Embed Size (px)
Citation preview

ELSEVIER
Cytogenetics of Gastric and Esophageal Adenocarcinomas 3q Deletion as a Possible Primary Chromosomal Change
Pulivarthi H. Rao, Susan Mathew, David P. Kelsen, and R. S. K. Chaganti
ABSTRACT: We report clonal chromosome abnormalities in short term cultures of seven gastric or esophageal adenocarcinomas and two squamous carcinomas of the esophagus and EG junction. The mast consistent aberration encountered was a del(3)(q13. 2q23) seen in six of nine tumors. This finding, together with a survey of published cytogenetic literature, suggested that del(3q) is the most common cytogenetic abnormality, and hence possibly of primary significance, in these tumors. In addition to del(3q), rear- mngements affecting lp13 (two cases), 6q15-q23 (two cases), 7p22 (two cases), 7q22 (two cases), and 11p11.2- p14 (three cases) were seen. Cytogenetic evidence for gene amplification in the form of homogeneously staining region (hsr) was seen at 9q13 in two cases.
INTRODUCTION
Relatively few adenocarcinomas of gastric and esophageal origin have been analyzed cytogenetically. Because of tech- nical difficulties encountered in solid tumor cytogenetics in general, and in the analysis of gastric and esophageal adenocarcinomas in particular, clonally abnormal karyotypes have been published for only 43 cases [1-11). So far, only one study described non-random structural aberrations affecting the 11p13-15 region in adenocarcinomas of the stomach and esophagus [8]. We report here detailed chromosomal analy- sis of nine gastric and esophageal adenocarcinomas.
MATERIALS AND METHODS
Tumor tissues were obtained from a consecutively ascer- tained series of patients with gastric (five cases), esophageal (one case), and GE junction (three cases) cancers who un- derwent surgery at the Memorial Sloan Kettering Cancer Cen- ter. Of the nine patients with successful cytogenetic analy- sis, six were male and three were female. Tumor tissues for cytogenetic analysis were processed according to the method previously described by us [8].
From the Cell Biology and Genetics Program and the Cytogenetic Service (P. H. R., S. M., R. S. K. C.), Department of Pathology and Department of Medicine (D. P. K.), Memorial Sloan Kettering Can- cer Center, New York, New York.
Address reprint requests to: Dr. Pulivarthi H. Rao, Box #391, Memorial Sloan Fettering Cancer Center, 1275 York Avenue, New York, NY 10021.
Received January 12, 1994; accepted June 2, 1994.
Cancer Genet Cytogenet 81 :139-143 (1995) © Elsevier Science Inc., 1995 655 Avenue of the Americas , N e w York, NY 10010
Cytogenetic Analysis
Cells for cytogenetic analysis were harvested following short- term culture (1-10 days after seeding). Metaphase prepara- tions were G-banded for karyotypic analysis. Karyotypes were described according to ISCN (1991) [12]. Clonality was de- fined by the detection of two cells with the same structural abnormality or non-random gain of a given chromosome or three cells with loss of a given chromosome.
RESULTS
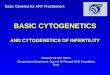
Of the 62 tumors processed for cytogenetic analysis, abnor- mal clones were found in nine tumors, six showed normal karyotypes, and the remaining 47 cultures were unsuccess- ful. Nine tumors and one cell line derived from one tumor (l16A) analyzed in the present study had clonal chromosome abnormalities. The modal chromosome numbers were near- diploid and hyperdiploid in one tumor each, near-triploid in two tumors, hypotriploid in one tumor, hypertriploid in two tumors, near-tetmploid in one tumor, and hypertetraploid in one tumor. Table 1 summarizes the histopathologic and cytogenetic data on the nine fresh tumors and the cell line. Chromosomes 1, 3, 7, 9, and 11 were frequently involved in structural abnormalities.
