Embed Size (px)
Citation preview

Polymorphisms and Haplotypes of the Regulator ofG Protein Signaling-2 Gene in Normotensives
and HypertensivesEvan L. Riddle, Brinda K. Rana, Kenton K. Murthy, Fangwen Rao, Eleazar Eskin,
Daniel T. O’Connor, Paul A. Insel
Abstract—Regulator of G protein signaling (RGS) proteins stimulate the GTPase activity of G� subunits of heterotrimericG proteins, thereby negatively regulating G protein-coupled receptor signaling. RGS2, which preferentially altersG�q-mediated signaling, may be important for cardiovascular health, because knockout of RGS2 in mice is associatedwith altered smooth muscle relaxation and hypertension. In this study, we determined genetic variation in the humanRGS2 gene by sequencing DNA in normotensive and hypertensive populations of whites (n�128) and blacks (n�122).We identified 14 single nucleotide polymorphisms and 2 two-base insertion/deletions (in/del; 1891 to 1892 TC and 2138to 2139 AA). Although most of the genetic variants were found at low allelic frequency, in particular in coding regions,the 1891 to 1892 TC and 2138 to 2139 AA intronic in/del were in linkage disequilibrium and were associated withhypertension in blacks (P�0.05). We defined several haplotypes for the RGS2 gene, certain of which showed strikingdifferences between whites and blacks. Additionally, 2 haplotypes had significantly different frequencies betweenhypertensive and normotensive black groups (P�0.05). We conclude that RGS2 is genetically conserved within codingregions but that the intronic in/del define ethnicity-specific haplotypes. Moreover, certain RGS2 variants that occur atgreater frequency in hypertensive blacks may serve as ethnicity-specific genetic variants for this disease. (Hypertension.2006;47:1-6.)
Key Words: hypertension, genetic � G proteins � signal transduction � blood pressure
G protein–coupled receptor (GPCR) signaling via hetero-trimeric G proteins and G protein–regulated effector
molecules is critical for normal cardiovascular function, andabnormalities in GPCR signaling have been noted in numer-ous cardiovascular disorders.1–3 Moreover, a wide variety ofdrugs that are effective in the treatment of cardiovasculardisorders target GPCRs. Regulators of G protein signaling(RGS) proteins negatively regulate GPCR signaling by ac-celerating the inactivation of G� proteins by stimulation oftheir GTPase-activating protein (GAP) activity. From a con-ceptual standpoint, RGS proteins have the potential to beimportant in cardiovascular physiology because of theirmodulation of GPCR signaling. Indeed, RGS proteins haveemerged as important components of the cardiovascularsystem. Among the �30 known RGS proteins, �20 areexpressed in the heart and vasculature.4,5
Recently, numerous reports6–9 have demonstrated an im-portant role for RGS2 in cardiovascular regulation. Specifi-cally, the data provide evidence that (1) RGS2 is required fornormal vascular function and blood pressure7; (2) RGS2-deficient mice exhibit a hypertensive (HT) phenotype6; (3)
RGS2 is involved in NO/cGMP-mediated vascular relax-ation8; and (4) both peripheral vascular mechanisms, as wellas a central nervous system mechanism, may be involved.9
Heximer et al6 have demonstrated that both rgs2�/� andrgs2�/� mice are HT, suggesting that genetic variation inRGS2 function or expression may be a risk factor for thedevelopment of hypertension in humans. In the present study,we set out to test the hypothesis that genetic variation inRGS2 is associated with human hypertension.
