Embed Size (px)
Citation preview

DBA TEC
Age Infancy 1-3y/o
Inherited? Inherited? Acquired
Antecedent illness No Viral illness
Abnormal facies/anomalies
Yes: 25-50% No
RBC Adenosine Deaminase
High Normal
MCV High Normal(?high in recovery)
Hgb F High Normal(?high in recovery

Differences: DBA and TEC
DBA may be considered premalignant syndrome
• Laughing: Pediatric Boards
DBA TEC
Spontaneous Recovery Rarely Almost always
Transfusion Common Uncommon
Steroids Helpful No
Incidence Rare Common

CAUTION!Both DBA and Fanconi Anemia can have:
Thumb abnormalities, urogenital defects, severe anemia
DBA will typically be ISOLATED ANEMIA

Think about it
12 month oldSevere anemia (Hbg 3)Recent viral illnessReticulocytosis
TEC in recovery phase

Question 5
Name the syndrome which is characterized by microangiopathic hemolytic anemia caused by a giant hemangioma.
A: Stendhal Syndrome B: Kasabach-Merritt Syndrome C: Capgras Syndrome D: Cotard Syndrome
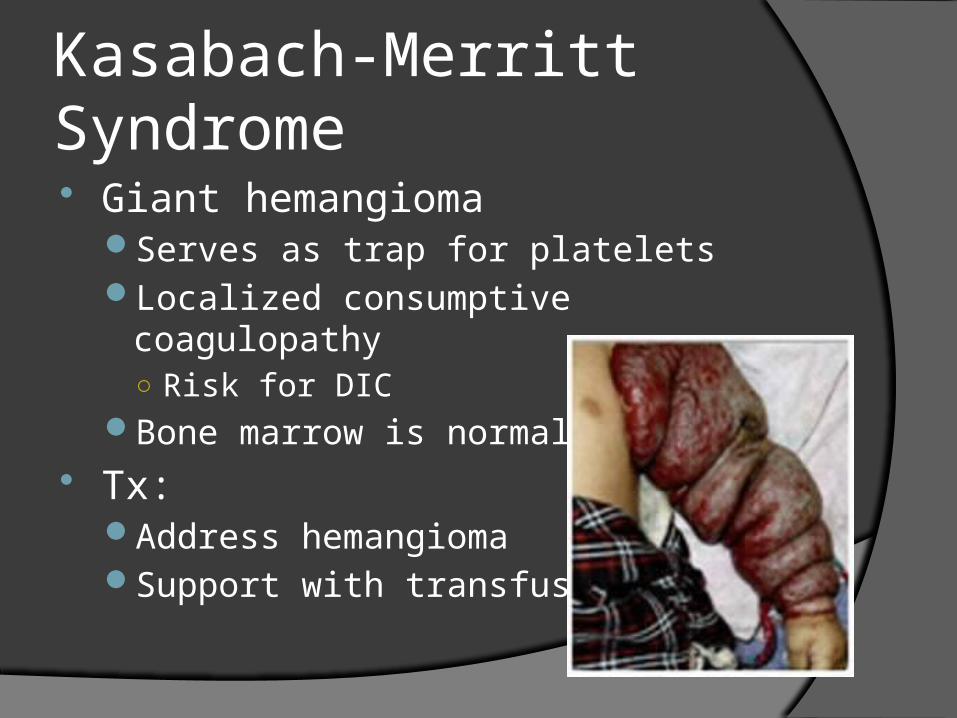
Kasabach-Merritt Syndrome Giant hemangioma
Serves as trap for plateletsLocalized consumptive coagulopathy
○ Risk for DICBone marrow is normal
Tx:Address hemangiomaSupport with transfusions

White blood cells

Leukemoid Reaction
Differentiated from leukemia by B.M. Biopsy
Leukocyte alkaline phosphatase (LAP)Increased in leukemoid reaction
Down SyndromeTransient leukemoid reaction as neonate20-30% of these: leukemia in 1st 3 yrs of life

Reilly (Alder-Reilly) Bodies WBC metachromatic prominent granules
Stained with toluidine blue Pathognomonic for Hurler syndrome