Numerical changes included loss of the X chromosome in three cases and loss of the Y chromosome in one case. Gain of chromosomes 1 and 12 were noted in three cases. No major differences in types of abnormalities were encoun- tered in adenocarcinomas of the stomach, esophagus, or in the junction between stomach and esophagus.
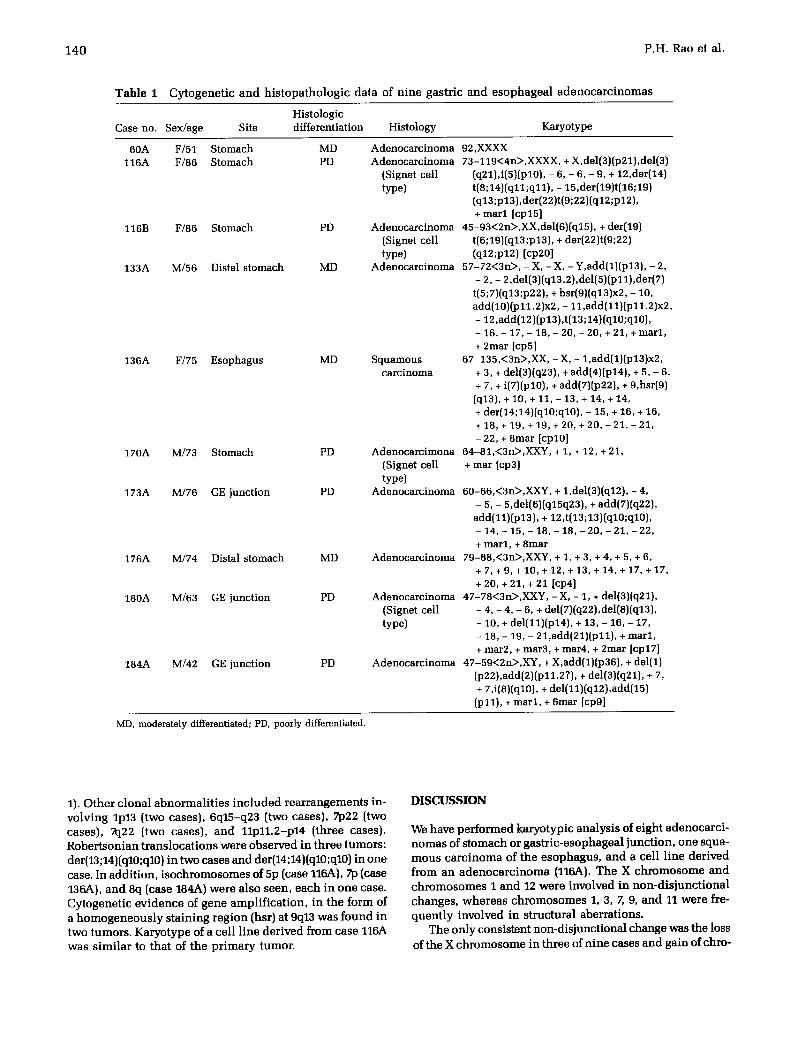
The most frequent structural aberration encountered was a del(3q)(q13q23), which was seen in six of nine tumors (Fig.
0165-4608/95/$9.50 SSDI 0165-4608(94)00113-P
1 4 0 P . H . R a o e t a l .