MethodsSubjects and DNA SamplesA cohort of 250 HT and normotensive (NT) subjects was recruitedfor this study by advertisement and referral from a general popula-tion in the San Diego area, as well as a hypertension specialty clinic.Seated blood pressure (BP) was measured in triplicate with acalibrated oscillometric device (Dinamap, Critikon). NT subjectswere healthy, based on laboratory tests and clinical history. HTpatients were ascertained from outpatient clinics of University ofCalifornia San Diego/Veteran’s Administration, either hypertensionspecialty clinic or primary care (general internal medicine) clinic. Allof the patients had a diagnosis of hypertension based on repeated BPmeasurements in the outpatient clinic, in the seated position, using
Received September 23, 2005; first decision October 12, 2005; revision accepted November 20, 2005.From the Departments of Pharmacology (E.L.R., D.T.O., P.A.I.), Medicine (F.R., D.T.O., P.A.I.), Psychiatry (B.K.R., K.K.M.), and Computer Science
and Engineering (E.E.), University of California San Diego, La Jolla.Correspondence to Paul A. Insel, University of California San Diego, Department of Pharmacology, 9500 Gilman Drive, La Jolla, CA 92093. E-mail
[email protected]© 2006 American Heart Association, Inc.
Hypertension is available at http://www.hypertensionaha.org DOI: 10.116110.1161/01.HYP.0000200714.81990.61
1
by guest on March 24, 2018
http://hyper.ahajournals.org/D
ownloaded from

aneroid manometers operated by trained nurses. Secondary hyperten-sion was excluded by history, examination, and screening laboratoryevaluation. Among the HT patients, 64% were receiving anti-HTmedications. As is common in random populations, the age, bodymass index, and body surface area were slightly higher in the HTgroup when compared with the NT controls. However, none of theRGS2 variants were significantly associated with age, body massindex, or body surface area (data not shown).
DNA samples were obtained with informed consent that wasapproved by the University of California San Diego Human SubjectsCommittee. Genomic DNA from 250 unrelated human individuals(white and black) was extracted from 10-mL mouthwash usingGentra’s PureGene DNA Purification kit (Gentra Systems Inc)according to the manufacturer’s protocol. Ethnicity of the subjectswas determined by self-identification and identification of bothparents and all 4 grandparents. Amplification of genomic DNA wascarried out on 5-ng samples and 2 H2O-negative controls usingGenomiPhi DNA Amplification kit (Amersham Biosciences) ac-cording to the recommended protocol.10
PCR and Sequencing ReactionsPCR reactions were performed in MJ Research Dyad thermalcyclers. Four sets of oligonucleotide primers were designed togenerate overlapping fragments of RGS2 (Genbank: NT_004671.15)sequence: (1) 5�-CACTGAAGACTCTCCATCTGC-3� and 5�-GGT-TAAATCTGGGTGATGCTC-3�; (2) 5�-AGTTCTTGCTTTGCC-TTATGC-3� and 5�-GAACCAGACCACACAATATCACC-3�; (3)5�-CCTGCA TCTCACACTCATCG-3� and 5�-CTTTATTTCCCA-GGGTTTAAC-3�; and (4) 5�-AGCACAATCTGGACATCTTTAGC-3�and 5�-GGTAGTGAATCAGGAAGCCAGTA-3�.
Twenty-five–�L PCR reactions were performed using 25 ng ofDNA (or H2O for negative controls), 25 mmol/L of MgCl2,10 mmol/L of 2�-deoxynucleoside 5�-triphosphates, 20 �mol/L ofprimer, and 0.5 U/reaction of Amplitaq Gold TaqDNA Polymerase(Applied Biosystems). Taq polymerase was heat activated by incu-bation at 95°C for 15 minutes. The reaction was cycled 40 times witha denaturation step of 95°C for 30 seconds, an annealing step of65.8°C for 1 minute, an elongation step of 72°C for 1 minute, and afinal elongation step of 72°C for 8 minutes. Verification of theidentity of the amplified PCR product (or the absence of amplifiedproduct in negative controls) was by electrophoresis on a 1% agarosegel. PCR products (15 �L) were purified with exonuclease I (3U/reaction) and shrimp alkaline phosphatase (0.8 U/reaction) byincubation at 37°C for 30 minutes and then at 85°C for 15 minutes.
Sequencing reaction was performed according to Applied Biosys-tem BigDye Terminator v3.1 Cycle Sequencing Kit Protocol (2002).Sequencing reaction was purified using Sephadex G-50 DNA Gradebeads (Sigma Scientific). Ten �L of Hi-Di Formamide was added tothe purified sequencing reaction. Sequencing was performed on anABI Prism 3100 Genetic Sequencer (Applied Biosystems).