Question 6
A previously healthy 4 year old girl is seen for petechiae and diffuse bruises. She is anxious but afebrile, alert and not in any distress. She is noted to have bleeding from the gums and moderately severe epistaxis. Lab studies reveal: Hgb 12.5; WBC 7 with a normal diff; platelets 4000. Part of the initial management would include . . . . .
A. Immediate bone marrow exam for suspected leukemia
B. Blood cultures and IV antibiotics
C. Careful PE, review of the smear and consideration of IVIG therapy
D. Type and cross match and infusion of FFP
E. Emergency splenectomy following platelet transfusion

Bleeding Disorders

Bleeding DisordersDisorders of Platelets Coagulopathies
Mucocutaneous bleeding Purpura Petechiae Ecchymoses
Deep tissue bleeding Joint bleeds
Bleeding Disorders
Bleeding in either may beTraumaSurgeryHematuriaGuaiac-positive stoolsMenorrhagiaCNS bleeding
EpistaxisMore likely to be nose picking, dry mucous
membranes or rarely HTN

Bleeding Disorders
EvaluationCBC c diffPlatelet countPTPTTBleeding time or closure time

Platelet Disorders Isolated Thrombocytopenia
Idiopathic or immune thrombocytopeniasHypersplenismDICConsumption
○ Intracardiac defect or bypassWashout from exchange transfusionLocal microangiopathic disease
○ HUSLocal thrombosis
○ Renal vein thrombosis

Platelet Disorders ITP
Look at the smear!Large platelets = platelet
destructionHx
○ Recent viral infectionTx
○ IVIG○ Anit-D antibody
Only if pt is Rh positive
○ Splenectomy when unresponsive
Bone marrow○ When unresponsive

Platelet Disorders Isoimmune Thrombocytopenia in the Newborn
Fetal platelets cross the placenta into maternal circulation
Maternal IgG produced against the platelet antigenSuspect when
○ Maternal platelets normalRisk
○ Cephalohematoma○ Bleeding from umbilicus○ ICH
Tx○ Washed maternal platelets○ IVIG

Platelet Disorders Decreased production =
decreased or absent megakaryocyte precursorsTAR syndrome
○ Thrombocytopenia-absent radius Amegakaryocytic
thrombocytopenia○ Leukemoid reactions○ CHD○ FTT
In both conditions, thrombocytopenia resolves with age

Platelet Disorders
Qualitative or functional platelet disordersNormal number and clotting studies but
poorly functioning plateletsFirst ask for history of . . .
○ Drug exposure○ Uremia○ Hypothyroidism○ Hyperbilirubinemia ○ IBD
Von Willebrand disease
Question 7A 16 month old boy is brought to the ER with persistent crying and
refusal to move his right arm. The history is negative for fever and trauma. Past history is significant for bleeding from his circumcision and easy bruising. PE shows boggy, tender swelling of the right elbow with marked decrease in ROM. The Hb is 11.2; WBC, plts and inflammatory markers are normal. You plan would be . . . .
A. Obtain a skeletal survey to r/o child abuse
B. Admit the patient for evaluation of a bone tumor
C. Request an orthopedic consultation for aspiration of the elbow joint.
D. Obtain a FH, PT, PTT, factor assay and consider factor replacement therapy
E. Close monitoring of the patient w/o intervention for the presumptive diagnosis of HSP

Coagulopathies Deficiency in factors Causes
Decreased production○ Genetic defects○ Acquired conditions
Overutilization of factors Testing
PT○ Extrinsic and common
PTT○ Intrinsic and common
Make sure you check age related values

Coagulopathies Hemophilia A (VIII) and B (IX)
X-linked recessive○ Males
Prolonged PTTVariable degrees of deficiency and diseaseMild
○ 5-30% factor activity○ Bleeding with surgery or major trauma
Moderate○ 1-5% factor activity○ Localized hemorrhage in response to trauma
Severe○ <1% factor activity○ Spontaneous soft tissue hemorrhages or bleeding with minor
trauma