T a b l e 1 C y t o g e n e t i c a n d h i s t o p a t h o l o g i c d a t a o f n i n e g a s t r i c a n d e s o p h a g e a l a d e n o c a r c i n o m a s
His to logic Case no. Sex/age Site d i f ferent ia t ion His to logy Karyo type
60A F/51 S t o m a c h MD 116A F/86 S t o m a c h PD
116B F/86 S t o m a c h PD
133A M/56 Distal s t o m a c h MD
136A F/75 E s o p h a g u s MD
170A M/73 S t o m a c h
173A M/76 GE j unc t i on
176A M/74 Distal s t o m a c h MD
180A M/63 GE j unc t i on PD
184A M/42 GE j unc t i on PD
PD A d e n o c a r c i m o n a (Signet cell type)
PD A d e n o c a r c i n o m a
A d e n o c a r c i n o m a 92,XXXX A d e n o c a r c i n o m a 73-119<4n>,XXXX, +X,del(3)(p21),del(3)
(Signet cell (q21),i(5)(p10), - 6, - 6, - 9, + 12,der(14) type) t (8 ;14) (q11;q11) , - 15,der(19)t(16;19)
(q13;p13),der(22)t(9;22)(q12;p12), + m a r l [cp15]
A d e n o c a r c i n o m a 45-93<2n>,XX,del (6) (q15) , + der(19) (Signet cell t(6;19)(q13;p13), + der(22)t(9;22) type) (q12;p12) [cp20]
A d e n o c a r c i n o m a 5 7 - 7 2 ( 3 n > , - X, - X, - Y,add(1)(p13), - 2, - 2, - 2,del(3)(q13.2),del(5)(p11),der(7)
t(5;7)(q13;p22), + hsr(9)(q13)x2, - 10, add(10)(p11.2)x2, - 11,add(11)(p11.2)x2, - 12,add(12)(p13), t(13;14)(q10;q10), - 16, - 17, - 18, - 20, - 20, + 21, + m a r l , + 2mar [cpS]
S q u a m o u s 6 7 - 1 3 5 , ( 3 n > , X X , - X, - 1,add(1)(p13)x2, c a r c i n o m a + 3, + del(3)(q23), + add(4)(p l4) , + 5, - 6,
+ 7, + i(7)(p10), + add(7)(p22), + 9,hsr(9) (q13), + 10, + 11, - 13, + 14, + 14, + der(14;14)(q10;q10), - 15, + 16, + 16, + 18, + 19, + 19, + 20, + 20, - 21, - 21, - 22, + 8 m a r [cpl0]
64 -81 ,<3n> ,XXY, + 1, + 12, + 21, + mar [cp3]
60 -66 ,<3n> ,XXY, + 1,del(3)(q12), - 4, - 5, - 5,del(6)(q15q23), + add(7)(q22),
add(11)(p13), + 12,t(13;13)(q10;q10), - 1 4 , - 1 5 , - 1 8 , - 1 8 , - 2 0 , - 2 1 , - 22, + m a r l , + 8 m a r
A d e n o c a r c i n o m a 79-88 ,<3n> ,XXY, + 1, + 3, + 4, + 5, + 6, + 7 , + 9 , +10 , + 12, + 13 ,+ 14 ,+ 17, + 17, + 20, + 21, + 21 [cp4]
A d e n o c a r c i n o m a 4 7 - 7 8 < 3 n > , X X Y , - X , - 1, + del(3)(q21), (Signet cell - 4, - 4, - 6, + del(7)(q22),del(8)(q13), type) - 10, + del(11)(p14), + 13, - 16, - 17,
- 18, - 19, - 21,add(21)(p11), + m a r l , + mar2 , + mar3 , + mar4, + 2mar [cp17]
A d e n o c a r c i n o m a 4 7 - 5 9 < 2 n > , X Y , + X,add(1)(p36), + del(1) (p22),add(2)(p11.27), + del(3)(q21), + 7, + 7,i(8)(q10), + del(11)(q12),add(15) (p11), + m a r l , + 6mar [cpg]
MD, moderately differentiated; PD, poorly differentiated.
1). O t h e r c l o n a l a b n o r m a l i t i e s i n c l u d e d r e a r r a n g e m e n t s i n -
v o l v i n g l p13 ( two c a s e s ) , 6 q 1 5 - q 2 3 ( two c a s e s ) , 7p22 ( two c a s e s ) , 7q22 ( two c a s e s ) , a n d 1 1 p 1 1 . 2 - p 1 4 ( t h r e e c a s e s ) .