Data AnalysisThe Phred, Phrap, Consed suite of sequence analysis software wasused to automate base calling, assemble sequence fragments, andvisualize sequence data. PolyPhred was used to detect heterozygoussites; SNPs and insertion/deletion (in/del) polymorphisms werereverified via Consed graphical interface and manually on the ABIchromatogram. Haplotype analysis was performed on Phase v.2analysis software.11–13 HAP-Haplotype Resolution 3.0 was used toinfer the phylogenic relationship of haplotypes.14 ANOVA was usedto determine whether significant differences existed in physiologicalmeasures between genotypes. �2 analysis was used to determineethnic specificity of variants, as well as association of variants withdichotomous NT and HT phenotypes.
ResultsThe entire coding region of RGS2 was sequenced fromgenomic DNA isolated from 250 unrelated individuals (Table1). The sample population consisted of 128 white (73 NT and
55 HT) and 122 black (62 NT and 60 HT) individuals. Asnoted above, HT individuals were categorized via clinicalhistory, physical examination, and clinical laboratory studies.
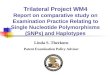
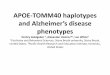
Figure 1 and Table 2 provide the RGS2 sequence and thelocation of each variant. Fourteen SNPs and 2 two-basein/dels were identified (Table 2). All of the coding sequencevariants had a minor allelic frequency �5%. In the codingregion (see Figure 1) we detected 1 nonsynonymous and 2synonymous SNPs. Three black subjects, 2 of whom wereHT, carried the Gln50Lys nonsynonymous SNP of exon 2. AtAla144(GCT) of exon 4, 2 subjects carried a T3C transition,and at Phe189 (TTC) of exon 5, 1 subject carried a C3Ttransition. The remaining 14 variants were found in noncod-ing regions with the majority located upstream of the ATGstart codon. In white subjects, 4 variants had frequencies�1%: �43 (17.5%), 1892 (22.1%), 2138 (22.1%), and 2297(19.2%). The black subjects exhibited 7 variants with afrequency �4%: �161 (4.9%), �43 (4.8%), �38 (10.1%),�3 (4.4%), 1891 to 1892 (24.8%), 2138 to 2139 (24.8%), and2297 (4.1%). �2 analysis revealed significant ethnic differ-ences in SNP frequencies for SNPs at positions �161, �43,�38, �3, and 2297 (Table 2). Association studies of geno-type with BP status revealed that the TC and AA in/dels, atpositions 1891 to 1892 and 2138 to 2139, respectively, weresignificantly associated with higher BP (P�0.05) in blacksubjects but not in white subjects (Figure 2). Other RGS2variants were not associated with BP status or BP phenotypes.
Pairwise linkage disequilibrium (LD) calculation was per-formed among the 4 most common variants (�43 A�T, 1891 to1892 TC in/del, 2138 to 2139 AA in/del, and 2297 A�G). Theresults revealed high levels of LD among these variants with theposition 1891 to 1892CT and 2138 to 2139AA in/del incomplete LD in both ethnic groups (D��1.0, �2�1.0;P�0.0001). Additionally, in both ethnic groups, SNPs located at�43 and 2297 were observed to be in near-absolute LD(D��0.956, �2�0.894; P�0.0001). Therefore, either one of thein/del or SNPs can serve as a marker for its nearby in/del or SNPin black and white populations.
Haplotype analysis revealed 11 distinct haplotypes (Table3), all of which exhibited either the presence or absence ofboth 1891 to 1892CT and 2138 to 2139AA in/del. In addition,
TABLE 1. Characteristics of Sample Population
Parameter
White Black
NT HT NT HT
n 73 55 62 60
Sex (male/female) 52/21 48/7 49/13 52/8
Age, y 42.0�1.0 57.1�1.7* 40.4�1.2 52.2�1.4*
BMI, kg/m2 25.8�0.6 30.5�1.0* 27.9�0.9 29.0�0.7
BSA, m2 1.9�0.3 2.1�0.04* 2.0�0.03 2.1�0.04*
HR 75.3�1.3 72.3�1.74 77.9�1.6 75.2�1.7
DBP 72.2�1.0 85.4�1.8* 73.3�1.4 87.5�1.9*
SBP 120.8�1.5 150.2�3.8* 126.6�2.4 149.3�3.4*
BMI indicates body mass index; BSA, body surface area; DBP, diastolic bloodpressure; SBP, systolic blood pressure. For continuous variables, values aremean�SD.
