasma DNA sequencing. Obstet Gynecol2012;119:890-901.2. Palomaki GE, Deciu C, Kloza EM, et al. DNAsequencing of maternal plasma reliably identifiestrisomy 18 and trisomy 13 as well as Downsyndrome: an international collaborative study.Genet Med 2012;14:296-305.3. Palomaki GE, Kloza EM, Lambert-Messerlian GM, et al. DNA sequencing ofmaternal plasma to detect Down syndrome: aninternational clinical validation study. Genet Med2011;13:913-20.4. Ashoor G, Syngelaki A, Wagner M, Birdir C,Nicolaides KH. Chromosome-selectivesequencing of maternal plasma cell-free DNA forfirst-trimester detection of trisomy 21 and tri-somy 18. Am J Obstet Gynecol 2012;206:322.e1-5.
MONTH 2014 Am
� YMOB10068_proof � 21 October 2014 � 8:
5. AshoorG, Syngelaki A,WangE, et al. Trisomy13 detection in the first trimester of pregnancyusing a chromosome-selective cell-free DNAanalysis method. Ultrasound Obstet Gynecol2013;41:21-5.6. Norton ME, Brar H, Weiss J, et al. Non-invasive chromosomal evaluation (NICE) study:results of a multicenter prospective cohortstudy for detection of fetal trisomy 21 and tri-somy 18. Am J Obstet Gynecol 2012;207:137.e1-8.7. Sparks AB, Struble CA, Wang ET, Song K,Oliphant A. Noninvasive prenatal detection andselective analysis of cell-free DNA obtained frommaternal blood: evaluation for trisomy 21 andtrisomy 18. Am J Obstet Gynecol 2012;206:319.e1-9.8. Sparks AB, Wang ET, Struble CA, et al. Se-lective analysis of cell-free DNA in maternalblood for evaluation of fetal trisomy. PrenatDiagn 2012;32:3-9.9. Nicolaides KH, Syngelaki A, Gil M,Atanasova V, Markova D. Validation of targetedsequencing of single-nucleotide polymorphismsfor non-invasive prenatal detection of aneuploidyof chromosomes 13, 18, 21, X, and Y. PrenatDiagn 2013;33:575-9.10. Nicolaides KH, Syngelaki A, Gil MD,Quezada MS, Zinevich Y. Prenatal detection offetal triploidy from cell-free DNA testing inmaternal blood. Fetal Diagn Ther 2014;35:212-7.11. Samango-Sprouse C, Banjevic M, Ryan A,et al. SNP-based non-invasive prenatal testingdetects sex chromosome aneuploidies with highaccuracy. Prenat Diagn 2013;33:643-9.12. Pergament E, Cuckle H, Zimmermann B,et al. Single-nucleotide polymorphism-basednoninvasive prenatal testing in a high-risk andlow-risk cohort. Obstet Gynecol 2014;124:210-8.13. Zimmermann B, Hill M, Gemelos G, et al.Noninvasive prenatal aneuploidy testing ofchromosomes 13, 18, 21, X, and Y, using tar-geted sequencing of polymorphic loci. PrenatDiagn 2012;32:1233-41.14. Futch T, Spinosa J, Bhatt S, de Feo E,Rava RP, Sehnert AJ. Initial clinical laboratoryexperience in noninvasive prenatal testing forfetal aneuploidy from maternal plasma DNAsamples. Prenat Diagn 2013;33:569-74.15. Dar P, Curnow KJ, Zimmermann B, et al.Clinical experience and follow-up with largescale single-nucleotide polymorphism-basednoninvasive prenatal aneuploidy testing. Am JObstet Gynecol 2014. Q
16. Spellacy WN, Handler A, Ferre CD. A case-control study of 1253 twin pregnancies from a1982-1987 perinatal data base. Obstet Gynecol1990;75:168-71.17. Ananth CV, Chauhan SP. Epidemiology oftwinning in developed countries. Semin Perinatol2012;36:156-61.18. American College of Obstetricians and Gy-necologists. Invasive prenatal testing for aneu-ploidy. ACOG Practice bulletin no. 88. ObstetGynecol 2007;110:1459-67.