R o b e r t s o n i a n t r a n s l o c a t i o n s w e r e o b s e r v e d i n t h r e e t u m o r s :
der(13;14)(q10;q10) i n t w o c a s e s a n d der(14;14)(q10;q10) i n o n e
case . I n a d d i t i o n , i s o c h r o m o s o m e s o f 5p ( c a s e 116A), 713 ( ca se
136A), a n d 8 q ( c a s e 184A) w e r e a l s o s e e n , e a c h i n o n e ca se .
C y t o g e n e t i c e v i d e n c e o f g e n e a m p l i f i c a t i o n , i n t h e f o r m o f
a h o m o g e n e o u s l y s t a i n i n g r e g i o n (hs r ) a t 9q13 w a s f o u n d i n t w o t u m o r s . K a r y o t y p e o f a c e l l l i n e d e r i v e d f r o m c a s e 116A
w a s s i m i l a r to t h a t o f t h e p r i m a r y t u m o r .
D I S C U S S I O N
W e h a v e p e r f o r m e d k a r y o t y p i c a n a l y s i s o f e i g h t a d e n o c a r c i -
n o m a s o f s t o m a c h o r g a s t r i c - e s o p h a g e a l j u n c t i o n , o n e s q u a - m o u s c a r c i n o m a o f t h e e s o p h a g u s , a n d a c e l l l i n e d e r i v e d
f r o m a n a d e n o c a r c i n o m a (116A). T h e X c h r o m o s o m e a n d
c h r o m o s o m e s 1 a n d 12 w e r e i n v o l v e d i n n o n - d i s j u n c t i o n a l
c h a n g e s , w h e r e a s c h r o m o s o m e s 1, 3, 7, 9, a n d 11 w e r e f re -
q u e n t l y i n v o l v e d i n s t r u c t u r a l a b e r r a t i o n s . T h e o n l y c o n s i s t e n t n o n - d i s j u n c t i o n a l c h a n g e w a s t h e l o s s
o f t h e X c h r o m o s o m e i n t h r e e o f n i n e c a s e s a n d g a i n o f c h r o -

Gastric and Esophageal Adenocarcinomas 141
136A f
173A
180A
1114 A
Figure 1. Partial karyotypes of six of the tumors studied show- ing deletions affecting 3q13.2-q23.
mosomes I and 12 in three cases. Loss of the Y chromosome has previously been reported in gastric and esophageal adenocarcinomas by conventional cytogenetics, as well as by interphase cytogenetics by FISH [8,13,14]. In this study, we found the loss of the Y chromosome in only one case.
Deletion (3p) has been reported previously in many epi- thelial tumors; e.g., small cell lung carcinoma [15] and car- cinomas of kidney [16], ovary [17], breast [18,19], and stom- ach [8] and one or more candidate tumor suppressor genes have been postulated [20]. In the present study we found del(3) (p21) in only one tumor (116A). Interestingly, we found del(3q) (q13.2q23) in six of nine tumors leading to loss of 3q material. This finding prompted us to review cytogenetic data
0
0 0
0
0
N
m o ~
i
+
& £
I

142 P.H. Rao et al.
on the 3q deletions reported in gastric and esophageal adenocarcinomas. Structural changes affecting 3(t11-<127 have been reported in 17 of 52 (33%) of these tumors, inc luding the present study (Table 2). Rodriguez et al. [8] reported two cases with structural aberration affecting the 3q21 band. Xiao et al. reported three cases affecting 3q11-q21 region in gas- tric adenocarcinomas. Bullerdiek et al. [4], Ochi et al. [5], and Tzeng et al. [9] noted the structural aberrations affect- ing 3q25, 3q21, and 3q27, respectively, in one tumor each. The del(3q) reported here, as in the publ ished cytogenetics. literature, suggests that this abnormali ty may be a frequent and hence possibly a primary event in these tumors. Fur- ther, this finding may represent a feature important in a subset of epithelial tumors, indicating loss of a candidate tumor sup- pressor gene(s). Recent allelotype analysis in osteosarcomas strongly suggests the existence of tumor suppressor gene(s) on the long arm of chromosome 3 [21].