*Value significantly different from NT group (P�0.05).
2 Hypertension March 2006
by guest on March 24, 2018
http://hyper.ahajournals.org/D
ownloaded from

SNPs �43 and 2297 were in strong LD: �98% of white andblack subjects had the �43A/2297A or �43T/2297G geno-type. Haplotype analysis revealed ethnic specificity that wasnot seen in the assessment of individual allelic frequencies.Although we found no ethnic difference for individual 1891to 1892TC and 2138 to 2139AA in/dels, when analyzed incombination with the �43 and 2297 variants, substantialethnic diversity was observed. Thus, haplotype C was muchmore common in white subjects, whereas haplotype D wasmore common in black subjects. �2 analysis demonstratedthat haplotypes A and B differ significantly between HT andNT black subjects: the HT group was more likely to have
haplotype B (�2�4.55; P�0.05) and less likely to exhibithaplotype A (�2�6.33; P�0.025).
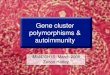
Phylogenetic haplotype analysis was conducted to infer theancestral RGS2 haplotypes and molecular evolution patternof other haplotypes (Figure 3). Analysis of all of the subjectsrevealed that haplotypes A, B, and C are the inferred ancestralhaplotypes with the fourth common haplotype D found inblack subjects derived from a mutation event in ancestralhaplotype A. Haplotypes E and G, which are present in higherfrequencies in the black subjects than white subjects, werederived from mutation events in ancestral haplotype A aswell. Haplotype K, which was only identified in a black
Figure 1. RGS2 sequence with labeledvariants. Coding regions are shown inbold and underlined. SNPs and in/delsare depicted in bold.
TABLE 2. RGS2 Variants and Allelic Frequency in White and Black Subjects
No. PositionReference SNP
(RefSNP ID)White
(n�128), %Black
(n�122), %
1. �213 G�A 0 0.9
2. �162 C�T 0 1.3
3. �161 G�T rs16834859 0.4 4.9*
4. �69 C�T 0.4 0
5. �65 G�A 0 0.4
6. �43 A>T rs12130714 17.5 4.8†
7. �38 C�T 0.4 10.1‡
8. �3 A�T 0 4.4§
9. 160 A�T 0 9
10. 180 C�G 0.4 0
11. 1132 C�A (Q50K) 0% 1.3
12. 1891 to 1892TC in/del rs3053226 22.1% 24.8
13. 2067 T�C (A144A) 0.6% 0.5
14. 2138 to 2139AA in/del rs10607546 22.1% 24.8
15. 2297 A>G rs17647363 19.2% 4.1�
16. 2456 C�T (F189F) 0.4% 0
Position indicates nucleotide position with respect to ATG start codon. Variant notation denotes major allele�minorallele, and deletions are minor variants. Variants with an allelic frequency �4% are bolded. Variants exhibiting asignificant difference between ethnicities: *�2�4.55, P�0.05; †�2�9.35, P�0.01; ‡�2�11.24, P�0.001;§�2�5.38, P�0.025; ��2�13.06, P�0.001.
Riddle et al RGS2, Hypertension, and Genetic Variation 3
by guest on March 24, 2018
http://hyper.ahajournals.org/D
ownloaded from

subject, is likely derived from a recombination event inhaplotypes E and G. The other rare haplotypes are likelyderived from recombination events of haplotypes A and C.