Coagulopathies Hemophilia
Presentation○ Birth
Circumcision
○ 12-18 months Increased mobility and bleeding with
minor trauma
○ Most commonly affected systemsMusculoskeletal
- Hemarthroses- Soft tissue bleeding with
intramuscular hematomasCNSUrinary

Coagulopathies
HemophiliaSecondary hemophiliac
arthropathy○ Knees ○ Elbows○ Ankles
ContracturesPainful arthritis Compartment
syndrome○ Intramuscular bleeding

Von Willebrand Disease Most common heritable bleeding disorder Bleeding time or closure time is increased
with or without an increase in the PTT Most are AD Most are asymptomatic and found
incidentally If symptomatic
Abnormal mucosal bleeding○ Frequent epistaxis○ Menorrhagia

Von Willebrand Disease
What does VWF do?Responsible for the adherence of platelets
to damaged endotheliumRequired for normal Factor VIII function
TypesI and III
○ Quantitative○ I is most common
II○ Qualitative

Von Willebrand Disease Testing
Von Willebrand factor antigenVon Willebrand factor ristocetin cofactor activityFactor VIII levels
TreatmentDDAVP
○ Causes release of factor stores from platelets and endothelial cells
○ QuantitativeFactor replacement
○ Donor blood products○ Qualitative

Acquired Disorders
InhibitorsTesting
○ Mix patients plasma with normal plasma○ PT or PTT will fail to correct
Example○ Lupus anticoagulant
Actually predisposes to thrombosis
○ 10% of patients with Lupus○ Also acquired after some medications or other
infectious organisms○ Persists for months

Thrombotic disorders

Thrombosis
Disruption in the balance of procoagulant and antithrombotic factors
Rare in childrenInfants and
adolescents Incidence increasing
Due to use of indwelling lines

Thrombosis Increased risk
Retardation of blood flow○ Severe dehydration○ Immobilization
Endothelial damage○ Indwelling catheters
Family historyPast history of thrombosisRecurrent spontaneous abortionsThrombosis during pregnancyNephrotic syndrome

Thrombosis
Protein C Vitamin K dependentInhibits procoagulant factors Va and VIIIaDecreases clot formation
Protein SCofactor required for anticoagulant activity
of protein C Deficiency of either leads to clot
formation

Thrombosis Antithrombin III
Inhibitor○ Complexes with thrombin, factor Xa and factor IXa
Deficiency lead to loss of inhibition and thrombosis Paroxysmal Nocturnal Hemoglobinuria
RareCells with an increased sensitivity to complementLeads to
○ Abdominal and back pain○ Chronic intravascular hemolysis○ Intermittent hemoglobinuria○ Diffuse venous thrombosis

Thrombosis Factor V Leiden
Mutations lead to protein C resistance○ Can’t degrade procoagulant factors
Factor II prothrombin gene variantIncreased factor II
Methylene tetrahydrofolate reductase (MTHFR) gene mutationThermolabile variantIncreased plasma homocyteine levels
Genetic testing may be doneNot affected by anticoagulants

Question 8
An infant you are seeing in the newborn nursery is born with hypoplastic thumbs and some abnormal skin pigmentation. You suspect that the patient may have Fanconi’s anemia. What test should confirm the diagnosis?
A. Chromosomal analysis
B. Bone Marrow Biopsy
C. CBC with peripheral smear
D. CBC with reticulocyte count
E. CBC with diff

Pancytopenia

Pancytopenia
DefinitionReduction in all three formed elements of
the blood
Results from a number of disease processesBone marrow failureDepressed marrow function and increased
cellular destruction

Aplastic Anemia Insult to the bone marrow
Drugs Toxins Solvents Radiation Autoimmune Postinfectious Idiopathic
○ 50%
Bone marrow failure Death from infection or
bleeding unless there is an intervention

Fanconi Anemia Autosomal recessive Signs
Pancytopenia○ Marrow hypoplasia
Congenital anomalies○ Abnormal skin pigmentation○ Growth retardation○ Skeleton
Absent or hypoplastic thumb
○ CNS ○ GU
Testing Fragility of the chromosomes
○ Breaks, gaps and rearrangements
Treatment Frequent transfusions Bone marrow transplant






