Chromosome 11 was involved in structural aberration in four of n ine tumors with clustering of breakpoints at 11p11.2, 11p13, 11p14, and 11q12. Rodriguez et al. [8] reported non- random rearrangements involving the region 11p13-15 in eight of n ine tumors. Cagle et al. [7] reported a case with a deletion at 11p12. Recently, Seruca et al. [11] reported rear- rangements affecting 11p13-p15 in two cases. Genetic changes affecting the 11p13-15 region have previously been reported in several types of solid tumors, notably hepatoblastoma [22] and carcinomas of the bladder [23] and breast [24]. It has been suggested that these changes may indicate loss of a tu- mor suppressor gene(s) [2 2-24]. However, no loss of hetero- zygosity affecting polymorphic DNA markers on 11p has been found in a study of 41 gastric tumors [25]. Other structural aberrations observed inc luded rearrangements involving lp13, 7p22, X122, and 9q13.
We found no major differences in types of chromosome abnormalities in adenocarcinomas developing in the gastric, lower esophageal, and junct ion region, suggesting a com- mon pathway of origin at all three anatomical sites.
The non-random structural aberration reported earlier af- fecting the 11p13-p15 region and the present site at 3(t13.2-q23 identified in the present study may represent two different sites of importance in the etiology of gastric and esophageal adenocarcinomas. Further molecular studies are needed to define the precise region of aberration in these demonstrated sites.
This investigation was supported in part by the NIH grants CA-05826 and CA-08748. We thank Marc Ladanyi for reviewing histopathol- ogy of the cases.
R E F E R E N C E S
1. Van der Riet-Fox MF, Retief AE, Van Niekerk WA (1979): Chro- mosome changes in 17 human neoplasms studied with band- ing. Cancer 44: 2108-2119.
2. Togawa A, Hasegawa K, Mitake T, Mannoji M, Takemoto Y, Yamada O, Miyajima K, Yoshlmoto M, Yawata Y, Yamada K (1981): A chromosome analysis in a patient with chronic myelogenous leukemia and gastric cancer. Acta Haematol Jpn 44:590-594.
3. Ochi H, Takeuchi J, Douglass HO Jr, Sandberg AA (1984): Trisomy X as a possible initial chromosome change in a gastric cancer. Cancer Genet Cytogenet 12:57-61.
4. Bullerdiek J, Bartnitzke S, Kahrs E, Schloot W (1985): Further evidence for non-random chromosome changes in carcinoma cells. A report of 28 cases. Cancer Genet Cytogenet 16:33-43.
5. Ochi H, Douglass HO Jr, Sandberg AA (1986): Cytogenetic studies in primary gastric cancer. Cancer Genet Cytogenet 22:295-307.
6. Ferti-Passantonopoulou AD, Panani AD, Vlachos JD, Raptis SA (1987): Common cytogenetic findings in gastric cancer. Cancer Genet Cytogenet 21:361-364.
7. Cagle PT, Taylor LD, Schwartz MR, Ramzy I, Elder FFB (1989): Cytogenetic abnormalities common to adenocarcinoma meta- static to the pleura. Cancer Genet Cytogenet 39:219-225.
8. Rodriguez E, Rao PH, Ladanyi M, Altorki N, Albino AP, Kelsen DP, Jhanwar SC, Chaganti RSK (1990): 11p13-15 Is a specific re- gion of chromosomal rearrangement in gastric and esophageal adenocarcinomas. Cancer Res 50:6410-6416.
9. Tzeng CC, Meng CL, Jin L, Hsieh HF (1991): Cytogenetic studies of gastric adenocarcinoma. Cancer Genet Cytogenet 55:67-71.
10. Xiao S, Geng JS, Feng XL, Liu XO~ Liu QZ, Li P (1992): Cytogenetic studies of eight primary gastric cancers. Cancer Ge- net Cytogenet 58:79-84.