DiscussionOver the past decade since their discovery, RGS proteins haveemerged to become potentially important disease and drugtargets,15–17 including the possibility that their genetic variationmay contribute to disease.18 GPCRs have long been known toregulate numerous physiological processes, and, as knowledgeof RGS proteins grows, it is apparent that these proteins arelikely to be critical regulators of human physiology.4,5
RGS2, one of the best-studied RGS proteins, is found inmany tissues, including those involved in cardiovascularregulation,4,5,19,20 and as a quantitative trait locus that modu-lates anxiety in mice.21 RGS2 is unique in that it may be themost potent GAP for G�q with selectivity for that G�.22,23 Thisis likely to be physiologically important, because a widevariety of key neurotransmitters and hormones that are activein the cardiovascular system (eg, acetylcholine, norepineph-rine, angiotensin II, thromboxane A2, thrombin, and endothe-lin 1) are agonists for GPCRs that signal via G�q. In additionto GAP activity, RGS2 can bind and inhibit adenylyl cy-clase24,25 and interact with G�s,26–28 GPCRs,29 and othercomponents involved in GPCR signaling.30
Studies with RGS2-deficient mice have demonstrated thatboth homozygous and heterozygous knockout mice exhibit anHT phenotype. This suggests that genetic alterations in RGS2that produce a decrease in function and/or protein expressionlevels may contribute to the development (or exacerbation) ofhypertension. Moreover, patients with Bartter’s/Gitelman’ssyndrome, a hypotensive disorder, have enhanced expressionof RGS2, consistent with a role of RGS2 in vascular regula-tion in humans.31
In this study, we identify 16 genetic variants in the RGS2gene obtained from a population of 250 individuals of whiteand black ethnicities. Many of these variants occur at lowfrequencies (�4%) with only 3 in coding regions, 2 of whichare silent polymorphisms. We identified 1 nonsynonymousSNP, which converts a glutamine to a lysine (Gln50Lys) thatwas expressed in a heterozygous manner in 2 HT and 1 NTblack subjects. Because its allelic frequency is only 1.3%, alarge population would be required to determine whether thisvariant is associated with hypertension, implying that thisnonsynonymous variant is unlikely to be a major contributorto the HT phenotype.
By contrast, various RGS2 SNPs are found at a frequency�4% (SNPs �161, �43, �38, �3, 1891 to 1892, 2138 to 2139,and 2297), several of which show a statistically significantethnic (black versus white) specificity (SNPs �161, �43, �38,
TABLE 3. RGS2 Haplotype Distribution
No.
RGS2 Variant White Black
�161 �43 �38 �3 1891 to 1892 2138 to 2139 2297 NT (n�146), % HT (n�108), % NT (n�116), % HT (n�118), %
A. G A C A I I A 59.3 56.5 73.3 57.6*
B. G A C A D D A 21.3 23.1 7.8 16.9†
C.‡ G T C A I I G 15.3 19.4 3.4 4.2
D.§ G A T A D D A � � � 0.9 6.9 9.3
E. T A C A I I A 0.7 � � � 1.7 5.9
F. G A C A I I G 2.7 � � � � � � � � �
G. G A C G I I A � � � � � � 0.9 2.5
H G A C G D D A � � � � � � 0.9 2.5
I. G A T A I I A � � � � � � 2.6 � � �
J. G T C A I I A 0.7 � � � 1.7 � � �
K. T A C G I I A � � � � � � 0.9 0.8
n represents the No. of chromosomes sequenced; D, deletion; I, insertion. Haplotypes exhibiting a significant difference between NT and HT groups: *�2�6.33,P�0.025; †�2�4.55, P�0.05. Haplotypes exhibiting significant difference between Whites and Blacks: ‡�2�22.27, P�0.001; §�2�18.81; P�0.001.
Figure 2. In/del mutations are associatedwith hypertension in blacks. �2 analyseswere performed among hypertensive andNT white and black populations for boththe 1891 to 1892TC and 2138 to 2139AAin/dels. because both in/dels occur incomplete LD, graphs depict data foreither in/del.