erican Journal of Obstetrics & Gynecology 1.e755 pm � ce

Research Obstetrics ajog.org
783784785786787788789790791792793794795796797798799800801802803804805806807808809810811812813814815816817818819820821822823824825826827828829830831832833834835836837838
839840841842843844845846847848849850851852853854855856857858859860861862863864865866867868869
19. Manzur A, Goldsman MP, Stone SC,Frederick JL, Balmaceda JP, Asch RH.Outcome of triplet pregnancies after assistedreproductive techniques: how frequent are thevanishing embryos? Fertil Steril 1995;63:252-7.20. Porreco RP, Garite TJ, Maurel K, et al.Noninvasive prenatal screening for fetal tri-somies 21, 18, 13 and the common sex chro-mosome aneuploidies from maternal bloodusing massively parallel genomic sequencing ofDNA. Am J Obstet Gynecol 2014;211:365.e1-12.21. Rijhsinghani A, Yankowitz J, Strauss RA,Kuller JA, Patil S, Williamson RA. Risk of pre-eclampsia in second-trimester triploid pregnan-cies. Obstet Gynecol 1997;90:884-8.22. Seckl MJ, Sebire NJ, Berkowitz RS.Gestational trophoblastic disease. Lancet2010;376:717-29.23. Joergensen MW, Niemann I,Rasmussen AA, et al. Triploid pregnancies, ge-netic and clinical features of 158 cases. Am JObstet Gynecol 2014;211:370.e1-19.24. Zaragoza MV, Surti U, Redline RW, Millie E,Chakravarti A, Hassold TJ. Parental origin andphenotype of triploidy in spontaneous abortions:predominance of diandry and association withthe partial hydatidiform mole. Am J Hum Genet2000;66:1807-20.25. Lurain JR. Gestational trophoblastic diseaseI: epidemiology, pathology, clinical presentationand diagnosis of gestational trophoblastic dis-ease, and management of hydatidiform mole.Am J Obstet Gynecol 2010;203:531-9.26. Sergi C, Schiesser M, Adam S, Otto HF.Analysis of the spectrum of malformations inhuman fetuses of the second and third trimester
1.e8 American Journal of Obstetrics & Gynecology
FLA 5.2.0 DTD
of pregnancy with human triploidy. Pathologica2000;92:257-63.27. Centers for Disease Control and PreventionASfRM, Technology SfAR. 2010 Assistedreproductive technology national summaryreport. Atlanta, GA: US Department of Healthand Human Services, Centers for DiseaseControl and Prevention; 2012.28. Martin JA, Hamilton BE, Osterman MLK.Three decades of twin births in the UnitedStates, 1980e2009. Hyattsville, MD: NationalCenter for Health Statistics, Centers for DiseaseControl and Prevention; 2012.29. Sampson A, de Crespigny LC. Vanishingtwins: the frequency of spontaneous fetalreduction of a twin pregnancy. UltrasoundObstet Gynecol 1992;2:107-9.30. Landy HJ, Weiner S, Corson SL, Batzer FR,Bolognese RJ. The “vanishing twin”: ultrasono-graphic assessment of fetal disappearance inthe first trimester. Am J Obstet Gynecol1986;155:14-9.31. Landy HJ, Keith LG. The vanishing twin: areview. Hum Reprod Update 1998;4:177-83.32. Kelly MP, Molo MW, Maclin VM,Binor Z, Rawlins RG, Radwanska E. Humanchorionic gonadotropin rise in normal andvanishing twin pregnancies. Fertil Steril1991;56:221-4.33. Dickey RP, Taylor SN, Lu PY, et al. Spon-taneous reduction of multiple pregnancy: inci-dence and effect on outcome. Am J ObstetGynecol 2002;186:77-83.34. Snijders RJ, Sebire NJ, Nicolaides KH.Maternal age and gestational age-specific riskfor chromosomal defects. Fetal Diagn Ther1995;10:356-67.
MONTH 2014
� YMOB10068_proof � 21 October 2014 � 8:
35. Jacobs PA, Angell RR, Buchanan IM,Hassold TJ, Matsuyama AM, Manuel B. Theorigin of human triploids. Ann Hum Genet1978;42:49-57.36. Mathews TJ, Hamilton BE. Mean age ofmother, 1970e2000, Vol 51. Hyattsville,MD: National Center for Health Statistics,Centers for Disease Control and Prevention;2002.37. Mathews TJ, Hamilton BE. Delayed child-bearing: more women are having their first childlater in life. Hyattsville, MD: National Center forHealth Statistics, Centers for Disease Controland Prevention; 2009.38. Mansour R, Serour G, Aboulghar M,Kamal O, Al-Inany H. The impact of vanishingfetuses on the outcome of ICSI pregnancies.Fertil Steril 2010;94:2430-2.39. Lathi RB, Gustin SL, Keller J, et al. Reliabilityof 46,XX results on miscarriage specimens: areview of 1,222 first-trimester miscarriagespecimens. Fertil Steril 2013;101:178-82.40. Levy B, Sigurjonsson S, Pettersen B, et al.Genomic imbalance in products of conception:single nucleotide polymorphism chromosomalmicroarray analysis. Obstet Gynecol 2014;124:202-9.41. Yin A, Ng EH, Zhang X, He Y, Wu J,Leung KY. Correlation of maternal plasma totalcell-free DNA and fetal DNA levels with shortterm outcome of first-trimester vaginal bleeding.Hum Reprod 2007;22:1736-43.42. Lim JH, Kim MH, Han YJ, et al. Cell-freefetal DNA and cell-free total DNA levels inspontaneous abortion with fetal chromo-somal aneuploidy. PLoS One 2013;8:e56787.
870871872873874875876877878879880881882883884885886887888889890891892893894
55 pm � ce

ajog.org Obstetrics Research
895896897898899900901902903904905906907908909910911912913914915916917918919920921922923924925926927928929930931932933934935936937938939940941942943944945946947948949950
951952
APPENDIXSUPPLEMENTARY TABLEConfirmation methods for patients with diagnostic testsCase Outcome Method
1 Triploidy CVS
2, 3, 4 Triploidy POC
5 Euploid Amniocentesis
6 Euploid CVS
7 Trisomy 18 CVS
CVS, chorionic villus sampling; POC, products of conception testing.
Curnow. SNP-based NIPT detects vanishing twin pregnancies. Am J Obstet Gynecol 2014.
MONTH 2014 American Journal of Obstetrics & Gynecology 1.e9
9539549559569579589599609619629639649659669679689699709719729739749759769779789799809819829839849859869879889899909919929939949959969979989991000100110021003100410051006
FLA 5.2.0 DTD � YMOB10068_proof � 21 October 2014 � 8:55 pm � ce