11. Senlca R, Castedo S, Correia C, Gomes P, Carneiro F, Soares P, de Jong B, Sibrinho-Simoes M (1993): Cytogenetic findings in eleven gastric carcinomas. Cancer Genet Cytogenet 68:42-48.
12. ISCN (1991): Guidelines for Cancer Cytogenetics, Supplement to An International System for Human Cytogenetic Nomencla- ture, F Mitelman (ed); S. Karger; Basel.
13. van Dekken H, Pizzolo JG, Kelsen DP, Melamed MR (1990): Tar- geted cytogenetic analysis of gastric tumors by in sitn hybrid- ization with a set of chromosome-specific DNA probes. Cancer 66:491-497.
14. Rao PH, Mathew S, Lauwers G, Rodriguez E, Kelsen DP, Chaganti RSK (1993): Intarphase cytogenetics of gastric and esophageal adenocarcinomas. Diagn Mol Pathol 2(4):264-268.
15. Whang-Peng J, Bunn Jr PA, Kao-Shan CS, Lee EC, Carney DN, Gazdar A, Minna JD (1982): A nonrandom chromosomal abnor- mality, del 3p(14-23), in human small cell lung cancer (SCLC). Cancer Genet Cytogenet 15:335-347.
16. Kovacs G, Frisch S (1989): Clonal chromosome abnormalities in tumor cells from patients with sporadic renal cell carcinomas. Cancer Res 49:651-659.
17. Pejovic T, Heim S, Mandahl N, Baldetorp B, Elmfors B, Folderus UM, Furgyik S, Helm G, Himmelmann A, Willen H, Mitelman F (1992): Chromosome aberrations in 35 primary ovarian carci- nomas. Genes Chromosomes & Cancer 4:58-68.
18. Zhang R, Wiley J, Howard SP, Meisner LF, Gould MN (1989): Rare clonal karyotypic variants in primary cultures of human breast carcinoma cells. Cancer Res 49:444-449.
19. Pandis N, Jin Y, Limon J, Bardi G, Idvall I, Mandahl N, Mitel- man F, Heim S (1993): Interstitial deletion of the short arm of chromosome 3 as a primary chromosome abnormality in carci- nomas of the breast. Genes Chromosomes & Cancer 6:151-155.
20. Yokoyama S, Yamakawa K, Tsuchiya E, Murata S, Sakiyama S, Nakamura Y (1992): Deletion mapping on the short arm of chro- mosome 3 in squamous cell carcinoma and adenocarcinoma of the lung. Cancer Res 52:873-877.
21. Yamaguchi T, Toguchida J, Yamamura T, Kotoura Y, Takada N, Kawaguchi N, Kaneko Y, Nakamura Y, Sasaki MS, Ishizaki K (1993): Allelotype analysis in osteosarcomas: Frequent allele loss on 3q, 13q, 17p, and 18q. Cancer ires 52:2419-2423.
22. KOuios A, Hansen ME Copeland NG, Jenkins NA, Lampkin BC,

Gastr ic and Esophagea l A d e n o c a r c i n o m a s 143
23.
Cavanee WK (1985): Loss of heterozygosity in three embryonal tumors suggests a common pathogenic mechanism. Nature (Lon- don) 316:330-334.
Fearon ER, Fienberg AP, Hamilton SH, Vogelstein B (1985): Loss of genes on the short arm of chromosome 11 in bladder cancer. Nature (London) 318:377-380.
24. Theillet C, Lidereau R, Escot C, Hutzell P, Brunet M, Gest J, Schlom J, Callahan R (1986): Loss of a c-H-ms-1 allele and ag- gressive human primary breast carcinomas. Cancer Res 46: 4776-4781.
25. Wada M, Yokota J, Mizoguchi H, Sugimura T, Terada M (1988): Infrequent loss of chromosomal heterozygosity in human stom- ach cancer. Cancer Res 48:2988-2992.