4 Hypertension March 2006
by guest on March 24, 2018
http://hyper.ahajournals.org/D
ownloaded from

�3, and 2297). Two of the 16 variants, the 1891 to 1892TC and2138 to 2139AA in/del, which are in complete LD, are morecommon, each occurring 20% to 25% in both whites and blacks.These variants appear to be associated with hypertension in theblack, but not the white, population. It would be of interest todetermine whether the 1891 to 1892TC and 2138 to 2139AAin/del variants alter RGS2 activity or expression, although bothvariants are in intronic regions. The 1891 to 1892TC in/deloccurs in 17 to 18 nucleotides before the start of exon 4, at alocation that may affect splicing.
Haplotype analysis revealed additional associations be-tween genetic variation and hypertension. The frequencies ofhaplotypes A and B are significantly different among the NTand HT black populations (Table 3) suggesting that a com-bination of variants in RGS2 may be required for thepromotion of the HT phenotype.
While this article was being written, Yang et al32 describedgenetic variations of RGS2 in a Japanese population. Only 6of the 16 variants that we identified were found in thatpopulation, suggesting ethnic variation in the RGS2 gene.Neither we nor Yang et al32 observed a contribution of these6 variants (�161, �43, 1891 to 1892, 2067, 2297, and 2456)to HT status or BP in white Americans, blacks, or Japanese.Interestingly, Yang et al32 found that the 1891 to 1892 TCin/del was significantly associated with HT in Japanesewomen. We also observed an association with HT for thisvariant, albeit only in our black population with no apparentgender specificity. Approximately 40% of Japanese individ-uals in the sample of Yang et al32 had the 1891 to 1892 TCin/del, a slightly higher frequency than we noted, but the 2138to 2139 AA in/del was not found in their population, althoughwe found it was in complete LD with the 1891 to 1892 TCin/del in both whites and blacks. Perhaps the regions of DNAsequenced by Yang et al32 did not include the 2138 to 2139nucleotides.
In summary, our results indicate that RGS2 is a relativelyconserved gene with little genetic variation, in particular in itsin coding sequence. This may be indicative of the importanceof this molecule in regulating human physiology. However,the intronic 1891 to 1892TC and 2138 to 2139AA in/del, aswell as haplotype B, are associated with hypertension in
blacks and, thus, should be considered potential ethnic-specific genetic contributors to this disorder.
AcknowledgmentsThis work was supported by grants from the National Institutes ofHealth (HL69758, HL58120).
References1. Asico LD, Ladines C, Fuchs S, Accili D, Carey RM, Semeraro C,
Pocchiari F, Felder RA, Eisner GM, Jose PA. Disruption of the dopamineD3 receptor gene produces rennin-dependent hypertension. J ClinInvest. 1998;102:493–498.
2. Bengtsson K, Melander O, Orho-Melander M, Lindblad U, Ranstam J,Rastam L, Groop L. Polymorphism in the beta(1)-adrenergic receptorgene and hypertension. Circulation. 2001;104:187–190.
3. Bray MS, Krushkal J, Li L, Ferrell R, Kardia S, Sing SF, Turner ST,Boerwinkle E. Positional genomic analysis identifies the beta(2)-adrenergic receptor gene as a susceptibility locus for human hypertension.Circulation. 2000;101:2877–2882.
4. Riddle EL, Schwartzman RA, Bond M, Insel PA. Multi-tasking RGSproteins in the heart: the next therapeutic target? Circ Res. 2005;96:401–411.
5. Wieland T, Mittmann C. Regulators of G-protein signaling: multifunc-tional proteins with impact on signaling in the cardiovascular system.Pharmacol Ther. 2003;97:95–115.
6. Heximer SP, Knutsen RH, Sun X, Kaltenbronn KM, Rhee MH, Peng N,Olivera-dos-Santos A, Penninger JM, Muslin AJ, Steinberg TH, WyssJM, Mecham RP, Blumer KJ. Hypertension and prolonged vasocon-striction signaling in RGS2-deficient mice. J Clin Invest. 2003;111:445–452.
7. Tang KM, Wang G, Ping L, Karas RH, Aronovitz M, Heximer SP,Kaltenbronn KM, Blumer KJ, Siderovski DP, Zhu Y, Mendelsohn ME.Regulator of G-protein signaling-2 mediates vascular smooth musclerelaxation and blood pressure. Nat Med. 2003;9:1506–1512.
8. Sun X, Kaltenbronn KM, Steinberg TH, Blumer KJ. RGS2 is a mediatorof nitric oxide action on blood pressure and vasoconstrictor signaling.Mol Pharm. 2005;67:631–639.
9. Gross V, Tank J, Obst M, Plehm R, Blumer KJ, Diedrich A, Jordan J, LuftFC. Autonomic nervous system and blood pressure regulation in RGS2-deficient mice. Am J Physiol Regul Comp Physiol. 2005;288:R1134–R1142.
10. Murthy KK, Mahboubi VS, Santiago A, Barragan MT, Knoll R, SchultheissHP, O’Conor DT, Schork NJ, Rana BK. Assessment of multiple dis-placement amplification for polymorphism discovery and haplotype deter-mination at a highly polymorphic locus, MC1R. Hum Mutat. 2005;26:145–152.
11. Stephens M, Smith NJ, Donnelly P. A new statistical method for hap-lotype reconstruction from population data. Am J Hum Genet. 2001;68:978–989.
Figure 3. Inferred phylogeny of humanRGS2 haplotypes based on 7 of themost common variants (�161, �43,�38, �3, 1891 to 1892, 2138 to 2139,and 2297). Numbers of chromosomes(Num) for each haplotype are given.Solid arrows indicate probable pointmutations between haplotypes. Twodashed arrows converging on a haplo-type indicate a probable recombinationevent. Ancestral haplotypes differ fromone another by �2 variants. D indicatesdeletion; I, insertion; CauNT, NT white;CauHT; hypertensive white; AfrNT, NTblack; AfrHT, hypertensive black.
Riddle et al RGS2, Hypertension, and Genetic Variation 5
by guest on March 24, 2018
http://hyper.ahajournals.org/D
ownloaded from

12. Li N, Stephens M. Modeling linkage disequilibrium and identifyingrecombination hotspots using single-nucleotide polymorphism data.Genetics. 2003;165:2213–2233.
13. Stephens M, Donnelly P. A comparison of Bayesian methods for hap-lotype reconstruction from population genotype data. Am J Hum Genet.2003;73:1162–1169.
14. Halperin E, Eskin E. Haplotype Reconstruction from genotype data usingimperfect phylogeny. Bioinformatics. 2004;20:1842–1849.
15. Huailing Z, Neubig RR. Regulator of G protein signaling proteins: novelmultifunctional drug targets. J Pharmacol Exp Ther. 2002;297:837–845.
16. Neubig RR. Regulators of G protein signaling (RGS proteins): novelcentral nervous system drug targets. J Peptide Res. 2002;60:312–316.
17. Chasse SA, Dohlman HG. RGS proteins: G protein-coupled receptorsmeet their match. Assay Drug Dev Technol. 2003;1:357–364.
18. Berman DM, Wang Y, Liu Z, Dong Q, Burke LA, Liotta LA, Fisher R,Wu X. A functional polymorphism in RGS6 modulates the risk of bladdercancer. Cancer Res. 2004;64:6820–6826.
19. Grant SL, Lassegue B. Griendling KK, Ushio-Fukai M, Lyons PR,Alexander RW. Specific regulation of RGS2 messenger RNA by angiotensinII in cultured vascular smooth muscle cells. Mol Pharm. 2000;57:460–467.
20. Larminie C, Murdock P, Walhin JP, Duckworth M, Blumer KJ,Scheideler MA, Garnier M. Selective expression of regulators ofG-protein signaling (RGS) in the human central nervous system. BrainRes Mol Brain Res. 2004;122:24–34.
21. Yalcin B, Willis-Owen SA, Fullerton J, Meesaq A, Deacon RM, RawlinsJN, Copley RR, Morris AP, Flint J, Mott R. Genetic dissection of abehavioral quantitative trait locus shows that RGS2 modulates anxiety inmice. Nature Genet. 2004;36:1145–1147.
22. Heximer SP, Watson N, Linder ME, Blumer KJ, Hepler JR. RGS2/GOS8is a selective inhibitor of Gqalpha function. Proc Natl Acad Sci U S A.1997;94:14389–12393.
23. Heximer SP, Srinivasa SP, Bernstein LS, Bernard JL, Linder ME, HeplerJR, Blumer KJ. G protein selectivity is a determinant of RGS2 function.J Biol Chem. 1999;274:34253–34259.
24. Salim S, Sinnarajah S, Kehrl JH, Dessauer CW. Identification of RGS2and type V adenylyl cyclase interaction sites. J Biol Chem. 2003;278:15842–15849.
25. Sinnarajah S, Dessauer CW, Srikumar D, Chen J, Yuen J, Yilma S,Dennis JC, Morrison EE, Vodyanoy V, Kehrl JH. RGS2 regulates signaltransduction in olfactory neurons by attenuating activation of adenylylcyclase III. Nature. 2001;409:1051–1055.
26. Tseng CC, Zhang XY. Role of regulator of G protein signaling indesensitization of the glucose-dependent insulinotropic peptide receptor.Endocrinology. 1998;139:4470–4475.
27. Ko JK, Choi KH, Kim IS, Jung EK, Park DH. Inducible RGS2 is a cross-talkregulator for parathyroid hormone signaling in rat osteoblast-like UMR106cells. Biochem Biophys Res Commun. 2001;287:1025–1033.
28. Roy AA, Baragli A, Bernstein LS, Hepler JR, Hebert TE, Chidiac P.RGS2 interacts with Gs and adenylyl cyclase in living cells. Cell Signal.2006;18:336–348.
29. Hague C, Bernstein LS, Ramineni S, Chen Z, Minneman KP, Hepler JR.Selective inhibition of alpha1A-adrenergic receptor signaling by RGS2association with the receptor third intracellular loop. J Biol Chem. 2005;280:27289–27295.
30. Wang X, Zeng W, Soyombo AA, Tang W, Ross EM, Barnes AP,Milgram SL, Penninger JM, Allen PB, Greengard P, Muallem S. Spi-nophilin regulates Ca2� signalling by binding the N-terminal domain ofRGS2 and the third intracellular loop of G-protein-coupled receptors.Nature Cell Biol. 2005;7:405–411.
31. Calo LA, Pagnin E, Davis PA, Sartori M, Ceolotto G, Pessina AC,Semplicini A. Increased expression of regulator of G protein signaling-2(RGS-2) in Bartter’s/Gitelman’s syndrome. A role in the control ofvascular tone and implication for hypertension. J Clin Endocrinol Metab.2004;18:4153–4157.
32. Yang J, Kamide K, Kokubo Y, Takiuchi S, Tanaka C, Banno M,Yoshikazu M, Masayoshi Y, Takeshi H, Okayama A, Tomoike H,Kawano Y, Miyata T. Genetic variations of regulator of G-protein sig-naling 2 in hypertensive patients in the general population. J Hypertens.2005;23:1497–1505.
6 Hypertension March 2006
by guest on March 24, 2018
http://hyper.ahajournals.org/D
ownloaded from

O'Connor and Paul A. InselEvan L. Riddle, Brinda K. Rana, Kenton K. Murthy, Fangwen Rao, Eleazar Eskin, Daniel T.
Normotensives and HypertensivesPolymorphisms and Haplotypes of the Regulator of G Protein Signaling-2 Gene in
Print ISSN: 0194-911X. Online ISSN: 1524-4563 Copyright © 2006 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Hypertension published online January 23, 2006;Hypertension.
http://hyper.ahajournals.org/content/early/2006/01/23/01.HYP.0000200714.81990.61.citationWorld Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://hyper.ahajournals.org//subscriptions/
is online at: Hypertension Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer this process is available in the
click Request Permissions in the middle column of the Web page under Services. Further information aboutOffice. Once the online version of the published article for which permission is being requested is located,
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the EditorialHypertensionin Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on March 24, 2018
http://hyper.ahajournals.org/D
ownloaded from